Chole Stasis PDF
3
Letters to the Editor Journal of Gastroenterology and Hepatology 21 (2006) 1634–1639 © 2006 The Authors 1635 Journal compilation © 2006 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd citrulline level (764 mmol/L, normal range 19–46 mmol/L) and liver biopsy revealed micronodular liver cirrhosis with marked fatty infiltration. Hepatic ASS activity was markedly reduced to 4% of control. Mutation analysis of the SLC25A13 gene was performed with informed consent of the patient and his family. The patient was a homozygote for the mutation of IVS11 + 1G > A 1 and CTLN2 was diagnosed. Both his mother and brother were heterozygotes for the mutation. In January 2000, the patient received living-related liver transplantation from his younger brother. After liver transplantation, blood chemistry including liver function tests and hyperlipidemia returned to nor- mal levels without any dietary restriction (Fig. 1). It is difficult to diagnose CTLN2 before the onset of encephal- opathy. To make an early diagnosis, it is important to clarify the preceding symptoms of CTLN2. Although increased serum levels of pancreatic secretory trypsin inhibitor (PSTI) have been reported as a diagnostic marker for CTLN2, 2 the measurement of PSTI is not performed routinely in clinical practice. After the discovery of the gene responsible for CTLN2, an infantile form of the disease was elucidated in patients with neonatal cholestasis (NICCD; MIM#605814). 3 Clinical features of NICCD patients include cholestasis, hepatic steatosis, hypoproteinemia and hyperami- noacidemia. Among the manifestations of citrin deficiency in both adults (CTLN2) and neonates (NICCD), steatosis is associated in most patients. The present patient also had fatty liver in association with idio- pathic hypertriglyceridemia. Saheki et al . considered that a mech- anism of fatty liver and hypertriglyceridemia was based on the function of citrin as the AGC. 4 A function of AGC is to transport NADH reducing equivalent from the cytosol into the mitochondria as a member of the malate aspartate shuttle. Citrin deficiency may cause dysfunction of this shuttle and NADH may accumulate in the cytosol. Conversely , two alternative NADH shuttle systems are known, the glycerophosphate shuttle and the citrate malate shuttle. The citrate malate shuttle, which is a part of the fatty acid synthe- sis pathway, might operate compensatory to reduce cytosolic NADH reducing equivalent. Activation of this system leads to production of acetylCoA in the cytosol and stimulates fatty acid synthesis, resulting in fatty liver and hypertriglyceridemia. 4 How- ever, it needs to be proved whether or not these compensatory processes are taking place in each patient with citrin deficiency. Another interesting feature is the progression of fibrosis during the first and second liver biopsy . The pathological features resem- bled those of nonalcoholic steatohepatitis (NASH). Although the mechanism of inflammation and fibrosis with NASH patients is not clear, a possible explanation for the initiation of inflammation might be that accumulation of excessive fat may develop oxidative stress which stimulates collagen production and fibrosis. 5 Also, in patients with CTLN2, citrin deficiency may increase cytosolic NADH and the increased cytosolic NADH may induce reductive stress and subsequent oxidative stress. Although the mechanism of hypertriglyceridemia with fatty liver in CTLN2 remains to be clarified, it might be a useful marker for the early diagnosis of CTLN2. Ryo Terada,* Kazuhide Yamamoto, † Keiko Kobayashi, ‡ Kohsaku Sakaguchi,* Yoshiaki Iwasaki,* Takeyori Saheki ‡ and Yasushi Shiratori* * Department of Medicine and Medical Science, Okayama, Okayama University Graduate School of Medic ine and Dentistry, † Okayama Saiseikai General Hospital, Okayama, and ‡ Department of Molecular Metabolism and Biochemical Genetics, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan References 1 Koba yashi K, Sin asac DS, Iij ima M et al. The gene mutated in adult- onset type II citrullinaemia encodes a putative mitochondrial carrier protein. Nat. Genet. 1999; 22 : 159–63. 2 Koba yashi K, Horiuc hi M, Saheki T. Pancrea tic secret ory trypsin inhib - itor as a diagnostic marker for adult-onset type II citrullinemia. Hepa- tology 1997; 25 : 1160–5. 3 Yamaguc hi N, Kob ayashi K, Yasuda T et al. Screening of SLC25A13 mutations in early and late onset patients with citrin deficiency and in the Japanese population: Identification of two novel mutations and establishment of multiple DNA diagnosis methods for nine mutations. Hum. Mutat. 2002; 19 : 122–30. 4 Saheki T, Kobayash i K, Iijima M et al. Adult-onset type II citrullinemia and idiopathic neonatal hep atitis caused by citrin deficiency: involve- ment of the aspartate glutamate carrier for urea synthesis and mainte- nance of the urea cycle. Mol. Genet. Metab. 2004; 81 (Suppl. 1): S20–6. 5 Sanya l AJ, Ca mpbell- Sarge nt C, Mirshahi F et al. Nonalcoholic steato- hepatitis: association of insulin resistance and mitochondrial abnormal- ities. Gastroenterology 2001; 120 : 1183–92. Figure 1 Clinical course of the patient. Hypertriglyceridemia and ammonia normalized after liver transplantation. ( ᭹ ) Triglyceride, left ( ᭺ ) ammonia, right. 0 200 400 600 800 1000 1200 1400 1600 97/10 98/4 98/10 99/4 99/10 00/4 00/10 01/4 01/10 0 50 100 150 200 250 300 350 400 1st liver biopsy 2nd liver biopsy Transplantation T r i g l y c e r i d e ( m g / d l ) Bezafibrate 400mg A m m o n i a ( m m o l / l ) Blackwell Publishing AsiaMelbourne, Austral iaJGHJournal of Gastroenterology and Hepatology0815-93192006 Blackwell Publishing Asia Pty Ltd 200621016341639Letter to the Editor Letters to the EditorLetters to the Editor LETTER TO THE EDITOR Unusual case of hepatitic cholestasis resembling fibrosing cholestatic hepatitis in a dialysis patient with chronic hepatitis B infection To the Editor, A 48-year-old man, a non-drinker with no known history of liver disease, presented with end-stage renal failure of unknown
-
Upload
roro-widyastuti -
Category
Documents
-
view
246 -
download
0
Transcript of Chole Stasis PDF

7/29/2019 Chole Stasis PDF
http://slidepdf.com/reader/full/chole-stasis-pdf 1/3
Letters to the Editor
Journal of Gastroenterology and Hepatology21 (2006) 1634–1639 © 2006 The Authors
1635
Journal compilation © 2006 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd
citrulline level (764 mmol/L, normal range 19–46 mmol/L) and
liver biopsy revealed micronodular liver cirrhosis with marked
fatty infiltration. Hepatic ASS activity was markedly reduced to
4% of control. Mutation analysis of the SLC25A13
gene was
performed with informed consent of the patient and his family.
The patient was a homozygote for the mutation of
IVS11 +
1G >
A
1
and CTLN2 was diagnosed. Both his mother
and brother were heterozygotes for the mutation. In January 2000,the patient received living-related liver transplantation from his
younger brother. After liver transplantation, blood chemistry
including liver function tests and hyperlipidemia returned to nor-
mal levels without any dietary restriction (Fig. 1).
It is difficult to diagnose CTLN2 before the onset of encephal-
opathy. To make an early diagnosis, it is important to clarify the
preceding symptoms of CTLN2. Although increased serum levels
of pancreatic secretory trypsin inhibitor (PSTI) have been reported
as a diagnostic marker for CTLN2,
2
the measurement of PSTI is
not performed routinely in clinical practice. After the discovery of
the gene responsible for CTLN2, an infantile form of the disease
was elucidated in patients with neonatal cholestasis (NICCD;
MIM#605814).
3
Clinical features of NICCD patients include
cholestasis, hepatic steatosis, hypoproteinemia and hyperami-noacidemia. Among the manifestations of citrin deficiency in both
adults (CTLN2) and neonates (NICCD), steatosis is associated in
most patients.
The present patient also had fatty liver in association with idio-
pathic hypertriglyceridemia. Saheki et al
. considered that a mech-
anism of fatty liver and hypertriglyceridemia was based on the
function of citrin as the AGC.
4
A function of AGC is to transport
NADH reducing equivalent from the cytosol into the mitochondria
as a member of the malate aspartate shuttle. Citrin deficiency may
cause dysfunction of this shuttle and NADH may accumulate in
the cytosol. Conversely, two alternative NADH shuttle systems are
known, the glycerophosphate shuttle and the citrate malate shuttle.
The citrate malate shuttle, which is a part of the fatty acid synthe-sis pathway, might operate compensatory to reduce cytosolic
NADH reducing equivalent. Activation of this system leads to
production of acetylCoA in the cytosol and stimulates fatty acid
synthesis, resulting in fatty liver and hypertriglyceridemia.
4
How-
ever, it needs to be proved whether or not these compensatory
processes are taking place in each patient with citrin deficiency.
Another interesting feature is the progression of fibrosis during
the first and second liver biopsy. The pathological features resem-
bled those of nonalcoholic steatohepatitis (NASH). Although the
mechanism of inflammation and fibrosis with NASH patients is
not clear, a possible explanation for the initiation of inflammation
might be that accumulation of excessive fat may develop oxidativestress which stimulates collagen production and fibrosis.
5
Also, in
patients with CTLN2, citrin deficiency may increase cytosolic
NADH and the increased cytosolic NADH may induce reductive
stress and subsequent oxidative stress. Although the mechanism of
hypertriglyceridemia with fatty liver in CTLN2 remains to be
clarified, it might be a useful marker for the early diagnosis of
CTLN2.
Ryo Terada,* Kazuhide Yamamoto,
†
Keiko Kobayashi,
‡
Kohsaku Sakaguchi,* Yoshiaki Iwasaki,* Takeyori Saheki
‡
and
Yasushi Shiratori*
*
Department of Medicine and Medical Science, Okayama,
Okayama University Graduate School of Medicine and Dentistry,
†
Okayama Saiseikai General Hospital, Okayama, and
‡
Department of Molecular Metabolism and Biochemical Genetics,
Kagoshima University Graduate School of Medical and Dental
Sciences, Kagoshima, Japan
References
1 Kobayashi K, Sinasac DS, Iijima M et al.
The gene mutated in adult-
onset type II citrullinaemia encodes a putative mitochondrial carrier
protein. Nat. Genet.
1999; 22
: 159–63.
2 Kobayashi K, Horiuchi M, Saheki T. Pancreatic secretory trypsin inhib-
itor as a diagnostic marker for adult-onset type II citrullinemia. Hepa-
tology
1997; 25
: 1160–5.
3 Yamaguchi N, Kobayashi K, Yasuda T et al.
Screening of SLC25A13
mutations in early and late onset patients with citrin deficiency and inthe Japanese population: Identification of two novel mutations and
establishment of multiple DNA diagnosis methods for nine mutations.
Hum. Mutat.
2002; 19
: 122–30.
4 Saheki T, Kobayashi K, Iijima M et al.
Adult-onset type II citrullinemia
and idiopathic neonatal hepatitis caused by citrin deficiency: involve-
ment of the aspartate glutamate carrier for urea synthesis and mainte-
nance of the urea cycle. Mol. Genet. Metab.
2004; 81
(Suppl. 1): S20–6.
5 Sanyal AJ, Campbell-Sargent C, Mirshahi F et al.
Nonalcoholic steato-
hepatitis: association of insulin resistance and mitochondrial abnormal-
ities. Gastroenterology
2001; 120
: 1183–92.
Figure 1
Clinical course of the patient. Hypertriglyceridemia and
ammonia normalized after liver transplantation. (
᭹
) Triglyceride, left (
᭺
)
ammonia, right.
0
200
400
600
800
1000
1200
1400
1600
97/10 98/4 98/10 99/4 99/10 00/4 00/10 01/4 01/10
0
50
100
150
200
250
300
350
400
1st liverbiopsy
2nd liverbiopsy
Transplantation
T r i g l y c e r i d e
( m g / d l )
Bezafibrate 400mg
Amm oni a ( mm ol / l )
Blackwell Publishing AsiaMelbourne, AustraliaJGHJournal of Gastroenterology and Hepatology0815-93192006 Blackwell Publishing Asia Pty Ltd
200621016341639Letter to the Editor
Letters to the EditorLetters to the Editor
LETTER TO THE EDITOR
Unusual case of hepatitic cholestasisresembling fibrosing cholestatichepatitis in a dialysis patient withchronic hepatitis B infection
To the Editor,
A 48-year-old man, a non-drinker with no known history of
liver disease, presented with end-stage renal failure of unknown

7/29/2019 Chole Stasis PDF
http://slidepdf.com/reader/full/chole-stasis-pdf 2/3
1636
Journal of Gastroenterology and Hepatology21 (2006) 1634–1639 © 2006 The Authors
Journal compilation © 2006 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd
Letters to the Editor
(a)
b
c
d
600 600
500
umol/L
400
300
200
100
0
500
400
300 I U / L
200
100
0
A u g - 9 7
F e b - 9 8
A u g - 9 8
F e b - 9 9
A u g - 9 9
F e b - 0 0
A u g - 0 0
Date
F e b - 0 1
A u g - 0 1
F e b - 0 2
A u g - 0 2
F e b - 0 3
A u g - 0 3
etiology. In August 1997, he was started on continuous ambula-
tory peritoneal dialysis (CAPD), which was subsequently
switched to hemodialysis after an episode of severe peritonitis in
2001.
Upon presentation in August 1997, the patient was found to
have acute hepatitis flare. His serum alkaline phosphatase (ALP)
level peaked at 246 IU/L; alanine transaminase (ALT) level was
294 IU/L and total bilirubin was 10 µ
mol/L during that episode
(Fig. 1a). All serology and virology markers were negative, except
for a positive hepatitis B surface antigen (HBsAg) and a hepatitisB e antigen (HBeAg). The serum HBV DNA detected by Digene
Hybrid Capture II assay (Digene, Beltsiville, MD, USA) was
69 ρ
g/mL, in which 1ñg/mL represented 2.83 ×
10
5
copies/mL.
Abdominal ultrasonography revealed a small and lobulated liver
and a normal size spleen. Histological findings in liver biopsy
were consistent with chronic hepatitis B infection with early
cirrhosis.
Effective nucleoside analogs such as lamivudine were not avail-
able at that time and the patient was kept under close observation
without antiviral therapy. The liver function then improved sponta-
neously with the ALP level returning to 117 IU/L and ALT to
40 IU/L 6 months later, and he has also been HBeAg negative
since December 1998. However, follow-up HBV DNA levels andanti-HBe antibody status were not available.
The serum ALT then stabilized below 1.5 times the upper limit
of normal (ULN) (
<
60 IU/L) over the following 4 years. Neverthe-
less, the ALP slowly increased with time and the patient was found
to have portal hypertension with esophageal varices and splenom-
egaly in March 2002. In addition, he had pancytopenia with a
normal bone marrow examination finding.
The total bilirubin level also started to increase in April 2003. At
the end of July 2003, it increased to 236 µ
mol/L while ALT
remained 41 IU/L. The patient complained of severe anorexia,
general malaise and jaundice. Physical examination revealed that
he had jaundice, hepatomegaly and bilateral ankle edema. There
was no evidence of gastrointestinal bleeding. There had been no
recent changes in his medications and he denied recent use of herbs, alcohol or over-the-counter medications. He remained
HBeAg negative and was tested negative for IgM anti-HAV, anti-
HCV, hepatitis D, and anti-HIV 1 and 2 antibodies. Liver ultra-
sonography revealed normal biliary tract with no space occupying
lesions. However, the patient’s serum HBV-DNA level was ele-
vated to 3781 ρ
g/mL. In view of his rapidly deteriorating liver
function and the high HBV-DNA level, the patient was started on
an adjusted renal dose of lamivudine 10 mg daily, during which
time his total bilirubin level had gone up to 420 µ
mol/L with
prothrombin time (PT) 2.9 International Normalized Ratio (INR).
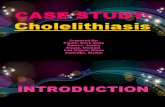
Figure 1
(a) Serial serum alkaline phosphatase (ALP), alanine ami-
notransferase (ALT) and bilirubin levels from August 1997 to August
2003. GGT, gamma-glutamyltranspeptidase. (b) Light microscopy of
liver biopsy sections shows hepatocytes ballooning, mild chronic inflam-
matory cell infiltrate, perisinusoidal fibrosis and cholestasis (hematoxylin
and eosin stain, original magnification ×
40). (c) In immunohistochemical
study, the hepatocytes strong cytoplasmic staining to HBsAg. (d) Strong
nuclear staining to HBcAg.

7/29/2019 Chole Stasis PDF
http://slidepdf.com/reader/full/chole-stasis-pdf 3/3
Letters to the Editor
Journal of Gastroenterology and Hepatology21 (2006) 1634–1639 © 2006 The Authors
1637
Journal compilation © 2006 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd
Nevertheless, his condition continued to deteriorate and he devel-
oped hepatic encephalopathy and died of hepatic failure 5 days
after the commencement of lamivudine.
A postmortem liver biopsy was performed. Histological exami-
nation showed severe hepatocyte injuries and dysfunction with
marked intracytoplasmic cholestasis, focal intracanalicular
cholestasis and balloon degeneration (Fig. 1b). There was only
scanty inflammatory infiltrate. Marked perisinusoidal fibrosis wasseen. In immunohistochemical studies, the hepatocytes showed
diffuse and strong reactivity to HBsAg in the cytoplasm (Fig. 1c),
and focal but strong reactivity to hepatitis B core antigen (HbcAg)
in the nuclei (Fig. 1d). The overall findings were similar to those
described for fibrosing cholestatic hepatitis.
The possible spontaneous development of fibrosing cholestatic
hepatitis (FCH)-like severe cholestatic hepatitis, as shown in our
case, represents a rare but serious and potentially fatal complica-
tion in dialysis patients with chronic HBV infection. Although
uremia is associated with a wide range of impairment in the
lymphocyte and granulocyte functions, FCH has not been reported
in this group of patients without immunosuppressive treatment.
1,2
As the entity ‘FCH’ is used to refer to the rapid evolution of severe
disease in patients without underlying cirrhosis,
3
and our patienthad been found to have liver cirrhosis several years before the
development of cholestatic hepatitis, it would be difficult to ascer-
tain the pathogenic origin of the fibrosis in the autopsy findings.
Therefore, it might not be appropriate to label our patient as a case
of FCH. Nevertheless, given its dominant hepatic cholestasis,
modest increase in hepatic transaminases, rapid clinical course,
high HBV DNA level together with prominent HBcAg cytoplas-
mic staining and histological features in the postmortem liver
biopsy, the condition occurring in our case probably shares a
similar clinical-pathological mechanism with cases of FCH, in
which the hepatic injury is related to the direct cytotoxic effects of
high viral loads and accumulation of viral antigens, in particular,
large surface protein. The possible pathogenic role of this largesurface protein was first suggested by an experimental study with
a transgenic mice model, in which hepatic overexpression of HBV
large surface protein was associated with the development of hepa-
tocellular apoptosis and chronic hepatitis.
4
It was further sup-
ported by another study, in which cultured hepatoma cells being
transfected with a plasmid selectively expressing the viral large
surface protein developed numerous large vacuoles and apoptosis
resembling findings observed in FCH.
5
However, it remains unknown whether or not there are factors
other than uremia contributing to the viral reactivation and devel-
opment of this condition in our case. Previous studies have
shown that patients with HBV precore mutants might be at a
greater risk of developing FCH as compared with those carrying
wild types, and many of the FCH cases reported in the literaturewere HBeAg negative related.
6–8
It was speculated that the lack
of HBeAg could enable the virus to escape immune recognition
and predispose to unchecked viral replication. It is interesting to
note that HBeAg negative HBV mutants also play a pivotal role
in our case. Our patient had been tested negative for HBeAg
since late 1998 following resolution of an acute hepatitis flare.
Although follow-up HBV DNA levels and anti-HBe status were
not available, the clinical course was compatible with HBeAg
seroconversion. Since then, there had not been any major
derangement in his serum ALT levels and there had been no
definite evidence to suggest an occurrence of severe flares of
hepatitis, which might be able to give rise to prolonged hepatic
cholestasis in this case. Conversely, given a common occurrence
of serum ALT depression in dialysis patients, ongoing hepatic
activity could still occur with a modest elevation of serum ALT.
9
In fact, with a high frequency of HBeAg negative mutants in the
Asian population, progressive deterioration of liver function is
commonly seen even after HBeAg seroconversion in this locality,especially in patients with advanced liver disease. In our patient,
HBeAg negative mutants probably emerged after HBeAg loss
and accounted for the progressive liver disease and subsequent
FCH-like cholestatic hepatitis. Nevertheless, the exact identity of
the responsible mutant (precore or basal core-promoter mutant)
remains undefined without performing mutation analysis and
DNA sequencing.
FCH is a rapidly fatal condition, in which successful treatment
would largely rely on early diagnosis with liver biopsy and timely
treatment with a nucleoside analog type of antiviral agent such as
lamivudine.
10
A similar clinical approach probably should also be
applied to patients with a FCH-like cholestatic hepatitis, as shown
in our case.
Ping-Nam Wong,* Tang-Tat Fung,
†
Alice NH Chan,
‡
Pak-Kwan Hui,
‡
Siu-Ka Mak,* Kin-Yee Lo,* Gensy MW Tong,*
Yuk Wong,* Ching-Kong Loo,
†
Eric KM Lam
†
and
Andrew KM Wong*
*
Division of Nephrology and †
Gastroenterology Department of
Medicine and Geriatrics, and ‡
Department of Pathology,
Kwong Wah Hospital, Hong Kong SAR, China
References
1 Kohler H. Hepatitis B immunization in dialysis patients—is it worth-
while? Nephrol. Dial. Transplant.
1994; 9
: 1719–20.2 Pesanti EL. Immunologic defects and vaccination in patients with
chronic renal failure. Infect. Dis. Clin. North Am.
2001; 15
: 813–32.
3 Davies SE, Portmann BC, O’Grady J et al.
Hepatic histological find-
ings after transplantation for chronic hepatitis B virus infection,
including a unique pattern of fibrosing cholestatic hepatitis. Hepatol-
ogy
1991; 13
: 150–7.
4 Chisari FV, Filippi P, Buras J et al.
Structural and pathological effects
of synthesis of hepatitis B virus large envelope polypeptide in trans-
genic mice. Proc. Natl. Acad. Sci. USA
1987; 84
: 6909–13.
5 Foo NC, Ahn BY, Ma X, Hyun W, Yen TS. Cellular vacuolization and
apoptosis induced by hepatitis B virus large surface protein. Hepatol-
ogy
2002; 36
: 1400–7.
6 Angus PW, Locarnini SA, McCaughan GW, Jones RM, Mcmillan JS,
Bowden DS. Hepatitis B virus precore mutant infection is associated
with severe recurrent disease after liver transplantation. Hepatology
1995; 21
: 14–18.
7 Trautwein C, Schrem H, Tillmann HL et al.
Hepatitis B virus muta-
tions in the pre-S genome before and after liver transplantation. Hepa-
tology
1996; 24
: 482–8.
8 Jung S, Lee HC, Han JM et al.
Four cases of hepatitis B virus-related
fibrosing cholestatic hepatitis treated with lamivudine. J. Gastroen-
terol. Hepatol.
2002; 17
: 345–50.
9 Wong PN, Fung TT, Mak SK et al.
Hepatitis B virus infection in
dialysis patients. J. Gastroenterol. Hepatol.
2005; 20
: 1641–51.
10 Gane E, Pilmore H. Management of chronic active hepatitis before and
after renal transplantation. Transplanatation
2002; 74
: 427–37.