Biology and Treatment of Aggressive Fibromatosis or ... · Fibromatosis or Desmoid Tumor Keith M....
18
Biology and Treatment of Aggressive Fibromatosis or Desmoid Tumor Keith M. Skubitz, MD Abstract Aggressive fibromatosis, also known as desmoid-type fibromatosis (DTF) or desmoid tumor, is an uncommon locally invasive tumor. Because of its low incidence and variable behavior, DTF is often first seen by physicians who are not familiar with it, and recent advances in understanding this disease have led to changes in treatment approaches. The Wnt (b-catenin) pathway appears to play a key role in DTF pathogenesis, and recent studies of DTF biology suggest a possible model of DTF pathogenesis. Histologically, DTF shows a poorly circumscribed proliferation of myofibroblast-like cells with variable collagen deposition, similar to the proliferative phase of wound healing, and DTF has been associated with trauma and pregnancy. Desmoid-type fibromatosis may be a useful model of the tumor stroma in carcinomas as well as other fibrosing diseases such as progressive pulmonary fibrosis. The clinical course of DTF can vary greatly among patients, complicating the determination of the optimal treatment approach. Treatment options include surgery, nonsteroidal anti-inflammatory drugs with or without hormonal manipulation, chemotherapy, radiation therapy, and other forms of local therapy. Many treatments have been used, but these are not without toxicities. Because of the variable nature of the disease and the potential morbidity of treatment, some cases of DTF may do better without treatment; simple observation is often the best initial treatment. This review used a PubMed search from January 1, 1980, through October 31, 2016, using the terms fibromatosis and desmoid and discusses DTF disease characteristics, pathophysiology, and treatment options as well as examines several cases illustrating key points in the biology and treatment of this heterogeneous disease. ª 2017 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2017;92(6):947-964 T he term fibromatosis encompasses 2 general groups of tumors: superficial and deep fibromatoses. The superficial fibromatoses include palmar fibromatosis or Dupuytren contracture, plantar fibromatosis, and penile fibromatosis or Peyronie disease. Deep or aggressive fibromatosis, also known as desmoid-type fibromatosis (DTF) or des- moid tumor, is a clonal locally invasive tumor that does not metastasize. 1-8 However, although uncommon, DTF may be multifocal. The word desmoid derives from the Greek desmos meaning “bandlike, bond, or fastening.” 9,10 Desmoid-type fibromatosis was originally described by McFarlane in 1832 11 and termed “desmoid tumor” by Mueller in 1838. By 1904, about 400 cases had been reported. 10-13 The term fibromatosis was later introduced by Stout. 14 This review used a PubMed search from January 1, 1980, through October 31, 2016, using the terms fibromatosis and desmoid. Histologically, DTF shows a poorly circumscribed proliferation of myofibroblast- like cells with variable collagen deposition. These myofibroblastic cells are histologically similar to the proliferative phase of wound healing, and DTF has been associated with trauma, pregnancy, and oral contraceptive use. 3 Trauma is a common inciting agent for the development of DTF, 3,15-17 and surgery may sometimes promote growth of DTF. The natural history of DTF is highly variable. This review discusses DTF disease characteris- tics, pathophysiology, and treatment options as well as examines several cases illustrating key points in the biology and treatment of this heterogeneous disease. EPIDEMIOLOGY OF DTF Desmoid-type fibromatosis most commonly arises between the ages of 15 and 60 years, with a female predominance of 2- to 3-fold. 18,19 The incidence of DTF is about 2 From the Department of Medicine, University of Minnesota Medical School, Minneapolis. REVIEW Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012 www.mayoclinicproceedings.org n ª 2017 Mayo Foundation for Medical Education and Research 947
Transcript of Biology and Treatment of Aggressive Fibromatosis or ... · Fibromatosis or Desmoid Tumor Keith M....

Biology and Treatment of Aggressive
Fibromatosis or Desmoid Tumor
Keith M. Skubitz, MD
Abstract
Aggressive fibromatosis, also known as desmoid-type fibromatosis (DTF) or desmoid tumor, is an uncommonlocally invasive tumor. Because of its low incidence and variable behavior, DTF is often first seen byphysicians who are not familiar with it, and recent advances in understanding this disease have led tochanges in treatment approaches. The Wnt (b-catenin) pathway appears to play a key role in DTFpathogenesis, and recent studies of DTF biology suggest a possible model of DTF pathogenesis.Histologically, DTF shows a poorly circumscribed proliferation of myofibroblast-like cells with variablecollagen deposition, similar to the proliferative phase of wound healing, and DTF has been associated withtrauma and pregnancy. Desmoid-type fibromatosis may be a useful model of the tumor stroma incarcinomas as well as other fibrosing diseases such as progressive pulmonary fibrosis. The clinical courseof DTF can vary greatly among patients, complicating the determination of the optimal treatmentapproach. Treatment options include surgery, nonsteroidal anti-inflammatory drugs with or withouthormonal manipulation, chemotherapy, radiation therapy, and other forms of local therapy. Manytreatments have been used, but these are not without toxicities. Because of the variable nature of thedisease and the potential morbidity of treatment, some cases of DTF may do better without treatment;simple observation is often the best initial treatment. This review used a PubMed search from January 1,1980, through October 31, 2016, using the terms fibromatosis and desmoid and discusses DTF diseasecharacteristics, pathophysiology, and treatment options as well as examines several cases illustrating keypoints in the biology and treatment of this heterogeneous disease.
ª 2017 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2017;92(6):947-964
The term fibromatosis encompasses 2general groups of tumors: superficialand deep fibromatoses. The superficial
fibromatoses include palmar fibromatosis orDupuytren contracture, plantar fibromatosis,and penile fibromatosis or Peyronie disease.Deep or aggressive fibromatosis, also knownas desmoid-type fibromatosis (DTF) or des-moid tumor, is a clonal locally invasive tumorthat does not metastasize.1-8 However,although uncommon, DTF may be multifocal.The word desmoid derives from the Greekdesmos meaning “bandlike, bond, orfastening.”9,10 Desmoid-type fibromatosis wasoriginally described by McFarlane in 183211
and termed “desmoid tumor” by Mueller in1838. By 1904, about 400 cases had beenreported.10-13 The term fibromatosis was laterintroduced by Stout.14 This review used aPubMed search from January 1, 1980, throughOctober 31, 2016, using the terms fibromatosisand desmoid.
Histologically, DTF shows a poorlycircumscribed proliferation of myofibroblast-like cells with variable collagen deposition.These myofibroblastic cells are histologicallysimilar to the proliferative phase of woundhealing, and DTF has been associated withtrauma, pregnancy, and oral contraceptiveuse.3 Trauma is a common inciting agent forthe development of DTF,3,15-17 and surgerymay sometimes promote growth of DTF. Thenatural history of DTF is highly variable.This review discusses DTF disease characteris-tics, pathophysiology, and treatment optionsas well as examines several cases illustratingkey points in the biology and treatment ofthis heterogeneous disease.
EPIDEMIOLOGY OF DTF
Desmoid-type fibromatosis most commonlyarises between the ages of 15 and 60 years,with a female predominance of 2- to3-fold.18,19 The incidence of DTF is about 2
From the Department of
Medicine, University of
Minnesota Medical School,
Minneapolis.
REVIEW
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org n ª 2017 Mayo Foundation for Medical Education and Research947

to 4 per million per year in the general popu-lation.20-23 In contrast, the incidence of DTFhas been reported to be about 1000-foldhigher in patients with familial adenomatouspolyposis (FAP), in which the adenomatouspolyposis coli gene (APC) is mutated.24-26
Familial adenomatous polyposiseassociatedDTF is more frequently abdominal, especiallyin the Gardner variant of FAP, which ischaracterized by intestinal polyposis, oste-omas, fibromas, and epidermal inclusion(“sebaceous”) cysts.9,27-29 Desmoid-type fibro-matosis develops in approximately 5% to 30%of patients with FAP, usually in the mesen-tery.20,21,25,30-32 In some studies, FAP-associated DTF represents about 2% of DTFcases9; in 1 Dutch study, nearly 10% ofpatients with DTF have or will developFAP.21,33 With aggressive follow-up ofpatients with FAP and in those receiving pro-phylactic colectomy, DTF has been reported tobe the most common cause of death.32,34,35
Kindreds of familial DTF without the colonicfeatures of FAP have also been reported inwhich mutations occur in a different regionof APC.36,37 Genetic predisposition to DTFin patients with FAP independent of germ
line APC mutation has also been described,suggesting the existence of genes independentof APC that influence DTF formation in FAP.38
Although common in patients with FAP, mostcases occur sporadically in young adults15,18
and are associated with a mutation inb-catenin (CTNNB1).19,39-44 Desmoid-typefibromatosis and a related disease, infantileaggressive fibromatosis, may also differ be-tween children and adults.45,46 Infantile fibro-matosis (so-called diffuse or mesenchymaltype of fibromatosis) is not discussed hereand usually occurs before the age of 2,most commonly in the first few months oflife; it may recur locally, but does notmetastasize.
HISTOLOGY OF DTF
Histologically, DTF appears as a poorly cir-cumscribed proliferation of myofibroblasticcells with variable collagen deposition. Typi-cally, the margins of the tumor are difficultto assess at the time of surgery, and the finalmargins are often positive. Desmoid-typefibromatosis tumors are morphologically het-erogeneous and may exhibit striking morpho-logical intra- and intertumoral heterogeneity(Figure 1, A). In some areas tumors mayresemble fibroblasts of inactive fibrous tissue,whereas other areas resemble the active fibro-blasts of wound healing. This morphologicalheterogeneity covers a spectrum rangingfrom areas in which cells have oval nuclei con-taining pale-staining vesicular euchromatinand small nucleoli to areas in which cellshave elongated nuclei that stain darkly withhematoxylin, reflecting heterochromatin.47,48
Cells with more euchromatin are presumablymore “transcriptionally active,” whereas cellswith more heterochromatin are felt to bemore “transcriptionally inactive.”47 Figure 1,B, shows an area that appears inactive, withsparse cells with narrow, darker-stainingnuclei and few mitoses, in which in generalthere is more collagen deposition, impartinga more pink (collagenous) coloration to theseinactive areas. Typically the areas with more“transcriptionally inactive” cells are often sepa-rated by extensive collagen.48 Figure 1, C,from the same tumor shows an area that ap-pears histologically active, characterized bycells with plump, light-staining oval nuclei,
ARTICLE HIGHLIGHTS
d The clinical course of desmoid-type fibromatosis (DTF), an
uncommon locally invasive tumor, can vary greatly among pa-
tients, complicating the determination of the optimal treatment
approach.
d The Wnt (b-catenin) pathway appears to play a key role in DTF
pathogenesis.
d Treatment options include surgery, nonsteroidal anti-
inflammatory drugs with or without hormonal manipulation,
chemotherapy, radiation therapy, and other forms of local
therapy. Many treatments have been used, but these are not
without toxicities.
d Because of the variable nature of the disease and the potential
morbidity of treatment, some cases of DTF may do better
without treatment; simple observation is often the best initial
treatment.
d Desmoid-type fibromatosis may be a useful model of the tumor
stroma in carcinomas as well as other fibrosing diseases such as
progressive pulmonary fibrosis.
MAYO CLINIC PROCEEDINGS
948 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

greater cell density, increased mitotic activity,and less collagen. Digital assessment of chro-matin density and average nuclear size andpathological assessment of tumor activitywere strongly correlated in 1 study,48 andthere was a spatial correlation of proteinexpression of genes overexpressed in DTFand nuclear morphology.48
GENETIC CHANGES IN DTF
The Wnt (b-catenin) pathway appears to playa key role in DTF pathogenesis,2,41-43,49-51
with a mutation in the b-catenin gene inmost sporadic cases,39,41,42,45,49,50,52-56 or amutation in APC, which regulates b-catenindegradation, in cases associated withFAP.2,15,24,25,30,32,36,37,57-59 In 1 study a
FIGURE 1. Hematoxylin and eosin staining of desmoid-type fibromatosis specimens. A, Desmoid-type
fibromatosis samples exhibit striking morphological intra- and intertumoral heterogeneity. B, Some
tumor areas appear inactive, with sparse cells with narrow, darker-staining nuclei and few mitoses. In
general, more collagen deposition is evident in regions in which cells appeared inactive, imparting a more
pink (collagenous) coloration to these inactive areas. C, Other areas appeared histologically active,
characterized by cells with plump, light-staining oval nuclei, greater cell density, increased mitotic activity,
and less collagen.
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org949

CTNNB1 mutation was found in 223 of 254sporadic DTF cases (88%),42 with only 3 mu-tations reported: S45P, S45F, and T41A. S45Fand T41A were the most common, with S45Pseen in less than 10% of cases. Several cases ofAPC mutations have also been found in spo-radic cases of DTF.2,43 Clonal chromosomalchanges have been reported in about 45%of cases of deep DTF and approximately10% of superficial fibromatosis cases,60 withseveral recurrent chromosomal changesreported.41-43,60 In a study of 17 FAP-associated DTF and 38 sporadic DTF casesusing comparative genomic hybridizationand multiple ligation-dependent probe ampli-fication, a limited number of genetic changeswas observed in 44% of tumors.43,61 A higherfrequency of copy number abnormalities wasseen in FAP-associated DTF (59%) ascompared with sporadic DTF (37%).61 Theincidence and severity of DTF in FAP is relatedto the site of APC mutation.62
MOLECULAR BIOLOGY OF DTF
Desmoid-type fibromatosis exhibits a mono-clonal proliferation of myofibroblasts, present-ing a true neoplastic process,6-8 and asdescribed above, the Wnt or b-cateninpathway has been strongly implicated inDTF pathogenesis.2,3,41-44,49-51,54,57,63,64 Inaddition, induction of stabilized b-catenin ina transgenic mouse model leads to hyper-plastic cutaneous wounds and the develop-ment of DTF, providing further evidence thatb-catenin plays a role in these fibroprolifera-tive diseases.63 Similarly, mice with germ linemutations in APC have a high incidence ofDTF.65 Abnormal growth factor production(including transforming growth factor [TGF]and platelet-derived growth factor [PDGF])has been associated with hereditary gingivalfibromatosis and plantar fibromatosis66-68
and may play a role in DTF as well. Murinestudies suggest that DTF can originate inmesenchymal stem cells, in some cases derivedfrom pericytes.69,70
b-Catenin, encoded by the CTNNB1 gene,is also mutated or overexpressed in variouscancers71 and has 2 recognized functions. Itis part of the cadherin complex involved incell-cell adhesion, in which it binds the cyto-plasmic domain of cadherin,72 and also, aspart of the Wnt signaling pathway, can
translocate to the nucleus in which it regulatesgene transcription.73,74 b-Catenin is regulatedby a destruction complex (Figure 2) includingAPC, which has multiple b-catenin bindingsites, axin, b-catenin, casein kinase 1 (CK1),glycogen synthase kinase 3b (GSK3), and pro-tein phosphatase 2A. b-Catenin is phosphory-lated in this complex by GSK3 after a“priming” phosphorylation by CK1, whichleads to ubiquitination and subsequent degra-dation in the proteasome.74 Wnt signalingfrom the cell surface leads to disruption ofthe APC/axin/GSK3 complex and thus inhibitsb-catenin phosphorylation by the complex,leading to increased nuclear b-catenin.74
Nuclear b-catenin can act as a transcriptionalactivator when bound to a member ofthe T-cell factor/lymphocyte enhancerfamily, leading to the formation of nuclearb-catenin/T-cell factor/lymphocyte enhancercomplexes, changing the way they bind pro-motor regions of DNA and altering gene tran-scription.73,74 The hedgehog signalingpathway and b-catenin signaling pathwaysregulate each other’s activity, and 1 studyfound that hedgehog signaling is activated inhuman and murine desmoid tumors.75
Four genesda disintegrin and metallopro-teinase gene 12 (ADAM12), fibroblast activa-tion protein 1a (Fap-1a), Wnt 1 induciblesignaling pathway protein-1 (WISP1), andSRY-box 11 (SOX11)dhave been reported tobe overexpressed in DTF compared with 16nonneoplastic tissues,51 and immumohisto-chemistry studies have exhibited proteinexpression of ADAM12, Fap-1a, WISP1, andSOX11 in DTF.48 Fap-1a is a serine proteaselocalized to the cell surface and cytoplasm.Fap-1a has been found in tumor stroma andseveral fibrotic diseases including idiopathicpulmonary fibrosis.76 ADAM12 plays a rolein cell-cell and cell-matrix interactions andregulates integrin signaling77,78; ADAM12expression has also been found in Dupuytrendisease79 and idiopathic pulmonary fibrosis(reviewed in reference 80). ADAM12 identifiesa proinflammatory subset of PDGF receptor-a(PDGFR-a)epositive stromal cells residing inthe perivascular space that can be activatedby acute injury and can differentiate into myo-fibroblasts and act as progenitors for a largefraction of the collagen-producing cells gener-ated in scarring; these cells are progressively
MAYO CLINIC PROCEEDINGS
950 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

eliminated during normal wound healing.80
WISP1 is a secreted protein that can act as agrowth factor and regulate various cellularfunctions.81 WISP1 has been detected in anumber of tumors, including the desmoplastictumor stroma of carcinomas82 andDTF.48,51,83,84 WISP1 is up-regulated in idio-pathic pulmonary fibrosis and stimulatesextracellular matrix (ECM) deposition by fi-broblasts.85 SOX11 is a nuclear transcriptionfactor that is temporally regulated in develop-ment and not expressed in most adult tissues.SOX11 is deregulated in various tumors86 andoverexpressed in liposarcomas.87 SOX11 ismore highly expressed in mesenchymal stem
cell lines than in fibroblasts and may aidmesenchymal stem cell proliferation andpluripotent potential retention.88
Thus, the available data suggest a possiblemodel of DTF pathogenesis, in which an acti-vating stimulus, such as trauma with associ-ated inflammation and growth factorproduction, in the setting of deregulationof b-catenin, leads to up-regulation ofb-catenin48 (Figure 3, right side). Reactive ox-ygen species produced by neutrophils havebeen shown to have the potential to inducemutations in DNA. In rare cases the incitingevent may stimulate a progenitor cell thatdoes not have baseline b-catenin dysregulation
Wnt
Cadherin
Membrane
Nucleus
β-Catenin
β-Catenin
β-Catenin
β-Catenin P04
Axin
CK1 GSK3β
Proteasome
PP2AAPC
TCF
DNA
FIGURE 2. b-Catenin forms part of the cadherin complex involved in cell-cell adhesion, in which it
binds the cytoplasmic domain of cadherin. As part of the Wnt signaling pathway, b-catenin can also
translocate to the nucleus, in which it regulates gene transcription. b-Catenin is regulated by a
destruction complex including adenomatous polyposis coli gene (APC), axin, b-catenin, casein kinase 1
(CK1), glycogen synthase kinase 3b (GSK3), and protein phosphatase 2A (PP2A). b-Catenin is
phosphorylated by GSK3 and CK1, leading to ubiquitination and subsequent degradation in the
proteasome. Wnt signaling from the cell surface leads to disruption of the APC/axin/GSK3 complex
and thus inhibits b-catenin phosphorylation by the complex, leading to increased nuclear b-catenin.
Nuclear b-catenin can act as a transcriptional activator when bound to a member of the T-cell factor
(TCF)/lymphocyte enhancer (LEF) family, changing the way they bind promotor regions of DNA and
altering gene transcription.
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org951

(left-hand-side of the figure). b-Catenin canthen translocate to the nucleus, complexto transcription factors, bind the WISP1promotor, and increase WISP1 production.WISP1 may then bind its receptor and induceb-catenin nuclear translocation,89 resulting ina prosurvival signal, and further stimulateWISP1 production, and production of ECMproteins including collagen, leading to fibrosis.WISP1 binding to the tumor cells can thenfurther stimulate tumor growth. Myofibro-blasts are functionally heterogeneous and canbe generated from multiple cell types.80
WISP1, by binding to its receptor on othercells, may also recruit nonclonal (normal) pro-fibrotic ADAM12-positive cells from a PDGFR-positive precursor pool,80 potentially addingnonclonal normal myofibroblasts to the
tumor. These recruited cells, whether normalor part of the true clonal tumor, are Fap-1 pos-itive and produce a number of ECM proteins,including collagen, leading to fibrosis.Although the role of SOX11 is not clear,studies have reported that SOX11 assistsmesenchymal stem cell proliferation andretention of pluripotent potential.88 In somecases DTF tumors, and their constituent cells,may stabilize or regress, with a decrease inexpression of ADAM12, FAP-1a, WISP1, andSOX11 (Figure 4). In most cases of DTF,different areas of the tumor show either activeor inactive areas,48 indicating that the balanceof these factors leading to progression orregression operate differently in different partsof the tumor. The mechanisms regulatingthese factors are unknown.
Profibrotic ADAM12 +
PDGFR-α + precursor
WISP1 Production
ProliferationECM protein production
β-Catenin dysregulation
Increase in β-Catenin
β-Catenin translocationto the nucleus
Inflammation, growth factors,reactive oxygen species
Trauma
β-Catenin translocation to the nucleusWISP1 productionSOX11 (mesenchymal cell proliferation)ADAM12 (modify signals)FAP-1 (protease)α
FIGURE 3. A possible model of desmoid-type fibromatosis pathogenesis, in which an activating stimulus,
such as trauma with associated inflammation and growth factor production, in the setting of deregulation
of b-catenin, leads to up-regulation of b-catenin. b-Catenin can then translocate to the nucleus, complex
to transcription factors, bind the WISP1 promotor, and increase WISP1 production. WISP1 may then bind
its receptor and induce b-catenin nuclear translocation, resulting in a prosurvival signal, and further
stimulate WISP1 production and production of extracellular matrix (ECM) proteins including collagen,
leading to fibrosis. WISP1 binding to the tumor cells can also further stimulate tumor growth. WISP1,
by binding to its receptor on other cells, may also recruit nonclonal (normal) profibrotic ADAM12-positive
cells from a PDGFR-a-positive precursor pool, potentially adding nonclonal normal myofibroblasts to the
tumor. These recruited cells, whether normal or part of the true clonal tumor, are Fap-1 positive and
produce a number of ECM proteins, leading to fibrosis. In rare cases, an inciting stimulus may activate cells
that lack b-catenin dysregulation (left-hand-side of the figure). The exact role of ADAM12 and Fap-1 are
unknown, but may modify signaling via protease activity. Although the role of SOX11 is also not clear,
studies have reported that SOX11 assists mesenchymal stem cell proliferation and retention of pluripotent
potential.
MAYO CLINIC PROCEEDINGS
952 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

EVIDENCE FOR CLINICAL TREATMENTS OF
DTF
The natural clinical course of DTF can varygreatly among patients, complicating the deter-mination of the optimal treatment approach.Clinical trials exhibiting the best approach ina particular patient are lacking. Treatment op-tions include surgery, nonsteroidal anti-inflammatory drugs with or without hormonalmanipulation, chemotherapy, radiation ther-apy, and other forms of local therapy. Manytreatments have been used, but these are notwithout toxicities. Because of the variablecourse of the disease and the potentialmorbidity of treatment with the result thatsome cases of DTF may do better without treat-ment, Lewis et al,90 Mitchell et al,91 and Rocket al92 were among the first to suggest that sim-ple observation may often be the best initialapproach, and this recommendation hasbecome more common.93-103 Some studiessuggest that approximately 50% of cases willhave an indolent course93 and that patientswith DTF who have stable disease for morethan 1 year are unlikely to require activetreatment.96,104 The therapeutic approach of
adults with DTF and children with eitherDTF or infantile aggressive fibromatosis mayalso differ.45,46
Abdominal wall desmoids are mostcommonly associated with pregnancy andcould relate to “trauma” of stretching theabdominal wall musculature or possibly hor-monal changes or both.14 However, pregnancyis also associated with changes in circulatinggrowth factors and immune modulators,including vascular endothelial growth factor,TGF-b, and insulin-like growth factor 1; theseall could also be involved.105-108 Spontaneousregression of cases of abdominal wall DTFoccurred in about 30% of patients in 1 seriesof 122 patients not treated with surgery forDTF.96 In another study of 147 patients,97% of whom were young women withabdominal wall DTF, 102 underwent initialobservation; of these, 29 had spontaneousregression and only 16% went to surgery by3 years.95 Although the rate of progression ofDTF diagnosed during pregnancy is high, itsprognosis is generally good,109 and is notnecessarily, a contraindication for furtherpregnancies.110
Trauma, as from surgery, may worsen DTF,and DTF has a high risk of local recurrence aftersurgery ranging from about 25% to 60% at 5years.19,31,59,94,111-120 Inflammation from othertypes of trauma also may augment or stimulaterecurrence; however, DTF does not metastasize.Although a marginal resection is associated witha worse outcome than a complete resection, thenature of the surgical procedure is stronglyinfluenced by tumor location and associatedanatomical and functional consequences.94 Ina retrospective study of a subgroup of patients,the 3-year event-free survival with a nonsurgicalapproach was similar to that after a completeresection.94 A multivariate analysis of 495 pa-tients undergoing gross resection found thatonly age, tumor size, and tumor location sitewere associated with recurrence, with youngerage having a worse prognosis.121 In anothermultivariate analysis of 426 cases of sporadicDTF, 87% of cases were treated surgically, andabout 50% of cases recurred; only age, tumorsize, and tumor site were independent prog-nostic factors of recurrence.102 Tumors of theextremity recurred more frequently and micro-scopic assessment of the surgical margin hadno influence on recurrence.102,121 The high
Stimulus
β-Catenin dysregulation
Proliferation
Regression ProgressionStabilizationDecreased
ADAM12, WISP1,
FAP-1 , SOX11
pro-inflammatory
and/or profibrotic stimuli
α
FIGURE 4. Variable progression of desmoid-
type fibromatosis (DTF). In some cases of
DTF, a stimulus, such as trauma with associated
inflammation, in the setting of b-catenin dysre-
gulation can induce proliferation of clonal
myofibroblasts, forming a DTF tumor. These
tumors may progress, but in some cases DTF
tumors, and their constituent cells, may stabilize
or regress, with a decrease in expression of
ADAM12, FAP-1a, WISP1, and SOX11.
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org953

recurrence rate after surgery suggests that aclinical trial of an adjuvant tolerable chemo-therapy or other treatment shortly after surgerymight be worthy of study in some cases.41 Adju-vant chemotherapy after surgery might beparticularly useful after abdominal surgery inpatients at high risk of DTF, such as patientswith Gardner syndrome, although it has notbeen well studied.
In some cases radiation therapy can beuseful97,103,112,122-127; although radiationtherapy has been reported to decrease localrecurrence after marginal surgery in severaluncontrolled studies, other retrospectivestudies have found no benefit.128 The role ofradiation therapy among the varioustreatment options remains controversialbecause of long-term sequelae, includingedema, pain, and second malignantneoplasm.4,19,94,97,103,112,116,121,123,129-131 In1 study of 6 radiation-induced sarcomas inpatients with DTF whose original tumor hada mutation in CTNNB1, 3 had the sameCTNNB1 mutation as the original DTF, and3 had no CTNNB1 mutation, suggesting thatsome cases of DTF were not derived fromthe original DTF tumor clone.132
Cryoablation has also been used in anattempt to decrease the trauma associatedwith more extensive surgery, although itsrole remains to be defined.133
Various medical therapies have been usedfor DTF, ranging from those with lowtoxicity such as nonsteroidal anti-inflammatorydrugs9,18,134-136 or hormonal therapy9,18,31,137-140
to aggressive combination chemotherapy.141-148
Colchicine has also been used,149 and a casereport suggests a possible response to1,2-dihydroxyvitamin D3.
150 Comparative evalua-tion of different therapies is hindered by the factthat most case series are not randomized; the vari-able natural history of DTF further complicates theinterpretation of these studies. In cases thatrespond to drug, the optimal length of treatmentis unknown. Treatment approaches range fromholding treatment at an arbitrary time in the settingof stable disease to prolonged treatment in re-sponders, followed by abrupt cessation of therapyor gradually weaning treatment intervals or dose.
Magnetic resonance imaging (MRI) is thebest imaging technique for diagnosis and moni-toring of DTF.151-154 In some cases MRI mayreveal changes associated with increased
collagen deposition and decreased cellularity,such as a loss of T2 signal, suggesting either aresponse to treatment or a spontaneous decreasein disease activity.155,156 Changes in contrastenhancement may provide similar information.
Expression of estrogen receptor b is oftenpresent and, along with the occasional rela-tionship of DTF activity to pregnancy, pro-vides some rationale for hormonaltherapy.9,31,97,138-140,157-159 It has been re-ported that estrogen treatment can inducethe formation of desmoid tumors that regressafter discontinuing the drug or after addingprogesterone.160 In 1 study of 25 patientswith DTF (8 sporadic and 17 associated withFAP), a regimen of tamoxifen (120 mg/d)and sulindac (300 mg/d) was not highly effec-tive in preventing DTF recurrence after sur-gery, but was still felt to be potentially usefulin other settings, in which stable disease wasthe most common response.9 The optimaldose of tamoxifen for DTF is not well defined,and a range of doses has been used.9 Nonste-roidal anti-inflammatory drugs, typicallyibuprofen or sulindac, have also been usedwith some efficacy.9,18,134-136,158 Desmoid-type fibromatosis also expresses androgen re-ceptors; testosterone can stimulate DTF cellgrowth in vitro and DTF development inmouse models, suggesting androgen blockadeas another potential hormonal approach.161
A combination of methotrexate andvinblastine was one of the first chemotherapyregimens widely used for DTF, with responserates ranging from 30% to 50%.162-165
Because this regimen does have considerabletoxicity, vinorelbine has largely replacedvinblastine in this regimen.166 Methotrexatecombined with vinblastine or vinorelbine ismore difficult to deliver over a prolongedcourse in adults because of toxicity.143,167
Other agents include more aggressive chemo-therapy such as anthracyclines, gemcitabine,and even ifosfamide in rarecases.18,129,130,141,145-147,168,169 Tyrosine ki-nase inhibitors also have activity in someDTF cases, and meaningful responses havebeen described.64,155,156,169-174 In at least 1case the tumor was responsive to sunitinibbut not imatinib at the usual doses,169 suggest-ing that in some cases efficacy may be dueto effects on targets other than KIT (kitproto-oncogene receptor tyrosine kinase).
MAYO CLINIC PROCEEDINGS
954 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

TABLE. Ongoing Trials for Desmoid-Type Fibromatosis
Intervention Title Phase Location Clinical trial identifier Status
Sirolimus A pilot study evaluating the use of mTor
inhibitor sirolimus in children and young
adults with desmoid-type fibromatosis
Pilot phase 1/II Maine Medical Center NCT01265030 Recruiting
Cryotherapy Evaluation of the cryodestruction of non
abdominopelvic desmoid tumors in patients
progressing despite medical treatment
Phase II University Hospital, Strasbourg NCT02476305 Recruiting
PF-03084014 Phase II trial of the gamma-secretase inhibitor
PF-03084014 in adults with desmoid
tumors/aggressive fibromatosis
Phase II National Cancer Institute NCT01981551 Closed to accrual
Pazopanib Pazopanib efficacy and tolerance in desmoid
tumors
Randomized phase II:
pazopanib vs
methotrexate-vinblastine
Institut Bergonié NCT01876082 Recruiting
Imatinib Imatinib in patients with desmoid tumor and
chondrosarcoma
Phase II Italian Sarcoma Group NCT00928525 Closed to accrual
Sulindac and
tamoxifen
Sulindac and tamoxifen in treating patients
with desmoid tumor
Phase II Children’s Oncology Group NCT00068419 Closed to accrual
Sorafenib Sorafenib tosylate in treating patients with
desmoid tumors or aggressive fibromatosis
Phase II National Cancer Institute NCT02066181 Closed to accrual
Observation till-
progression
Tailored beta-catenin mutational approach in
extra-abdominal sporadic desmoids tumor
patients
Observational Fondazione IRCCS Istituto
Nazionale dei Tumori, Milano
NCT02547831 Recruiting
Imatinib Study to evaluate imatinib in desmoid tumors Phase II Heidelberg University NCT01137916 Closed to accrual
5-Aminolevulinic
acid (5-ALA)
and photodynamic
therapy
Safety and efficacy study using 5-ALA oral
administration as an adjuvant therapy on the
rate of local tumor recurrence in patients
who have desmoid tumors
Phase II adjuvant Tel-Aviv Sourasky Medical Center NCT01898416 Recruiting
Imatinib A trial of imatinib for patients with aggressive
desmoid tumor (aggressive fibromatosis)
Phase II Yonsei University NCT02495519 Closed to accrual
AGGRESSIVEFIB
ROMATOSIS
ORDESMOID
TUMOR
Mayo
Clin
Proc.
nJune2017;92(6):9
47-964
nhttp
://dx.doi.org/10.1016/j.m
ayocp.2017.02.012
www.m
ayoclin
icproceedings.org
955

Trials of tyrosine kinase inhibitors in DTF areongoing (Table). Pegylated-liposomal doxoru-bicin (PLD) is particularly attractive, given itsefficacy and low toxicity profile and isbecoming widely used.18,129,130,169
Antibodies to WISP1 inhibit fibrosis inmouse models of bleomycin lung toxicity,suggesting this as a potential target for thefuture treatment of select cases of DTF aswell. Similarly, the beneficial response ofDTF to certain chemotherapy approachessuggests that a similar approach could beuseful in severe cases of idiopathic pulmo-nary fibrosis. Altering Notch signaling withg-secretase inhibition is also under study,and an adenosine monophosphateeactivatedprotein kinase activator inhibits peritonealfibrosis (a complication of peritonealdialysis) in a mouse model.175 Preliminarydata suggest activity of a g-secretase inhibi-tor in DTF. Some ongoing trials for DTFare listed in the Table.
In some cases DTF tumors, and their con-stituent cells, may stabilize or regress, with adecrease in expression of biochemical markersof disease activity (Figure 4). The observationthat DTF tumors sometimes stabilize orregress implies that the tumor myofibroblastsretain sensitivity to a regulatory system, likelyan autocrine or more likely paracrine signalingsystem, similar to that of wound healing. ThatDTF tumors may still subsequently becomeactive again after stabilization or regression im-plies that a population of cells remains that re-tains the ability to respond to someproinflammatory and/or profibrotic stimuli,in some cases induced by trauma, associatedinflammation, or other physiological condi-tions, such as pregnancy. The degree to whichrecruited normal myofibroblasts contribute tothe mass of clonal myofibroblasts in an indi-vidual DTF tumor could potentially affect thetumor behavior.
PREDICTING DTF BEHAVIOR
Predicting which treatment is most appro-priate for a particular patient, such as theobservation approach, would be useful. Anomogram using tumor size, location, and pa-tient age has been reported to be useful in pre-dicting recurrence after surgery.121 Somestudies, but not all, have suggested that thelocation of the b-catenin mutation correlates
with differences in clinical course of sporadicDTF. For example, tumors with S45F muta-tions in CTNNB1 may be at a higher risk ofrecurrence.40-42,45,49,53,56,102 One study foundthat DTF tumors with an S45 b-catenin muta-tion had a higher progression arrest rate thandid wild-type tumors when treated with imati-nib,176 and a European position paper encour-aged b-catenin mutation testing in DTF.177
Another study found that higher nuclearb-catenin expression (>20% of tumor cellsexpressing nuclear b-catenin) had a higherrecurrence rate than did lower expression.178
Trisomy 8 has also been associated with ahigher risk of recurrence.179 In 1 study,immunohistochemical staining for ADAM12,Fap-1a, and WISP1 correlated with nuclearchromatin density and was higher in patientswith an early recurrence (<1 year after surgerycompared with no recurrence at 5 years).48
Other studies suggest that gene expressionpatterns may also correlate with biologicalbehavior48,51,180,181 and might be useful inidentifying patients who would more likelybenefit from therapy.
DESMOID-TYPE FIBROMATOSIS AS A
MODEL FOR THE ROLE OF TUMOR
STROMA IN OTHER DISEASES
The tumor stroma in invasive carcinomasfrequently exhibits a desmoplastic responsewith proliferation of myofibroblasts, andtumors have been described as “wounds thatdo not heal.”182,p1650 Fibroblasts and myofi-broblasts in neoplasms can secrete varioustrophic, mitogenic, and proinflammatorygrowth factors including hepatocyte growthfactor, epidermal growth factor, TGF-b, andinsulin-like growth factor 1 (reviewed inreference 183), possibly influencing growthof the clonal neoplastic cells. Because oftheir potential contribution to tumor biology,targeting the normal stromal myofibroblastsin tumors is an interesting potential approachto cancer treatment.184 As DTF closely resem-bles wound healing, it may be a potentiallyuseful model to study the role of tumorstroma. Indeed, some studies suggest thatgene signatures similar to that seen in DTFcorrelate with clinical outcome in somemalignancies.84,185-188 Desmoid-type fibro-matosis may also provide a model for
MAYO CLINIC PROCEEDINGS
956 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

other fibrosing diseases such as progressivepulmonary fibrosis.
DESMOID-TYPE FIBROMATOSIS CASE
EXAMPLES
As described above, DTF can have a differentcourse in different patients. Thirteen cases ofDTF are summarized here (10 in SupplementalMaterials, Supplemental Figure 2, availableonline at http://www.mayoclinicproceedings.org) to illustrate important principles of DTFbiology and treatment.
Case 1: Slow Spontaneous Regression of an
Extra-Abdominal DTF in a Man
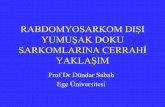
A28-year-oldmannoted a smallmass inhis rightchest near the sternum. He developed psoriaticarthritis 8 months later and began treatmentwith methotrexate. A year after initiating metho-trexate, etanercept was added. At presentation 8months after starting etanercept, he was not surethe mass had grown over the part year, but henow had occasional twinges of pain lasting afew seconds, from none to several times a day.Thus, the tumor progressed symptomaticallywhile on methotrexate. Examination revealed afirm, fixed, nontender parasternal mass.Computed tomography revealed a massinvolving the sternumgrowing through the chestwall (Figure 5, top panel) and a biopsy revealedDTF. Consultation at another institution recom-mended surgical removal of the chest wall mass;however, he was observed, and 3 months laterhis symptoms and imaging of the mass were un-changed. Ten months after the biopsy, the masswas slightly smaller and symptoms were un-changed. At 35 months after the biopsy, hissymptoms had resolved and the mass wassmaller (Figure 5, bottom panel). He remainssymptom free 50 months after the biopsy andcontinues the observation. This case exhibitsslow spontaneous regression of an extra-abdominalDTF in aman, not related to estrogen.
Case 2: DTF Caused by Local Trauma/
Inflammation and Stable Disease After
Methotrexate and Vinblastine
A 33-year-old man presented with a painfulmass in the arm. He had an influenza shot1.5 years before presentation, and shortlythereafter he became aware of a persistentdiscomfort in the region of the injection sitethat gradually progressed, and a painful mass
developed. The size of the mass and degreeof pain progressed markedly over the 2months before presentation. Examinationrevealed a slightly tender warm 10 cm hardmass fixed to the underlying tissue in theproximal right arm. Magnetic resonance imag-ing revealed a 7�5�8.5 cm mass along the tri-ceps muscle that was hyperintense on a fluid-sensitive image with some areas of heterogene-ity (Supplemental Figure 1, available online athttp://www.mayoclinicproceedings.org). Atru-cut biopsy revealed DTF, and an openbiopsy performed to exclude a low-grade sar-coma also revealed DTF. Surgical treatmentwas felt to require shoulder disarticulation. Assurgical treatment was felt to result in signifi-cant morbidity, chemotherapy with metho-trexate and vinblastine was begun. At 6 weeksof treatment, there was no clear evidence ofchange in tumor size or symptoms, and hemoved to a different state in which chemo-therapy was continued for 2 more monthswithout change in tumor size. The tumor wasthen surgically excised. He was sent for consid-eration of postoperative radiation therapy andthereafter lost to follow-up. This case exhibitsDTF development after local trauma/inflamma-tion, potential significant morbidity of treat-ment (shoulder disarticulation or more limiteddisfiguring surgery), and disease stabilizationwith methotrexate and vinblastine.
Case 3: Aggressive Multifocal DTF
Controlled With PLD
A 32-year-old man with Gardner syndromepresented with painful extra-abdominal des-moid tumors as well as large intra-abdominaldesmoids requiring opiates. He also had a pul-monary embolus and venous thrombosis andwas taking coumadin. He had been treated ayear earlier with tamoxifen for 8 weeks, buttumors grew during this period. He begantreatment with PLD and had a good response.Treatment was held after 6 cycles. Desmoid-type fibromatosis progression was noted 10months after the last chemotherapy, and hereceived imatinib 400 mg/d orally, but it pro-gressed. He began treatment with PLD andnoted stabilization of pain after 1 month andsome tumor shrinkage at 3 months. Threemonths later, imaging revealed further tumorregression, and the interval between PLDtreatments was increased. Subsequent imaging
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org957

revealed continued gradual tumor shrinkageand then stabilization, and PLD was discontin-ued after 1.5 years of treatment. Imagingfound stable disease at 3 years after reinitiatingPLD, but 4 months later (40 months after firstinitiating chemotherapy) he developedincreasing pain and progression of DTF on im-aging, and PLD was reinitiated. One monthlater he developed small bowel obstruction,bacteremia, and renal failure and had adecompressive gastrostomy tube placed. Hissubsequent course was complicated, and heeventually entered a hospice program anddied 5.3 years after initial chemotherapy.This case exhibits aggressive multifocal DTF,long-term control with PLD, and severeDTF-associated morbidity.
FUTURE STUDIES
Controlled trials are needed to better defineoptimal treatment approaches. Future clinicaltrials must consider several aspects of DTFbiology. First, because of the highly variableclinical course of DTF, patients must be care-fully stratified at entry. Factors to considerinclude rate of tumor growth (tumor growthrate should be quantitated before treatment).Other stratification variables should includeage at diagnosis, tumor location (mesenteric,abdominal wall, central extra-abdominal, andextremity), b-catenin mutation and APC muta-tion status, relation to pregnancy, symptoms,and tumor size. Samples should be obtainedfor future, more detailed genetic analysis;consideration should be given to obtainingcore biopsies from different parts of the tumor,if possible, given the known intratumoral vari-ability. Watchful waiting should be the firsttreatment, if possible, and when treatment isinitiated, randomization to 2 treatments isneeded. The “standard” treatment can bedebated, but given its efficacy, tolerability,and increasing popularity, PLD would be oneconsideration. Finally, a decision on howlong to treat a responding tumor and how toquantify tumor response must be considered.RECIST (Response Evaluation Criteria In SolidTumors) is known to be a poor measure ofresponse in DTF, but some measure of size(optimally careful analysis of tumor volume)and tumor “activity” (possibly determined by
FIGURE 5. Slow spontaneous regression of an extra-abdominal desmoid-
type fibromatosis (DTF) in a man. A 28-year-old man developed a firm,
fixed, nontender parasternal mass. Computed tomography revealed a mass
involving the sternum growing through the chest wall (top panel), and a
biopsy revealed DTF. He was observed, and 10 months after the biopsy the
mass was slightly smaller. At 35 months after the biopsy, his symptoms had
resolved and the mass was smaller.
MAYO CLINIC PROCEEDINGS
958 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

contrast enhancement or changes in T1/T2signal on MRI) need to be considered. Becausetumor stabilization can be a beneficialoutcome, a measure of symptoms experiencedby the patient should be included as well,including a quality of life assessment such asQLQ-C30 or FACTG. Perhaps better thannonlinear subjective variables such as a “painscale” are clear measures such as the following:is a pain medication required, how much painmedication is used, does the tumor interferewith sleep (yes/no), how far can the patientwalk before tumor pain limits the activity(this could be objectively determined at eachclinic visit for cases with serious symptoms),and what is the range of motion of the affectedbody part. Only with carefully controlled trialsthat use careful stratification based on knownvariables can the best treatment approaches forDTF be determined.
SUMMARY
Because of the heterogeneity of the biologicalbehavior of DTF, the optimal approach totreatment is unclear. Historically, surgery wasthe mainstay of treatment, but recurrence aftersurgery is common.9,31,59,111,113,115 In addi-tion, trauma can stimulate DTF growth, andsurgery is a form of trauma associated withinflammation and production of variousgrowth factors important in wound healingthat may also stimulate clonal DTF cells; thisis especially true in the case of FAP-associated mesenteric DTF.3,9,31,58,119,189
Although surgery remains an option for theinitial treatment in which the expectedmorbidity is low and the chance of completeremoval is high, given the usually slow pro-gression of DTF, a regimen with low toxicityis the preferred initial approach and observa-tion has become more standard.91,93-102 Ofcourse, the appropriate clinical decision de-pends on the particular case, and some requireaggressive chemotherapy initially.
CONCLUSION
Desmoid-type fibromatosis is an uncommonlocally invasive tumor. Because of the variablenature of the disease and the potentialmorbidity of treatment, some cases of DTFmay do better without treatment; simpleobservation is often the best initial treatment.
ACKNOWLEDGMENTS
We thank Shelly Marette, MD, for assistance ininterpreting magnetic resonance images,Michael Franklin, MS, for editorial assistance,and J. Carlos Manivel, MD, for a critical reviewof the manuscript.
SUPPLEMENTAL ONLINE MATERIAL
Supplemental material can be foundonline at: http://www.mayoclinicproceedings.org. Supplemental material attached to journalarticles has not been edited, and the authorstake responsibility for the accuracy of all data.
Abbreviations and Acronyms: APC = adenomatous
polyposis coli gene; CK1 = casein kinase 1; DTF = desmoid-
type fibromatosis; ECM = extracellular matrix; FAP = familial
adenomatous polyposis; Fap-1a = fibroblast activation
protein 1a; GSK3 = glycogen synthase kinase 3; MRI =
magnetic resonance imaging; PDGF = platelet-derived
growth factor; PDGFR-a = platelet-derived growth factor
receptor-a; PLD = pegylated-liposomal doxorubicin; TGF =
transforming growth factor
Correspondence: Address to Keith M. Skubitz, MD,
Department of Medicine, University of Minnesota Medical
School, Box 286 University Hospital, Minneapolis, MN
55455 ([email protected]).
REFERENCES
1. Alman BA, Goldberg MJ, Naber SP, Galanopoulous T,
Antoniades HN, Wolfe HJ. Aggressive fibromatosis. J Pediatr
Orthop. 1992;12(1):1-10.
2. Alman BA, Li C, Pajerski ME, Diaz-Cano S, Wolfe HJ.
Increased b-catenin protein and somatic APC mutations in
sporadic aggressive fibromatoses (desmoid tumors). Am J
Pathol. 1997;151(2):329-334.
3. Bertario L, Russo A, Sala P, et al; Hereditary Colorectal Tu-
mours Registry. Genotype and phenotype factors as determi-
nants of desmoid tumors in patients with familial
adenomatous polyposis. Int J Cancer. 2001;95(2):102-107.
4. Goldblum JR, Fletcher JA. Desmoid-type fibromatosis. In:
Fletcher DM, Bridge JA, Hogendoorn P, Mertens F, eds.
WHO Classification of Tumors of Soft Tissue and Bone, 4th ed.
Lyon: IARC; 2013:72-73.
5. Hoos A, Lewis JJ, Antonescu CR, et al. Characterization of
molecular abnormalities in human fibroblastic neoplasms: a
model for genotype-phenotype association in soft tissue
tumors. Cancer Res. 2001;61(7):3171-3175.
6. Li M, Cordon-Cardo C, Gerald WL, Rosai J. Desmoid fibro-
matosis is a clonal process. Hum Pathol. 1996;27(9):939-943.
7. Lucas DR, Shroyer KR, McCarthy PJ, Markham NE, Fujita M,
Enomoto TE. Desmoid tumor is a clonal cellular proliferation:
PCR amplification of HUMARA for analysis of patterns of
X-chromosome inactivation. Am J Surg Pathol. 1997;21(3):
306-311.
8. Middleton SB, Frayling IM, Phillips RK. Desmoids in familial
adenomatous polyposis are monoclonal proliferations. Br J
Cancer. 2000;82(4):827-832.
9. Hansmann A, Adolph C, Vogel T, Unger A, Moeslein G. High-
dose tamoxifen and sulindac as first-line treatment for des-
moid tumors. Cancer. 2004;100(3):612-620.
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org959

10. Muller J. About the fine structure and types of pathological tu-
mors [in German]. Erste Lieferung. 1838:60.
11. MacFarlane J. Clinical Report on the Surgical Practice of Glasgow
Royal Infirmary. Glasgow, UK: D. Robertson; 1832:63.
12. Ledderhose G. Desmoide Geschwulste der Bauchdecken.
Deutsch Chir. 1890;45:52-77.
13. Pfeiffer C. Die Desmoide der Bauchdecken und ihre Prog-
nose. Beitr z klin Chir. 1904;44:334-401.
14. Stout AP. Fibrosarcoma the malignant tumor of fibroblasts.
Cancer. 1948;1(1):30-63.
15. Clark SK, Neale KF, Landgrebe JC, Phillips RK. Desmoid tu-
mours complicating familial adenomatous polyposis. Br J
Surg. 1999;86(9):1185-1189.
16. Enzinger FM, Shiraki M. Musculo-aponeurotic fibromatosis of
the shoulder girdle (extra-abdominal desmoid): analysis of
thirty cases followed up for ten or more years. Cancer.
1967;20(7):1131-1140.
17. Urist MR. Trauma and neoplasm: report of a case of desmoid
tumor following simple fracture of the radius and ulna. Am J
Surg. 1957;93(4):682-688.
18. de Camargo VP, Keohan ML, D’Adamo DR, et al. Clinical
outcomes of systemic therapy for patients with deep
fibromatosis (desmoid tumor). Cancer. 2010;116(9):
2258-2265.
19. Lev D, Kotilingam D, Wei C, et al. Optimizing treatment of
desmoid tumors. J Clin Oncol. 2007;25(13):1785-1791.
20. Fallen T, Wilson M, Morlan B, Lindor NM. Desmoid
tumorsda characterization of patients seen at Mayo Clinic
1976-1999. Fam Cancer. 2006;5(2):191-194.
21. Nieuwenhuis MH, Casparie M, Mathus-Vliegen LM,
Dekkers OM, Hogendoorn PC, Vasen HF. A nation-wide
study comparing sporadic and familial adenomatous
polyposis-related desmoid-type fibromatoses. Int J Cancer.
2011;129(1):256-261.
22. Reitamo JJ, Häyry P, Nykyri E, Saxén E. The desmoid tumor. I.
Incidence, sex-, age- and anatomical distribution in the Finnish
population. Am J Clin Pathol. 1982;77(6):665-673.
23. Shields CJ, Winter DC, Kirwan WO, Redmond HP. Desmoid
tumours. Eur J Surg Oncol. 2001;27(8):701-706.
24. Giardiello FM, Petersen GM, Piantadosi S, et al. APC gene mu-
tations and extraintestinal phenotype of familial adenomatous
polyposis. Gut. 1997;40(4):521-525.
25. Gurbuz AK, Giardiello FM, Petersen GM, et al. Desmoid tu-
mours in familial adenomatous polyposis. Gut. 1994;35(3):
377-381.
26. Hizawa K, Iida M, Mibu R, Aoyagi K, Yao T, Fujishima M. Des-
moid tumors in familial adenomatous polyposis/Gardner’s
syndrome. J Clin Gastroenterol. 1997;25(1):334-337.
27. Gardner EJ. A genetic and clinical study of intestinal polyposis,
a predisposing factor for carcinoma of the colon and rectum.
Am J Hum Genet. 1951;3(2):167-176.
28. Nichols RW. Desmoid tumors: a report of thirty-one cases.
Arch Surg. 1923;7:227-236.
29. Smith WG. Multiple polyposis, Gardner’s syndrome and des-
moid tumors. Dis Colon Rectum. 1958;1(5):323-332.
30. Clark SK, Phillips RK. Desmoids in familial adenomatous polyp-
osis. Br J Surg. 1996;83(11):1494-1504.
31. Jones IT, Jagelman DG, Fazio VW, Lavery IC, Weakley FL,
McGannon E. Desmoid tumors in familial polyposis coli. Ann
Surg. 1986;204(1):94-97.
32. Klemmer S, Pascoe L, DeCosse J. Occurrence of desmoids in
patients with familial adenomatous polyposis of the colon. Am
J Med Genet. 1987;28(2):385-392.
33. Nieuwenhuis MH, Mathus-Vliegen EM, Baeten CG, et al. Eval-
uation of management of desmoid tumours associated with
familial adenomatous polyposis in Dutch patients. Br J Cancer.
2011;104(1):37-42.
34. Arvanitis ML, Jagelman DG, Fazio VW, Lavery IC,
McGannon E. Mortality in patients with familial adenomatous
polyposis. Dis Colon Rectum. 1990;33(8):639-642.
35. Caspari R, Olschwang S, Friedl W, et al. Familial adenomatous
polyposis: desmoid tumours and lack of ophthalmic lesions
(CHRPE) associated with APC mutations beyond codon
1444. Hum Mol Genet. 1995;4(3):337-340.
36. Eccles DM, van der Luijt R, Breukel C, et al. Hereditary des-
moid disease due to a frameshift mutation at codon 1924
of the APC gene. Am J Hum Genet. 1996;59(6):1193-1201.
37. Scott RJ, Froggatt NJ, Trembath RC, Evans DG, Hodgson SV,
Maher ER. Familial infiltrative fibromatosis (desmoid tumours)
(MIM135290) caused by a recurrent 30 APC gene mutation.
Hum Mol Genet. 1996;5(12):1921-1924.
38. Sturt NJ, Gallagher MC, Bassett P, et al. Evidence for genetic
predisposition to desmoid tumours in familial adenomatous
polyposis independent of the germline APC mutation. Gut.
2004;53(12):1832-1836.
39. Amary MF, Pauwels P, Meulemans E, et al. Detection of b-cat-
enin mutations in paraffin-embedded sporadic desmoid-type
fibromatosis by mutation-specific restriction enzyme digestion
(MSRED): an ancillary diagnostic tool. Am J Surg Pathol. 2007;
31(9):1299-1309.
40. Dômont J, Salas S, Lacroix L, et al. High frequency of b-catenin
heterozygous mutations in extra-abdominal fibromatosis: a
potential molecular tool for disease management. Br J Cancer.
2010;102(6):1032-1036.
41. Lazar AJ, Tuvin D, Hajibashi S, et al. Specific mutations in the
b-catenin gene (CTNNB1) correlate with local recurrence in
sporadic desmoid tumors. Am J Pathol. 2008;173(5):1518-1527.
42. Le Guellec S, Soubeyran I, Rochaix P, et al. CTNNB1 muta-
tion analysis is a useful tool for the diagnosis of desmoid
tumors: a study of 260 desmoid tumors and 191 potential
morphologic mimics. Mod Pathol. 2012;25(12):1551-1558.
43. Salas S, Chibon F, Noguchi T, et al. Molecular characterization
by array comparative genomic hybridization and DNA
sequencing of 194 desmoid tumors. Genes Chromosomes Can-
cer. 2010;49(6):560-568.
44. Tejpar S, Nollet F, Li C, et al. Predominance of b-catenin mu-
tations and b-catenin dysregulation in sporadic aggressive
fibromatosis (desmoid tumor). Oncogene. 1999;18(47):
6615-6620.
45. Bo N, Wang D, Wu B, Chen L, Ruixue M. Analysis of
b-catenin expression and exon 3 mutations in pediatric spo-
radic aggressive fibromatosis. Pediatr Dev Pathol. 2012;15(3):
173-178.
46. Meazza C, Bisogno G, Gronchi A, et al. Aggressive fibromato-
sis in children and adolescents: the Italian experience. Cancer.
2010;116(1):233-240.
47. Francastel C, Schübeler D, Martin DI, Groudine M. Nuclear
compartmentalization and gene activity. Nat Rev Mol Cell
Biol. 2000;1(2):137-143.
48. Misemer BS, Skubitz AP, Carlos Manivel J, et al. Expression of
FAP, ADAM12, WISP1, and SOX11 is heterogeneous in
aggressive fibromatosis and spatially relates to the histologic
features of tumor activity. Cancer Med. 2014;3(1):81-90.
49. Colombo C, Miceli R, Lazar AJ, et al. CTNNB1 45F mutation
is a molecular prognosticator of increased postoperative pri-
mary desmoid tumor recurrence: an independent, multicenter
validation study. Cancer. 2013;119(20):3696-3702.
50. Lacroix-Triki M, Geyer FC, Lambros MB, et al. b-Catenin/Wnt
signalling pathway in fibromatosis, metaplastic carcinomas and
phyllodes tumours of the breast. Mod Pathol. 2010;23(11):
1438-1448.
51. Skubitz KM, Skubitz AP. Gene expression in aggressive fibro-
matosis. J Lab Clin Med. 2004;143(2):89-98.
52. Miyoshi Y, Iwao K, Nawa G, Yoshikawa H, Ochi T,
Nakamura Y. Frequent mutations in the b-catenin gene in
desmoid tumors from patients without familial adenomatous
polyposis. Oncol Res. 1998;10(11-12):591-594.
53. Mullen JT, DeLaney TF, Rosenberg AE, et al. b-Catenin muta-
tion status and outcomes in sporadic desmoid tumors. Oncol-
ogist. 2013;18(9):1043-1049.
MAYO CLINIC PROCEEDINGS
960 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

54. Saito T, Oda Y, Kawaguchi K, et al. Possible association be-
tween higher b-catenin mRNA expression and mutated
b-catenin in sporadic desmoid tumors: real-time semiquantita-
tive assay by TaqMan polymerase chain reaction. Lab Invest.
2002;82(1):97-103.
55. Shitoh K, Konishi F, Iijima T, et al. A novel case of a sporadic
desmoid tumour with mutation of the b catenin gene. J Clin
Pathol. 1999;52(9):695-696.
56. van Broekhoven DL, Verhoef C, Grünhagen DJ, et al.
Prognostic value of CTNNB1 gene mutation in primary spo-
radic aggressive fibromatosis. Ann Surg Oncol. 2015;22(5):
1464-1470.
57. Couture J, Mitri A, Lagace R, et al. A germline mutation at
the extreme 30 end of the APC gene results in a severe
desmoid phenotype and is associated with overexpression
of b-catenin in the desmoid tumor. Clin Genet. 2000;57(3):
205-212.
58. Harvey JC, Quan SH, Fortner JG. Gardner’s syndrome compli-
cated by mesenteric desmoid tumors. Surgery. 1979;85(4):
475-477.
59. Rodriguez-Bigas MA, Mahoney MC, Karakousis CP, Petrelli NJ.
Desmoid tumors in patients with familial adenomatous polyp-
osis. Cancer. 1994;74(4):1270-1274.
60. De Wever I, Dal Cin P, Fletcher CD, et al. Cytogenetic, clin-
ical, and morphologic correlations in 78 cases of fibromatosis:
a report from the CHAMP Study Group. CHromosomes And
Morphology. Mod Pathol. 2000;13(10):1080-1085.
61. Robanus-Maandag E, Bosch C, Amini-Nik S, et al. Familial
adenomatous polyposis-associated desmoids display signifi-
cantly more genetic changes than sporadic desmoids. PLoS
One. 2011;6(9):e24354.
62. Church J, Xhaja X, LaGuardia L, O’Malley M, Burke C,
Kalady M. Desmoids and genotype in familial adenomatous
polyposis. Dis Colon Rectum. 2015;58(4):444-448.
63. Cheon SS, Cheah AY, Turley S, et al. b-Catenin stabilization
dysregulates mesenchymal cell proliferation, motility, and inva-
siveness and causes aggressive fibromatosis and hyperplastic
cutaneous wounds. Proc Natl Acad Sci U S A. 2002;99(10):
6973-6978.
64. Heinrich MC, McArthur GA, Demetri GD, et al. Clinical and
molecular studies of the effect of imatinib on advanced
aggressive fibromatosis (desmoid tumor). J Clin Oncol. 2006;
24(7):1195-1203.
65. Smits R, van der Houven van Oordt W, Luz A, et al.
Apc1638N: a mouse model for familial adenomatous
polyposis-associated desmoid tumors and cutaneous cysts.
Gastroenterology. 1998;114(2):275-283.
66. Alman BA, Greel DA, Ruby LK, Goldberg MJ, Wolfe HJ.
Regulation of proliferation and platelet-derived growth fac-
tor expression in palmar fibromatosis (Dupuytren contrac-
ture) by mechanical strain. J Orthop Res. 1996;14(5):
722-728.
67. de Andrade CR, Cotrin P, Graner E, Almeida OP, Sauk JJ,
Coletta RD. Transforming growth factor-b1 autocrine stim-
ulation regulates fibroblast proliferation in hereditary gingival
fibromatosis. J Periodontol. 2001;72(12):1726-1733.
68. Magro G, Lanteri E, Micali G, Paravizzini G, Travali S,
Lanzafame S. Myofibroblasts of palmar fibromatosis
co-express transforming growth factor-a and epidermal
growth factor receptor. J Pathol. 1997;181(2):213-217.
69. Carothers AM, Rizvi H, Hasson RM, et al. Mesenchymal
stromal cell mutations and wound healing contribute to
the etiology of desmoid tumors. Cancer Res. 2012;72(1):
346-355.
70. Sato S, Tang YJ, Wei Q, et al. Mesenchymal tumors can
derive from Ng2/Cspg4-expressing pericytes with b-catenin
modulating the neoplastic phenotype. Cell Rep. 2016;16(4):
917-927.
71. Morin PJ. b-Catenin signaling and cancer. Bioessays. 1999;
21(12):1021-1030.
72. McCrea PD, Turck CW, Gumbiner B. A homolog of the
armadillo protein in Drosophila (plakoglobin) associated
with E-cadherin. Science. 1991;254(5036):1359-1361.
73. Minde DP, Anvarian Z, Rüdiger SG, Maurice MM. Messing up
disorder: how do missense mutations in the tumor suppressor
protein APC lead to cancer? Mol Cancer. 2011;10:101.
74. Willert K, Jones KA. Wnt signaling: is the party in the nucleus?
Genes Dev. 2006;20(11):1394-1404.
75. Ghanbari-Azarnier R, Sato S, Wei Q, Al-Jazrawe M,
Alman BA. Targeting stem cell behavior in desmoid tumors
(aggressive fibromatosis) by inhibiting hedgehog signaling.
Neoplasia. 2013;15(7):712-719.
76. Acharya PS, Zukas A, Chandan V, Katzenstein AL, Puré E.
Fibroblast activation protein: a serine protease expressed at
the remodeling interface in idiopathic pulmonary fibrosis.
Hum Pathol. 2006;37(3):352-360.
77. Lafuste P, Sonnet C, Chazaud B, et al. ADAM12 and a9b1
integrin are instrumental in human myogenic cell differentia-
tion. Mol Biol Cell. 2005;16(2):861-870.
78. Thodeti CK, Fröhlich C, Nielsen CK, et al. ADAM12-mediated
focal adhesion formation is differently regulated by b1 and b3
integrins. FEBS Lett. 2005;579(25):5589-5595.
79. Shih B, Brown JJ, Armstrong DJ, Lindau T, Bayat A. Differential
gene expression analysis of subcutaneous fat, fascia, and skin
overlying a Dupuytren’s disease nodule in comparison to con-
trol tissue. Hand (N Y). 2009;4(3):294-301.
80. Dulauroy S, Di Carlo SE, Langa F, Eberl G, Peduto L. Lineage
tracing and genetic ablation of ADAM12(þ) perivascular cells
identify a major source of profibrotic cells during acute tissue
injury. Nat Med. 2012;18(8):1262-1270.
81. Niehrs C. The complex world of WNT receptor signalling.
Nat Rev Mol Cell Biol. 2012;13(12):767-779.
82. Bauer M, Su G, Casper C, He R, Rehrauer W, Friedl A.
Heterogeneity of gene expression in stromal fibroblasts of hu-
man breast carcinomas and normal breast. Oncogene. 2010;
29(12):1732-1740.
83. Bacac M, Migliavacca E, Stehle JC, et al. A gene expression
signature that distinguishes desmoid tumours from nodular
fasciitis. J Pathol. 2006;208(4):543-553.
84. West RB, Nuyten DS, Subramanian S, et al. Determination of
stromal signatures in breast carcinoma. PLoS Biol. 2005;3(6):
e187.
85. Königshoff M, Kramer M, Balsara N, et al. WNT1-inducible
signaling protein-1 mediates pulmonary fibrosis in mice and
is upregulated in humans with idiopathic pulmonary fibrosis.
J Clin Invest. 2009;119(4):772-787.
86. Brennan DJ, Ek S, Doyle E, et al. The transcription factor
Sox11 is a prognostic factor for improved recurrence-free
survival in epithelial ovarian cancer. Eur J Cancer. 2009;45(8):
1510-1517.
87. Skubitz KM, Cheng EY, Clohisy DR, Thompson RC,
Skubitz AP. Differential gene expression in liposarcoma, li-
poma, and adipose tissue. Cancer Invest. 2005;23(2):105-118.
88. Kubo H, Shimizu M, Taya Y, et al. Identification of mesen-
chymal stem cell (MSC)-transcription factors by microarray
and knockdown analyses, and signature molecule-marked
MSC in bone marrow by immunohistochemistry. Genes Cells.
2009;14(3):407-424.
89. Venkatesan B, Prabhu SD, Venkatachalam K, et al. WNT1-
inducible signaling pathway protein-1 activates diverse cell
survival pathways and blocks doxorubicin-induced cardiomyo-
cyte death. Cell Signal. 2010;22(5):809-820.
90. Lewis JJ, Boland PJ, Leung DH, Woodruff JM, Brennan MF. The
enigma of desmoid tumors. Ann Surg. 1999;229(6):866-872;
discussion 872-873.
91. Mitchell G, Thomas JM, Harmer CL. Aggressive fibromatosis:
evidence for a stable phase. Sarcoma. 1998;2(3-4):149-154.
92. Rock MG, Pritchard DJ, Reiman HM, Soule EH, Brewster RC.
Extra-abdominal desmoid tumors. J Bone Joint Surg Am. 1984;
66(9):1369-1374.
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org961

93. Bonvalot S, Desai A, Coppola S, et al. The treatment of des-
moid tumors: a stepwise clinical approach. Ann Oncol. 2012;
23(suppl 10):x158-x166.
94. Bonvalot S, Eldweny H, Haddad V, et al. Extra-abdominal
primary fibromatosis: Aggressive management could be
avoided in a subgroup of patients. Eur J Surg Oncol. 2008;
34(4):462-468.
95. Bonvalot S, Ternes N, Fiore M, et al. Spontaneous regres-
sion of primary abdominal wall desmoid tumors: more
common than previously thought. Ann Surg Oncol. 2013;
20(13):4096-4102.
96. Colombo C, Miceli R, Le Péchoux C, et al. Sporadic extra
abdominal wall desmoid-type fibromatosis: surgical resection
can be safely limited to a minority of patients. Eur J Cancer.
2015;51(2):186-192.
97. Eastley N, McCulloch T, Esler C, et al. Extra-abdominal
desmoid fibromatosis: a review of management, current guid-
ance and unanswered questions. Eur J Surg Oncol. 2016;42(7):
1071-1083.
98. Garbay D, Le Cesne A, Penel N, et al. Chemotherapy in
patients with desmoid tumors: a study from the French
Sarcoma Group (FSG). Ann Oncol. 2012;23(1):182-186.
99. Gronchi A, Colombo C, Le Péchoux C, et al. Sporadic
desmoid-type fibromatosis: a stepwise approach to a non-
metastasising neoplasmda position paper from the Italian
and the French Sarcoma Group. Ann Oncol. 2014;25(3):
578-583.
100. Nakayama T, Tsuboyama T, Toguchida J, Hosaka T,
Nakamura T. Natural course of desmoid-type fibromatosis.
J Orthop Sci. 2008;13(1):51-55.
101. Roussin S, Mazouni C, Rimareix F, et al. Toward a new strat-
egy in desmoid of the breast? Eur J Surg Oncol. 2015;41(4):
571-576.
102. Salas S, Dufresne A, Bui B, et al. Prognostic factors influencing
progression-free survival determined from a series of sporadic
desmoid tumors: a wait-and-see policy according to tumor
presentation. J Clin Oncol. 2011;29(26):3553-3558.
103. Joglekar SB, Rose PS, Sim F, Okuno S, Petersen I. Current per-
spectives on desmoid tumors: the Mayo Clinic approach. Can-
cers (Basel). 2011;3(3):3143-3155.
104. Briand S, Barbier O, Biau D, et al. Wait-and-see policy as a
first-line management for extra-abdominal desmoid tumors.
J Bone Joint Surg Am. 2014;96(8):631-638.
105. Boyne MS, Thame M, Bennett FI, Osmond C, Miell JP,
Forrester TE. The relationship among circulating insulin-like
growth factor (IGF)-I, IGF-binding proteins-1 and -2, and birth
anthropometry: a prospective study. J Clin Endocrinol Metab.
2003;88(4):1687-1691.
106. Forbes K, Westwood M. Maternal growth factor regulation of
human placental development and fetal growth. J Endocrinol.
2010;207(1):1-16.
107. Singh M, Orazulike NC, Ashmore J, Konje JC. Changes in
maternal serum transforming growth factor b-1 during preg-
nancy: a cross-sectional study. Biomed Res Int. 2013;2013:
318464.
108. Vonnahme KA, Wilson ME, Li Y, et al. Circulating levels of ni-
tric oxide and vascular endothelial growth factor throughout
ovine pregnancy. J Physiol. 2005;565(pt 1):101-109.
109. Fiore M, Coppola S, Cannell AJ, et al. Desmoid-type fibroma-
tosis and pregnancy: a multi-institutional analysis of recurrence
and obstetric risk. Ann Surg. 2014;259(5):973-978.
110. Cates JM. Pregnancy does not increase the local recurrence
rate after surgical resection of desmoid-type fibromatosis. Int
J Clin Oncol. 2015;20(3):617-622.
111. Anthony T, Rodriguez-Bigas MA, Weber TK, Petrelli NJ. Des-
moid tumors. J Am Coll Surg. 1996;182(4):369-377.
112. Ballo MT, Zagars GK, Pollack A, Pisters PW, Pollack RA. Des-
moid tumor: prognostic factors and outcome after surgery, ra-
diation therapy, or combined surgery and radiation therapy.
J Clin Oncol. 1999;17(1):158-167.
113. Dong-Heup K, Kim DH, Goldsmith HS, Quan SH,
Huvos AG. Intra-abdominal desmoid tumor. Cancer. 1971;
27(5):1041-1045.
114. Gronchi A, Casali PG, Mariani L, et al. Quality of surgery and
outcome in extra-abdominal aggressive fibromatosis: a series
of patients surgically treated at a single institution. J Clin Oncol.
2003;21(7):1390-1397.
115. Johnson JG, Gilbert E, Zimmermann B, Watne AL. Gardner’s
syndrome, colon cancer, and sarcoma. J Surg Oncol. 1972;4(4):
354-362.
116. Leibel SA, Wara WM, Hill DR, et al. Desmoid tumors: local
control and patterns of relapse following radiation therapy.
Int J Radiat Oncol Biol Phys. 1983;9(8):1167-1171.
117. Pignatti G, Barbanti-Bròdano G, Ferrari D, et al. Extraabdomi-
nal desmoid tumor: a study of 83 cases. Clin Orthop Relat Res.
2000;(375):207-213.
118. Posner MC, Shiu MH, Newsome JL, Hajdu SI, Gaynor JJ,
Brennan MF. The desmoid tumor. Not a benign disease.
Arch Surg. 1989;124(2):191-196.
119. Reitamo JJ. The desmoid tumor. IV. Choice of treatment, re-
sults, and complications. Arch Surg. 1983;118(11):1318-1322.
120. Sørensen A, Keller J, Nielsen OS, Jensen OM. Treatment of
aggressive fibromatosis: a retrospective study of 72 patients
followed for 1-27 years. Acta Orthop Scand. 2002;73(2):
213-219.
121. Crago AM, Denton B, Salas S, et al. A prognostic nomogram
for prediction of recurrence in desmoid fibromatosis. Ann
Surg. 2013;258(2):347-353.
122. Jelinek JA, Stelzer KJ, Conrad E, et al. The efficacy of radio-
therapy as postoperative treatment for desmoid tumors. Int
J Radiat Oncol Biol Phys. 2001;50(1):121-125.
123. Kiel KD, Suit HD. Radiation therapy in the treatment of
aggressive fibromatoses (desmoid tumors). Cancer. 1984;
54(10):2051-2055.
124. Kriz J, Eich HT, Haverkamp U, et al. Radiotherapy is effective
for desmoid tumors (aggressive fibromatosis)dlong-term re-
sults of a German multicenter study. Oncol Res Treat. 2014;
37(5):255-260.
125. McCollough WM, Parsons JT, van der Griend R, Enneking WF,
Heare T. Radiation therapy for aggressive fibromatosis: the
experience at the University of Florida. J Bone Joint Surg Am.
1991;73(5):717-725.
126. Mendenhall WM, Zlotecki RA, Morris CG, Hochwald SN,
Scarborough MT. Aggressive fibromatosis. Am J Clin Oncol.
2005;28(2):211-215.
127. Suit H, Spiro I. Radiation in the multidisciplinary management
of desmoid tumors. Front Radiat Ther Oncol. 2001;35:107-119.
128. Ma D, Li S, Fu R, et al. Long-term outcomes of 47 patients
with aggressive fibromatosis of the chest treated with surgery.
Eur J Surg Oncol. 2016;42(11):1693-1698.
129. Constantinidou A, Jones RL, Scurr M, Al-Muderis O, Judson I.
Pegylated liposomal doxorubicin, an effective, well-tolerated
treatment for refractory aggressive fibromatosis. Eur J Cancer.
2009;45(17):2930-2934.
130. Constantinidou A, Jones RL, Scurr M, Al-Muderis O, Judson I.
Advanced aggressive fibromatosis: effective palliation with
chemotherapy. Acta Oncol. 2011;50(3):455-461.
131. Nuyttens JJ, Rust PF, Thomas CR Jr, Turrisi AT III. Surgery
versus radiation therapy for patients with aggressive fibroma-
tosis or desmoid tumors: a comparative review of 22 articles.
Cancer. 2000;88(7):1517-1523.
132. Verschoor AJ, Cleton-Jansen AM, Wijers-Koster P, et al. Radi-
ation-induced sarcomas occurring in desmoid-type fibromato-
sis are not always derived from the primary tumor. Am J Surg
Pathol. 2015;39(12):1701-1707.
133. Schmitz JJ, Schmit GD, Atwell TD, et al. Percutaneous cryoa-
blation of extraabdominal desmoid tumors: a 10-year experi-
ence. AJR Am J Roentgenol. 2016;207(1):190-195.
134. Klein WA, Miller HH, Anderson M, DeCosse JJ. The use of
indomethacin, sulindac, and tamoxifen for the treatment of
MAYO CLINIC PROCEEDINGS
962 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org

desmoid tumors associated with familial polyposis. Cancer.
1987;60(12):2863-2868.
135. Waddell WR, Gerner RE. Indomethacin and ascorbate inhibit
desmoid tumors. J Surg Oncol. 1980;15(1):85-90.
136. Waddell WR, Kirsch WM. Testolactone, sulindac, warfarin,
and vitamin K1 for unresectable desmoid tumors. Am J Surg.
1991;161(4):416-421.
137. Kinzbrunner B, Ritter S, Domingo J, Rosenthal CJ. Remission of
rapidly growing desmoid tumors after tamoxifen therapy. Can-
cer. 1983;52(12):2201-2204.
138. Lim CL, Walker MJ, Mehta RR, Das Gupta TK. Estrogen and
antiestrogen binding sites in desmoid tumors. Eur J Cancer
Clin Oncol. 1986;22(5):583-587.
139. Mukherjee A, Malcolm A, de la Hunt M, Neal DE. Pelvic fibro-
matosis (desmoid)dtreatment with steroids and tamoxifen.
Br J Urol. 1995;75(4):559-560.
140. Wilcken N, Tattersall MH. Endocrine therapy for desmoid tu-
mors. Cancer. 1991;68(6):1384-1388.
141. Gega M, Yanagi H, Yoshikawa R, et al. Successful chemother-
apeutic modality of doxorubicin plus dacarbazine for the
treatment of desmoid tumors in association with familial
adenomatous polyposis. J Clin Oncol. 2006;24(1):102-105.
142. Hutchinson RJ, Norris DG, Schnaufer L. Chemotherapy: a suc-
cessful application in abdominal fibromatosis. Pediatrics. 1979;
63(1):157-159.
143. Kasper B, Ströbel P, Hohenberger P. Desmoid tumors: clinical
features and treatment options for advanced disease. Oncolo-
gist. 2011;16(5):682-693.
144. Lynch HT, Fitzgibbons R Jr, Chong S, et al. Use of doxorubicin
and dacarbazine for the management of unresectable intra-
abdominal desmoid tumors in Gardner’s syndrome. Dis Colon
Rectum. 1994;37(3):260-267.
145. Okuno SH, Edmonson JH. Combination chemotherapy for
desmoid tumors. Cancer. 2003;97(4):1134-1135.
146. Patel SR, Benjamin RS. Desmoid tumors respond to chemo-
therapy: defying the dogma in oncology. J Clin Oncol. 2006;
24(1):11-12.
147. Patel SR, Evans HL, Benjamin RS. Combination chemotherapy
in adult desmoid tumors. Cancer. 1993;72(11):3244-3247.
148. Stein R. Chemotherapeutic response in fibromatosis of the
neck. J Pediatr. 1977;90(3):482-483.
149. Dominguez-Malagon HR, Alfeiran-Ruiz A, Chavarria-
Xicotencatl P, Duran-HernandezMS. Clinical and cellular effects
of colchicine in fibromatosis. Cancer. 1992;69(10):2478-2483.
150. Ferah Y, Ayse K, Mustafa C, Ugur S, Murat G, Lale AI. Possible
therapeutic role of vitamin D3 in aggressive fibromatosis. Jpn J
Clin Oncol. 2004;34(8):472-475.
151. Ahn JM, Yoon HK, Suh YL, et al. Infantile fibromatosis in child-
hood: findings on MR imaging and pathologic correlation. Clin
Radiol. 2000;55(1):19-24.
152. Guglielmi G, Cifaratti A, Scalzo G, Magarelli N. Imaging of su-
perficial and deep fibromatosis. Radiol Med. 2009;114(8):
1292-1307.
153. Lee JC, Thomas JM, Phillips S, Fisher C, Moskovic E. Aggressive
fibromatosis: MRI features with pathologic correlation. AJR Am
J Roentgenol. 2006;186(1):247-254.
154. O’Keefe F, Kim EE, Wallace S. Magnetic resonance imaging in
aggressive fibromatosis. Clin Radiol. 1990;42(3):170-173.
155. Gounder MM, Lefkowitz RA, Keohan ML, et al. Activity of Sor-
afenib against desmoid tumor/deep fibromatosis. Clin Cancer
Res. 2011;17(12):4082-4090.
156. Martin-Liberal J, Benson C, McCarty H, Thway K, Messiou C,
Judson I. Pazopanib is an active treatment in desmoid tumour/
aggressive fibromatosis. Clin Sarcoma Res. 2013;3(1):13.
157. Deyrup AT, Tretiakova M, Montag AG. Estrogen receptor-b
expression in extraabdominal fibromatoses: an analysis of 40
cases. Cancer. 2006;106(1):208-213.
158. Janinis J, Patriki M, Vini L, Aravantinos G, Whelan JS. The phar-
macological treatment of aggressive fibromatosis: a systematic
review. Ann Oncol. 2003;14(2):181-190.
159. Waddell WR. Treatment of intra-abdominal and abdominal
wall desmoid tumors with drugs that affect the metabolism
of cyclic 30 ,50-adenosine monophosphate. Ann Surg. 1975;
181(3):299-302.
160. Svanvik J, Knutsson F, Jansson R, Ekman H. Desmoid tu-
mor in the abdominal wall after treatment with high
dose estradiol for prostatic cancer. Acta Chir Scand.
1982;148(3):301-303.
161. Hong H, Nadesan P, Poon R, Alman BA. Testosterone regu-
lates cell proliferation in aggressive fibromatosis (desmoid
tumour). Br J Cancer. 2011;104(9):1452-1458.
162. Azzarelli A, Gronchi A, Bertulli R, et al. Low-dose chemo-
therapy with methotrexate and vinblastine for patients
with advanced aggressive fibromatosis. Cancer. 2001;92(5):
1259-1264.
163. Skapek SX, Hawk BJ, Hoffer FA, et al. Combination chemo-
therapy using vinblastine and methotrexate for the treatment
of progressive desmoid tumor in children. J Clin Oncol. 1998;
16(9):3021-3027.
164. Weiss AJ, Lackman RD. Low-dose chemotherapy of desmoid
tumors. Cancer. 1989;64(6):1192-1194.
165. Weiss AJ, Lackman RD. Therapy of desmoid tumors and
related neoplasms. Compr Ther. 1991;17(12):32-34.
166. Weiss AJ, Horowitz S, Lackman RD. Therapy of desmoid tumors
and fibromatosis using vinorelbine [published correction appears
in Am J Clin Oncol. 1999;22(3):followi. Lackmen RD [corrected to
Lackman RD]]. Am J Clin Oncol. 1999;22(2):193-195.
167. van der Hul RL, Seynaeve C, van Geel BN, Verweij J. Low
dose methotrexate and vinblastine, given weekly to patients
with desmoid tumours, is associated with major toxicity.
Sarcoma. 2003;7(3-4):153-157.
168. Seiter K, Kemeny N. Successful treatment of a desmoid tumor
with doxorubicin. Cancer. 1993;71(7):2242-2244.
169. Skubitz KM, Manivel JC, Clohisy DR, Frolich JW. Response of
imatinib-resistant extra-abdominal aggressive fibromatosis to
sunitinib: case report and review of the literature on response
to tyrosine kinase inhibitors. Cancer Chemother Pharmacol.
2009;64(3):635-640.
170. Chugh R, Wathen JK, Patel SR, et al; Sarcoma Alliance for
Research through Collaboration (SARC). Efficacy of imatinib
in aggressive fibromatosis: results of a phase II multicenter Sar-
coma Alliance for Research through Collaboration (SARC)
trial. Clin Cancer Res. 2010;16(19):4884-4891.
171. Mace J, Sybil Biermann J, Sondak V, et al. Response of extra-
abdominal desmoid tumors to therapy with imatinib mesylate.
Cancer. 2002;95(11):2373-2379.
172. Penel N, Le Cesne A, Bui BN, et al. Imatinib for progressive
and recurrent aggressive fibromatosis (desmoid tumors): an
FNCLCC/French Sarcoma Group phase II trial with a long-
term follow-up. Ann Oncol. 2011;22(2):452-457.
173. Wcislo G, Szarlej-Wcislo K, Szczylik C. Control of aggressive
fibromatosis by treatment with imatinib mesylate: a case
report and review of the literature. J Cancer Res Clin Oncol.
2007;133(8):533-538.
174. Dao A, Benchakroun N, Jabir H, et al. Five years of local
control of subscapularis aggressive fibromatosis managed
by surgery and imatinib: a case report. J Med Case Rep.
2014;8:416.
175. Ju KD, Kim HJ, Tsogbadrakh B, et al. HL156A, a novel AMP-
activated protein kinase activator, is protective against perito-
neal fibrosis in an in vivo and in vitro model of peritoneal
fibrosis. Am J Physiol Renal Physiol. 2016;310(5):F342-F350.
176. Kasper B, Gruenwald V, Reichardt P, Bauer S, Hohenberger P,
Haller F. Correlation of CTNNB1 mutation status with pro-
gression arrest rate in RECIST progressive desmoid-type fibro-
matosis treated with imatinib: translational research results
from a phase 2 study of the German Interdisciplinary Sarcoma
Group (GISG-01). Ann Surg Oncol. 2016;23(6):1924-1927.
177. Kasper B, Baumgarten C, Bonvalot S, et al; Desmoid Working
Group. Management of sporadic desmoid-type fibromatosis: a
AGGRESSIVE FIBROMATOSIS OR DESMOID TUMOR
Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org963

European consensus approach based on patients’ and profes-
sionals’ expertiseda sarcoma patients EuroNet and European
Organisation for Research and Treatment of Cancer/Soft Tis-
sue and Bone Sarcoma Group initiative. Eur J Cancer. 2015;
51(2):127-136.
178. Gebert C, Hardes J, Kersting C, et al. Expression of b-catenin
and p53 are prognostic factors in deep aggressive fibromato-
sis. Histopathology. 2007;50(4):491-497.
179. Fletcher JA, Naeem R, Xiao S, Corson JM. Chromosome ab-
errations in desmoid tumors: trisomy 8 may be a predictor of
recurrence. Cancer Genet Cytogenet. 1995;79(2):139-143.
180. Dufresne A, Paturel M, Alberti L, et al. Prediction of desmoid
tumor progression using miRNA expression profiling. Cancer
Sci. 2015;106(5):650-655.
181. Salas S, Brulard C, Terrier P, et al. Gene expression profiling
of desmoid tumors by cDNA microarrays and correlation
with progression-free survival. Clin Cancer Res. 2015;21(18):
4194-4200.
182. Dvorak HF. Tumors: wounds that do not heal. Similarities be-
tween tumor stroma generation and wound healing. N Engl J
Med. 1986;315(26):1650-1659.
183. Hanahan D, Coussens LM. Accessories to the crime: functions
of cells recruited to the tumor microenvironment. Cancer Cell.
2012;21(3):309-322.
184. Brennen WN, Rosen DM, Wang H, Isaacs JT,
Denmeade SR. Targeting carcinoma-associated fibroblasts
within the tumor stroma with a fibroblast activation
protein-activated prodrug. J Natl Cancer Inst. 2012;104(17):
1320-1334.
185. Skubitz KM, Francis P, Skubitz AP, Luo X, Nilbert M. Gene
expression identifies heterogeneity of metastatic propensity
in high-grade soft tissue sarcomas. Cancer. 2012;118(17):
4235-4243.
186. Skubitz KM, Geschwind K, Xu WW, Koopmeiners JS,
Skubitz AP. Gene expression identifies heterogeneity of met-
astatic behavior among gastrointestinal stromal tumors. J Transl
Med. 2016;14:51.
187. Skubitz KM, Skubitz AP, Xu WW, et al. Gene expression iden-
tifies heterogeneity of metastatic behavior among high-grade
non-translocation associated soft tissue sarcomas. J Transl
Med. 2014;12:176.
188. Beck AH, Espinosa I, Gilks CB, van de Rijn M, West RB. The
fibromatosis signature defines a robust stromal response in
breast carcinoma. Lab Invest. 2008;88(6):591-601.
189. Friedl W, Caspari R, Sengteller M, et al. Can APC mutation
analysis contribute to therapeutic decisions in familial adeno-
matous polyposis? Experience from 680 FAP families. Gut.
2001;48(4):515-521.
MAYO CLINIC PROCEEDINGS
964 Mayo Clin Proc. n June 2017;92(6):947-964 n http://dx.doi.org/10.1016/j.mayocp.2017.02.012
www.mayoclinicproceedings.org




![Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis · intra-abdominal and involving the small bowel mesentery [2]. TREATMENT Surgery Margin-negative resection has historically](https://static.fdocuments.net/doc/165x107/5e5a290071d21b380f5b7e74/intra-abdominal-and-abdominal-wall-desmoid-fibromatosis-intra-abdominal-and-involving.jpg)