
Harrison_Amelia_RP_Word
46
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers. 12095238 The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers. Department of Exercise and Sport Science, Manchester Metropolitan University, Crewe, Cheshire, United Kingdom. BSc Exercise and Sport Science Amelia Molly Harrison 1
-
Upload
amelia-harrison -
Category
Documents
-
view
9 -
download
0
Transcript of Harrison_Amelia_RP_Word
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
12095238
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Department of Exercise and Sport Science, Manchester Metropolitan University, Crewe, Cheshire, United Kingdom. BSc Exercise and Sport Science
Amelia Molly Harrison
Abstract:
Caffeine has social acceptance with widespread use with 90% of people consuming it in the
form of a coffee beverage in the United States of America (Burke, 2008). Caffeine has mainly
been used for its stimulant properties in daily life and in an athletic population as it’s been
shown to increase wakefulness and motor skills including attention and increase time to
exhaustion. Although caffeine is said to have varying effects both in a cognitive,
physiological and cardiovascular way performance results have been inconsistent partially
1
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
due to exceedingly too high dosages or too low, Furthermore many studies have not
accounted for other factors such as age, gender, habitual usage, smoking and dietary intake.
The primary aim of the present study was to investigate caffeine’s effects on cardiovascular
parameters at rest, comparing habitual high versus habitual low consumers who drink either
black tea or coffee. Seven participants were segregated based on their consumption habits,
habitual low = (0-1 cup/day) and habitual high = 92-3+/day), and reported for testing on two
occasions. The single blind study involved collecting blood pressure (BP), Blood glucose and
blood flow vascular kinetic changes using colour Doppler ultrasound method. (FV1, RI, IMT
and Vm) at 0, 10, 20, 30 and 60 minutes post ingestion. Heart rate (HR) data was obtained
every three minutes. One session contained a caffeinated beverage and the other a
decaffeinated beverage (placebo) based on a 6mg/Kg body weight dosage. No significant
differences were found between Treatment, History or Time*History*treatment. This may be
partially due to small sample sizes or methodological issues within the study which should be
considered in future studies.
Acknowledgements:
I would like to thank all of my participants who gave up their time to take part in this
research project, my supervisor Gladys Ombele Pearson for all the help and support during
my final year and throughout my dissertation. Finally, I would like to thank my parents and
friends for their undivided love and support through this stressful year.
2

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Table of ContentsAbstract:............................................................................................................................................2
Acknowledgements:..........................................................................................................................2
Key words.............................................................................................................................................3
Introduction:......................................................................................................................................3
Method..............................................................................................................................................6
Subjects and ethics............................................................................................................................6
Procedures:.......................................................................................................................................7
Statistical analysis:...........................................................................................................................10
3

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Results:............................................................................................................................................10
Discussion:...........................................................................................................................................16
Limitations:..........................................................................................................................................21
Statistical difference tests:..................................................................................................................22
Conclusion:..........................................................................................................................................23
References:..........................................................................................................................................23
Key words:
Caffeine, Coffee, Habitual, High, Low, Rest.
1. Introduction:
The drug caffeine is commonly consumed by the global population with reports suggesting
90% of adults consuming it in their everyday diets (Burke, 2008). The average consumption
of coffee within adults is equivalent to approximately two to three cups or 272 milligrams
4

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
(mg) per day (Corti et al. 2002). The gastrointestinal track absorbs caffeine rapidly and peak
plasma caffeine concentrations are reached within 30-60 minutes after ingesting the beverage
(Greer, 1998).
The stimulating effects of caffeine on improving daily performance such as motivation and
attention have been targeted, not only by athletes but by shift workers, long-haul truck
drivers, and members of the armed forces. These individuals regularly need to fight fatigue
and prolong their capacity to undertake their occupational activities during stressful
conditions (Burke, 2008). Although caffeine is consumed for the taste in the form of coffee
and tea, many consume it for its stimulant properties. Previous research has indicated that
caffeine may be a beneficial ergogoenic aid for athletes in various exercise modes, intensities
and durations (Douglas et al. 2002). It must be noted, however, that many studies have not
focused on testing participants in solely resting conditions, as well as this studies have not
investigated habitual high and habitual low history during rest. This may be helpful when
looking at the interaction between coffee consumption and tolerance levels over a specified
time period within different groups of people. Jackman et al. (1996) suggested that one key
benefit sort after by athletes is the delayed feeling of fatigue. Increased time to exhaustion
and increased fatty acid oxidation has also been reported to be a beneficial effect of
consuming caffeine (Chad and Quinele, 1989). Furthermore, previous research has also
shown that antioxidants found in coffee, such as chlorogenic acids have been recognised to
improve glucose metabolism and insulin sensitivity (Vandam, 2013). Not only this, but
coffee has been also demonstrated to have cardiovascular effects such as increased blood
pressure (BP) (by up to 14mmHg) in normative subjects under resting conditions (Robertson
et al. 1987). Previous authors Mahmud and Freely. (2001), stated that in males, caffeine
increases BP by increasing vascular resistance with no effect on cardiac output (Q). Hearltey
et al. (2004), stated that the vascular resistance increase is consistent with the blockage of
5

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
vascular adenosine receptors in caffeine, which enhances the action of noradrenalin (Hatano
et al.1995). Several effects are thought to be correlated with high caffeine drinking on
cardiovascular parameters such as increased HR, vascular resistance (RI) and BP. Not only
this, but caffeine has also been found to impact on physiological parameters such as,
potassium (K+) accumulation. The increase in K+ has the effect of inhibiting muscle
contractions as caffeine interferes with the uptake of calcium (CA2+) by the sarcoplasmic
reticulum in striated muscle. This action can account for observations, that such
concentrations of caffeine increase the strength of contractions in both skeletal and cardiac
muscle (Graham, 2001). Fat metabolism has also been shown to increase with the
consumption of caffeine (O’keefe et al. 2013). In resting conditions, caffeine causes increases
in BP (Robertson et al. 1978; Sung et al. 1990) and systemic vascular resistance (Sung et al.
1990). Moreover, caffeine has been shown to produce increases in plasma rennin activity
(Robertson et al. 1978; Van Soeren et al. 1993) and it has been further hypothesised that this
is through a plasma Angiotensin II (ANG II) concentration response (Daniels et al. 1988).
Although Lane and Williams (1985), suggest potential caffeine stress interactions, the results
were obtained from subjects who were not regularly exposed to caffeine. However, Lane et
al. (1987), reported that the regular caffeine consumer would be at a greater risk from
caffeine stress interactions, due to their increased exposure. Moreover, one could however
argue that regular use of caffeine might lead to the development of drug tolerance that could
lead to a reduction, or eliminate the caffeine-stress interactions seen to date (Lane et al.
1987).
In view of these factors, this study sought to compare high habitual caffeine drinkers (two +
cups of coffee/tea) versus low caffeine drinkers (one cup or less). The intervention was
6

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
provided through the ingestion of a coffee beverage in one session, and a de-caffeinated
coffee beverage (placebo) in the second session, separated from the first session by seven
days. It should be noted that although the decaffeinated beverage served the purpose of a
placebo condition it does in fact contain a small dosages of caffeine. Where decaffeinated
coffee contains around 2mg per cup and instant caffeinated cup contains 27mg (Suleman et
al. 1994). The primary aim of this study was to determine the acute effects of caffeine on
cardiovascular parameters. These included blood flow kinetics. And the effects over a period
of 60 minutes, within habitual high versus habitual low populations. The secondary second
aim of the study was to investigate the metabolic effects of caffeine ingestion and blood
glucose level and indirect calorimetry. It was hypothesised that ingestion of caffeine would
increase BP, heart rate (HR) and blood plasma volume. It was also hypothesised that through
the ingestion of caffeine, vasoconstriction will occur more so in habitual low consumers.
2. Method:
2.1 Subjects and Ethics
This study was granted ethical approval by the Manchester metropolitan university taught
programmes Ethics committee TPEC prior to testing beginning. Seven healthy active males
who participated in physical activity over 30 minutes weekly, were recruited to participate in
this study. Participants were informed of the procedures, methods, benefits and possible risks
(slight headaches and minimal bruising from the finger tip sample) during a familiarisation
session before written consent was obtained.
Of the seven recruited participants, two participants withdrew from the study creating an
attrition rate of 29% .The remaining five participants were split into two groups according to
7
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
their habitual consumption of coffee or black tea beverages. The two groups being Habitual
high (2-3+ cups) n=3 versus Habitual low drinkers (0-1) n=2.
2.2 Inclusion Criteria:
The following inclusion criteria were applied. Participants were between the ages of 18-25,
physically active at least three times weekly, non resistance trained. Participants were also
free of any underlying health conditions such as diabetes and must have been injury free for
three months prior to testing.
Participants were asked to abstain from alcohol, caffeine and exercise 24 hours prior to
testing although they must have drank coffee on a regular basis three times a week
consuming either 0-1 coffee/tea (habitual low n=2) or consume 2+ cups daily (habitual high
n=3) these constraints were constructed in order to minimise any experimental error and for
the purpose of group habitual segregation.
2.3 Procedures:
Baseline measurements of body height and mass were collected using a wall mounted
Stadiometer ( 222 stadiometer, Seca, Birmingham) and balance scales (711, Seca,
Birmingham), respectively. These measures were obtained prior to testing in order to
determine the dosage required based on 6mg/Kg of body weight dosage with 250ml of hot
water (Daniel’s et al. 1989). During the single blind study, participants reported to the
laboratory at the Manchester Metropolitan Cheshire campus, on two occasions with a seven
day wash out period. During the first session participants were provided with a decaffeinated
(placebo – rich roast decaffeinated instant coffee granules, the co-operative, Manchester)
beverage and given five minutes time to consume it. During the second session participants
8

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
were provided with a caffeinated (fair-trade rich roast caffeinated instant coffee granules, the
co-operative, Manchester) beverage and as per session one participant’s were given a five
minute consumption time. Both tests were preceded by a standardized five minute rest period
for rest HR collection.
In order to reduce the effects of circadian variations and physiological responses to the
environment (i.e. excitement owing to lighting and/or noise) both sessions were conducted at
the same time of day in as close to the same laboratory environmental conditions as possible.
Resting cardiovascular (CV) kinetics was obtained. These included, Heart rate using a (Polar
FTI 90037558, Polar Oulu, Finland HR monitor), BP using a manual blood pressure
sphygmanomomeitor (Omron M2 Basic digital automatic BP monitor Hoofddorp,
Netherlands) and blood glucose using finger tip sampling methods (Accutrend Roche Bascel,
Switzerland). The (AU5 Harmonic colour Doppler ultrasound Genoa, Italy) the ultrasound
scanning was conducted colour Doppler mode. The probe was placed on the carotid artery as
parallel as each participant’s vasculature would 1cm distal from the carotid node; the depth of
the scanning was 55.3mm with a frequency of US beams of 27 of to note any vascular kinetic
changes were obtained using a 60 º inclination angle. The vasculature kinetic measurements
obtained via ultrasound methods included (FV1),VM2, intermedial thickness (IMT) and RI
index. All stated tests were performed pre consumption of the beverages and then 10, 20, 30
and 60 minutes post ingestion, with the exception of HR data which was collected every three
minutes for 45 continuous minutes.
9

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
2.4 Statistical Analysis:
Data compiled was analysed and checked for parametricity based on the four parametric
assumptions. Homogeneity of variance was tested using a Shapiro Wilkes, with sphercity
tested using Mauchley’s test of sphercity given the repeated measures design of the study.
Normality of distribution was assessed using the Levenes test and the data was known to be
ratio or interval and independently collected. Having followed these procedures, Thus data
was found to be parametric (DBP and Vm) and non-parametric (SBP, HR, RI, IMT, FV1,
Blood glucose). In the case of non-parametric data a Friedman’s signed rank test was
performed in. Where data was parametric a repeated measures analysis of variance
(ANOVA) was performed across both the decaffeinated and caffeinated conditions, as well as
between habitual high and habitual low participants. Data was analysed in statistical package
10
Figure 1. Indicating the set up of the testing protocol
before the consumption of either beverage. Pre tests at
0 minutes had been performed
Figure 2. Colour Doppler AU5 ultrasound on
the carotid artery after the consumption of the
caffeinated beverage. (A) Vessel dimensions
including intermal diameter and IMT thickness.
Figure 3. Indicates blood flow kinetics. These included the capture of the vascular flow integral peaks
with the Fv1, RI and Vm data for one participant after a caffeinated beverage. An average was taken
after 15 peak traces, at each phase of the intervention
A

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
for the social sciences (SPSS) Data are presented as mean ± Standard Deviations (Mean ±
SD). A significant Alpha was set at P<0.05 95%.
3. Results:
Mean ± SDHistory N Height (cm) Weight (KG) Age (yrs)
Habitual High Drinkers 3 175.5± 1.15 71.0± 11.1 20 ± 1.15
Habitual Low Drinkers 2 185.6 ± 10.9 71.2 ± 10.9 22 ±1.41Table 1. Indicates Anthropometric Demographic Data. Height (cm), Mass (Kg), Age (yrs)
collected from the study cohort.
11
Figure 4. Indicates mean and SD error bars for both treatment conditions, for BP Diastolic (mmHg). Square represents Caffeine beverage and triangles denotes the Decaf condition.
0 10 20 30 40 50 6050
55
60
65
70
75
80
85
90
Habitual High
Habitual Low
Time (m)
DBP
Deca
ffina
ted
(mm
Hg)
0 10 20 30 40 50 6050
60
70
80
90
100
110
120
Habitual High
Habitual Low
Time (m)
DBP
Caffe
ine
(mm
Hg)

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
A Repeated measures ANOVA was conducted on diastolic blood pressure (DBP) with no
statistical significance found between treatment conditions, time and history. Within the time
element, there were no significance in DBP F (1, 4) =.899 P>0.05. Analysing history between
habitual high and low consumers found no significant difference F (1, 4 =) 2.095 P<0.05.
Treatment also indicated no significant effect F=.200 P>0.05 There were also no significant
interaction between the interaction within treatment and history F (1, 4) =.705 P>0.05
Nonetheless it is interesting to note that the caffeine condition DBP peaked at 30 minutes
post ingestion with a mean 80.8 +9.25 mmHg, where as during the Decaffeinated condition
DBP peaked at 10 minutes post ingestion mean value 80.6 +6.10mmHg (Figure 4).
12
0 10 20 30 40 50 60110
112
114
116
118
120
122
124
126
128
130
Habitual HighHabitual Low
Time (m)
SBP
caffi
nate
d (m
mHg
)
0 10 20 30 40 50 60100
105
110
115
120
125
130 Habitual High
Habitual Low
Time (m)
SBP
Deca
ffina
ted
(mm
Hg)

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Mean average results for the decaffeinated condition indicate the largest decline was 10
minutes post ingestion. Whereas in the caffeine condition, results show a slower progression
with no immediate drop in systolic blood pressure (SBP) until 30 minutes post ingestion. The
largest declines in SBP between the caffeinated and decaffeinated condition was 5% and the
difference in the highest reported results in both treatments were 0.8%. There was no
statistical difference between SBP and interaction between time, treatment, history nor
time*history interactions. Decaffeinated treatment χ2 (4) =6.833 p>0.05, caffeine treatment
χ2 (4) = .330 P>0.05. Within the History there were no significant interactions. High history
χ2 (4) = 2.345 P>0.05, Low history χ2 (4) = 2.359 P>0.05
13
Figure 5. Mean and SD error bars for SBP values, across the elected five time periods, for both treatment conditions.

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
A Friedman’s signed rank test was conducted on treatment conditions. No significant
interactions were found between HR and treatment conditions, in the decaffeinated condition
14
0 10 20 30 6050.0
55.0
60.0
65.0
70.0
75.0
80.0
85.0
90.0
Habitual High
Habitual low
Time (m)
Hear
t Rat
e (B
PM) c
affei
ne
0 10 20 30 6050.0
55.0
60.0
65.0
70.0
75.0
80.0
85.0
90.0
95.0
100.0
Habitual high
Habitual low
Time (m)
Hear
t Rat
e (B
PM) D
ecaffi
nate
d
Indicates mean values with SD error bars, HR (BPM) over a period of
five time intervals. The Grey bars represent the Caffeine condition and the black
represents Decaf condition (placebo)

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
χ2 (4) = 4.939 p>0.05or the caffeinated condition χ2 (4) = 5.388 p>0.05. A one way repeated
measures ANOVA was conducted based on the participant’s history F (1,4) =.148 p>0.05and
no significant effect was found.
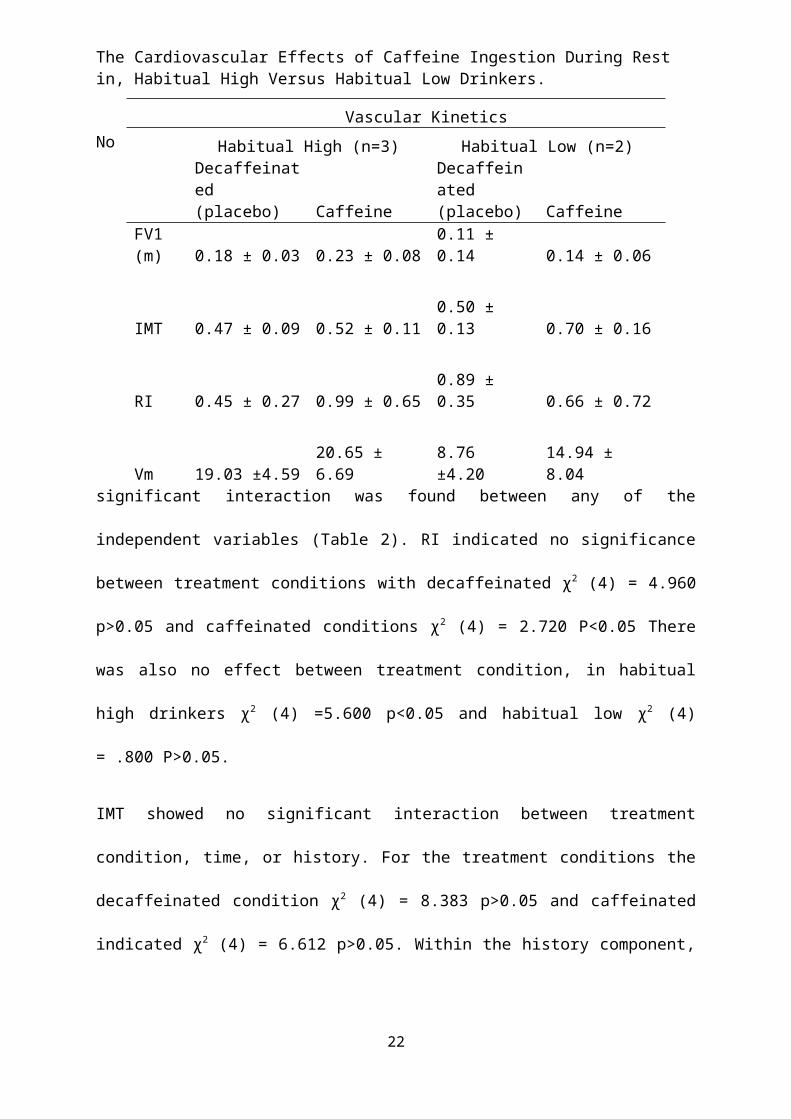
Table 2. Indicates the (mean ± SD) vascular kinetics obtained from the AU5 colour Doppler ultrasound during both conditions, segregated by habitual consumption of caffeinated drinks.
No significant interaction was found between any of the independent variables (Table 2). RI
indicated no significance between treatment conditions with decaffeinated χ2 (4) = 4.960
p>0.05 and caffeinated conditions χ2 (4) = 2.720 P<0.05 There was also no effect between
treatment condition, in habitual high drinkers χ2 (4) =5.600 p<0.05 and habitual low χ2 (4)
= .800 P>0.05.
IMT showed no significant interaction between treatment condition, time, or history. For the
treatment conditions the decaffeinated condition χ2 (4) = 8.383 p>0.05 and caffeinated
15
Vascular Kinetics
Habitual High (n=3) Habitual Low (n=2)
Decaffeinated (placebo) Caffeine
Decaffeinated (placebo) Caffeine
FV1 (m) 0.18 ± 0.03 0.23 ± 0.08 0.11 ± 0.14 0.14 ± 0.06
IMT 0.47 ± 0.09 0.52 ± 0.11 0.50 ± 0.13 0.70 ± 0.16
RI 0.45 ± 0.27 0.99 ± 0.65 0.89 ± 0.35 0.66 ± 0.72
Vm 19.03 ±4.59 20.65 ± 6.69 8.76 ±4.20 14.94 ± 8.04
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
indicated χ2 (4) = 6.612 p>0.05. Within the history component, there was also no significance
for habitual high χ2 (4) = 3.593 p>0.05 and habitual low χ2 (4) = 4.821 P>0.05
No significant interaction occurred in blood flow between treatment, history or time. Within
the treatment conditions the decaffeinated condition indicated χ2 (4) = 4.583 P>0.05 and the
caffeinated condition χ2 (4) = 6.424 P>0.05 Participants history failed to reach significance
as habitual high was χ2 (4) = 8.339 p>0.05 and habitual low was χ2 (4) = 4.400 p>0.05.
There was statistically no significant effect of Vm on history F (1, 4) = 9.304 P>0.05. There
was no significant interaction between Vm and treatment conditions F (1,4) =2.219 p>0,05,
the ANOVA also conducted tests looking at the effect between history and time although
there was a significant interaction between history based on habitual high and habitual low
conditions there was no significant effect shown
F (1,4) = .758 P>0.05.
16
0 10 20 30 600.0
1.0
2.0
3.0
4.0
5.0
6.0
Habitual High
Habitual Low
Time (m)
Bloo
d gl
ucos
e De
caffi
nate
s (m
mol
/L)
0 10 20 30 600.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0Habitual High
Habitual low
Time (m)
BLoo
d Gl
ucos
e Ca
ffina
ted
(mm
ol/L
)

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
When assessing Glucose in the treatment conditions the decaffeinated condition indicated no
statistical interaction over the five time periods χ2 (4) = 3.958 P>0.05 and in the caffeinated
condition χ2 (4) = 1.933 P>0.05. History also had no significant interaction between the five
time periods χ2 (4) = 4.385 p>0.05 and habitual low χ2 (4) = 2.187 P>0.05.
Within the two treatment conditions the change of caffeine from the decaffeinated condition
showed an 11.2% increase in Blood glucose scores. Within the two treatment conditions
habitual high consumers in the caffeinated condition showed a 12% increase compared to the
habitual Low group. When looking at the decaffeinated condition, Habitual High and a 9%
increase over the habitual low counterparts.
4. Discussion:
The primary aim of this study was to determine the effects of caffeine on cardiovascular
parameters, in habitual high and habitual low coffee/tea drinkers over a period of 60 minutes.
The secondary aim of this study was to compare the clearing time of caffeine on the studied
populations. It was hypothesised that the ingestion of caffeine would increase BP as a result
17
Mean ± SD Blood Glucose scores for all participants over five time periods in the decaffeinated condition.

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
of vasoconstriction. As a consequence of this increased BP, caffeine would also increase HR,
and blood plasma volume. Finally it was hypothesised that these effects would be more
noticeable in habitual low caffeine drinkers as a result of caffeine stress interactions and a
reduced tolerance.
Within this study HR, BP (both systolic and diastolic), blood glucose, FV1, IMT, RI and Vm
were found to be non significant when consuming the caffeinated and decaffeinated
beverages, which is in contrast to some epidemiological studies. (Robertson et al. 1989) In
these cases the sample size for the current study was likely to be insufficient to provide
statistical power, making direct comparisons difficult to conclude on. Methodological issues
within the study may also have been an impacting factor such as, the allowance for caffeine
to digest into the blood stream, to notice significant changes within blood glucose and other
hemodynamic variables. Peak volumes are assumed to occur at 60 minutes as suggested by
Daniels et al. (1988). There is, however, considerable interindividual variability in the rate of
absorption. Some studies such as Robertson et al. (1978), have suggested that waiting three
hours may be more optimal, as the caffeine induced effect of lipolyis is larger than at earlier
times after ingestion. The peak plasma concentrations of caffeine are usually obtained
between 30 -2 hours after the consumption of an oral beverage. The results of this study are
in accordance to that of Robertson et al. (1978) and state that performance may be improved
3–4 h after the ingestion of caffeine, as this time would correspond with elevated free fatty
acids (FFA) levels.
However, other inconsistent findings have been reported in the literature, this is possibly due
to the doses of the drug that have either been too low or exceedingly high (Glade et al. 2010).
The decision to use a 6mg/Kg body weight dosage was selected, on the basis of its similarity
18

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
doses of 3-6mg/Kg of body weight, previously shown to increase BP at rest or during
exercise, without provoking side effects, intolerance or decrease in exercise performances
(Sung et al. 1998). Although this has been suggested across many studies, there was no
significant change over time owing to caffeine, found within any of the variables in the
current study having used a 6mg/Kg of body weight dosage. This may not be due to a
function of dosage, but when considering that the participants were habitual consumers, it
may be due to other confounding factors such as tolerance or added additives and lifestyle
habits such as smoking, dietary habits, and medication. All of these factors in turn can play a
part in the interaction of caffeine absorption and effects. The difference in tolerance after
taking the beverage through oral and intravenous administrations of caffeine may be another
view of the situational specificity of tolerance. Previous research indicates that drug tolerance
is due to the environment, interceptive and exproceptive stimuli that participants are exposed
to (Siegel et al. 2013). That is, drug tolerance is more pronounced when normal cues are
present such as smell and taste (Siegel et al. 2013). Finally, caffeine given in coffee is self-
administered where the participant administers the caffeine/coffee to themselves. In contrast,
intravenous caffeine is provided and given by the experimenter not the participant, which was
the process within the current study. If a drug is self-administered, response cues are
concurrent with the drug’s effects. Results of various studies indicate that greater tolerance is
displayed when self administering due to normal cues than to the same dose of an
experimenter providing the beverage, (externally received) (Siegel et al, 2000). This effect of
the self-administration contingency on tolerance has been demonstrated with a variety of
drugs, including cocaine, caffeine, nicotine, and alcohol in rats. Situational specificity of
tolerance has been implicated in tolerance to a variety of effects of many drugs, including
opiates, alcohol, nicotine, immunoenhancing drugs, cholecystokinin, carisoprodol,
haloperidol, and several benzodiazepines (Siegal et al. 2000). Given that caffeine is a drug
19

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
that operates in similar fashion to the previously listed drugs, though the effects are currently
unknown in the literature they must be considered. The effects of self administration and
situational specificity must be considered.
Within the BP variable, no significant interaction between time, history and treatment was
found (P > 0.05). Within history, habitual consumption of coffee or caffeine was associated
with elevated SBP at 60 minutes post consumption of the caffeinated beverage not the
decaffeinated beverage. However, many of the epidemiological studies showed no relation,
and some even showed a small inverse relationship between self reported coffee consumption
and BP (Nurminen et al. 1999). It must be noted that habitual high consumers may need
higher dosages of caffeine to induce the same effects of caffeine witnessed in habitual low
consumers because of the resistance build up to caffeine which can occur after 3-5 days of
consumption. (O’Keefe et al. 2013). It seems that caffeine is the active component for this
effect given that placebo conditions have demonstrated no effect which is also in line with the
results of this study. It is also interesting to note that within the results of SBP within the
habitual high group, they responded more to the caffeine at 60 minutes than the habitual low
group. SBP decreased in the habitual high group to 118 mmHg compared to 127mmHg in
Habitual low consumers which was a 9mmHg decrease. This may be due to greater
absorption rates in those habitual high drinkers as it also indicated their SBP peaked at 20
minutes, 10 minutes earlier than the habitual low consumers who peaked at 30 minutes post
ingestion. (Table 2) indicates large differences between the two groups at baseline; this may
be due to a function of habitual consumption and the long term adaptations that take place.
Those who drink small amounts of caffeine have higher SBP than those who consume more.
The regular consumption of caffeine is also associated with an increase of the number of
adenosine receptors within the brain, as a result of these effects of adenosine receptor
20

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
blockage including the release of adrenaline, it has been stated that these are key mechanisms
which may explain the ergogenic effect of the drug (Bell and Mclellean, 2002), on high
versus low consumers of a caffeinated beverage and the figures in (Table 2).
In a study of 15 volunteers (including 6 habitual consumers) it was demonstrated that coffee
drinking increases BP, however habitual consumers showed no increase in BP (Daniels et al.
1998). In this study by Greer et al. (2010) there was also no effect on BP when using a
250mg dosage which is equivalent to two cups of coffee the authors concluded that caffeine
is not solely responsible for the CV effects associated with short and long term coffee
consumption, as caffeine is one compound of 1,000 components At 60 minutes post ingestion
for habitual consumers the change was not significant (0.73.4mmHg, t4 4.4, P0.012), even
though there was a significant and linear time interaction for coffee, in both conditions (Greer
et al. 2010). Corti et al. (2002), suggested that the development of tolerance during habitual
consumption may explain why drinking coffee in some epidemiological studies, did not have
a clear effect on BP with negative results. The observed results in some of the studies have
been inconsistent due to some individuals being more sensitive than others. It could also be
that inconsistencies are of a result of gender, body mass index (BMI) and smoking.
This study has suggested that HR results also showed no significant interaction (P> 0.05),
although the previously mentioned statistical limitations must be noted. It has been indicated
that men have a greater vascular resistance indicating a vasodilator effect (Sung et al. 1994),
However, it must be noted that the present study did not investigate gender effects. The
presser effect has often been accompanied by small decreases in HR (Nurimen et al. 1999). In
the present study, the caffeine condition HR showed more variability than the decaffeinated
condition. These results are in agreement with the previous findings of other studies
(Heartley, 2004; Nurmien et al. 1990).
21
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Caffeine was consumed in the form of coffee mainly due to accessibility and prevalence
within the world. In the United States of America, 90% of the population consume coffee,
with energy drinks only equating to 50% of the population (Burke, 2008) Coffee therefore,
represented the most ecologically valid modality for provision of caffeine within the study
cohort. Other administrative forms could have been used such as chewing gum, energy drinks
or in the form of a caffeine content spray. Energy drinks were not administered in the present
study due to them having other substances including taurine, ginseng and vitamin B12. To
date research has yet to investigate the effects of these substances on the CV system, which
could make CV effects more pronounced than just caffeine itself. In a separate study
conducted by. Emily Fletcher of the David Grant Air Force Medical Centre, healthy
volunteers experienced a greater increase in BP after they consumed an energy drink
compared to when they drank coffee which contained the same amount of caffeine. This
result, suggests that ingredients in energy drinks other than caffeine combine to produce
greater increase in BP. This is not to say, however, that caffeine has other unrecognisable
compounds and was found to be less effective when administered in an anhydrous form
(Graham et al.1998). A liquid form of consuming caffeine is the best delivery method as it
represents the most efficient process of absorbing caffeine with the most caffeine being
absorbed in the least amount of time (examine.com 2014) 99% of the caffeine contained
within a coffee beverage is available to be absorbed compared to 90% in capsules and 77% in
chewing gum. (Caffeine informer 2012: online) Whilst caffeine contained in gum is absorbed
quicker the volume of caffeine absorbed when compared to liquid forms is less overall.
Circadian variations when drinking coffee may also have an effect upon BP readings (Guo &
Stein, 2003). The highest levels of BP occur after 10am with a peak around noon following
this from noon until 6pm BP plateaus, and in the majority of people BP increases by up to
22

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
20/15mmHg (Pickering, 1990). As a consequence of circadian variations it is suggested that
participants may require increased dosages of caffeine when testing in the morning in order to
increase their peak BP more than those who were tested from noon onwards (Pickering,
1990). Although participants were asked to abstain from any caffeinated beverages, exercise
and alcohol for 24 hours prior to testing, it has been previously stated that those who
consume coffee habitually, may also consume other dietary products such as cream, sugar or
other foods that have a diluting effect of caffeine (Live science, 2015: online).
No significant effect was found between blood glucose at any point during the protocol.
However, when observational analysis was conducted, blood glucose seemed to peak earlier
than the caffeine condition. In the decaffeinated treatment blood glucose peaked at 20
minutes where as the caffeine condition peaked at 60 minutes. Greer et al. (2001), reported
that a physiological concentration of caffeine resulted in a 20-25% decrease in glucose uptake
in a rodent contracting perfusion. In a separate study conducted by Greer et al. (1998), that
there was no effect of treatment on blood glucose concentration, at any time during the
protocol. it is important to note, that the changes may not be entirely due to caffeine. Caffeine
ingestion usually increases the plasma concentration of adrenaline, a hormone with
widespread effects. Caffeine is formed of a Trimethylxanthine which descends into three
Dimethylxanthines ( i.e. Paraxanthyne, Theophylline and Theobromine) The concentrations
of these metabolites increase in the plasma, as the caffeine concentration declines. Thus, as a
result of the complexities presented by the chemical makeup of caffeine it is difficult to
identify which tissues are affected (Graham and Spriet, 1996).
4.1 Limitations:
23

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
The most notable limitation to the present study was that such a small sample size created a
loss of power, as a small population doesn’t reliably reflect the population mean and lacks
representation of a phenomenon occurring, which increases the likelihood of outliers and
extreme observations (Field, 2010). Although a power analysis was conducted, which stated a
sample size of 26 was needed, due to limited time and resources of an undergraduate research
project only five participants could be recruited. One of the primary aims of the study was to
investigate the influences of caffeine consumption and history. In this study these were
defined as habitual high and habitual low consumers. The sample size for the study did not
provide statistical power making direct comparisons between the habitual high and habitual
low groups difficult to conclude on due to differing sample numbers within each group
(habitual high n=3, habitual low n=2). Other methodological defects also lie within the study
including the design. This study utilised a single blind protocol where by all participants were
unaware of the condition they were undertaking at the time of testing. However, as the
experimenter was aware of the condition this may have created unintentional external error
and bias. It is noted that Randomized double blind placebo control (RDBPC) studies are
considered the “gold standard” of epidemiologic studies. (Misra, 2012). RDBPC studies
eliminate the influence of immeasurable cofounding variables that may lead to an under or
over estimation of the treatment effect and bias (Misra, 2012). By blinding the participants
and experimenter this study design type eliminates the possibility that the observed effects
are due to the use of other treatment conditions. Participants were asked to abstain from
alcohol, caffeine and exercise 24 hours prior to testing, so the effects of the treatments and
other substances would be accurate and nothing other than diet would interact with the
mechanisms by which caffeine works. Although factors such as age, gender, smoking and
habitual consumption of caffeine were monitored and accounted for, it is not always possible
to 100% control these factors as supervision was not constant between experimental sessions.
24
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Therefore, participants may have consumed caffeine in other sources which they may have
not known about such as chocolate or chewing gum. Having not fasted this increased the
likelihood that glucose results would be inaccurate, or not solely due to the effects of
caffeine. Other factors that would have affected the internal validity of the study would have
been that participants were not tested under the same resting environments. In some testing
sessions the laboratories contained other experimenters carrying out various other studies.
Furthermore, differing rooms may have influenced the variation in results as some had
brighter lighting which may have caused more excitement within the participants. Future
studies should consider more strict regimes of monitoring environmental factors than those
utilised in the current study (e.g. use of a Lux meter).
4.2 Statistical Difference tests:
Statistical analysis differences within Friedman’s and two way repeated measures ANOVA’s
compared to multiple t-tests increases type two errors each time an ANOVA was conducted.
Parametric data is said to be more powerful than non parametric data However, it may not
always be a better representation of the data (Field, 2010). Further to this, having had larger
sample numbers the data may have possibly have been parametric allowing less error to be
induced.
5. Conclusion:
Discrepancies in the reported study can partially be attributed to methodological differences
and failure to control confounding variables, diet, alcohol intake and stress. These stated
reasons have an effect on caffeine’s absorption. Due to such a small sample the power within
the study was reduced and therefore no significant interaction was found between any of the
25
The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
independent variables. It is therefore difficult to draw a representative conclusion of any
comparisons between treatment and history. Therefore, it is suggested that this study may
serve as a pilot study and be useful in the conduction of further research into these topic areas
with greater sample sizes and further control within the methods. Previous studies have not
investigated the time course of the treatment of a substantial period of time, therefore, the
effects of caffeine may need to be investigated into a period of time over 60 minutes utilising
a randomised double blind placebo controlled design.
6. References:
Bell, G. D., and Mclellan, M.T. (2002) ‘Exercise endurance 1,3 and 6h after caffeine
ingestion in caffeine users and non users.’ Journal of Applied Physiology, 93, pp. 1227-1234.
Burke, M. L., (2008) ‘Caffeine and sports performance.’ Applied Physiology Nutrition and
Metabolism, 33, pp. 1319-1334.
Caffeine informer (2012) ‘Caffeine absorption, how quickly does caffeine enter the blood
stream’. [Online] [Accessed on 27th November 2014]
Chad, K., and Quigley, B. (1989) ‘The effects of substrate utilization, manipulated by
caffeine, on post exercise O2 consumption in untrained female subjects.’ Journal of Applied
Physiology, 59, pp. 48-52.
Corti, R., Binggeli, C,. Sudano, I,. Spieker, L., Hanseler, E., Ruschitzka, F., Chaplin. F.W.,
Luscher, F. T., and Noll, G. (2002) ‘Coffee acutely increases sympathetic nerve activity and
BP independently of caffeine content role of habitual versus nonhabitual drinking’. Journal
of American Heart Association, 106, pp. 2935-2940.
26

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Daniels, W. J,. Mole, A. P., Shaffrath, D. J., and Stebbins, L.C. (1998) ‘Effects of caffeine
on BP, heart rate, and forearm blood flow during dynamic leg exercise’. Journal of Applied
Physiology, 98, pp. 154-159.
Examine.com (2014) ‘Caffeine is a stimulatory anti-sleep compound extracted from coffee
beans. Habitual caffeine use leads to tolerance which dulls several of caffeine’s effects’ .
[Online] [Accessed on 25th Novemeber 2014].
Field, A. (2005) Discovering Statistics Using SPSS (and sex and drugs and rock ‘n’ roll). 3rd
ed., London: SAGE.
Glade, J. M., (2010) ‘Caffeine- not just a stimulant’. Journal of Nutrition,26, pp. 932-938.
Graham, E. T., and Spriet, L. L., (1991) ‘Performance and metabolic responses to a high
caffeine dose during prolonged exercise.’ Journal of Applied Physiology,71 (6), pp. 2292-
2298.
Graham, E. T., Hibbert, E., and Sathasivam, P. (1998) ‘Metabolic and exercise endurance
effects of coffee and caffeine ingestion.’ Journal of Applied Physiology, 98, pp. 883-889.
Graham, T. E. (2001) ‘Caffeine and exercise metabolism endurance and performance.’
Journal of Sports Medicine, 31, pp. 785-802.
Graham, T., and Spiret, L. (1996) ‘Caffeine and exercise performance.’ Gatorade Sport
Science Institute, 9(1), pp. 1-5.
Greer, F., Mclean, C., and Graham, E. T. (1998) ‘Caffeine, performance, and metabolism
during repeated Wingate exercise tests.’ Journal of Applied Physiology,85 (4), pp. 1502-
1508.
Guo, Y. F., Stein, P. K. (2003) ‘Circadian rhythm in the cardiovascular system’
chronocardiology.’ American Heart Journal, 86, pp. 145-779.
27

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Hartley, R.T., Lovallo, R. W., and Whitsett, L. T., (2004) ‘Cardiovascular effects of caffeine
in men and women.’ American Journal of Cardiology, 93, pp. 1022-1026.
Hatano, Y., Mizumoto, K., Yoshivama, T., Yamamoto, M., and Iranami, H. (1995)
‘Endothelium dependent and inderpendent vasodilation of isolated rat aorta induced by
caffeine.’ American Journal of Physiology, 269, pp. 1679-1684.
Jackman, P.M., Wendling, D. F., and Graham, T. E. (1996) ‘Metabolic, cathecholine
responces during intense exercise.’ American Physiological Society, 96(1), pp. 1658-1663.
James, J. E. (1994) ‘Chronic effects of habitual caffeine consumption on laboratory and
ambulatory blood pressure levels.’ Journal of Cardiovascular Risk, 1, pp. 159-164.
Lane, D. J., and Williams, B.R. (1987) ‘Cardiovascular effects of caffeine and stress in
regular coffee drinkers.’ The Journal of Psychophysiology, 24(2) pp. 157-164.
Lane, J. D., and Williams, R.B. (1985) ‘Caffeine effects cardiovascular responses to stress.’
Journal of Psychophysiology, 22, pp. 648-655.
Mahmud, A. and Feely, J. (2001) ‘Acute effect of caffeine on arterial stiffness and aortic
pressure waveform.’ Journal of Hypertension, 38, pp. 227–231.
Misra, S. (2012) ‘Randomised double blind placebo controlled studies, the “Gold standard”
in intervention based studies. Journal of Sexually Transmitted Diseases, 33(2), pp. 131-134.
Nurminen, M.L., Niittynen, L. K., R. and Vapaatalo, H. (1999) ‘Coffee, caffeine and BP: a
critical review’. European Journal of Clinical Nutrition. 53(11), pp. 831-839.
O’Keefe, H. J., Bhalti, K. S., Patil, R.H., DiNicolantonio, J. J., Lucan, C.S., and Lavie, J. C.,
(2013) ‘Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular
health, and all-cause mortality.’ Journal of the American College of Cardiology, 62(12), pp.
1043-1051.
28

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
Pickering, T. G. (1990) ‘The clinical significance of diurnal blood pressure variations:
dippers and non-dippers.’ Journal of Circulation, 81, pp. 700-702.
Roberston, D., D. Wade, R. Workman., and Woosley, R.L.(1989) ‘Tolerance to the humoral
and hemodynamic effects of caffeine in man,’ Journal of Clinical Investigation, 67(4), pp.
1111–1117.
Robertson, D. J. C. Frolich, R. K. Carr, J. T., Watson, J. W., Hollifield, D. G., Shand, and J,
A. Oates. (1978) ‘Effects of caffeine on plasma rennin activity, catecholamines and blood
pressure.’ New England Journal of Medicine, 298 (4), pp. 181–186.
Siegel, S., Baptista, M. A. S., Kim, J. A., McDonald, R. V., & Weise-Kelly, L. (2000) ‘The
associative basis of tolerance. Experimental and Clinical Psychopharmacology.’ Journal of
psychopharmacology, 8, pp. 276–293.
Sung, B. H., Lovallo, W.R. , Pincombe, G.A., and Wilson, M.F., (1990) ‘Effects of caffeine
on blood pressure response during exercise in normotensive healthy young men.’ American
Journal of Cardiology, 65, pp. 909–913.
Sung, B. H., Whitsett, T. L., Lovallo, W. R., al'Absi M, Pincomb, G. A., & Wilson, M. F.
(1994). ‘Prolonged increase in blood pressure by a single oral dose of caffeine in mildly
hypertensive men.’ American Journal of Hypertension, 7(8), pp. 755 -758.
Van Soeren, M. H., Sathasivam, P., Spriet, l., and Graham., T. E (1993) ‘Caffeine
metabolism and epinephrine responses during exercise in users and nonusers.’ Journal of
applied Physiology, 75, pp. 805–812.
VanDam, R.M. (2013) ‘Coffee and type 2 diabetes: from beans to beta cells.’ Journal of
Nutrition, Metabolism and Metabolic Disease, 16, pp. 69-77.
Wanjek, C. (2015) ‘Energy drinks raise blood pressure study finds’ Live Science [online]
[Accessed on 29th March 2015].
29

The Cardiovascular Effects of Caffeine Ingestion During Rest in, Habitual High Versus Habitual Low Drinkers.
30


















