IHC on cytology specimens from pancreas, liver and bile...
5
IHC on cytology specimens from pancreas, liver and bile ducts David F. Schaeffer Department of Anatomical Pathology Vancouver General Hospital A ‘quick’ practical review Disclosure • No relevant financial relationship with commercial interest to disclose. Multiple choice question A single large hepatic mass is identified on screening ultrasound in a 44 year old woman with negative hepatitis serology. FNA shows malignant cells, that label focally positive with CK19 and CK7, while other areas are HepPar-1 positive. IDH-1 shows focal positivity. These features are most consistent with: A. Fibrolamellar HCC B. Metastatic gastroesophageal carcinoma C. Combined Hepatocellular-Cholangiocarcinoma D. Intrahepatic cholangiocarcinoma. E. Bile duct hamartoma Learning objectives • Review specimen procurement in hepatobiliary and pancreatic (HPB) cytology. • Discuss the addition of immunohistochemistry in increasing the diagnostic accuracy of fine needle aspiration specimens. • Discuss diagnostic pitfalls in HPB cytology. Hepatobiliary and pancreatic diseases Public domain http://www.hopkinsmedicine.org/gastroenterology_hepatology/clinical_services/ad vanced_endoscopy/endoscopic_retrograde_cholangiopancreatography.html Endoscopic retrograde cholangiopancreatography (ERCP)
Transcript of IHC on cytology specimens from pancreas, liver and bile...

IHC on cytology specimens from pancreas, liver and bile ducts
David F. Schaeffer
Department of Anatomical Pathology
Vancouver General Hospital
A ‘quick’ practical review
Disclosure
• No relevant financial relationship with commercial interest to disclose.
Multiple choice question
A single large hepatic mass is identified on screening ultrasound in a 44 year old woman with negative hepatitis serology. FNA shows malignant cells, that label focally positive with CK19 and CK7, while other areas are HepPar-1 positive. IDH-1 shows focal positivity. These features are most consistent with:
A. Fibrolamellar HCC
B. Metastatic gastroesophageal carcinoma
C. Combined Hepatocellular-Cholangiocarcinoma
D. Intrahepatic cholangiocarcinoma.
E. Bile duct hamartoma
Learning objectives
• Review specimen procurement in hepatobiliary and pancreatic (HPB) cytology.
• Discuss the addition of immunohistochemistry in increasing the diagnostic accuracy of fine needle aspiration specimens.
• Discuss diagnostic pitfalls in HPB cytology.
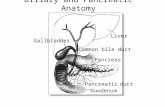
Hepatobiliary and pancreatic diseases
Public domainhttp://www.hopkinsmedicine.org/gastroenterology_hepatology/clinical_services/ad
vanced_endoscopy/endoscopic_retrograde_cholangiopancreatography.html
Endoscopic retrograde cholangiopancreatography (ERCP)

Endoscopic ultrasound (EUS)
http://trialx.com/curebyte/2012/10/20/images-related-to-endoscopic-ultrasound/
http://arabhealthmagazine.com/endoscopic-ultrasound/
1.5 cm
FNA specimens after EUS
Eltoum A et al. Arch Pathol Lab Med. 2012;136:447–453
Does IHC help in increasing accuracy?
Site n (%)
Pancreas 62 (73)
Stomach 8 (9)
Lymph nodes 6 (7)
Retroperitoneum 5 (6)
Bile duct 3 (4)
Duodenum 1 (1)
Total 85
EUS characteristics
Size of lesions [range] 4 cm [0.5 – 16]
Visible mass 98%
Needle size [22G] 82%
Needle passes [avg] 2.6 [1-4]
O’Connor et al. Cancer Cytology 2014 (submitted)
Cytology result
IHC
Follow-up
Category nBenign Malignant/
Neoplastic
Malignant 45 (53%) 20 (44%) 0 45 (100%)
Suspicious 8 (10%) 3 (38%) 0 6* (75%)
Atypical 6 (7%) 0 2 (33%) 4 (67%)
Benign 24 (28%) 0 16 (67%) 6* (25%)
Non Diagnostic 2 (2%) 0 0 2 (100%)
Total 85 (100%) 23 (27%)
Diagnostic yield and accuracy
*no follow up for 4 biopsies (5%)
Accuracy – Malignant / Neoplastic
Cytologic Diagnosis n=45 Excision/imaging confirmation n
Adenocarcinoma 34 (76%) Adenocarcinoma 34 (100%)
IPMN 1 (2%) (invasive) IPMN 1 (100%)
NET 3 (7%) NET (G1 (33%); G2 (66%)) 3 (100%)
GIST 4 (9%) GIST 4 (100%)
Lymphoma 2 (4%) High grade lymphoma 2(100%)
SPPT 1 (2%) SPPT 1(100%)

Cytology result Follow-up
Category n Dx n
Suspicious 8 (10%)
AdenoCa
Lymphoma
GIST
No f/u
3 (37%)
2 (25%)
1 (13%)
2 (25%)
Atypical 6 (7%)
AdenoCa
Benign
NET
SCA
2 (33%)
2 (33%)
1 (17%)
1 (17%)
Benign 24 (28%)
AdenoCa
Cystic neoplasm
GIST
No f/u
3 (13%)
2 (8%)
1 (4%)
2(8%)
Non Diagnostic 2 (2%)GIST
NET
12 (50%)
1 (50%)
Discrepant Follow-up Comparison studies
Study Accuracy Diagnostic yield
Without on site evaluation
Iglesias et al. 67% 87%
Kim et al. 46% 95%
Nguyen et al. 78% 97%
Our study 72% 98%
With on site evaluation
Iglesias et al. 91% 99%
Turner et al. 80% 98%
Eloubeidi et al. 83% 98%
Nguyen et al. Gastrointest Endosc 2009; 69: 1264-1270
Turner et al. Gastrointest Endosc 2012; 71: 91-98
Eloubeidi et al. Cancer Cytopathol 2003; 99: 285-292
Iglesias et al. Am J Gastroenterol 2011;106:1705-1710
Kim et al. J Clin Gastroenterol 2013;doi 10.11112
Critical adjunct information
Cytopathology is a triple test:
1. Clinical impression/information
2. Radiologic impression
3. Cytologic features
Endoscopy report:
� Demographics
� Hx of obstruction/stent
insertion
� Metabolic/hormonal
changes
� Weight loss
� Location of lesion
� Size
� Solid vs cystic
� If cystic -> association
with pancreatic duct
� Lymph nodes
Cytopathology is a quadruple test:
1. Clinical impression/information
2. Radiologic impression
3. Cytologic features
4. Immunohistochemical results
Diagnostic pitfalls
• HCC vs metastatic malignancies
• wd-HCC vs hepatic adenoma/FNH
• Cystic neoplasms of the pancreas
• IgG4 staining in the setting of pancreatitis
1. HCC vs. Metastatic malignancies
Hepatocellular carcinoma:
• Trabecular/acinar
• Sinusoidal endothelial cells
• Bile production
Cell block
HepPar-1IHC in HCC:
• HepPar-1
-> can be lost in poorly differentiated lesions
• pCEA/CD10
• AFP
-> beware of hepatoid (metastatic) carcinomata
CD10
1. HCC vs. Metastatic malignancies
Features that are associated with frequent misclassification of metastatic adenocarcinoma as HCC:
• Moderate amounts of granular cytoplasm
• Round nuclei with even chromatin
• Prominent trabeculae, bare nuclei and endothelial wrapping
Renshaw, A. A., J. Haja, et al. (2006). "Fine-needle aspirates of hepatocellular
carcinoma that are misclassified as adenocarcinoma: correlating cytologic
features and performance in the College of American Pathologists
Nongynecologic Cytology Program." Arch Pathol Lab Med 130(1): 19-22.
If in doubt: HepPar 1 +/- CD10

Cholangiocarcinoma
68 yr old woman:
• Known chronic HBV
• New liver lesion
Cell Block CK19
HepPar-1
Combined HCC-Cholangiocarcinoma
IDH1 in intrahepatic cholangiocarcinoma:
• IDH1 R132C mutation present in 30%
• Positive staining for IDH1
• Not yet verified in CytoLyte® preparations
Neuroendocrine tumours
Neuroendocrine tumours:
• Isolated (stripped) cells
• Eccentrically place nuclei
• Salt and pepper chromatin
IHC - NET:
• Synaptophysin
• Chromogranin A -> serum levels
• ki67
Synaptophysin Ki-67
Ki67 in FNA of NETs:
• Interpret with caution
• Sampling may over- or under call
• ‘Hot Spots’
Metastatic melanoma
76 yr old man:
• Known choroidal melanoma
• US showed suspicious new lesion
Melanoma IHC - CytoLyte®:
• HMB45
• Melan A
• S100 – may stain some CA
Varying success
BRAFV600E
Resection
2. wd-HCC vs. hepatic adenoma / FNH
If possible, advise to perform core needle biopsy!
Hepatic adenoma:
• Virtually impossible to separate from wd-HCC
• Advise against subclassification on FNA
• I do not perform beta-catenin
FNH – Glutamin synthetase:
• Marks hepatocytes in large anastomosing areas in a ‘map-like’ pattern.
• Not expressed in hepatocyte close to fibrotic bands
• Positive in wdHCC but in a diffuse pattern
HA - Glypican 3:
• High sensitivity for HCC
• Less helpful in wdHCC:
• Only 50% of wdHCCpositive
• HA and large regenerative nodules negative
• 43% of high-grade dysplastic nodules positive
Shafi zadeh N, et al. Utility and limitations of glypican-3expression for the diagnosis of hepatocellular carcinoma at both ends of the differentiation
spectrum. Mod Pathol. 2008;21:1011–1018.Bioulac-Sage P, et al. Over-expression ofglutamine synthetase in focal
nodular hyperplasia: a novel easy diagnostictool in surgical pathology. Liver Int. 2009;29(3):459–465.
FNH:
• Abundant normal-appearing hepatocytes
• Numerous ductal-type epithelium in sheets and clusters
3. Cystic neoplasms of the pancreas
Tumor Cytologic features
Serous cystadenoma Loose sheets and groups of single
monomorphic cuboidal/low columnar epithelial
cells; often proteinaceous background.
Mucinous Cystic neoplasm Sheets and groups of columnar epithelium
with variable degree of nuclear atypia and
crowding; variable amount of mucin in
background.
Solid Pseudopapillary tumor Fragments with fibrovascular cores lined by
bland cells with nuclear grooves and scant
cytoplasm.
Endocrine tumor Monomorphic, often discohesive,
monomorphic plasmacytoid cells with ‘salt
and pepper’ chromatin.
SPPTIHC - SPPT:
• Beta-catenin (nuclear)
• A1AT
• PR
• Racemase (P504s)
• Synapthophysin
• Chromogranin A
Beta-catenin
A1ATProgesterone Receptor
Cyst fluid analysis
• Kras based testing
• Proprietary systems
• Likely to supplement cytological assessment
• To be evaluated in conjunction with clinical info and cyst fluid marker assessment

4. IgG4 staining – pancreatitis
Autoimmune pancreatitis:
• Lymphoplasmacytic sclerosing pancreatitis
• Duct-destructive chronic pancreatitis
• Sclerosing chronic pancreatitis
54 year old woman with pancreas ‘mass’ on EUS.
? AIP
Do IgG4.
Periductal lymphoplasmacytic inflammationIgG4 – Type 1Storiform fibrosis
4. IgG4 staining – pancreatitis
54 year old woman with pancreas ‘mass’ on EUS.
? AIP
Do IgG4.
IgG4
Definitive diagnosis requires core needle biopsy.
?
4. AIP Diagnosis – Ampullary bx
IgG4 IgG4 + cells in Ampulla:
• >50/hpf - highly suggestive
• 10-50/hpf - equivocal
• < 10/hpf - unlikely
Moon Sh, Kim MH, Park D. et al. IgG4 immunostaining of
duodenal papillary biopsy specimens may be useful for
supporting a diagnosis of autoimmune pancreatitis. GastrointestEndosc. 2010 May;71(6):960-6.
Multiple choice question
A single large hepatic mass is identified on screening ultrasound in a 44 year old woman with negative hepatitis serology. FNA shows malignant cells, that label focally positive with CK19 and CK7, while other areas are HepPar-1 positive. IDH-1 shows focal positivity. These features are most consistent with:
A. Fibrolamellar HCC
B. Metastatic gastroesophageal carcinoma
C. Combined Hepatocellular-Cholangiocarcinoma
D. Intrahepatic cholangiocarcinoma.
E. Bile duct hamartoma
A. Fibrolamellar HCC
B. Metastatic gastroesophageal carcinoma
C. Combined Hepatocellular-Cholangiocarcinoma
D. Intrahepatic cholangiocarcinoma.
E. Bile duct hamartoma
Thank you!