Dr. Kayla Laserson INDEPTH AGM, Ghana, September 2010 INDEPTH Tuberculosis Working Group.
17
Dr. Kayla Laserson INDEPTH AGM, Ghana, September 2010 INDEPTH Tuberculosis Working Group
-
Upload
stella-anderson -
Category
Documents
-
view
227 -
download
2
Transcript of Dr. Kayla Laserson INDEPTH AGM, Ghana, September 2010 INDEPTH Tuberculosis Working Group.

Dr. Kayla LasersonINDEPTH AGM, Ghana, September 2010
INDEPTH
Tuberculosis Working Group

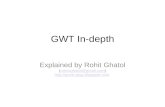
Tuberculosis Notification Rate, 2008
0 - 24
25 - 49
50 - 99
100 or more
No report
Notified TB cases (new and relapse) per 100 000 population
22 High Burden Countries: 11 have at least 1 HDSS Center (Bangladesh, Ethiopia, India, Indonesia, Kenya, Mozambique, South Africa, Tanzania, Thailand, Uganda, Vietnam)

April 2010: First Face-to-Face Meeting, Kisumu, Kenya
• Facilitators – Dr. Kayla Laserson –
KEMRI/CDC HDSS, Kisumu, Kenya
– Dr. Christian Wejse – Bandim HDSS, Guinea
• The workshop intended to facilitate INDEPTH centers to create a TB research agenda within HDSS centers
• Centers presented background of their site and TB activities to date
• Participating INDEPTH centers • Ballabgarh, India • Bandim, Guinea Bissau • Dodalab, Vietnam • Dodowa, Ghana • Filabavi, Vietnam • Kanchanaburi, Thailand • Karonga, Malawi • Kintampo, Ghana • Kisumu, Kenya • Matlab, Bangladesh • Navrongo, Ghana • Nouna, Burkina Faso • Vadu, India

Initial TB-related Activities for HDSS Centers
• Link National Program TB patient registers to HDSS data– A primary step to evaluate TB in the context of an HDSS; draw
upon other groups/studies which are linking data, such as INESS
• Link SES data/asset scores/etc to notified TB cases (or TB prevalence data if it exists)– To establish the association between TB and SES/other RF in the
HDSS's and allow the DSS's to compare across centers
• Evaluate the association between recent/new in-migrants and TB and HIV (where possible)

Groups and Group Leaders
• Collaborative prevalence studies/risk factors (WHO) and other regular prevalence surveys – Dr. Sanjay Juvekar
• Clinical trials readiness – Dr. K. Zaman
• Effect of being a TB suspect or having TB on HHS, SES and mortality (VA) – Dr. Christian Wejse
• Mapping – Prof. Amara

Assessment for Linking/Using TB/HIV Data
TB data can be linked to HDSS
Does TB pat get HDSS ID
Collect SES
Collect migration
Collect HIV and can link to HDSS
Freq of Rounds
Conduct VA
Conducted GCP trials
Kenya: KEMRI/CDC
Yes No Yes Yes Yes Every 4 m Yes Yes
Guinea Bissau: Bandim
Yes Yes Yes Yes Yes Annually Yes-but not whole pop
Yes
Ghana-Dodowa
Yes Not yet Yes Yes No Every 6 m Yes Yes
Ghana-Navrongo
Yes No Yes Yes No Every 4 m Yes Yes
Ghana-Kintampo
Yes No Yes Yes No Every 6 m Yes Yes
Vietnam-Doda Yes No Yes Yes No Every 3 m No YesVietnam-Filabavi
Yes No Yes Yes No Every 3 m Yes Yes
Thailand-Kan No No Yes Yes No Annually No NoMalawi Yes Yes Yes Yes Yes Monthly Yes YesIndia-Vadu Yes Yes Yes Yes No Every 6 m Yes YesIndia-Ball Yes Yes if res Yes Yes No Monthly Yes YesBangladesh Yes Yes if res Yes Yes No Every 2 m Yes YesKenya: Kibera Yes Yes if res Yes Yes Yes Every
weekYes No/ GCP
trainedBurkina Faso-Nouna
Yes Yes if res Yes Yes No Every 4 m Yes Yes
Kenya: Walter Reed
No No Yes Yes No Every 6 m No No

Surveillance of TB Risk Factors
• Specific objectives – Document available data on TB risk factors – Establish surveillance of selected TB risk factors – Study the prevalence of reported TB
• Methods– Routine update : Adding one question to round: Since the last time we visited
your house, is there anybody living in this house who has been diagnosed with TB/ has had regular contact with an individual who has TB?
– Periodic surveys
• All centers are currently using different tools– Should use INDEPTH SES tool– Other important risk factors: migration, crowding, pollution in general, mental
illness/stress, worm infestation, other infectious diseases, diabetes, malnutrition

Establish TB Trial Network
• Objectives – To assess the capacity and identify gaps to conduct clinical trials – To evaluate investigational products in dx, treatment and prevention of TB – To provide evidence to health planners and policy makers– Utilize the HDSS for long term safety monitoring
• HDSS network has the required strength – Large population sample – Ability to follow participants long term – Can follow contacts as well – Can recruit more than 2000 smear +ve TB in a year – Differing epidemiology of TB – Long term follow up of adverse events– Established communication between INDEPTH network centers – Available data on SES, and other determinants (e.g. nutrition, GIS) – Available data on other diseases/morbidity (cost-saving to sponsor)

INDEPTH Centers as TB Intervention Trial Platforms:
Potential Number of TB Cases• Kisumu HDSS, Kenya: 800 smear +ve • HDSS Filabavi & Dodolab, Vietnam: 100 smear +ve • Bandim HDSS, Guinea Bissau: 100 smear +ve • Matlab HDSS, Bangladesh: 150 smear +ve • Karonga HDSS, Malawi: 150 smear +ve • Filabavi HDSS, Vietnam: 400 smear +ve • Nouna HDSS, Bukina Faso: 40 smear +ve • All HDSS centers, Ghana: 150 smear +ve • KEMRI/WRP: 100 smear +ve • Kanchanaburi HDSS, Thailand: 150 smear +ve • KEMRI/CDC Kibera, Kenya: 50 smear +ve • Ballargbarh HDSS, India: 100 smear +ve More than 2000 smear +veAll centers are GCP compliant except Kibera, Kenya and Kanchanaburi, Thailand

• TB suspects who are assumed not to have TB/TB cases/ no TB or suspect– 3 years data
• Analysis - Compare longitudinal outcomes in compounds with assumed TB negative with compounds without such persons
• Work on-going In Bandim: Christian Wejse will present an update at the TB Working Group meeting
Effects of Assumed Negative/ Having TB on Health Outcomes

Comprehensive Mapping Exercise
• TB data collected by each site, clinical/lab/pharmaceutical capacity at each site, and how linkages are made based on HDSS
• Site Assessment Forms– Summary will be presented in TB Working
Group Session

Critical Path to TB Drug Regimens (CPTR)
• INDEPTH invited to June 2010 launch after GATES call with ED, and INDEPTH TB working group
• Mission– To bring novel scientific tools, strategies, and
approaches that incorporate the most advanced methods into TB product development
• INDEPTH to participate in Research Resources Group and expects to serve as a clinical trials platform
• Application made to US FDA for a cooperative agreement to support CPTR (pending)– Letter of support from INDEPTH
• Steve Wandiga, Kisumu, Kenya HDSS: POC

WHO TB Research Movement
• Basic research• Development of new tools (drugs, diagnostics, and
vaccines)• Operational/ implementation research– Workshop May 2010– Report shared with INDEPTH centers
• Helping to identify centers for clinical trials– Identified INDEPTH as ideal
• Pursuing discussions/search for funding

WHO Assessment of Possible TB Operational/Implementation
Research Areas for INDEPTH centers• Incidence
– Link with NTP data– Service provider mapping combined with universal referral and notification of
TB cases – GIS mapping– Repeated prevalence surveys
• Prevalence• Death
– Verbal autopsy– Link with death registration and hospital data
• Risk factors and social determinants– Effect size, interaction, multilevel analysis to explore pathways, population
attributable fractions– Link with incidence, prevalence and death data– Expand baseline data on TB risk factors

WHO Assessment of Possible TB Research Areas for INDEPTH
centers (2)• Effectiveness of intensified case finding approaches
– Service provider mapping and engagement - referral, notification, diagnosis
– Contact investigations, link with baseline data– Universal screening for chronic cough - referral– Universal X-ray and cough screening, diagnosis with smear
microscopy and culture (prevalence survey methodology)– Targeted screening of risk groups (risk factors, poverty,
migration, etc)
• Completeness of case notification and detection
• Completeness of treatment adherence

Conclusion/ Way Forward
• Considerable interest and capacity at INDEPTH centers
• Considerable interest by GATES (CPTR) and WHO
• Further analyses at centers (where possible/affordable) to build up body of data/publications
• Further discussions/funding applications: core support from INDEPTH?
• Please join the TB Working Group! – Meets Tomorrow 5-6:30pm

Thank you!