Cardiovascular Diseases on Pregnancy
38
Fetomaternal Division Obstetrics & Gynecology Department Dr. Soetomo General Hospital S U R A B A Y A CARDIOVASCULAR DISEASES ON PREGNANCY dr. Aditiawarman,SpOG
-
Upload
pogisurabaya -
Category
Health & Medicine
-
view
187 -
download
0
Transcript of Cardiovascular Diseases on Pregnancy
Fetomaternal Division
Obstetrics & Gynecology Department
Dr. Soetomo General Hospital
S U R A B A Y A
CARDIOVASCULAR DISEASES
ON
PREGNANCY
dr. Aditiawarman,SpOG
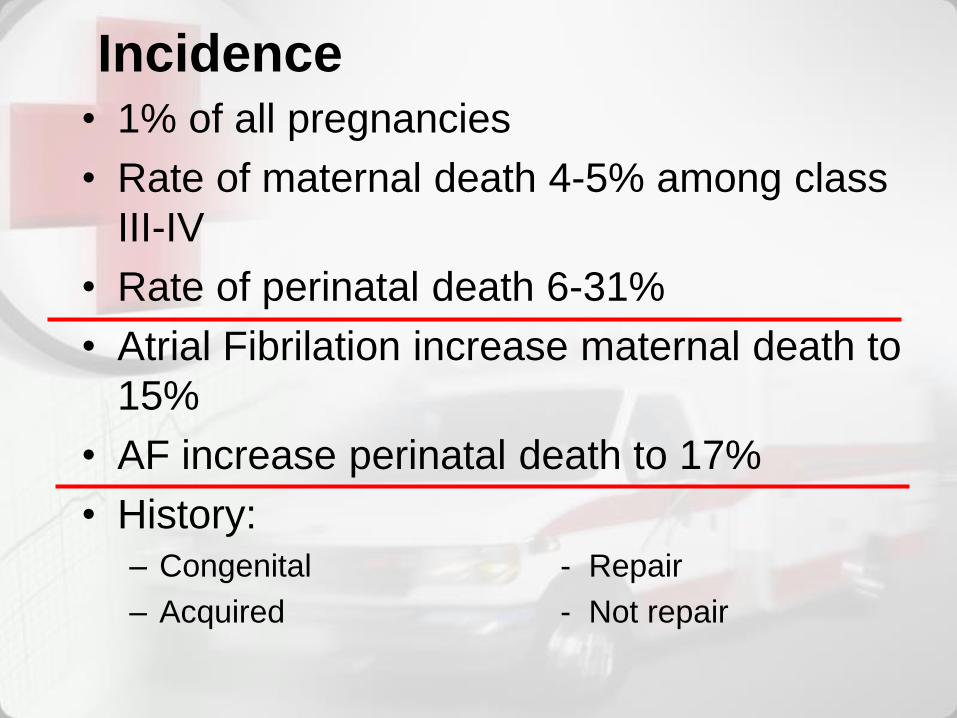
Incidence• 1% of all pregnancies
• Rate of maternal death 4-5% among class
III-IV
• Rate of perinatal death 6-31%
• Atrial Fibrilation increase maternal death to
15%
• AF increase perinatal death to 17%
• History:– Congenital - Repair
– Acquired - Not repair
• Cardiac disease in pregnancy complicates a
small percentage of all pregnancies in
developed countries (eg, only 1 to 4 percent
of pregnancies in the United States
• Congenital heart disease the most
common form of heart disease complicating
pregnancy in the United States
advances in the treatment of congenital
heart disease more affected children to
reach adulthood and attempt pregnancy
• Rheumatic heart disease was the most
common form of cardiac disease in pregnant
women predominates in developing
countries and in immigrant populations in the
United States
0
5
10
15
20
25 24
7
12
2
4 4
1
4
1
7
1 1
2
1
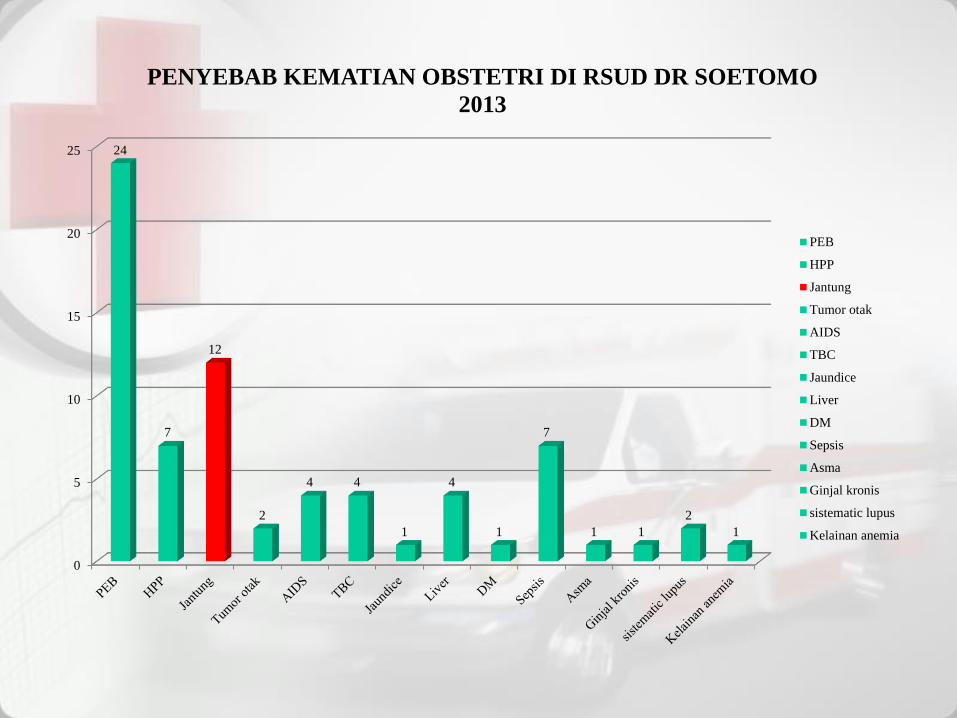
PENYEBAB KEMATIAN OBSTETRI DI RSUD DR SOETOMO
2013
PEB
HPP
Jantung
Tumor otak
AIDS
TBC
Jaundice
Liver
DM
Sepsis
Asma
Ginjal kronis
sistematic lupus
Kelainan anemia
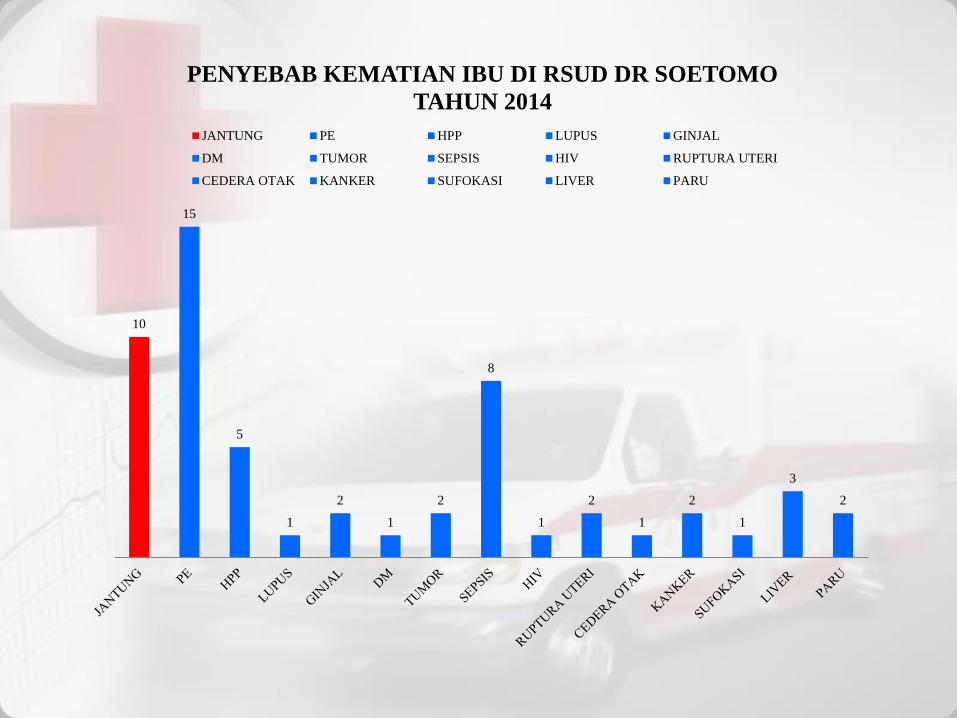
10
15
5
1
2
1
2
8
1
2
1
2
1
3
2
PENYEBAB KEMATIAN IBU DI RSUD DR SOETOMO
TAHUN 2014
JANTUNG PE HPP LUPUS GINJAL
DM TUMOR SEPSIS HIV RUPTURA UTERI
CEDERA OTAK KANKER SUFOKASI LIVER PARU
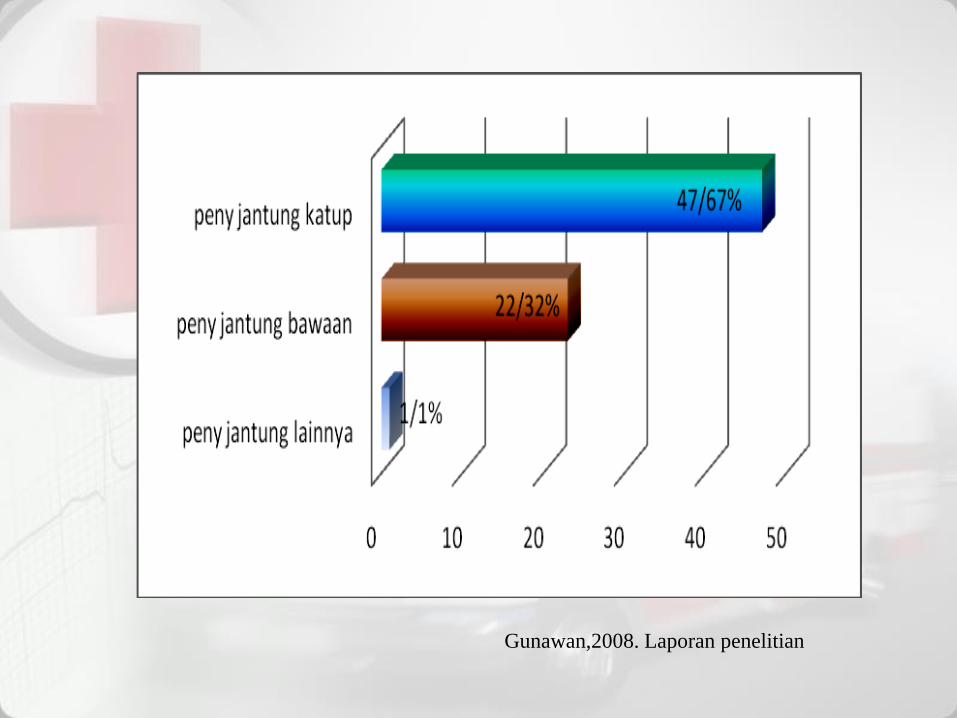
Gunawan,2008. Laporan penelitian
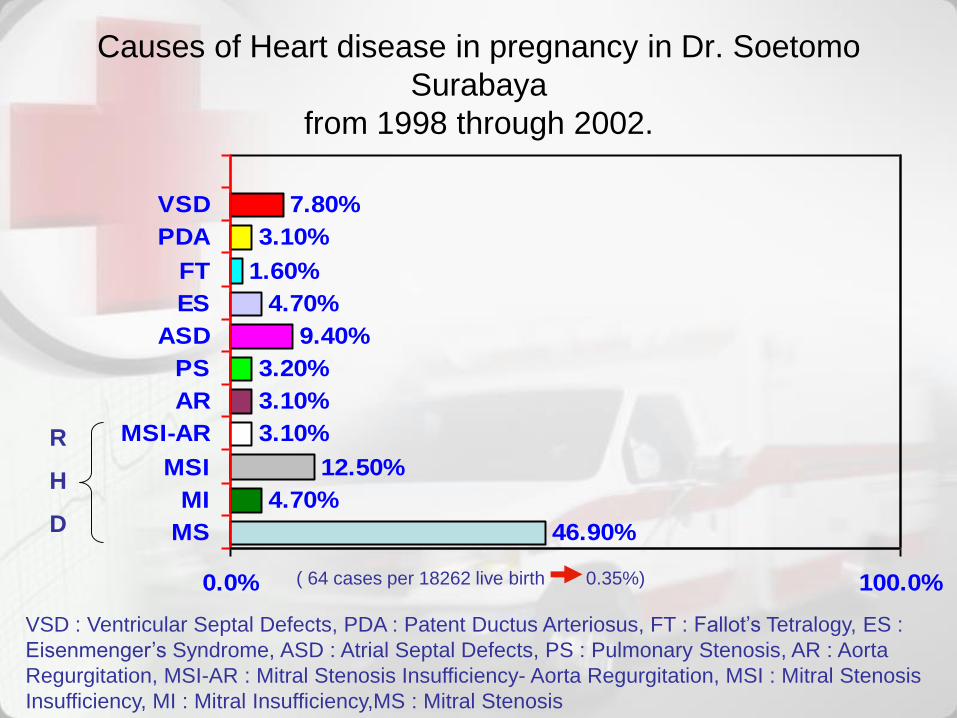
Causes of Heart disease in pregnancy in Dr. Soetomo
Surabaya
from 1998 through 2002.
46.90%
4.70%
12.50%
3.10%
3.10%
3.20%
9.40%
4.70%
1.60%
3.10%
7.80%
0.0% 100.0%
MS
MI
MSI
MSI-AR
AR
PS
ASD
ES
FT
PDA
VSD
R
H
D
VSD : Ventricular Septal Defects, PDA : Patent Ductus Arteriosus, FT : Fallot’s Tetralogy, ES :
Eisenmenger’s Syndrome, ASD : Atrial Septal Defects, PS : Pulmonary Stenosis, AR : Aorta
Regurgitation, MSI-AR : Mitral Stenosis Insufficiency- Aorta Regurgitation, MSI : Mitral Stenosis
Insufficiency, MI : Mitral Insufficiency,MS : Mitral Stenosis
( 64 cases per 18262 live birth 0.35%)
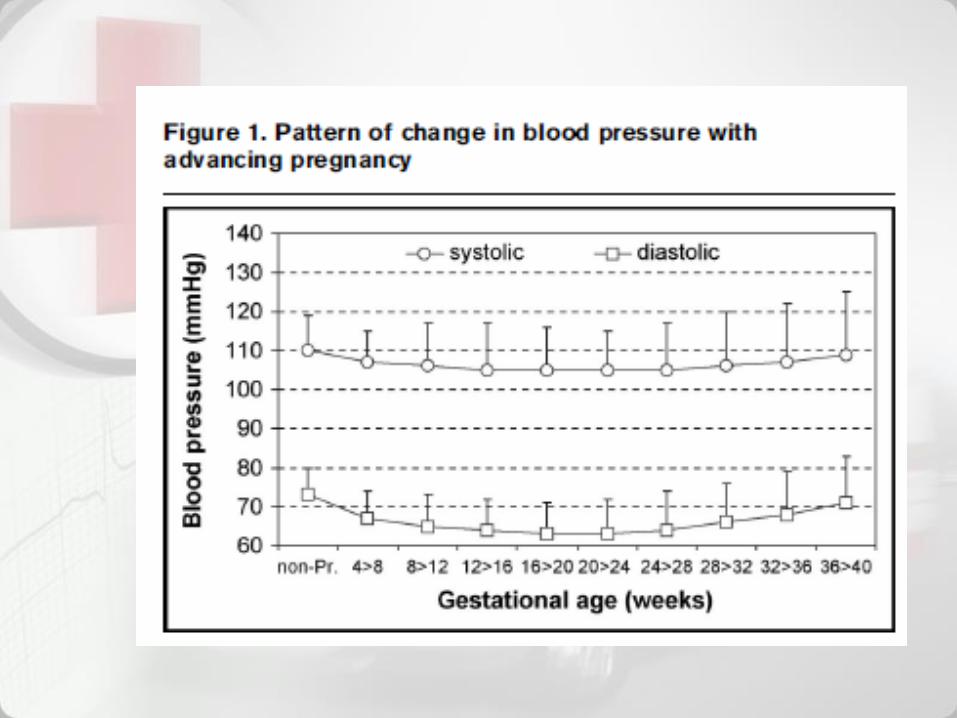
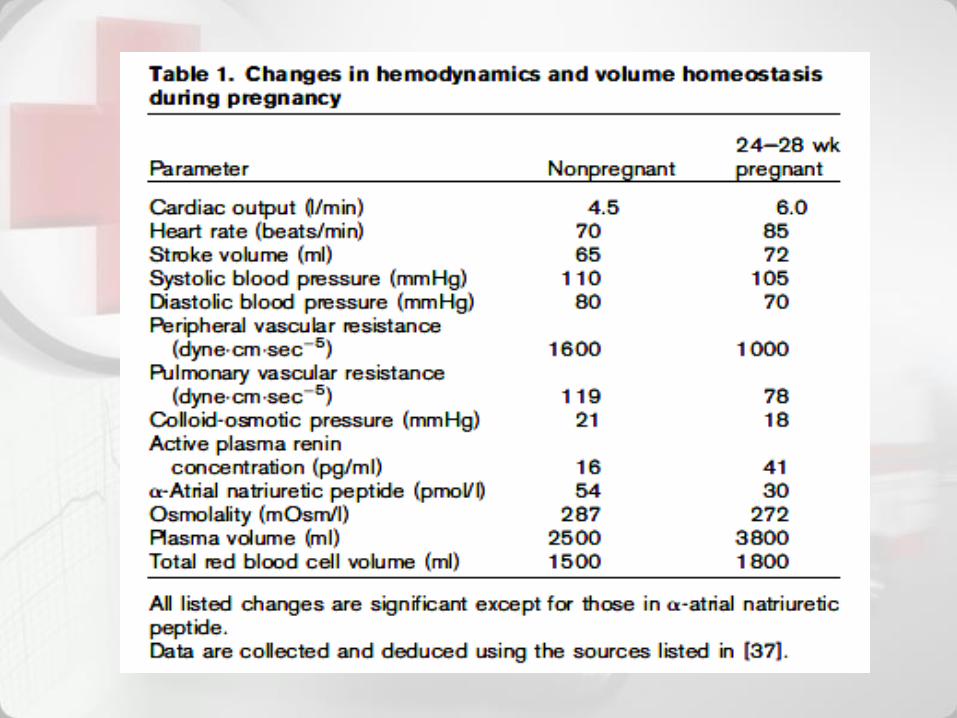
Hemodynamic changes
maternal neonatal survival• Premarital counseling
• Pre conceptional counseling
• Antenatal care
• Family planning
START
Pregnancy stimulate the marked
hemodynamic changes have profound
effect on underlying heart disease.
1.Increased cardiac out put 30 to 50%
2.Increased resting pulse
3.Increased diastolic filling
PHYSIOLOGICAL
CONSIDERATION
Cardiac disease
• Congenital heart disease
–Acyanotic
–Cyanotic
• Acquired
–RHD
• Others:
–Coronary heart disease
Symptoms
Progressive dyspnea or orthopnea
Nocturnal cough
Hemoptysis
Syncope
Chest pain
Some Clinical Indicators of Heart
Disease During Pregnancy

Clinical Findings
– Cyanosis
– Clubbing of fingers
– Persistent neck vein distention
– Systolic murmur grade 3/6 or greater
– Diastolic murmur
– Cardiomegaly
– Persistent arrhythmia
– Persistent split-second sound
– Criteria for pulmonary hypertension
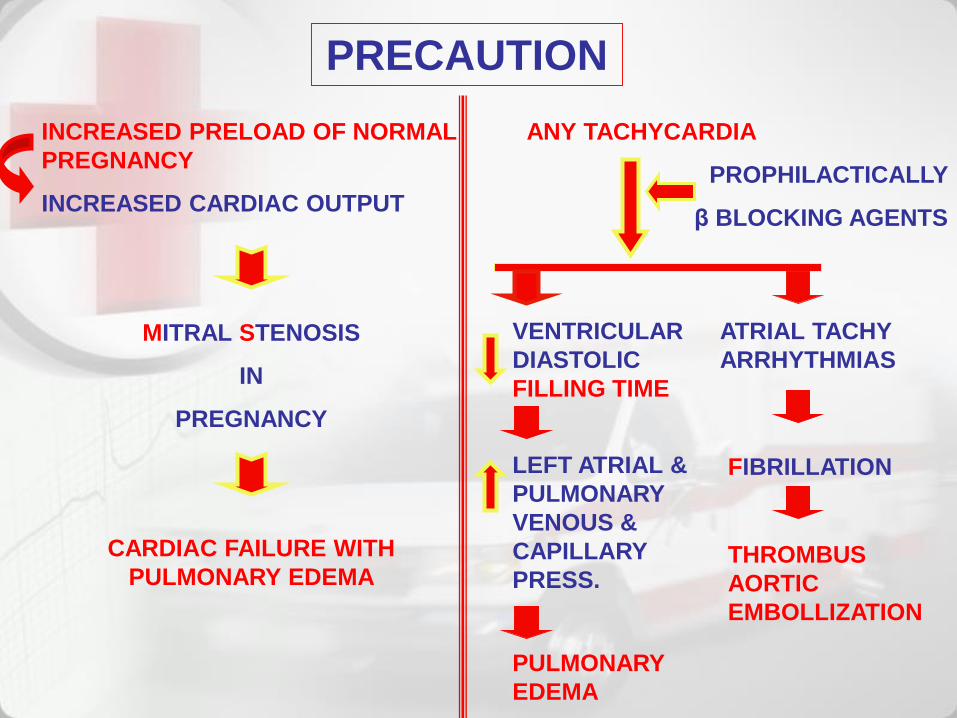
PRECAUTION
INCREASED PRELOAD OF NORMAL
PREGNANCY
INCREASED CARDIAC OUTPUT
MITRAL STENOSIS
IN
PREGNANCY
CARDIAC FAILURE WITH
PULMONARY EDEMA
ANY TACHYCARDIA
PROPHILACTICALLY
β BLOCKING AGENTS
VENTRICULAR
DIASTOLIC
FILLING TIME
ATRIAL TACHY
ARRHYTHMIAS
LEFT ATRIAL &
PULMONARY
VENOUS &
CAPILLARY
PRESS.
PULMONARY
EDEMA
FIBRILLATION
THROMBUS
AORTIC
EMBOLLIZATION
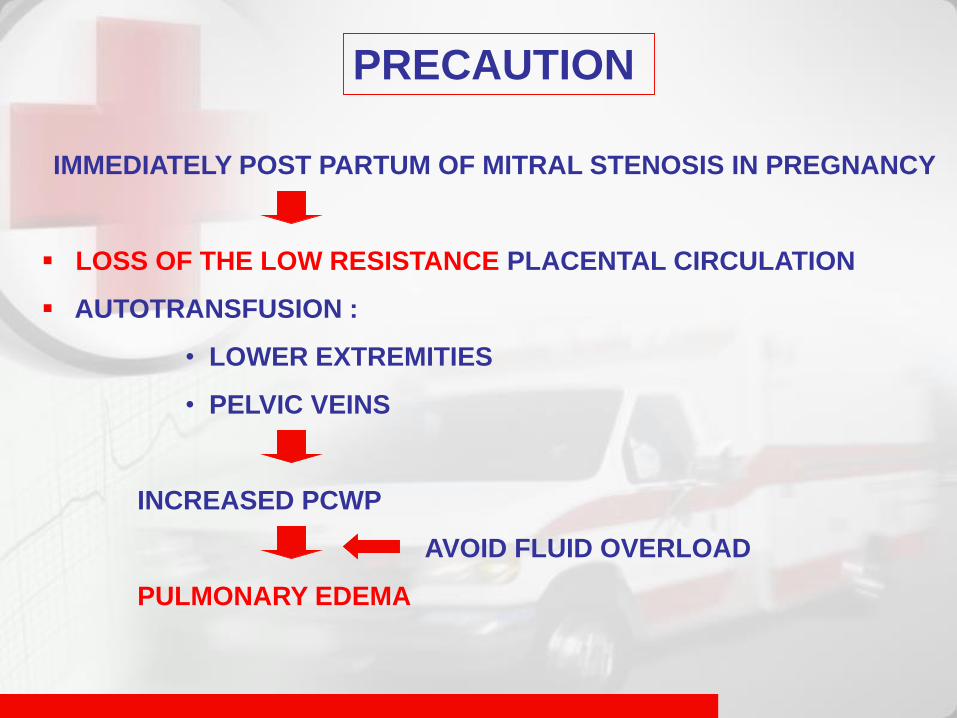
IMMEDIATELY POST PARTUM OF MITRAL STENOSIS IN PREGNANCY
LOSS OF THE LOW RESISTANCE PLACENTAL CIRCULATION
AUTOTRANSFUSION :
• LOWER EXTREMITIES
• PELVIC VEINS
INCREASED PCWP
AVOID FLUID OVERLOAD
PULMONARY EDEMA
PRECAUTION
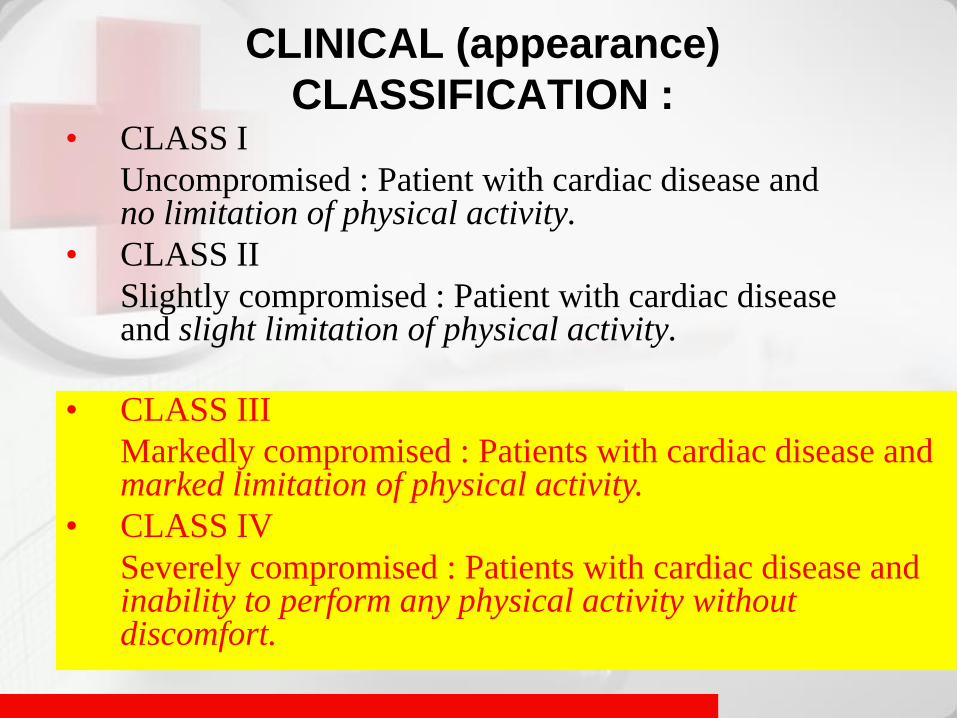
CLINICAL (appearance)
CLASSIFICATION :• CLASS I
Uncompromised : Patient with cardiac disease and no limitation of physical activity.
• CLASS II
Slightly compromised : Patient with cardiac disease and slight limitation of physical activity.
• CLASS III
Markedly compromised : Patients with cardiac disease and marked limitation of physical activity.
• CLASS IV
Severely compromised : Patients with cardiac disease and inability to perform any physical activity without discomfort.
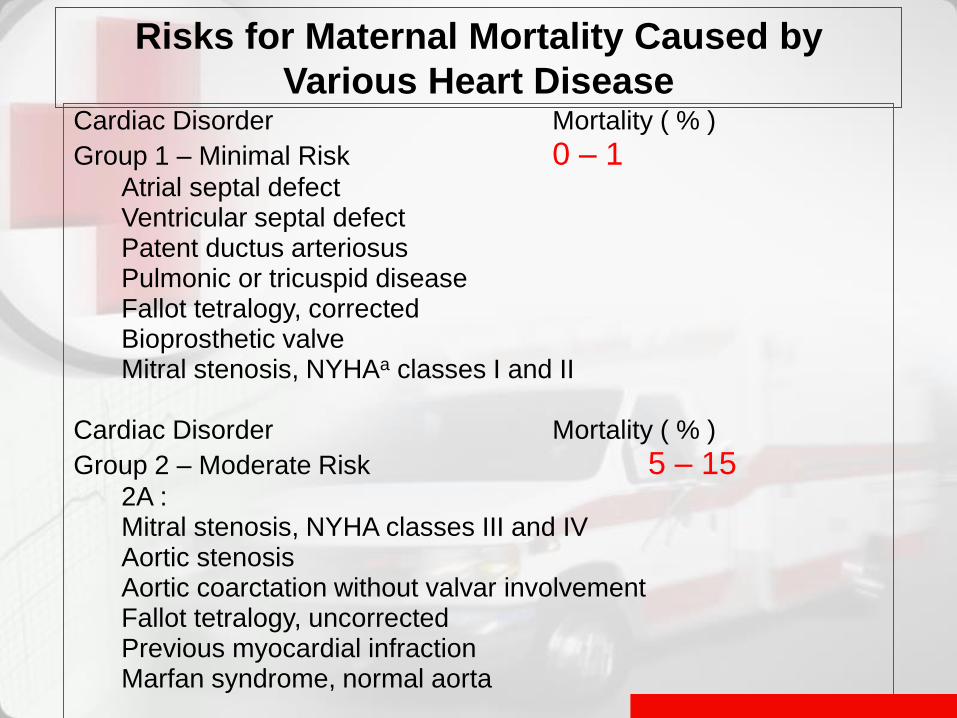
Risks for Maternal Mortality Caused by
Various Heart DiseaseCardiac Disorder Mortality ( % )
Group 1 – Minimal Risk 0 – 1 Atrial septal defectVentricular septal defectPatent ductus arteriosusPulmonic or tricuspid diseaseFallot tetralogy, correctedBioprosthetic valveMitral stenosis, NYHAa classes I and II
Cardiac Disorder Mortality ( % )
Group 2 – Moderate Risk 5 – 15 2A :Mitral stenosis, NYHA classes III and IVAortic stenosisAortic coarctation without valvar involvementFallot tetralogy, uncorrectedPrevious myocardial infractionMarfan syndrome, normal aorta
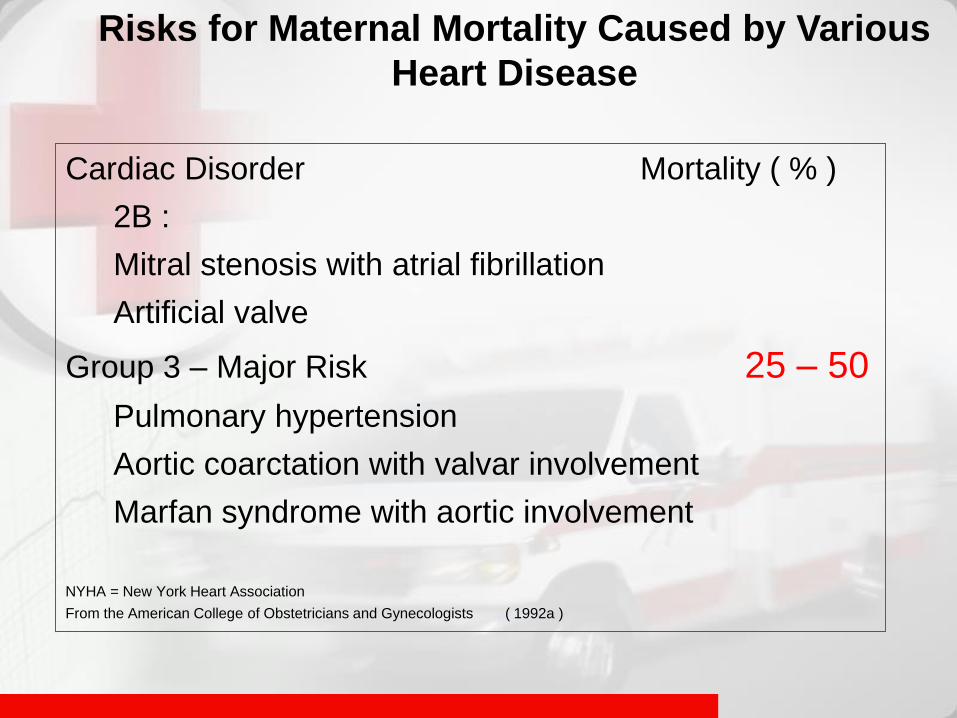
Risks for Maternal Mortality Caused by Various
Heart Disease
Cardiac Disorder Mortality ( % )
2B :
Mitral stenosis with atrial fibrillation
Artificial valve
Group 3 – Major Risk 25 – 50
Pulmonary hypertension
Aortic coarctation with valvar involvement
Marfan syndrome with aortic involvement
NYHA = New York Heart Association
From the American College of Obstetricians and Gynecologists ( 1992a )
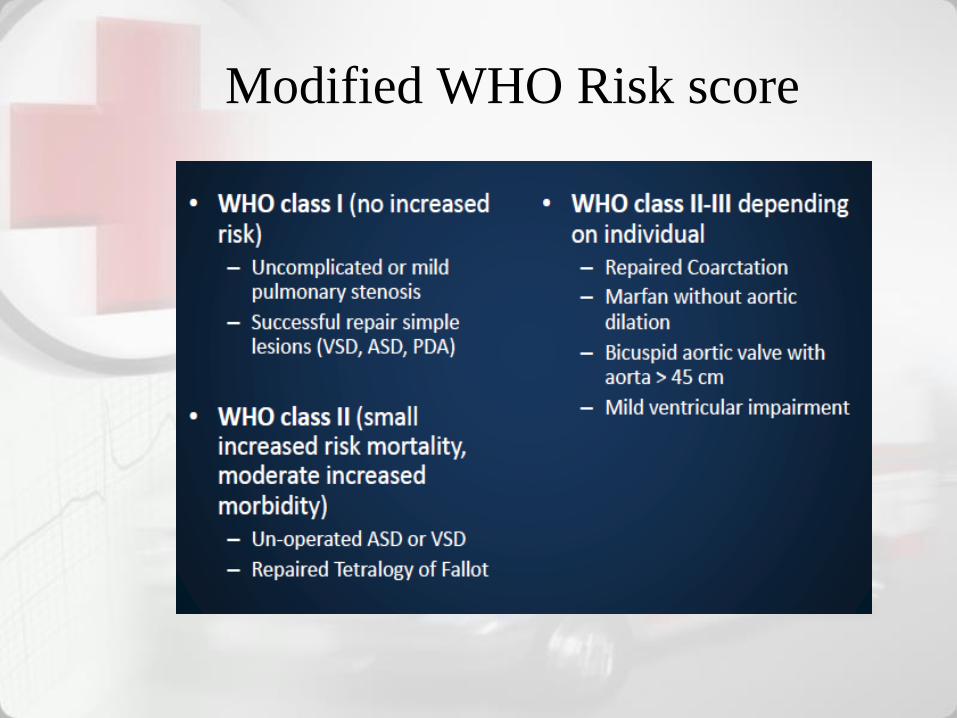
Modified WHO Risk score
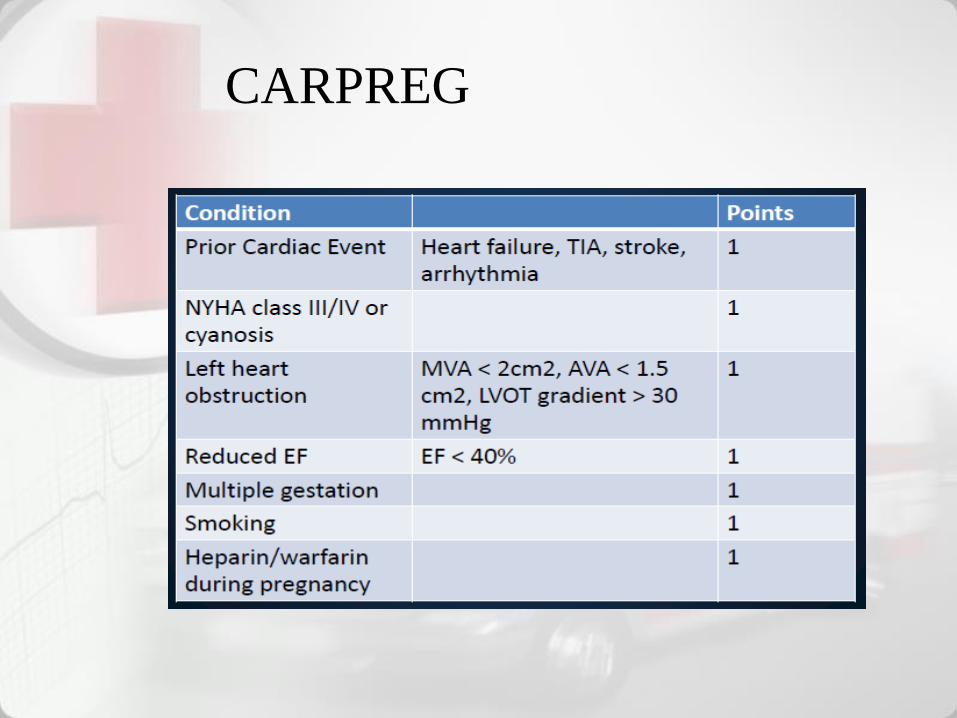
CARPREG
Risk of maternal cardiovascular
complication:
Heart failure, arrhythmia, death
0 points 5%
1 point 27%
2 points 75%
Risk of offspring higher with higher
score no percent assigned
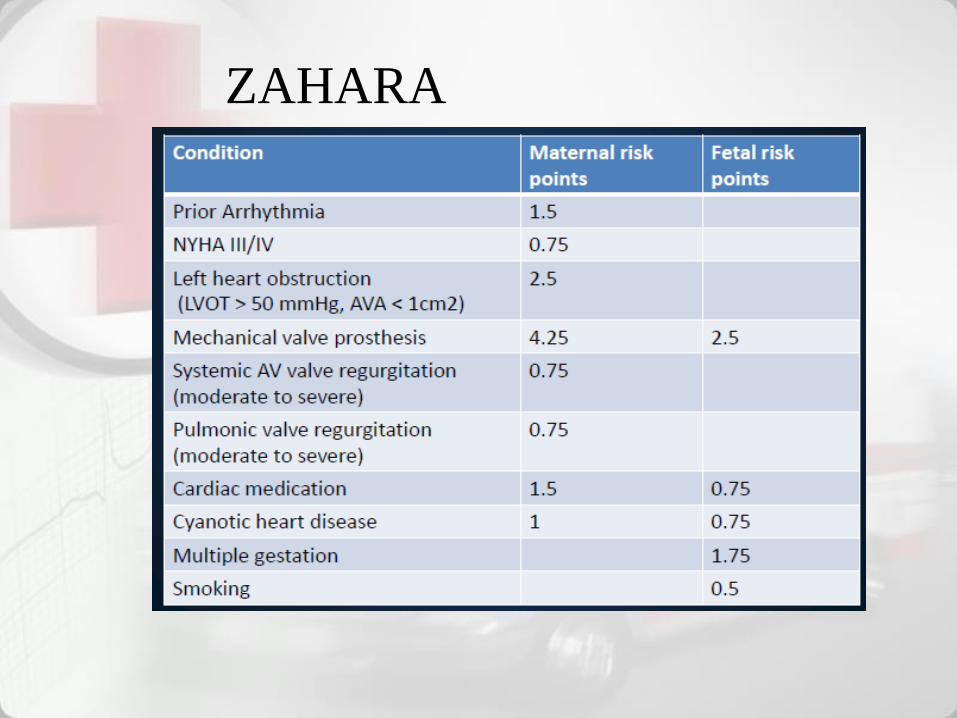
ZAHARA
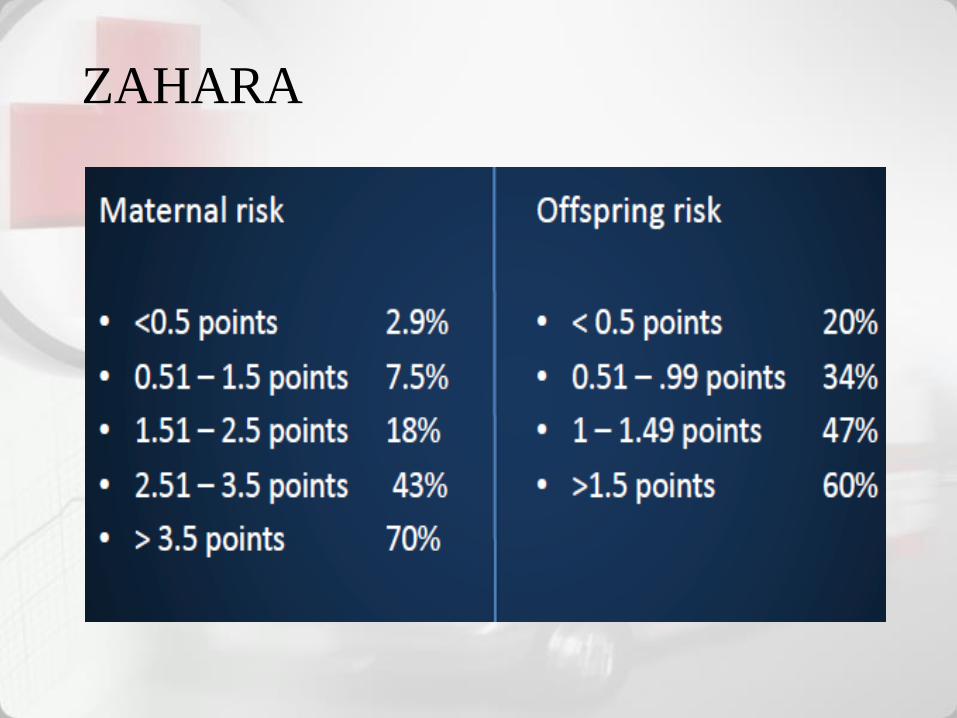
ZAHARA
Management
• Counseling
• Rest
• Team approach
• Infection prevention –
Endocartitis;Rhematoid
• Delivery
• Diet
• Family Planning
PRE CONCEPTIONAL COUNSELING
Preconceptional Counseling :
• Is preventive medicine for obstetrics
• All factors that could potentially affect maternal and perinatal outcome are identified, the woman is advised of her risk, and a strategy is provided to reduce or eliminate the pathological influences made evident by her family, medical, or obstetrical history and/or specific testing.
PRECONCEPTIONAL COUNSELING
• The women with significant heart diseases may benefit from counseling before the decision to become pregnant
• Maternal mortality generally varies directly with functional classification at pregnancy onset
• Wowen with a significant risk of mortality should be advised to reconsider pregnancy
• Evaluation of cardiac function, surgical records are reviewed, all medications evaluated for fetal safety and pedigree should be obtained to define the fetal risk
Normal clinical findings that can
mimic heart disease in pregnancy
• Raised jugular venous pressure .
• Volume-loaded left ventricle; full, sharp and collapsing
pulse
• Warm extremities
• Peripheral edema
• Palpitations
• Tachycardia
• Premature atrial/ventricular beats
• Increased intensity of mitral closure sound
• Third heart sound
• Systolic murmur
• Continuous murmur from venous hum, mammary soufflé
Management
• Multidiscipline approach obstetricians, cardiologist, anesthesist, pediatriacians
• Cardiology:– Medical
– Surgical
• Mode of delivery– Vaginal
– CS
• Anesthesia– Painless labor
Multidiscipline team
Management in pregnancy
• Cardiac disease + pregnancy are managed by a
Multidisciplinary team.
• This includes:
– Cardiologist with expertise in pregnancy or obstetric
physician;
– Obstetrician or fetal medicine specialist;
– Midwives with experience in medical problems;
– Obstetric anaesthetist; and
– Neonatal paediatrician.
Poor Prognosis
• Poor functional class (poor exercise
tolerance);
• Previous cardiac event (arrhythmia,
pulmonary oedema, stroke);
• Left heart obstruction.
Mitral Stenosis and PTMC
• Rheumatoid fever Mitral
stenosis 2 years
• Maternal death
– 75% cardiac failure
– 3rd trimester or early postpartum
Post PTMC experiences dr
Soetomo
• Maternal mortality 2-3%
• IUGR 1 of 7 babies with birth weight
less 2500 gram
• None IUFD

Terima kasih