Radiotherapy And Fibromatosis
34
Radiotherapy and fibromatosis Martin Robinson 2008
-
Upload
fondas-vakalis -
Category
Health & Medicine
-
view
1.398 -
download
1
Transcript of Radiotherapy And Fibromatosis
Radiotherapy and fibromatosis
Martin Robinson 2008


Copyright © 2006 by the American Roentgen Ray Society
Lee, J. C. et al. Am. J. Roentgenol. 2006;186:247-254
--28-year-old woman who presented with painful lump in upper arm

Copyright © 2007 by the American Roentgen Ray Society
Lee, J. C. et al. Am. J. Roentgenol. 2006;186:247-254
--60-year-old man who presented with incidental finding on conventional radiography

McCollough 1991 – response to RT

Park RT
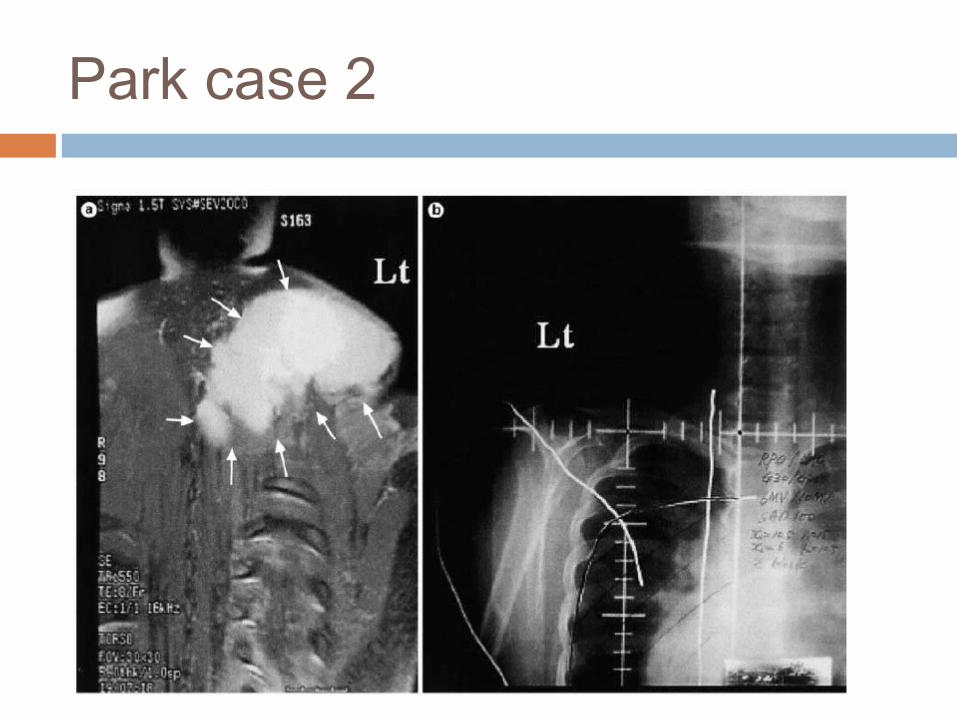
Park case 2
8
S u r g e r y v e r s u s R a d ia t io n Th e r a p y f o r P a t ie n t s w it h
Ag g r e s s iv e F ib r o m a t o s is o r D e s m o id Tu m o r s
2 2 A C o m p a r a t iv e R e v ie w o f A r t ic le s
Nuttyens 2000

9
Nuttyens
Dose Radiotherapy 10 - 72Gy
Median follow up 5-10 years.

1 0
Surgery 381
Radiation 102
S + RT
297
Nuttyens
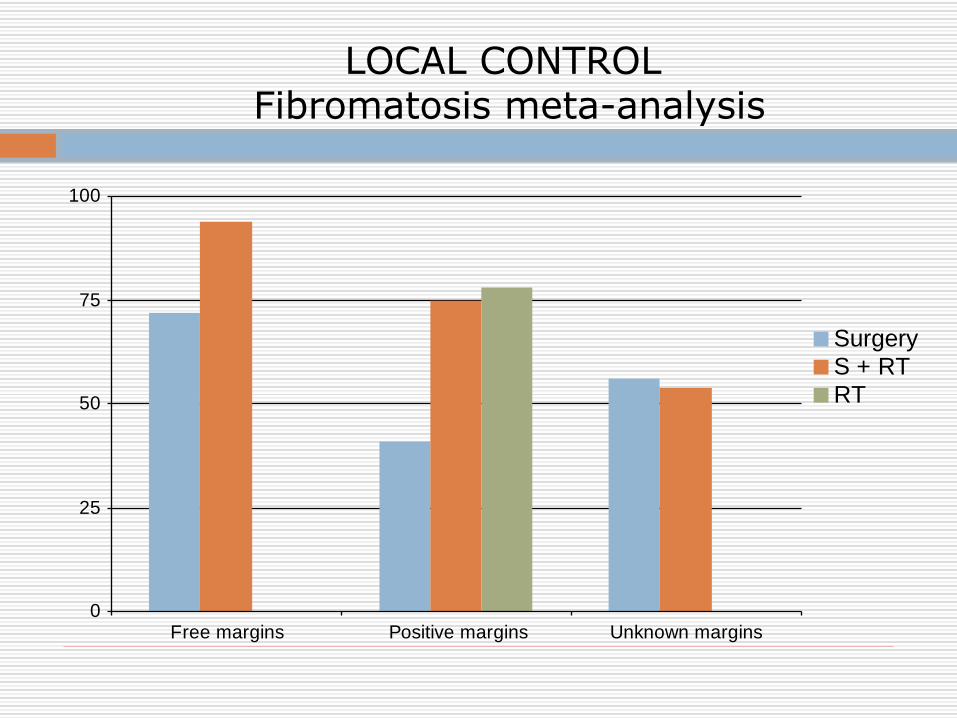
LOCAL CONTROL Fibromatosis meta-analysis
0
25
50
75
100
Free margins Positive margins Unknown margins
SurgeryS + RTRT

12
Effect of RT on local relapse
28% 59%
6% 25%
free margins +ve margins

Percentage Local control according Primary or Recurrent Fibromatosis
.0
22.5
45.0
67.5
90.0
Primary Recurrent Unknown
SurgerySurgery + RTRT aloneall having RT
% local control

Local control according to Primary/Recurrent and Margins
0
25
50
75
100
Free Primary Free Recurrence Positive primary Positive recurrence
SurgerySurgery +RT
% local control

15
Overall local control 70-80%
Whether primary or recurrent disease

Location and frequency of recurrences after radiotherapy
0
15
30
45
60
RT alone Surgery + RT Surgery + RT or RTalone
Total (%)
In fieldMarginalOut of field

Percentage of in field recurrences by dose
0
15
30
45
60
RT alone Surgery + RT Total
<50Gy50-59Gy>60Gy

18
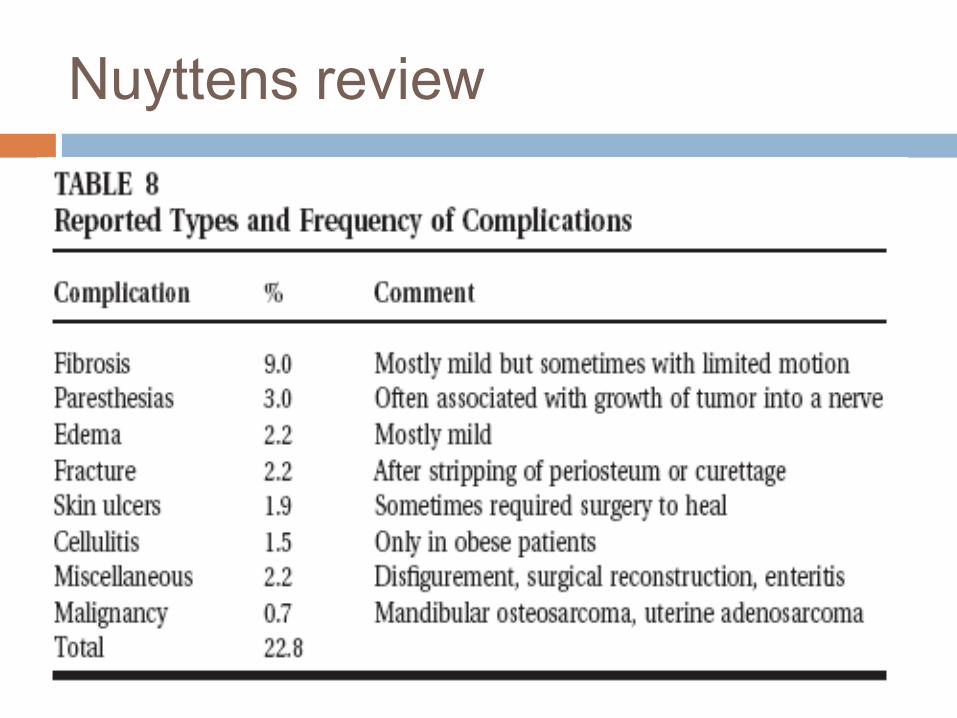
Nuyttens review

Zelefsky 1991 – role of brachytherapy in 38 patients with desmoid tumours.
Previous recurrence 75%Size >8cm 50%Gross residual disease post-op
16%
Marginal resection 79%

Zelefsky 1991 - results
Overall local control 66%
In-field local control rate 75%
Recurrence at periphery implant 4/12
Recurrence >3cm from treated volume 4/12
Local control at 5 years after salvage including 2 amputations
95%

Radiotherapy research
EORTC - Phase II study of moderate dose radiotherapy for inoperable aggressive fibromatosis. 56 Gy in 28 fractions 2 Gy per fraction 5
fractions per week Local control, defined as absence of local
progression 3 years after registration Proposed trial of adjuvant radiotherapy
following surgery for same circa 2003. IGRT sarcoma.

EORTC aggressive fibromatosis accrual

24

25

Hong 2004

3d-CRT v IMRT Hong 2004

28
29

NCI patient information for treatment of Paediatric desmoid
Treatment of desmoid tumour will be surgery whenever possible.
If surgery to completely remove the tumour is not possible, treatment may include the following:
External Radiation therapy to shrink the tumour before surgery.
Internal radiation therapy to kill any remaining tumour cells after surgery.
A non steroidal anti-inflammatory drug (NSAID). Antiestrogen therapy. Chemotherapy.
Watchful waiting. A clinical trial of targeted drug therapy with
imatinib (Gleevec).

31

32
Conclusions
Individualised treatment plan to balance risks of disease and surgery/radiotherapy.
Often fail locally despite clear surgical margin.
Gross local disease may remain quiescent.

33
Conclusions
Consider conservative therapy or observation for lesions which have not already recurred or behaved aggressively.
Previous recurrence or multifocal presentation may predict worse prognosis.

34
Radiotherapy
Radiotherapy improves recurrence free survival particularly where positive surgical margins or previous recurrence.
May be first choice therapy where surgery would result in major functional deficit.
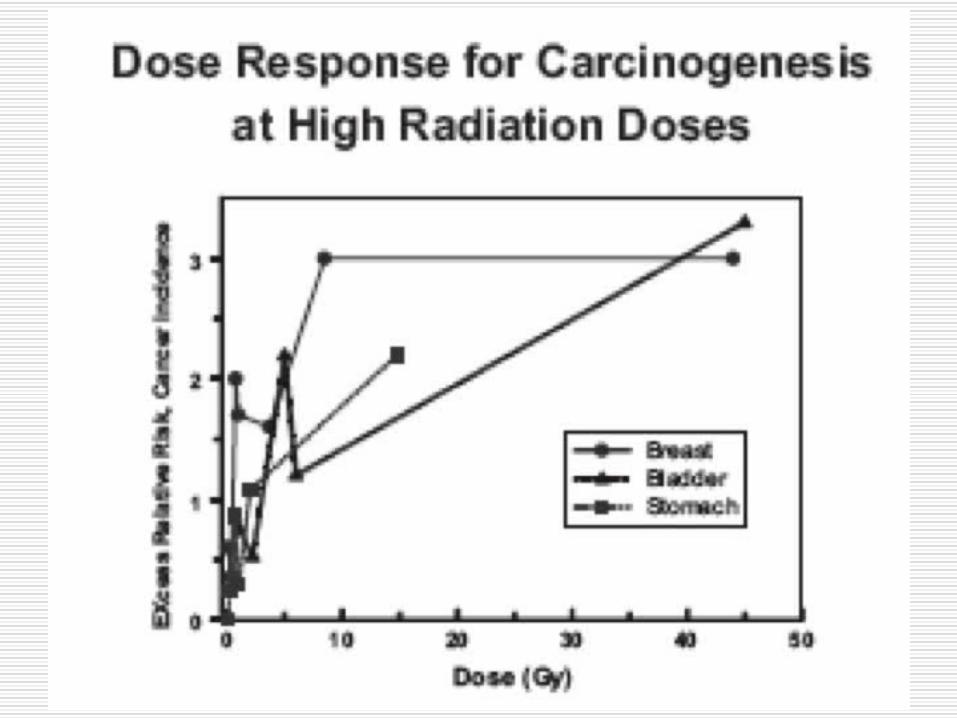
Need to use an adequate margin e.g 5-7cm. Indications to be balanced against significant risk of
inducing malignancy particularly in young.