Intravascular stents A biased and limited account.
44
Intravascular stents A biased and limited account
-
Upload
bertha-carter -
Category
Documents
-
view
214 -
download
0
Transcript of Intravascular stents A biased and limited account.

Intravascular stents
A biased and limited account

Outline
• Background– Occlusive vascular disease and its treatment by PCI
and stenting
• Assessment of a novel compliance matching stent and comparison with a commercially available device– In vivo radiographic measurement in pig carotid and
iliac arteries– Development of a micro CT method for stented vessel
morphometry on excised arteries

Cardiovascular Disease statistics
• Heart and circulatory disease are the UK's biggest killers.
• In 2006, cardiovascular disease caused 40% of deaths in the UK, and killed over 245,000 people.
• Coronary arterial disease causes over 120,000 deaths a year in the UK: approximately one in four deaths in men and one in six deaths in women.

Revascularisation techniques
• Coronary Artery Bypass Graft (CABG)
• Percutaneous Coronary Intervention (PCI)– Angioplasty– Plus stenting (94%)

Balloon angioplasty
What is an intravascular stent?
• A small tubular mesh usually made of either stainless steel or Nitinol. (Shape memory alloy)
• Inserted into stenotic (blocked) arteries to keep the lumen patent. Normally during angioplasty.
• Used at various sites including the coronary, renal, carotid and femoral arteries.
• Non-arterial uses e.g. in bronchus, trachea, ureter, bile duct.

History
• The concept of vascular stents is accredited to Charles Dotter in 1969, who implanted stainless steel coils in canine peripheral arteries.– Not followed up in humans because of
haemodynamically significant narrowing.
• Not in clinical practice until 1980s.• Market leader is the Palmaz stent designed by
Julio Palmaz in 1985.– Initially, 18 grafts placed in canine vessels, with
patency rates approaching 80% at 35 weeks.

Varied stent geometries
11651216
70,142
73,612
0
200
400
600
800
1000
1200
1400
1600
1800
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
PC
I pe
r m
illio
n
0
10000
20000
30000
40000
50000
60000
70000
80000
PC
I P
roce
dure
Num
bers
PCI per million
PCI Procedures
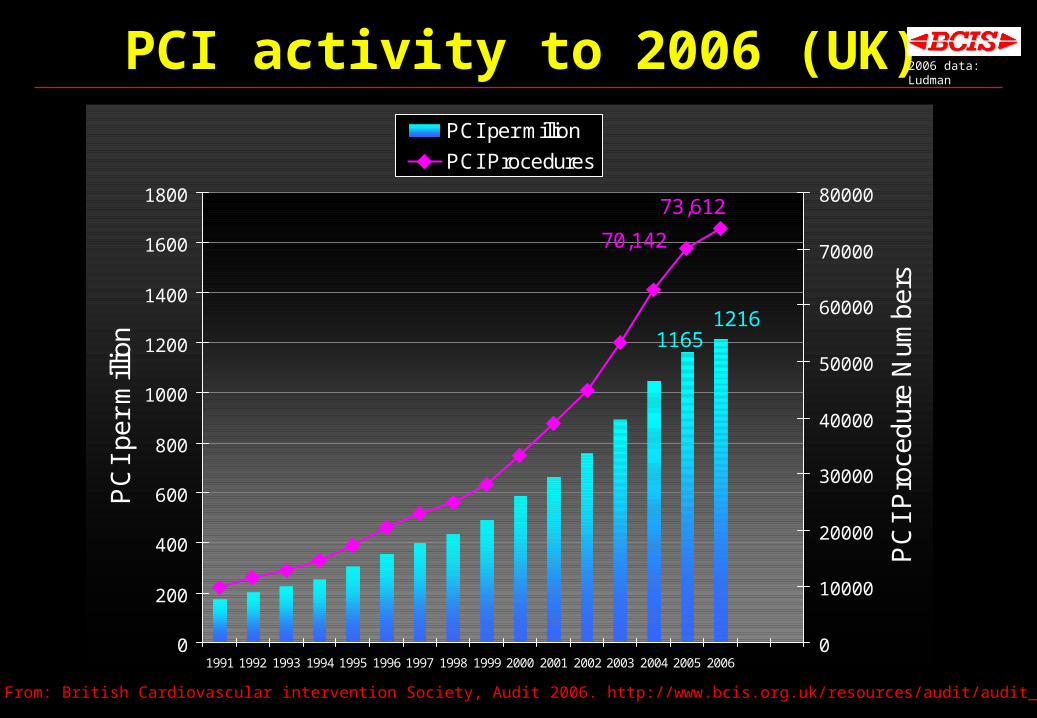
PCI activity to 2006 (UK) 2006 data: Ludman
From: British Cardiovascular intervention Society, Audit 2006. http://www.bcis.org.uk/resources/audit/audit_2006

High Tech 2007, MarseilleHigh Tech 2007, Marseille
Nombres de PCI dans certains pays Européens
0
500
1000
1500
2000
2500
3000
3500
4000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Par 106
habitantsGEGE
BEBE
UKUK
Bernard De Bruyne, Aalst, Belgium

Demographics2006 data: Ludman Age (mean) 64.2 yrs
Diabetic 17.5%
Previous CABG 8.9%
Ethnic Origin
Caucasian 91.2%
Asian 7.5%
Black 1.1%
Oriental 0.2%http://www.bcis.org.uk/resources/audit/audit_2006

Demographics - Age2006 data: Ludman
02000400060008000
100001200014000
No. PCIs<
=30
31-4
0
41-5
0
51-6
0
61-7
0
71-8
0
81-9
0
>90
Age (yrs)
Male
Female
Male: mean = 62.3Female: mean = 67.4
http://www.bcis.org.uk/resources/audit/audit_2006

Procedures using Stents
94.4
0102030405060708090
100
% of Procedures
'92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04 '05 '06
Year
2006 data: Ludman
http://www.bcis.org.uk/resources/audit/audit_2006
The problem with stents.
Restenosis. (7 – 20%)
Rate depends on
lesion type, length and severity

Mechanical cause of restenosis
• ↓ shear stress• Intimal Hyperplasia• ↓ lumen• ↑ shear stress• If baseline shear stress not restored – continuing
intimal hyperplasia and RESTENOSIS

Factors Which Contribute toIn-stent Restenosis (1)
• Thrombus/platelet/fibrin adherence to stent struts.– Anticoagulants
• Heparin – systemically or coated on stent.• Inhibition of the GP IIb-IIIa receptor:
– Prevents platelet aggregation.
– Associated with raised incidence of MI.– PTFE coated stents.
Factors Which Contribute toIn-stent Restenosis (2)
• Metabolic disorder/smoking/atherogenic diet.– Life style changes– Restenosis rate double in insulin dependent
diabetics.
Factors Which Contribute toIn-stent Restenosis (3)
• Intimal hyperplasia due to wall injury from the stent– Brachytherapy:
• Delivery: Radioactive stents, catheter radiation.• May cause necrosis.
– Drug eluting stents• Anti-proliferative agents e.g. rapamycin (Sirolimus)• Improved short term survival and maintenance of vessel patency• More work needed to clarify longer term outcome (Circulation
2008, 118, 1817
• No improvement in outcome in insulin dependent diabetics when compared to bare metal stents
• Impaired ‘healing’ late thrombosis, some doubt about how serious this is. More studies needed. (Circulation 2008, 118, 1783)

Drug Eluting Stent cases2006 data from 86 of 91 centres
?
17
5362 63.5
01020304050607080
% D
ES
ca
se
s
2002 2003 2004 2005 2006
2006 data: Ludman Mean of % use by Centres
http://www.bcis.org.uk/resources/audit/audit_2006

BMS and DES use V PCI for Restenosis
0
10
20
30
40
50
60
70
80
90
100
'92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04 '05 '06
0
2
4
6
8
10
12
14
% Stent
%DES
% Restenosis
2006 data: Ludman
http://www.bcis.org.uk/resources/audit/audit_2006
Factors Which Contribute toIn-stent Restenosis (4)
• Mechanical factors– Stress concentration/bending at end of stent.
• Raised hoop and bending stress sensed by vascular smooth muscle cells → fibrosis/ remodelling
– Flow disturbance within stented region.• Time varying shear stress sensed by vascular endothelium →
release of vasoactive mediators in the short term and remodelling/intimal hyperplasia in the longer term
– Compliant-ended stent

Compliant Ended Stent
• Rigid in the centre to provide recoil resistance
• Parabolic and cantilevered struts– gradual change in compliance and
matching to native vessel– reduces stress concentration and
bending– Less disturbed flow

Experimental assessment of compliant ended stent
Aims• To compare the performance of the CES
and SMART stents over 28 days on vessel and stent dimensions. – To compare the effect of 2 levels of stent
stiffness– To compare the effect of stent oversize

Stents used in the Study
SMART stent
(Commercially available)
Compliant Ended Stent

Method
• 65 stents implanted in the iliac and carotid arteries of 17 Large White pigs
• Lumen diameter determined before and after implantation by angiography– Follow-up angiography on days 3,7 and 28 – At day 28 the arteries were pressure perfused
and removed for histology and micro CT scanning

CESSM
CES
CES
P9 Iliac (day 3)
P12 Carotid (day 7)
CES & Smart stents in common iliac arteries

Vessel dimensions
4
5
6
7
0 5 10 15 20 25 30 35
Position along stent [mm]
Lum
en d
iam
eter
[m
m]

MeasurementsSD Stent diameterLD Lumen diameter
SOS Stent OversizeLOS Lumen OversizeMH Migration/Hyperplasia
100.
pre
prepost
LD
LDSDSOS
LOS LDpost LDpre
LDpre.100
MH SDpost LDpost
LDpost.100

Changes in % lumen oversize with time
SMART (n = 16)
CES (n = 28)
*
LOS LDpost LDpre
LDpre.100
Lumen tends to pre implant dimensions within 1 month
LOS
[%]
5
10
15
20
25
0 10 20 30
Time since implant [day]

Changes in % stent oversize with time
SMART
CES
SOS SDpost LDpre
LDpre
.100
Stent diameter changes little up to 1 month after implantation
SO
S [%
]
15
20
25
30
35
40
0 10 20 30
Time since implant [day]

Changes in stent migration orintimal hyperplasia with time
SMART
CES
MH SDpost LDpost
LDpost.100
CES induces less migration or intimal hyperplasia than Smart stent control
MH
[%]
0
10
20
30
40
50
0 10 20 30
Time since implant [day]
*
*

Palmaz CES
6 week post implantation

Limitations
• Limited resolution of in-vivo X-ray images• Limited study duration
– Part of a larger study with later endpoint
• Can not distinguish between stent migration and intimal hyperplasia– Histology in progress
• Difference in stiffness not yet quantified• Response of carotids & iliacs different to that of
coronaries– NIH develops more slowly

Conclusions
• Lumen diameter relative to immediate post implant diameter decreases with time
• Stent diameter changes little with time• Degree of stent migration or intimal hyperplasia
increases with time.– Effect is small in the compliant ended stent
Micro CT of excised vessels
• Vessels pressure fixed in situ (10% formol saline)
• Excised and immersed in oil based contrast medium
• Custom built Micro CT scanner (Dental Biophysics QMUL)
• Voxel size (30 x 30 x 30µm)
• Images processed on custom software developed under
KS400 (Zeiss) image analysis system


Image processing
Original slice Thresholded Media/Adventita only
Stent struts Ellipse fitted

Slice measurements
x-position [μm]
Intimal hyperplasia in vicinity of struts.Less wall movement?
3D rendering

3D rendering
xy yzxz


Future work1.44-01
1.35-01
1.25-01
1.16-01
1.06-01
9.70-02
8.76-02
7.82-02
6.89-02
5.93-02
4.99-02
4.05-02
3.11-02
2.17-02
1.23-02
2.91-03
0
0.2
0.4
0.6
0.8
1.0
1.2
0 5 10 15 20 25 30 35 40
Axial Position (mm)
Nor
mal
ized
Com
plia
nce
CMS Palmaz
• More extensive experimental study– Effect of stent oversize and stiffness on
intimal hyperplasia– Comparison of different stent types
• Modelling & measurement of interactions between blood/arterial wall/stent
– Haemodynamics and solid mechanics

Who did the work.Joel Berry Engineer Stent designDepartment of Biomedical EngineeringWake Forest UniversityWinston-Salem NC, USA
James Moore Jr. Engineer Stent designDepartment of Biomedical EngineeringTexas A & M UniversityCollege Station, TX, USA
Gemma Ryder PhD student In vivo studyInstitute of Cell and Molecular ScienceBarts and the LondonSchool of Medicine and DentistryLondon, UK
Graham Davis Physicist Micro CTDepartment of Dental BiophysicsQueen Mary, University of LondonLondon, UK
Luke Timmins PhD student Image processingDepartment of Biomedical EngineeringTexas A & M UniversityCollege Station, TX, USA