Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes

of 16
-
Upload
mike-scarlett -
Category
Documents
-
view
226 -
download
0
Transcript of Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
1/16
R E V I E W A R T I C L E Sports Med 2010; 40 (6): 493-6070112-1642/10/(XX)6-0493/S49 96/0 2010 Adis Data In farmot ion BV Aii r i ghts reserved.
Physical Activity and PregnancyCardiovascular Adaptations, Recommendations and PregnancyOutcomesKatarina Melzer}'^ Yves Schutz^ Michel Boulvain^ and Bengt Kayser^1 Institute of Mo vem ent Sciences and Sports Med icine, Faculty of Medicine, University of Geneva, Geneva,Switzerland2 Department of Obstetrics and Gynaecology, University Hospitals of Geneva, Faculty of Medicine,University of Geneva, Geneva, Sw itzerland3 Department of Physiology, U niversity of Lausanne, Lausanne, Switzerland
ContentsAbstract 4931, Cardiovascular Adaptations to Training and Detraining in Pregnant and Nonpregnant States , , , , 495
1.1 Cardiovascular Adaptations to Training 495.,2 Cardiovascuiar Adaptations to Detraining 495
2, Cardiovascuiar Changes due to Pregnancy 4962.1 Cardiovascular Ci^anges during Labour and Deiivery 4962.2 Postpartum Cardiovascular Cinanges 497
3, Piiysicai Activity and Pregnancy 4973.1 Submaximai Aerobic Capacity during Pregnancy 4973.2 Wori< Efficiency 4983.3 Maximum Aerobic Capacity during Pregnancy 4983.4 Maximai Heart Rate during Pregnancy 4984, Pir/sical Activity Recommendations during Pregnancy 4984,1 Recommended iHeart Rate Target Zones for Aerobic Exercise in Pregnancy 500
5, Compiiance witi i Pi ysicai Activity Recommendations during Pregnancy 5006, Effects of Phvsicai Activity on Pregnancy Outcomes 5017, Conclusions 503
A bstract Regular physical activity is associated with improved physiological, meta-bolic and psychological param eters, and with reduced risk of morbidity andmortality. Current recommendations aimed at improving the health and well-being ofnonpreg nant subjects advise that an accumulation of>30 minutes ofmoderate physical activity should occur onmost, if not all, days of the week.Regardless of the specific physiological changes induced by pregnancy,which are primarily developed to meet the increased metabolic demands ofmother and fetus, pregnant women benefit from regular physical activity thesame way as nonpregnant subjects.Changes in submaximal oxygen uptake (VO2) during pregnancy dependon the type of exercise performed. During maternal rest or submaximalweight-bearing exercise (e.g. walking, stepping, treadmill exercise), absolute
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
2/16
494 Melzer
maternal VO2 is significantly increased com pared with the nonpr egna nt stateThe magnitude of change is approximately proportional to maternal weighgain.When pregnant women perform submaximal weight-supported exerciseon land (e.g. level cycling), the findings are contradictory. Some studies reported significantly increased absolute VO2, while many others reportedunchanged or only slightly increased absolute VOT compared with the nonpregnant state. The latter findings may be explained by the fact that themetabolic demand of cycle exercise is largely independent of the maternabody m ass, resulting in no ab solute VO2 alteration.
Few studies that directly measured changes in maternal maximal VO2(V02niax) showed no difference in the abso lute V02max between preg nan t andnonpregnant subjects in cycling, swimming or weight-bearing exercise. Efficiency of work during exercise appears to be unchanged during pregnancy innon-weight-bearing exercise. During weight-bearing exercise, the work efficiency was shown to be improved in athletic women who continue exercisingand those who stop exercising during pregnancy. When adjusted for weightgain, the increased efficiency is maintained throughout the pregnancy, withthe improvement being greater in exercising women.
Regular physical activity has been proven to result in marked benefits formother and fetus. Maternal benefits include improved cardiovascular function, limited pregnancy weight gain, decreased musculoskeletal discomfortreduced incidence of muscle cramps and lower limb oedema, mood stability,attenuation of gestational diabetes mellitus and gestational hypertensionFetal benefits include decreased fat mass, improved stress tolerance, andadvanced neurobehavioural maturation. In addition, few studies that havedirectly examined the effects of physical activity on labour and delivery in-dicate that, for women with normal pregnancies, physical activity is accom-panied with shorter labour and decreased incidence of operative delivery.
However, a substantial proportion of women stop exercising after theydiscover they are pregnant, and only few begin participating in exerciseactivities during pregnancy. The adoption or continuation of a sedentarylifestyle during pregnancy may contribute to the development of certain dis-orders such as hypertension, maternal and childhood obesity, gestationaldiabetes, dyspnoea, and pre-eclampsia. In view of the global epidemic ofsedentary behaviour and obesity-related pathology, prenatal physical activitywas shown to be useful for the prevention and treatment of these conditionsFurther studies with larger sample sizes are required to confirm the associa-tion between physical activity and outcomes of labour and delivery.
Re gular physical activity is associated with the health and well-being of no np reg na nt simprov ed physiological, metab olic and psyc ho- jects advise tha t an accu mu lation of 30 minulogical p ara me ters, and with reduced risk of or mo re of m ode rate physical activity should mo rbidity and m orta hty from diseases such as cur on mo st, if not all, days of the week.'^'card iovas cular disease, hype rtension , diabetes Rega rdless of the specific physiological ch
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
3/16
Physical Activity and Pregnancy 495
from regular physical activity the same way asnonpregnant subjects.'^^' However, a substantialproportion of women stop exercising and de-crease their general physical activity level afterthey discover they are pregnant, and only fewbegin participating in exercise or sport activitiesduring pregnancy.''*' The adoption or continua-tion of a sedentary lifestyle during pregnancymay contribute to development of certain dis-orders such as hypertension, maternal and child-hood obesity, gestational diabetes, dyspnoea andpre-eclampsia.'-^' In view of the global epidemic ofsedentary behaviour and obesity-related patho-logy, prenatal physical activity has been shown tobe useful for the prevention and treatment ofthese conditions.'^'A systematic literature review was conductedon physical activity and pregnancy. The searchincluded articles published in MEDLINE and ISIWeb of Science databases. Keywords used were:'physical activity' OR 'physical exercise', 'preg-nancy' OR 'gestation', 'pregnancy outcomes','labour', 'cardiovascular ada ptations', 'heart rate','training', 'detraining', 'physical activity recom-mendations' AND 'pregnancy'. In a first round,there were no restrictions to certain yearsof publication. In a second round, publicationspublished between 2007 and 2009 were specifi-cally reviewed to assure inclusion of any relevantnew publication.The aim of this article was to review the cur-rent state of knowledge on (i) the cardiovascularadaptations to physical activity in the pregnantand nonpregnant states; (ii) the compliance ofpregnant women with current physical activityrecommendations; and (iii) the effects of physicalactivity on pregnancy outcomes.
1 . Card iovasc ular A dapta tions to Trainingan d Detraining in Pregnant a ndNonpregnant States1.1 Cardiovas cular Ad apta tions to TrainingRepeated episodes of physical activity per-formed over a longer period (i.e. training) causeadaptations in the respiratory, cardiovascularand neuromuscular systems that enable physi-
cally trained persons to exercise for longer ata given absolute exercise intensity, or to ex-ercise at a higher exercise intensity for a givenduration.'^' The adaptations in metabolic andphysiological systems depend on the type of ex-ercise overload imposed. Short dura tion activitiesdemanding high levels of anaerobic metabohsmfavour the adaptation of the immediate andshort-term energy systems, with limited impacton the aerobic system. Regular endurance train-ing, on the other hand, improves overall aerobiccapacity.'^"'^1For public health concerns and in contrast totraining for sports-specific improvement, currentinterest in physical activity participation ariseslargely from a desire to improve health-relatedfitness components, primarily cardiorespiratoryfitness.''"' Aerobic training produces significantchanges to the cardiovascular system: enlargedleft ventricular cavity of the heart; enhancedblood and stroke volume; increased maximumcardiac output (Q); and decreased resting and sub-maximal exercise heart rate.'^'' The lower restingand sub-maximum exercise heart rate generallyreflect an improved submaximal and maximaloxygen uptake (VO2max) and a correspondinglyhigher level of cardiovascular fitness.
1,2 Cardiovascular Adaptations to DetrainingWhile regular physical activity is accompaniedby better cardiovascular fitness, a reduction orcessation of physical activity leads to partialor complete reversal of the physiological adap-tations. Inactivity is accompanied by a rapiddecline in VO^max and blood volume. Conse-quently, submaximal exercise heart rate increasesbut insufficiently to counterbalance decreasedstroke volume, thus resulting in a reduction of
maximal Q.'"' Measurable alterations in physio-logical functions take place after only a week ortwo of detraining.'**! Total loss of training im-provements occurs within several months.'**' As aresult, any sudden physical effort imposed on thedetrained subjects leads to physiological andmetabolic stress, as they are not able to respondto imposed physical exertion as efficiently astrained subjects. 2010 Adis Dat a in form at ion BV. All r ights reserved. Sports Med 2010; 40 (6)
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
4/16
496 Melzer
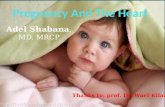
2. Cardiovascular Changes due toPregnancyRegardless of training status, women who be-come pregnant undergo profound cardiovascularsystem a lteration s (figure 1). The first haem ody -namic change during pregnancy is a rise in heartrate, both at rest and during submaximal work-out. It starts between 2 and 5 weeks of pregnanc yand continues well into the third trimester.I'^^ Onaverage, the resting heart rate raises 8 beats/minby the eighth week, and reaches an increase of
16 beats/min by the end of pregnancy.' '^' The ef-fect is less evident in supine or lateral positionsand more evident during sitting.'"'*' The mechan-ism of the increased heart rate is not yet clearlyidentified. It may be attributed to cho rionic go na-dotropin, or to sympathetic reflex adjustments tomaintain arterial blood pressure despite reducedperipheral vascular resistance.' ' ' ' 'Between 10 and 20 weeks of pregnancy, a no-table increase in blood volum e takes place due to an
increase in both plasma and e rythrocytes.' '*'^^ Thisrepresents a rise of approximately 1500mL,' '^ ofwhich 1000 m L is plasma volume and 500 m L iserythrocytes.t'**' Since plasma volume amplifiesmore than red blood cell volume, a relative dilu-tional anaemia occurs.'"' Blood volume expansionmay be even greater in multifetal gestations.' '^'Res ting Q is increase d as early as the fifth weekof pregnancy as a result of the increased heart
rate, stroke volume and blood volume.' '^-Resting Q increases by 1 L/min at 8 weeks of ation, which represents >50% of the ovechange in pregnancy.'^' During the third trster, resting Q increases only minimally, primily because of the increase in heart rate as tapproaches.'-^'I In multifetal pregnancies, resmaternal Q is greater by approximately 2com pared with singleton preg nan cies . '" ' Q is affected by the positional changes of women.''"' After 20 weeks of gestation, the gruterus may obstruct the aorta and inferior vcava, causing a decrease in uteroplacental blflow and venous return to the heart, ' ' ' especiwhen the woman is in the supine position. left lateral position quickly relieves compresof the inferior vena cava.'*'' Left uterine placement also tends to prevent aortocaval cpression, although it is less optimal than the lateral position.''**'
Blood pressure is not increased in norpregnancy due to decreased peripheral vascresistance.''^1 In fact, systolic pressure remquite stable, whereas diastoiic pressure decreup to 15 mm Hg in '
2.1 Cardiovascular Changes during Laboan d DeliveryAlthough Q remains relatively constant inlatter half of pregnancy, there is a signifi
Increase in resting and Increase in resting andsub-maxim al heart rate
Descrease inblood pressure Increase in plasma an dred blood cell massregnancy-inducedcardiovascular changes
ncrease in blood volume
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
5/16
Physical Activity and Pregnancy 497
increase during active labour and immediately afterdelivery. A study' '^ ' of normal labour in womenwithout epidural anaesthesia repo rted an increasein Q of 12% and 34% between co ntractions and atfull dilatation, respectively. The increase in Qseems to be caused by an increase in heart rateand stroke volume. Such changes are thought tobe sympathetically mediated and are likely due tothe combined effects of pain, increased metabolicdemand and increased venous return duringuterine contractions.'*"*' Circulating blood vol-ume also increases during contractions by anadditional 300-500 mL due to blood au to-transfusion from the placenta.'-"*'
The physical effort of normal labour doesnot impose high energy demands on the parturi-ent. The energy requirement is affected more bythe frequency and duration of uterine contrac-tions than by the total duration of labour.'^^'Katz et al. measured energy expenditure of la-bou r in 23 healthy women.'^-^' Th e results showedoxygen uptake (VO2) of 0.255 L/min during uter-ine relaxation (at 4 cm dila tatio n), 0.338 L/minduring con tractions (at 4 cm dilatation), and0.510 L/min at delivery. Th us , the VO2, wh ichincreases -20% during normal pregnancy, mayincrease an additional 60% during the contrac-tions, but remains rather low when comparedwith the increase observed during physical ac-tivity (walking, running, cychng). It is higher inmultiparous women than in nulliparous womenand is highest in those women with the shortestlabour.'-^) If the process of expulsion is pro-longed (>30 minutes), the increased demand foroxygen is partially met by anaerobic metabolismcausing an increase in maternal blood lactate
'25'The haemodynamic changes seen during la-bour and delivery are infiuenced by anaestheticand analgesic techniques. ' - ' ' Lumbar epiduralanaesthesia during labour reduces maternaladrenaline (epinephrine) levels, '^^' and decreasesthe work of breathing, VO2,'"'^**' fetal heartrate,'^'' ' maternal Q and blood pressure.'-'O"-^-' Thehaem odyna mic changes are also influenced by theposit ion of the parturient. For example, Q andstroke volume are significantly decreased in thesupine, compared with the lateral, position.'-'-^'
2.2 Postpartum Cardiovascular ChangesWithin the first 15-20 minutes after deliveryof the fetus and placenta there is a substantialincrease in Q, as the blood is no longer divertedto the uteroplacental vascular bed, but ratherredirected to the maternal circulation. '- ' ' By24 hours after delivery, Q is no longer signifi-cantly different from pre-labour values,'^'*' andfully returns to pre-pregnant values by 2 weeksafter delivery. Stroke volume also decreaseswithin 2 week s, altho ugh there is a further smallreduction up to 6 mo nths after d elivery.' '^ '3. Physical Activity a nd PregnancyAlthough pregnancy induces an increase in Q,stroke volume and heart rate, women who con-tinue aerobic exercise training during pregnancyhave lower resting heart rate and higher strokevolume than matched sedentary controls.'-^''-^^' Inaddition, aerobically fit women have greater VO2response at a given heart rate compared withtheir sedentary counterparts. '-^^'3.1 Submaximal Aerobic Ca pa city duringPregnancyChanges in submaximal VO2 during preg-nancy depend on the type of exercise performed.During maternal rest or submaximal weight-bearing exercise (e.g. walking, stepping, treadmillexercise), absolute maternal VO2 (L/min) is signi-ficantly increased compared with the nonpreg-nant state.'-^^-^**' The magnitude of change isapproximately proportional to maternal weightgain. At the same speed or grade of walking orrunnin g, the values for VO2 expressed in mL/kg/minare thus similar or only slightly higher duringpregnancy compared wi th the nonpregnant'"3'4"When pregnant women perform submaximaweight-supported exercise on land (e.g. level cycling), where the energy cost of locomotion is notaltered by maternal morphological changes, thefindings are contrad ictory. S ome studies reportedsignificantly increased absolute V02,' '^' ' '' ' '^while many others''5-''^-^'*''*"'*''-4^' reported unchanged or only slightly increased absolute VO2
2010 Adis Data in form at ion BV. All r ights reserved. Sports Me d 2010; 40 (6
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
6/16
498 Melzer e
compared with the nonpregnant state. The lat terfindings may be explained by the fact that themetabolic demand of cycle exercise is largely in-dependent of the maternal body mass, result ingin no absolute VO2 alteration.
3.2 Work EfficiencyNet efficiency of work during exercise, i.e. theslope of the relationship between VO2 and workrate, appears to be unchanged during pregnancyin non-weight-bearing exercise (e.g. cycle ergo-
m eter testing).i- '*-'*'''**'! The efficiency of weig ht-bearing exercise (e.g. treadmill testing), on theother hand, was shown to be improved in earlypregnancy in athletic women who continue ex-ercising and those who stop exercising duringpregnancy.''*'^-''"' The increase in exercise efficiencyis obscured after the fifteenth week of pregnancyby pregnancy-associated increases in maternalweight. When adjusted for weight gain, the in-creased efficiency is m aintain ed th rou gh ou t thepregnancy, with the improvement being greater inwomen who continue exercising during preg-nancy.'^' '3.3 Maximum A erobic C ap acity duringPregnancy
2max' as a criterion measure of cardio-vascular fitness, is poorly documented in preg-nancy . M easu ring VO2max during gestation holdsa theoretical risk of inducing fetal stress due toblood distribution favouring maternal skeletalmuscle at the expense of uterine blood flow. Forethical reasons, most studies report estimatedvalues obtained by extrapolating individual sub-maxim al heart rate-VO2 curves rather than actualmeasured values at peak exercise intensity. Thefew studies (table I) that directly measuredchanges in maternal VO2max showed no differ-ence in the VO2max (L/min) between pregnant andnonpregnant subjects in cycling,'''^''*^-^*'"-''-^! swim-ming or weight-bearing exercise.'"*^-^"-^''''' Wellcondit ioned women or athletes who maintain amoderate to high level of exercise during and
training effect in well conditioned, recreatiosports women.
3,4 Maximal Heart Rate during Pregna ncyAlthough the V02max values do not seemdiffer significantly in the preg nan t com pare d wthe nonpregnant state, maximal heart rate wreported to be approximately 4 beats/min lowin pregnancy compared with post partum.'^"' Tblunted heart rate responses to maximal exercmay be due to reduced sympathoadrenal r
ponses to heavy exertion during pregnancy.'"*^As a result of the increased resting heart rate adecreased maximal heart rate, heart rate reservereduced and heart rate rises to a lesser extent wincreasing VO2, lowering the slope of the heart raVO2 relationship during pregnancy compared wthe nonpregnant state.' '^-'*'' However, with the ception of resting heart rate, the change in the herate-V02 relationship appears not to be afiecsignificantly by a woman's habitual exercise beviour throughout pregnancy.'"'*!
4. Physical Activity Recommendationsduring PregnancyIn the past , recommendations for physical tivity were based on cultural and traditiomores rather than scientific evidence. In 1950s, continuation of household chores and1.6 km (1 mile) walk per da y, pre ferably divid
into several short sessions, was advised, whersports and exercise were discouraged.'"'1 In 19the American College of Obstetricians and Gycologists (ACOG) formulated one of the firecommendations for exercising during prnanc y. It was advised th at the intensity of exercshould not induce an increase in heart rate abo140 beats/m in an d tha t stren uou s exercise shono t last m or e th an 15 minutes.'-' ' Since th en , edence has accumulated on the type, intensiduration and frequency of exercise beneficial mother and offspring,'^*' leading to the revisiof the guidelines.
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
7/16
Physieal Activity and Pregnancy 499
Table I. Studies reporting actual mea sured maxim al oxygen uptake (V02max) n pregnant w omenStudy (year) No. otsubjects
Measurements Findings
Heenan et al. l" ' 14(2001)
Lotgering et a l . l== ' l 33(1991, 1992)
McMurray et al. l ^l 10(1991)
Sady et aLl^^l(1988)
45
Sady et al.!"" ' 45(1989)Spinnewijn et al.'""'' 11(1996)
VO2 (Umin) measurements in pregnant women(350.4wk) and age-matched nonpregnant controlgroup (n = 14) while cycling m aximally. Low age-specitic aerobic capacity levelsVO2 measurements (L/min) at 16, 25 and 35 wk otpregnancy and 7 wk post partum at increasing levelsof cycling and treadmill exercise until maxim umaerobic power was reached . Average age-specificaerobic capacity levelsV02 m easurements (Um in) at 25- 35 wk of pregnancyand 9-11 wk post partum during cycling andswimming maximally. Average age-specific aerobiccapacity levelsVO2 (L/min) measurem ents in pregnant women(26 3 wk) and a nonpregnant control group (n = 10)while cycling maximaily. Low age-specific aerobiccapacity levelsVO2 (Umin) measurements at 26 3 wk of pregnancyand 8 2 wk post partum while cycling m aximally. Lowage-specific aerobic capacity ievelsVO2 measurements (L/min) at 30-34 wk of pregnancyand 8-12 wk post partum during cycling andswimming maximaily. Average age-specific aerobiccapacity levels
No significant differences in V02max in pregnantvs control group
No significant differences inpregnancy period vs post partum during cyclingand treadmill exercise
No significant differences inpregnancy period vs post partum during cycling.The swim V02max was significantly greater postpartum than in the 35th swim triaisNo significant differences ivs control group
x in pregnant
No significant differences in VO2max inpregnancy period vs post partumNo significant differences in V02max inpregnancy period vs post partum during bicycleand swimming
2 = oxygen uptake.
Canadian Society of Exercise Physiology(CSEP),' '**' advise that pregnant women who arefree of medical or obstetric complications followthe American College of Sports Medicine-Centers of Disease Control and Prevention(ACSM-CDC) guidelines for physical activityand exercise. According to these guidelines,pregnant women may safely engage in >30 minutesof moderate physical activity on most, if not all,days of the week.' '^' Moderate physical activity isdefined as an activity performed at an intensity ofthree to six metabolic equ ivalents (ME Ts), whichcorrespo nds to brisk w alking at - 5 -7 km/h(3-4 mph ). ' ' '' ! Previously sedentary w omen shouldstart with 15 minutes of continuo us exercise threetimes a week, increasing gradually to 30-minutesessions four times a week.' **' Th e aim of exercisingduring pregnancy is to maintain a good conditionwithout trying to reach a peak fitness level.'^**'
Because of the potential risk of certain activ-ities, healthcare professionals should adapt theexercise prescriptions accordingly, prescribing
activities such as walking, swimming, stationarycycling and aquafit rather than gymnastics,horseback riding, skiing, racquet sports or con-tact sports. The risks of injury associated withfalling are increased in latter activities due to in-creased levels of oestrogen and relaxin, whichaugment l igamentous laxity and hypermobi-lj(y [54.60] pg]vic su pp or t be lts an d c ore stab ilityexercise can be used to enable women to remainactive in spite of these changes. In addition,muscle conditioning (light weight-lifting in mod-erate repetitions) is suggested to maintain flex-ibility and muscle tone, prevent gestational lowerback pain, and promote general conditioning. '*' 'Ab do min al streng thenin g is difficult to per-form due to the development of diastasis rectiand associated abdominal muscle weakness.' ' ' '*For that reason, pregnant women should avoidexercising in the supine position after ~16 weeksof gestation. Scuba diving is also to be avoidedthrou gho ut pregnanc y, as the fetus is not protectedfrom deco mp ression sickness an d g as embolism.'- '^
2010 Adis Data inform at ion BV. Aii r ig i its reserved. Sports Me d 2010. 40 (6
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
8/16
500 Melzeret
Exertion at a ltitudes abov e 2500 m (8250 feet) isadvised only after 4-5 days of exposure and accli-matization to such high altitudes.'*^'Metabolic responses during exercise in preg-nancy are related to the duration and intensityof exercise. Blood glucose of pregnant womendecreases at a faster rate and to a significantlylower level post-exercise than in nonpregnantwomen.'' ' ' '1 This decrease does not seem to causehypoglycaemia, even after 40 minutes of moder-ate walking or aerobic dancing.'^''' '^' However,consuming adequate calories and l imiting ex-ercise sessions to
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
9/16
Physieal Activity and Pregnancy 501
Table III. Borg's rating ot perceived exertion' (reproduced fromDavies et al.. '^* ' with permission from the Society of Obstetriciansand Gynaecologists of Canada)Borg's rating of perceived exertion
67 Very, very light89 Somewhat light
1011 Fairly light1213 Somewhat hard1415 Haid1617 Very hard1819 Very, very hard20a A rating of 12-14 is appropriate for most pregnant wom en.
with physically strenuous professions are morelikely to stop working during the last trimester ofpregnancy than women working in less physicallydem and ing occupations.'**'' 'The decrease in activity-related energy ex-penditure during pregnancy can be observed inboth the developed and the developing world.Compared wi th nonpregnant women, energyexpended on physical activity during pregnancyis decreasing, on avera ge, by 233 kcal/day (20%)at 30 weeks in Sw eden,'^*' 201 kca l/day (22%) at25 weeks and 240 kcal/day (23%) at 35 weeks inColom bia,'"! and 103 kcal/day (13%) at 38 weeksin Switzerland.'^"'As a result , few women reach the recommen-ded physical activity (>30 minutes of moderatephysical activity on most, if not all, days of theweek) during pregnan cy. In the U S, only 16% ofpregnant women comply with the physical ac-tivity recommendations, compared with 26% ofnonpregnant women. '" ' Even heal thy, otherwiseactive women decrease physical activity due topregnan cy. For examp le, 70% of women living inSwitzerland complied with the recommendationsduring pregnancy compared with 89% in thenonpregnant state. '"- '
6. Effects of Physical Activity onPregnancy O utcomesThe influence of physical activity on preg-nancy outco mes is widely debated. Traditionally,pregna nt w omen were advised to reduce their lev-els of physical activity. This advice was based onconcerns that exercise would affect pregnancyoutcomes by raising core body temperature, byincreasing the risk of maternal musculoskeletalinjury due to changes in posture, centre of gravityand ligamentous laxity, and by moving transportof oxygen and nutrients to maternal skeletalmuscle rather than to the developing fetus.'^'*'In the meantime, research has provided a sig-
nificant amount of new information about how apregnant woman and her fetus respond to regularengagement in moderate physical activity. '" ' 'New investigations have shown no adversematernal or neonatal outcomes, no abnormal fe-tal growth and no increase in early pregnancy lossor late pre gn anc y complications.'- **'On the contrary, regular physical activity hasproven to result in marked benefits for motherand fetus. Maternal benefits include improvedcardiovascular function, l imited pregnancyweight gain,'"'*' decreased musculoskeletal dis-comfort , ' ' ' reduced incidence of muscle crampsand lower limb oedema,'**"' mood stability'**^-"''and attenuation of gestational diabetes and ge-stational hypertension.'"' ' ' Fetal benefits includedecreased fat mass, improved stress tolerance,and advanced neurobehavioural maturation. '"^'The most common fetal response to maternalexercise is alteration in fetal heart rate. The fetalheart rate was reported to increase in the im-mediate post-exercise period, and to be correlatedwith both duration and intensity of maternalexercise.' '^"**' Increases in maternal core tempe-rature and maternal-fetal transfer of catechola-mines have been reported as causes of post-exercisefetal tachycardia. '""' Transient decrease in fetalheart rate was also reported during mild ormoderate intensity exercise or in studies involvinghigh intensity maternal exertion.'"^-""' Reduceduterine blood flow caused by a rapid post-exercise fall in Q was postulated as a cause of thebradycardia, although firm physiological bases
2010 Adls Data Inform at ion BV. All r ights reserved. Sports Me d 2010: 40 (6)
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
10/16
502 Melzer e
for these changes are still lacking.'^'l Despite theoverall alterations of fetal heart rate due tomaternal exercise, no abnormal birth outcomeshave been noted in healthy women undergoing anormal pregnancy.''^''!Only a few studies so far have directly examinedthe effects of physical activity on labour and deliv-ery. One of them was performed by Clapp'"'"' on131 well conditioned recreational athletes. Thosewho co ntinued to exercise at or abo ve 50% of theirpre-pregnancy performance level throughoutpregnancy had a lower incidence of operative
abdominal and vaginal deliveries and fewer fetuseswith acute fetal distress in labour. Erdelyi''"'! re-ported that among 172 Hungarian athletes, thefrequency of caesarean section was almost 50%lower than in a control group of 184 non-athletes.Even sporadic exercisers, who participatedin a structured exercise programme for at least1 hour, twice weekly for a minimum of 12 weeksduring pregnancy, were more likely to have aspontaneous vaginal delivery than their non-
exercising coun terparts.' '"^' Hall and Kau fma nn''"^'studied 845 pregnant women who were given theoption to part icipate in exercise programmesdesigned specifically for pregnant women. Theyreported that the incidence of caesarean deliverywas 6.7% in the high-exercise group (women whocompleted 64 exercise sessions [range 60-99]during pregnan cy), compa red with 28.1% in thesedentary group (0.8 sessions [range 0-10] duringpregnancy) [p30 minutesof moderate physical activity per day on preg-nancy outcomes in 44 healthy Swiss women. Ac-tive women had a lower risk of operative deliverycom pared with inactive wom en (odds ratio =3.67; 95 % CI 1.02, 13.1). Ad justm ent for pa rity,maternal weight gain and infant weightstrengthened the association between lack ofphysical activity and operative delivery (adjustedod ds rati o = 7.65; 95% CI 1.27, 45.84).Prior studies showed a strong correlationbetween length of labour and physical fit-ness [100-102,104.105] Penttinen and Erkkola,""' on
no significant difference in labour duration tween recreationally active women and thcontrols. Lastly, maternal exercise has been ported to increase,'"^-^-'"'^-""' decrease''""' or hno effect'^'*' '"^'"'-"^' on newborn birthweightThe inconsistent results on the effects of ercise on the newborn's birthweight may due to the differences in type, timing, frequeand duration of the exercise regimen impo(table IV). Clapp et al ." '^ ' demonstrated twomen who begin a regular, modera te regimenweight-bearing exercise (treadmill, step aero
or stair stepper) in early pregnancy (for 20 minu3-5 times per week) gave birth to larger newbbirthweights compared with non-exercising mthers. Other studies further indicated that womwho stayed active throughout the pregnancy aexperienced improved fetal growth. '" ' - '" '"^Physical activity during pregnancy may thusan important mechanism for improving placenfunctional capacity, circulation and gas exchanwhich in turn increases nutrient dehvery aoverall growth rate of the fetus.'"' ' '"-^'Nevertheless, weight-bearing exercise wshown to influence fetal growth in both a timdependent and exercise volume-dependent faion.'""'^ Women who increased the volume their moderate weight-bearing exercise (tremill, step aerobic or stair stepper) in late prnancy (20 minutes 3-5 times per week throuweek 20, gradually increasing to 60 minu5 days per week by week 24 and maintaining tregimen until delivery) experienced a significanlower newborn birthweight than those womwho maintained the high volume of exerciseearly pregnancy and then decreased it by twthirds in late pregnancy.'"'*' For women who ercised to term, the drop in infant weight wattributed mainly to differences in newborn mass. Clapp and Capeless'"*^' concluded tmost of the variabihty in birthweight (40%) cbe explained by the relative level of weigsupported exercise performance in the last 5 monof pregnancy. Other studies have been unabledemonstrate decreased birthweight in wom
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
11/16
Physical Activity and Pregnancy 503
Table IV. Effect of a strijctured exercise programme during pregnancy on a newborn's birthweightStudy (year) Number of subjects Exercise mode Newborn birthweightBeci50% of preconception level(preconception level; running,14-68 km/wk, 51-83% VOs^g^; aerobics,3-11 sessions/wk, 25-30 min at 54-90%
No statistical difference inbirthweight between exercise andcontrol group (3,69 0,3 vs3,65 0.3 kg)Exercise group had heavier babiesthan those born to controi groupwomen (3,78 0,4 vs 3,37 0,3 kg;p = 0,01)
Clapp et al,'^'l 34 exercise group; 31 control group(1999)
Clapp et a l , ' " ' ' 22 exercise group; 24 control group(2000)
Clapp et a l , ' " " ' 26 L-H; 24 M-M; 25 H-L(2002)
Collingset al,l'^l(1983)Hail andKaufman(1987)
Kardel andKasel"21(1998)
Controi group had heavier babiesthan those born to exercise groupwomen (3,640,05vs3,440,1 kg;p = 0,01)Exercising mothers had heavierbabies than those born to controlwomen (3,75 0,8 vs 3,49 0,7 kg;p = 0,05)H-L group had heavier babiescompared with the M-M and H-Lgroups (3,900,1 vs 3,440,1 vs3 ,340 .1kg ;p20 min, >55% VOa^axWeight-bearing exercise (treadmill, stepaerobics or stair stepper) from the 8th wkof pregnancy, 20min, 3-5x/wk at55-60% pre-pregnancy VOamaxFrom the 8th wk of pregnancy, at55-60% V02max: L-H, 20min, 5x/wkthrough wk 2 0, increasing to 60 min5x/wk by wk 24 and maintaining thatlevel until delivery; M-M, 40 min, 5x/wk;H-L, 60 min, 5x/wk through wk 20,decreasing to 20 min, 5x/wk by wk 24and maintaining that level until deliveryDuring the 2nd and 3rd trimester ofpregnancy; aerobic exercise 3x/wk,>25 min, 65-70% VOs^^,Throughout pregnancy, exercise sessionconsisted of 3 components; warm-up(5 min treadmill at 5- 6 km/h, or 5 minbicycle at 50 W) + 5x/wk, 45 min weight-iifting + bicycie ergometer (-85% ofmaximal HR but
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
12/16
504 Melzer e
and should be encouraged. Unfortunately, en-ergy expended on physical activity often de-creases as pregnancy advances, which may havenegative consequences on mother and infant,including maternal cardiovascular fitness andcapacity to sustain efforts required during labourand delivery. Further studies with larger samplesizes are required to confirm the association be-tween physical activity and outcomes of labourand delivery.
AcknowledgementsThe study was supported in part by a competit ive grantattributed to Drs Boulvain and Kayser by the Clinical Re-search Centre, Faculty of Medicine, University of Geneva,and was further supported by the Faculty of Medicine ofthe University of Geneva, and the University Hospitals ofGeneva, Switzerland. The SOGC guideline has been providedfree of charge courtesy of the Society of Obstetricians andGynecologists of Canada. The authors have no conflicts ofinterest that are directly relevant to the content of this review.
References1. Melzer K, Kayser B, Pichard C. Physical activity: thehealth benefits outweigh the risks. Curr Opin Clin NutrMetab Care 2004; 7: 641-72. American College of Sports Medicine. ACSM's guidelinesfor exercise testing and prescription. Philadelphia (PA):Up pinc ott Williams & Wilkins. 20063. Wolfe LA, Weissgerber TL. Clinical physiology of exercisein pregnancy: a literature review. J Obstet Gynaecol Can2003; 25: 473-834. Zhang J. Savitz DA. Exercise during pregnancy among US
wom en. Ann Epidemiol 1996; 6: 53-95. Pivarnik JM. Chambliss HO. Clapp JF. et al. Specialcommunications, roundtable consensus statement: impactof physical activity during pregnancy and postpartumon chronic disease risk. Med Sei Sports Exerc 2006; 38:989-10066. Jones AM, Carter H. The efTect of endurance training onparam eters of aerob ic fitness. Sports Med 2000; 29: 373-867. Fujimoto T , Kemppainen J, Kalliokoski K K, et al. Skeletalmuscle glucose uptake response to exercise in trained anduntrained men. Med Sei Sports Exerc 2003; 35: 777-838. McArdle W, Katch F, Katch V. Essentials of exercisephysiology. Philadelphia (PA): Lippincott Williams &Wilkins. 20009. Wibom R. Hultman E, Johansson M, et al. Adaptation ofmitochondrial ATP production in human skeletal muscle
11. Mujika L Padilla S. Cardiorespiratory and metabocharacteristics of detraining in humans. Med Sei SpExerc 2001; 33: 413-2112. Hunter S, Robson SC. Adaptation of the maternal hearpregnancy. Br Heart J 1992; 68: 540-3
13. Clapp III JF. Maternal heart rate in pregnancy. Am J stet Gyn ecol 1985; 152: 659-6014. Ueland K, Novy MJ, Peterson EN, et al. Matercardiovascular dynamics, IV: the influence of gestatioage on the maternal cardiovascular response to postand exercise. Am J Obstet Gynecol 1969; 104: 856-6415. Wolfe LA, Mo ttola M F. Aerobic exercise in pregnancyupdate. Can J Appl Physiol 1993; 18: 119-4716. Pritchard JA. Changes in the blood volume during pr
nancy and delivery. Anesthesiology 1965; 26: 393-917. Cunningham FG, Gant NF, Leveno KJ, et al. Williaobstetrics. New York: McGraw-Hill, 200518. Yeomans ER. Gilstrap III LC. Physiologic changespregnancy and their impact on critical care. Crit CMed 2005; 33: S256-819. Wadlington J, Natale M, Crowley M. Anesthesia for stetrics and gynecology. In: Hurford WE, et al., editoClinicai anesthesia procedures of the MassachusGeneral H ospital. Philadelphia (PA): Lippincott W illia& Wilkins, 1998:523-4520 . Capeless EL, Clapp JF. Cardiovascular changes in eaphase of pregnancy. Am J Obstet Gynecol 1989; 1
1449-5321 . Fujitani S, Baldissed MR. Hemodynamic assessment ipregnant and peripartum patient. Crit Care Med 2005;S354-6I22. Ezmerli NM . Exercise in pregnancy. Prim Care U pdate Gyns 2000; 7: 260-523 . Hemmings GT. Whalley DG. O'Connor PJ. et al. Invasmonitoring and anaesthetic management of a parturiwith mitral stenosis. Can J Anaesth 1987; 34: 182-524. Ueland K. Hansen JM. Maternal cardiovascular dynami3: labor and delivery under local and caudal analgesAm J Obstet Gynecol 1969; 103: 8-1825. Katz M, Kroll D, Shapiro Y. et al. Energy expenditurenormal labor. Isr J Med Sei 1990; 26: 254-726. Shnider SM, Abboud TK, Artal R, et al. Maternal techolamines decrease during labor after lum bar epiduanesthesia. Am J Obstet Gynecol 1983; 147: 13-527. Hagerdal M, Morgan CW, Sumner AE. et al. Minventilation and oxygen consumption during labor wepidural analgesia. A nesthesiology 1983; 59: 425-728. Sangoul F, Fox GS, Houle GL. Effect of regional analgeon maternal oxygen consum ption during the first stagelabor. Am J Obstet Gynecol 1975; 121: 1080-329. Kreiser D, Katorza E, Seidman DS, et al. The effectephedrine on intrapartum fetal heart rate after epiduanalgesia. Obstet Gynecol 2004; 104: 1277-8130 . Cascio M, Pygon B. Bernett C, et al. Labour analgesia wintrathecal fentanyl decreases maternal stress. Can J A
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
13/16
Physical Activity and Pregnancy 505
32. Manninen T . Aantaa R. Salonen M . et al. A comparison ofthe hemodynamic effects of paracervical block and epi-dural anesthesia for labor analgesia. Acta AnaesthesiolScand 2000; 44: 441-533 . Danilenko-Dixon DR. Tefft L. Cohen RA, et al. Positionaleffects on maternal cardiac output during labor with epi-dural an algesia. Am J O bstet Gynecol 1996: 175: 867-7234. Robson SC. Dunlop W, Boys RJ, et al. Cardiac outputduring labour. Br Med J (Clin Res Ed) 1987; 295; 1169-7235. OToole ML. Physiologic aspects of exercise in pregnancy.Clin Obstet Gynecol 2003; 46: 379-8936. Pivarnik JM, Ayres NA, Mauer MB, et al. Effects ofmaterna l aerobic fitness on cardiorespiratory responses toexercise. Med Sei Sports Exerc 1993; 25; 993-837. Carpenter MW. Sady SP. Sady MA, et al. Effect ofmaternal weight gain during pregnancy on exercise per-formance. J Appl Physiol 1990; 68; 1173-638. Knuttgen HG. Emerson Jr K. Physiological response to
pregnancy at rest and during exercise. J Appl Physiol1974; 36; 549-5339. Artal R. Exercise and pregnancy. Clin Sports Med 1992;11; 363-7740 . Pivarnik JM. Lee W, Miller JF. Physiological and percep-tual responses to cycle and treadmill exercise duringpregnancy. Med Sei Sports Exerc 1991; 23; 470-541 . Artal R. Wiswell R, Romem Y. et al. ^^llmonary responses toexercise in pregnancy. Am J O bstet Gynecol 1986; 154; 378-8342 . Pernoll ML. Metcalfe J. Schlenker TL. et al. Oxygen con-sumption at rest and durin g exercise in pregnancy. RespirPhysiol 1975; 25; 285-9343 . Bonen A, Campagna P, Gilchrist L, et al. Substrate andendocrine responses during exercise at selected stages ofpregn ancy . J App l Physiol 1992; 73; 134-4244. Heenan AP, Wolfe LA. Davies GA. Maximal exercisetesting in late gestation; maternal responses. ObstetGynecol 2001; 97; 127-3445. Sady SP, Carpenter MW. Sady MA, et al. Prediction ofVO,n,a, during cycle exercise in pregnant women. J ApplPhysiol 1988; 65; 657-6146. Sady SP, Carpenter MW, Thompson PD, et al. Cardio-vascular response to cycle exercise during and after preg-nancy. J Appl Physiol 1989; 66; 336-4147. Spinnewijn WE. Wallenburg HC. Struijk PC, et al. Peakventilatory responses during cycling and swimming inpregnant and nonpregnant women. J Appl Physiol 1996;81; 738-4248. Spaaij CJ. van Raaij JM. de Groot LC, et al. No changesduring pregnancy in the net cost of cycling exercise. Eur J
Cl inN utr 1994; 48; 513-2149. Clapp III JF. Oxygen consumption during treadmill ex-ercise before, during, and after pregnancy. Am J ObstetGynecol 1989; 161; 1458-6450. Lotgering FK, van Doom MB, Struijk PC. et al. Maximalaerobic exercise in pregnant women; heart rate, O2 con-sumption, C02 production, and ventilation. J Appl Phy-siol 1991; 70; 1016-2351. Lotgering FK, Struijk PC, van Doom MB, et al. Errors inpredicting maximal oxygen consumption in pregnantwomen. J Appl Physiol 1992; 72; 562-7
52. McMurray RG, Hackney AC, Katz VL, et al. Pregnancy-induced changes in the maximal physiological respotisesduring swimming. J Appl Physiol 1991; 71; 1454-953. Kardel KR. Effects of intense training during and after
pregnancy in top-level athletes. Scand J Med Sei Sports2005; 15:79-8654. Clapp III JF, Capeless E. The VOjma, of recreational ath-letes before and after pregnancy. Med Sei Sports Exerc1991; 23; 1128-3355. Pivarnik JM , Stein A D, Rivera JM . Effect of pregnancy onheart rate/oxygen consumption calibration curves. MedSei Sports Exerc 2002; 34; 750-556. McMurray RG, Mottola MF, Wolfe LA, et al. Recentadvances in understanding maternal and fetal responsesto exercise. Med Sei Sports Exerc 1993; 25; 1305-2157. Artal R, OTo ole M. Guidelines of the American College ofObstetricians and Gynecologists for exercise duringpregnancy and the postpartum period. Br J Sports Med2003; 37; 6-1258. Davies GA, Wolfe LA, Mottola MF, et al. JointSOGC/CSEP clinical practice guideline; exercise in preg-nancy and the postpartum period. J Obstet Gynaecol Can2003; 25; 516-2959. Pate RR, Pratt M, Blair SN, et al. Physical activity andpublic health; a recommendation from the centers fordisease control and prevention and the American Collegeof Sports M edicine. JAMA 1995; 273; 402-760. Arena B, Maffulli N. E xercise in pregna ncy; ho w safe is it?Sports Med Arthroscop Rev 2002; 10; 15-2261. Wolfe LA, Davies GA. Canadian guidelines for exercise inpregnancy. Clin Obstet Gynecol 2003; 46; 488-9562. Huch R. Physical activity at altitude in pregnancy. SeminPerina tol 1996; 20; 303-1463 . Soultanakis HN, Artal R, Wiswell RA. Prolonged exercisein pregnancy; glucose h omeostasis, ventilatory and cardio-vascular respo nses. Semin P erinatol 1996; 20; 315-2764 . Lokey EA. Tran ZV, Wells CL, et al. Effects of physicalexercise on pregnancy outcomes; a meta-analytic review.Med Sei Sports Exerc 1991; 23; 12.34-965. McM urray R G, Hackney AC , Guion WK, et al. Metabolicand hormonal responses to low-impact aerobic danceduring p regnancy. Med Sei Sports Exerc 1996; 28; 41-666. Milunsky A, Ulcickas M, Rothman KJ. et al. Maternalheat exposure and neural tube defects. JAMA 1992; 268;882-567. Jones RL, Botti JJ, Anderson WM, et al. Thermorgula-tion during aerobic exercise in pregnancy. Obstet Gy necol1985; 65; 340-568. McM urray R G, Katz VL. Thermorgulation in pregnancy;implications for exercise. Sports Med 1990; 10; 146-5869. Borg G. Borg's perceived exertion and pain scales. Cham-paign (IL); Human Kinetics. 199870. Butte NF. Wong WW, Treuth MS, et al. Energy require-ments during pregnancy based on total energy ex-penditure and energy deposition. Am J Clin Nutr 2004;79; 1078-8771. Clarke PE. Rousham EK. Gross H, et al. Activity patternsand time allocation during pregnancy; a longitudinalstudy of British wom en. Ann Hum Biol 2005; 32; 247-58
2010 Adis Da ta i nform af ion BV. All r ights reserved. Sports Me d 2010; 40 (6)
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
14/16
506 Melzer
72. Lawrence M. Whitehead RG. Physical activity and totalenergy expetiditure of child-bearing Gambian villagewom en. Eur J Clin Nu tr 1988; 42; 145-6073 . Lof M. Forsum E. Activity pattern and energy expen dituredue to physical activity before and during pregnancy inhealthy Swedish women. Br J Nutr 2006; 95; 296-302
74. Rousham EK. Clarke PE. Gross H. Significant changes inphysical activity among pregnant women in the UK asassessed by accelerometry and self-reported activity. EurJ Clin Nutr 2006; 60; 393-40075 . Haakstad LA. Voldner N. Henriksen T. et al. Physicalactivity level and weight gain in a cohort of pregnant Nor-wegian women. Acta Obstet Gynecol Scand 2007; 86; 559-6476. Forsum E, Kabir N. Sadurskis A, et al. Total energy ex-penditure of healthy Swedish women during pregnancyand lactatio n. Am J Clin Nutr 1992; 56: 334-4277 . Heini A. Schutz Y. Diaz E, et al. Free-living energy expen-diture measured by two independent techniques in preg-nant and nonpregnant Gambian women. Am J Physiol1991; 261; E9-1778. Lawrence M. Singh J. Lawrence F. el al. The energy cost ofcommon daily activities in African women; increased ex-penditure in pregnancy? Am J Clin Nutr 1985; 42; 753-6379. Singh J. Prentice AM, Diaz E, et al. Energy expenditure ofGambian women during peak agricultural activity mea-sured by the doubly-labelled water method. Br J Nutr1989; 62; 315-2980. Borodulin KM. Evenson KR. Wen F. et al. Physical ac-tivity patterns during pregnancy. Med Sei Sports Exerc2008; 40: 1901-881 . Gaw ade P. Pekow P. Markenson G. et al. Physical activitybefore and during pregnancy and duration of'second stageof labor among H ispanic women. J Rep rod M ed 2009- 54-429-3582 . van Raaij JM. Schonk CM. Vermaat-Miedema SH, et al.Body fat mass and basal metabolic rate in Dutch womenbefore, during, and after pregnancy: a reappraisal of en-ergy cost of pregnancy. Am J Clin Nutr 1989; 49; 765-7283. Poudevigne MS. O'Connor PJ. A review of physical ac-tivity patterns in pregnant women and their relationshipto psychological health. Sports Med 2006; 36: 19-3884. DiNallo JM . Le Masurier GC . Williams NL et al. Walkingfor health in pregnancy: assessment by indirect calorimetryand accelerometry. Res Q Exerc Spo rt 2008; 79: 28-3585. Nagy LE. King JC . Energy expenditure of pregnant womenat rest or walking self-paced. Am J Clin Nu tr 1983; 38:369-7686. Chasan-Taber L. Schmidt MD, Pekow P. et al. Correlatesof physical activity in pregnancy among Latina women.Matern Child Health J 2007; II: 353-6387 . Pereira MA. Rifas-Shiman SL, Kleinman KP, et al. Pre-dictors of change in physical activity during and afterpregnancy: Project Viva. Am J Prev Med 2007; 32: 312-988. Jarrett JC. Spellacy WN. Jogging during pregnancy: animproved outcome? Obstet Gynecol 1983; 61; 705-989. Dufour DL. Reina JC. Spurr G. Energy intake and ex-
metabolic rate in Switzerland. Eu r J Clin N utr 20091185-9191. Petersen AM. Leet TL. Brownson RC. Correlates of sical activity amon g pregn ant women in the U nited StMed Sei Sports Exerc 2005; 37: 1748-5392 . Melzer K. Schutz Y. Soehnchen N. et al. Effects ocommended levels of physical activity on pregnancycomes. Am J O bstet Gynecol 2010; 202 (3): 266.el-693 . Gavard JA. Artal R. Effect of exercise on pregnancy come. Clin Obstet Gynecol 2008; 51: 467-8094. Mottola MF. Exercise prescription for overweight obese women: pregnancy and postpartum. Obstet Gcol Clin North Am 2009; 36: 301-16. viii95. Poudevigne M S. O'C onn or PJ. Physical activity and r
during p regnancy. M ed Sei Sports Exerc 2005; 37: 13796. Artal R. Exercise: the alternative therapeutic intervenfor gestational diabetes. Clin Obstet Gynecol 2003479-8797 . Clapp III JF. Lopez B. Harcar-Sevcik R. Neonatal bvioral profile of the offspring of women who continueexercise regularly throughout pregnancy. Am J ObGyneco l 1999; 180: 91-498. Clapp III JF. Exercise and fetal health. J Dev Physiol 115:9-1499. Wolfe LA, Charlesworth SA, Glenn NM, et al. Effectpregnancy on maternal work tolerance. Can J Appl siol 2005; 30: 212-32
100. Clapp III JF. The course of labor after enduranceercise during pregna ncy. Am J Obstet Gy necol 1990;1799-805101. Erdelyi GJ. Gynecological survey of female athlJ Sports Med Phys Fitness 1962; 2; 174-9102. Beckmann CR . Beckmann CA . Effect of a structantepartum exercise program on pregnancy and loutcome in prim paras. J Reprod Med 1990; 35: 704-103. Hall DC. Kaufmann DA. Effects of aerobic and streconditioning on pregnancy outcomes. Am J ObGynecol 1987; 157: 1199-203104. Wong SC. McKenzie DC. Cardiorespiratory fitness dupregnancy and its effect on outcome. Int J Sports 1987; 8; 79-83105. Kardel KR. Johansen B. Voldner N. et al. Associationtween aerobic fitness in late pregnancy and duratiolabor in nulliparous women. Acta Obstet Gynecol Sc2009; 88; 948-52106. Penttinen J, Erkkola R. Pregnancy in endurance athleScand J Med Sei Sports 1997; 7; 226-8107. Collings CA, Curet LB, Mullin JP. Maternal and fetalsponses to a maternal aerobic exercise program. AObstet Gynecol 1983; 145; 702-7108. Rice PL. Fort IL. The relationship of maternal exercislabor, delivery and health of the newborn. J Sports M
Phys Fitness 1991; 31; 95-9109. Erkkola R. The physical work capacity of the expecmother and its effect on pregnancy, labor and the n
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
15/16
Physical Activity and Pregnancy 507
111. Magann EF. Evans SF. Weitz B. et al. Antepartum, in-t rapartum. and neonatal significance ofexercise on heal-thy low-risk pregnant working women. Obstet Gynecol2002: 99: 466-72112. Kardel KR.Kase T. Training in pregnant women: effectson fetal development and birth. Am J Obstet Gynecol1998; 178:280-6113. Clapp III JF. Kim H. Burciu B. et al. Beginning regularexercise in early pregnancy: effect on fetoplacentalgrowth. Am J Obstet Gynecol 2000; 183: 1484-8114. Clapp III JF. Kim H. Burciu B, et al. Continuing regularexercise during pregnancy: effect of exercise volume on
fetoplacental growth. Am J Obstet Gynecol 2002; 186:142-7115. Clapp III JF. Capeless EL. Neonatal morphometricsafter endurance exercise during pregnancy. Am J Obstet
Gynecol 1990; 163: 1805-11Correspondence: Professor Bengt Kayser, Director, Instituof Movement Sciences and Sports Medicine, Facult deMdecine, Universit de Genve, 10 rue du Conseil Gn-ral, 1205 Genve, Switzerland.E-mail: [email protected]
2010 Adis Data informot ion BV. Aiir ig t its reserve d. Sports Me d 2010; 40 (6
-
7/28/2019 Physical Activity and Pregnancy Cardiovascular Adaptations, Recommendations and Pregnancy Outcomes
16/16
Copyright of Sports Medicine is the property of ADIS International Limited and its content may not be copied
or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.