Functional Training may Lower New Injury Risk … · through the Functional Movement Screen (FMS)...
8
Central Annals of Sports Medicine and Research Cite this article: Gali JC, Separovic Faria FA, Gali Filho JC, da Silva PAC (2017) Functional Training may Lower New Injury Risk Assessment after Anterior Cruciate Ligament Reconstruction. Ann Sports Med Res 4(3): 1110. *Corresponding author Julio Cesar Gali, Department of Orthopaedic Surgery, Catholic University of São Paulo, Rua Joubert Wey, 290. Sorocaba - SP, Brazil, Tel: 55-015-3233-4171; Fax: 55-015- 3233-4171; Email: Submitted: 10 April 2017 Accepted: 17 May 2017 Published: 19 May 2017 ISSN: 2379-0571 Copyright © 2017 Gali et al. OPEN ACCESS Keywords • Knee injuries; Ligaments; Rehabilitation; Neuromuscular training Abstract Background: Rehabilitation program is usually incorporated to anterior cruciate ligament reconstruction (ACLR) in order to recover joint mobility, muscular strength, proprioception and to return to sports. However neuromuscular deficits commonly persist after surgical reconstruction and standard rehabilitation. Hypothesis/Purpose: The goal of our study was to evaluate if functional training may lower the assesment of a new injury risk to patients who had ACLR through the Functional Movement Screen (FMS) Scoring System. The hypothesis tested was that our functional training algorithm might diminish the chance of a new injury risk. Study design: Prospective cohort study. Methods: Our training protocol consisted of 6 phases, each of 6 weeks duration. It began two months after ligament reconstruction. The study group was compounded of 10 individuals who had completed our proposed protocol after ACLR. The control group consisted of 10 people who were allowed to return to sports activities after completing a regular ACLR rehabilitation protocol. The FMS was used to compare the study and control group performance. Patients with a score of 14 or less on the FMS were considered more likely to suffer an injury than those with a higher score. Results: The average FMS score of the study group was 16.6 compared to the control group at 12.3. Functional training for ACLR rehabilitation added a statistically significant benefit ( p < 0,0002) to diminish the risk of new injury evaluation, compared to regular ACLR rehabilitation protocol. Conclusion: Functional training may be included in regular ACLR rehabilitation with regard to possibly diminish the risk of a new injury, before returning to sports. Level of Evidence: Level II. Research Article Functional Training may Lower New Injury Risk Assessment after Anterior Cruciate Ligament Reconstruction Julio Cesar Gali 1,2 *, Felipe Alexandre Separovic Faria 2 , Julio Cesar Gali Filho 2 , and Phelipe Augusto Cintra da Silva 2 1 Department of Orthopaedic Surgery, Catholic University of São Paulo, Brazil 2 Núcleo de Ortopedia e Traumatologia do Esporte. R. Caracas, Brazil ABBREVIATIONS ACL: Anterior Cruciate Ligament; ACLR: Anterior Cruciate Ligament Reconstruction; FMS: Functional Movement Screen INTRODUCTION In the United States of America approximately 90% of patients who underwent an anterior cruciate ligament (ACL) injury had their ligament reconstructed [1]. After surgery, specific rehabilitation programs are used in order to re-establish joint motion, improve muscular strength and conditioning, and provide a safe return to sports participation. However, standardized anterior cruciate ligament reconstruction (ACLR) rehabilitation is not a guarantee for resumption of the previous level of activity and continued participation in the desired sport [2]. After an ACL lesion, proprioception and neuromuscular control of the knee are impaired and this deficiency may persist subsequentially to surgery reconstruction and rehabilitation [3]. On the other hand, improper neuromuscular control may be a risk for the first ACL injury [4,5] and also for recurrent instability [6]. Neuromuscular training program has been used to prevent ACL injuries in female athletes [7-9] and also to avoid lesions in adolescents and adults [10]. Risberg et al., suggested that neuromuscular training should be part of the rehabilitation program following ACLR [11] and Wiggins et al., in a systematic review and meta-analysis, proposed that neuromuscular training may help athletes younger than 25 years return more safely to sports and reduce second injury risk [12]. Closed kinetic chain assessment has been used to evaluate patients’ strength and capacity to advance to a more complex functional level [13]. Functional tests, such as the single-legged
Transcript of Functional Training may Lower New Injury Risk … · through the Functional Movement Screen (FMS)...

Central Annals of Sports Medicine and Research
Cite this article: Gali JC, Separovic Faria FA, Gali Filho JC, da Silva PAC (2017) Functional Training may Lower New Injury Risk Assessment after Anterior Cruciate Ligament Reconstruction. Ann Sports Med Res 4(3): 1110.
*Corresponding authorJulio Cesar Gali, Department of Orthopaedic Surgery, Catholic University of São Paulo, Rua Joubert Wey, 290. Sorocaba - SP, Brazil, Tel: 55-015-3233-4171; Fax: 55-015-3233-4171; Email:
Submitted: 10 April 2017
Accepted: 17 May 2017
Published: 19 May 2017
ISSN: 2379-0571
Copyright© 2017 Gali et al.
OPEN ACCESS
Keywords•Knee injuries; Ligaments; Rehabilitation;
Neuromuscular training
Abstract
Background: Rehabilitation program is usually incorporated to anterior cruciate ligament reconstruction (ACLR) in order to recover joint mobility, muscular strength, proprioception and to return to sports. However neuromuscular deficits commonly persist after surgical reconstruction and standard rehabilitation.
Hypothesis/Purpose: The goal of our study was to evaluate if functional training may lower the assesment of a new injury risk to patients who had ACLR through the Functional Movement Screen (FMS) Scoring System. The hypothesis tested was that our functional training algorithm might diminish the chance of a new injury risk.
Study design: Prospective cohort study.
Methods: Our training protocol consisted of 6 phases, each of 6 weeks duration. It began two months after ligament reconstruction. The study group was compounded of 10 individuals who had completed our proposed protocol after ACLR. The control group consisted of 10 people who were allowed to return to sports activities after completing a regular ACLR rehabilitation protocol. The FMS was used to compare the study and control group performance. Patients with a score of 14 or less on the FMS were considered more likely to suffer an injury than those with a higher score.
Results: The average FMS score of the study group was 16.6 compared to the control group at 12.3. Functional training for ACLR rehabilitation added a statistically significant benefit ( p < 0,0002) to diminish the risk of new injury evaluation, compared to regular ACLR rehabilitation protocol.
Conclusion: Functional training may be included in regular ACLR rehabilitation with regard to possibly diminish the risk of a new injury, before returning to sports.
Level of Evidence: Level II.
Research Article
Functional Training may Lower New Injury Risk Assessment after Anterior Cruciate Ligament ReconstructionJulio Cesar Gali1,2*, Felipe Alexandre Separovic Faria2, Julio Cesar Gali Filho2, and Phelipe Augusto Cintra da Silva2
1Department of Orthopaedic Surgery, Catholic University of São Paulo, Brazil2Núcleo de Ortopedia e Traumatologia do Esporte. R. Caracas, Brazil
ABBREVIATIONSACL: Anterior Cruciate Ligament; ACLR: Anterior Cruciate
Ligament Reconstruction; FMS: Functional Movement Screen
INTRODUCTIONIn the United States of America approximately 90% of
patients who underwent an anterior cruciate ligament (ACL) injury had their ligament reconstructed [1]. After surgery, specific rehabilitation programs are used in order to re-establish joint motion, improve muscular strength and conditioning, and provide a safe return to sports participation. However, standardized anterior cruciate ligament reconstruction (ACLR) rehabilitation is not a guarantee for resumption of the previous level of activity and continued participation in the desired sport [2].
After an ACL lesion, proprioception and neuromuscular
control of the knee are impaired and this deficiency may persist subsequentially to surgery reconstruction and rehabilitation [3]. On the other hand, improper neuromuscular control may be a risk for the first ACL injury [4,5] and also for recurrent instability [6].
Neuromuscular training program has been used to prevent ACL injuries in female athletes [7-9] and also to avoid lesions in adolescents and adults [10]. Risberg et al., suggested that neuromuscular training should be part of the rehabilitation program following ACLR [11] and Wiggins et al., in a systematic review and meta-analysis, proposed that neuromuscular training may help athletes younger than 25 years return more safely to sports and reduce second injury risk [12].
Closed kinetic chain assessment has been used to evaluate patients’ strength and capacity to advance to a more complex functional level [13]. Functional tests, such as the single-legged

Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 2/8
hop and the vertical jump, are generally used to determine knee function following knee ligament reconstruction [14,15]. Nevertheless, there is lack of one accepted and objective evaluation method to determine how an athlete will develop in the final phase of rehabilitation and his safe return to sports [16].
Recently, a score ≤ 14 measured by the Functional Movement Screen (FMS) was considered a detectable risk factor for injury in professional football players [17]. Using the FMS score, Boyle et al., found that adolescents were at an increased risk for lower extremity injury at 9 months after ACLR [18].
However, there is no sound manner to appraise neuromuscular control in individuals whose ACL has been reconstructed. The goal of our study was to evaluate if our functional training algorithm may diminish a new injury risk evaluation to patients who had ACLR, using the FMS Scoring System.
METHODS Informed consent was obtained from all patients participating
in the study and it was approved by the Ethical Committee of our Institution. All of the patients had primary anatomic single-bundle hamstring tendon grafts ACLR for chronic lesions and none of them had revision nor combined ligament reconstruction. None of the patients were professional athletes but they had a minimum of 50 hours of sport activities per year.
Full weight-bearing with crutches and complete range of motion were allowed since the first post-operative day. No brace was used. Crutches were removed after 10 days if no limp was present. Then an accelerated rehabilitation program began and was sustained for two months [19].
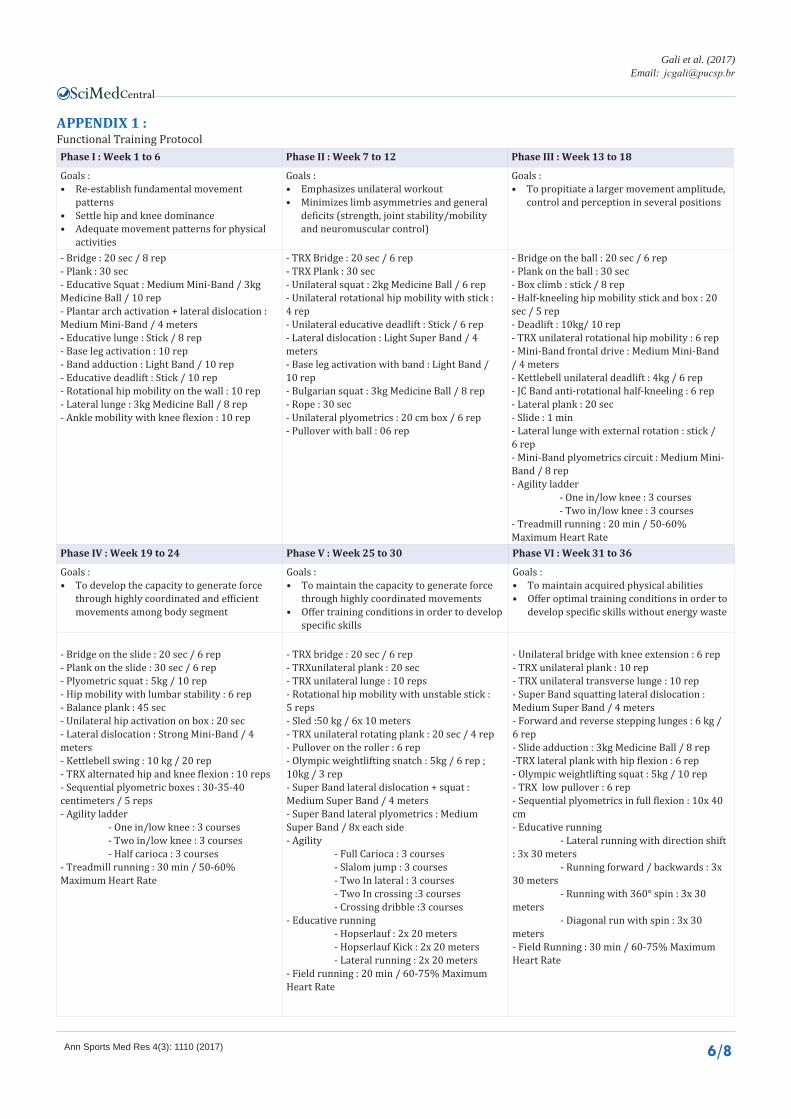
Our training protocol consisted of a 36 week training period starting right after the rehabilitation period. Training was divided into six phases of six weeks each one and the exercises were performed three times a week. It was based on core stability exercises, and limb asymmetries and neuromuscular deficits correction in order to improve neuromuscular control and to minimize the risk of further injury (Appendix 1).
Patients were divided into study and control groups. The study group consisted of ten individuals who had completed our proposed protocol after two months of physical therapy rehabilitation. In this group there were eight males and two females whose ages varied from 25 to 53 years with an average of 37.5 years. Six of the treated knees were right and four left.
The control group also consisted of ten people, nine males and one female, who had done two months of physical therapy and a regular ACLR rehabilitation protocol including muscular strengthening, endurance, proprioception, plyometrics and sport specific training for six months [20] (Appendix 2). Their ages ranged from 19 to 46 years with an average of 32.1 years. There were five right and five left knees treated in this group. Both groups had comparable range of motion, joint stability and thigh muscle trophism.
The FMS was used to compare the performance of the two groups. The study group was evaluated just after the 36 weeks of functional training and the control group was assessed immediately after the standard ACLR rehabilitation.
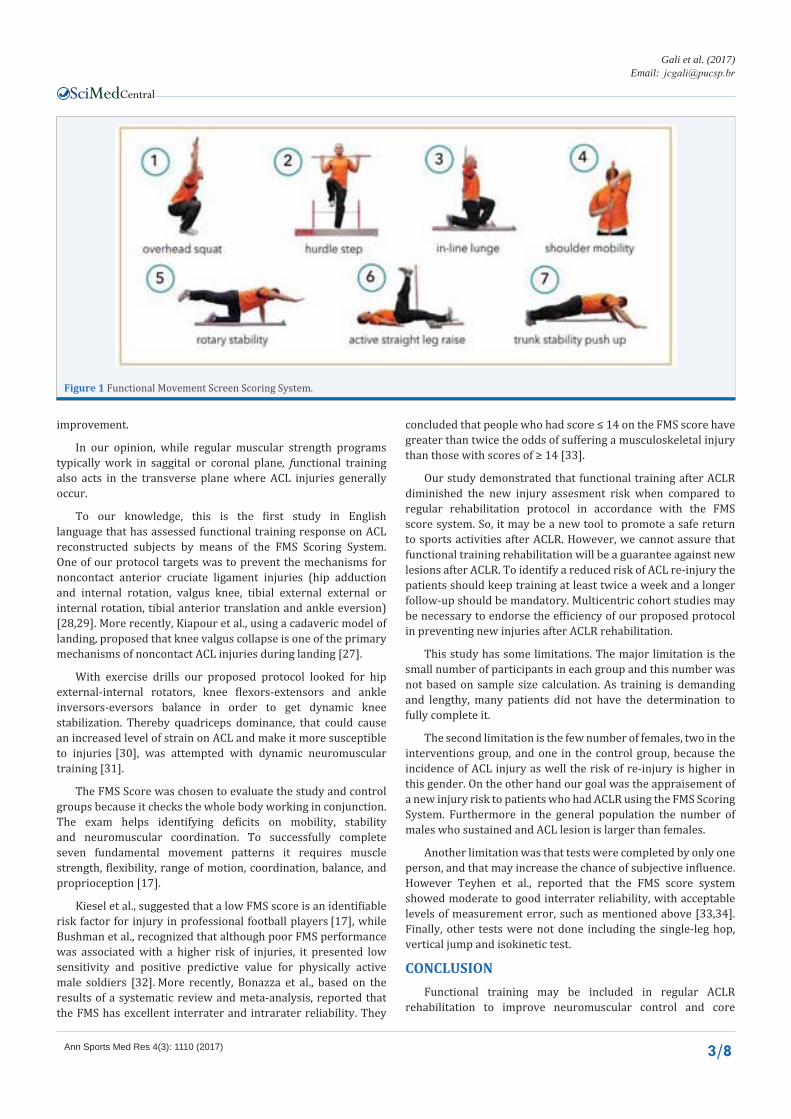
This exam analyses the quality of seven fundamental movement patterns applied to check mobility, stability, neuromuscular and motor control, in order to diagnose limitations and/or asymmetries (Figure 1). Patients with a score of 14 or less on the FMS were considered more likely to suffer an injury than those with a higher score [21,22]. All tests were performed by a discerning and experienced physical trainer.
STATISTICAL ANALYSISThe Mann-Whitney test and Fisher’s exact test were used to
compare the FMS score, age, gender and affected side of the two groups. The significance level (α) established was 0.05 or 5%.
RESULTSThere was no significant statistical correlation among age,
gender, involved side and FMS score. The average FMS score of the study group was 16.6 compared to the control group at 12.3. Demographic data and FMS Score are shown in Tables (1,2).
According to the FMS score, functional training for ACL reconstructed knees rehabilitation added a statistically significant benefit (p < 0,0002) to decrease the risk of new injury, compared to regular rehabilitation protocol.
DISCUSSION The outcomes of our study may recommend functional
training as a requirement for ACLR rehabilitation programs. Literally functional means outlined mainly from the conception required, then we may say that this workout was specially planned for ACLR rehabilitation.
Functional training combines neuromuscular control, joint mobility and stability, core stability, alignment of the trunk and lower limb joints. Ageberg & Roos defined neuromuscular control (sensorimotor control) as the ability to produce controlled movement through coordinated muscle activity [23]. Core stability seeks the strengthening of abdominal, paraspinal and gluteal musculature in order to produce maximum stability in the abdomen and spine. It can be defined as the ability of the lumbopelvic-hip complex to prevent buckling of the vertebral column and return it to equilibrium following perturbation [24]. Core stability provides a stable base for movement of extremities and its training uses core muscles in daily tasks and sport-specific activities [25]. Moreover, muscular fatigue by altering neuromuscular control, decreases core strength and proprioception and may increase the non-contact ACL injuries risk [26].
Different from traditional muscular strength programs, during functional training, multiple joints and muscles are exercised on three planes of motion, challenging simultaneously the brain and body. In fact, intervention programs that aim multiple planes of load are needed to effectively reduce the ACL injury risk [27].
In our protocol the agonist and antagonist muscles are coactivated to maintain balance of loaded segments in static and dynamic situations. Functional training can also provide muscular strength, power and endurance. In this kind of practice efficiency and quality of movements are mandatory. Patients’ compensatory patterns can also be assessed and continuous supervision may provide eventual adjustments for function
Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 3/8
Figure 1 Functional Movement Screen Scoring System.
improvement.
In our opinion, while regular muscular strength programs typically work in saggital or coronal plane, functional training also acts in the transverse plane where ACL injuries generally occur.
To our knowledge, this is the first study in English language that has assessed functional training response on ACL reconstructed subjects by means of the FMS Scoring System. One of our protocol targets was to prevent the mechanisms for noncontact anterior cruciate ligament injuries (hip adduction and internal rotation, valgus knee, tibial external external or internal rotation, tibial anterior translation and ankle eversion) [28,29]. More recently, Kiapour et al., using a cadaveric model of landing, proposed that knee valgus collapse is one of the primary mechanisms of noncontact ACL injuries during landing [27].
With exercise drills our proposed protocol looked for hip external-internal rotators, knee flexors-extensors and ankle inversors-eversors balance in order to get dynamic knee stabilization. Thereby quadriceps dominance, that could cause an increased level of strain on ACL and make it more susceptible to injuries [30], was attempted with dynamic neuromuscular training [31].
The FMS Score was chosen to evaluate the study and control groups because it checks the whole body working in conjunction. The exam helps identifying deficits on mobility, stability and neuromuscular coordination. To successfully complete seven fundamental movement patterns it requires muscle strength, flexibility, range of motion, coordination, balance, and proprioception [17].
Kiesel et al., suggested that a low FMS score is an identifiable risk factor for injury in professional football players [17], while Bushman et al., recognized that although poor FMS performance was associated with a higher risk of injuries, it presented low sensitivity and positive predictive value for physically active male soldiers [32]. More recently, Bonazza et al., based on the results of a systematic review and meta-analysis, reported that the FMS has excellent interrater and intrarater reliability. They
concluded that people who had score ≤ 14 on the FMS score have greater than twice the odds of suffering a musculoskeletal injury than those with scores of ≥ 14 [33].
Our study demonstrated that functional training after ACLR diminished the new injury assesment risk when compared to regular rehabilitation protocol in accordance with the FMS score system. So, it may be a new tool to promote a safe return to sports activities after ACLR. However, we cannot assure that functional training rehabilitation will be a guarantee against new lesions after ACLR. To identify a reduced risk of ACL re-injury the patients should keep training at least twice a week and a longer follow-up should be mandatory. Multicentric cohort studies may be necessary to endorse the efficiency of our proposed protocol in preventing new injuries after ACLR rehabilitation.
This study has some limitations. The major limitation is the small number of participants in each group and this number was not based on sample size calculation. As training is demanding and lengthy, many patients did not have the determination to fully complete it.
The second limitation is the few number of females, two in the interventions group, and one in the control group, because the incidence of ACL injury as well the risk of re-injury is higher in this gender. On the other hand our goal was the appraisement of a new injury risk to patients who had ACLR using the FMS Scoring System. Furthermore in the general population the number of males who sustained and ACL lesion is larger than females.
Another limitation was that tests were completed by only one person, and that may increase the chance of subjective influence. However Teyhen et al., reported that the FMS score system showed moderate to good interrater reliability, with accept able levels of measurement error, such as mentioned above [33,34]. Finally, other tests were not done including the single-leg hop, vertical jump and isokinetic test.
CONCLUSIONFunctional training may be included in regular ACLR
rehabilitation to improve neuromuscular control and core

Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 4/8
Table 1 : Study Group Patients' Age, Gender, Side and FMS Score.
Patient # Age Gender Side FMS Score
1 27 M R 18
2 43 M R 14
3 37 M L 16
4 32 F R 19
5 53 M R 16
6 34 M L 16
7 25 M R 18
8 42 M R 16
9 45 M L 15
10 37 F L 18
Average 37.5 16.6
Table 2 : Control Group Patients' Age, Gender, Side and FMS Score.
Patient # Age Gender Side FMS Score
1 38 M L 13
2 31 M R 12
3 19 M R 14
4 26 M R 13
5 45 M L 12
6 34 M L 12
7 46 M R 11
8 19 F L 12
9 23 M L 13
10 40 M R 11
Average 32.1 12.3
stability, to correct limb asymmetries and possibly to lower the recurrent instability risk, prior to returning to sports.
ACKNOWLEDGEMENTSWe give special thanks to Dr. Julio C. Gali Filho, Mr. John
Peel and Mrs. Rachel Hunter for their support on writing this manuscript.
REFERENCES1. Linko E, Harilainen A, Malmivaara A, Seitsalo S. Surgical versus
conservative interventions for anterior cruciate ligament ruptures in adults. Cochrane Database Syst Rev. 2005; 18: CD001356.
2. Hewett TE, Di Stasi SL, Myer GD. Current Concepts for Injury Prevention in Athletes After Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2013; 41: 216-224.
3. Hewett TE, Paterno MV, Myer GD. Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop Relat Res. 2002; 76-94.
4. Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005; 33: 492-501.
5. Myer GD, Martin L Jr, Ford KR, Paterno MV, Schmitt LC, Heidt RS Jr,
et al. No association of time from surgery with functional deficits in athletes after anterior cruciate ligament reconstruction: evidence for objective return-to-sport criteria. Am J Sports Med. 2012; 40: 2256-2263.
6. Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010; 38: 1968-1978.
7. Mandelbaum BR, Silvers HJ, Watanabe DS, Knarr JF, Thomas SD, Griffin LY, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med. 2005; 33: 1003-1010.
8. Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: Part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006; 34: 490-498.
9. Wingfield K. Neuromuscular training to prevent knee injuries in adolescent female soccer players. Clin J Sport Med. 2013; 23: 407-408.
10. Gagnier JJ, Morgenstern H, Chess L. Interventions designed to prevent anterior cruciate ligament injuries in adolescents and adults: a systematic review and meta-analysis. Am J Sports Med. 2013; 41: 1952-1962.
11. Risberg MA, Holm I, Myklebust G, Engebretsen L. Neuromuscular
Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 5/8
training versus strength training during first 6 months after anterior cruciate ligament reconstruction: a randomized clinical trial. Phys Ther. 2007; 87: 737-750.
12. Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis. Am J Sports Med. 2016; 44: 1861-1876.
13. Anderson MA, Gieck JH, Perrin DH, Weltman A, Rutt RA, Denegar CR. The Relationships among Isometric, Isotonic, and Isokinetic Concentric and Eccentric Quadriceps and Hamstring Force and Three Components of Athletic Performance. J Orthop Sports Phys Ther. 1991; 14: 114-120.
14. Reid A, Birmingham TB, Stratford PW, Alcock GK, Giffin JR. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys Ther. 2007; 87: 337-349.
15. Paterno MV, Ford KR, Myer GD, Heyl R, Hewett TE. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin J Sport Med. 2007; 17: 258-262.
16. Myer GD, Paterno MV, Ford KR, Hewett TE. Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. J Strength Cond Res. 2008; 22: 987-1014.
17. Kiesel K, Plisky PJ, Voight ML. Can Serious Injury in Professional Football be Predicted by a Preseason Functional Movement Screen? N Am J Sports Phys Ther. 2007; 2: 147-158.
18. Boyle MJ, Butler RJ, Queen RM. Functional Movement Competency and Dynamic Balance After Anterior Cruciate Ligament Reconstruction in Adolescent Patients. J Pediatr Orthop. 2016; 36: 36-41.
19. MacDonald PB, Hedden D, Pacin O, Huebert D. Effects of an accelerated rehabilitation program after anterior cruciate ligament reconstruction with combined semitendinosus-gracilis autograft and a ligament augmentation device. Am J Sports Med. 1995; 23: 588-592.
20. Physiotherapy following acl reconstruction protocol. Fowler Kennedy.
21. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: the use of fundamental movements as an assessment of function - part 1. Int J Sports Phys Ther. 2014; 9: 396-409.
22. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: the use of fundamental movements as an assessment of function-part 2. Int J Sports Phys Ther. 2014; 9: 549-563.
23. Ageberg E, Roos EM. Neuromuscular exercise as treatment of degenerative knee disease. Exerc Sport Sci Rev. 2015; 43: 14-22.
24. Pope MH, Panjabi M. Biomechanical definitions of spinal instability. Spine (Phila Pa 1976). 1985; 10: 255-256.
25. Willson JD, Dougherty CP, Ireland ML, Davis IM. Core stability and its relationship to lower extremity function and injury. J Am Acad Orthop Surg. 2005; 13: 316-325.
26. Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lázaro-Haro C, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc. 2009; 17: 705-729.
27. Kiapour AM, Demetropoulos CK, Kiapour A, Quatman CE, Wordeman SC, Goel VK, et al. Strain Response of the Anterior Cruciate Ligament to Uniplanar and Multiplanar Loads During Simulated Landings: Implications for Injury Mechanism. Am J Sports Med. 2016; 44: 2087-2096.
28. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004; 32: 1002-1012.
29. Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. Am J Sports Med. 2006; 34: 299-311.
30. Renström P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH. Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med. 1986; 14: 83-87.
31. Hewett TE, Johnson DL. ACL prevention programs: fact or fiction. Orthopedics. 2010; 33: 36-39.
32. Bushman TT, Grier TL, Canham-Chervak M, Anderson MK, North WJ, Jones BH. The Functional Movement Screen and Injury Risk: Association and Predictive Value in Active Men. Am J Sports Med. 2016; 44: 297-304.
33. Bonazza NA, Smuin D, Onks CA, Silvis ML, Dhawan A. Reliability, Validity, and Injury Predictive Value of the Functional Movement Screen. Am J Sports Med. 2017; 45: 725-732.
34. Teyhen DS, Shaffer SW, Lorenson CL, Halfpap JP, Donofry DF, Walker MJ, et al. The Functional Movement Screen: a reliability study. J Orthop Sports Phys Ther. 2012; 42: 530-540.
Gali JC, Separovic Faria FA, Gali Filho JC, da Silva PAC (2017) Functional Training may Lower New Injury Risk Assessment after Anterior Cruciate Ligament Reconstruction. Ann Sports Med Res 4(3): 1110.
Cite this article
Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 6/8
APPENDIX 1 : Functional Training ProtocolPhase I : Week 1 to 6 Phase II : Week 7 to 12 Phase III : Week 13 to 18
Goals :• Re-establish fundamental movement
patterns• Settle hip and knee dominance• Adequate movement patterns for physical
activities
Goals :• Emphasizes unilateral workout• Minimizes limb asymmetries and general
deficits (strength, joint stability/mobility and neuromuscular control)
Goals :• To propitiate a larger movement amplitude,
control and perception in several positions
- Bridge : 20 sec / 8 rep- Plank : 30 sec- Educative Squat : Medium Mini-Band / 3kg Medicine Ball / 10 rep- Plantar arch activation + lateral dislocation : Medium Mini-Band / 4 meters- Educative lunge : Stick / 8 rep - Base leg activation : 10 rep- Band adduction : Light Band / 10 rep- Educative deadlift : Stick / 10 rep- Rotational hip mobility on the wall : 10 rep- Lateral lunge : 3kg Medicine Ball / 8 rep - Ankle mobility with knee flexion : 10 rep
- TRX Bridge : 20 sec / 6 rep- TRX Plank : 30 sec- Unilateral squat : 2kg Medicine Ball / 6 rep- Unilateral rotational hip mobility with stick : 4 rep- Unilateral educative deadlift : Stick / 6 rep- Lateral dislocation : Light Super Band / 4 meters- Base leg activation with band : Light Band / 10 rep- Bulgarian squat : 3kg Medicine Ball / 8 rep- Rope : 30 sec- Unilateral plyometrics : 20 cm box / 6 rep- Pullover with ball : 06 rep
- Bridge on the ball : 20 sec / 6 rep- Plank on the ball : 30 sec- Box climb : stick / 8 rep- Half-kneeling hip mobility stick and box : 20 sec / 5 rep- Deadlift : 10kg/ 10 rep- TRX unilateral rotational hip mobility : 6 rep- Mini-Band frontal drive : Medium Mini-Band / 4 meters- Kettlebell unilateral deadlift : 4kg / 6 rep- JC Band anti-rotational half-kneeling : 6 rep- Lateral plank : 20 sec- Slide : 1 min- Lateral lunge with external rotation : stick / 6 rep- Mini-Band plyometrics circuit : Medium Mini-Band / 8 rep- Agility ladder - One in/low knee : 3 courses - Two in/low knee : 3 courses- Treadmill running : 20 min / 50-60% Maximum Heart Rate
Phase IV : Week 19 to 24 Phase V : Week 25 to 30 Phase VI : Week 31 to 36
Goals :• To develop the capacity to generate force
through highly coordinated and efficient movements among body segment
Goals :• To maintain the capacity to generate force
through highly coordinated movements• Offer training conditions in order to develop
specific skills
Goals :• To maintain acquired physical abilities• Offer optimal training conditions in order to
develop specific skills without energy waste
- Bridge on the slide : 20 sec / 6 rep- Plank on the slide : 30 sec / 6 rep- Plyometric squat : 5kg / 10 rep- Hip mobility with lumbar stability : 6 rep- Balance plank : 45 sec- Unilateral hip activation on box : 20 sec- Lateral dislocation : Strong Mini-Band / 4 meters- Kettlebell swing : 10 kg / 20 rep- TRX alternated hip and knee flexion : 10 reps- Sequential plyometric boxes : 30-35-40 centimeters / 5 reps- Agility ladder - One in/low knee : 3 courses - Two in/low knee : 3 courses - Half carioca : 3 courses- Treadmill running : 30 min / 50-60% Maximum Heart Rate
- TRX bridge : 20 sec / 6 rep- TRXunilateral plank : 20 sec- TRX unilateral lunge : 10 reps- Rotational hip mobility with unstable stick : 5 reps- Sled :50 kg / 6x 10 meters- TRX unilateral rotating plank : 20 sec / 4 rep- Pullover on the roller : 6 rep- Olympic weightlifting snatch : 5kg / 6 rep ; 10kg / 3 rep- Super Band lateral dislocation + squat : Medium Super Band / 4 meters- Super Band lateral plyometrics : Medium Super Band / 8x each side- Agility - Full Carioca : 3 courses - Slalom jump : 3 courses - Two In lateral : 3 courses - Two In crossing :3 courses - Crossing dribble :3 courses- Educative running - Hopserlauf : 2x 20 meters - Hopserlauf Kick : 2x 20 meters - Lateral running : 2x 20 meters- Field running : 20 min / 60-75% Maximum Heart Rate
- Unilateral bridge with knee extension : 6 rep- TRX unilateral plank : 10 rep- TRX unilateral transverse lunge : 10 rep- Super Band squatting lateral dislocation : Medium Super Band / 4 meters- Forward and reverse stepping lunges : 6 kg / 6 rep- Slide adduction : 3kg Medicine Ball / 8 rep-TRX lateral plank with hip flexion : 6 rep- Olympic weightlifting squat : 5kg / 10 rep- TRX low pullover : 6 rep- Sequential plyometrics in full flexion : 10x 40 cm- Educative running - Lateral running with direction shift : 3x 30 meters - Running forward / backwards : 3x 30 meters - Running with 360° spin : 3x 30 meters - Diagonal run with spin : 3x 30 meters- Field Running : 30 min / 60-75% Maximum Heart Rate

Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 7/8
APPENDIX 2 : Regular ACLR Rehabilitation Protocol
9 - 12 Weeks PO
GOALS
• Flexibility exercises
• Quadriceps strength progression
• Address documented hamstring strength deficits (high speed, eccentric 95-60°)
• Lower chain concentric/eccentric strengthening of quadriceps & hamstrings, both inner range (60- 95°) & full range
• Proprioceptive progression
• Sport specific cardiovascular fitness
Muscular Strength & Endurance
Quadriceps:
• Progress resistance of Shuttle™: full range of motion (ROM) and inner range (60-95°), working on strength & endurance, 2 → 1 leg
• Static Lunge (full range) → 7 dynamic lunge → 7 lunge walking all with proper trunk and leg alignment
• Backward step up 4-6-8” step
• Clock face lunges with Bungee™ using mini pylon markers
• Quick walk forward/backward with Bungee™
• Quick side stepping with Bungee™
• Quick lunge forward with control (upright trunk, no forward thrust, no hip hiking)
• Eccentric Bungee™
• Eccentric step down with control on 6 → 8” step
• Shuttle™ jumping (Iow resistance) 2 legs → alternate legs (jogging) → single leg
• Shuttle™ ski hops (side-to-side)
• Continue / progress isokinetic program if patient is appropriate and equipment is available
Hamstrings/Gluteals:
• Prone/standing pulley knee flexion
• Chair walking
• Prone eccentric hamstrings with pulleys/tubing, alternating inner range and full range
• Hydrafitness™ (hamstrings & quadriceps): 90-30°, resistance 1-3
• Continue hip strengthening with increased weights/tubing resistance
• Sitting and standing hamstring curls - Bungee™/pulleys/ weights sitting and standing positions - address full range concentrically and inner range from 95-60°eccentrically and high velocity (if pain free & without difficulty)
• Supine eccentric hamstrings with knee in extension
Calves:
• Eccentric heel drops
Proprioception
• On boards/Dynadisc™/BOSU™/foam roller/mini trampoline: catch and throw (2 hands/1hand) at varying angles and directions with partner or
using rebounder
• Dynadisc™ or BOSU™ throwing on rebounder feet side-to-side, forward/backward, 2-1 foot
• Perturbation drills with tubing on boards/ Dynadisc™/BOSU™ /foam roller/mini trampoline
• Single leg stance on Dynadisc™ or BOSU™ with unaffected leg performing kicking drills +/- tubing/pulleys
• Single leg stance on Dynadisc™ or BOSU™ performing kicking drills +/- tubing/ pulleys
• Single leg stance on Dynadisc™ or BOSU™ performing higher end upper body skills
Hydrotherapy / Pool
• Increase time, speed, repetitions of exercises
• Pool running
Cardiovascular Fitness
• Bike: increased resistance and time parameters
• Fitter™: slalom skiing without ski pole support
•Treadmill walk +/- incline → quick walk
12-16 Weeks PO
GOALS
• Continue with flexibility exercises for the lower chain
• Continue strengthening of the lower chain
• Sport specific quadriceps & hamstrings strengthening
• Sport specific proprioception training
• Sport specific cardiovascular fitness
Muscle Strength & Endurance
• Continue with concentric and eccentric strengthening of hamstrings and quadriceps, working through full & inner range
• Backward lunge - progress to backward lunge walking (with proper trunk and leg alignment)
• Bungee™ jogging - progress to running
• Split squat jumps - progress to BOSU™
• Single leg drop landing 2” step
Agility
• Ladder drills - forward/backward, side-to-side (focus on footwork/speed/timing)
• 2 legged lateral and forward jumping
• Side step-overs (hurdle) - progress to side hop-overs
• Carioca patterning
• Tuck jumps
• Skipping
• Initiate 2 legged hop tests (hop for distance, 6-m timed hop, triple hop, crossover hop) prior to single leg hop tests in next stage - ensure patterning and landing is proficient prior to 1 leg progression
Proprioception
• Mini trampoline: 2 feet jump & land → jogging → 1leg hopping (lL/1R, 2L/2R, 3L/3R ... )

Central
Gali et al. (2017)Email:
Ann Sports Med Res 4(3): 1110 (2017) 8/8
• Continue progressing skill difficulty
• Single leg stance - tap down clock drill with mini pylons
• Dynadisc™ or BOSU™: 1 leg balance with upper body or opposite leg skill i.e. throwing, phantom kicking with Bungee™ resistance, hockey shot....
Hydrotherapy / Pool
• Progress to plyometrics: 2 leg hopping, forward/backward/side-to-side
• Split squat jumping
Cardiovascular Fitness
• Bike - standing with interval training
• Sport specific cardiovascular training: aerobic vs. anaerobic training
• Jogging - straight on flat ground, no cuts/no downhill
• Treadmill- jog → interval running → running
16-20 Weeks PO
GOALS
• Sport specific quadriceps, hamstrings and lower chain strengthening progressing to plyometrics
• Proprioception training
• Sport specific cardiovascularfitness
Muscle Strength & Endurance
• Continue with lower extremity strengthening with specific emphasis on client-specific deficits
• 2 → 1 leg progression for all exercises
Plyometrics and Agility
• Ladder drills - incorporate lateral movements/diagonals, adding single leg and crossover patterns
• Running/lunging/vertical jump/ run-plant-sidestep with Bungee™ - may incorporate upper/lower body skill - kicking, jumping, catching, pass & shoot
• Shuttle™ hopping 2 - alt -1 (high resistance, increased speed)
• Shuttle™ Ski hops (high resistance, increased speed)
• Carioca 3/4 jog
• Mini trampoline: 2 leg jump off - 2 leg land with progression to one leg land on/off balance pad/BOSU™ (watch for proper landing mechanics)
• Single leg forward and lateral hopping
• Hop tests: single hop, 6-m timed hop, triple hop, crossover hop
• Vertical jumps - single leg
• Box hop up /down
• Box jump down with sprint forward
• Box drop jump 2 legs with proper form may progress to drop jump with vertical hop for maximum height
• Single leg drop landing 4-6-8-10” step
Proprioception
• Continue progressions e.g. mini trampoline with upper skills
• Forward hop and lateral hop - maintain balance for 5 sec on landing
• Cutting drills with quick stop and maintain balance
• Bungee™ run plant/push off L&R
Cardiovascular Fitness
• Increase distance, duration or intensity with bike, Stairmaster™, treadmill, outdoor running/cycling depending on the demands of the particular sport
• Treadmill: running → sprinting: assess sprinting form - should have normal pain-free rhythmic stride (audible monitoring of foot contact)
• Jogging and running on an uneven surface
• Jogging with turns 90/180/360°
• Jogging and cutting with 45° change of direction
• Acceleration and deceleration running, add on tight turns and hills as tolerated
• Cycling outdoors
• Swimming - no whipkick
20-24 Weeks PO
GOALS
• Adequate cardiovascular fitness, strength, power, agility neuromuscular control, symmetry and stability
• Continue with upper body strengthening
• Back to sport practice for upper skills (as able)
• Return to sport skills on own at practice with minimal rlsk of re-injury
Plyometrics and Agility
• Single leg drop jump 6” step
• large Figure 8’s
• Carioca running full speed
• Last minute decision drills
• 2 and 1 foot hopping with control
• Forward and lateral hop with control and comparable distance L&R
• Triple jump and landing with control and comparable distances L&R
• Single limb hop for distance (within 15% of uninvolved side)
• Single-limb crossover triple hop for distance (within 15% of uninvolved side)
• Single-limb timed hop over 6 m (within 15% of uninvolved side)
• Single limb vertical power hop (within 15% of uninvolved side)
• Single limb drop landing (within 15% of uninvolved side)
• Single limb drop-jump
• 10 second single Iimb maximum vertical hop (both sides)