EndoBarrier Gastrointestinal Liner · 2017-10-19 · sphincter of Oddi (in part mediated by...
18
PHD THESIS DANISH MEDICAL JOURNAL DANISH MEDICAL JOURNAL 1 This review has been accepted as a thesis together with four original papers by University of Copenhagen, Denmark July 7th 2016 and defended on August 15th 2016. Tutor(s): Filip K Knop, Tina Vilsbøll and Jens J Holst Official opponents: Sten Madsbad (DK), Henning Grønbæk (DK) and Baptist Gallwitz (DE) Correspondence: Center for Diabetes Research, Gentofte Hospital, University of Copenhagen, Hellerup, Denmark E-mail: [email protected] Dan Med J 2016;63(11):B5309 The thesis is based on these four original papers 1. Rohde U, Hedbäck N, Gluud LL, Vilsbøll T, Knop FK: Effect of the EndoBarrier Gastrointestinal Liner on obesity and type 2 diabetes: protocol for systematic review and meta-analysis of clinical studies. BMJ Open 2013; 3: e003417. (Study I) 2. Rohde U, Hedbäck N, Gluud LL, Vilsbøll T, Knop FK. Effect of the EndoBarrier Gastrointestinal Liner on obesity and type 2 diabetes: a systematic review and meta-analysis. Diabetes, Obesity and Metabolism 2016; 18: 300-5. (Study II) 3. Rohde U, Federspiel CA, Vilmann P, Langholz E, Friis SU, Krakauer M, Rehfeld JF, Holst JJ, Vilsbøll T, Knop FK. The Im- pact of EndoBarrier Gastrointestinal Liner in Obese Patients with Normal Glucose Tolerance and Patients with Type 2 Diabetes. Manuscript accepted for publication September 2016 in Diabetes, Obesity and Metabolism.(Study III) 4. Rohde U, Sonne DP, Christensen M, Hansen M, Brønden A, Toräng S, Rehfeld JF, Holst JJ, Vilsbøll T, Knop FK. Chole- cystokinin-Induced Gallbladder Emptying and Single-Dose Metformin Elicit Additive Glucagon-Like Peptide-1 Respon- ses. The Journal of Clinical Endocrinology and Metabolism 2016; 101: 2076–2083. (Study IV) INTRODUCTION At a worrying pace, the prevalence of overweight and obesity has reached epidemic proportions. In their latest prognosis, The World Health Organization (WHO) has estimated that more than a quarter of the global population is overweight (body mass index (BMI) ≥25 kg/m 2 ), and 600 million are obese (BMI ≥30 kg/m 2 ) (1). Overweight and obesity entail an increased risk of a number of diseases including cardiovascular diseases, musculoskeletal disea- ses, certain cancers (e.g. colon, breast and endometrial cancers) and type 2 diabetes (T2D) that increase all-cause mortality and reduce life expectancy (2). Given the high prevalence and serious consequences of obesity, therapeutic approaches to overcome obesity have become nume- rous. From a simplistic point-of-view, it is ‘just’ a matter of decre- asing energy input or increasing energy expenditure (or both). Diet alone or combination therapy with the intestinal lipase inhi- bitor orlistat, or exercise combined with amfepramon (closely related to metamfetamin) represent regimens that reduce energy input and increase energy expenditure, respectively. However, placebo-controlled studies have shown that these regimens result in small-to-moderate and non-maintainable long-term weight losses often accompanied by frequent pharmacological side ef- fects (3–5). These discouraging effects and the fact that it over time is nearly impossible to maintain a weight loss (6) leave us with the conclusion that effective medical or lifestyle intervention based treatment of obesity is virtually impossible. Bariatric surgery comprises a range of different surgical procedu- res with the common aim of reducing body weight. The Roux-en-Y gastric bypass (RYGB) procedure probably represents one of the most frequently used type of bariatric surgery and has proven effective in inducing and maintaining substantial weight losses of up to 40% of the excess body weight (defined as percentage of excess body weight lost from a BMI in excess of 25 kg/m 2 ) (7). In parallel to the positive effects of weight loss on cardiovascular and musculoskeletal diseases (e.g. arthritis), insulin sensitivity is known to improve (8). Indeed, studies have shown that 40-80% of obese patients with T2D undergoing RYGB achieved remission of diabetes (9,10). Additionally, long-term studies have shown that dysregulated patients with T2D randomised to RYGB plus intensi- ve medical therapy or intensive medical therapy maintained better glycaemic control (11), and that bariatric surgery signifi- cantly reduces all-cause mortality (12,13). Thus, without doubt bariatric surgery is truly effective. One fundamental issue that remains to be fully elucidated is how the RYGB procedure mediates its effects. Interestingly, the impro- vement in glucose metabolism occurs shortly (days) after surgery and before any major weight loss is achieved (14,15). It has been speculated that the altered gastrointestinal tract anatomy follo- wing RYGB represents one of the main explanations of the impro- ved glucose metabolism. Increasing evidence suggests that gut- derived hormones are important determinants of this improve- ment. Especially, RYGB-induced potentiation of the secretion of the appetite and glucose-lowering incretin hormone glucagon-like EndoBarrier Gastrointestinal Liner Delineation of underlying mechanisms and clinical effects Ulrich Rohde
Transcript of EndoBarrier Gastrointestinal Liner · 2017-10-19 · sphincter of Oddi (in part mediated by...

PHDTHESIS DANISHMEDICALJOURNAL
DANISH MEDICAL JOURNAL 1
ThisreviewhasbeenacceptedasathesistogetherwithfouroriginalpapersbyUniversityofCopenhagen,DenmarkJuly7th2016anddefendedonAugust15th2016.Tutor(s):FilipKKnop,TinaVilsbøllandJensJHolstOfficialopponents:StenMadsbad(DK),HenningGrønbæk(DK)andBaptistGallwitz(DE)Correspondence:CenterforDiabetesResearch,GentofteHospital,UniversityofCopenhagen,Hellerup,DenmarkE-mail:[email protected];63(11):B5309Thethesisisbasedonthesefouroriginalpapers1. RohdeU,HedbäckN,GluudLL,VilsbøllT,KnopFK:Effectof
theEndoBarrierGastrointestinalLineronobesityandtype2diabetes:protocol for systematic reviewandmeta-analysisofclinicalstudies.BMJOpen2013;3:e003417.(StudyI)
2. RohdeU,HedbäckN,GluudLL,VilsbøllT,KnopFK.EffectoftheEndoBarrierGastrointestinalLineronobesityandtype2diabetes: a systematic reviewandmeta-analysis.Diabetes,ObesityandMetabolism2016;18:300-5.(StudyII)
3. Rohde U, Federspiel CA, Vilmann P, Langholz E, Friis SU,KrakauerM,RehfeldJF,HolstJJ,VilsbøllT,KnopFK.TheIm-pactofEndoBarrierGastrointestinalLinerinObesePatientswith Normal Glucose Tolerance and Patients with Type 2Diabetes. Manuscript accepted for publication September2016inDiabetes,ObesityandMetabolism.(StudyIII)
4. RohdeU,SonneDP,ChristensenM,HansenM,BrøndenA,Toräng S, Rehfeld JF, Holst JJ, Vilsbøll T, Knop FK. Chole-cystokinin-Induced Gallbladder Emptying and Single-DoseMetformin Elicit AdditiveGlucagon-Like Peptide-1 Respon-ses. The Journal of Clinical Endocrinology andMetabolism2016;101:2076–2083.(StudyIV)
INTRODUCTIONAtaworryingpace,theprevalenceofoverweightandobesityhasreached epidemic proportions. In their latest prognosis, TheWorldHealthOrganization(WHO)hasestimatedthatmorethanaquarteroftheglobalpopulationisoverweight(bodymassindex(BMI)≥25kg/m2),and600millionareobese(BMI≥30kg/m2)(1).Overweight and obesity entail an increased risk of a number ofdiseasesincludingcardiovasculardiseases,musculoskeletaldisea-ses, certain cancers (e.g. colon,breastandendometrial cancers)
and type 2 diabetes (T2D) that increase all-causemortality andreducelifeexpectancy(2).Given thehighprevalenceand serious consequencesofobesity,therapeuticapproachestoovercomeobesityhavebecomenume-rous.Fromasimplisticpoint-of-view,itis‘just’amatterofdecre-asing energy input or increasing energy expenditure (or both).Dietaloneorcombinationtherapywiththeintestinallipaseinhi-bitor orlistat, or exercise combined with amfepramon (closelyrelatedtometamfetamin)representregimensthatreduceenergyinput and increase energy expenditure, respectively. However,placebo-controlledstudieshaveshownthattheseregimensresultin small-to-moderate and non-maintainable long-term weightlosses often accompanied by frequent pharmacological side ef-fects (3–5). These discouraging effects and the fact that it overtime is nearly impossible tomaintain aweight loss (6) leave uswiththeconclusionthateffectivemedicalorlifestyleinterventionbasedtreatmentofobesityisvirtuallyimpossible.Bariatricsurgerycomprisesarangeofdifferentsurgicalprocedu-reswiththecommonaimofreducingbodyweight.TheRoux-en-Ygastricbypass (RYGB)procedureprobably representsoneof themost frequently used type of bariatric surgery and has proveneffectiveininducingandmaintainingsubstantialweightlossesofup to 40%of the excess bodyweight (defined as percentage ofexcessbodyweightlostfromaBMIinexcessof25kg/m2)(7).Inparallel to the positive effects of weight loss on cardiovascularandmusculoskeletal diseases (e.g. arthritis), insulin sensitivity isknowntoimprove(8).Indeed,studieshaveshownthat40-80%ofobesepatientswithT2DundergoingRYGBachievedremissionofdiabetes (9,10).Additionally, long-term studieshave shown thatdysregulatedpatientswithT2DrandomisedtoRYGBplusintensi-ve medical therapy or intensive medical therapy maintainedbetter glycaemic control (11), and that bariatric surgery signifi-cantly reduces all-cause mortality (12,13). Thus, without doubtbariatricsurgeryistrulyeffective.OnefundamentalissuethatremainstobefullyelucidatedishowtheRYGBproceduremediatesitseffects.Interestingly,theimpro-vementinglucosemetabolismoccursshortly(days)aftersurgeryandbeforeanymajorweightlossisachieved(14,15).Ithasbeenspeculated that the altered gastrointestinal tract anatomy follo-wingRYGBrepresentsoneofthemainexplanationsoftheimpro-ved glucosemetabolism. Increasing evidence suggests that gut-derived hormones are important determinants of this improve-ment. Especially, RYGB-induced potentiation of the secretion oftheappetiteandglucose-loweringincretinhormoneglucagon-like
EndoBarrierGastrointestinalLiner
Delineationofunderlyingmechanismsandclinicaleffects
UlrichRohde

DANISH MEDICAL JOURNAL 2
peptide-1 (GLP-1) seems tobe important (16,17).GLP-1and therelated incretin hormone glucose-dependent insulinotropic po-lypeptide (GIP) are secreted fromenteroendocrine L cells andKcells, respectively, and play a pivotal role inmaintaining normalfastingandpostprandialglucoselevelsbyincreasinginsulinsecre-tionfollowingingestionofnutrients(18).Thisisreferredtoastheincretineffect,whichaccountsforupto70%of insulinsecretionfollowingoralingestionofglucoseinhealthysubjects.InpatientswithT2Dhowever,theincretineffectisimpaired,whichisconsi-deredasignificantandearlypartofthepathogenesisinT2D(19).Following RYGB, undigested nutrients bypass the proximal in-testines and are expedited to distal and L cell-rich parts of thesmall bowel, giving rise to increased GLP-1 secretion and sub-sequent insulin secretion, which is a consistent finding in RYGBstudies.Ontheotherhand,theimpactofRYGBonthesecretionof GIP from enteroendocrine K cellswhich are found in highestnumbers in theproximal small intestine,variesandpostprandialGIPresponseshavebeenreportedattenuated,unalteredorevenincreasedafterRYGB(15,17).Another,andhighlyclinicallyrelevantissueaboutbariatricsurge-ryistheinvasivenessoftheprocedures,andtheriskofcomplica-tions, both short-term (e.g. bleeding, anastomosis leak, ileus,internalherniationandthromboembolicepisodes)andlong-term(nutritional deficiencies due to micronutrient malassimilation,dumpingsyndromeoranastomoticstrictures/bowelobstruction)complications. Indeed, in a systematic review Chang et al. (7)reportedanoverallpostoperativecomplicationrateof21%follo-wingRYGB,aperioperativemortalityratewithin30daysof0.38%and a postoperative (>30 days) mortality rate of 0.72% withpulmonary embolism being the leading cause of death. Additio-nally,upto20%ofpatientsundergoingRYGBrequirereoperationdueto long-termcomplications (20)and51.3%and22.7%deve-lop iron deficiency or iron deficiency anaemia within one yearaftersurgery,respectively(21).Thesesideeffectsandcomplicati-ons remain aworrisome clinical problemand there is anunmetneedforsimplerandlessinvasivealternatives.TheEndoBarrierGastrointestinalliner(orduodenal-jejunalbypasssleeve(DJBS))couldrepresentsuchanalternative.Itisareversib-le and endoscopic procedure for obesity and T2D treatment,which is thought tomimic the intestinalbypass componentofaRYGB.TheDJBSconsistsofa60cmlong,hollowandhighlyflexib-le sleeve that is implanted into the upper proximal and post-pyloric part of the small intestines. Following meal ingestion,gastricchymeflowsdownand insidethesleeve.Thesleevepre-vents the gastric chyme from stimulating the duodenal andproximal jejunal mucosa, thus shunting ingested nutrients tomoredistalpartsof the intestines. The few (small-sized) studiesthat have appeared so far demonstrated that subjects treatedwith theDJBS loseweight, and that some subjects improve glu-cose metabolism (22,23). Despite intended as a RYGB mimetic,theexactmechanismsbehindDJBS’effectsstillremaintobefullyelucidated.Inaddition tostimulationofguthormonesecretion, food intakeelicits contraction of the gallbladder and relaxation of the
sphincter of Oddi (in part mediated by nutrient-induced chole-cystokinin (CCK) secretion from enteroendocrine I cells in theproximal gut) and flow of bile acids into the small intestinal lu-men. The facilitation of lipid absorption has traditionally beenconsideredthemostimportanteffectofmeal-inducedejectionofbile into the duodenum. However, over the last decade it hasbecomeclearthatbileacidsarenotonlyfat-emulsifiersnecessaryforlipidassimilation,butalsoactaskeymetabolicintegratorsofglucoseandenergymetabolism.Thismodeofaction isbelievedtoinvolveactivationofthenuclearfarnesoidXreceptor(FXR)andthe membrane bound G-protein-coupled receptor 5 (TGR5) bybileacidsinthegut.Theexactpathwaysbywhichthesereceptorsmediatetheireffects remaintobeunravelled,but, interestingly,several in vitro and animal studies have reported bile acid-inducedGLP-1secretionviastimulationofTGR5(24–26). Impor-tantly, these findings have been confirmed in humans (27–31).However, the physiological impact of gallbladder emptying andsubsequent ejection of bile acids into the intestines for humanGLP-1secretionremainstobeclarified.AsDJBShasbeenshownto increase bile acid concentrations in obese patients with T2D(32), onemight speculate that the reported glycaemic improve-ments following DJBS treatment may involve bile acid-inducedGLP-1secretion.Moreover,themostwidelyusedandfirst-in-lineglucose-loweringdruginthemanagementofT2D,metformin,hasremarkably been shown to increase GLP-1 secretion (33–35),whichmayconstitutean importantpartofmetformin’sglucose-loweringeffect.Theexactmechanismsunderlyingthisphenome-non remain relatively unclear, but in vitro studies suggest thatmetformininhibitsbileacidreuptakethroughtheapicalsodium-dependent bile acid transporter (ASBT) in the ileum (36,37),whichinturncanbethoughttoincreasebileacid-inducedactiva-tion of TGR5 on L cells and thereby elicit GLP-1 secretion. Also,metformin-induced inhibition of ASBT may reduce intracellularconcentrations of bile acids in enteroendocrine L cells and,consequently, reduce activation of the nuclear FXR, which mayincrease GLP-1 production and secretion as suggested from re-cent studies by Trabelsi et al. (38). In line with these notions,increasedfaecalbileacidexcretioninpatientswithT2Dfollowingmetforminhasbeenobserved(34,39).Nevertheless,theeffectofgallbladderemptyingonhumanGLP-1secretionanditspotentialrole in metformin-induced GLP-1 secretion remain unknown.Hypothetically, metformin-induced GLP-1-secretion may be de-pendentonthepresenceofbileinthegutlumenand,thus,gall-bladderemptying.WhetherandhowDJBS(coveringtheproximalsmallintestinalmucosa,whichisrichinCCK-secretingIcells)mayinterferewithgallbladderemptyingandbileacidandmetformin-induced GLP-1 secretion remains unknown. Interestingly, howe-ver, results from theprematurely terminatedENDO trial, rando-mising obese patientswith inadequately controlled T2D on oralantidiabeticmedicationtoDJBSorsham-procedure(40),showedthatDJBSleadtogreaterglycatedhaemoglobinA1c(HbA1c)redu-ctionsthansham.Sincethemajorityofparticipantsweretreatedwith metformin, one may speculate that metformin combined

DANISH MEDICAL JOURNAL 3
with DJBS could contribute to any increase in GLP-1 secretionduringDJBStreatment.In thepresent thesis, theclinicalefficacyandsafetyofDJBStre-atmentinsubjectswithobesityandpatientswithT2Dwasevalu-ated and the physiological impact of DJBS was investigated.Furthermore,the impactofgallbladderemptyingandmetforminonhumanGLP-1-secretionwasassessed.
BARIATRICSURGERYROUX-EN-YGASTRICBYPASS(RYGB)SURGERYThe history of bariatric surgery takes it beginningwhenKremenand Varco in the early 1950s performed the jejunoileal bypass(41). Following this procedure, the proximal jejunum was con-nected to the terminal ileumbywhich themajorityof the smallintestines were bypassed. The jejunoileal bypass was indeedeffective in termsofbodyweight loss,buthadseveral importantside effects and complications since many patients developedsteatorrhea, diarrhoea, and electrolyte derangement, nephro-lithiasis,vitamindeficienciesandliverfailurepostoperatively.Theprocedurewasthereforeabandoned.In1967theRYGBprocedu-rewas first introduced (42).Firstasanopensurgicalprocedure,and later in 1993 as a laparoscopic procedure (43). RYGB altersthegastrointestinaltractanatomy(Fig.1).Initially,thestomachisdividedintotwoparts;aproximalsmall(30ml)pouchconnectedtotheoesophagus,anda largerdistalpartstillconnectedtotheduodenumandproximal jejunum.Approximately30cmdistaltotheLigamentofTreitzthesmallintestineisdividedandthedistalintestinal segment is brought up to the small gastric pouch tomake a gastroenterostomy. Some 100 cm below the point ofdivision, the bypassed segment (encompassing the remnantstomach,duodenumandproximaljejunum)isre-connectedintoaY-configuration. This blind-ending part of the gastrointestinaltract constitutes the bilio-pancreatic limb. Thedistal part of thejejunum,anastomosedtothesmallgastricpouch,nowrepresentstheRouxoralimentarylimb.Thecommonlimbreferstothesmallintestines from the Y-intersection to valvula Bauhini (44). Thereconfigured gastrointestinal tract anatomy entails that orallyingested nutrients pass down the oesophagus into the smallgastricpouchanddirectlyintoarelativelydistalpartofthesmallintestines; bypassing the stomach, duodenum and the proximaljejunum (45). The RYGB has traditionally been considered anirreversible restrictive andmalabsorptiveprocedure. In termsofmalabsorption, it is generally accepted that RYGB compromisesintestinaluptakeofmicronutrients,i.e.cobalamin,vitaminDandiron (46–48). However, the absorption of macronutrients doesnotseemtobeaffectedbytheprocedure(49,50)andtherestric-tivecomponentoftheprocedurealsoseemuncleargiventhefactthat thepouchemptiesalmost instantaneouslyuponmeal inge-stion, even of solid foods (51). Therefore, classifying RYGB as a‘restrictive’ and ‘malabsorptive’ procedure seems inappropriate.Asaforementioned,RYGBimpliesreroutingofnutrientsdowntomoredistalpartsofthesmallintestine,bypassingtheduodenumandupperjejunum,whereby,inparticularsecretionofthegluco-
homeostatic improving and satiety promoting incretin hormoneGLP-1 is enhanced. The bypassed gastrointestinal tract anatomywithitsincreasednutrient-stimulatedGLP-1responsesisthoughttoplayanimportantroleforthehighratesofT2Dremissionandsubstantialweightloss.
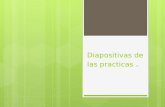
Figure 1.Normal anatomy of the gastrointestinal tract (left pa-nel), and the reconfigured gastrointestinal tract following RYGB(rightpanel).Foodpassesdownthealimentarylimb(redarrows).Digestive juices(containingbileandpancreatic juices)flowdownthebilio-pancreatic limb (greenarrows)andmixupwith food inthe common limb (red and green arrows). Fromwww.codsindia.com.
THEENDOBARRIERGASTROINTESTINALLINERDJBS is a fully reversible procedure developed to treat obesityandT2D(52).ItmimicstheintestinalbypasscomponentofRYGBbypreventingcontactbetweennutrientsand themucosaof theduodenumandproximaljejunum.OpposedtotheinvasivenessoftheRYGB,theDJBSisimplantedbytheuseofanendoscope.Thedeviceisapproximately60cminlengthandconsistsoftwoparts:a self-expanding stent-like proximal anchor made of nitinol (anickelandtitaniumalloy)thatexpandswithintheduodenalbulbupon implantation,anda60cm longsleeveconsistingofan im-permeable, highly flexible material made of fluoropolymer (Te-flon-likematerial).Theentiredeviceispre-packedintoacapsule,whichispositionedattheendofadeliverysystemencompassingaspecialisedcatheterandguidewiresystem.TheDJBSimplanta-tionprocedureisperformedusinganendoscopeandfluoroscopy.Once the subject is sedated (using general anaesthesia or cons-cioussedation(53,54)),anupperendoscopyisperformedtoruleoutpre-existinguppergastrointestinal tractpathology(e.g.ulce-rationsortumours)thatwouldcontraindicateDJBS implantation(Fig.2).Afterwards,thecapsuleis introducedviathemouthandplaced in the pylorus aided by the endoscope. Upon correctlypositioninginthepylorus,asmallnon-traumaticballattheendofthe capsule is pushed out into the duodenum and down to theproximaljejunumviaanover-the-wiresysteminsidethecatheter.Thenon-traumaticballisattachedtothedistalpartofthesleeve,andby pushing theball onwards the sleeve is pulledout of the

DANISH MEDICAL JOURNAL 4
capsule and into the upper small bowel. Fluoroscopy is used tomake sure the ball and sleeve progress unimpededly forward.Whenthesleeveisfoldedoutinfulllengthandtheballdetached,the anchor is pushedout of the capsule into theduodenal bulbwhereit instantaneouslyexpands.Theexpandingfeaturecombi-nedwithsmallbarbsengagingtheintestinalmucosa,ensuresthatthedevicestaysat itscorrectposition.Contrast fluidandairareusedtocheckpatencyofthedeviceaswellascorrectpositioningoftheanchor.Inordertominimisetheriskofpepticulcerforma-tionoruppergastrointestinaltractbleeding,subjectsareprescri-bed prophylactic proton pump inhibitor (PPI) (e.g. pantoprazole40mgtwice-daily)whenthedevice is insitu,andare instructedto continue for until three weeks after explantation. Dietaryrecommendations following device implantation include strictlyliquid foodthe firstweek,andsemisolid foodduring thesecondweek. From the third week and henceforth subjects implantedwith the DJBS are advised to chew food thoroughly, avoiddoughy/sticky/thready foods and drink lots of fluids (water) du-ringmealtimes tominimize the risk of food-induced device ob-struction. Ingested food passes naturally down the oesophagusandintotheventricleandthen-afterhavingpassedthroughthepylorus-enterstheDJBSattheopenproximalend.Itthenflowsdown the lumenof the sleeve inparallelwithbileanddigestivejuices flowing down on the outside between the sleeve and in-testinalwall.Duetothehighlyflexiblesleevematerial,peristalticmovements in the small intestines are capable of propellingnutrientsinsidethesleevefurtherdownthegastrointestinaltract.AtthedistalendoftheDJBSfoodandjuicesadmixanddigestionproceeds.UponDJBSexplantation(afteratreatmentdurationofmaximally12months),theendoscopist(s)usestheendoscopetograsp one of two drawstrings located on the anchor. Before in-troducing the endoscope to the stomach, a customised safetyhood is placed at the tip of the endoscope. When pulling thestring,theanchorcollapses,andtheanchor isretracted intothesafety hood. The entire device is then pulled out of the duode-num, up through the ventricle and oesophagus and out thesubject’s mouth while retracting the endoscope; during the re-tractionmanoeuvertheendoscopist(s)usesfluoroscopytomakesurethatthesafetyhoodencloseseverybarbtoavoiddamageofthestomachandoesophagus.
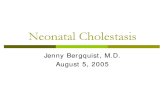
Figure2.SchematicpresentationoftheDJBSimplantationproce-dure.Theprocedurebeginswithanupperendoscopy to ruleout
pre-existinguppergastrointestinal tractpathology (1)before thecapsulecontainingthepre-packedDJBSdeviceispositionedinthepylorus upon DJBS implantation (2). (3) The DJBS (EndoBarrier)correctlypositioned in theupper small intestines. FromGIDyna-micsInc.
INCRETINHORMONEPHYSIOLOGYThe incretin hormones, GIP and GLP-1, are responsible for theincretineffect,whichcontributesimportantlytotheregulationofpostprandial glucose homeostasis (55–58). The incretin effectfollowingoralglucose ingestion isdefinedasthebetacellsecre-tory response evoked by gut derived factors other than glucoseitself, and is the difference in insulin secretion following oralglucose ingestion compared to isoglycaemic intravenous glucoseinfusion (59,60). Inhealthysubjects, the incretineffectaccountsforupto70%ofthetotalamountofinsulinreleasedinresponsetoanoralglucoseload(60).The insulinotropic actions of GIP (a 42-amino acid polypeptide)andGLP-1 (a 30-aminoacidpolypeptide), released fromentero-endocrineKandLcells,respectively,inthepresenceofintralumi-nal nutrients (61), result in an amplification of glucose-inducedinsulin secretion. GIP secreting K cells are mainly distributed inthe epithelium of the proximal small intestine, whereas GLP-1secreting L cells are foundwith increasingdensitydistally in thegastrointestinal tract (61–63). However, the perception of ‘onecell secretes one hormone’ have been questioned recently asstudieshavefoundenteroendocrinecellsco-expressingbothGIPandGLP-1,aswellasotherguthormones (i.e.peptideYY (PYY))(62,64–66).ThepotentiatingeffectsofGIPandGLP-1onglucose-mediated insulin secretion in healthy subjects play an essentialrole in glucose homeostasis - in particular postprandial glucoselevels (61). Additionally, GLP-1 enhances insulin biosynthesis aswellasinsulingenetranscription(67),up-regulatesthegenesforthecellular facilitationof insulinsecretion, includingtheglucoki-nase and GLUT-2 genes (68), stimulates beta cell growth andproliferation, enhances differentiation of new beta cells frompancreaticprogenitorcells,andinhibitsbetacellsapoptosis(69).Furthermore, GLP-1 strongly decreases pancreatic glucagon se-cretion from alpha cells (when glucose levels are above 4-5mmol/L),andthecombinedeffectsoninsulinandglucagonsecre-tionresultininhibitionofhepaticglucoseproduction(70).Lastly,GLP-1 reduces appetite and slowsgastrointestinalmotility - res-trainingpostprandialglucoseexcursionsfurther(62).Oncerelea-sed fromtheirendocrinecell into thecirculation,GLP-1andGIParedegradedbytheenzymedipeptidylpeptidase4(DPP-4).Dueto rapid and extensive degradation (the half-lives of GLP-1 andGIPare~2and5-7minutes, respectively),only10-15%ofnewlysecretedGLP-1reachestheperipheraltargetsasanactivemeta-bolite (62). The insulinotropic actions of GLP-1 and GIP are lostfollowingDPP-4mediateddegradation(62).AsGIPandGLP-1shareseveraleffects(i.e.stimulationofglucose-dependent insulin secretion and beta cell mass maintenance),andhasbeen shown to contributeequally andadditively to theincretin effect (18,71), it remains relatively unclearwhy the hu-manorganism isequippedwith two incretinhormones.Theydo

DANISH MEDICAL JOURNAL 5
differwithregardtosomeeffects,however.Thus, incontrasttothe glucagon-suppressive effect of GLP-1, GIP has in healthysubjectsbeenshowntoincreaseglucagonsecretionduringhypo-glycaemia(72)whichinturnwouldbethoughttostimulatehepa-ticglucoseoutput.Furthermore,duringhyperglycaemiaChristen-sen et al. (72) found no glucagonotropic effects in healthyparticipants but a strong insulinotropic effect. However, it hasbeendemonstratedthatthe insulinotropicpowerofGIP isseve-relycompromisedinpatientswithT2D(73)andthereforeleavesGIP as a primarily glucagonotropic hormone in these subjects.Also, there is growing evidence to suggest that GIP-mediatedeffectsconstituteakeylinkbetweenconsumptionanddepositionoffatandthedevelopmentofobesity,insulinresistanceandT2D(74). Lastly, recent observations byChia et al. (75) suggest thatGIPmay actually worsen postprandial glucose excursions in pe-oplewith T2D. Thus, there seems evidence to support the viewthatGIPperhapsconstitutesa‘diabetogenic’hormoneinpatientswithT2D.
TYPE2DIABETESAsaconsequenceoftheglobal increase inthenumberofobesesubjects, the prevalence of T2D increases correspondingly. Cur-rently, worldwide more than 400 million people have diabetes(76). A genetic predisposition to the disease and, perhaps evenmore importantly, obesity due to imbalance between energyintake and energy expenditure constitute pathogenic factors ofT2D (77). The central pathophysiological features characterisingT2Daredecreasedsensitivity to insulin (and thus impaired insu-lin-mediated glucose uptake in liver and muscles), diminishedbetacell function (andmass), increasedglucagonsecretionbothduring fasting and in response to ameal, and impaired incretineffect (19). The sum of these characteristics results in elevatedfasting blood glucose and exaggerated postprandial glucose ex-cursions. As elevated glucose concentrations increase, risk ofmicrovascular (e.g. nephropathy, neuropathy, retinopathy) andmacrovascularcomplications(e.g.cerebralandmyocardialinfarc-tion) increases,andthekeystone inT2Dtreatment, therefore, isgood glycaemic control along with treatment of T2D-associatedco-morbiditiessuchashypertensionanddyslipidaemia.However,it isunclear towhatextentpharmacological treatmentofT2D isable topreventordelay thecontinueddecline inbetacell func-tionandmass(78).
THEFOREGUTANDHINDGUTHYPOTHESESTwohypotheseshavebeensuggestedtoexplaintherapidRYGB-induced resolution of T2D: thehindgut hypothesis (79), and theforeguthypothesisormorecorrectly,thelowergutandtheupperguthypothesis(80)(Fig.3).Thelowerguthypothesissuggestsanexpedited delivery of ingested nutrients to distal parts of thesmallintestinetoaugmentsecretionoffactorsimprovingglucosemetabolism e.g. GLP-1 (GLP-1 responses have consistently beenfound to be enhanced after RYGB or other surgical proceduresexpediting the transit of ingested nutrients to the lower gut(9,15,81–85)), while the upper gut hypothesis postulates for an
anti-diabeticeffectofRYGB todependonexclusionofnutrientsfrom theduodenumandproximal jejunum (hindering releaseofassumed‘diabetogenicsignals’insusceptibleindividuals-e.g.GIPor glucagon (86)). The role of GIP in the upper gut hypothesisseemssupportedbyreportsofbluntedpostprandialGIPinRYGB-operated patients as opposed to laparoscopic adjustable gastricbanding-operatedpatients (the techniquedoesnotbypasspartsoftheintestines)andoverweightcontrolsubjects,andthatobesepatientswithT2DundergoingRYGBmayexperiencepostoperati-vedeclinesinGIPlevelsparalleledbytheirresolutionofdiabetes(87).Similarly,postprandialGIPconcentrationsdecreaseinobesepatientswithout T2D following surgery,which implies bypass oftheproximalK cell-richpartof the small intestines (88–91).Ho-wever, sinceother studieshave shownpostprandialGIP respon-sestoremainunchanged(14,15)orevenincrease(81,92)theroleofGIPintheupperguthypothesismaynotbethatapparent.It can be speculated, that RYGB-mediated circumvention of theuppergutcanleadtonon-releaseofahithertounknowndiabeto-genic signal (86). This, in combination with increased nutrientdeliverytothelowergutandconcomitantenhancedsecretionofGLP-1andperhapsotherunidentifiedantidiabetic factors,mightcontributetosomeoftheendocrinechanges leadingtothestri-kingproportionofpatientsbeing‘cured’forT2DafterRYGB(Fig. 3). Simultaneous to enhanced GLP-1 levels, levels of theanorectic hormone PYY, which is also secreted from the L cells(93) also increase after surgery (15,82). Along with reports ofdiminished levelsof theorexigenichormoneghrelin (15,94), thethree hormones may impair feelings of hunger sufficiently tofacilitate the substantial weight losses that would furthermoreimproveglucosemetabolism.Nevertheless, regardlessofalteredsecretionofseveralguthormones followingRYGB, it seemsthatespeciallytheincrementsinGLP-1secretionareimportantforthepositiveeffectofRYGBonT2D(95).
Figure 3. Normal gastrointestinal anatomy (left) and gastroin-testinal ‘architecture’afterRYGB (right).The lowergut (hindgut)hypothesisproposesthatantidiabeticsignalling(e.g.GLP-1secre-tion) from the distal part of the small intestine is potentiatedfollowing RYGB, which expedites the transit of nutrients to the

DANISH MEDICAL JOURNAL 6
lowergutwhereGLP-1secretingLcellsareabundant.Theuppergut(foregut)hypothesispostulatesthatuponover-stimulationoftheproximalpartofthesmallintestineswithnutrientsinsuscep-tible individuals, it releases a diabetogenic signal (perhaps GIPfrom the K cells found in high numbers in the duodenum andproximal jejunum and/or currently unknown diabetogenic fac-tors).Theupperguthypothesisemphasises that followingRYGB,diabetogenicsignallingisavoided.
BILEACIDSANDGLP-1Bileconsistsofwater,electrolytes(primarilysodium,chlorideandbicarbonate),bilirubin,phospholipids,fattyacids,cholesterolandbileacids.Stimulatedbysecretin,bileisactivelysecretedintothebile canaliculi by hepatocytes along with a watery bicarbonate-richfluidfromintraandextrahepaticbileducts.Bileflowsdownthebileductsandaccumulatesinthecommonhepaticductbefo-re entering the duodenum via ductus choledocus. In betweenmeals, half of the bile is diverted to the gallbladder where bileacids concentrate 10 to 20-fold due to reabsorption of sodiumchloride and bicarbonate; the rest flows to the intestines (96).Nutrients,especiallyproteinand lipids (97–99),elicitcontractionof the gallbladder and release of bile aftermeal ingestion. Thismechanism is partlymediated via CCK secreted from enteroen-docrine I cells in the duodenum and jejunum (100). Aside fromgallbladder contraction,which is known tobe correlated toCCKconcentration in plasma (101), CCK induces relaxation of thesmooth muscles in the common bile duct. Furthermore, CCKrelaxes the sphincterofOddi.Theseactionscombinedejectbilefrom the gallbladder. Additionally, CCK stimulates exocrine pan-creaticsecretionimportantfordigestionofcarbohydrate,proteinand lipids (102). Thehepatic synthesisofbile acids representsahighly complex process comprising numerous enzymatic proces-sesinitiatedbyconvertingcholesterol intotheprimarybileacidscholic acid (CA) and chenodeoxycholic acid (CDCA). The rate-limitingstep inbileacidsynthesis ishydroxylationof thecarbonat position number seven in the cholesterol molecule by 7α-hydroxylase.Hepatocytesreleasebileacidsasconjugatedprimarybile acids. In the intestine, primary bile acids are either activelyabsorbed in the terminal ileum via the apical sodium bile salttransporter (ASBT) on the enterocytes or passively throughoutthe entire small and large intestines (103,104). In total, 95% ofbile acids are absorbed and returned to the liver through theportal circulation - known as the enterohepatic circulation. Theremainingbileacidsareexcretedthroughfaeces.Bileacidsregu-latetheirownsynthesisbynegativefeedbackmechanisms.Post-prandially, the (re)uptake of bile acids via ASBT (105) stimulatethenuclearreceptorfarnesoid-X-receptor(FXR)withintheenter-ocytes. Following FXR activation transcription of the hormonefibroblastgrowthfactor19(FGF19)geneisenhanced(106).Rele-asedfromtheenterocytes,FGF19hastwodistincteffects.Firstly,itbindstothereceptorcomplexFGFR4/β-klothoonthehepatocy-terepressingtranscriptionofthe7α-hydroxylase-gene(105–107).Secondarily, FGF19 induces refilling of the gallbladder with bileacids.Additionally, adiminishedcholesterol formationby inhibi-ting 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reduc-
tase activity has been reported and further, bile acid-inducedFGF19secretionfromenterocytesseemtosuppressexpressionofASBT, thus inhibiting active ileal and hepatic bile acid reuptake(108).Bilefacilitateslipiddigestionmediatedbythemicelleformingbileacids.However,bileacidshaverecentlybeenproposedtoactasalink in the integration of food intake, glucose metabolism andenergyexpenditure.Watanabeetal.(109)showedthatbileacid-induced TGR5 activation mediated deiodination of the inactivethyroid hormone thyroxine (T4) to active triiodothyronine (T3),which caused energy expenditure to increase in brown adiposetissue. In terms of glucose metabolism, a FXR-FGF19 pathwayseemstobeinvolved,asFXRknock-outmiceareinsulinresistant(110,111) and FGF19 activates glycogen synthase and inhibitsgluconeogenesis (112). Additionally, bile acids are capable ofinducing another gluco-regulatory mechanism. Cell and murinestudieshave shown thatbileacids stimulateGLP-1 release fromenteroendocrine L cells via activation of TGR5 (24–26). Humanstudies have confirmed these pre-clinical reports (27–29) andfoundincreasedGLP-1concentrationsfollowingeitherrectal(28)or oral (31) administration of bile acids. In addition to TGR5-mediated GLP-1 release, a recent study in mice reported theexistenceanFXR-GLP-1pathwayasGLP-1secretionwasattenua-tedfollowingbileacid-inducedFXRactivationinLcells(38).Theseresultsemphasisethatbileacidsarenotsolelyfatemulsifiers,butconstitute a link between bile and energy expenditure andmayplayan importantrole inglucosemetabolismmediatedbyTGR5andFXRactivationintheintestinalLcells(113).
METFORMINANDGLP-1Metformin,abiguanidederivative,hasbeenknownandusedasan antidiabetic drug formore than 50 years. In parallel with li-festylemodifications, metformin is the first-in-line drug for tre-atmentofT2D(114).Metforminiseffectivewithregardtoglyca-emiccontrol,atleastinitially,ithasagoodsafetyprofileanditisconsideredweightneutral.Additionally,theclinicalexperienceisextensive; it does not increase the risk of hypoglycaemia and isinexpensive. Aside from metformin’s antidiabetic actions, datahave shown that it also exerts cardio-protective (115) and anti-inflammatory (116) actions, and even reduces the risk of somecancers(117–120).Itisgenerallyacceptedthattheliverisamainsiteofactionformetformin.Viatheorganiccationtransporter-1(OCT-1) metformin enters the hepatocytes and directly inhibitsthe mitochondrial respiratory chain (complex 1). As aconsequence, energy production (adenosine triphosphate (ATP)production via Kreb’s cycle) declines leading to elevated intra-cellular adenosinemonophosphate (AMP) concentrations in thehepatocyte.IncreasedAMPdiminishesadenylatecyclaseconver-sionofATPtocyclicAMP(cAMP),whichdecreasesproteinkinaseA (PKA) activity, which, in turn, diminishes expression of gluco-neogenetic enzymes. Additionally, increased intracellular AMPinhibits fructose-1,6-biphosphatase, a keygluconeogeneticenzy-me,andincreasesAMPkinase(AMPK)activityinhibitinglipidandcholesterol synthesis (121). The sum of these actions is a net

DANISH MEDICAL JOURNAL 7
reduction inhepaticglucoseproductionanda reductionofplas-ma glucose. OCT-1 seems crucial for the actions of metformin.Shuetal.(122)demonstratedthatOCT-1knock-outmicerespondpoorly tometformin.Complex1maynotbe theonly siteofac-tionformetformin.Uponbindingtoitsreceptoronthehepatocy-te, glucagon stimulates cAMP formation fromATP via adenylatecyclase, and increaseshepatic glucoseoutput (123). cAMP is, asdescribedearlier,vitalforfurtherPKAactivityandthusgluconeo-genesis. In a gain and loss-of-function study,Miller et al. (124)reportedhowbiguanidesseemtoantagoniseglucagon-mediatedcAMP formation, thus inhibiting hepatic glucose production,supportinganother(yetstillhepatic)molecularactionofmetfor-min.Even though, the liver is thought tobe it’smain siteofac-tion,increasedglucosedisposalhasalsobeensuggestedtocont-ributetotheglucose-loweringeffectofmetformin;thus,both invitroandinvivostudiesreportedincreasedglucoseuptake(125–127) and glucose utilisation in skeletalmuscles (128) aftermet-formin administration.Duca et al. (129) recently proposed thathepatic glucose output was not only dependent on metformin-induced hepatic AMPK activity. In a murine setting, the resear-chersreportedincreasedduodenalAMPKactivityinparallelwitha decreased hepatic glucose production following intraduodenalbolus administration of metformin in insulin resistant rats.Furthermore, subsequent duodenal AMPK inhibition abated thediminished metformin-induced hepatic glucose output. GLP-1seemed to be the link underlying this action via an intestinalAMPK-GLP-1-PKA pathway stimulating neural activity, whicheventuallycausedthereductioninhepaticglucoseoutput.Howe-ver, the importanceofduodenalAMPKactivityandextrahepaticglucose uptake in addition tometformin’s direct hepatic actionremainsunclear.Metformin has also been shown to enhance endogenous GLP-1secretion(34,130,131)andseveralhumanstudiesinpatientswithT2D(e.g.Scarpelloetal. (39)andNapolitanoetal. (34))showedthatorallyadministratedmetforminincreasedfaecalexcretionofbile acids and decreased serumbile acid concentrations. Intere-stingly, in an in vitro study several years earlier, Caspary andCreutzfeldt observed that biguanides inhibited conjugated bileacidabsorption(37).Asaforementioned,bileacidsarecapableofinducingGLP-1 secretion through TGR5 and FXR interaction in Lcells (25–29,31). Therefore, itmay be thatmetformin’s capacityto increase intestinal content of bile acids may induce GLP-1secretion via the L cell and the two receptors TGR5 and FXR.However, otherGLP-1 secretingmechanismsofmetforminhavebeenpostulated.Inaninvitrostudyusingmurineenteroendocri-necells,chronicmetforminadministrationwasfoundtoprotectLcells from lipid-induced apoptosis thereby increasingGLP-1 syn-thesis (132).Additionally, it isspeculatedthatmetformin increa-ses GLP-1 secretion via parasympathetic nervous activity (133)and that metformin prolongs the half-life of GLP-1 by DPP-4-independent mechanisms (33,134). Furthermore, it has beenhypothesised that metformin alters gut microbiota compositionwhich in turn might foster formation of specific bile acids withGLP-1secretingfeatures(25,29).
Despite several hypotheses on metformin’s GLP-1 enhancingproperty, thebileacidmediatedpathwayseemsmostattractiveasmetforminreducesilealbileacidreabsorption,whichhasbeenfound to increaseGLP-1viaTGR5activationanddiminishedFXRactivityintheLcell.Thismayrepresentanimportantextrahepa-ticmodeofactionformetformin.
HYPOTHESISANDOBJECTIVESSince the current thoughts regarding the effects of theDJBS onweight loss and glycaemic regulation stem from a few rathersmall studies, we decided to retrieve and systematically reviewcurrentevidenceandperformmeta-analysis inordertoevaluatethe clinical effects and safety of the DJBS for the treatment ofobesity and T2D (study I and study II). We hypothesised that;collectingandanalysing study resultsaccording toapre-definedprotocolwouldobjectifyDJBS’effectsinanunbiasedmannerandtherebyhelpguideclinicaldecision-making,whichmightresultinbetterobesityandT2Dtreatment.Mainobjectiveswerechangesin body weight, changes in HbA1c and safety. The objective ofstudy IIIwastomaptheendocrine impactofDJBSandevaluatethe‘acute’(1week)and‘long-term’(26weeks)effectsonglucosehomeostasis in obese subjects with normal glucose tolerance(NGT)andobesepatientswithT2D.WeinvestigatedtheinfluenceofDJBSonfastingplasma/serumconcentrationsandpostprandialplasma/serumresponsesofGIP,GLP-1,PYY,CCK,gastrin,insulin,C-peptideandglucagon.Furthermore,weaimedtoassesssensa-tionsofappetiteandsatietyandregisteredfoodintake.Wehypo-thesised, in line with the upper gut and lower gut hypotheses,thatDJBSwouldcausechangesinpostprandialsecretionofincre-tin hormones favouring secretion of insulin and inhibition ofglucagonfromthepancreaticislets,which,inturn,wouldgiveriseto an improvement in postprandial glucose metabolism. More-over, we speculated that DJBS would increase the secretion ofsatietyhormones(e.g.GLP-1andPYY)and,consequently,increa-se sensationof satietyand thusdiminish food intake. Lastly,wemonitored the effect on weight loss and the safety of DJBS. InstudyIV,weaimedtoelucidatetheroleofgallbladderemptyingandmetforminonhumanGLP-1-secretion.WehypothesisedthatCCK-inducedgallbladderemptyingwouldelicitaGLP-1response.Furthermore, we speculated that metformin administrationwouldinhibitbileacidreuptakefromthesmallintestines,interactwith TGR5/FXR in enteroendocrine L cells and, thus, potentiatethe GLP-1 response mediated by CCK-induced gallbladder em-ptying.
SUMMARYOFSTUDIESStudyIandIIInstudyIIwecollecteddataontheDJBSinordertoinvestigateitsclinicalefficacyandsafetyinobesityandT2Dtreatment.Basedonapreviouslypreparedprotocol(studyI)weundertookasystema-tic review with meta-analyses of eligible trials according to thePreferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (135) and the CochraneHandbook for Syste-matic Reviews of Interventions (136). We searched for human

DANISH MEDICAL JOURNAL 8
trials reporting weight loss and glycaemic improvements. Giventhe novelty of DJBS, we expected rather few publications, andtherefore includedall typesofpublications (e.g. full textarticlesand abstracts), irrespective of language, and included bothrandomised controlled trials (RCT) and observational studies inorder to increase amountof data forour analyses. If necessary,corresponding authors were contacted for further information.Primaryendpointswereweight loss,changeinHbA1candsafety.Secondary endpoints encompassed proportion of patients withT2Dreducingordiscontinuingantidiabeticmedication,changesinfastingplasmaglucoseandchangesincholesterollevels.Randomand fixed effects meta-analyses were performed and resultsdisplayedasmeandifferences(MD).Intertrialheterogeneitywasassessedby I2 statistics (anumberbetween0 to100%).Hetero-geneityinincludedstudieswasclassifiedas:mightnotbeimpor-tant (I2 0-40%), may represent moderate heterogeneity (I2 30-60%), may represent substantial heterogeneity (I2 50-90%) andconsiderableheterogeneity(I275-100%).FiveRCTs(n=235subjects)andtenobservationalstudies(n=211)were included. All studies had high risk of bias in at least onedomain (e.g. allocation concealment or blinding of participantsandpersonnel).IntheRCTs,subjectswereallocatedtotheinter-vention group (DJBS + diet or lifestyle modifications, n=136) orthe control group (sham + diet/lifestyle modifications ordiet/lifestylemodificationsalone,n=99).Theobservationalstudi-esreportedtheeffectoftheDJBSalone,orcombinedwithdietorlifestylemodifications. In total,20subjectscouldnotbe implan-tedwith the DJBS due to anatomical difficulties (i.e. short duo-denalbulb).Medianfollow-upwas12and52weeksforRCTsandobservational studies, respectively. Overall, the subjects had aBMIrangingfrom30.0to49.2kg/m2and10-100%hadT2D.Me-ta-analyses showed thatDJBS lead toanadditionalbodyweightloss and excess weight loss of -5.1 kg and 12.6%, respectively,comparedtodietorlifestylemodifications.Furthermore, inpati-entswithT2D,meta-analysesfoundnoadditionaldeclineinHbA1cor fasting plasma glucose. In general, patientswith T2D treatedwith antidiabeticmedication whowere allocated to DJBS treat-mentwerenotreducingordiscontinuingantidiabeticmedication.Adverse events consisted mainly of dyspepsia, and 66 subjectshadtheDJBSremovedearlierthanplannedduetotheoccurrenceofaseriousadverseevent(e.g.gastrointestinalbleedingordevicemigration). No liver abscesses or deaths occurred. Cholesteroldatawerescarceanddidnotallowmeta-analysisasonlyoneRCTreportedthisoutcome.WeconcludedthatDJBStreatmentledtoamoderateweightlossinobesesubjectscomparedtodietand/orlifestylemodifications,andhadnosubstantialimpactonglycaemiccontrol.Theinciden-ceofadverseeventswashigh,butthesymptomswereingeneralmildand transientandoccurredwithin the firstweeksafter im-plantation.Nearly20%discontinuedDJBStreatmentearly.Giventheseresults,weinferredthatfurtherresearchseemednecessaryinordertoevaluatetheapplicabilityofDJBSinclinicalpractice.
StudyIIIWeaimedatdescribingDJBS’ impactonpostprandialphysiologyalongwith registration of its clinical effects. In a 26-week openobservationalprospectivestudy,tenNGTobesesubjectsandnineage,bodyweightandBMI-matchedpatientswithT2DimplantedwiththeDJBS(Table1)werestudiedpriortoimplantation(base-line), oneweek (1w) after implantation and following 26weeks(26w)ofDJBStreatment.Accordingtostudyprotocoland,giventhattheDJBSwaswelltoleratedandtheparticipantsconsented,theimplantationperiodwasextendedbyanadditional26weeks.Study III reports the results of the first 26-week period. At thebaseline,1wand26wstudydays,eachsubjectunderwentastan-dardised525kilocalories(kcal) liquidmixedmealtestandasub-sequent ad libitum meal test.Wemeasured fasting and 4-hourpostprandialplasmaconcentrationsofglucose,aswellaspancre-atic and gut hormones. Additionally, appetite, food intake, gall-bladder emptying and resting energy expenditure were evalua-ted.Gastricemptyingrateswereassessedusingtheparacetamolmethod (137). Furthermore, the participants consulted a studynurse once amonthwhere anthropometricmeasurements (e.g.body weight) and type of adverse events were registered. Atbaselineandat26w,totalandvisceralfatmassesweremeasuredbyDualEnergyX-rayAbsorptiometry.During 26 weeks, obese NGT subjects and obese patients withT2D, respectively, lost amedian (range)of 6.8 (2.5-16.1) kg and6.2(0.7-11.0)kg,whichwereaccompaniedbysignificantreducti-ons in total and visceral fatmasses.Onall three studydays, fa-stingplasmaglucosewassignificantlyhigherinpatientswithT2Dcompared toNGT subjects.Otherwise, fastingNGT subjects andpatientswithT2Dhadsimilarconcentrationsofinsulin,C-peptide,glucagon, GIP, GLP-1, PYY, CCK and gastrin. Noteworthy, fastingplasma gastrin concentrations in both groups of participantstended to increase throughout the 26-week study period, likelydue to theprophylactic PPI treatment. PostprandialGIP respon-ses were unaffected by DJBS in patients with T2D, but we sawattenuated 0-60 minutes postprandial plasma GIP responses inNGTsubjectsat1wand26wcomparedtobaseline.Additionally,postprandial levels of GLP-1 and PYY increased one week afterDJBS implantation in patientswith T2D.GLP-1 increased furtherat26w,butPYYconcentrationsremainedstable(andequalto1w)at26w.IntheNGTsubjects,postprandialconcentrationsofGLP-1andPYYweresimilaratbaseline,1wand26w.Postprandialglu-cose, insulin, C-peptide, glucagon, CCK and gastrin responsesweresimilarandunaffectedbyDJBS inbothgroups.Satietyandfullness sensations were significantly stronger and food intakereducedat1winNGTsubjects,butreturnedtobaselinelevelsat26w; similar trends in appetite sensations or food intakeswereobserved in the T2D group. DJBS did not effect gallbladder em-ptyingor gastric emptying.Adverse events consistedofmild-to-moderate dyspepsia. However, due to serious adverse events,five devices (21%) were removed earlier than planned due tointolerablerecurrentabdominalpain(n=4)andonecaseofdeviceobstructioncausedbysleeveinvagination(138).

DANISH MEDICAL JOURNAL 9
In conclusion, 26 weeks of DJBS treatment resulted in modestweightlossesinobeseindividualswithandwithoutdiabetes.Theonlymarginalalterationsinpostprandialphysiology(e.g.GIPandGLP-1secretion)inducedbyDJBS,mightexplaintheabsenteffectonpostprandialglucosemetabolisminourpatientswithT2D.
Table1.Subjectcharacteristics
NGT T2D
n(male) 10(4) 9(4)
Age(years) 49(27-60) 50(40-67)
Weight(kg) 101.1(89.0-117.2) 103.7(80.9-131.9)
BMI(kg/m2) 34.3(30.3-36.8) 38.6(31.6-40.5)
HbA1c(mmol/mol)
31(25-43) 50(32-77)*
Fastingplasmaglucose(mmol/L)
5.4(5.2-6.5) 8.7(7.0-16.1)*
DurationofT2D(months)
NA 36(16-81)
Median(ranges),*P<0.05
StudyIVIn study IV we investigated the role of gallbladder emptying,single-dose metformin, and the combination, on human GLP-1secretion. On four separate days, ten young healthy lean maleNGTsubjectswithnofamilyhistoryofdiabeteswerestudied.Inadouble-blinded fashion and in a randomised order, the partici-pants were subjected to metformin or placebo at time point 0(instilled in the stomachviaanasogastric tube), anda concomi-tant 60-minute intravenous infusion of saline or CCK (0.4pmol/kg/min).Bloodwassubsequentlysampledforfourhourstoevaluatepostprandialresponsesofglucose,aswellaspancreaticandguthormoneresponses.Additionally,gallbladdervolumewasmeasuredusingbedsideultrasonography.CCK-inducedgallbladderemptyingandmetforminadministration,respectively, elicited significantGLP-1 responses. In addition, anadditive effect was seen when combining metformin with CCK-inducedgallbladderemptying.Metforminaloneorcombinedwithgallbladderemptyingaugmented thePYY responses.GallbladderemptyingaloneincreasedPYYresponsestoo,howevernotsignifi-cantly.Ashort-lasting(0-60min)increaseinGIP, independentofmetformin, was seen following gallbladder emptying. The sametrendwasseenwithregardstoglucagonsecretion.CCKinfusionsmediatedan immediate gallbladder contractionanda rapid andmajordecreaseingallbladdervolume.Gallbladdervolumeincrea-sed after CCK-infusions had terminated. Gallbladder volumeremained unaffected by metformin. No effects were seen onglucose, insulin, C-peptide or gastrin concentrations, and gastric
emptyingrates,assessedbytheparacetamolmethod(137),werenotdelayed.We concluded that CCK-induced gallbladder emptying elicitssignificantGLP-1secretion,whichwaspotentiatedbysingle-dosemetformin. Further,we found increased PYY andGIP responsesfollowing gallbladder emptying. It made us speculate, that gall-bladderemptyingandsubsequentTGR5stimulationbybileacidselicitedGLP-1,PYYandGIPsecretion,andsecondly,thatmetfor-min’s mode of action seems to encompass both bile acid-dependent and independent stimulation of gastrointestinal hor-monesecretion.
DISCUSSIONThe studies in this thesis provide evidence on the efficacy andsafetyofanovelendoscopictreatmentmodality,theDJBS,basedon a protocol-based systematic review with meta-analyses ofexistingdata,andanewobservationalclinicalstudy.Additionally,we provide newdata characterising the postprandial physiology(including gut hormone secretion) following DJBS treatment.Furthermore,weshowedhowgallbladderemptyingandmetfor-min,eitheraloneorcombined,enhanceshumanGLP-1secretion.SincethefirsthumanstudiesreportedontheeffectoftheDJBS,severalreviewshavebeenconducted(139–144). In linewiththeonly other systematic review (byZechmeister-Koch et al. (145)),our results from study II showed that DJBS treatment entailssignificant,yetmoderate,weightlossesinobesesubjectsaccom-paniedbyminorimprovementsinglycaemiccontrolamongobesepatients with T2D. Given the novel nature of the DJBS, theamountofevidence isnotascomprehensiveasbariatricsurgery(e.g.RYGB).Resultsandimpactofmeta-analysesrelyonnumberandqualityofstudies.Thisfactinevitablyinfluencesourfindings.Indeed, the low number of rather small sized RCTs (with highdropoutrates)providingthebasisofouranalysesdefinitelylimitthevalidityofourresults.Furthermore,allstudieshadbiasissuesandmoderate-to-considerable intertrial heterogeneity. In additi-on,wefoundfunnelplotasymmetryinourprimaryendpointsofweight loss,as thenumberofeligible trialswas low (orperhapsduetoreportingbias).Theselimitationscompromisedthequalityofourmeta-analysisandcouldpotentiallyoverestimateresults.Conventionalbariatricsurgery(e.g.RYGB)havereportedimpres-siveweightlosses(7)andremissionratesofT2D(146).Incontrasttobariatric surgery, and in linewithourmeta-analysis (study II)(147),wedidnot seeany improvements in glycaemic control inour own observational study (study III), andweight losseswereonlymoderate.However,intermsofweightloss,ourparticipantsshowed great individual variances. Accordingly, some publishedstudies reported excess weight losses comparable to the onesachieved by RYGB (148). RYGB is known to induce long-termweight losses, but so far only one study reported long-termweightlossdataafterterminationofDJBStreatment.Koehestanieetal.(23)followedsubjectstreatedwiththeDJBSforanadditio-nalsixmonthsafterdeviceexplantation.TheirdatashowedthatDJBS (+diet) versusdiet alone induceda 10.6 and5.3 kgweightloss, respectively. Despite both groups regaining weight, the

DANISH MEDICAL JOURNAL 10
weightlosswasstilllowerintheDJBSgroupcomparedtothedietgroup.However,sincetheseresultswerebasedonfewobserva-tionstheyshouldbeinterpretedcautiously.ThemoderateclinicaleffectsmediatedbyDJBStreatment(studyIII) could be explained by the small changes in postprandial guthormone secretion. Since DJBS is designed tomimic the bypasscomponent of a RYGB, expediting undigested nutrients to thelowergut,enhancedreleaseofantidiabeticand/orsatietypromo-ting gut hormones (e.g. GLP-1 and PYY) would theoretically beexpected.DJBSledtosmall incrementsofGLP-1andPYYinpati-entswithT2D.Despitebeingsignificant,peakGLP-1plasmacon-centrationwas onlymodestly increased by two-fold as opposedtothe~10-to-20-foldincreaseseenshortlyafterRYGB(14,15,85).Since GLP-1 exerts powerful insulinotropic and glucagonostaticeffects(62),weexpectedincreasedinsulinsecretionanddiminis-hedglucagonrelease.Additionally,asaconsequenceofduodenalexclusionbyDJBS,GIPlevelswouldbeexpectedtofallinlinewiththeupperguthypothesis.InNGTsubjects(notpatientswithT2D)GIP responses displayed a 0-60 minute decline after one weekand26weeksoftreatment.Opposedtoitssisterincretinhormo-ne,GIPstimulatesglucagonsecretionfromthealphacells.There-fore, increasedGLP-1anddiminishedGIPcouldact inconcerttolower postprandial plasma glucose values via increased insulinand diminished concentrations of glucagon. However, this wasnot thepicture.de Jongeetal. (22) foundgreater impactof theDJBS in their 17 obese patientswith T2D. In contrast to our re-sults, they saw improvedglycaemic control inparallelwithatte-nuatedGIP and glucagon responses, aswell as enhancedGLP-1secretion,but inconsistencywithourresults, insulin levelswerenotaffected.Asglucagonpromoteshepaticglucoseoutput(149)deJongeandco-authorsspeculatedthatimprovedfastingplasmaglucoseandpostprandialglucoseexcursionswereduetodecrea-sedendogenous(hepatic)glucoseproduction.GLP-1,PYYandCCKareconsideredanorectichormones(15,101).We quantified food intake and qualified satiety sensation insubjectsimplantedwiththeDJBS.ObeseNGTsubjectsfeltsignifi-cantly stronger satiety, greater fullness and reported smallerprospective food consumption. The sum of these sensationsresultedinareducedcaloricintakeshortlyafterDJBSimplantati-on.However, the sensation abated at the 26thweek, as did thereductioninfoodintake.Thealterationsinpostprandialguthor-monalreleasesfollowingDJBStreatmentmayrepresentthemainexplanationforthetransientappetiteandfoodintakereduction,and thus weight loss. Without doubt, nausea (a frequent andtransientadverseeventofDJBS)couldaffectfoodintake.Howe-ver,sensationofnauseawasunchanged,perhapsrulingthisout.Energy expenditure following RYGB remains controversial asstudies have shown divergent results (150). However, if DJBSwereto increaseenergyexpenditure,asFariaetal. (151)repor-tedfollowingRYGB,thismightcontributetoourobservedweightlosses.Nevertheless,asrestingenergyexpenditurewassimilaronthe three study days, changes in resting energy expenditure donot seem to influence body weight in DJBS treated obesesubjects.
Aside from inducing satiety, CCK elicits gallbladder contraction(101).AswithGIP,completeduodenalexclusionwouldtheoreti-callyhindernutrientstimulationofandreleaseofCCKfromIcells.Wedidnotconfirmthishypothesis. In linewiththe inconclusivechanges in CCK secretion following RYGB (15,87,152,153), andcompared to the opposing results byde Jonge et al. (154)whofound decreased CCK concentrations, the effect of DJBS on CCKsecretion remains unclear. Given that CCK was unaltered, onecould question whether the DJBS is capable of fully preventingnutrients from contact with the mucosa of the duodenum andproximal jejunum. If the anchorwere not fully expandedwithinthe duodenal bulb, nutrients would unimpededly flow on theoutsideofthesleeve,mediatingCCKrelease.IftheDJBSisindeedtightly fitting within the intestines and thereby fully prevents‘nutrient leak’ on the outside of the sleeve, the abundance of Icells in the distal part of the jejunum (155) could explain theunalteredCCKconcentrations.InstudyIII,weexperiencedthesamerateofearlyDJBSexplanta-tion (approximately 20%) as reported in our systematic review(study II).Additionally,weobserved the same typeofdyspepticadverse events as well as their duration compared to previousDJBSstudies.Themostseriousadverseeventwasdeviceobstruc-tion due to sleeve invagination (138).We did not see any liverabscesses,whichhavebeenreportedrecently(156)andleadtheFood andDrug Administration to terminate theUSmulti-centreENDOTrialprematurely(obesepatientswithT2Drandomisedtoeither DJBS or sham (157)) as the occurrence of liver abscesses(3.5%)exceededapre-definedsafetythresholdof2%(158).InstudyIV,weobservedincreasedandadditiveGLP-1responsesin healthy male subjects, mediated by CCK-induced gallbladderemptyingandmetformin.Previously,effortshavebeenmade toinvestigate the impact of gallbladder emptying and subsequentreleaseofbileacidsintotheintestinesonGLP-1secretion.Ahrénet al. (159) infused saline and CCK in two matched groups ofpostmenopausalwomenandfoundinsignificanteffectsofCCKonpostprandial GLP-1 secretion compared to saline. As they, inparallel to the infusions, administered a mixedmeal containingenoughfattoelicitcompletegallbladdercontractioninitself,theeffectof gallbladderemptyingper seonGLP-1 secretion cannotbederivedfromthisstudy.AdirecteffectofCCKonGLP-1secre-tionfromenteroendocrineLcellsshouldbeconsidered.However,several studies have shown that infusion of CCK-8 in isolatedperfused rat ileum and colon had no effect on GLP-1 secretion(160–163).HansenandHolst(164)investigatedtheeffectofCCK-8 onGLP-1 secretion in a setup using an isolated porcine ileumandfoundthatonlyhighconcentrationsofCCK-8(100–500timesnormalpostprandiallevels)wasabletostimulateGLP-1secretionslightly. Based on these studies, it seems improbable that thedoseofCCK-8usedinourstudy(leadingtoslightlysupraphysiolo-gical CCK concentrations) induced significant GLP-1 secretion.UtilisingCCKreceptorantagonismcouldshedlightonthequesti-onofwhetherCCKhasadirecteffectonGLP-1secretion.Howe-ver, several considerations need to be taken into accountwheninterpretingsuchstudies.InvivoadministrationoftheCCKrecep-

DANISH MEDICAL JOURNAL 11
torantagonistloxiglumidewouldantagoniseCCK-reducedgastricemptying. As the rate of gastric emptying is essential for post-prandial GLP-1 secretion (62), the accelerated gastric emptyingelicitedbyCCKreceptorantagonismmayexplainwhyloxiglumidewasshowntoreduceoleate-inducedGLP-1response(165).Ano-therexplanation couldbe that aCCK receptor antagonistwouldinhibit pancreatic exocrine secretion, causing less intraduodenallipase to enzymatically cleaving triglycerides (oleate) into 2-monoacylglycerol, which appears to be responsible for lipid-induced GLP-1-secretion. Furthermore, the intact GLP-1 respon-sesobservedbyBeglingeretal.(165)werequitesmall(between1 and 4 pmol/L) and actually below the detection limit of theassay raising doubt about the validity of the result. Given theabove,itseemsunlikelythatCCKdirectlyelicitsGLP-1secretion.As metformin consistently has been shown to increase faecalcontent of bile acids (34,39), our metformin-induced GLP-1 re-sponsesmaywell be in linewith the hypotheses that increasedintraluminal concentrationsofbileacidsdue tometformin, acti-vatesbothTGR5andFXRreceptors.ThedelayedresponsesofPYY,oftenconsideredtobeco-secretedwithGLP-1fromtheLcells,couldbeexplainedbystudiesreport-ingtheexistenceofproximalGLP-1-secretingcellsanddistalGLP-1/PYY-secretingenteroendocrinecells (64,65)andperhapsdistalcellssecretingPYYalone.Furthermore,asChoetal.(64)pointedtowardstheexistenceofenteroendocrinecellsub-typessecretingbothGLP-1andGIPthiswould,inlinewiththeexistenceofother‘dual-secreting’ enteroendocrine cell sub-types (e.g. distal GLP-1+PYY),representaplausibleexplanationtoourGIPfindings.
STUDYLIMITATIONSIn study II,wewere limitedby a lownumberof availableRCTs,probably due to the novelty of DJBS as an obesity and/or T2Dtreatment. Therefore, we were not able to perform meta-regression analysis or evaluate other dichotomous outcomes.However,we still believe that itwas important to conducta sy-stematic review (with meta-analyses) in order to objectify theadvantages anddisadvantages of theDJBS.Additionally, despitesubstantial efforts to contact corresponding authors, only a fewresponded. Of these only one gave us access to additional rawand unpublished data, the rest merely confirmed accuracy ofreportedresults.Weconductedanobservationalprospectivestudy.Itwouldhavebeen a stronger design if the study had been a double-blindedsham-controlledrandomisedstudy.Nevertheless,wehadtotakeethical considerations into account. For instance, as the DJBSpreviously has been shown to induceweight loss, itmay be ar-gued that a sham-arm involving anaesthesia and endoscopicprocedures similar to DJBS implantation could be problematicfrom an ethical perspective. Circumventing this ethical issuecould,tosomeextend,bedonebyincludingadiet/lifestylemodi-ficationarmorperhapsanarmtreatedwithGLP-1receptorana-logues.Moreover,intermsofmaximisingweightloss,onemightargue that a low-caloric diet should have been combined withDJBS.However,asdietsarenotoriouslydifficult tomaintainand
have not proven effective in long-term weight loss, we believethatthepresentstudydesignallowforabetterdescriptionoftheeffect of DJBS per se. Additionally, the patients with T2D wereratherheterogeneousintermsofglycaemiccontrol,andfurther-morewewouldhave likedthediabeticpatientstobemoredys-regulated.However,therelativelyextensivelistofcontraindicati-ons for DJBS implantation (e.g. ischaemic heart disease,anticoagulant therapy, history of coagulopathy, bleeding diathe-sis, inability todiscontinueuseof non-steroid anti-inflammatorydrugs,knownpresenceofgallstones,pancreatitis)hamperedtheplannedrateofrecruitment.
CONCLUSIONSInourprotocol-based systematic reviewwithmeta-analyses,weshowthatDJBScomparedtodietorlifestylemodificationsresultsin significantbutmoderateweight reductions inobese subjects.Unexpectedly, the data also showed that DJBS did not improveglycaemiccontrolinpatientswithT2D.Despitethefactthatmostadverseeventsweretransientandmild-to-moderateofnature,arelativelyhigh rateof earlyDJBS removalswasobserved. Inourownhands,a26-weekperiodofDJBStreatmentresultedinsimi-lar modest weight losses along with small gastrointestinal tracthormone responses in obese NGT subjects and obese patientswith T2D. However, in spite of the preconditions being present(i.e. weight loss and enhanced GLP-1 secretion), DJBS did notimproveglucosemetabolismandthusnopatientswithT2Dachi-eved disease remission. In addition, adverse events and rate ofearlydevice removaldue toseriousadverseeventsweresimilartoourfindingsinthereview.Basedonourresults,thefeasibilityofDJBSasa standardofcare in themanagementofobesepati-entswithT2Dseemsquestionable.Finally,ourfindingsthatCCK-inducedgallbladderemptyingmedi-ated GLP-1 secretion in humans, a new observation, which hasnever been shown before, might contribute to a better under-standing of the mechanisms underlying meal-induced GLP-1secretion. Additionally, we have shed light on a potential newmode of action for metformin, as metformin stimulated GLP-1secretion and potentiated GLP-1 responses induced by gallblad-deremptying.TheseactionsmaybemediatedviaTGR5andFXRactivationandmayidentifythisolddrugasaGLP-1secretagoguemany are looking for. Furthermore, as DJBS does not interferewith gallbladder emptying and therefore does not hinder bileacids from eliciting their effects in the intestines, DJBS-inducedGLP-1secretionmayalsodependontheactionsofbileacids.
FUTUREPERSPECTIVESANDRESEARCHDatafrom325of500participantsintheENDOTrial,randomisedto either a DJBS or sham-arm, shows that DJBS resulted in a0.71% greater reduction in HbA1c compared to sham. Theremaining results (includingweight loss data) from this trial areawaitedwithgreat interest.EventhoughthefuturefortheDJBSseemsuncertain, theDJBSconcept remains intriguing.However,several aspects of the endocrine impact of the DJBS have notbeen investigated; for instance, given our findings of increased

DANISH MEDICAL JOURNAL 12
postprandial GLP-1 concentrations in patients with T2D, wouldDJBSbecapableof restoring the (lost) incretineffect inpatientswithT2D?Oralglucosetolerancetestsandsubsequent intraven-ousisoglycaemicglucoseinfusions(clampingtechnique)wouldbenecessary toaddress thisquestion.Additionally,byantagonisingthe GLP-1 receptor with the specific GLP-1 receptor antagonistexendin 9-39, it should be possible to tease out the impact ofDJBS-inducedincrementsinpostprandialGLP-1responsesforthepostoperativechanges.Furthermore,testingtheDJBSagainsteitherconventionalbariat-ric surgery or GLP-1-receptor analogues (GLP-1RA), assessingglycaemic control and weight loss, would provide informationabout theefficacyandsafetyofDJBScompared to theseweightand glycaemia improving drugs including a comparison of cost-benefit relationships. In this regard, it will be interesting to seethe results of the on-going REVISE-Diabesity Study (166) whichrandomisesobesepatientswithT2DtoeithertreatmentwiththeGLP-1RALiraglutide,DJBSaloneorDJBS+Liraglutide.In agreement with the fact that the subjects in study IV weremetabolicallyhealthy,wedidnotseeanychangestopostprandialglucoseprofiles.Therefore,itseemsobvioustoperformasimilarstudyinpatientswithT2D.Withinourresearchgroup,suchstudyiscurrentlyunderway.
SUMMARYBariatric surgery (e.g.Roux-en-Y gastric bypass (RYGB)) has pro-venthemosteffectivewayofachievingsustainableweightlossesandremissionoftype2diabetes(T2D).Studies indicatethattheeffectivenessof RYGB ismediatedby an altered gastrointestinaltract anatomy, which in particular favours release of the gutincretinhormoneglucagon-likepeptide-1(GLP-1).TheEndoBarri-erGastrointestinalLinerorduodenal-jejunalbypasssleeve(DJBS)isanendoscopicdeployableminimallyinvasiveandfullyreversib-le technique designed to mimic the bypass component of theRYGB.Not only GLP-1 is released when nutrients enter the gastroin-testinal tract. Cholecystokinin (CCK), secreted from duodenal Icells, elicits gallbladder emptying. Traditionally, bile acids arethought of as essential elements for fat absorption. However,growingevidencesuggeststhatbileacidshaveadditionaleffectsinmetabolism.Thus,bileacidsappeartoincreaseGLP-1secretionviaactivationoftheTGR5receptorontheintestinalLcell.Recent-lyFXRreceptorswerepostulatedtocontributetoGLP-1secretiontoo.Furthermore,metforminhasbeenshowntoincreasecircula-ting GLP-1 levels but although the exactmechanism is not fullyelucidated it may involve metformin-induced inhibition of bileacidreuptakefromthesmallintestines.Small-sized studies reported varyingdegreesofweight loss and,in some, improvement of glucose metabolism. Therefore, theobjectives of this thesis were to collect existing information ontheDJBS inorder toevaluateclinicalefficacyandsafety (study Iand II). Furthermore, since the endocrine impact of the DJBS isnot fully elucidated, and DJBS is expected to mimic RYGB, weinvestigated postprandialmetabolic changes following 26weeks
of DJBS treatment in ten obese subjects with normal glucosetolerance (NGT) andninematchedpatientswith T2D (study III).Finally, we studied the single and combined effects of CCK-induced gallbladder emptying and single-dose metformin onhuman GLP-1 secretion in ten healthy subjects (study IV). Wehypothesized thatmetformin-induced GLP-1 secretion - at leastpartly - would be dependent on gallbladder emptying and thepresenceofbileacidsinthegut.DJBSappearstoleadtomoderateweightlossesinobesesubjectscompared to diet or lifestyle modifications (study II). DJBS hadinsignificant and small effects (compared to diet) on glycaemicregulation.Adverseeventsconsistedmainlyofmild-to-moderatetransient dyspepsia.Nearly 20% (n=66) ofDJBS treated subjectsexperienced a serious adverse event (e.g. gastrointestinalbleeding or device migration), which resulted in early deviceremovals. No deaths or liver abscesseswere reported followingDJBStreatment.InourownstudyIIIwefoundsimilar,moderateweightlossesasin study II. GLP-1 and PYY concentrations increased in patientswith T2D (notNGT subjects) after implantation.DJBS had no orminoreffectsonpostprandiallevelsofglucose,insulin,C-peptide,glucagon, GIP, CCK or gastrin. Food intake decreased in parallelwithanincreasedsensationofsatietyinobeseNGTsubjects,butwere transient.Dyspepticepisodesoccurred innearlyallpartici-pants.Fivedevices(21%)wereexplantedearlyduetoabdominalpain,and fewchangesofon-goingantidiabeticmedicationweremade.Finally, study IV showed that both CCK-induced gallbladder em-ptying andmetformin alone elicited significant GLP-1 responsesthatwere additive upon combination.Moreoverwe saw signifi-cant PYY and short-lasting glucose-dependent insulinotropicpolypeptide(GIP)responsesfollowinggallbladderemptying.In conclusion, in spite of increased GLP-1 responses in patientswithT2Dandamodestweight loss,DJBShadnoeffectonpost-prandialglucosemetabolism,and thereforenopatientwithT2Dachieved disease remission. Based on our results, we cannotrecommend DJBS to be implemented as a standard of medicalcaremanagementofobesepatientswithT2D.Futurelargertrialsmay lead to different conclusions. In addition, the observed guthormone responses following CCK-induced gallbladder emptyingandmetformin,makesuggestthatbileacidreleaseintothesmallintestineswith subsequentTGR5andFXR involvement contribu-tes to stimulation of GLP-1 secretion and, therefore, that met-formin’smode of action encompasses both bile acid-dependentandindependentstimulationofguthormonesecretion.REFERENCES1. WHO|Obesityandoverweight[Internet].WHO.[cited
2016Mar2].Availablefrom:http://www.who.int/mediacentre/factsheets/fs311/en/
2. AdamsKF,SchatzkinA,HarrisTB,KipnisV,MouwT,Ballard-Barbash R, et al. Overweight, obesity, and mortality in alarge prospective cohort of persons 50 to 71 years old. NEnglJMed.2006Aug24;355(8):763–78.

DANISH MEDICAL JOURNAL 13
3. Hauptman J, Lucas C, Boldrin MN, Collins H, Segal KR.Orlistat in the long-term treatment of obesity in primarycaresettings.ArchFamMed.2000Feb;9(2):160–7.
4. Haddock CK, Poston WSC, Dill PL, Foreyt JP, Ericsson M.Pharmacotherapyforobesity:aquantitativeanalysisoffourdecades of published randomized clinical trials. Int J ObesRelat Metab Disord J Int Assoc Study Obes. 2002Feb;26(2):262–73.
5. Dansinger ML, Tatsioni A, Wong JB, Chung M, Balk EM.Meta-analysis: the effect of dietary counseling for weightloss.AnnInternMed.2007Jul3;147(1):41–50.
6. LarsenTM,DalskovS-M,vanBaakM,JebbSA,PapadakiA,Pfeiffer AFH, et al. Dietswith high or low protein contentand glycemic index for weight-loss maintenance. N Engl JMed.2010Nov25;363(22):2102–13.
7. ChangS-H,StollCRT,SongJ,VarelaJE,EagonCJ,ColditzGA.Theeffectivenessandrisksofbariatricsurgery:anupdatedsystematic review and meta-analysis, 2003-2012. JAMASurg.2014Mar;149(3):275–87.
8. ZhangM, Hu T, Zhang S, Zhou L. Associations of DifferentAdiposeTissueDepotswithInsulinResistance:ASystematicReviewandMeta-analysisofObservationalStudies.SciRep.2015;5:18495.
9. Dirksen C, Jørgensen NB, Bojsen-Møller KN, Jacobsen SH,Hansen DL, Worm D, et al. Mechanisms of improved gly-caemiccontrolafterRoux-en-Ygastricbypass.Diabetologia.2012Jul;55(7):1890–901.
10. BuchwaldH,AvidorY,BraunwaldE, JensenMD,PoriesW,FahrbachK,etal.Bariatricsurgery:asystematicreviewandmeta-analysis.JAMA.2004Oct13;292(14):1724–37.
11. Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Brethauer SA,Navaneethan SD, et al. Bariatric surgery versus intensivemedical therapy for diabetes--3-year outcomes. N Engl JMed.2014May22;370(21):2002–13.
12. Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B,Wedel H, et al. Effects of bariatric surgery onmortality inSwedish obese subjects. N Engl J Med. 2007 Aug23;357(8):741–52.
13. EliassonB,LiakopoulosV,FranzénS,NäslundI,SvenssonA-M,OttossonJ,etal.Cardiovasculardiseaseandmortalityinpatientswithtype2diabetesafterbariatricsurgeryinSwe-den: a nationwide, matched, observational cohort study.LancetDiabetesEndocrinol.2015Nov;3(11):847–54.
14. Jørgensen NB, Jacobsen SH, Dirksen C, Bojsen-Møller KN,Naver L, Hvolris L, et al. Acute and long-term effects ofRoux-en-Ygastricbypassonglucosemetabolisminsubjectswith Type 2 diabetes and normal glucose tolerance. Am JPhysiolEndocrinolMetab.2012Jul1;303(1):E122–31.
15. Jacobsen SH, Olesen SC, Dirksen C, Jørgensen NB, Bojsen-Møller KN, Kielgast U, et al. Changes in gastrointestinalhormone responses, insulin sensitivity, and beta-cell func-tionwithin2weeksaftergastricbypassinnon-diabeticsub-jects.ObesSurg.2012Jul;22(7):1084–96.
16. Jørgensen NB, Dirksen C, Bojsen-Møller KN, Jacobsen SH,WormD,HansenDL, et al. Exaggeratedglucagon-likepep-tide 1 response is important for improved β-cell functionandglucosetoleranceafterRoux-en-Ygastricbypass inpa-tientswithtype2diabetes.Diabetes.2013Sep;62(9):3044–52.
17. Svane MS, Bojsen-Moller KN, Nielsen S, Jørgensen NB,Dirksen C, Bendtsen F, et al. Effects of endogenous GLP-1andGIPonglucosetoleranceafterRoux-en-Ygastricbypass
surgery. Am J Physiol Endocrinol Metab. 2016 Jan19;ajpendo.00471.2015.
18. VilsbøllT,KrarupT,MadsbadS,HolstJJ.BothGLP-1andGIPare insulinotropic at basal and postprandial glucose levelsand contribute nearly equally to the incretin effect of ameal in healthy subjects. Regul Pept. 2003 Jul 15;114(2-3):115–21.
19. Holst JJ, Knop FK, Vilsbøll T, Krarup T,Madsbad S. Loss ofincretineffectisaspecific,important,andearlycharacteris-tic of type 2 diabetes. Diabetes Care. 2011May;34 Suppl2:S251–7.
20. DaellenbachL,SuterM.Jejunojejunal intussusceptionafterRoux-en-Y gastric bypass: a review. Obes Surg. 2011Feb;21(2):253–63.
21. ObinwanneKM, FredricksonKA,MathiasonMA, Kallies KJ,FarnenJP,KothariSN. Incidence,treatment,andoutcomesof iron deficiency after laparoscopic Roux-en-Y gastric by-pass: a 10-year analysis. J Am Coll Surg. 2014Feb;218(2):246–52.
22. de Jonge C, Rensen SS, Verdam FJ, Vincent RP, Bloom SR,Buurman WA, et al. Endoscopic duodenal-jejunal bypassliner rapidly improves type 2 diabetes. Obes Surg. 2013Sep;23(9):1354–60.
23. Koehestanie P, de Jonge C, Berends FJ, Janssen IM, BouvyND, Greve JWM. The effect of the endoscopic duodenal-jejunalbypasslineronobesityandtype2diabetesmellitus,a multicenter randomized controlled trial. Ann Surg. 2014Dec;260(6):984–92.
24. Katsuma S, Hirasawa A, Tsujimoto G. Bile acids promoteglucagon-likepeptide-1secretionthroughTGR5inamurineenteroendocrine cell line STC-1. Biochem Biophys ResCommun.2005Apr1;329(1):386–90.
25. ThomasC,GioielloA,NoriegaL,StrehleA,OuryJ,RizzoG,etal.TGR5-mediatedbileacidsensingcontrolsglucoseho-meostasis.CellMetab.2009Sep;10(3):167–77.
26. Brighton CA, Rievaj J, Kuhre RE, Glass LL, Schoonjans K,HolstJJ,etal.BileacidstriggerGLP-1releasepredominantlyby accessing basolaterally-located G-protein coupled bileacidreceptors.Endocrinology.2015Aug17;en20151321.
27. AdrianTE,BallantyneGH,LongoWE,BilchikAJ,GrahamS,BassonMD,etal.Deoxycholate isan importantreleaserofpeptideYYandenteroglucagonfromthehumancolon.Gut.1993Sep;34(9):1219–24.
28. Adrian TE, Gariballa S, Parekh KA, Thomas SA, Saadi H, AlKaabiJ,etal.RectaltaurocholateincreasesLcellandinsulinsecretion, and decreases blood glucose and food intake inobese type 2 diabetic volunteers. Diabetologia. 2012Sep;55(9):2343–7.
29. WuT,BoundMJ,StandfieldSD,GedulinB, JonesKL,Horo-witzM,etal.Effectsofrectaladministrationoftaurocholicacidonglucagon-likepeptide-1andpeptideYYsecretioninhealthy humans. Diabetes Obes Metab. 2013May;15(5):474–7.
30. MurakamiM,UneN,NishizawaM,SuzukiS,ItoH,HoriuchiT. Incretin secretion stimulated by ursodeoxycholic acid inhealthysubjects.SpringerPlus.2013Dec;2(1):20.
31. HansenM,ScheltemaMJ,SonneDP,HansenJS,SperlingM,Rehfeld JF, et al. The effect of chenodeoxycholic acid andthebileacidsequestrantcolesevelamonglucagon-likepep-tide-1secretion.DiabetesObesMetab.2016Feb17;
32. Munoz. Duodenojejunal Bypass Liner Increases Bile AcidsLevels inPatientswithSevereObesityandType2Diabetes

DANISH MEDICAL JOURNAL 14
Mellitus. 1906-P. [Internet]. [cited 2016May 8]. Availablefrom: http://app.core-apps.com/tristar_ada14/abstract/e8d61d02f7113c57d153b01651b1c06b
33. Migoya EM, Bergeron R, Miller JL, Snyder RNK, TanenM,Hilliard D, et al. Dipeptidyl peptidase-4 inhibitors adminis-tered in combinationwithmetformin result in an additiveincrease in the plasma concentration of active GLP-1. ClinPharmacolTher.2010Dec;88(6):801–8.
34. Napolitano A,Miller S, Nicholls AW, Baker D, Van Horn S,ThomasE,etal.Novelgut-basedpharmacologyofmetfor-min in patients with type 2 diabetes mellitus. PloS One.2014;9(7):e100778.
35. MannucciE,OgnibeneA,CremascoF,BardiniG,MencucciA,PierazzuoliE,etal.Effectofmetforminonglucagon-likepeptide 1 (GLP-1) and leptin levels in obese nondiabeticsubjects.DiabetesCare.2001Mar;24(3):489–94.
36. CarterD,HowlettHCS,WiernspergerNF,BaileyCJ.Differen-tialeffectsofmetforminonbilesaltabsorptionfromtheje-junum and ileum. Diabetes Obes Metab. 2003Mar;5(2):120–5.
37. CasparyWF,CreutzfeldtW.Inhibitionofbilesaltabsorptionby blood-sugar lowering biguanides. Diabetologia. 1975Apr;11(2):113–7.
38. Trabelsi M-S, Daoudi M, Prawitt J, Ducastel S, Touche V,Sayin SI, et al. Farnesoid X receptor inhibits glucagon-likepeptide-1productionbyenteroendocrineLcells.NatCom-mun.2015;6:7629.
39. Scarpello JH, Hodgson E, Howlett HC. Effect ofmetforminonbilesaltcirculationand intestinalmotility in type2dia-betes mellitus. Diabet Med J Br Diabet Assoc. 1998Aug;15(8):651–6.
40. Safety andEfficacyof EndoBarrier in SubjectsWithType2DiabetesWhoAreObese-FullTextView-ClinicalTrials.gov[Internet]. [cited 2016 May 1]. Available from:https://clinicaltrials.gov/ct2/show/study/NCT01728116
41. PoriesWJ.Bariatricsurgery:risksandrewards.JClinEndo-crinolMetab.2008Nov;93(11Suppl1):S89–96.
42. MasonEE, ItoC.Gastricbypass inobesity. SurgClinNorthAm.1967Dec;47(6):1345–51.
43. Wittgrove null, Clark null, Tremblay null. LaparoscopicGastricBypass,Roux-en-Y:PreliminaryReportofFiveCases.ObesSurg.1994Nov;4(4):353–7.
44. NavezB,ThomopoulosT,StefanescuI,CoubeauL.CommonLimbLengthDoesNotInfluenceWeightLossAfterStandardLaparoscopic Roux-En-Y Gastric Bypass. Obes Surg. 2015Dec10;
45. Alverdy JC, Prachand V, Flanagan B, Thistlethwaite WA,SieglerM,GarfinkelM,etal.Bariatric surgery:ahistoryofempiricism,afutureinscience.JGastrointestSurgOffJSocSurgAlimentTract.2009Mar;13(3):465–77.
46. Shah M, Simha V, Garg A. Review: long-term impact ofbariatric surgeryonbodyweight, comorbidities, andnutri-tional status. J Clin Endocrinol Metab. 2006Nov;91(11):4223–31.
47. Clements RH, Katasani VG, Palepu R, Leeth RR, Leath TD,RoyBP, et al. Incidenceof vitamindeficiency after laparo-scopicRoux-en-Ygastricbypassinauniversityhospitalset-ting.AmSurg.2006Dec;72(12):1196–202;discussion1203–4.
48. Lindberg K. Nutrient Deficiency in Gastric Bypass SurgeryPatients-LongitudinalResultsfromtheSwedishObeseSub-
jects (SOS) Study [Internet]. [cited 2015 Apr 22]. Availablefrom: http://app.core-apps.com/tristar_ada14/abstract/e3048dedfd3d5fbcc516bc86387927e3
49. Sandoval D. Bariatric surgeries: beyond restriction andmalabsorption.IntJObes2005.2011Sep;35Suppl3:S45–9.
50. Wang G, Agenor K, Pizot J, Kotler DP, Harel Y, Van DerSchuerenBJ,etal.Acceleratedgastricemptyingbutnocar-bohydratemalabsorption1yearaftergastricbypasssurgery(GBP).ObesSurg.2012Aug;22(8):1263–7.
51. Dirksen C, DamgaardM, Bojsen-Møller KN, Jørgensen NB,KielgastU,JacobsenSH,etal.Fastpouchemptying,delayedsmall intestinal transit, and exaggerated gut hormone re-sponsesafterRoux-en-Ygastricbypass.NeurogastroenterolMotilOffJEurGastrointestMotilSoc.2013Apr;25(4):346–e255.
52. FishmanE,MelansonD,LamportR,LevineA.Anovelendo-scopicdeliverysystemforplacementofaduodenal-jejunalimplant for the treatment of obesity and type 2 diabetes.Conf Proc Annu Int Conf IEEE Eng Med Biol Soc IEEE EngMedBiolSocAnnuConf.2008;2008:2501–3.
53. SchoutenR,Rijs CS,BouvyND,HameetemanW,KoekGH,JanssenIMC,etal.Amulticenter,randomizedefficacystudyof the EndoBarrier Gastrointestinal Liner for presurgicalweight loss prior to bariatric surgery. Ann Surg. 2010Feb;251(2):236–43.
54. KoehestanieP,BetzelB,DoganK,BerendsF,JanssenI,AartsE, et al. The feasibilityof delivering aduodenal-jejunal by-pass liner (EndoBarrier)endoscopicallywithpatientsunderconscioussedation.SurgEndosc.2014Jan;28(1):325–30.
55. HansotiaT,DruckerDJ.GIPandGLP-1asincretinhormones:lessons from single and double incretin receptor knockoutmice.RegulPept.2005Jun15;128(2):125–34.
56. MiyawakiK,YamadaY,YanoH,NiwaH,BanN,IharaY,etal.Glucoseintolerancecausedbyadefectintheentero-insularaxis: a study in gastric inhibitory polypeptide receptorknockout mice. Proc Natl Acad Sci U S A. 1999 Dec21;96(26):14843–7.
57. ScrocchiLA,BrownTJ,MaCluskyN,BrubakerPL,AuerbachAB,JoynerAL,etal.Glucoseintolerancebutnormalsatietyinmicewithanullmutation intheglucagon-likepeptide1receptorgene.NatMed.1996Nov;2(11):1254–8.
58. Tseng CC, Zhang XY, Wolfe MM. Effect of GIP and GLP-1antagonistsoninsulinreleaseintherat.AmJPhysiol.1999Jun;276(6Pt1):E1049–54.
59. Nauck M, Stöckmann F, Ebert R, Creutzfeldt W. Reducedincretin effect in type 2 (non-insulin-dependent) diabetes.Diabetologia.1986Jan;29(1):46–52.
60. Nauck MA, Homberger E, Siegel EG, Allen RC, Eaton RP,EbertR,etal.IncretineffectsofincreasingglucoseloadsinmancalculatedfromvenousinsulinandC-peptiderespons-es.JClinEndocrinolMetab.1986Aug;63(2):492–8.
61. Holst JJ.On thephysiologyofGIPandGLP-1.HormMetabResHormStoffwechselforschungHormMétabolisme.2004Dec;36(11-12):747–54.
62. Holst JJ. Thephysiologyof glucagon-likepeptide1.PhysiolRev.2007Oct;87(4):1409–39.
63. Jorsal T, Rhee NA, Pedersen J, Jepsen S, Wahlgren CD,MortensenB,etal.CharacterizingtheDistributionofEnter-oendocrineCellsinPatientswithType2DiabetesandNon-diabetic Controls. 2015(64 (suppl 1)). Available from:http://app.core-apps.com/tristar_ada15

DANISH MEDICAL JOURNAL 15
64. Cho H-J, Kosari S, Hunne B, Callaghan B, Rivera LR, BravoDM,etal.DifferencesinhormonelocalisationpatternsofKandLtypeenteroendocrinecellsinthemouseandpigsmallintestineandcolon.CellTissueRes.2015Feb;359(2):693–8.
65. Svendsen B, Pedersen J, Albrechtsen NJW, Hartmann B,Toräng S, Rehfeld JF, et al. An analysis of cosecretion andcoexpressionofguthormones frommale ratproximalanddistalsmallintestine.Endocrinology.2015Mar;156(3):847–57.
66. MortensenK,ChristensenLL,Holst JJ,OrskovC.GLP-1andGIP are colocalized in a subset of endocrine cells in thesmallintestine.RegulPept.2003Jul15;114(2-3):189–96.
67. FehmannHC,GökeR,GökeB.Cellandmolecularbiologyofthe incretinhormonesglucagon-likepeptide-Iandglucose-dependent insulin releasingpolypeptide.EndocrRev.1995Jun;16(3):390–410.
68. Wang Y, Perfetti R, Greig NH, Holloway HW, DeOre KA,Montrose-Rafizadeh C, et al. Glucagon-like peptide-1 canreversetheage-relateddeclineinglucosetoleranceinrats.JClinInvest.1997Jun15;99(12):2883–9.
69. Buteau J, El-Assaad W, Rhodes CJ, Rosenberg L, Joly E,PrentkiM.Glucagon-likepeptide-1preventsbetacellgluco-lipotoxicity.Diabetologia.2004May;47(5):806–15.
70. LarssonH,HolstJJ,AhrénB.Glucagon-likepeptide-1reduc-eshepaticglucoseproductionindirectlythroughinsulinandglucagon in humans. Acta Physiol Scand. 1997Aug;160(4):413–22.
71. Nauck MA, Bartels E, Orskov C, Ebert R, Creutzfeldt W.Additive insulinotropic effects of exogenous synthetic hu-man gastric inhibitory polypeptide and glucagon-like pep-tide-1-(7-36) amide infused at near-physiological insulino-tropic hormone and glucose concentrations. J ClinEndocrinolMetab.1993Apr;76(4):912–7.
72. Christensen M, Vedtofte L, Holst JJ, Vilsbøll T, Knop FK.Glucose-dependent insulinotropic polypeptide: a bifunc-tionalglucose-dependent regulatorofglucagonand insulinsecretioninhumans.Diabetes.2011Dec;60(12):3103–9.
73. Nauck MA, Heimesaat MM, Orskov C, Holst JJ, Ebert R,Creutzfeldt W. Preserved incretin activity of glucagon-likepeptide1 [7-36amide]butnotof synthetichumangastricinhibitory polypeptide in patients with type-2 diabetesmellitus.JClinInvest.1993Jan;91(1):301–7.
74. IrwinN,FlattPR.Evidenceforbeneficialeffectsofcompro-mised gastric inhibitory polypeptide action in obesity-relateddiabetesandpossibletherapeuticimplications.Dia-betologia.2009Sep;52(9):1724–31.
75. ChiaCW,CarlsonOD,KimW,ShinY-K,CharlesCP,KimHS,etal.Exogenousglucose-dependentinsulinotropicpolypep-tideworsens post prandial hyperglycemia in type 2 diabe-tes.Diabetes.2009Jun;58(6):1342–9.
76. WHO|Diabetes[Internet].WHO.[cited2016Apr6].Avail-able from:http://www.who.int/mediacentre/factsheets/fs312/en/
77. Kahn SE, Cooper ME, Del Prato S. Pathophysiology andtreatmentoftype2diabetes:perspectivesonthepast,pre-sent, and future. Lancet Lond Engl. 2014 Mar22;383(9922):1068–83.
78. U.K. prospective diabetes study 16. Overview of 6 years’therapyoftypeIIdiabetes:aprogressivedisease.U.K.Pro-spective Diabetes Study Group. Diabetes. 1995Nov;44(11):1249–58.
79. MasonEE.Themechanismsofsurgicaltreatmentoftype2diabetes.ObesSurg.2005Apr;15(4):459–61.
80. RubinoF,GagnerM.Potentialof surgery for curing type2diabetesmellitus.AnnSurg.2002Nov;236(5):554–9.
81. LaferrèreB,HeshkaS,WangK,KhanY,McGintyJ,TeixeiraJ,et al. Incretin levels and effect are markedly enhanced 1monthafterRoux-en-Ygastricbypass surgery inobesepa-tients with type 2 diabetes. Diabetes Care. 2007Jul;30(7):1709–16.
82. Borg CM, le Roux CW, Ghatei MA, Bloom SR, Patel AG,Aylwin SJB. Progressive rise in gut hormone levels afterRoux-en-Y gastric bypass suggests gut adaptation and ex-plainsalteredsatiety.BrJSurg.2006Feb;93(2):210–5.
83. le Roux CW, Aylwin SJB, Batterham RL, Borg CM, Coyle F,Prasad V, et al. Gut hormone profiles following bariatricsurgery favorananorectic state, facilitateweight loss,andimprove metabolic parameters. Ann Surg. 2006Jan;243(1):108–14.
84. NäslundE,GrybäckP,HellströmPM,JacobssonH,HolstJJ,TheodorssonE,etal.Gastrointestinalhormonesandgastricemptying20yearsafterjejunoilealbypassformassiveobe-sity. Int JObesRelatMetabDisord J IntAssocStudyObes.1997May;21(5):387–92.
85. Bojsen-Møller KN, Dirksen C, Jørgensen NB, Jacobsen SH,SerupAK, Albers PH, et al. Early enhancements of hepaticandlaterofperipheral insulinsensitivitycombinedwithin-creased postprandial insulin secretion contribute to im-provedglycemiccontrolafterRoux-en-Ygastricbypass.Di-abetes.2014May;63(5):1725–37.
86. Knop FK. Resolution of type 2 diabetes following gastricbypass surgery: involvement of gut-derived glucagon andglucagonotropic signalling? Diabetologia. 2009Nov;52(11):2270–6.
87. RubinoF,GagnerM,GentileschiP,KiniS,FukuyamaS,FengJ,etal.TheearlyeffectoftheRoux-en-Ygastricbypassonhormones involved in bodyweight regulation and glucosemetabolism.AnnSurg.2004Aug;240(2):236–42.
88. GuidoneC,MancoM,Valera-MoraE, IaconelliA,GniuliD,MariA,etal.Mechanismsofrecoveryfromtype2diabetesafter malabsorptive bariatric surgery. Diabetes. 2006Jul;55(7):2025–31.
89. KornerJ,BesslerM,InabnetW,TaverasC,HolstJJ.Exagger-ated glucagon-like peptide-1 and blunted glucose-dependent insulinotropic peptide secretion are associatedwith Roux-en-Y gastric bypass but not adjustable gastricbanding.SurgObesRelatDisOffJAmSocBariatrSurg.2007Dec;3(6):597–601.
90. RodieuxF,GiustiV,D’AlessioDA,SuterM,TappyL.Effectsofgastricbypassandgastricbandingonglucosekineticsandgut hormone release. Obes Silver Spring Md. 2008Feb;16(2):298–305.
91. Jorde R, Burhol PG, Johnson JA. The effect of jejunoilealbypassonpostprandial releaseofplasmagastric inhibitorypolypeptide(GIP).ScandJGastroenterol.1981;16(2):313–9.
92. Falkén Y, Hellström PM, Holst JJ, Näslund E. Changes inglucosehomeostasisafterRoux-en-Ygastricbypasssurgeryfor obesity at day three, twomonths, and one year aftersurgery:roleofgutpeptides.JClinEndocrinolMetab.2011Jul;96(7):2227–35.
93. BatterhamRL,CohenMA,EllisSM,LeRouxCW,WithersDJ,FrostGS,etal.InhibitionoffoodintakeinobesesubjectsbypeptideYY3-36.NEnglJMed.2003Sep4;349(10):941–8.

DANISH MEDICAL JOURNAL 16
94. Cummings DE, Weigle DS, Frayo RS, Breen PA, Ma MK,DellingerEP,et al. Plasmaghrelin levels afterdiet-inducedweight loss or gastric bypass surgery. N Engl JMed. 2002May23;346(21):1623–30.
95. HolstJJ,MadsbadS.MechanismsofSurgicalControlofType2Diabetes:GLP-1istheKeyFactor.SurgObesRelatDis[In-ternet]. [cited 2016 Mar 23]; Available from:http://www.sciencedirect.com/science/article/pii/S1550728916000782
96. WheelerHO.Concentratingfunctionofthegallbladder.AmJMed.1971Nov;51(5):588–95.
97. Liddle RA, Goldfine ID, RosenMS, Taplitz RA,Williams JA.Cholecystokinin bioactivity in human plasma. Molecularforms,responsestofeeding,andrelationshiptogallbladdercontraction.JClinInvest.1985Apr;75(4):1144–52.
98. Rehfeld JF. Accurate measurement of cholecystokinin inplasma.ClinChem.1998May;44(5):991–1001.
99. SonneDP,RehfeldJF,HolstJJ,VilsbøllT,KnopFK.Postpran-dial gallbladderemptying inpatientswith type2diabetes:potential implications for bile-induced secretion of gluca-gon-like peptide 1. Eur J Endocrinol Eur Fed Endocr Soc.2014Oct;171(4):407–19.
100. BuffaR,SolciaE,GoVL.Immunohistochemicalidentificationofthecholecystokinincell intheintestinalmucosa.Gastro-enterology.1976Apr;70(4):528–32.
101. Rehfeld JF. Clinical endocrinology and metabolism. Chole-cystokinin. Best Pract Res Clin Endocrinol Metab. 2004Dec;18(4):569–86.
102. Kerstens PJ, Lamers CB, Jansen JB, de Jong AJ, HesselsM,Hafkenscheid JC. Physiological plasma concentrations ofcholecystokinin stimulatepancreaticenzymesecretionandgallbladder contraction in man. Life Sci. 1985 Feb11;36(6):565–9.
103. TraunerM,BoyerJL.Bilesalttransporters:molecularchar-acterization, function, and regulation. Physiol Rev. 2003Apr;83(2):633–71.
104. Boron WF, Boulpaep EL. Medical Physiology. Vol. 2003.Saunders;
105. DawsonPA,LanT,RaoA.Bileacidtransporters.JLipidRes.2009Dec;50(12):2340–57.
106. Kliewer SA, Mangelsdorf DJ. Bile Acids as Hormones: TheFXR-FGF15/19 Pathway. Dig Dis Basel Switz.2015;33(3):327–31.
107. PotthoffMJ, Kliewer SA,Mangelsdorf DJ. Endocrine fibro-blast growth factors 15/19 and 21: from feast to famine.GenesDev.2012Feb15;26(4):312–24.
108. SinhaJ,ChenF,MilohT,BurnsRC,YuZ,ShneiderBL.beta-KlothoandFGF-15/19 inhibit theapical sodium-dependentbileacidtransporterinenterocytesandcholangiocytes.AmJPhysiolGastrointestLiverPhysiol.2008Nov;295(5):G996–1003.
109.WatanabeM,HoutenSM,MatakiC,ChristoffoleteMA,KimBW,SatoH,et al.Bile acids induceenergyexpenditurebypromotingintracellularthyroidhormoneactivation.Nature.2006Jan26;439(7075):484–9.
110. CariouB, vanHarmelen K,Duran-SandovalD, vanDijk TH,GrefhorstA,AbdelkarimM,etal.ThefarnesoidXreceptormodulates adiposity and peripheral insulin sensitivity inmice.JBiolChem.2006Apr21;281(16):11039–49.
111.MaK,SahaPK,ChanL,MooreDD.FarnesoidX receptor isessentialfornormalglucosehomeostasis.JClinInvest.2006Apr;116(4):1102–9.
112. Kir S, Beddow SA, Samuel VT, Miller P, Previs SF, Suino-Powell K, et al. FGF19 as a postprandial, insulin-independentactivatorofhepaticproteinandglycogensyn-thesis.Science.2011Mar25;331(6024):1621–4.
113. LiT,ChiangJYL.Bileacidsasmetabolicregulators.CurrOpinGastroenterol.2015Mar;31(2):159–65.
114. 2016-Standards-of-Care.pdf[Internet].[cited2016Mar20].Available from:http://care.diabetesjournals.org/site/misc/2016-Standards-of-Care.pdf
115. Intensive blood-glucose control with sulphonylureas orinsulin compared with conventional treatment and risk ofcomplications inpatientswith type2diabetes (UKPDS33).UKProspectiveDiabetesStudy(UKPDS)Group.LancetLondEngl.1998Sep12;352(9131):837–53.
116. Glossmann H, Reider N. Amarriage of two “Methusalem”drugsforthetreatmentofpsoriasis?:Argumentsforapilottrial with metformin as add-on for methotrexate. Derma-toendocrinol.2013Apr1;5(2):252–63.
117. NotoH,GotoA,TsujimotoT,NodaM.Cancerriskindiabet-icpatientstreatedwithmetformin:asystematicreviewandmeta-analysis.PloSOne.2012;7(3):e33411.
118.MoralesDR,MorrisAD.Metforminincancertreatmentandprevention.AnnuRevMed.2015;66:17–29.
119. Libby G, Donnelly LA, Donnan PT, Alessi DR, Morris AD,EvansJMM.Newusersofmetforminareatlowriskofinci-dentcancer:acohortstudyamongpeoplewithtype2dia-betes.DiabetesCare.2009Sep;32(9):1620–5.
120. Gong Z, Aragaki AK, Chlebowski RT,Manson JE, Rohan TE,Chen C, et al. Diabetes, metformin and incidence of anddeathfrominvasivecancerinpostmenopausalwomen:Re-sultsfromthewomen’shealthinitiative.IntJCancer.2016Apr15;138(8):1915–27.
121. RenaG,PearsonER,SakamotoK.Molecularmechanismofaction of metformin: old or new insights? Diabetologia.2013Sep;56(9):1898–906.
122. ShuY, SheardownSA,BrownC,OwenRP, Zhang S, CastroRA, et al. Effect of genetic variation in the organic cationtransporter 1 (OCT1) on metformin action. J Clin Invest.2007May;117(5):1422–31.
123. JiangG,ZhangBB.Glucagonandregulationofglucoseme-tabolism. Am J Physiol Endocrinol Metab. 2003Apr;284(4):E671–8.
124.Miller RA, ChuQ, Xie J, ForetzM, Viollet B, BirnbaumMJ.Biguanidessuppresshepaticglucagonsignallingbydecreas-ing production of cyclic AMP. Nature. 2013 Feb14;494(7436):256–60.
125. Hundal HS, Ramlal T, Reyes R, Leiter LA, Klip A. Cellularmechanism of metformin action involves glucose trans-porter translocation froman intracellular pool to theplas-ma membrane in L6 muscle cells. Endocrinology. 1992Sep;131(3):1165–73.
126. TurbanS,StrettonC,DrouinO,GreenCJ,WatsonML,GrayA,etal.DefiningthecontributionofAMP-activatedproteinkinase (AMPK) and protein kinase C (PKC) in regulation ofglucoseuptakebymetformininskeletalmusclecells.JBiolChem.2012Jun8;287(24):20088–99.
127. Kristensen JM, Treebak JT, Schjerling P, Goodyear L,Wojtaszewski JFP. Two weeks of metformin treatment in-ducesAMPK-dependentenhancementofinsulin-stimulatedglucoseuptakeinmousesoleusmuscle.AmJPhysiolEndo-crinolMetab.2014May15;306(10):E1099–109.

DANISH MEDICAL JOURNAL 17
128. ZhouG,MyersR,LiY,ChenY,ShenX,Fenyk-MelodyJ,etal.RoleofAMP-activatedproteinkinaseinmechanismofmet-forminaction.JClinInvest.2001Oct;108(8):1167–74.
129. Duca FA, Côté CD, Rasmussen BA, Zadeh-Tahmasebi M,RutterGA,FilippiBM,etal.MetforminactivatesaduodenalAmpk-dependentpathwaytolowerhepaticglucoseproduc-tioninrats.NatMed.2015May;21(5):506–11.
130.WuT,ThazhathSS,BoundMJ,JonesKL,HorowitzM,RaynerCK.Mechanismof increase inplasma intactGLP-1bymet-forminintype2diabetes:stimulationofGLP-1secretionorreductioninplasmaDPP-4activity?DiabetesResClinPract.2014Oct;106(1):e3–6.
131. LugariR,Dell�AnnaC,SartiL,CoppiS,VerlatoCA,SbordoneP, et al. Effects ofMetformin on Intestinal and PancreaticEndocrineSecretioninType2(Non-Insulin-Dependent)Dia-betes.In:MolinattiGM,PortaM,BelfioreF,LorenziM,edi-tors. Frontiers inDiabetes [Internet]. Basel: KARGER; 1998[cited 2016 May 10]. p. 161–3. Available from:http://www.karger.com/doi/10.1159/000060906
132. KappeC, PatroneC,Holst JJ, ZhangQ, SjöholmA.Metfor-minprotectsagainst lipoapoptosisandenhancesGLP-1se-cretion from GLP-1-producing cells. J Gastroenterol. 2013Mar;48(3):322–32.
133.MulherinAJ,OhAH,KimH,GriecoA,LaufferLM,BrubakerPL.Mechanismsunderlyingmetformin-inducedsecretionofglucagon-like peptide-1 from the intestinal L cell. Endocri-nology.2011Dec;152(12):4610–9.
134. ThondamSK,CrossA,CuthbertsonDJ,WildingJP,DaousiC.Effects of chronic treatmentwithmetformin on dipeptidylpeptidase-4 activity, glucagon-likepeptide1 andghrelin inobesepatientswithType2diabetesmellitus.DiabetMedJBrDiabetAssoc.2012Aug;29(8):e205–10.
135.MoherD, LiberatiA,Tetzlaff J,AltmanDG,PRISMAGroup.Preferredreportingitemsforsystematicreviewsandmeta-analyses: the PRISMA statement. J Clin Epidemiol. 2009Oct;62(10):1006–12.
136. Cochrane Handbook for Systematic Reviews of Interven-tions [Internet]. [cited 2015 Apr 14]. Available from:http://handbook.cochrane.org/
137.Medhus AW, Lofthus CM, Bredesen J, Husebye E. Gastricemptying: the validity of the paracetamol absorption testadjusted for individual pharmacokinetics. Neurogastroen-terol Motil Off J Eur Gastrointest Motil Soc. 2001Jun;13(3):179–85.
138. Rohde U, Federspiel CA, Vilmann P, Friis SU, Langholz E,Vilsbøll T, et al. Premature explantation of an EndoBarriergastrointestinallinerbecauseofsleeveinvagination.Endos-copy.2015;47Suppl1:E275–6.
139. Patel SRH, Hakim D, Mason J, Hakim N. The duodenal-jejunal bypass sleeve (EndoBarrier Gastrointestinal Liner)forweightlossandtreatmentoftype2diabetes.SurgObesRelatDisOffJAmSocBariatrSurg.2013Jun;9(3):482–4.
140. Verdam FJ, Liedorp PR, Geubbels N, Schouten R, JanssenIMC,KoekGH,etal.[EndoBarrierforcounteractingobesityand metabolic syndrome]. Ned Tijdschr Geneeskd.2012;156(13):A3844.
141. RohdeU,GylvinS,VilmannP,FriisSU,LangholzE,VilsbøllT,etal. [Duodenal-jejunalbypasssleeve-apotentialalterna-tive to bariatric surgery?]. Ugeskr Laeger. 2014 Sep8;176(37).
142. NeffKJ,MirasAD,leRouxC.Duodenal-jejunalbypassliners:outcomes in glycaemic control andweight loss. Curr OpinEndocrinolDiabetesObes.2013Oct;20(5):420–8.
143. Kim D. Endoscopic, duodenal-jejunal bypass liner exertsrobust improvement inglycemiaandbodyweight inobesepatients with type 2 diabetes [Internet]. [cited 2015 May19]. Available from: http://app.core-apps.com/tristar_ada14/abstract/e3048dedfd3d5fbcc516bc8638757fd3
144.MuñozR,EscalonaA.Duodenal-jejunalbypasslinertotreattype 2 diabetes mellitus in morbidly obese patients. CurrCardiolRep.2014Mar;16(3):454.
145. Zechmeister-Koss I, Huić M, Fischer S, European NetworkforHealthTechnologyAssessment(EUnetHTA).Theduode-nal-jejunalbypasslinerforthetreatmentoftype2diabetesmellitus and/or obesity: a systematic review. Obes Surg.2014Feb;24(2):310–23.
146. Sjöström L, Peltonen M, Jacobson P, Ahlin S, Andersson-Assarsson J, Anveden Å, et al. Association of bariatric sur-gerywith long-termremissionof type2diabetesandwithmicrovascular and macrovascular complications. JAMA.2014Jun11;311(22):2297–304.
147. RohdeU,HedbäckN,GluudLL,VilsbøllT,KnopFK.EffectoftheEndoBarrierGastrointestinalLineronobesityandtype2diabetes: a systematic review andmeta-analysis. DiabetesObesMetab.2016Mar;18(3):300–5.
148. EscalonaA,PimentelF,SharpA,BecerraP,SlakoM,TurielD,etal.Weightlossandmetabolicimprovementinmorbid-lyobese subjects implanted for1 yearwithanendoscopicduodenal-jejunal bypass liner. Ann Surg. 2012Jun;255(6):1080–5.
149. KnopFK,VilsbøllT,MadsbadS,HolstJJ,KrarupT. Inappro-priatesuppressionofglucagonduringOGTTbutnotduringisoglycaemici.v.glucoseinfusioncontributestothereducedincretin effect in type 2 diabetes mellitus. Diabetologia.2007Apr;50(4):797–805.
150. Schmidt JB, Pedersen SD, Gregersen NT, Vestergaard L,NielsenMS,RitzC,etal.EffectsofRYGBonenergyexpendi-ture, appetite and glycaemic control: a randomized con-trolledclinicaltrial.IntJObes2005.2016Feb;40(2):281–90.
151. FariaSL,FariaOP,CardealMdeA,deGouvêaHR,Buffing-tonC.Diet-inducedthermogenesisandrespiratoryquotientafterRoux-en-Ygastricbypass.SurgObesRelatDisOffJAmSocBariatrSurg.2012Dec;8(6):797–802.
152. KellumJM,KuemmerleJF,O’DorisioTM,RayfordP,MartinD, Engle K, et al. Gastrointestinal hormone responses tomeals before and after gastric bypass and vertical bandedgastroplasty.AnnSurg.1990Jun;211(6):763–70;discussion770–1.
153. Schmidt JB, Pedersen SD, Gregersen NT, Vestergaard L,NielsenMS,RitzC,etal.EffectsofRYGBonenergyexpendi-ture, appetite and glycemic control: a randomized con-trolledclinicaltrial.IntJObes2005.2015Aug25;
154. de Jonge C, Rensen SS, Verdam FJ, Vincent RP, Bloom SR,BuurmanWA, et al. Impact of Duodenal-Jejunal ExclusiononSatietyHormones.ObesSurg.2016Mar;26(3):672–8.
155. AgersnapM,RehfeldJF.Nonsulfatedcholecystokininsinthesmallintestineofpigsandrats.Peptides.2015Sep;71:121–7.
156.MaggiU,FormigaA,LauroR.Hepaticabscessasacomplica-tionofduodenal-jejunalbypasssleevesystemandreviewofthe literature. SurgObes RelatDis [Internet]. 2016 Feb 23

DANISH MEDICAL JOURNAL 18
[cited 2016 Apr 10];0(0). Available from:http://www.soard.org/article/S1550728916000630/abstract
157. EndoBarrier®Clinical Study [Internet]. [cited2015Apr 14].Availablefrom:http://www.endobarriertrial.com/
158. GI Dynamics Concludes ENDO Trial [Internet]. [cited 2016May 5]. Available from: http://gidynamics.com/media-press-release.php?id=148
159. Ahrén B, Holst JJ, Efendic S. Antidiabetogenic action ofcholecystokinin-8 in type 2 diabetes. J Clin EndocrinolMetab.2000Mar;85(3):1043–8.
160. RobergeJN,BrubakerPL.Regulationof intestinalprogluca-gon-derived peptide secretion by glucose-dependent insu-linotropic peptide in a novel enteroendocrine loop. Endo-crinology.1993Jul;133(1):233–40.
161. Brubaker PL. Regulation of intestinal proglucagon-derivedpeptide secretion by intestinal regulatory peptides. Endo-crinology.1991Jun;128(6):3175–82.
162. DumoulinV,DakkaT,PlaisancieP,Chayvialle JA,Cuber JC.Regulationofglucagon-likepeptide-1-(7-36)amide,peptideYY,andneurotensinsecretionbyneurotransmittersandguthormonesintheisolatedvascularlyperfusedrat ileum.En-docrinology.1995Nov;136(11):5182–8.
163. PlaisancieP,BernardC,Chayvialle JA,Cuber JC.Regulationof glucagon-likepeptide-1-(7-36) amide secretionby intes-tinalneurotransmittersandhormonesintheisolatedvascu-larly perfused rat colon. Endocrinology. 1994Dec;135(6):2398–403.
164. Hansen L, Holst JJ. The effects of duodenal peptides onglucagon-likepeptide-1secretionfromtheileum.Aduode-no--ilealloop?RegulPept.2002Dec31;110(1):39–45.
165. Beglinger S, Drewe J, Schirra J, Göke B, D’Amato M,BeglingerC.Roleoffathydrolysisinregulatingglucagon-likePeptide-1 secretion. J Clin Endocrinol Metab. 2010Feb;95(2):879–86.
166. Randomisation to Endobarrier Alone Versus With IncretinAnalogue in SustainEd Diabesity (REVISE-Diabesity) - FullTextView -ClinicalTrials.gov [Internet]. [cited2016Apr9].Available from:https://clinicaltrials.gov/ct2/show/NCT02055014?term=REVISE-Diabesity&rank=1