Brandauer Insomnia Presentation - movementdisorders.org · 1/6/2015 1 Insomnia Elisabeth Brandauer,...
10
1/6/2015 1 Insomnia Elisabeth Brandauer, MD Department of Neurology, Innsbruck Medical University, Austria Movement Disorders in Sleep Barcelona, Jan 30-31 CharacteristicsofInsomnia • Persistent difficultywithsleepinitiation, duration, consolidationorqualitythatoccursdespiteadequate opportunityandcircumstancesforsleep, andresultson some form ofdaytimeimpairment; • Daytimesymptomstypicallyincludefatigue, decreasedmood orirritability, generalmalaiseandcognitiveimpairment, but not fallingasleepduringdaytime; International Classificationof SleepDisorders3rd American AcademyofSleepMedicine, 2014 International Classificationof Sleep Disorders–ICSD 2 • Insomnia – AdjustmentInsomnia – Psychophysiological Insomnia – ParadoxicalInsomnia – IdiopathicInsomnia – InsomniaDue to a Mental Disorder – InadequateSleepHygiene – InsomniaDue toDrug orSubstance – InsomniaDue to a Medical Condition – InsomniaNot Due toSubstanceorKnownPhysiologic Condition, Unspecified – Physiologic(Organic) Insomnia, Unspecified
Transcript of Brandauer Insomnia Presentation - movementdisorders.org · 1/6/2015 1 Insomnia Elisabeth Brandauer,...

1/6/2015
1
Insomnia
Elisabeth Brandauer, MD Department of Neurology, Innsbruck Medical University, Austria
Movement Disorders in SleepBarcelona, Jan 30-31
Characteristics of Insomnia
• Persistent difficulty with sleep initiation, duration,
consolidation or quality that occurs despite adequate
opportunity and circumstances for sleep , and results on some
form of daytime impairment;
• Daytime symptoms typically include fatigue, decreased mood
or irritability, general malaise and cognitive impairment, but
not falling asleep during daytime;
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
International Classification of Sleep
Disorders – ICSD 2
• Insomnia– Adjustment Insomnia
– Psychophysiological Insomnia
– Paradoxical Insomnia
– Idiopathic Insomnia
– Insomnia Due to a Mental Disorder
– Inadequate Sleep Hygiene
– Insomnia Due to Drug or Substance
– Insomnia Due to a Medical Condition
– Insomnia Not Due to Substance or Known PhysiologicCondition, Unspecified
– Physiologic (Organic) Insomnia, Unspecified
1/6/2015
2
ICSD 3
1. Chronic Insomnia Definition ICSD-3 Alternate Names: Chronic insomnia, primary insomnia, secondary insomnia, comorbid insomnia, disorder of initiating and
maintaining sleep, behavioral insomnia of childhood, sleep-onset association disorder, limit-setting sleep disorder.
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
Diagnostic Criteria
Criteria A-F must be met
A. The patient reports, or the patient's parent or caregiver observes, one or more of
the following:
1. Difficulty initiating sleep.
2. Difficulty maintaining sleep.
3. Waking up earlier than desired.
4. Resistance to going to bed on appropriate schedule.
5. Difficulty sleeping without parent or caregiver intervention.
B. The patient reports, or the patient's parent or caregiver observes, one or more of
the following related to the nighttime sleep difficulty:
1. Fatigue/malaise.
2. Attention, concentration, or memory impairment.
3. Impaired social, family, occupational, or academic performance.
4. Mood disturbance/irritability.
5. Daytime sleepiness.
6. Behavioral problems (e.g., hyperactivity, impulsivity, aggression).
7. Reduced motivation/energy/initiative.
8. Proneness for errors/accidents.
9. Concerns about or dissatisfaction with sleep.
C. The reported sleep/wake complaints cannot be explained purely by inadequate
opportunity (i.e., enough time is allotted for sleep) or inadequate circumstances (i.e.,
the environment is safe, dark, quiet, and comfortable) for sleep.
D. The sleep disturbance and associated daytime symptoms occur at least three times
per week.
E. The sleep disturbance and associated daytime symptoms have been present for at
least three months
F. The sleep/wake difficulty is not better explained by another sleep disorder.
2. Short-Term Insomnia Definition ICSD-3 Alternate Names: Acute insomnia, adjustment insomnia.
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
Diagnostic Criteria
Criteria A-E must be met
A. The patient reports, or the patient's parent or caregiver observes, one or more of the
following:
1. Difficulty initiating sleep.
2. Difficulty maintaining sleep.
3. Waking up earlier than desired.
4. Resistance to going to bed on appropriate schedule.
5. Difficulty sleeping without parent or caregiver intervention.
B. The patient reports, or the patient's parent or caregiver observes, one or more of the
following related to the nighttime sleep difficulty:
1. Fatigue/malaise.
2. Attention, concentration, or memory impairment.
3. Impaired social, family, vocational, or academic performance.
4. Mood disturbance/irritability.
5. Daytime sleepiness.
6. Behavioral problems (e.g., hyperactivity, impulsivity, aggression).
7. Reduced motivation/energy/initiative.
8. Proneness for errors/accidents.
9. Concerns about or dissatisfaction with sleep.
C. The reported sleep/wake complaints cannot be explained purely by inadequate
opportunity (i.e., enough time is allotted for sleep) or inadequate circumstances (i.e.,
the environment is safe, dark, quiet, and comfortable) for sleep.
D. The sleep disturbance and associated daytime symptoms have been present for less
than three months.
E. The sleep/wake difficulty is not better explained by another sleep disorder.

1/6/2015
3
3. Other Insomnia Definition ICSD-3 Alternate Names: none.
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
Diagnostic Criteria
This diagnosis is reserved for individuals who complain of
difficulty initiating and maintaining sleep and yet do not
meet the full criteria for either chronic insomnia disorder
or short-term insomnia disorder. In some cases, this
diagnosis may be assigned on a provisional basis when
more information is needed to establish a diagnosis of
chronic insomnia disorder or short-term insomnia
disorder. It is expected that this diagnosis will be used
sparingly, given its nonspecific nature.
Demographics
Chronic Insomnia
• Full clinical syndrome in 10%
of population
• Transient Insomnia symptoms
in 30-35%
• Female > male
• At any age, but more
commonly in older age (age
related deterioration in sleep
continuity, medical
comorbidities, medication that
increase insomnia risk)
Short –Term Insomnia
• Can occur at any age, more
prevalent in older age groups
• Exact prevalence unknown
• One year prevalence in adults
in range of 15-20%
• Females > males
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
Pathophysiology
Chronic Insomnia
• increased physiological arousal, characterized by increased heart rate, altered heart rate variability, increased whole body metabolic rate, elevated cortisol, adrenocorticotropichormone and CRF levels, increasedbody temperature and increasedhigh-frequenzy EEG activity duringNREM sleep;
• Heightened activity of thesympathetic nervous system andhypothalamic-pituitary-adrenal axis
• No discrete structural brainpathology
Short –Term Insomnia
• Research on the pathology andpathophysiology of short-term variants of insomnia disorder isgenerally lacking because themajority of studies addressing thisissue have focused on samples withchronic insomnia disorders.
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014

1/6/2015
4
Differential Diagnosis
• Circadian Rhythm Sleep Disorders
• Sleep difficulties arising from sleep-disruptive environmental circumstances
• Insufficient sleep syndrome
• Insomnia as comorbidity with other sleep disorders:
• Sleep apnea
• Restless Legs Syndrome
• Parasomnias
International Classification of Sleep Disorders 3rd
American Academy of Sleep Medicine, 2014
Diagnostic steps in Insomnia
Clinical history
• Sleep habits, structured interview on sleep disorders
• Clinical findings
Actigraphy and sleep log
• Verification of subjective sleep
• Detection of circadian rhythm sleep disorders
Diagnostic steps in Insomnia
Polysomnography:
Especially useful to rule out other sleep disorders
• Findings in insomnia:
• Increased sleep latency
• Increased wake after sleep onset
• Reduced sleep efficiency
• Increased stage 1 sleep
• Decreased slow wave sleep
• Elevated high frequency power in EEG
MSLT (Multiple Sleep Latency Test)
• Normal daytime alertness
1/6/2015
5
Insomnia in Parkinson´s Disease
• Insomnia one of the most common non-motor symptoms in PD
• 40-50% of PD patients affected (Lee 2007, Martinez-Martin 2007),
37% (Barone 2009)
• Increase with disease duration
• Main complaints: sleep fragmentation and early awakening;
• Most common sleep complaint in PD is fatigue: 58% (Barone 2009)
Poewe W, Högl B: Curr Opin Neurol 2000,13:423-26
Sleep Disorders in PDContributing Factors
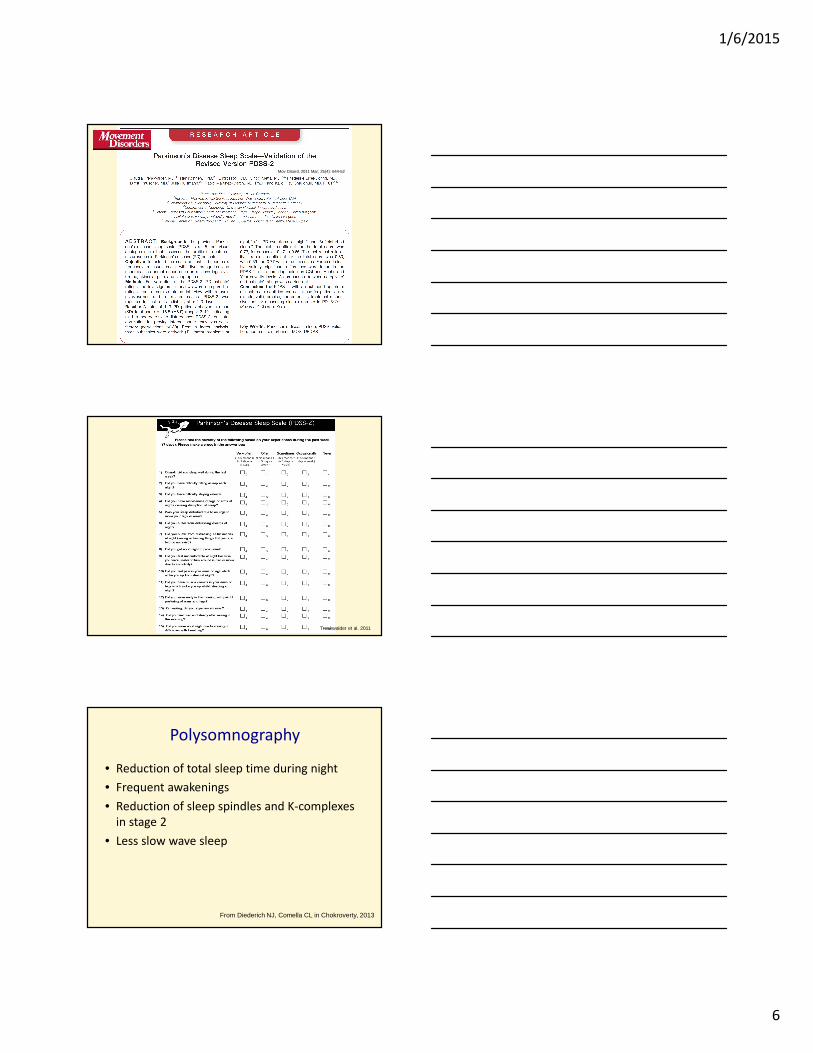
Sleep-Regulating nuclei possibly underlying primary slee pdisturbances in Parkinson‘s disease
Nucleus /Area Main Transmitter FunctionConsequence ofDysfunction in PD
Nucleus pedunculopontinus Ach
Regulation of REM sleepRBD
Locus coeruleus NARegulation of REM sleep Reduction / absence of
REM sleep
Area peri-locuscoeruleus ?
Inhibition of spinal motoneurons via nucleus magnocellularis
Loss of muscle atoniaduring REM → RBD
Raphe nuclei in midbrain and pons
5HT Regulation of slow-wave sleep Reduction of SWS
From Diederich NJ, Comella CL in Chokroverty, 2013
Midbrain tegmentalarea
DA Thalamocortical arousal Reduction of SWSExcessive daytimesleepiness
Hypothalamus Orexin/Hypocretin
Maintenance of daytimevigilance
Abrupt napping andmicrosleeps duringdaytime
1/6/2015
6
Mov Disord. 2011 Mar; 25(4): 644-52
Trenkwalder et al. 2011
Polysomnography
• Reduction of total sleep time during night
• Frequent awakenings
• Reduction of sleep spindles and K-complexes
in stage 2
• Less slow wave sleep
From Diederich NJ, Comella CL in Chokroverty, 2013
1/6/2015
7
Insomnia in Other Movement
Disorders
• Multiple System Atrophy
– Sleep onset and maintenance insomnia
– Sleep fragmentation more common than in PD;
caused by rigidity and bradykinesia
– Reduced sleep efficiency
– Disrupted circadian pattern
Iranzo, 2007
Abbott et al. 2014
• Corticobasal Degeneration
– Reduced total sleep time and sleep efficiency (Roche 2007)
• Progressive Supranuclear Palsy
– Frequency of sleep disturbance: 50% in a questionnaire study (Santacruz 1998)
– Insomnia worse than in PD patients
– Decreased total sleep time and REM sleep, increase in number and duration of noctural awakenings; decreased spindles, increased alpha-activity (Abbott 2014,
review)
– Status dissociatus with advanced disease (Gross 1978)
• Huntington´s Disease
– Hansotia 1985: reduced sleep efficiency, SWA and
REM sleep, prolonged REM latencies
– Arnulf 2008: early sleep onset; increased N1;
delayed and shortenend REM sleep
– Morton 2005: circadian disturbances in HD,
resulting from pathology in the suprachiasmatic
nucleus; reversal of normal nighttime/daytime
activity patterns
1/6/2015
8
Treatment of Insomnia
Non Drug Treatment: Relaxation
• Relaxation Training
• Biofeedback
• Yoga, Meditation
Non Drug Treatment: sleep hygiene rules
• Getting up same time every day, including
weekends
• Avoid napping during the day
• Avoid falling asleep while watching TV
• No TV, tablet etc. in the bedroom, the
bedroom is just for sleeping
• Avoid caffeine too late in daytime
• Avoid large meals before bed
• Daytime activity, but avoid exercise 2-4 h
before bedtime
• Bedroom should be cool, dark and quiet
Non Drug Treatment: cognitive
behavioral therapy

1/6/2015
9
Drug Treatment of Insomnia
• Benzodiazepins
• Nonbenzodiazepin receptor agonists
• Sedative antidepressants
• Neuroleptics
• Antihistamines
• Herbal Medications
• Melatonin and melatonergic substances
Choice of Drug Treatment
• Disease duration? (chronic insomnia, short term
insomnia)
• Comorbidity? (Depression, Anxiety disorder, medical
disorders, history of substance abuse?)
• Sleep initiation or maintenance disturbance?
• Compliance?
• Age?
Drug Treatment of Insomnia in Parkinsons Disease
• Optimize motor symptoms (slow release levodopa,
dopaminagonist)
• L-Dopa: low dosage can improve sleep continuity
• L-Dopa: higher dosages have an awakening effect
• Drug treatment: cave neuroleptics

1/6/2015
10
Drug Treatment of Insomnia in Parkinsons Disease
Efficacy Safety Practice implications
Controlled-release
formulation of
levodopa/carbidopa
Insufficient evidence Acceptable risk without
specialized monitoring
Investigational
Pergolide Insufficient evidence Acceptable risk with
specialized monitoring
Not useful
Eszopiclone Insufficient evidence Acceptable risk without
specialized monitoring
Investigational
Melatonin 3-5mg Insufficient evidence Acceptable risk without
specialized monitoring
Investigational
Melatonin 50mg Insufficient evidence Insufficient evidence Investigational
Seppi 2011, The Movement Disorder Society Evidence Based Medicine Review
Update: Treatments for the Non-Motor Symptoms of Parkinsons Disease