


Handouts Available at the Web Site Next Week: www ... Decompensated Heart Failure (ADHF) 9 Common...
90
Handouts Available at the Web Site Next Week: www.cardionursing.com Drawing at the end of todays program. Sneak peek of our book. Must be present to win. 1
Transcript of Handouts Available at the Web Site Next Week: www ... Decompensated Heart Failure (ADHF) 9 Common...

Handouts Available at the Web Site Next Week:
www.cardionursing.com
Drawing at the end of todays program.
Sneak peek of our book.
Must be present to win. 1

Presented By
Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN
2 2014 www.cardionursing.com

3
They may forget your
name, but they will never
forget how you made
them feel.
-Maya Angelou

Definitions
4

Definition of Heart Failure
Classification Ejection
Fraction Description
I. Heart Failure with
Reduced Ejection
Fraction (HFrEF)
≤40% Also referred to as systolic HF. Randomized clinical trials have
mainly enrolled patients with HFrEF and it is only in these
patients that efficacious therapies have been demonstrated to
date.
II. Heart Failure
with Preserved
Ejection Fraction
(HFpEF)
≥50% Also referred to as diastolic HF. Several different criteria have
been used to further define HFpEF. The diagnosis of HFpEF is
challenging because it is largely one of excluding other potential
noncardiac causes of symptoms suggestive of HF. To date,
efficacious therapies have not been identified.
a. HFpEF,
Borderline
41% - 49% These patients fall into a borderline or intermediate group. Their
characteristics, treatment patterns, and outcomes appear similar to
those of patient with HFpEF.
b. HFpEF
Improved
>40% It has been recognized that a subset of patients with HFpEF
previously had HFrEF. These patients with improvement or
recovery in EF may be clinically distinct from those with
persistently preserved or reduced EF. Further research is needed
to better characterize these patients. 5

Stages, Phenotypes and Treatment of HF
STAGE AAt high risk for HF but
without structural heart
disease or symptoms of HF
STAGE BStructural heart disease
but without signs or
symptoms of HF
THERAPY
Goals
· Control symptoms
· Improve HRQOL
· Prevent hospitalization
· Prevent mortality
Strategies
· Identification of comorbidities
Treatment
· Diuresis to relieve symptoms
of congestion
· Follow guideline driven
indications for comorbidities,
e.g., HTN, AF, CAD, DM
· Revascularization or valvular
surgery as appropriate
STAGE CStructural heart disease
with prior or current
symptoms of HF
THERAPYGoals· Control symptoms· Patient education· Prevent hospitalization· Prevent mortality
Drugs for routine use· Diuretics for fluid retention· ACEI or ARB· Beta blockers· Aldosterone antagonists
Drugs for use in selected patients· Hydralazine/isosorbide dinitrate· ACEI and ARB· Digoxin
In selected patients· CRT· ICD· Revascularization or valvular
surgery as appropriate
STAGE DRefractory HF
THERAPY
Goals
· Prevent HF symptoms
· Prevent further cardiac
remodeling
Drugs
· ACEI or ARB as
appropriate
· Beta blockers as
appropriate
In selected patients
· ICD
· Revascularization or
valvular surgery as
appropriate
e.g., Patients with:
· Known structural heart disease and
· HF signs and symptoms
HFpEF HFrEF
THERAPY
Goals
· Heart healthy lifestyle
· Prevent vascular,
coronary disease
· Prevent LV structural
abnormalities
Drugs
· ACEI or ARB in
appropriate patients for
vascular disease or DM
· Statins as appropriate
THERAPYGoals· Control symptoms· Improve HRQOL· Reduce hospital
readmissions· Establish patient’s end-
of-life goals
Options· Advanced care
measures· Heart transplant· Chronic inotropes· Temporary or permanent
MCS· Experimental surgery or
drugs· Palliative care and
hospice· ICD deactivation
Refractory symptoms of HF at rest, despite GDMT
At Risk for Heart Failure Heart Failure
e.g., Patients with:
· Marked HF symptoms at
rest
· Recurrent hospitalizations
despite GDMT
e.g., Patients with:
· Previous MI
· LV remodeling including
LVH and low EF
· Asymptomatic valvular
disease
e.g., Patients with:
· HTN
· Atherosclerotic disease
· DM
· Obesity
· Metabolic syndrome
or
Patients
· Using cardiotoxins
· With family history of
cardiomyopathy
Development of
symptoms of HFStructural heart
disease
6

7
Classification of Heart Failure New York Heart Association

8
Stages / Classification of Heart Failure

Sudden or gradual onset of the signs
and symptoms of heart failure requiring unplanned office visits, emergency room visits, or hospitalizations.
Associated with pulmonary and systemic congestion due to increased left and right heart filling pressures.
Rehospitalization rate predicted to be 50% at 6 months
1-year mortality of approximately 30% of ADHF admissions (ACCF/AHA 2013 HF Guidelines)
Acute Decompensated Heart Failure (ADHF)
9

Common Precipitating Factors of ADHF
Non adherence with Medications
Dietary sodium intake
Fluid intake
Acute MI
Arrhythmias Atrial fibrillation
Persistent hypertension
Recent addition of negative inotrope
Pulmonary embolism
Nonsteroidal anti-inflammatory drugs
Excessive alcohol or drug use
Endocrine abnormality
Concurrent infection
New anemia
10

ACS / coronary ischemia (troponins typically elevated
with ADHF)
Severe hypertension
Atrial or ventricular arrhythmias
Infections
Pulmonary emboli
Renal failure
Medical or dietary compliance
Valvular heart disease
New onset anemia
Potential Contributing
Precipitating Factors and/or Comorbidities
11

Evidence of severe ADHF, including:
Hypotension
Worsening renal function
Altered mentation
Dyspnea at rest
Typically reflected by resting tachypnea
Less commonly reflected by oxygen saturation <90%
Hemodynamically significant arrhythmia - including new onset of rapid atrial fibrillation
Acute coronary syndromes
Hospitalization Recommended
12

Worsened congestion: Even without dyspnea Signs and symptoms of pulmonary or systemic congestion Even in the absence of weight gain Major electrolyte disturbance Associated comorbid conditions Pneumonia Pulmonary embolus Diabetic ketoacidosis Symptoms suggestive of transient ischemic accident or
stroke Repeated ICD firings Previously undiagnosed HF with signs and symptoms of systemic or pulmonary congestion
Hospitalization Should be Considered
13
Improve symptoms, especially congestion and low-output symptoms
Optimize volume status
Identify etiology
Identify and address precipitating factors
Optimize chronic oral therapy
Minimize side effects
Identify patients who might benefit from revascularization
Identify patients who might benefit from device therapy
Identify risk of thromboembolism and need for anticoagulant therapy
Educate patients concerning medications and self management of HF
Consider and, where possible, initiate a disease management program
Treatment Goals
14

Based on signs and symptoms
B-type natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-proBNP)
Good to assess in patients with dyspnea being evaluated for HF
Should not be used as the sole tool to diagnose HF
Must be used in concert with signs and symptoms
Special consideration with renal insufficiency and obesity.
Diagnosis
15

Patient 1: Volume overload (Backwards Failure)
Patient 2: Profound depression of cardiac output –hypoperfusion (Forwards Failure)
Patient 3: Signs and symptoms of both fluid overload and hypoperfusion (cardiogenic shock)
3 Clinical Presentations
16

Determine
Volume Status
Perfusion Status
Role of / or presence of precipitating factors and/or comorbidities
Ejection fraction HFpEF
HFrEF
Evaluation Guides Treatment Decisions
17

Hypoperfusion vs. Volume Overload
18
Intravascular Volume Overload Elevated jugular
venous pressure
Hepatojugular reflex
Orthopnea
Dyspnea
Crackles
Weight gain
Peripheral edema
Hypoperfusion Narrow pulse pressure
Resting tachycardia
Cool Skin
Altered mentation
Decreased urine output
Increased BUN/Creatinine
Cheyne Stokes Respirations

0
1
4
3
2
5
20 18 16 14 12 10 8 6 4 2 32 30 28 26 24 22 34 36
Preload: PWP, lung sounds (dry or wet)
Fo
rward
s F
low
:
CI,
Sk
in t
em
p (
warm
or
cold
) Normal Hemodynamics (I) No pulmonary congestion:
• PWP < 18; Dry lungs No hypoperfusion:
• CI > 2.2; Warm skin
Backwards Failure (II) Pulmonary congestion
• PWP > 18; Wet lungs No hypoperfusion
• CI > 2.2; Warm skin
Forwards Failure (III) No pulmonary congestion
• PWP < 18; Dry lungs Hypoperfusion
• CI < 2.2; Cold skin
The Shock Box (IV) Pulmonary congestion
• PWP > 18; Wet lungs Hypoperfusion
• CI < 2.2; Cold skin
19
Hemodynamic and Clinical Subsets

Treatment for Acute Decompensated Heart Failure
Congestion with Adequate Perfusion
Subset II
Reduce Preload
Hypoperfusion with No Congestion
Subset III Increase contractility Assure adequate preload
Hypoperfusion with Congestion
Subset IV
Reduce Afterload 21

0
1
4
3
2
5
20 18 16 14 12 10 8 6 4 2 32 30 28 26 24 22 34 36
Preload
Fo
rwar
d F
low
: C
ard
iac
Ind
ex
S
kin
te
mp
(w
arm
or
cold
) Changing Preload: Moves patient along the current curve
22
Warm and Dry
Cold and Wet

0
1
4
3
2
5
20 18 16 14 12 10 8 6 4 2 32 30 28 26 24 22 34 36
Changing Contractility: moves patient to a higher curve
23
Preload: PWP, lung sounds (dry or wet)
Fo
rward
s F
low
:
CI,
Sk
in t
em
p (
warm
or
cold
)

0
1
4
3
2
5
20 18 16 14 12 10 8 6 4 2 32 30 28 26 24 22 34 36
Changing Afterload:: moves patient up and to the left
(improves forwards flow and reduces preload)
24
Fo
rward
s F
low
:
CI,
Sk
in t
em
p (
warm
or
cold
)
Preload: PWP, lung sounds (dry or wet)

25
Acute Decompensated Heart Failure
Reduce Afterload Arterial vasodilators High dose Nitroglycerin Nitroprusside Neseritide
Intra aortic balloon pump
Increase Contractility Positive Inotropes
Dobutamine
Milronone
Dopamine
Reduce Preload Diuretics Venous Vasodilators Low dose NTG Neseritide
Ultrafiltration

26
Pharmacological Options for Decreasing
Preload
Stop or decrease fluid
Diuretics ▪ A loop diuretic such as furosemide eliminates
circulating volume
Venous
Vasodilators
▪ Intravenous nitroglycerin, neseritide, or
morphine sulfate
(Venous vasodilatation pools blood away from
the heart and decreases preload)
ACE Inhibitors or
Angiotensin II
Receptor Blockers
(ARBs)
▪ Interrupt renin- Angiotensin- aldosterone system. (RAAS).
Aldosterone secretion is decreased and there is less sodium and
water retention.
▪ ACE inhibitors end in “pril” / ARBs end in “sartan”
Aldosterone
antagonists
▪ Spironolactone or epleranone
▪ Directly block aldosterone and there is decreased sodium and water
retention.
IV not PO Early intervention - ED
Dose high enough to relieve signs and symptoms of congestion Should equal or exceed chronic oral dose
Caution for signs of over diuresis Hypotension: check orthostatics
Worsening renal failure
Monitor e-lytes (potassium, magnesium, sodium) Arrhythmias
Muscle cramps
Monitor for gout
Frequent reassessment
Reduce Preload Loop Diuretics
27

Diuretics and Renal Function
Role of venous congestion in worsening renal function
Role of volume depletion / hypotension and worsening renal function
28

Moderate to severe renal dysfunction with fluid
overload
Continue to treat with diuretics
In severe fluid overload renal dysfunction my improve with continued treatment
May need to hold ACE I secondary to AKI
Venous congestion plays a role in worsening renal function (not just hypoperfusion)
Cardiorenal Syndrome
29

30
Loop Diuretics
Bumetanide (Bumex) Equivalents Furosemide 40 mg Torsemide 20 mg Bumetanide 1 mg
Dosing
Adequate to relieve symptoms Start equal or greater than home maintenance dose
Furosemide (Lasix)
Torsemide (Demadex)

More on Loop Diuretics
31
DOSE Trial NEJM: Felker et al., 2011
No significant difference in symptoms or renal function between continuous drip versus intermittent dosing
Non significant trend toward improvement in symptoms with high dose (IV at 2.5 x PO dose)
versus low dose; (IV at same as PO dose) no change in renal function

Bumetanide Furosemide Torsemide
Lack of randomized control data with comparison to furosemide. Better pharmacokinetic profile (oral bioavailability) than furosemide but turosemide has evidence of more efficacy and more safety. (Wargo &Banta, 2009)
BID Dosing when GFR is low
2 randomized trials comparing Torsemide and Furosemide N=471 Torsemide associated with reduction in HF and CV readmission in systolic HF with a trend towards reduction of all cause mortality. (DiNicolantonio, 2012)
Differences in Loop Diuretics
32

Preload Reduction Venous Vasodilators
Afterload Reduction Arterial Vasodilators
Three Primary Drugs NTG
IV Primary Venous Vasodilator
Neseritide
Mixed
Nitroprusside
Predominantly Arterial Vasodilator
Vasodilator Therapy
33
Nitroglycerin
Mixed venous and arterial vasodilator Dosage < 1mcg/kg/min = venous vasodilator Dosage > 1mcg/kg/min = arterial and venous
vasodilator Sublingual tablets provide high enough dosage to
dilate arteries and veins
Caution with severe Aortic Stenosis Decreases activity of Heparin
34

Nitroglycerin
35
Uses: Acute MI, unstable angina, CHF
Side Effects:
H/A, Hypotension, flushing
Nursing Considerations: Contraindicated with
Sildenefil like drugs Caution (all venous
vasodilators) with: Hypertrophic
cardiomyopathy, aortic stenosis, right ventricular MI
Treat H/A with pain meds
and decrease dose
Onset IV: 1-2 minutes Duration: 3-5 minutes

Nesiritide (Natrecor)
Recombinant form of human B type natriuretic peptide (BNP)
BNP is a naturally occurring cardiac neurohormone secreted by the heart in the body’s response to heart failure
BNP allows the heart to participate in the regulation of vascular tone and extracellular volume status
The BNP system and the renin-angiotensin system counteract each other in heart failure
BNP levels are elevated in heart failure
36

Nesiritide (Natrecor)
Balanced arterial and venous vasodilatation Causes rapid
reduction in right and left sided ventricular filling pressures (preload reduction)
Reduces afterload
Indicated for acutely decompensated heart failure patients who have dyspnea at rest
37

Nesiritide (Natrecor)
Patient must have systolic BP > 90 mmHg
PAOP should be estimated to be > 20 mmHg
Given by IV bolus and maintenance infusion (bolus to be taken from reconstituted IV bag and not from vial)
Infusion is usually 24-48 hours
38
Monitor BP closely during administration.

Nesiritide: Where do we stand?
39
Balanced venous and arterial vasodilator
Sackner-Bernstein JD, Kowalski M, Fox M, Aaronson K: Short-term risk of death after treatment with nesiritide for decompensated heart failure: a pooled analysis of randomized controlled trials. JAMA 2005, 293:1900-1905.
In the 3 trials, 485 patients were randomized to nesiritide and 377 to control therapy. Death within 30 days tended to occur more often among patients randomized to nesiritide therapy (35 [7.2%] of 485 vs 15 [4.0%] of 377 patients. No statistically significant difference.

ASCEND HF Trial
40
Effect of Nesiritide in Patients with Acute Decompensated Heart Failure
O'Connor et al.
July 7 2011
7,141 patients
Randomized
Nesiritide was not associated with an increase or a decrease in the rate of death and re-hospitalization.
It was not associated with a worsening of renal function, but it was associated with an increase in rates of hypotension.
Neseritide cannot be recommended for routine use.
Nitroprusside
Mixed venous and arterial dilator (primarily arterial)
Decreases BP, SVR, PVR, PAOP, RAP
Uses: Hypertensive crisis
CHF
Acute Mitral Regurgitation
Other Indications for Afterload Reduction
Side Effects: Hypotension Thiocyanate toxicity:
tinnitus, blurred vision, delirium, seizures, muscle twitching, absent reflexes, dilated pupils [several days – high doses]
Nursing Considerations: Onset: 1-2 minutes Duration: 1-10 minutes Monitor BP carefully-
arterial line encouraged
41

Persistent failure with aggressive diuresis and standard oral therapies NTG
Neseritide
Nitroprusside Especially helpful with severe hypertension or severe
MR
For rapid symptom relief in acute pulmonary edema with hypertension NTG / Nitroprusside
Do not give with hypotension
Reduce Preload Venous Vasodilators
42

If No Improvement With Preload Reduction
Na and fluid restrict Increase dose of loop
diuretic Continuous infusion of
loop diuretic Add 2nd diuretic PO Maximize loop diuretic Metalazone Spironolactone
OR IV chlorothiazide
Consider ultrafiltration
Diuretic Resistance
Reasons
High sodium levels
NSAIDs
Severe renal impairment
Renal hypoperfusion
43
Ultrafiltration
UNLOAD Trial Veno-venus ultrafiltration
(UF) vs standard IV diuretic therapy for hypervolemic HF
200 patients randomized UF with statistical
significance for: greater weight loss (48 hours), greater fluid loss (48 hours), less 90-day resource utilization for HF.
No statistically significant difference in dyspnea scores or creatinine levels (safety endpoint)
CARESS-HF Trial Treatment of ADHF,
worsening renal function, persistent congestion with stepped pharmacologic approach vs ultrafiltration
188 patients randomized
UF: inferior to pharmacologic therapy and associated with adverse events.
44

Goal: Relief of symptoms and end organ perfusion
Use in:
Low output states
Symptomatic hypotension or marginal blood pressure Despite good filling pressures
No magic blood pressure – look for symptoms
Unresponsive / intolerant of IV vasodilators
Diminished or worsening renal function
Use vasodilators first as able
Monitor closely for tachyarrhythmias and hypotension
Not recommended if normotensive (ACC)
Increase Contractility Inotropes
45

46
Dobutamine
What receptors are stimulated:
Primarily β1
Some alpha1 receptor stimulation
Some β2 stimulation
Modest β2 (more β2 than alpha1)
What are the resultant actions:
Increase contractility (+ inotrope) (β1)
Increase AV node conduction
Modest vasodilation
When and why do we use: Used as an inotrope (resultant preload reduction) with modest afterload reduction
(ACC / AHA Guidelines for Heart Failure*)
What are special nursing considerations:
Onset 1 to 2 minutes; Peak 10 minutes
Half-life 2 minutes
Note: Blood pressure response is variable; β2 causes vasodilatation; β1 increases cardiac output and may increase BP
Synthetic Compound

Phosphodiesterase Inhibitors: Non Sympathomimetic Inotropes
47
Used as an
Inotrope
BUT…..
Also has……
Preload
Reduction
Afterload
Reduction

Milrinone (Primacor)
Creates + inotropic effect by increasing availability of calcium Inhibits the degradation
of cyclic AMP which is indirectly responsible for increasing the influx of calcium through the calcium channel
Smooth muscle relaxant (venous and arterial vasodilator)
Indications: Refractory heart failure
(in combination with dobutamine)
Left ventricular failure in MI
Patients waiting transplant
Side Effects: Ventricular arrhythmias,
thrombocytopenia (new generation less)
OPTIME Trial
48
OPTIME Trial Milrinone approved by FDA based on hemodynamic data Future trials need to include symptom relief and post
discharge outcome data OPTIME Prospective trial, randomized, placebo controlled 951 patients Patients had indication for but not all required inotrope for end
organ perfusion. Results: No difference in LOS, No difference in subjective
improvement Treatment failures more common in milrinone group due to
hypotension, more atrial fibrillation in milrinone Not powered for mortality differences
Conclusion: Hemodynamic improvement does not translate into clinical improvement
49

Dopamine
What receptors are stimulated:
Dopaminergic at low doses (0.5-2.0 mcg/kg/min)
β1 also at moderate doses ( 2.0-10.0 mcg/kg/min)
Pure alpha stimulation at high doses > 10mcg/kg/min
What are the resultant actions:
Increase GFR at low doses
Increase contractility at moderate doses (greater effects on contractility than heart rate)
Vasoconstriction (alpha) at high doses
When and why do we use:
Refractory hypotension / shock
* Not indicated for routine treatment or prevention of acute renal failure
What are special nursing considerations:
Onset 1-2 minutes; Peak 10 minutes
Maximal effects @20/mcg/kg/min
Large IV line or central line; Regitine (alpha blocker) for infiltrate
50
Mimics endogenous dopamine;
metabolic precursor
of norepinephrine and epinephrine

Comparison of Dopamine to Norepinephrine in Shock
51
Backer et al.
Multi Center Randomized Controlled Trial
New England Journal of Medicine
March 4th 2010
There were no significant differences between the groups in the rate of death at 28 days or in the rates of death in the ICU, in the hospital, at 6 months, or at 12 months
More patients with arrhythmia in the dopamine group
Rate of death was higher in predefined subgroup analysis for patients with cardiogenic shock treated with dopamine.

Acute Decompensated Heart Failure
52
Reduce Preload Diuretics Venous vasodilators Low dose Nitroglycerin Neseritide
Ultrafiltration
Reduce Afterload Arterial vasodilators High dose Nitroglycerin Nitroprusside Neseritide
Intra aortic balloon pump
Increase Contractility Positive Inotropes Dobutamine
Milronone
Dopamine

53
Serelaxin RELAX –AHF Trail
Presented AHA November 2012
Recombinant human relaxin-2, vasoactive peptide hormone
Double blinded placebo controlled, randomized trial
Standard care plus 48 hours of serelaxin or placebo
1161 patients
Positive outcomes:
Dyspnea relief
Improvement in signs and symptoms of HF
Reduction in LOS
Decreased all cause and CV 180 day mortality (37% reduction in mortality)
No impact on readmissions
Europe Regulators - Denied approval January 2014
Breakthrough therapy designation by FDA – June 21 2013
Pending FDA approval Feb 13, 2014.

Additional Care Issues
54

Routine use not recommended
When to consider: Refractory to initial therapy
Volume status and cardiac filling pressures are unclear
Pulmonary and systemic pressures unclear
Clinically significant hypotension (SBP < 80 mm Hg)
Worsening renal function
Invasive Monitoring
55

Foley Catheter
Not recommended routinely in heart failure
If need to closely monitor hourly urine output
Possible outlet obstruction
High risk patients include those with BPH and or right sided volume overload
Foley Catheter
56

Dietary Sodium Restriction Water follows sodium
If hyponatremic Serum sodium < 130 mEq/L
2 liters per day
Serum Sodium < 125 mEq/L
Stricter fluid restriction may be considered
If persistent fluid overload Assure sodium restriction in conjunction with fluid
restriction
Fluid Restriction
57

Oxygen therapy is recommended if the patient exhibits hypoxemia
If not hypoxemic no need for oxygen therapy
Use of non-invasive positive pressure ventilation may be considered for severely dyspneic patients with clinical evidence of pulmonary edema.
58

Continue other evidence based practice medications
Daily monitoring of volume status via
Daily weights
Fluid balance
JVP
Orthopnea
Orthostatic pressures
Activity tolerance
Perceived dyspnea
Other considerations
59

Bridge to transplant (BBT) for those who are
transplant eligible
Destination therapy (DT) for those who are not transplant eligible.
Bridge to Decision (BTD)
Careful consideration for all therapies Some patients may be too ill with multisystem issues
to benefit from MCS
Some decisions are best made in the hands of the most experienced centers
60

Profile 1: Cardiogenic Shock Profound hypotension despite rapidly escalating inotropic
support; acidosis; “crash and burn”
Profile 2: Progressive decline Declining function despite IV inotropes, possible worsening
renal function; “sliding on inotropes”
Profile 3: Stable but inotrope-dependent Continuous IV inotropes +/- IABP or other mechanical
support, unable to be weaned
61
Profile of Severe Heart Failure
Margarita Camacho MD, FACS Surgical Director - Cardiac Transplant and Mechanical Assist Device Program Barnabas Health Heart Centers at Newark Beth Israel Medical Center, Newark, NJ

Profile 4: Resting Symptoms Daily congestion at rest or during ADL (activities of
daily living)
Profile 5: Exertion intolerant Comfortable at rest or with ADL, but unable to engage
in any other activity, living predominantly within house
Profile 6: Exertion limited Comfortable at rest and with ADL.
Profile 7: Advanced NYHA III Living comfortably with meaningful activity limited to
mild physical exertion
62
Profile of Severe Heart Failure

IABP
ECMO
Impella
CentriMag
Thoratec pVAD
Abiomed AB 5000
Abiomed BVS 5000
64
Temporary Assist Devices in Acute Shock
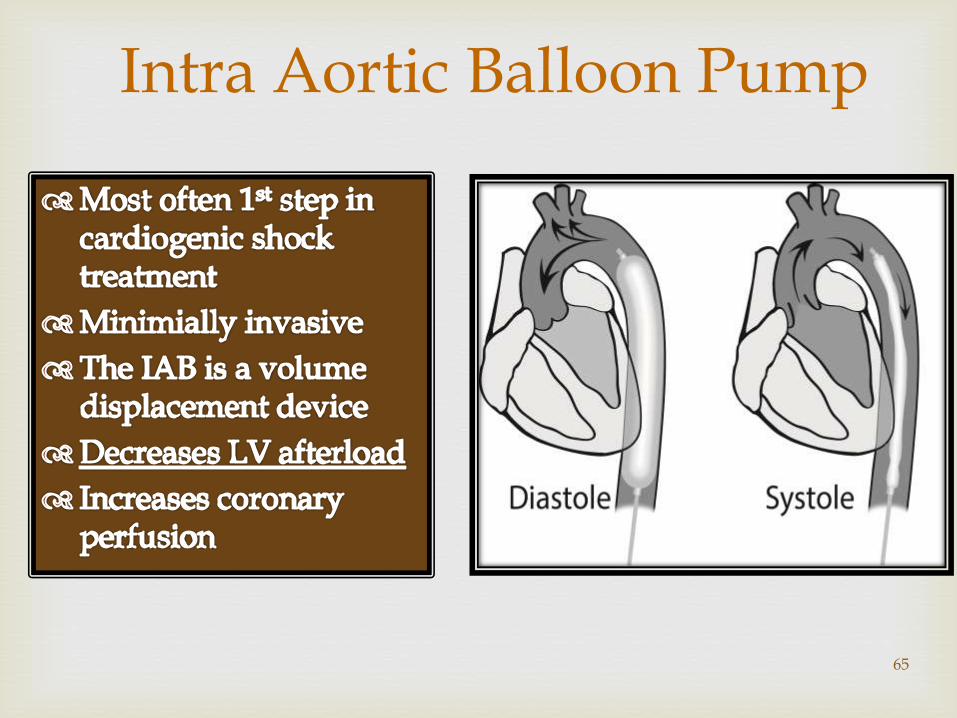
Intra Aortic Balloon Pump
65

66
Impella
Pulls blood from the left ventricle and expels blood into the ascending aorta.
Inserted via femoral artery, into the ascending aorta, across the valve and into the left ventricle.
Produces CO of 2.5 – 5.0 L/Min (2 different devices)

Impella
Mechanical Cirulatory Support Device
“Percutaneous VAD”
Minimally invasive
Unloads ventricle reducing myocardial workload
Produces 2.5 liters of cardiac output
Recommended for up to 7 days
Bridge to Recovery
67

ECMO
Extracorporeal Membrane Oxygenation
Used to treat medically refractory cardiogenic shock with poor oxygenation
Provides biventricular support
Not good for long term durability
Used in a short term situation
Requires perfusion support
Bridge to Recovery
68

69

Cardiac arrest with ongoing CPR
Cardiogenic shock, IABP-dependent on inotropes and pressors
Intra-operative failure to wean from cardiopulmonary bypass
Bridge to a decision: indeterminate neurologic status or other significant co-morbidity (i.e., possible incurable malignancy) with critical clinical deterioration
70
Who Gets a Device Acutely

CentriMag
AB5000
PVAD or IVAD
Alternate: Impella 5.0 or Tandem Heart
71
Cardiac Arrest with Ongoing CPR

CentriMag
Impella 5.0
Tandem Heart
PVAD or IVAD
72
Cardiogenic Shock, IABP Dependent on Inotropes and Pressors

CentriMAG
Tandem Heart or Impella 5.0
PVAD OR IVAD (if suspect patient will need long-term support)
AB5000 (concerns about coagulopathy/increased hemolysis after long bypass runs
73
Intra-operative failure to wean from CP Bypass

Bridge to a decision: indeterminate neurologic status
or other significant co-morbidity (i.e., possible incurable malignancy) with critical clinical deterioration
CentriMag
AB5000
Impella 5.0
Tandem Heart
74
Bridge to Decision

Thoratec pVAD
Abiomed AB 5000
Abiomed BVS 5000
Heart Mate XVE
Heart Mate II
HeartWare HVAD
Cardiowest Total Artificial Heart
75
BiV Bridge to Transplant

Long Term Therapy
BTT
Thoratec pVAD
Abiomed AB 5000
Abiomed BVS 5000
Heart Mate XVE
Heart Mate II
HeartWare HVAD
DT
Heart Mate XVE
Heart Mate II
HeartWare HVAD
76
Criteria for Discharge
Exacerbating factors addressed
Near optimal volume status achieved
Transition from intravenous to oral diuretic successfully completed
Patient and family education completed, including clear discharge instruction
LVEF documented
Smoking cessation counseling initiated
Near optimal pharmacologic therapy achieved, including ACE inhibitor and beta-blocker (for patients with reduced LVEF), or intolerance documented
Follow-up clinic visit scheduled, usually for 7 to 10 d 77

Criteria for Discharge
Advanced HF Patient or recurrent admission Oral medication regimen stable for 24 h
No intravenous vasodilator or inotropic agent for 24 h
Ambulation before discharge to assess functional capacity after therapy
Plans for post discharge management (scale present in home, visiting nurse or telephone follow up generally no longer than 3 d after discharge)
Referral for disease management, if available
78

Advanced HF
Decision Making
79

Currently 2.4% of adult population affected with HF
Over 11% of the expanding population is > 80 years
80
Things to Think About

Heart Failure Survival Score All cause mortalilty
Seattle Heart Failure Model All cause mortality, urgent transplantation or LVAD implant depts.washington.edu.shfm
EVEREST Risk Model Combined endpoint of mortality or persistently poor quality of life
over the 6 months after discharge EFFECT 30-day and 1-year mortality
ADHERE In-hospital mortality
ESCAPE Discharge Score 6 month mortality
81
Prognostic Models

>2 Prompt Referral for Advanced Rx
Hospitalization for HF on oral HF therapy
Inability to take ACEI/ARB/BB
BUN> 45, Creat>2.5, CrCl< 45 cc/min
BNP >4 x’s upper limit of normal
Na+ < 136
Malnutrition/Cachexia
VO2 <55% predicted
LVEDD >7.0 cm
82
Risk Factors for Mortality > 2 Referral for Advanced Treatment

83
Moderate to severe symptoms of dyspnea and/or fatigue at rest or with minimal exertion (NYHA functional class III or IV)
Episodes of fluid retention and/or reduced cardiac output
Objective evidence of severe cardiac dysfunction demonstrated by at least 1 of the following: Left ventricular ejection fraction <30%
Pseudonormal or restrictive mitral inflow pattern by Doppler
High left and /or right ventricular filling pressures, or
Elevated B-type natriuretic peptide
Severe impairment of functional capacity as demonstrated by either inability to exercise, 6-min walk distance 300 m, or peak oxygen uptake <12 to 14 mL g-1 min-1
History of at least 1 hospitalization in the past 6 months
Characteristics should be present despite optimal medical therapy
European Society of Cardiology Criteria for Advanced Chronic Heart Failure

84

85

Palliative Care versus Hospice
When should they be involved
Making an assessment
Having the discussion
86
End of Life Decision

+20% to -
68%
P=0.1566
-43% to -91%
P<0.0001
-70% to -96%
P<0.0001
Fonarow GC,Yancy CW. J Am Heart Assoc 2012;1:16-26.
87

Number of Therapies (vs 0 or 1 therapy)
2 therapies
3 therapies
4 therapies
5, 6, or 7 therapies
Odds Ratio (95% confidence interval)
0.63 (0.47-0.85) (p=0.0026)
0.38 (0.29-0.51) (p<0.0001)
0.30 (0.23-0.41) (p<0.0001)
0.31 (0.23-0.42) (p<0.0001)
0 0.5 1 1.5 2
Fonarow GC, … Yancy, C. J Am Heart Assoc 2012;1:16-26. 88

89
We must not, in trying to think about how we can make a big difference, ignore the small daily differences we can make which, overtime, add up to big differences that we often cannot foresee.
-Marian Wright Edelman
A Final Thought:

90
BE THE BEST THAT YOU CAN BE
EVERY DAY. YOUR PATIENTS ARE
COUNTING ON IT!


















