Poverty Reduction in Multigenerational Households Affected by Migration
Upload
idsCategory
view
1.096download
0description

1
Internal Migration and 'Rural/Urban‘
Households in China:
Implications for Health care

2
Origins of POVILL Research
• Anecdotal evidence from poor villages:
Elderly + young children
High prevalence of chronic illness
Vulnerability
• New Cooperative Medical Scheme (NCMS)
Government subsidy
Risk fund for inpatient care
• ‘Catastrophic healthcare expenditure’
Model: Get sick – Buy care – Get well
Extreme reductionism (Dennett)

3
The Limits of ‘Catastrophic
Healthcare Expenditure• High expenditure on healthcare (even relative to
income) not necessarily ‘catastrophic’.
• Adoption of approach by policy makers encouraged a
excessive focus on hospital inpatient expenditures
• Variety of mechanisms through which health shocks
and poverty may interact: Acute events requiring costly hospital care
Chronic illness requiring long-term medication
Less serious but often recurring acute illnesses
Long-term, possibly progressive, conditions that completely or
partially disable the sufferer
Stigmatising illnesses may induce loss of status, isolation, rejection
and persecution.
• Poorest often cannot afford ‘catastrophic health
expenditure’.

4
Illness-Poverty Links(China National Heath Service Survey 2008)
0 5 10 15 20 25 30
Lack labour
Natural conditions/disaster
Disease: low productivity
Disease: treatment cost
Unemployment
Man made causes
Other

5
The POVILL project• Aims:
Understand the potentially complex impacts of
major illness on household livelihoods for a
substantial number of households
Select households using a probability sampling
approach to make valid statistical inferences to the
overall study area populations.
• Major illness conceived very broadly: health problems
which had the potential to seriously damage household
livelihood strategies.
• Primary causal pathways to impoverishment seen as:
Increased expenditures on healthcare
Limitations on household activities, linked to illness-
induced changes in labour demand and supply.

6
Research Methods• Existing knowledge mainly derived from questionnaire
surveys that collect information on illness, care seeking
behaviour and expenditure, typically on the basis of a
two-week recall for acute illness episodes and a one
year recall for inpatient treatments.
• Even panel surveys have limited ability to capture the
step-by-step process whereby households cope, or fail
to cope, with consequences of ill-health.
• Alternatives:
Case studies: fascinating but limited scale
Monitoring surveys: increased reliability but limited
to relatively simple data and modest sample size
Demographic surveillance sites: interesting
possibility (if one exists), difficult ethical problems.

7
POVILL Approach
• Rapid and reasonably large-scale household
questionnaire survey using cluster sampling of
households within selected study areas:
identify households substantially affected by
different categories of serious health problem
estimate the proportions of such households in the
population.
• Sampled households stratified using survey data.
• Probability sample of households within selected strata
• In-depth studies (1-2 person days) of these household
undertaken by teams of social scientists

8
In-Depth Studies
• Collected both quantitative and qualitative data. Specific
intention to derive reasonably reliable estimates of
incomes, expenditures, health care cost, financial
support received, duration of illness or disability, etc.
• Underlying framework was an ‘illness narrative’ to
document the history of each health problem addressed.
• Four main components:
Narrative and construction of one year time line
Identification of ‘events’: start points for changes in
health status, treatment, assistance, assets, other.
Detailed description of events
Dating/quantifying events to the extent possible

9
Illustrative One-Year Timeline
2006 2007 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Back Village Condition Township Borrow money County pain. Health worse. Unable Hospital to buy drugs. Hospital limits Station to farm. Son activity returns to help

10
Three Transitions
• Demographic
Low mortality and low Fertility
•Epidemiological
Acute infectious disease → chronic NCDs
•Economic
Planned → ‘Socialist Market’

11
Resident and Migrant
PopulationsTotal
Population
Resident at
least 6 months
Absent more
than 6 months
0-14 15.9 20.2 7.6
15-19 9.2 5.9 15.5
20-39 29.9 12.8 63.4
40-49 12.8 14.4 9.6
50-59 15.3 21.5 3.1
60-69 10.2 15.1 0.7
70+ 6.8 10.1 0.2

12
Resident and Migrant
Populations
• Internal migration: 30% of rural population.
• 90% of men and 70% of women between the ages of 20 and 35 reported as living away from home for part of year (90% migrate 6 months or longer).
• So the resident population is dominated by those under 15 (21%) or over 50 (48%).
• 16.6% of rural residents aged 65 and over (UK:16%). 0
10
20
30
40
60
70
80
90
100
age
600 500 400 300 200 100 100 200 300 400 500 600Population
Male
Female
M-living away
F-living away
Population and living away from home

The countryside is exporting good
health and re-importing ill-health.
• First, young and healthy people are more
likely to migrate than elderly people,
leaving the weak and sick at home.
• Second, more serious and incapacitating
diseases and intensive-care conditions
result in a migrant’s return to the home in
the village to seek family support and to
avoid the high medical and living costs in
cities.

14
Reason given by migrants for
returning home
0 5 10 15 20 25 30
investment
marriage
can't find job
Pregnancy, delivery & upbring
take Care of family member
Too old
illhealth
%

15
Self reported serious illness
over previous year0
51
01
52
02
53
03
54
04
55
0p
rop
ort
ion
of p
op
ula
tio
n(%
)
15 20 25 30 35 40 45 50age
migration left behind

16
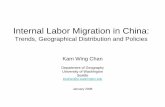
‘Rural/urban’ Households
Traditional
household
Return due
to illness
Return to care
for others
Rural/urban
household
Reunited in
urban area
Members left-
behind
Elde
rly on
ly
Thre
e ge
ne
ration
Migrants
Nuclear
family
Extended
family
Elde
rly + ch
ildre
n
Pare
nt +
child
ren
single
cou
ple
40% 60%
14% 23% 11% 12%
56%
44%

17
Four main health insurance
schemes in China
• Government staff(free medical service,FMS)
5% population 100% coverage
• Basic Medical Insurance (BMI)
Urban employees, 28% coverage 2006
• Urban Basic Medical Insurance (UBMI)
Other urban residents, aim: 100% coverage by 2010
• New Community Medical Scheme (NCMS)
Rural residents, 57% population, 87% coverage 2007

18
Heath insurance scheme
coverage for migrants in Beijing
none46%NCMS
41%
CI6%
BMIS2%
FMS2%
other3%

19
Reimbursement of NCMS

20
Chronic illness healthcare costs

21
Urban/Rural and Decentralisation
Poor county
Healthy labor exported
Less enterprises and jobs
Very limited govt revenue
Elderly less-healthy remain joined by returning ill migrants
Shanghai
Healthy labor imported
More enterprises and jobs
High government revenue
Well funded health insurance
demand
supplysupply
demand
Limited health insurance
Younger, healthier population
health
Ill-health

Shanghai compared to
Western provinces
• In Shanghai, the government plus
personal financial contribution to the rural
NCMS was around 450 yuan per person
• Compared with only 50 yuan per person
in most provinces in Western China.
22

23
Questions
• Can segmented (urban/rural) and highly
decentralised health care and health
insurance systems cope with these new
ways of constructing family units?
• What happens next?
• What are the implications for the Chinese
economy?
• How do we conduct research on these
new ‘households’?