Investigations on subjective and objective cyclorotatory...
8
Investigations on Subjective and Objective Cyclorotatory Changes After Inferior Oblique Muscle Recession Hermann Dieter Schworm, Silvia Eithoff, Markus Schaumberger, and Klaus-Peter Boergen Purpose. To determine subjective and objective cyclorotatory changes after surgery for oblique muscle disorders and to analyze the mechanisms of the well-known, long-term, postoperative, subjective cyclotorsional changes. Methods. Twenty-six patients underwent unilateral inferior oblique muscle recession for strabis- mus sursoadductorius (inferior oblique overfunction). Subjective and objective cyclodeviation were examined before surgery with and without diagnostic occlusion, as well as 1 day, 3 days, and 4 months after surgery. Subjective cyclodeviation was assessed by Harms' tangent scale. Objective cycloposition was measured by means of fundus cyclometry, a novel method using an infrared scanning laser ophthalmoscope. Results. Diagnostic occlusion did not lead to significant changes in either objective or subjective cyclodeviation. Preoperative objective excycloposition was nearly equally distributed between affected eyes and fellow eyes. Early surgically induced incyclorotatory effects were more pro- nounced objectively than subjectively. On long-term follow-up, a reduction in the incyclorota- tory effect was found to be smaller subjectively than objectively. A significant difference between subjective and objective cycloposition was seen early after surgery, and a significant difference between subjective and objective cyclorotatory change was found immediately after surgery and on long-term follow-up. Conclusions. Long-term regression of the incyclorotatory effect after inferior oblique muscle recession was confirmed objectively and subjectively and can be explained as a cessation of preoperatively required binocular compensatory innervation. The authors conclude that the difference between objective and subjective regression is caused by sensory cyclofusion. Invest Ophthalmol Vis Sci. 1997;38:405-412. Subjective cyclodeviation, when tested on orthoptic examination, can differ from real objective cycloposi- tion of the globe. 1 ' 2 It has been pointed out by Hessel 3 that the relation between sensory and motor cyclofu- sion in fusional cyclovergence is 3:1. In objective mea- surements of human cyclofusional response, Kertesz 4 found a fusion of disparities up to 5° without rotation of the globe. In Bielschowsky's head tilt test, sensory elements seemed to play an important role because pure motor compensatory counterrolling was found not to exceed 5 0 . 5 After surgery of the oblique muscles, torsional phenomena can be found that are still not From the Eye Hospital, Ludwig-Maximilians-University, Munich, Germany. Submitted for publication April 11, 1996; revised July 22, 1996; accepted September 30, 1996. Proprietary interest category: N. Reprint requests: Hermann Dieter Schiuorm, University Eye Hospital, MathUdmislrasse 8, 80336 Munich, Germany. clearly understood. As described by Herzau, 6 some persons complain of a postoperative subjective cyclor- otatory overcorrection that disappears after a certain period of time. Others reveal a regression of the sur- gery-induced rotatory effect by recurrence of a certain amount of subjective cyclodeviation without having shown an overcorrection. Litde has been reported so far on objective cyclorotatory changes after oblique muscle surgery, and little is known about the relation between subjective and objective cyclorota- tory changes. 7 ' 8 It was our aim to determine motor and sensory torsional elements in patients who underwent surgery of the oblique muscles to find an explanation for the above-mentioned phenomena. To that end, objective cycloposition and subjective cyclodeviation were mea- sured in patients with oblique muscle disorders before and after surgery. In addition, we tried to quantify the Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2 Copyright © Association for Research in Vision and Ophthalmology 405 Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018
Transcript of Investigations on subjective and objective cyclorotatory...

Investigations on Subjective and Objective CyclorotatoryChanges After Inferior Oblique Muscle Recession
Hermann Dieter Schworm, Silvia Eithoff, Markus Schaumberger, and Klaus-Peter Boergen
Purpose. To determine subjective and objective cyclorotatory changes after surgery for obliquemuscle disorders and to analyze the mechanisms of the well-known, long-term, postoperative,subjective cyclotorsional changes.
Methods. Twenty-six patients underwent unilateral inferior oblique muscle recession for strabis-mus sursoadductorius (inferior oblique overfunction). Subjective and objective cyclodeviationwere examined before surgery with and without diagnostic occlusion, as well as 1 day, 3 days,and 4 months after surgery. Subjective cyclodeviation was assessed by Harms' tangent scale.Objective cycloposition was measured by means of fundus cyclometry, a novel method usingan infrared scanning laser ophthalmoscope.
Results. Diagnostic occlusion did not lead to significant changes in either objective or subjectivecyclodeviation. Preoperative objective excycloposition was nearly equally distributed betweenaffected eyes and fellow eyes. Early surgically induced incyclorotatory effects were more pro-nounced objectively than subjectively. On long-term follow-up, a reduction in the incyclorota-tory effect was found to be smaller subjectively than objectively. A significant differencebetween subjective and objective cycloposition was seen early after surgery, and a significantdifference between subjective and objective cyclorotatory change was found immediately aftersurgery and on long-term follow-up.
Conclusions. Long-term regression of the incyclorotatory effect after inferior oblique musclerecession was confirmed objectively and subjectively and can be explained as a cessation ofpreoperatively required binocular compensatory innervation. The authors conclude that thedifference between objective and subjective regression is caused by sensory cyclofusion. InvestOphthalmol Vis Sci. 1997;38:405-412.
Subjective cyclodeviation, when tested on orthopticexamination, can differ from real objective cycloposi-tion of the globe.1'2 It has been pointed out by Hessel3
that the relation between sensory and motor cyclofu-sion in fusional cyclovergence is 3:1. In objective mea-surements of human cyclofusional response, Kertesz4
found a fusion of disparities up to 5° without rotationof the globe. In Bielschowsky's head tilt test, sensoryelements seemed to play an important role becausepure motor compensatory counterrolling was foundnot to exceed 50.5 After surgery of the oblique muscles,torsional phenomena can be found that are still not
From the Eye Hospital, Ludwig-Maximilians-University, Munich, Germany.Submitted for publication April 11, 1996; revised July 22, 1996; accepted September30, 1996.Proprietary interest category: N.Reprint requests: Hermann Dieter Schiuorm, University Eye Hospital,MathUdmislrasse 8, 80336 Munich, Germany.
clearly understood. As described by Herzau,6 somepersons complain of a postoperative subjective cyclor-otatory overcorrection that disappears after a certainperiod of time. Others reveal a regression of the sur-gery-induced rotatory effect by recurrence of a certainamount of subjective cyclodeviation without havingshown an overcorrection. Litde has been reportedso far on objective cyclorotatory changes afteroblique muscle surgery, and little is known about therelation between subjective and objective cyclorota-tory changes.7'8
It was our aim to determine motor and sensorytorsional elements in patients who underwent surgeryof the oblique muscles to find an explanation for theabove-mentioned phenomena. To that end, objectivecycloposition and subjective cyclodeviation were mea-sured in patients with oblique muscle disorders beforeand after surgery. In addition, we tried to quantify the
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2Copyright © Association for Research in Vision and Ophthalmology 405
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

406 Investigative Ophthalmology 8c Visual Science, February 1997, Vol. 38, No. 2
influence on cyclotorsion of binocular conditions incomparison to monocular conditions before and aftersurgery.
METHODS
Subjects
This research adhered to the tenets of the Declarationof Helsinki; informed consent was obtained from allpatients after the nature and possible consequencesof the study were explained. Twenty-six patients (17males, 9 females) with unilateral strabismus sursoad-ductorius (inferior oblique overfunction) were in-cluded in the study. Mean age was 39 years; the agerange was 9 to 74 years. Patients were excluded if theyhad any other squint or serious ocular disease. Theright eye was affected in 11 patients, and the left eyewas affected in 15 patients. Unilateral inferior obliquemuscle recession was performed on the affected eyeonly. Seven patients underwent recession of 8 mm, 9patients underwent recession of 10 mm, and 10 pa-tients underwent maximum recession (the techniquefor this has been described elsewhere).9
Assessment
Full orthoptic examination with assessment of subjec-tive cyclodeviation and objective cycloposition was per-formed before and after surgery. To detect the influ-ence of binocularity on cyclotorsion, subjective cyclo-deviation and objective cycloposition were assessedbefore surgery both without diagnostic occlusion andthen after 3 days of diagnostic occlusion. Subjectivecyclodeviation and objective cycloposition were mea-sured on the first postoperative day immediately afterremoval of the bandage and before binocular stimula-tion had been applied, on the third postoperative dayafter 2 days of binocular vision, and 4 months aftersurgery for long-term assessment. Evaluation of preop-erative cyclodeviation without diagnostic occlusionwas hampered in three patients because objective andsubjective data were missing and in one patient subjec-tive assessment was available only with fixation of theaffected eye.
Subjective cyclodeviation was assessed binocularlyunder complete dissociation by the tangent scale de-vised by Harms10 and further described by Mack-ensen" (Fig. 1). This method is applied in Germanyfor simultaneous assessment of horizontal, vertical,and cyclotorsional angles of squint in patients inwhom the image of the nonfixating eye is not ex-cluded. The screen is provided with a grid pattern,which indicates horizontal and vertical angles ofsquint, as well as with a scale for cyclotorsion. In thecenter of the screen, a metal box containing a white
FIGURE l. The tangent scale of Harms for assessment of sub-jective horizontal, vertical, and cyclorotational angles ofsquint (for further explanation, see Methods).
light is attached to serve as a fixation target. The shapeof the fixation light can be changed from circular toa horizontal streak of light by removing the top coverof the box. The box can be rotated by remote controlso that the horizontal streak of light can be turned toany oblique position, the degree of which is indicatedon a scale. The patient is seated 2.5 m from the screen,and the room is moderately dark. Proper head posi-tion is controlled by means of a special projector,attached to the forehead, that points a dim white lightto the scale.
Beginning with the circular fixation light, a darkred glass is held in front of the fixating eye, and thepatient is asked to fixate the red light. Because thedark red filter excludes anything but the fixation light,there is complete dissociation without any fusion re-sponse. The patient is given a green light pointer andis asked to point at the red fixation light. Because thefixating eye can see nothing but the red light, thegreen light has to be localized by the uncovered eyeto which the white light and the scale pattern arevisible. According to the principle of confusion, thered foveal image of the fixating eye is centrally super-imposed with the foveal image of the nonfixating,squinting eye. If the patient has central fixation andnormal retinal correspondence, the red light is local-ized according to the type of squint beside, above, orunder the white fixation light, and the angle of squintcan be read from the scale to which the patient pointswith the green light.
The fixation light then is changed to a horizontalstreak measuring 5° of arc at 2.5 m. The red streakappears oblique if there is subjective cyclodeviation.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

Cyclorotational Changes After Inferior Oblique Recession 407
FIGURE 2. Fundus cyciometry in primary position ("ger-ade") on a patient with right eye strabismus sursoadductor-ius (physiologic excycloposition not subtracted), (top) Be-fore surgery (objective excycloposition of 16° OD and 2°OS), (bottom) One day after maximum recession of the rightinferior oblique muscle (objective excycloposition of 6° ODand 4° OS).
The patient is asked to rotate the red streak by remotecontrol until it appears horizontal. The amount ofobliquity is read from the scale. As on routine or-thoptic examination, the angles of horizontal, vertical,and cyclorotatory squint are measured in the ninediagnostic positions of gaze controlled with the fore-head projector with right eye and left eye fixation.
Objective cycloposition was determined by funduscyclometry, a novel monocular technique of assessingreal, objective bulbar rotation described in detail else-where.12'13 Examinations were performed on right andleft eyes separately in primary position, right gaze, andleft gaze; the nonfixating eye was patched. Correcthead position was assured by the use of a bite bar.The patient had to look into an infrared scanninglaser ophthalmoscope (Rodenstock Instruments, Ot-tobrunn, Germany). Within a homogenous field ofdim red laser light, a bright red cross measuring 2° ofarc was presented as a fixation target. Images of theposterior pole were obtained without pupil dilationand were transferred to a computer system. After en-circling of the optic disk with the computer mouse,its geometric center was marked by the computer. Thispoint had to be connected with the fixation markindicating the location of the foveola. The angle be-tween this line and the horizontal line, representingthe amount of objective bulbar rotation, was calcu-lated by the computer. Figure 2 illustrates the resultof fundus cyclometry on one of our patients beforeand after surgery.
EvaluationOn examination of the subjective cyclodeviation onthe Harms tangent scale, the difference of cyclotor-sion between the fixating and the nonfixating eye wasassessed and included the amount of obliquity of botheyes. In fundus cyclometry, however, the amount of
obliquity was measured for each eye separately. There-fore, the angles of objective cycloposition of right andleft eye had to be added. As demonstrated by Bixen-man1 and Herzau,1'1 healthy persons show an averagephysiologic excycloposition of 7° per eye (range, 0° to12°). For a comparison of subjective to objective data,we subtracted 7° from the objective value of each eye.Because individual physiologic excyclopositions wereunknown, the preoperative value of objective cyclo-position served as a reference for induced changes.In the current study, only the primary position wasevaluated. Concerning the Harms tangent scale, onlyfixation with the affected eye was evaluated. Right andleft gaze of fundus cyclometry and fixation with theunaffected eye of the Harms tangent scale were omit-ted in this study to keep the amount of data withinreasonable limits.
RESULTS
Double vision in the primary position occurred in 20of 26 patients before surgery, and surgery cured it inall of them. Binocular functions were measured usingthe random dot stereo test by Lang (Lang II test)and the striated lens test by Bagolini. Stereopsis wasconsidered good if Lang test figures with a disparityof :s400 seconds of arc were recognized. Stereopsiswas reduced markedly before surgery in four patients.After surgery, only one patient still had poor stereop-sis. Similarly, good binocular function was obsen'edin 22 patients before and in 25 patients after surgery.
Data on subjective cyclodeviation and objectivecycloposition before and after surgery are listed inTables 1 to 4 and are illustrated in Figure 3. Theyrepresent the statistical mean of 26 patients. Table 1shows means, standard deviations and ranges of sub-jective cyclodeviation and objective cycloposition be-fore and after surgery. Table 2 lists the mean inducedsubjective and objective changes, their standard devia-tions, and the significances with P, t, and df values.Statistical significance was calculated using the paired-samples Hest. Table 3 shows the mean differences,the standard deviations, and the significances with P,iy and df values between subjective cyclodeviation andobjective cycloposition before and after surgery. Table4 lists the mean differences, their standard deviations,and the significances with P, t, and df values amongsubjective and objective surgically induced cyclorota-tory changes.
Effect of Diagnostic OcclusionDiagnostic occlusion had no statistically significant in-fluence on subjective or objective excyclodeviation.Mean preoperative subjective excyclodeviation was6.3° ± 6.4° (range, 0° to 22°) before diagnostic occlu-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018
408 Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
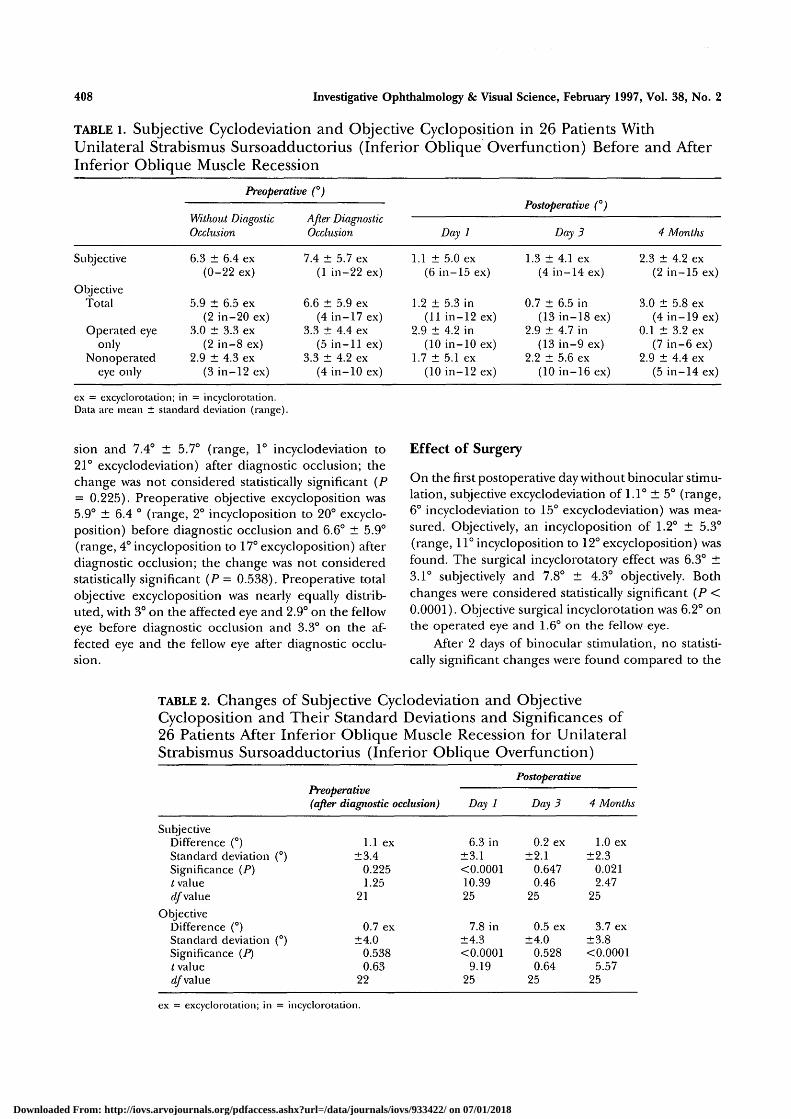
TABLE i. Subjective Cyclodeviation and Objective Cycloposition in 26 Patients WithUnilateral Strabismus Sursoadductorius (Inferior Oblique Overfunction) Before and AfterInferior Oblique Muscle Recession
Subjective
ObjectiveTotal
Operated eyeonly
Nonoperatedeye only
Preoperative (°)
Without DiagosticOcclusion
6.3 ± 6.4 ex(0-22 ex)
5.9 ± 6.5 ex(2 in-20 ex)
3.0 ± 3.3 ex(2 in-8 ex)
2.9 ± 4.3 ex(3 in-12 ex)
After DiagnosticOcclusion
7.4 ± 5.7 ex(1 in-22 ex)
6.6 ± 5.9 ex(4 in-17 ex)
3.3 ± 4.4 ex(5 in-11 ex)
3.3 ± 4.2 ex(4 in-10 ex)
Day 1
1.1 ± 5.0 ex(6 in-15 ex)
1.2 ± 5.3 in(11 in-12 ex)
2.9 ± 4.2 in(10 in-10 ex)
1.7 ± 5.1 ex(10 in-12 ex)
Postoperative (°)
Day 3
1.3 ± 4.1 ex(4 in-14 ex)
0.7 ± 6.5 in(13 in-18 ex)
2.9 ± 4.7 in(13 in-9 ex)
2.2 ± 5.6 ex(10 in-16 ex)
4 Montlis
2.3 ± 4.2 ex(2 in-15 ex)
3.0 ± 5.8 ex(4 in-19 ex)
0.1 ± 3.2 ex(7 in-6 ex)
2.9 ± 4.4 ex(5 in-14 ex)
ex = excyclorotation; in = incyclorotation.Data are mean ± standard deviation (range).
sion and 7.4° ± 5.7° (range, 1° incyclodeviation to21° excyclodeviation) after diagnostic occlusion; thechange was not considered statistically significant (P= 0.225). Preoperative objective excycloposition was5.9° ± 6.4 ° (range, 2° incycloposition to 20° excyclo-position) before diagnostic occlusion and 6.6° ± 5.9°(range, 4° incycloposition to 17° excycloposition) afterdiagnostic occlusion; die change was not consideredstatistically significant (P = 0.538). Preoperative totalobjective excycloposition was nearly equally distrib-uted, with 3° on the affected eye and 2.9° on the felloweye before diagnostic occlusion and 3.3° on the af-fected eye and the fellow eye after diagnostic occlu-
sion.
Effect of Surgery
On the first postoperative day without binocular stimu-lation, subjective excyclodeviation of 1.1° ± 5° (range,6° incyclodeviation to 15° excyclodeviation) was mea-sured. Objectively, an incycloposition of 1.2° ± 5.3°(range, 11° incycloposition to 12° excycloposition) wasfound. The surgical incyclorotatory effect was 6.3° ±3.1° subjectively and 7.8° ± 4.3° objectively. Bothchanges were considered statistically significant (P <0.0001). Objective surgical incyclorotation was 6.2° onthe operated eye and 1.6° on the fellow eye.
After 2 days of binocular stimulation, no statisti-cally significant changes were found compared to the
TABLE 2. Changes of Subjective Cyclodeviation and ObjectiveCycloposition and Their Standard Deviations and Significances of26 Patients After Inferior Oblique Muscle Recession for UnilateralStrabismus Sursoadductorius (Inferior Oblique Overfunction)
SubjectiveDifference (°)Standard deviationSignificance (P)t valuerf/"value
ObjectiveDifference (°)Standard deviationSignificance (P)I valuerf/" value
(
(
°)
°)
Preoperative(after diagnostic occlusion)
1.1 ex±3.4
0.2251.25
21
0.7 ex±4.0
0.5380.63
22
Day 1
6.3 in±3.1<0.000110.3925
7.8 in±4.3<0.0001
9.1925
Postoperative
Day 3
0.2 ex±2.1
0.6470.46
25
0.5 ex±4.0
0.5280.64
25
4 Months
1.0 ex±2.3
0.0212.47
25
3.7 ex±3.8<0.0001
5.5725
ex = excyclorotation; in = incyclorotation.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

Cyclorotational Changes After Inferior Oblique Recession 409
TABLE 3. Differences Between Subjective Cyclodeviation and Objective Cycloposition andTheir Standard Deviations and Significances of 26 Patients After Inferior Oblique MuscleRecession for Unilateral Strabismus Sursoadductorius (Inferior Oblique Overfunction)
Difference (°)Standard deviation (°)Significance (P)t valuedf value
Preoperative
Before Diagnostic /xjier uiagnosncOcclusion
+0.4±5.1
0.8380.21
21
Occlusion
+0.8±5.0
0.4240.81
25
Day 1
+2.3±4.9
0.0242.39
25
Postoperative
Day 3
+2.0±5.0
0.0492.07
25
4 Months
-0.7±4.7
0.4420.78
25
+ = more subjective than objective excyclodeviation; — = less subjective than objective excyclodeviation.
immediate postoperative positions. The mean surgicalincyclorotatory effect dropped by 0.2° ± 2.1° subjec-tively and by 0.5° ± 4° objectively; P = 0.647 and P =0.528, respectively.
Long-term Follow-up
Four months after surgery, subjective excyclodeviationincreased to 2.3° ± 4.2° (range, 2° incyclodeviation to15° excyclodeviation). The increase of 1° was statisti-cally significant (P = 0.021). During the same interval,a marked reduction of the objective surgical incycloro-tatory effect was found. Objective cyclopositionchanged from 0.7° incycloposition to 3° excycloposi-tion ± 5.8° (range, 4° incycloposition to 19° excyclo-position). The 3.7° change was considered statisticallysignificant (P< 0.0001). The objective incyclorotatoryeffect on the unoperated eye disappeared; it had been2.9° excycloposition both before and 4 months aftersurgery. Thus, surgically induced objective long-termincyclorotation of the operated eye was 2.9°. Surgicallyinduced subjective long-term incyclorotation was 4°.Objective and subjective long-term changes were con-
sidered statistically significant (P = 0.005 and P <0.0001, respectively).
Differences Between Subjective and ObjectiveData
The differences between subjective cyclodeviation andobjective cycloposition at each time of measurementare listed in Table 3. Except for days 1 and 3 aftersurgery, the values were small and not statistically sig-nificant. Before surgery, there was 0.4° more excyclo-deviation subjectively than objectively without diag-nostic occlusion and 0.8° more excyclodeviation sub-jectively than objectively after diagnostic occlusion.The differences were not statistically significant (P =0.838 and P = 0.424, respectively). After surgery, therewas 2.3° more excyclodeviation subjectively than objec-tively on day 1 and 2° more excyclodeviation subjec-tively than objectively on day 3. The differences wereconsidered statistically significant (P = 0.024 and P =0.049, respectively). Four months after surgery, therewas 0.7° less excyclorotation subjectively than objec-
TABLE 4. Differences Between Subjective and Objective SurgicallyInduced Cyclorotatory Changes and Their Standard Deviations andSignificances of 26 Patients After Inferior Oblique MuscleRecession for Unilateral Strabismus Sursoadductorius (InferiorOblique Overfunction)
Difference (°)Standard deviation (°)Significance (P)I valuedf value
Preoperative (afterdiagnostic occlusion)
0.4 +ex±4.2
0.4870.71
21
Day 1
1.5 - in±3.8
0.0532.03
25
Postoperative
Day 3
0.3 -ex±4.6
0.7360.34
25
4 Months
2.7 -ex±4.0
0.0023.51
25
+ex = subjectively more excyclorotatory effect than objectively; —ex = subjectively lessexcyclorotatory effect than objectively; —in = subjectively less incyclorotatory effect than objectively.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

410 Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
excyclo-position ("]
7 •
6 •
5
4 -
3
2 •
1 *
1 -
2 -
incyclo-potition [*]
'A• \ \
• \ \
• V\
preoperativei i
without withdiogn. occl.
• sub|ec'ive cyclodeviolion
O objective cycloposition
\ /A ^rX/'
postoperative
day 1 day 3 4 months
FIGURE 3. Change of subjective cyclodeviation and objectivecycloposition in 26 patients after inferior oblique musclerecession for unilateral strabismus sursoadductorius (infe-rior oblique overfunction).
tively; the difference was not considered statisticallysignificant (P = 0.442).
Differences between subjective and objective sur-gically induced cyclorotatory changes are listed in Ta-ble 4. The 0.4° mean difference after diagnostic occlu-sion before surgery was not considered statistically sig-nificant (P = 0.487). Immediately after surgery, thein cyclorotatory effect was 1.5° stronger objectivelythan subjectively. On the alpha = 0.1 level, the differ-ence was not considered statistically significant {P =0.053). Two days later, there was a difference of 0.3°,which was considered statistically significant (P =0.736). Four months after surgery, the reduction ofthe surgical incyclorotatory effect was 2.7° strongerobjectively than subjectively; the difference was statisti-cally significant (P = 0.002).
Summary of Results
The results can be summarized as follows:
1. A significant difference between subjective andobjective cycloposition was seen early after sur-gery.
2. A significant difference between subjective andobjective cyclorotatory changes was found imme-diately after surgery and on long-term follow-up.
3. Preoperative objective excycloposition was nearlyequally distributed between the affected and theunaffected eye.
4. Diagnostic occlusion did not show statistically
significant changes of objective and subjectivecyclodeviation.
5. The immediate surgical incyclorotatory effectwas more pronounced objectively than subjec-tively.
6. Short-term binocular stimulation for 2 days aftersurgery did not significantly influence subjectivecyclodeviation or objective cycloposition.
7. After 4 months of binocular stimulation, a reduc-tion of the surgical incyclorotatory effect wasfound, and it was more pronounced objectivelythan subjectively.
8. The surgically induced long-term incyclorotatoryeffect was more pronounced subjectively thanobjectively.
DISCUSSION
It was the aim of this study to measure subjective andobjective cyclorotatory changes in patients with strabis-mus sursoadductorius (inferior oblique overfunction)undergoing inferior oblique recession. These changeswere induced by interruption of binocularity, by sur-gery, and by short- and long-term binocular stimula-tion after surgery. The purpose of these investigationswas to determine motor and sensory elements ofcyclorotatory changes.
For the assessment of subjective cyclodeviation,we used the tangent scale devised by Harms.10 It is oneof the standard methods in Germany for simultaneousassessment of horizontal, vertical, and cyclotorsionalangles of squint in the nine positions of gaze8 in pa-tients who do not exclude the image of the nonfixat-ing eye. Examination of objective cycloposition wasachieved by fundus cyclometry, based on measure-ment of objective bulbar rotation by means of fundusphotography. Fundus cyclometry offers several advan-tages over fundus photography for the assessment ofcycloposition: There is no need for pupil dilation be-cause of infrared laser light, and, hence, further or-thoptic examination is not impaired, which makes itmore convenient for the patient; no photographic ma-terial has to be processed, and, therefore, results areavailable immediately; and computerized calculationof the angle of torsion is precise. The method provedto be reliable and has been discussed in detail else-where.12'13
As described by Kertesz and Jones4 and by Kert-esz,1"'' the size and complexity of the fixation targetmust be considered because they affect both cyclofu-sion and objective cycloposition under binocular con-ditions. In our study, however, the assessment of sub-jective cyclodeviation was performed under completedissociation with a dark red glass, and the measure-ment of objective cycloposition was made monocularly
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

Cyclorotational Changes After Inferior Oblique Recession 411
with the nonfixating eye patched. For that reason,there was no fusion, and objective cycloposition wasnot affected by the different sizes of the fixation tar-gets. On subjective measurement, space constancy,which also can affect cyclotorsional measurements,was interrupted by the dark red glass, which excludedanything to the fixating eye but the streak of light.On fundus cyclometry, there was no space constancybecause nothing but the fixation target was visible.For the same reasons, no visual context could haveinfluenced cycloposition.
On the assessment of preoperative subjectivecyclodeviation using the Harms tangent scale, the af-fected eye is situated in primary position when fixatingand in vertical deviation when not fixating, whereason fundus cyclometry each eye, is measured in primaryposition. Because it is known that a change of verticalposition can affect cyclodeviation, we compared pre-operative subjective cyclodeviation on fixation withthe affected eye to that on fixation with the nonaf-fected eye. No significant differences between cyclode-viations on either fixation were found. We concludedthat vertical deviation to the extent present in ourpatients did not significantly affect cyclodeviation.Thus, comparison of preoperative subjective cyclode-viation to preoperative objective cycloposition and ofpreoperative subjective cyclodeviation to postopera-tive subjective and objective cycloposition was possi-ble. Mean hypertropia of the affected eye in our pa-tients was 6° before surgery and 1° after surgery; hori-zontal deviation was not present. These results are inaccord with Boergen,9 who reported a mean verticalchange of 5° and no horizontal change in 28 patientsafter inferior oblique muscle recession.
When interpreting the data, intraindividual varia-tions in the measurement of cyclodeviation and cyclo-position must be considered. Apart from possiblespontaneous torsional eye movements as described byRoessler,16 Herzau found intraindividual fluctuationsof unilateral objective cycloposition up to 3.5°.6 Kraftreported intraindividual variations of subjective cyclo-deviation up to 70.17 The high levels of standard devia-tion in this study reflect these variations.
The observation of preoperative equal distribu-tion of objective excycloposition between the affectedand the fellow eye is in accord with Bixenman, whofound that some patients with unilateral superioroblique palsy have a greater degree of objective ex-cyclotorsion in the normal than in the paretic eye.1
Olivier18 reported 15 of 60 patients with unilateralsuperior oblique palsy who had subjective excyclo-tropia of the nonparetic eye. These patients habituallyfixated with the paretic eye. Olivier interpreted thisphenomenon as ". . . the result of a monocular sen-sorial adaptation to the cyclodeviation by means of a
reordering of the spatial response of retinal elementsalong new horizontal and vertical meridians."18
The effect of preoperative diagnostic occlusion oncyclodeviation was not statistically significant. In somepatients, however, there was a slight increase of ex-cyclodeviation that could be interpreted in terms ofcyclofusional mechanisms under binocular conditionsinterrupted by diagnostic occlusion. At this time, wecannot explain why the surgically induced incyclotorsi-onal effect was greater objectively than subjectivelyone day after surgery without binocular stimulationnor why an objective incyclorotatory effect was foundon the unoperated eye.
The observed long-term reduction of the surgi-cally induced incyclorotatory effect was more pro-nounced objectively than subjectively. What could bethe cause of postoperative subjective reduction of sur-gically induced incyclotorsion? Ruttum19 described asensory reorientation in patients with congenital andacquired cyclotropia that prevents awareness of tiltingof the environment. If this compensatory mechanismis no longer necessary, sensory reorientation couldgive rise to sensory excyclotorsion and, thereby, tosubjective weakening of the surgically induced incyclo-torsional effect. This suggestion, however, is not plau-sible because on average there was still subjective ex-cyclodeviation immediately after surgery; there was noreason for cessation of the compensatory mechanism.In patients with postoperative subjective overcorrec-tion, this phenomenon could be based on cyclofusio-nal mechanisms described by von Noorden,2 Herzau,1'1
and Boergen.20 If there was no overcorrection, weak-ening of the objective surgical effect could be interpre-ted by a cessation or reduction of preoperatively re-quired binocular compensatory innervation, as dis-cussed by Rolling.8 This, however, does not explain thedifference between objective and subjective reduction,which led to a long-term incyclorotatory effect of 3.6°objectively compared to 5.1° subjectively (related tothe preoperative examination after diagnostic occlu-sion). Figure 3 makes us question why objective andsubjective rotational changes behave nearly parallelup to the third day after surgery but show such amarked difference after 4 months. Analysis of individ-ual data, such as looking at patients with extreme varia-tions or comparing preoperative compensation ofcyclophoria, did not provide an explanation. The an-swer appears to be sensory cyclofusion as described byHerzau6 and von Noorden21; it partially compensatesthe postoperative motor weakening of the objectivesurgical incyclorotatory effect. In this study, theamount of sensory cyclofusion equaled the differencebetween subjective and objective torsional change.
Results of this study improved our knowledge ofsubjective and objective cyclorotatory behavior before
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018

412 Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
and after surgery, and this knowledge is important forthe management of oblique muscle disorders. Becauselong-term weakening of the surgical incyclorotatoryeffect after inferior oblique muscle recession has beenconfirmed, we advise refraining from early correctionif an immediate postoperative overeffect is present.
Key Words
cyclodeviation, fundus cyclometry, inferior oblique musclesurgery, objective-subjective, strabismus, torsional changes
Acknowledgments
The authors thank Prof. Dr. G. Rolling, Orthoptic Depart-ment, Eye Hospital, Ruprecht-Rarls—University (Heidel-berg, Germany) for his support concerning the interpreta-tion of the results.
References
1. Bixenman WW, von Noorden GK. Apparent fovealdisplacement in normal subjects and in cyclotropia.Ophthalmology. 1982; 89:58-62.
2. von Noorden GK. Clinical observations in cyclodevi-ations. Ophthalmology. 1979;86:1451-1461.
3. HeBel L, Herzau V. Erfolgt die fusionale Zyklovergenznach dem Heringschen Gesetz? Orthoptik-Pleoptik.1984; 11:45-51.
4. KerteszAE, Jones RW. Human cyclofusional response.Vision Res. 1970; 10:891 -896.
5. Inatomi A, Terao N, Okamoto K. Measurement ofcompensatory cycloduction by fundus photographicmethod. In: Reinecke RD, ed. Strabismus. New York:Grune & Stratton; 1978:405-413.
6. Herzau V, Joos E. Untersuchungen von Bewegungenund Stellungsfehlern der Augen um ihre sagittateAchse. Z prakt Augenheilkd. 1983;4:270-278.
7. Rolling G. Das Verhaltnis zwischen sensorisch wahr-genommener und motorisch objektivierbarer Trans-position der Zyklotropie bei Musculus obliquus supe-rior-Paresen. In: Herzau V, Naumann GOH, MerteHJ, Hollwich F, Gloor B, eds. Pathophysiologiedes Sehens,Biicherei des Augenarztes. Stuttgart: Enke; 1984:222-232.
8. Rolling G. Diagnostih und operative Koirektur von Vertikal-und Zyklodeviationen bei Storungen schrdger Augenmuskeln.Thesis ("Habilitationsschrift"). GieBen: Bruhlsche Uni-versitatsdaickerei; 1986:57-59.
9. Boergen R-P, Miiller Ch. Maximale Ch. Obliquus-infe-rior-Chirurgie bei Strabismus sursoadductorius. FoliaOphthalmol. 1992; 17:48-52.
10. Harms H. Uber die Untersuchung der Augenmuskel-lahmungen. Graefes Arch Clin Exp. 1941;4:129-139.
11. Mackensen G. Die Tangentenskala nach Harms. In:Hamburger FA, Hollwich F, eds. Augenmuskellah-mungen, Biicherei des Augenartztes. Stuttgart: Enke;1966:254-260.
12. Schworm HD, Boergen R-P, Ehrt O, Eithoff S. Funduscyclometria—a novel method for measuring objectivecycloduction. ARVO abstracts. Invest Ophthalmol VisSci 1995;36:S952.
13. Schworm HD, Boergen R-P, Eithoff S. Measurementof subjective and objective cyclodeviation in obliqueeye muscle disorders. Strabismus. 1995;3:115-122.
14. Herzau V, Joos-Rratsch E. Objective and subjectiveevaluation of cyclovergence and cyclofusion. Doc Oph-thalmol. 1984; 58:85-90.
15. Rertesz AE. The effect of stimulus complexity on humancyclofusional response. Vision Res. 1972; 12:699-704.
16. Rossler F. Die Hohenstellung des blinden Fleckes innormalen Augen. Arch Augenheilkd. 1920;86:55-88.
17. Rraft SP, O'Reilly C, Quigley PL, Allan R, Eustis HS.Cyclotorsion in unilateral and bilateral superioroblique paresis. / Pediatr Ophthalmol Strabismus.1993; 30:361-367.
18. Olivier P, von Noorden GR. Excyclotropia of the non-paretic eye in unilateral superior oblique muscle pa-ralysis. Am J Ophthalmol. 1982; 93:30-33.
19. Ruttum M, von Noorden GK. Adaptation to tilting ofthe visual environment in cyclotropia. Am J Ophthal-mol. 1983;96:229-237.
20. Boergen R-P, Brenner A. Surgical treatment of troch-lear palsy. In: Lenk-Schafer M, ed. Orthoptic Horizons—Transactions 6th International Orthoptic Congress. Harro-gate; 1987; 198-203.
21. von Noorden GR. Clinical and theoretical aspects ofcyclotropia. J Pediatr Ophthalmol Strabismus. 1984; 21:126-132.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933422/ on 07/01/2018