Pregnancy and Subsequent Cardiovascular Risk
42
Pregnancy and Subsequent Cardiovascular Risk March 23, 2017 Joan Briller, MD FACC, FASE, FAHA Division of Cardiology [email protected] University of Illinois at Chicago
Transcript of Pregnancy and Subsequent Cardiovascular Risk

Pregnancy and Subsequent Cardiovascular Risk
March 23, 2017
Joan Briller, MD FACC, FASE, FAHA
Division of Cardiology
University of Illinois at Chicago

US Cardiovascular Mortality by Gender
Women’s Mortality Has Now Declined to be in Line With Men’s
Benjamin EJ et al. 2017 Circulation: 135:e1-e459

Pregnancy Adaptations Mimic Metabolic Syndrome
Insulin Resistance
Up-regulation of
Inflammatory
Cascade
Hyperlipidemia Hypercoagulable
State
Increased GFR

Pregnancy Complications Associated with CV Risk
CV Risk
Gestational Diabetes
Pre-eclampsia
Prematurity SGA
Gestational Hypertension

Gestational DM
• Normal pregnancy associated with insulin resistance
• Facilitates glucose transfer to fetus
• Failure to compensate for increased insulin resistance

GDM and Subsequent DM Risk
RR 7.43
Bellamy L et al. Lancet 2009; 373: 1773
20 studies 675 455 W 10 859 DM
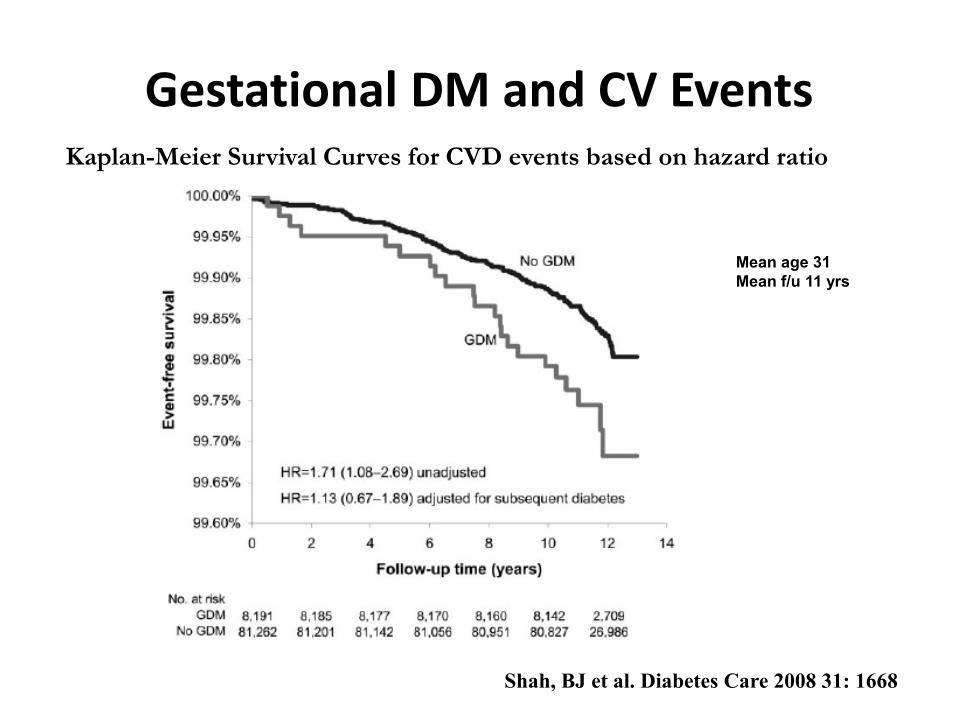
Gestational DM and CV Events Kaplan-Meier Survival Curves for CVD events based on hazard ratio
Shah, BJ et al. Diabetes Care 2008 31: 1668
Mean age 31
Mean f/u 11 yrs

Long Term Prognosis GDM
• Increased Type 1 and Type 2 DM
• ≥ 3 months post partum
– Abnormal post partum OGTT
– ↑ metabolic syndrome
– Atherogenic lipid profile
– Early vascular dysfunction
Russell et al. 2006 Obstet Gynecol 108: 1456; Retnakaran R et al. JClin EndocrinolMetab 2010; 95: 670; JClin EndocrinolMetab 2005; 90:4345; HeitritterSM et al. JClin EndocrinolMetab 2005; 90:3983
Myth: Risk Factors Improve

Prevalence GDM Illinois: 1989-2009
http://www.dph.illinois.gov/sites/default/files/publications/8-27-12diabetesburden.pdf Accessed Jan 15, 2017
Increased from 2.1 to 4.5%
Illinois PRAMS Facts 9.9% 2014

Chronic (Preexisting) Hypertension
Abnormal blood pressure predating pregnancy or before 20 weeks gestation
Gestational Hypertension
Abnormal blood pressure first developing in pregnancy
Preeclampsia
Gestational hypertension plus proteinuria
Superimposed Preeclampsia
Chronic hypertension with the development of preeclampsia
Postpartum Hypertension
New onset condition or persistent
Updated Classification of Hypertension in Pregnancy
Adapted from ILPQC hypertension toolkit 2016
2013 Illinois PRAMS data: — approx 11.1% pregnancies affected —16,338 women

Pre-Eclampsia and CVD Risk
Brown MC et al. EurJEpidemiol 2013 28: 1
> Doubles the Risk

Pre-eclampsia and CNS Risk
Brown MC et al. EurJEpidemiol 2013 28: 1
Almost Doubles Risk

Severity of Pre-Eclampsia and CVD Risk
0
1
2
3
4
5
6
7
8
MacDonald S et al. AmHJ 2008
Mild RR 2 Moderate RR 2.99 Severe RR 5.36
Mild Moderate Severe
Meta Regression 5 Case Control 10 Cohort Studies Pre-Eclampsia
111,175 W with Pre-eclampsia vs 2,259,579 W without

Pre-Eclampsia: Risk Factors Abn 1 yr PP
Pre-eclampsia Normotensive P value
Weight 77.3 71.8 <0.01
BMI 29 26 <0.01
% Obese 38.6 18.6 <0.05
MetSynd 18.6% 5.7% <0.05
BP systolic 120 111.3 <0.01
BP diastolic 81.5 72.2 <0.01
Glucose 4.93 4.81 NS
Insulin Level 63.6 44.7 <0.05
LDL Chol 2.71 2.37 <0.01
Smith, et al. AJOG 2009; 200:58
N = 140
Lost less weight Systolic BP higher Lipids less favorable More insulin resistance
Myth: Risk Factors Improve

Lifetime Cumulative Survival after Diagnosis Pre-Elampsia
Funai EF et al. Epidemiology 2005; Mar 16 (2): 206
No pre-eclampsia
Normal BP post pre-eclampsia
Pre-eclampsia unknown status

Gestational HTN and CV Risk
Gestational HTN
• HTN HR 2.7
– Younger age
• All CVD HR 1.59
• IHD HR 1.67
• MI HR 1.85
• MI death HR 4.49
• CHF HR 2.47
• CNS disease HR 1.67
• Increased DM, CKD
Männistӧ T et al. Circ 2013; 127:681


What’s the Link? Marker or Cause?
Shared Risk Factors
• Hypertension
• Diabetes
• Obesity
• Renal disease
• Family hx htn or dm
• African American
Potential Genetic Links
Shared Vascular Factors
• Pathologic lesions
• Endothelial dysfunction
• Vasomotor dysfunction

Intervention Opportunity
Sattar and Greer et al. BMJ 2002: 325(7356) 157

Adverse Pregnancy Outcomes Are Associated with increased CVD risk
• Predictive value rivals smoking and family history
• Predicts earlier than conventional screening tools
• 80% of women have a child
• ~ 30% women have adverse pregnancy outcome
• ~ 25% women have early CVD risk
Rich-Edwards, J et al 2014 36 Epidem Rev: 57


Screening Recommendations Risk Factor Initial Screen post partum Subsequent Screen
Hypertension 6 mo-1yr SBP 120-139 or DBP 80-90 screen annually BP < 120/80 every 2 year
Hyperlipidemia 12 weeks and post lactation Based on levels and ASCVD risk
Diabetes Within 6 weeks if GDM If IFG annually If hypertensive disorder annually Otherwise every 3 yrs
Obesity/BMI Annually Annually
Tobacco use Annually Annually
Nutrition First visit Each visit
Physical Activity First visit Each visit
Mehta PK et al. Seminars Perinatology 2015 39: 268
My Patient Failed the Stress Test: Now What?
• Primary prevention trumps secondary prevention

Lactation May Help
16.7
9.4 8.1 9.2 10.8
49.4
17.3 18.6
8.5
22.1
0-1month
>1-5months
6-9months
> 9months
All
Incidence Metabolic Syndrome at 20 y F/U
Non-GDM GDM
• CARDIA Study
• 704 Parous women (620 nonGDM, 84 GDM)
• Lactation associated with Risk Reduction metabolic syndrome
• Decrease in RR > in GDMs
Gunderson EP et al. Diabetes 2010 59:495
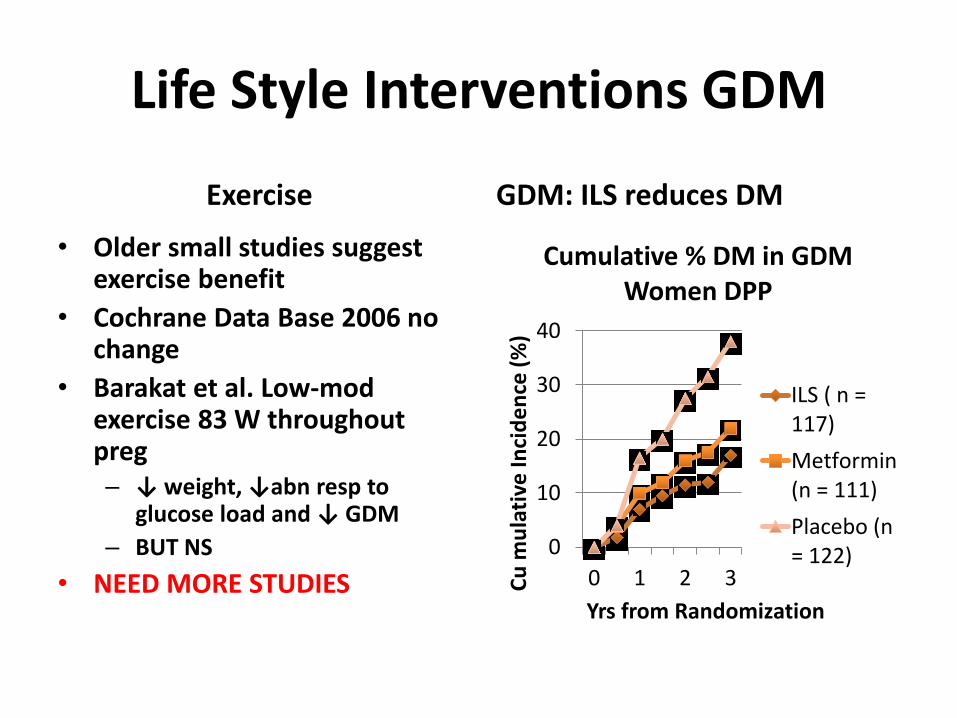
Life Style Interventions GDM
Exercise
• Older small studies suggest exercise benefit
• Cochrane Data Base 2006 no change
• Barakat et al. Low-mod exercise 83 W throughout preg – ↓ weight, ↓abn resp to
glucose load and ↓ GDM
– BUT NS
• NEED MORE STUDIES
GDM: ILS reduces DM
0
10
20
30
40
0 1 2 3Cu
mu
lati
ve In
cid
en
ce (
%)
Yrs from Randomization
Cumulative % DM in GDM Women DPP
ILS ( n =117)
Metformin(n = 111)
Placebo (n= 122)
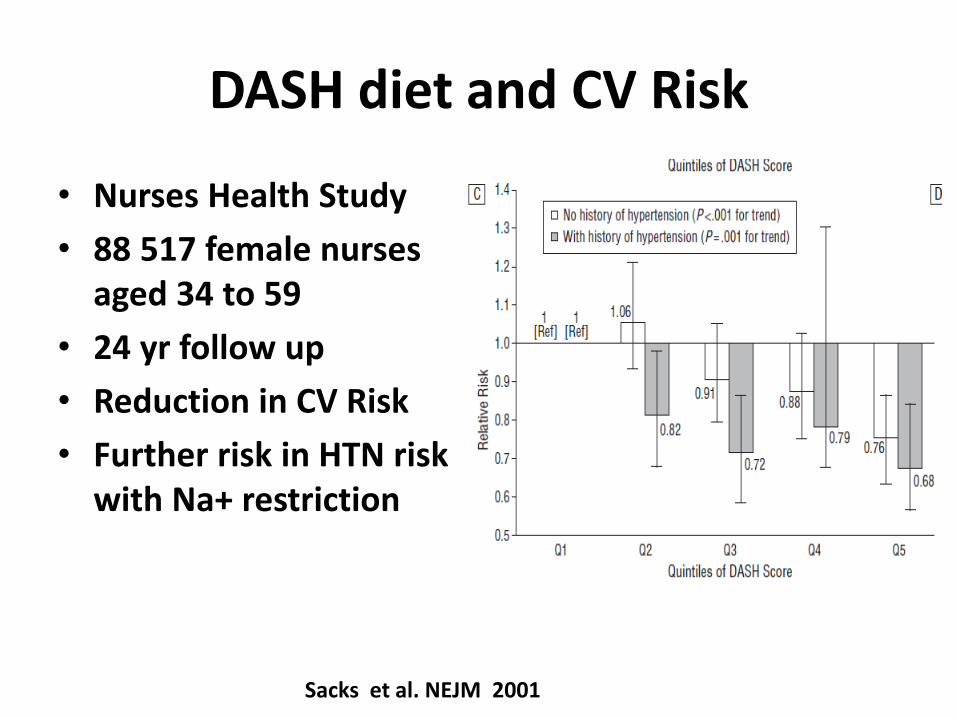
DASH diet and CV Risk
• Nurses Health Study
• 88 517 female nurses aged 34 to 59
• 24 yr follow up
• Reduction in CV Risk
• Further risk in HTN risk with Na+ restriction
Sacks et al. NEJM 2001

Lifestyle Intervention May Help
1.14 1.17
2.14
1.81 1.89
1.55
0.91 0.96
0
0.5
1
1.5
2
2.5
Cardiovascular Disease Stroke
Odds Ratio Risk Factors
Observed Odds RatioPre-Eclampsia
Attributable Odds RatioPre-eclampsia
Odds Ratio AfterLifestyle Intervention
Adapted from Berks D et al. BJOG 2013; 120: 924
CVD 0.91 Stroke 0.96

• No Data on Medical Therapy

Treatment for diabetes: Yes No
Smoker: Yes No
10 year Risk Lifetime Risk
Only calculated for 40-79 yo Calculated 39%; Optimal 8%
Male Female
White African-American
Other
Treatment for hypertension: Yes No
Total Cholesterol: 226 HDL Cholesterol: 46
Age: 33 Systolic BP:
136
2013 ASCVD Risk Predictor

Treatment for diabetes: Yes No
Smoker: Yes No
10 year Risk Lifetime Risk
Calculated 1.5%; Optimal 0.3% Calculated 39%; Optimal 8%
Male Female
White African-American
Other
Treatment for hypertension: Yes No
Total Cholesterol: 226 HDL Cholesterol: 46
Age: 40 Systolic BP:
136
2013 ASCVD Risk Predictor

Do We Counsel Appropriately?
• Framingham underestimates risk in women
• New ASCVD better but does not incorporate adverse pregnancy outcomes
• OB-Gyns: < 55% incorporate CVD prevention guidelines
• <10% internists, 38% counselled women with pre-eclampsia about increased risk
Mosca L et al Circ 2005: 111(4): 499; Young B et al. Hypertens Preg 2012 31(1): 50

Recognition of HTN: OB vs Medicine
Schmittdiehl J et al. Hypertension 2011 57 (4): 717

The MotHERS Program Mothers’ Health, Education, Research, Screening

Maternal Health Record
MotHERStm discharge package

Maternal Health Clinic
• Referred through standard post partum order sheets
• Calculated lifetime and 30 year risk
• Metabolic syndrome calculation
• Encourage lifestyle changes
Cuisamano MC et al. AmJAObstetGynecol; 210: 438 e1

CVD Risk Factor Profile
MHC Control
Life time risk
a. All optimal 16.3% 54.2%*
b. ≥ 1 elevated 20.7% 12.7*
c. ≥ 2 elevated 9.8% 0%*
30 year risk 7.5% 5.3%*
Metabolic syndrome 17.4% 6.8%**
* P < 0.0001; ** P < 0.05 Cusimano MC et al. AmJObstGynecol 2014; 210:438

MotHERS Programtm: Referrals
Specialty Service Referral Criteria
Cardiology 30 yr risk > 10%; lifetime risk > 39%; metabolic syndrome
Cardiac Rehab Discretion of cardiologist
Dietitian Discretion of cardiologist, rehab, FP
Endocrinology Abnormal glucose screen
Exercise Therapist Discretion of cardiologist, rehab, FP
Nephrologist Elevated urine albumin/creatinine ratio

MotHERS Programtm: Lifestyle Links

https://www.cmqcc.org/resource/cvd-risks-infographic-english-pdf accessed 2/22/17

How Do We Get There
• Need More Data
• Education/communication
– Training across disciplines
– Include h/o adverse pregnancy outcomes in screening women for CVD risk
– Counsel women with adverse outcomes about increased risk
– Healthy lifestyle

THANK YOU

Strategies for Improved Diet
• Educational campaigns
• Nutritional labeling
• Lower pricing healthy foods
• Campaigns in schools and workplaces
• Local environmental changes increase availabilty of healthy foods
• Restrictions on unhealthy foods
Estruch R and Ros E JACC 2017 69: 1113; Mozaffarian D et al. Circ 2012 126: 1514












![Heart Disease and Pregnancy - Home - Springer › content › pdf › 10.1007 › s40119-017-0096-4.pdfand delivering safely [1]. However, pregnancy has a profound effect on the cardiovascular](https://static.fdocuments.net/doc/165x107/5f10c7c87e708231d44ac85d/heart-disease-and-pregnancy-home-springer-a-content-a-pdf-a-101007-a.jpg)