CARDIOVASCULAR DISEASE SCREENING IN PREGNANCY- …
56
CARDIOVASCULAR DISEASE SCREENING IN PREGNANCY- ROLE OF THE CMQCC TOOLKIT AFSHAN HAMEED, MD, FACOG, FACC HS Professor, Maternal Fetal Medicine & Cardiology University of California, Irvine AWHONN California Section Conference, February 21 st 2020, Long Beach CA
Transcript of CARDIOVASCULAR DISEASE SCREENING IN PREGNANCY- …

CARDIOVASCULAR DISEASE SCREENING IN
PREGNANCY-
ROLE OF THE CMQCC TOOLKIT
AFSHAN HAMEED, MD, FACOG, FACC
HS Professor, Maternal Fetal Medicine & Cardiology
University of California, Irvine
AWHONN California Section Conference, February 21st 2020, Long Beach CA

WHY?Cardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit


Maternal MortalityChild Health USA 2013

0
5
10
15
20
25
Mat
ern
al M
ort
alit
y R
atio
(per
10
0,0
00
bir
ths)
1980 1990
2000 2008
Maternal Mortality Ratios in Selected Countries over the Past 30
Years
Hogan et al, Lancet 2010; 375: 1609–23

July 17, 2015
The US has the highest Maternal Mortality rate of any high resource country and the only country outside
of Afghanistan and Sudan where the rate is rising

Significant reductions in maternal mortality and morbidity can not be accomplished without addressing the
gaps in maternity care for black women
July 17, 2015
3-4 X

cdc.gov 8
1.6%
2X

350-400xSerious
Morbidity:
(prolonged
length of stay)
Maternal Morbidity andMortality: CVD
15-20x
Severe Maternal
Morbidity - ICU
13
13 Cardiovascular Related Mortalities/2007 in CA

LESSONS LEARNED FROM
MATERNAL MORTALITY REVIEWSCardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit

Cardiovascular Disease isthe leading cause of maternal mortality in CA and U.S.
under-recognized in pregnant or postpartum women
higher among African-American women
▪ 25% of deaths attributed to cardiovascular disease may have been prevented if the
woman’s heart disease had been diagnosed earlier
▪ Pregnancy is a period of frequent interaction with health care providers and offers an
opportunity to detect and treat heart disease, improve pregnancy outcomes, and affect
future cardiovascular health.
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI:
10.1016/j.ajog.2015.05.008

CA-PAMR FindingsIdentification and Confirmation of CVD Pregnancy-Related Deaths 2002-2006
California Birth Cohort, 2002-2006
N=2,741,220
Pregnancy-Associated Cohort
N=864
Pregnancy-Related Deaths
N=257
Cardiovascular Pregnancy-Related Deaths
N=64
Cardiomyopathy
N=42
Other Cardiovascular
N=22
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI:
10.1016/j.ajog.2015.05.008

Top 5 Causes of Death
2002-2005
Grouped Cause of Death,
per CA-PAMR Committee
Pregnancy-Related
Deaths
N (%)
Cardiovascular disease 49 (24)
Cardiomyopathy 30 (15)
Other cardiovascular 19 (9)
Preeclampsia/eclampsia 36 (17)
Obstetric hemorrhage 10 (10)
DVT/ PE 20 (10)
AFE 18 (9)
All other causes 64 (31)
TOTAL 207
CVD Pregnancy-Related Mortality Rate: 2.3 deaths /100,000 live births

23.7
17.4
9.7 9.78.7
0
5
10
15
20
25
CVD PreE/E OB Hem VTE AFE
% o
f P
reg
nan
cy-r
ela
ted
Mo
rtality
5 Leading Causes of Pregnancy-related Deaths
Main et al. Pregnancy-Related Mortality in California. Obstet Gynecol April 2015
Note: approx 30% of pregnancy-related deaths were from a variety of “other”
causes (each below 8% including sepsis, ICH, other hemorrhages)
Proportions for Each of the Leading 5 Causes of California Pregnancy-related
Mortality

3% 8% 6% 34% 48%
Preexisting (prior to pregnancy) Prenatal period At labor and delivery Postpartum period Postmortem
CA-PAMR Findings 2002-2006
Timing of Diagnosis and Death
▪ Timing of CVD Diagnosis (n=64)
▪ Timing of Death ▪ 30% of all CVD deaths were >42 days from birth/fetal demise vs. 7.3% of non CVD
pregnancy-related deaths
▪ Driven by Cardiomyopathy deaths, with 42.9% deaths >42 days
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI:
10.1016/j.ajog.2015.05.008

CA-PAMR Findings 2002-2006
Presentation of Women with CVD
▪ Abnormal physical exam findings
▪ HTN >140/90 (64%)
▪ HR >120 (59%)
▪ Crackles, S3 or gallop rhythm etc. (44%)
▪ O2 <90% (39%)
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI:
10.1016/j.ajog.2015.05.008

CA-PAMR Findings
Contributing Factors & Quality Improvement Opportunities (2002-2006) for CVD
HEALTH CARE PROVIDER RELATED
• Contributing Factors: (69% of all cases)▪ Delayed or inadequate response to clinical warning signs (61%) ▪ Ineffective or inappropriate treatment (39%)▪ Misdiagnosis (37.5%)▪ Failure to refer or consult (30%)
▪ Quality Improvement Opportunities
▪ Better recognition of signs and symptoms of CVD in pregnancy
▪ Shortness of breath, fatigue
▪ Tachycardia, blood pressure change, or low oxygen saturation
▪ Improved management of hypertension
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI: 10.1016/j.ajog.2015.05.008

▪ Contributing factors: (70% of all cases)
▪Presence of underlying medical conditions (64%)
▪Obesity (31%)
▪Delays in seeking care (31%)
▪ Lack of recognition of CVD symptoms (22%)
▪ Quality improvement opportunities
▪ Education around when to seek care for worrisome symptoms
▪ Support for improving modifiable risk factors, such as attaining healthier weight and
discontinuing drug use
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI: 10.1016/j.ajog.2015.05.008
CA-PAMR Findings
Contributing Factors & Quality Improvement Opportunities (2002-2006) for CVD
PATIENT RELATED

PREGNANCY SYMPTOMS VS.
CARDIOVASCULARCardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit

SYMPTOMS SIGNS
• Reduction of exercise
tolerance
• Hyperventilation -
shortness of breath
• Orthopnea
• Palpitations
• Light headedness
• Dizziness/Syncope
• Edema
• JVD
• Murmurs
• AUSCULTATION
• 96% have a “functional murmur”
• Mid-systolic and low intensity
• Third heart sound is common
Pregnancy Mimics
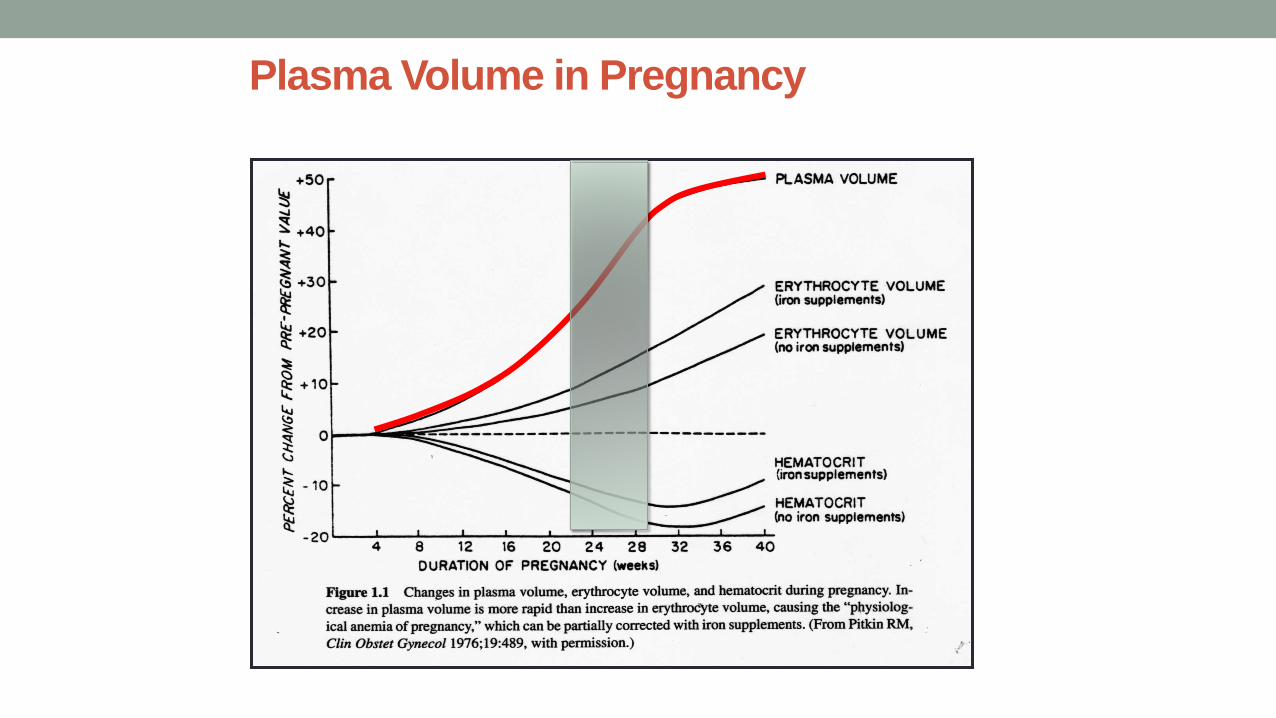
Plasma Volume in Pregnancy
Pitkin RM Clin Obstet Gyn 1976;19:489

Physiologic changes
Signs and Symptoms of Pregnancy that mimic heart
disease
Affect diagnostic tests


•Heart failure
•Arrhythmia
DEATH

History
SymptomsPhysical
Examination

CMQCC CARDIOVASCULAR
DISEASE TOOLKITCardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit

California Pregnancy-Associated Mortality Review
(CA-PAMR) Quality Improvement Review Cycle
1. Identification of cases
2. Information collection, review by multidisciplinary
committee
3. Cause of Death, Contributing Factors and Quality Improvement (QI) Opportunities identified
4. Strategies to improve care and
reduce morbidity and mortality
5. Evaluation and Implementation of QI strategies and tools
ToolkitsCVD
Venous Thromboembolism
HemorrhagePreeclampsia

IMPROVING HEALTH CARE RESPONSE TO
CARDIOVASCULAR DISEASE
IN PREGNANCY AND POSTPARTUM:
A CALIFORNIA QUALITY IMPROVEMENT
TOOLKIT
The CVD Toolkit was developed by CMQCC at Stanford University under contract with CDPH with funding from federal Title V MCH Block grant
© California Department of Public Health, 2017

Cardiovascular Disease in Pregnancy and Postpartum Task Force
Chair: Afshan Hameed MD—UC Irvine
Co-Chair: Christine H. Morton PhD—CMQCC
WRITING GROUP
◼ Deirdre Anglin MD, MPH—USC
◼ Julie Arafeh MSN, RN—Stanford
◼ Alisa Becket—WomenHeart
◼ Leona Dang-Kilduff, RN, MS, CDE—RPPC
◼ Elyse Foster, MD—UC San Francisco
◼ Abha Khandelwal, MD—Stanford
◼ Elizabeth Lawton, MHS—CDPH/MCAH
◼ Elliott Main, MD—CMQCC
◼ Barbara Murphy, MSN, RN—CMQCC
◼ Monica Sood, MD—Kaiser Walnut Creek
◼ Maryam Tarsa MD, MAS—UC San Diego
◼ Lisa Townsend—Sister to Sister
◼ Jan Trial, EdD, RN, CNM—Memorial Care
◼ Julie Vasher, DNP, MSN, RNC-OB, CNS-BC—CMQCC
REVIEWER GROUP
◼ Kathleen Belzer, CNM, NP—East Bay Perinatal
◼ Chloe Bird, PhD—RAND
◼ Susan Bogar, MSN, CNM—UCLA
◼ Elisabeth Chicoine, MS, RN, PNP—Sonoma County Department of
Health Services
◼ Karen Clemmer, MN, PHN—Sonoma County Department of Health
Services
◼ Uri Elkayam, MD—USC
◼ William (Bill) Gilbert, MD—Sutter Health System Sacramento
◼ Tipu Khan, MD—California Academy of Family Physicians
◼ Nathana Lurvey, MD—ACOG IX
◼ Karen Ramstrom, DO, MSPH—CDPH/ Center for Family Health
◼ Mari-Paule Thiet, MD—UCSF

CVD Case Presentation
▪25 year old obese (BMI 38) African-American G2P2 presents 10
days after an uncomplicated vaginal delivery with fatigue and
persistent cough since delivery.
▪BP 110/80, HR 110, RR 28, afebrile, with O2 sat 94% on room
air.
▪She gets diagnosed with respiratory infection and is prescribed
an antibiotic. Fatigue is attributed to lack of sleep.

CVD Case Presentation (CONTINUED)
▪One week later, she presents again with continued symptoms.
Antibiotics are switched and beta-agonists are added for presumptive
“new-onset asthma.”
▪Two days later, the patient experiences cardiac arrest at home and
resuscitation attempts are unsuccessful.
▪Autopsy findings were indicative of cardiomyopathy.

CVD Assessment Algorithm
for Pregnant and Postpartum Women

Suggestive of Heart Failure: • Dyspnea• Mild orthopnea• Tachypnea• Asthma unresponsive
to therapySuggestive of Arrhythmia:• Palpitations• Dizziness/syncopeSuggestive of Coronary Artery
Disease: • Chest pain• Dyspnea
SYMPTOMS *NYHA class > II
• Resting HR ≥110 bpm• Systolic BP ≥140 mm Hg• RR ≥24• Oxygen sat ≤96%
• Age ≥40 years• African American• Pre-pregnancy obesity
(BMI ≥35)• Pre-existing diabetes • Hypertension• Substance use (cocaine,
alcohol, methamphetamines)
• History of cardiotoxicchemotherapy
Heart: Loud murmur orLung: Basilar crackles
VITAL SIGNS ABNORMAL PHYSICAL EXAMINATION
RISK FACTORS
Modified from: ©California Department of Public Health, 2017; supported by Title V funds. Developed in
partnership with California Maternal Quality Care Collaborative Cardiovascular Disease in Pregnancy
and Postpartum Taskforce.
≥ 1 Symptom + ≥ 1 Vital Signs Abnormal + ≥ 1 Risk Factor orANY COMBINATION ADDING TO ≥ 4
Obtain: EKG, Echocardiogram, BNP +/- CXR; arrhythmia monitor
Consider: CBC, Comprehensive metabolic profile, Arterial blood gas, Drug screen, TSH, etc.
Follow-up within one week
NOYES
Consultation with
Pregnancy Heart Team
Results abnormalResults negative
Signs and symptoms resolved
Reassurance and routine follow-up

CVD Algorithm Validation
▪We applied the algorithm to 64 CVD deaths from 2002-2006 CA-
PAMR.
▪56 out of 64 (88%) cases of maternal mortality would have been
identified.
▪Detection increased to 93% when comparison was restricted to 60
cases that were symptomatic.
Hameed, AB, Morton, CH and A Moore. Improving Health Care Response to Cardiovascular Disease in Pregnancy and Postpartum Developed under contract #11-10006 with the California Department of
Public Health, Maternal, Child and Adolescent Health Division. Published by the California Department of Public Health, 2017.

11.1
7.7
10.0
14.6
11.8 11.7
14.0
7.4
7.3
10.9
9.7
11.6
9.2
6.2
16.9
8.9
15.1
13.1
12.19.9
9.9
9.8
13.3
12.7
15.5 16.916.6
19.3
19.9
22.0
0.0
3.0
6.0
9.0
12.0
15.0
18.0
21.0
24.0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Year
California Rate
United States Rate
Maternal Mortality Rate,
California and United States; 1999-2013
Ma
tern
al D
ea
ths
pe
r 1
00
,000
Liv
e B
irth
s
HP 2020 Objective – 11.4 Deaths per 100,000 Live Births
SOURCE: State of California, Department of Public Health, California Birth and Death Statistical Master Files, 1999-2013. Maternal mortality for
California (deaths ≤ 42 days postpartum) was calculated using ICD-10 cause of death classification (codes A34, O00-O95,O98-O99). United States data
and HP2020 Objective use the same codes. U.S. maternal mortality data is published by the National Center for Health Statistics (NCHS) through 2007
only. U.S. maternal mortality rates from 2008 through-2013 were calculated using CDC Wonder Online Database, accessed at http://wonder.cdc.govon
March 11, 2015. Produced by California Department of Public Health, Center for Family Health, Maternal, Child and Adolescent Health Division, March,
2015.
OB
Hemorrhage
QI Toolkit,
Collaboratives
Preeclampsia
QI Toolkit,
Collaboratives

Maternal Mortality Rate (early and late deaths),
California Residents; 1999-2013
11.1
7.7
10.014.6
11.8 11.7
14.0
7.4
7.3
10.9
9.7
11.6
9.2
6.2
16.9
10.2
19.1
13.4
15.2
9.9
7.7 10.9
19.0
13.8
16.315.7
18.017.1
15.5
15.2
0.0
5.0
10.0
15.0
20.0
25.0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Year
(standard MMR calculation)Early Maternal Deaths <=42 days postpartum
Early and Late Maternal Deaths up to one year postpartum
SOURCE: State of California, Department of Public Health, California Birth and Death Statistical Master Files, 1999-2013. Maternal mortality for
California (Early maternal deaths ≤ 42 days postpartum) was calculated using ICD-10 cause of death classification (codes A34, O00-O95,O98-O99) and
code O96 is also included when calculating Early and Late Maternal Deaths up to one year postpartum. Produced by California Department of Public
Health, Center for Family Health, Maternal, Child and Adolescent Health Division, March, 2015.
HP 2020 Objective – 11.4 Deaths per 100,000 Live Births
Ma
tern
al D
ea
ths
pe
r 1
00
,000
Liv
e B
irth
s

3% 8% 6% 34% 48%
Preexisting (prior to pregnancy)
Prenatal period
At labor and delivery
Postpartum period
Postmortem
CA-PAMR Findings 2002-2006
Timing of Diagnosis and Death
▪ Timing of CVD Diagnosis (n=64)
▪ Timing of Death ▪ 30% of all CVD deaths were >42 days from birth/fetal demise vs. 7.3% of non CVD
pregnancy-related deaths
▪ Driven by Cardiomyopathy deaths, with 42.9% deaths >42 days
Hameed A, Lawton E, McCain CL, et al. Pregnancy-Related Cardiovascular Deaths in California: Beyond Peripartum Cardiomyopathy. American Journal of Obstetrics and Gynecology 2015; DOI:
10.1016/j.ajog.2015.05.008

Timing of Diagnosis of Peripartum CardiomyopathyElkayam et al. Circulation 2005;111:2050
0
25
50
75
<27 28-32 33-36 37-40 1 2 3 4 5
Nu
mb
er
of
pati
en
ts
Early
Traditional
Weeks Months PPDELIVERY
N=123

BNP levels in Normal Pregnancy

B-Type Natriuretic Peptide
Increases natriuresis
and diuresis
Relaxes vascular
smooth muscle
Inhibits renin-angiotensin
aldosterone system

IMPLEMENTATION AT THE
HOSPITAL LEVELCardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit

UCI – QI Study Protocol
• Descriptive study of algorithm implementation
• Goals:
• Clinical burden of CVD screening
• Outcomes for women designated “at risk” based on the
algorithm
• Numbers
• Percentage of women with CVD
UCI – QI Study Protocol
• Applying algorithm to all patients:
• First prenatal visit
• Postpartum visit
• Anytime with symptoms and/or vital sign abnormalities with no
known cardiovascular disease


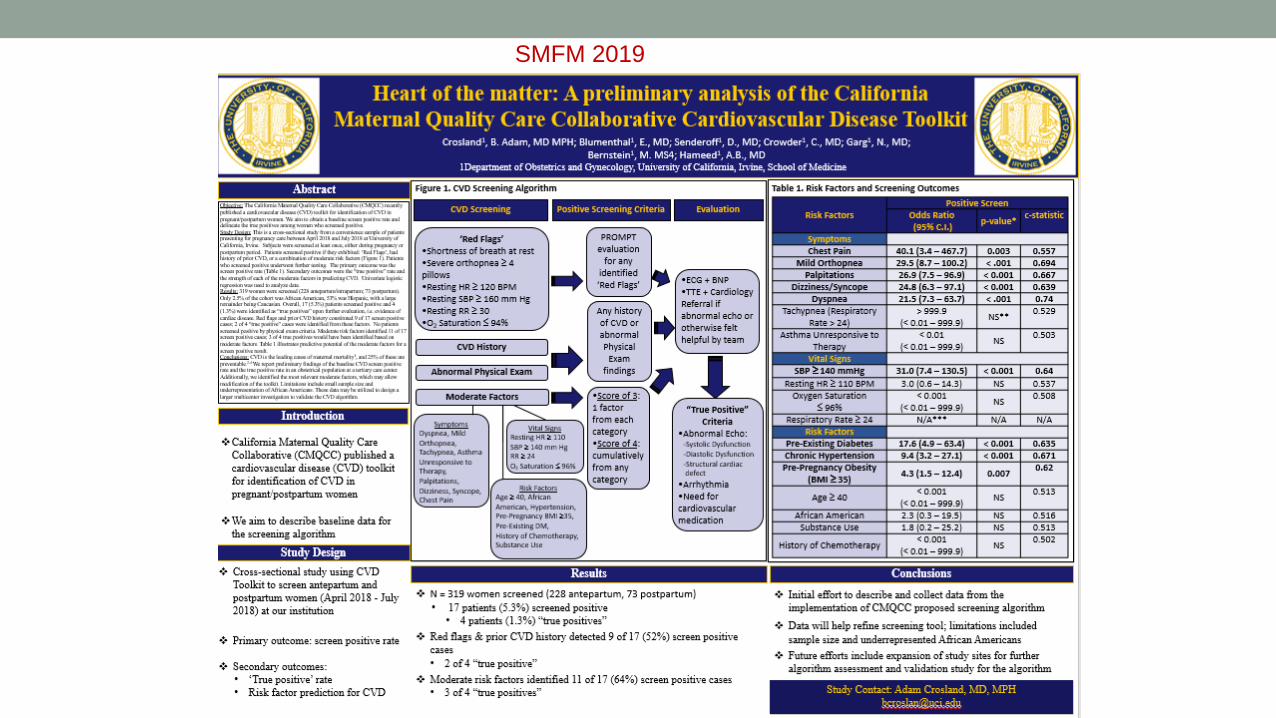
SMFM 2019

846 women screened
8% screen +
True + 1.5%
CVD confirmed in 30% of screen +
SMFM 2020
SMFM 2020


THE FUTURE: BROADER DISSEMINATION OF CVD SCREENING
Cardiovascular Disease Screening in Pregnancy – Role of the CMQCC Toolkit

DEVELOPING CARDIOVASULAR SCREENING MEASURES
FOR PREGNANT & POSTPARTUM WOMEN
KICK-OFF MEETING, SEATTLE, JAN. 10, 2020
Improving Diagnostic Excellence: Gordon and Betty Moore
Foundation
University of California, Irvine, Medical Center Health SystemsUCI Health 1,500 births a year, 3% black
Hameed/Thiel de Bocanegra/Crosland
University of California, San Diego, Medical Center Health SystemsUCSD Jacobs & Hillcrest 3,000 births a year, 5-6% black
Tarsa
University of Tennessee, St Thomas Health SystemsSt Thomas Health Systems 12,000 deliveries in 2018, 25% black
Graves

APPROACH
Integrate CVD algorithm into the EMR by placing and dot phrase with drop down menu
• Fill in the blanks in the dot phrase
• CVD screening added to problem list
Clinicians receive immediate score SCREEN POSITIVE
• Follow up imaging
• Follow up laboratory test
• Follow up consultations
Follow up monitored through EMR
Upload data to UCI RedCap
• Elicit feedback
• Review measures with the work group

Measures
1. CVD Risk Assessment =
Pregnant + postpartum women screened for CVD using algorithm
______________________________________________________
All pregnant + postpartum women seen at facility
2. CVD Risk Follow-up =
Women who received follow up for CVD risk
_____________________________________
Women who screened positive for CVD risk

Feasibility EvaluationAim of current study:
1. Demonstrate the feasibility to calculate meaningful and actionable
measures using data from the hospital wide network
- Potential to scale from pilot to system wide implementation
2. Explore whether the system wide administration of the measure will
produce a similar yield to that of the pilot studies
- Clinical and epidemiological value; important for business case

Summary
• Cardiovascular deaths are preventable
• 25% to 68%
• A large proportion of CVD deaths are beyond the 42 day
postpartum
• Most of the women who died of CVD have underlying risk
factors
• There is a need for universal screening for CVD to improve
maternal outcomes

For More Information and to
Download the
Toolkit
• Visit • www.cmqcc.org
• https://www.cdph.ca.gov
• Contact:[email protected]