Biliary - The Biliary Tract
67
The Biliary Tract Raymond W Pryor III M.D. July 31, 2008
-
Upload
cardiacinfo -
Category
Documents
-
view
3.847 -
download
11
description
Transcript of Biliary - The Biliary Tract
The Biliary TractRaymond W Pryor III M.D.
July 31, 2008

History

History
Circa 200 AD – Galen – the gallbladder as a subsidiary organ for the liver & responsible for yellow bile
Renaissance period – Gallbladder seat of many emotions (gall)
1652 - Thomas Bartholin – gallbladder part of bile tract from liver to intestine
1654 - Thomas Glisson – formed more detailed anatomy of liver & biliary tract
More relevant history
1420 - Antonio Benevieni – 1st account of gallstones
1687 - Stal Pert Von Der Wiel – 1st operation on gallstones
1733 – Jean-Louis Petit -1st successful removal of gallstones with fistula formation
1859 – J.L.W. Thudichum – Two stage cholecystostomy
July 15, 1867 – Dr John Stough Bobbs – Single stage cholecystostomy
Still More relevant History
1630 & 1667 – Zambecarri & Teckoff – proved the gall bladder not essential to life
1878 - Theodor Kocher – refined cholecystostomy procedure
July 15, 1882 – Dr Langenbuch – 1st open cholecystectomy
1886 – cholecystotomy 27% mortality vs 12% mortality for Langenbuch’s cholecystectomy – became gold standard
1940’s – Mirizzi introduced cholangiography for CBD stones
Into the Laparoscopic Age
Trocar insertion 1st described by Ezekiel and Celsus – 25 BC – AD 50
Term “Trocar” coined in 1706› “trocarter troise-quarts”
1901 Dimitri OH – gynaecologist, performed 1st endoscopic exam
1911 – Dr Bernheim published “Organoscopy” in Annals of Surgery
1938 Veress developed spring-loaded needle
Laparoscopic development
1952 – quartz rod to project light 1959 – closed circuit television 1966 – Kurt Semm – automatic insufflator device,
thermo coagulation, irrigation & aspiration system and endoloop applicator
1978 – Dr Hasson – direct placement of trochar 1982 – Liver biopsy via laparoscopy 1987 – Dr Mouret – 1st laparoscopic
cholecystectomy on human By 1989, procedure being done in US 1992 – NIH concluded Laparoscopic
cholecystectomy treatment of choice

Anatomy
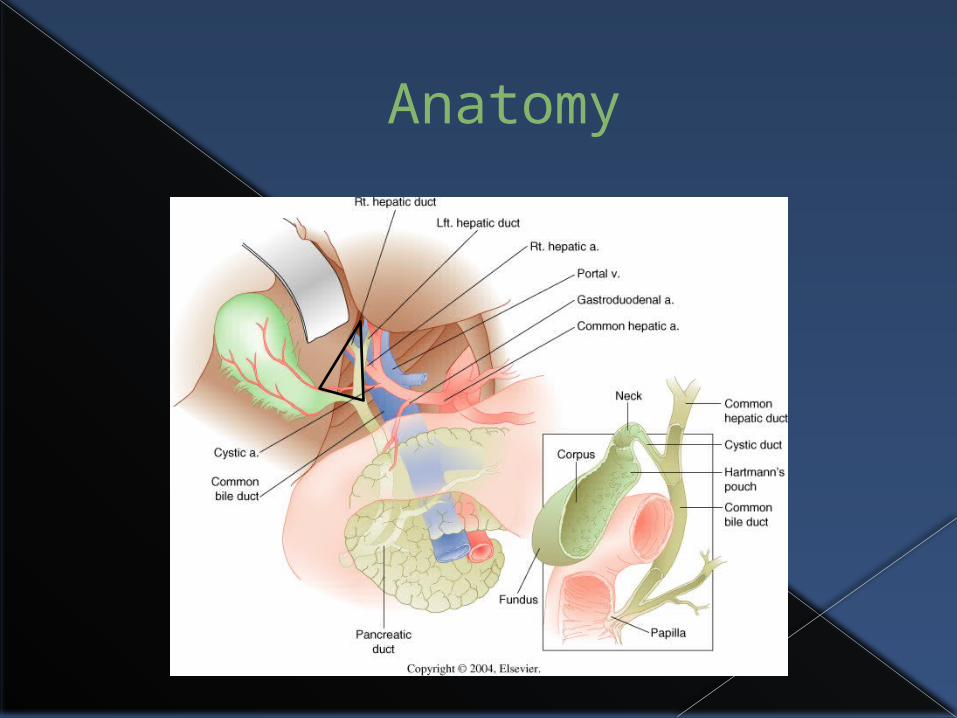
Anatomy
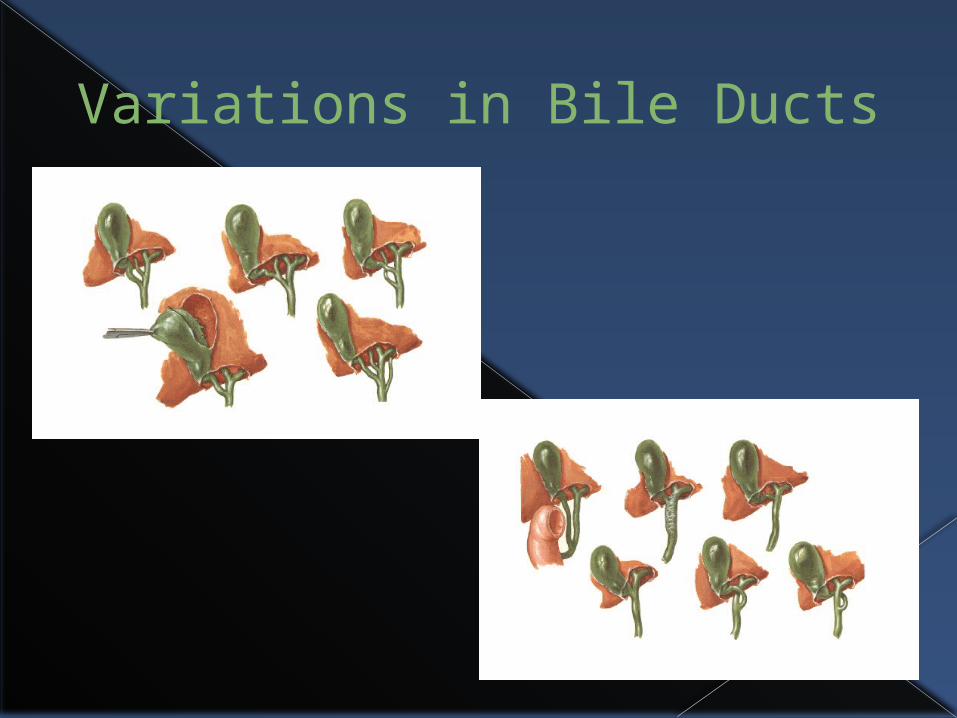
Variations in Bile Ducts
Biliary Physiology
Overall, the purpose is to modify, store and regulate the flow of bile
The gallbladder concentrates & stores bile, then releases bile in response to a meal
Biliary duct secretion of chloride-rich fluid controled by secretin, cholecystokinin (CCK) and gastrin.
Gallbladder physiology
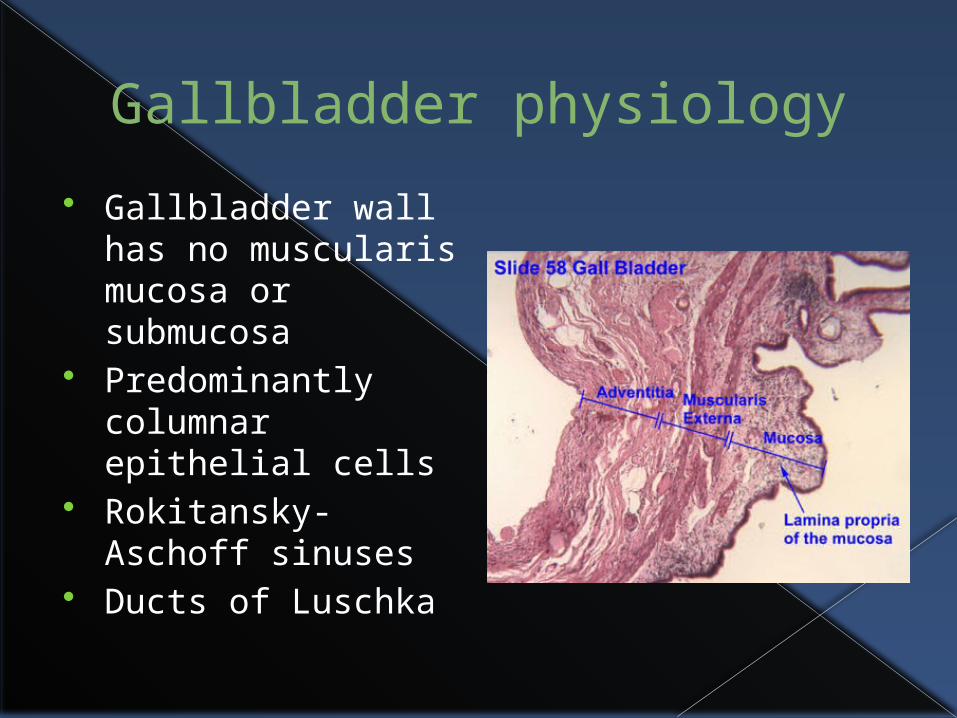
Gallbladder wall has no muscularis mucosa or submucosa
Predominantly columnar epithelial cells
Rokitansky-Aschoff sinuses
Ducts of Luschka
Gallbladder physiology
Normal capacity of 40-50 mL Liver secretes >600 mL of bile daily Gallbladder mucosa has greatest
absorptive capacity per unit area of any structure in body
Concentrates bile 5-10 fold NaCl transport by epithelium is driving
force and water passively absorbed
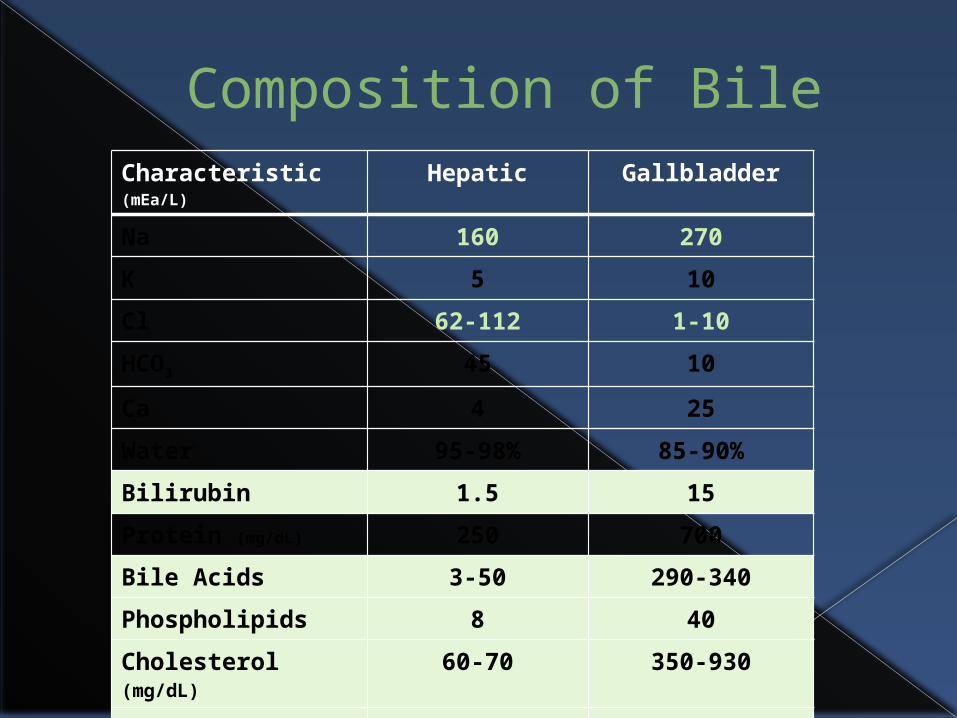
Composition of BileCharacteristic (mEa/L)
Hepatic Gallbladder
Na 160 270
K 5 10
Cl 62-112 1-10
HCO3 45 10
Ca 4 25
Water 95-98% 85-90%
Bilirubin 1.5 15
Protein (mg/dL) 250 700
Bile Acids 3-50 290-340
Phospholipids 8 40
Cholesterol (mg/dL)
60-70 350-930
Total Solids -- 125
pH 7.0 - 7.8 6.0 - 7.2
Biliary Motility
Filling is facilitated by contraction of ampullary sphincter (Sphincter of Otti)
Goes through cycles of partial emptying of 10-15% of volume to mix & concentrate bile
After meal, sphincter of Oddi relaxes & CCK released—causing contraction of gallbladder
When stimulated, 50-70% of contents ejected over 30-40 minutes
Refills over next 60-90 minutes
Bacteriology
Under “normal” conditions, the biliary tract is sterile
Positive cultures found:› 11-30% symptomatic stones & chronic
cholecystitis› 46% of acute cholecystitis› 58% with gallstones & CBD stones without
cholangitis› 94% with gallstones, CBD stones and
cholangitis
Organisms Gram-negative aerobes most common
› E. coli› Klebsiella› Pseudomonas› Enterobacter
Gram-positive aerobes› Enterococcus› Streptococcus viridans
Anaerobes (~25%)› Bacteroides fragilis› Clostridium
Fungal› Candida sp.
Parasitic› Opisthorchis sp. (Thailand) (Liver fluke)› Clonorchis sp. (China)
Approximately 50% of positive cultures will have 2 or more different bacteria species present
Antibiotic Choice 2008 Sanford Guide
Cholecystitis (E. coli, Klebsiella, Enterococci)› meropenem (Merrem)› piperacillin/tazobactam (Zosyn)› cefepime (Maxipime)
cefazolin + ampicillin (Ancef + ampicillin) ciprofloxacin + metrodazole (Cipro + Flagyl)
Emphysematous Cholecystitis (Clostridium perfringens +/- E. coli)› meropenem (Merrem)› piperacillin/tazobactam (Zosyn)
ertapenem (Invanz) ticarcillin./clavulanate (Timentin)
Cholangitis› meropenem (Merrem)› cefepime (Maxipime)› piperacillin/tazobactam (Zosyn)› Tigecycline (Tygacil)
ampicillin/sulbactam (Unasyn) imipenem/cilstatin (Primaxin) cefoperazone (Cefobid)
Antibiotics (cont’d)
PO Treatment of cholecystitis or cholangitis› clindamycin (Cleocin)› ciprofloxacin + metronidazole (Cipro + Flagyl)› levofloxacin (Levoquin)› moxifloxacin (Avelox)
Opisthorchis sp. & Clonorchis sp. (Liver fluke)› praziquantel (Biltricide)› albendazole (Albenza) **poor response to
above organisms
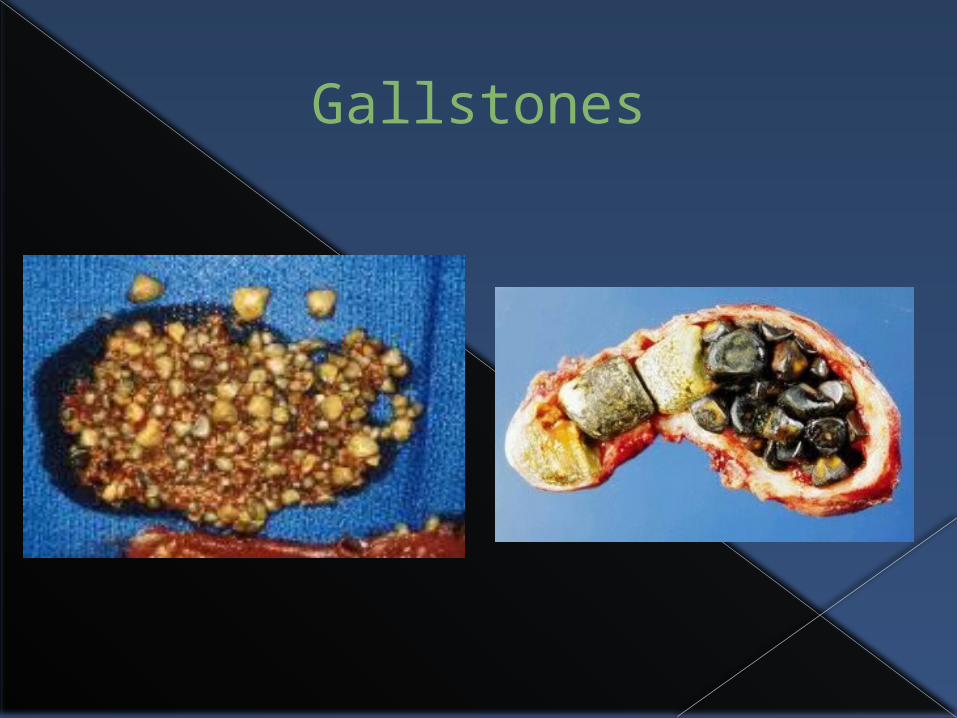
Gallstones
Cholelithiasis
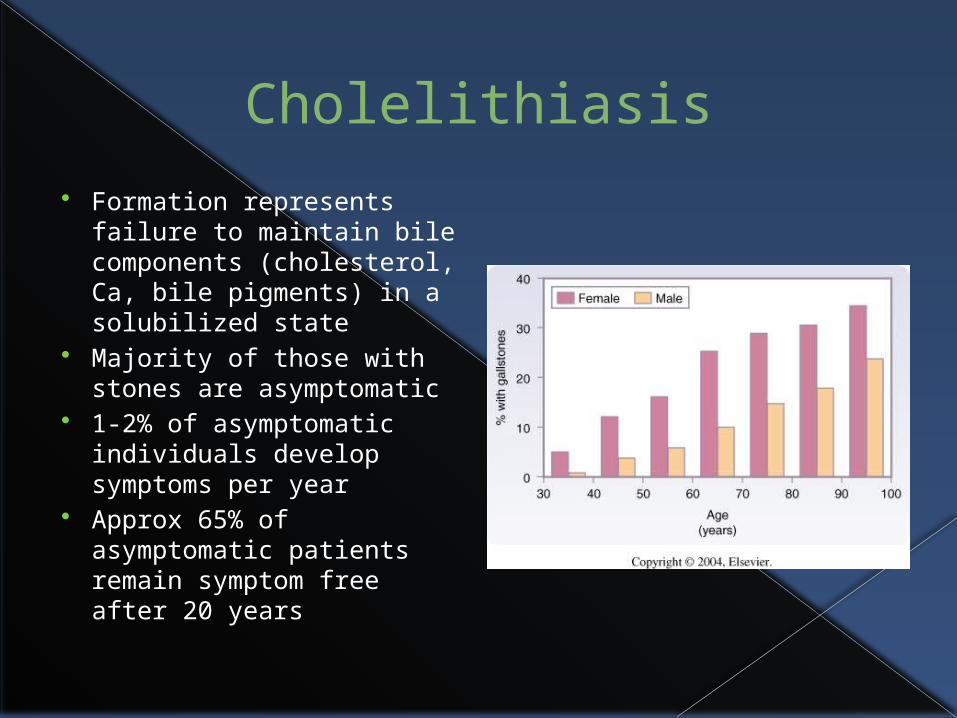
Formation represents failure to maintain bile components (cholesterol, Ca, bile pigments) in a solubilized state
Majority of those with stones are asymptomatic
1-2% of asymptomatic individuals develop symptoms per year
Approx 65% of asymptomatic patients remain symptom free after 20 years
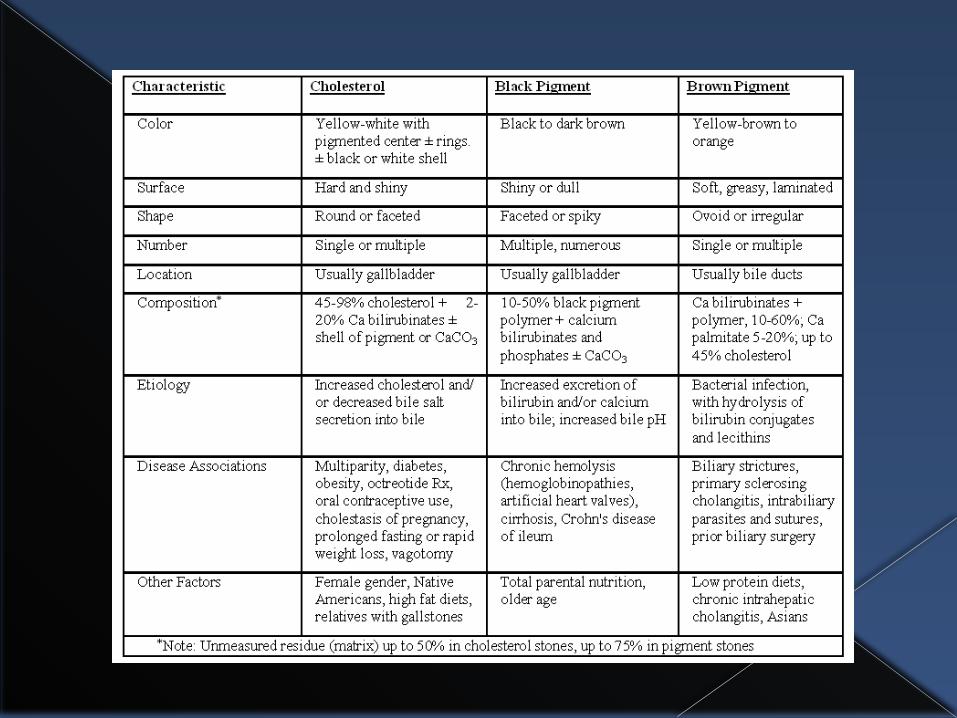
Cholesterol Gallstones
75% of all gallstones in United States
3 stages of formation› Cholesterol
supersaturation› Crystal nucleation› Stone growth
Risk factors› Female› Multi gravid› Estrogen use› Old age› Obesity› Rapid weight loss› Prolonged TPN
Pigment gallstones
25% of stones in US, 65% in Japan Black Pigment
› Made of Ca bilirubinate, bilirubin polymers & bile acids› Increased concentration of bilirubin & Ca › Hemolytic disorders & cirrhosis› Chronic TPN› Ileal resections› Exact mechanism unclear, may be due to presence of
bacterial b-glucuronidase that deconjugates bilirubin Brown Pigment
› Asian populations› Infection & bacterial hydrolysis of bilirubin› More commonly found in bile ducts
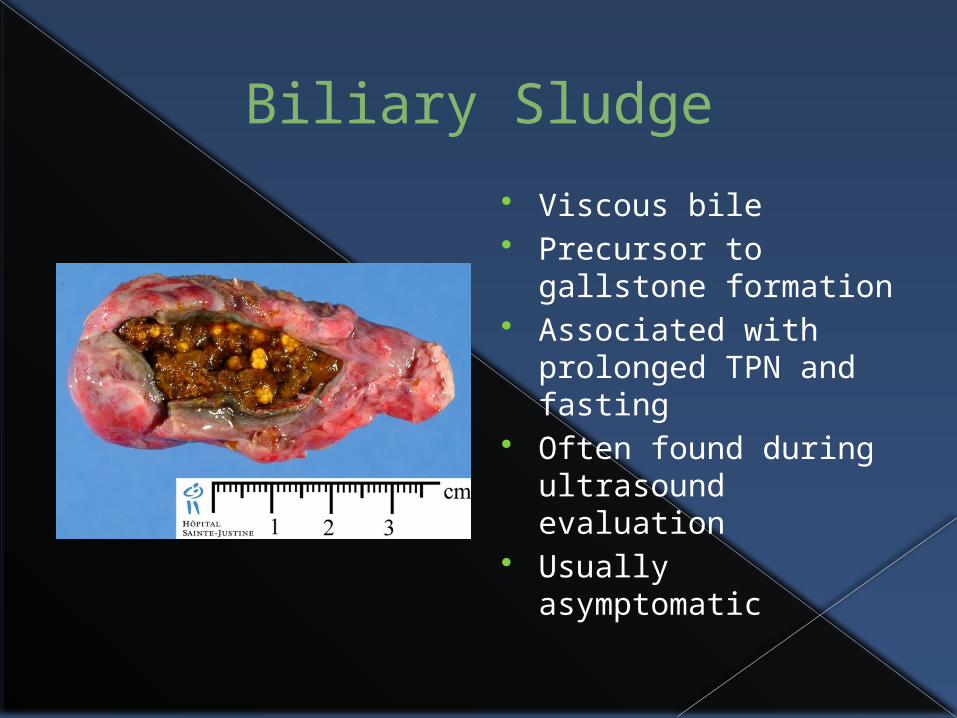
Biliary Sludge
Viscous bile Precursor to
gallstone formation Associated with
prolonged TPN and fasting
Often found during ultrasound evaluation
Usually asymptomatic
Is Everyone Still Awake?
Diagnosis of cholelithiasis Abdominal plain film
› rarely useful as 10-15% of stones radiopaque enough to be seen Ultrasound
› Non-invasive and cost-effective› 95-98% sensitive, 98% specific for documenting presence of gallstones› 80-95% sensitive, 78-80% specific for cholecystitis› Operator dependant
Radionuclide scan – hepatobiliary iminodiacetic acid (HIDA)› Good for detecting cystic duct obstruction or CBD obstruction› Also very useful in determining bile leaks after cholecystectomy› Acute cholecystitis: 94% sensitive, 65-85% specific› Chronic cholecystitis: 65% sensitive, 6-10% specific› Overall false positive (no filling of cystic duct or gallbladder) 15-20%
This is lowered with administration of morphine to 2-5% CT scan
› Less sensitive than ultrasound for detecting stones (50-70%) or cholecystitis.› More expensive
MRCP› Cost prohibitive› Most often used to detect common bile duct obstruction
Ultrasound
More images
CT Scan

MRCP
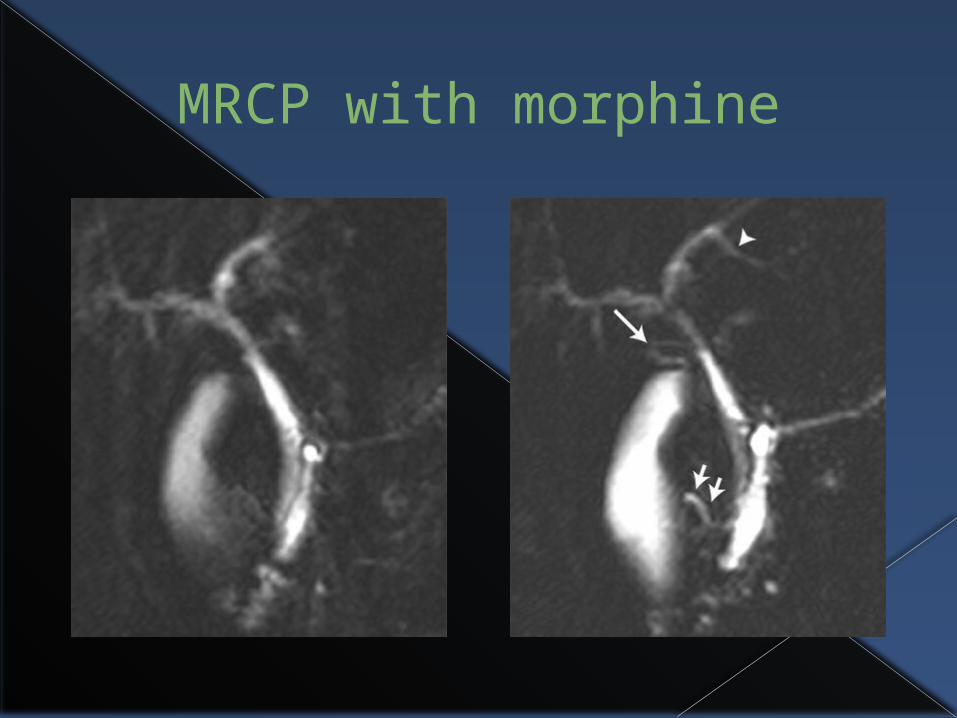
MRCP with morphine

Chronic Calculous Cholecystitis
Recurrent cystic duct obstruction & inflammation Presents with biliary colic Association with meals present in only 50% Symptoms
› Pain duration 1-5 hours (rare >24 hrs or <1 hr)› Nausea & vomiting present 60-70% of time› Bloating & belching in 50%› Fever & jaundice rare
Exam may be normal unless during attack Laboratory values usually normal Differentials include: GERD, PUD, IBS, pancreatitis Treatment is elective laparoscopic cholecystectomy
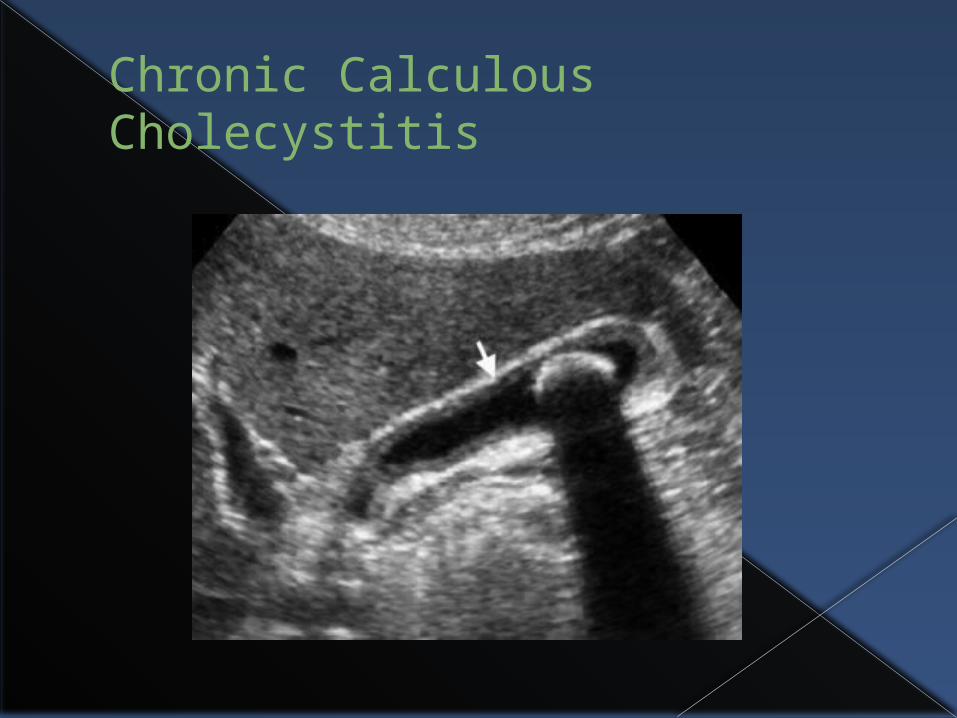
Chronic Calculous Cholecystitis
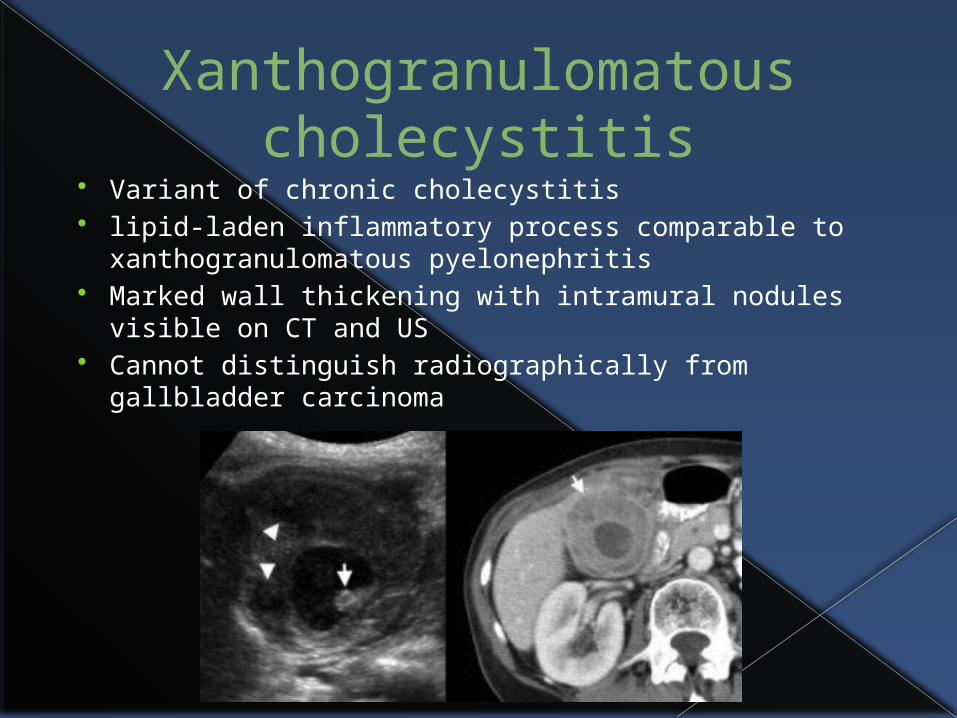
Xanthogranulomatous cholecystitis
Variant of chronic cholecystitis lipid-laden inflammatory process comparable to
xanthogranulomatous pyelonephritis Marked wall thickening with intramural nodules
visible on CT and US Cannot distinguish radiographically from gallbladder
carcinoma
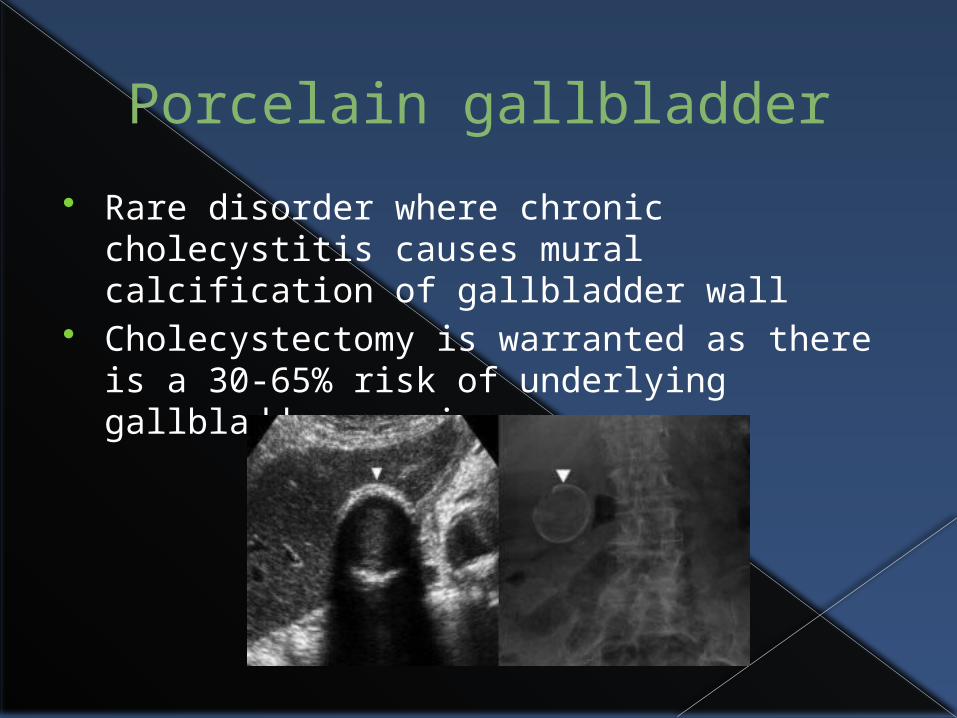
Porcelain gallbladder
Rare disorder where chronic cholecystitis causes mural calcification of gallbladder wall
Cholecystectomy is warranted as there is a 30-65% risk of underlying gallbladder carcinoma
Acute Calculous Cholecystitis Related to gallstones 90-95% of cases
› Non-resolving obstruction of cystic duct usually triggering event Can lead to ischemia and necrosis of gallbladder wall in 5-18% 46% will have positive bile cultures 75% will have had previous, less severe, attack of biliary colic Symptoms:
› RUQ pain lasting hours to days› Pain usually unremitting› Nausea, vomiting, anorexia & fevers common› Positive Murphy’s sign› Elevated alkaline phosphatase & WBC
Management:› NPO and IV fluids› Pain control (avoid narcotics if possible)› Antibiotics
Treatment is Laparoscopic cholecystectomy› Delayed vs immediate
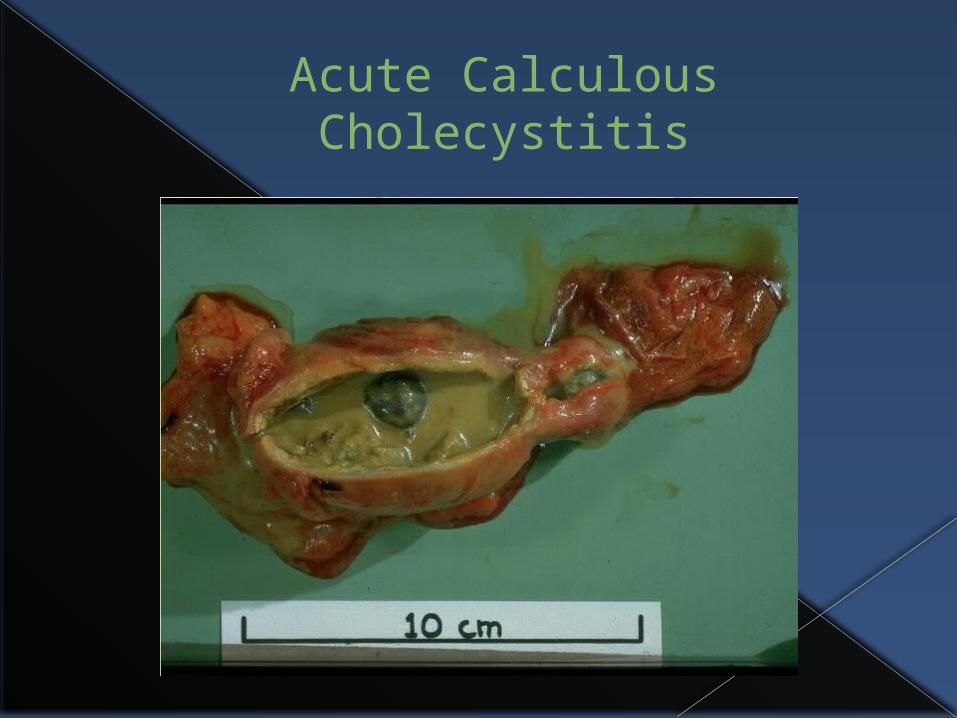
Acute Calculous Cholecystitis
Acute Acalculous Cholecystitis
5-10% of all patients with acute cholecystitis occur in absence of stones Frequently progresses to gangrene, empyema or
perforation Common following trauma, burns, long-term TPN, AAA
repair or cardiac bypass Exact etiology unclear, but may be related to ischemia
& stasis Symptoms similar to Acute Calculous cholecystitis HIDA scan has 40% false positive rate Emergency cholecystectomy or percutaneous
cholecystostomy is treatment of choice Mortality as high as 40% in some studies, due to
concomitant illnesses
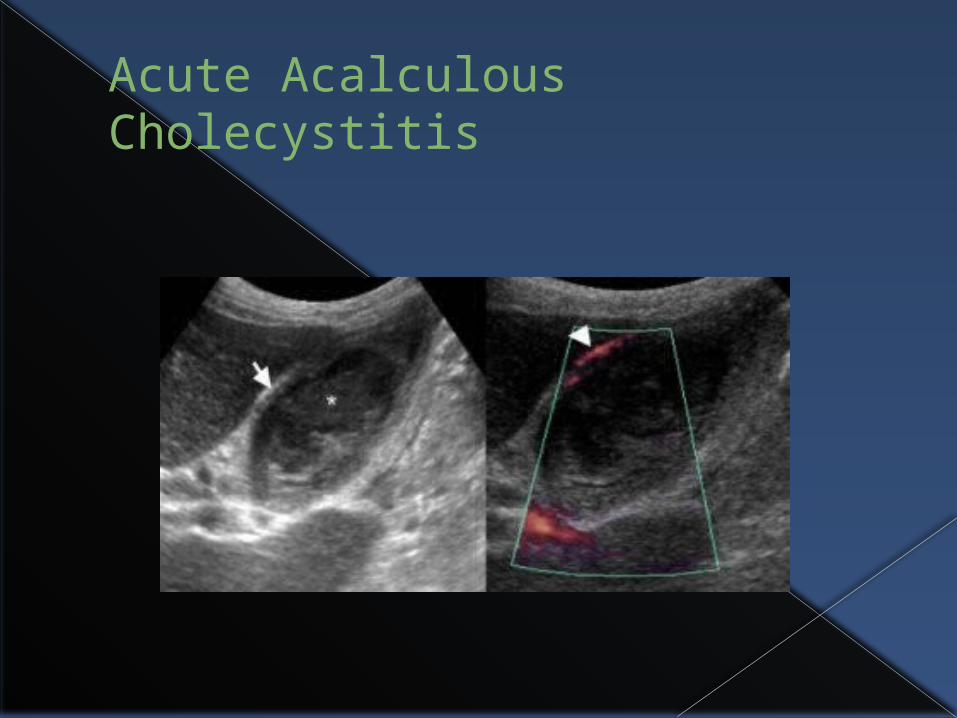
Acute Acalculous Cholecystitis
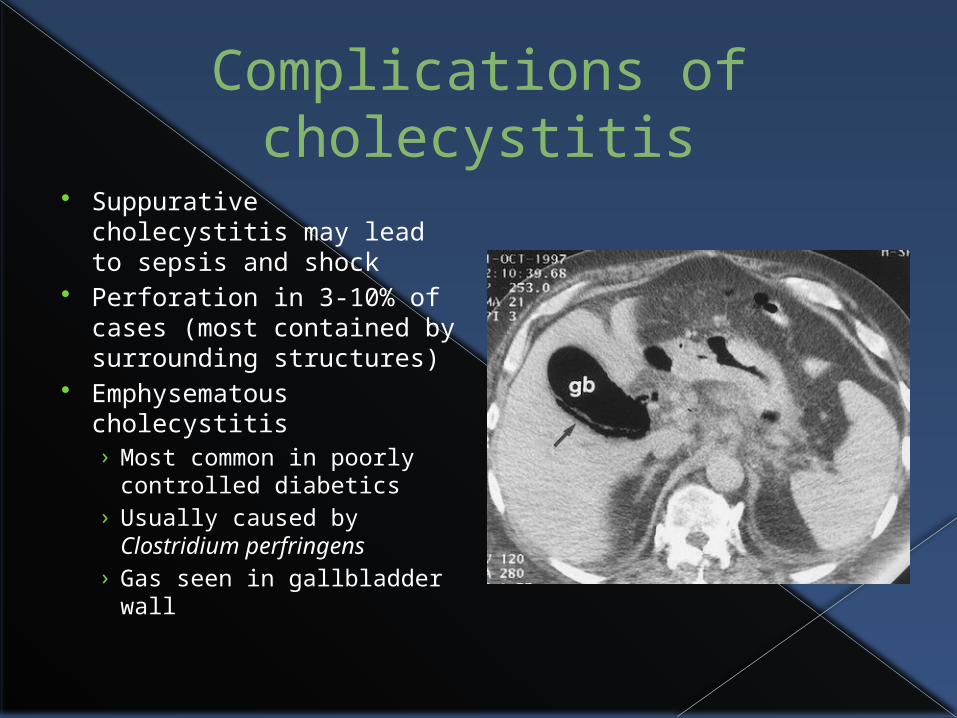
Complications of cholecystitis
Suppurative cholecystitis may lead to sepsis and shock
Perforation in 3-10% of cases (most contained by surrounding structures)
Emphysematous cholecystitis› Most common in poorly
controlled diabetics› Usually caused by
Clostridium perfringens› Gas seen in gallbladder
wall
Gallstone Ileus
Large gallstone the obstructs small bowel (distal ileum at ileocecal valve)
Fistula between gallbladder and duodenum (can be colon or stomach)
Most commonly in elderly (>70) females History of gallstone-related symptoms present in only 50% Only account for <1% of SBO cases <0.1% of those with gallstones will develop Up to 25% of SBO in elderly patients who have not had
previous abdominal surgery or have a hernia Treat with Ex-lap and enterotomy with removal of stone. Take
back for takedown of biliary-enteric fistula & cholecystectomy when more stable
On the ABSITE every year!!!
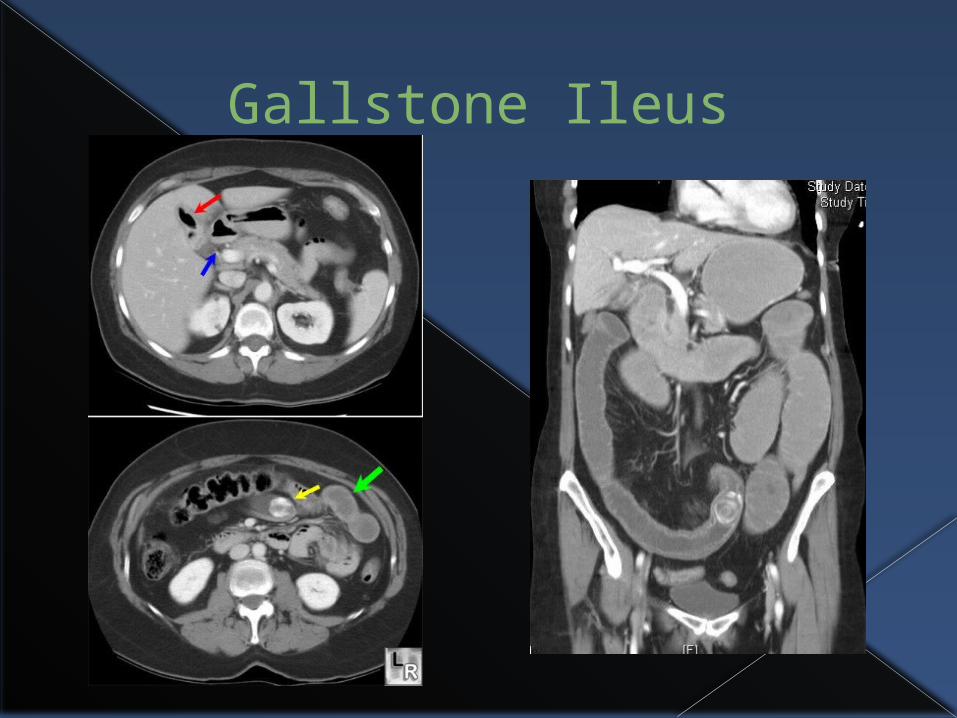
Gallstone Ileus
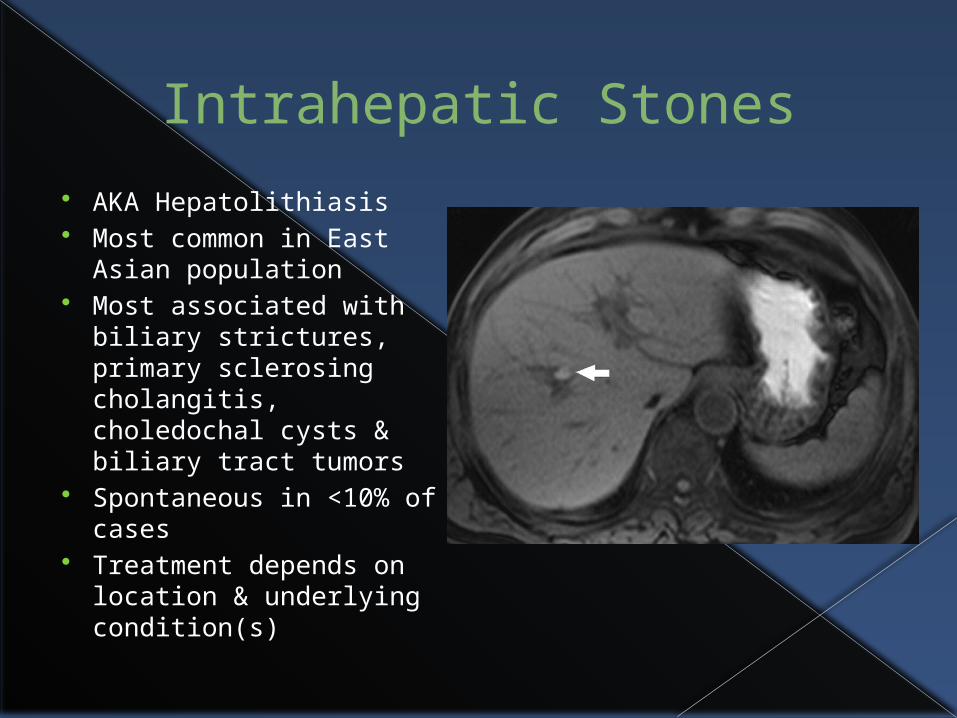
Intrahepatic Stones
AKA Hepatolithiasis Most common in East
Asian population Most associated with
biliary strictures, primary sclerosing cholangitis, choledochal cysts & biliary tract tumors
Spontaneous in <10% of cases
Treatment depends on location & underlying condition(s)
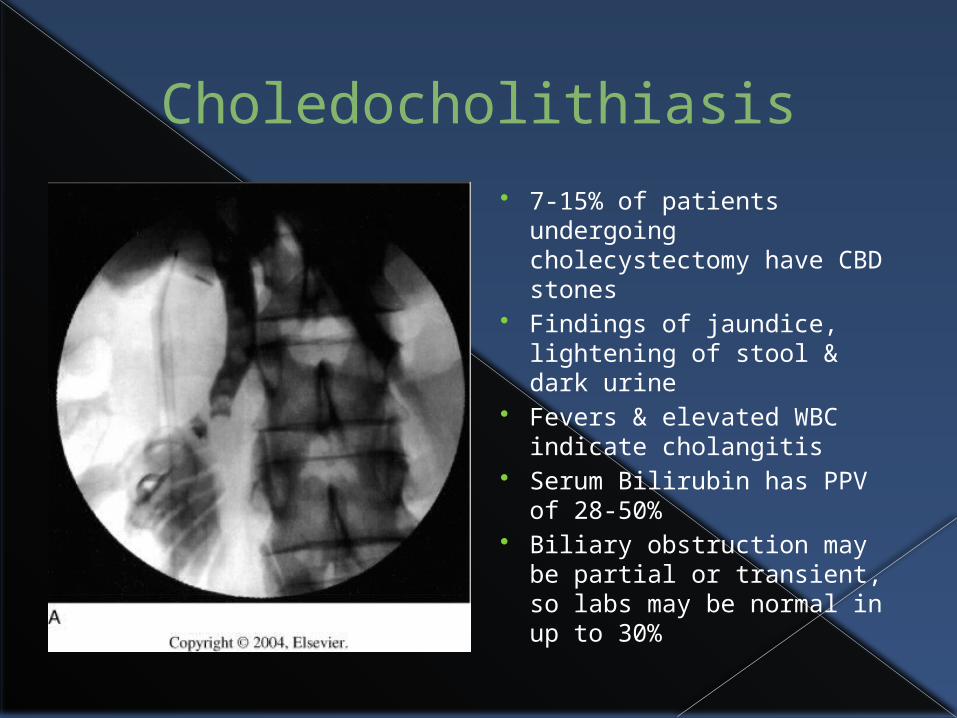
Choledocholithiasis
7-15% of patients undergoing cholecystectomy have CBD stones
Findings of jaundice, lightening of stool & dark urine
Fevers & elevated WBC indicate cholangitis
Serum Bilirubin has PPV of 28-50%
Biliary obstruction may be partial or transient, so labs may be normal in up to 30%
Choledocholithiasis (cont’d)
May have overlying pancreatitis (up to 45% of all cases of pancreatitis)
Dilated CBD in 58% of patients Ultrasound only 60-70% sensitive for CBD stones MRCP 95% sensitive & 89% specific ERCP Gold Standard
› Can both diagnose and treat 90% of time› Pancreatitis occurs in up to 5% of Patients
If unable to remove stone with ERCP (or none available) need to do laparoscopic or open CBD exploration
Stone found in CBD within 2 years of cholecystectomy is termed retained, >2 years is recurrent
Cholangitis
Acute bacterial infection of biliary tract Most common cause of biliary obstruction as often associated with
choledocholithiasis Occurs in 4-7% of ERCP and PTC (Percutaneous transhepatic
cholangiography) Other causes of obstruction associated with cholangitis:
› Strictures, neoplasms (rare), chronic pancreatitis, congenital cysts, duodenal diverticula
Presentation of fever, RUQ pain, jaundice › Charcot’s triad
May also have Hypotension & mental status change› Reynold’s pentad
Lab findings: Leukocytosis, elevated alk phos, AST, ALT, Bilirubin (direct)
Blood cultures positive 40-50% CT scan or Ultrasound can help make diagnosis
Treatment of Cholangitis
Immediate IV antibiotics and fluid resuscitation
If no response within 24 hours (15%), or in those with toxic cholangitis, emergency biliary decompression necessary› Endoscopic or percutaneous› May need open CBD exploration & T-tube
placement (higher mortality) Overall mortality 2% (5% with toxic
cholangitis) On ABSITE every year
Primary Sclerosing Cholangitis
Choleststic liver disease characterized by fibrotic strictures in the intrahepatic and extrahepatic biliary tree in ABSENCE of any known cause.
Associated with HLA B8/DR3, IDDM, Graves’ Disease, Sjögren’s syndrome, & Myasthenia gravis
Clinical presentation highly variable› Jaundice, pruritus, fatigue, abnormal LFT’s
Mean age 40-45 years Male : female 3:1 Diagnosis by ERCP Median survival after diagnosis 10-12 years Primary treatment is liver transplantation
Sclerosing cholangitis
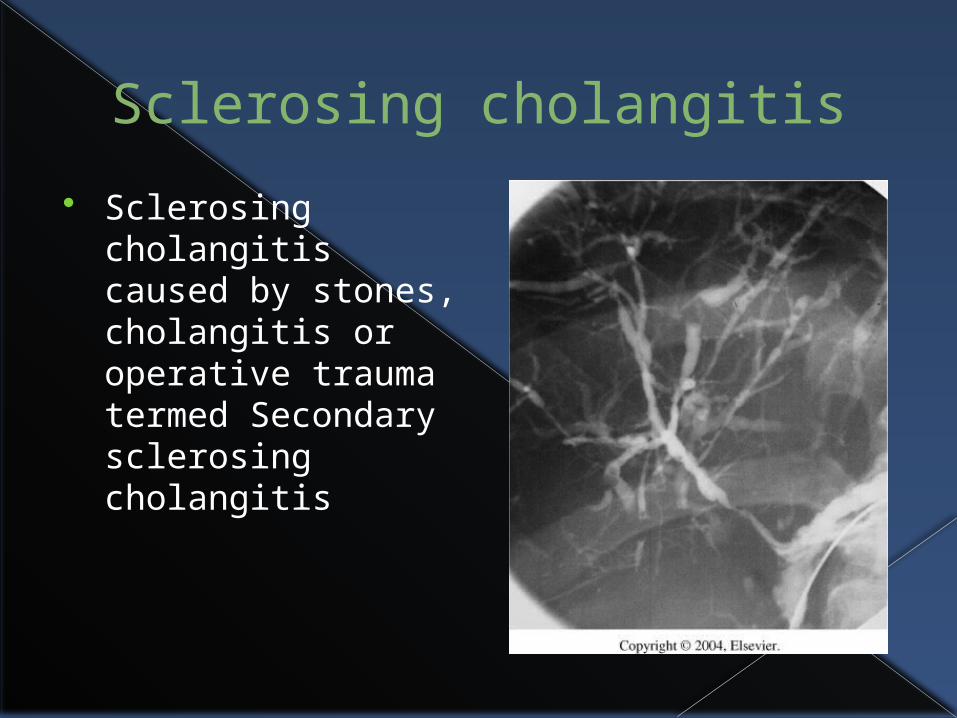
Sclerosing cholangitis caused by stones, cholangitis or operative trauma termed Secondary sclerosing cholangitis
Choledochal cysts
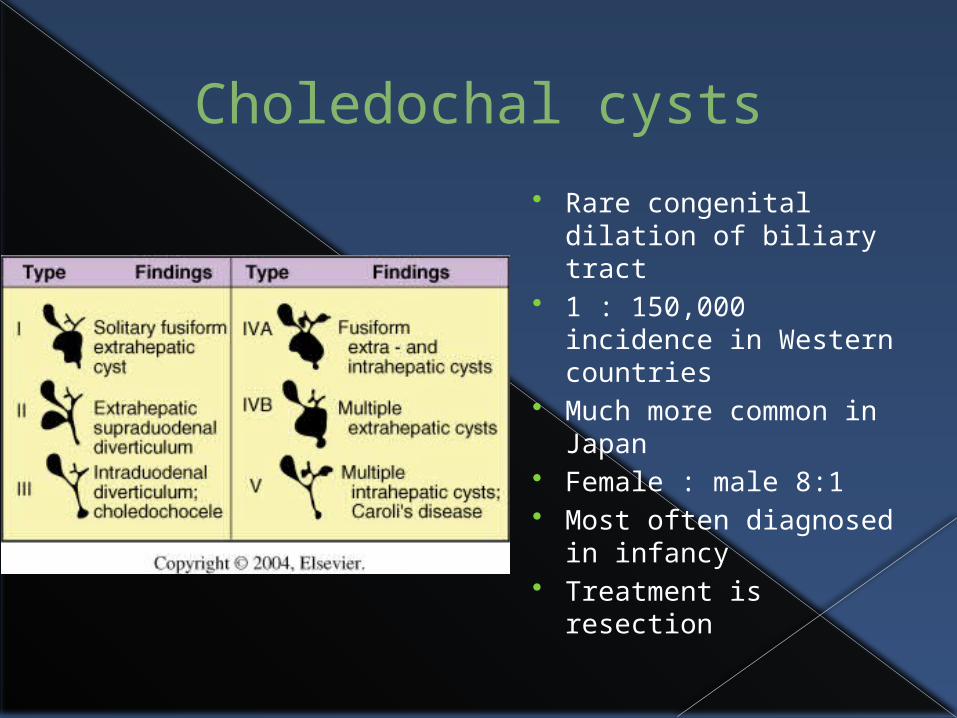
Rare congenital dilation of biliary tract
1 : 150,000 incidence in Western countries
Much more common in Japan
Female : male 8:1 Most often diagnosed
in infancy Treatment is
resection

Biliary Strictures & Bile duct injury 80-90% caused by iatrogenic
injuries Laparoscopic cholecystectomy
most common Present days to weeks after
surgery May be years after surgery as
scar tissue obstructs duct Treatment is decompression,
drainage, possible surgical resection.
Stenting being used with increasing frequency
With ligation of CBD & strictures, need Roux-en-Y hepaticojejunostomy
Gallbladder Cancer
5th most common GI tract malignancy 2-3 times more common in females 75% over age 65 5,000 new cases in US annualy Found incidentally in 1% to 3% of
cholecystectomy specimens Majority of the time, diagnosed in late stages
with distant mets Cholelithiasis present in 75-90% of cases
› Only 0.4% of those with gallstones develop cancer
Gallbladder Cancer Over 90% are adenocarcinoma
› 60% scirrhous, 25% papillary, 15% mucoid Squamous cell, oat cell, undifferentiated,
adenosquamous & carcinoid tumors less common Only 10% are correctly diagnosed preoperatively 1-3 out of every 100 cholecystectomy
specimens will show carcinoma at pathology At diagnosis:
› 25% contained to gallbladder wall› 35% metastases to regional lymph nodes› 40% have metastasized to distant sites
Average survival is 6 months after diagnosis
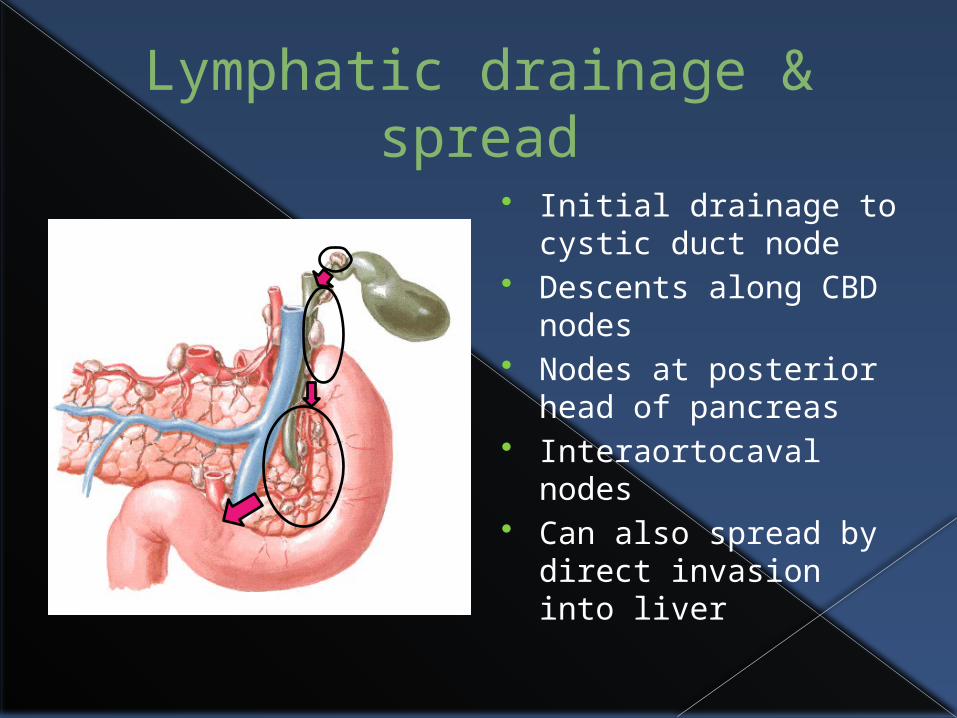
Lymphatic drainage & spread
Initial drainage to cystic duct node
Descents along CBD nodes
Nodes at posterior head of pancreas
Interaortocaval nodes
Can also spread by direct invasion into liver
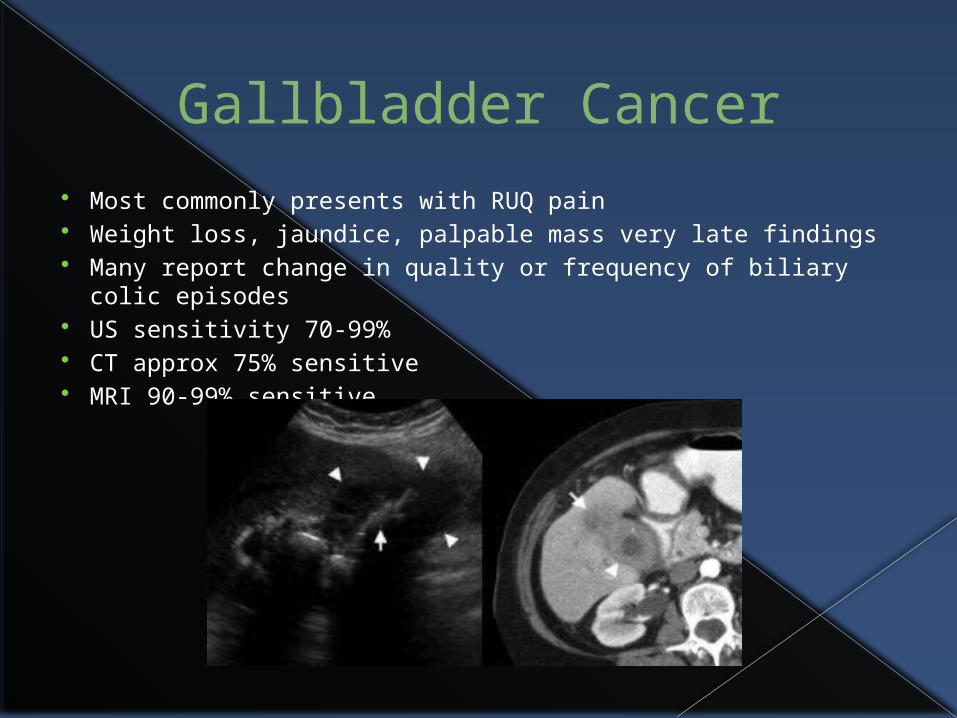
Gallbladder Cancer Most commonly presents with RUQ pain Weight loss, jaundice, palpable mass very late findings Many report change in quality or frequency of biliary colic
episodes US sensitivity 70-99% CT approx 75% sensitive MRI 90-99% sensitive

Management & Prognosis Tumor confined to mucosa or
submucosa (T1a) or to muscularis (T1b) have overall 5-year survival of 100% & 85%
Spillage of bile during cholecystectomy can seed abdomen
Invasion beyond muscularis (T2 & T3) need extended cholecystectomy with lymph node dissection
Stage III has ~15% 5-year survival
Stage IV has median survival of 1-3 months from diagnosis
Majority of cases, therapy is palliative
Chemo & radiation hot been shown to increase survival
Survival following radical resection of T2 gallbladder
cancer vs simple cholecystectomy
Cholangiocarcinoma
Uncommon tumor anywhere along intrahepatic or extrahepatic biliary tree
60-80% occur at bifurcation Most present with obstructive jaundice, hepatomegaly,
palpable gallbladder (Courvoisier’s sign) or cirrhosis (advanced disease)
2,500-3,000 new cases in US annualy Mean age in 50’s, men & women equal Increased risk with choledochal cysts, intrahepatic
stones, Liver flukes, dietary nitrosamines & exposure to dioxin
Following biliary-enteric anastomosis, 5% will develop Tend to spread by direct extension
Staging & classification
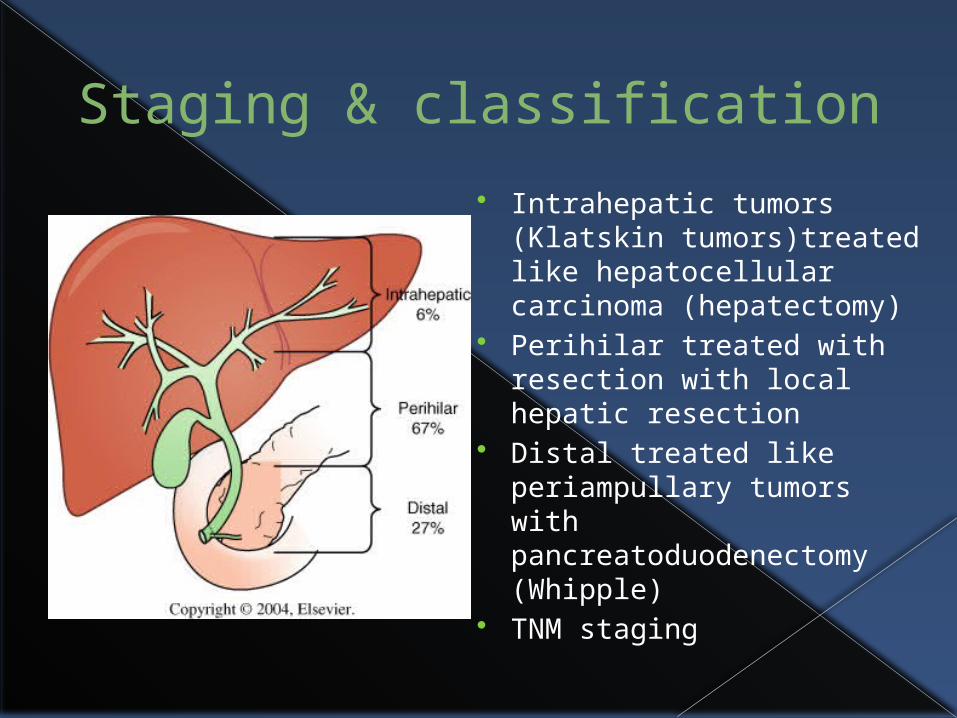
Intrahepatic tumors (Klatskin tumors)treated like hepatocellular carcinoma (hepatectomy)
Perihilar treated with resection with local hepatic resection
Distal treated like periampullary tumors with pancreatoduodenectomy (Whipple)
TNM staging
Diagnosis
Intrahepatic easily visualized on CT scan
Perihilar & distal tumors difficult to visualize on US and CT
ERCP & MRCP have near equal sensitivity (85-95%)
Most patients have serum Bilirubin >10, elevated Alk Phos & CA 19-9
Treatment
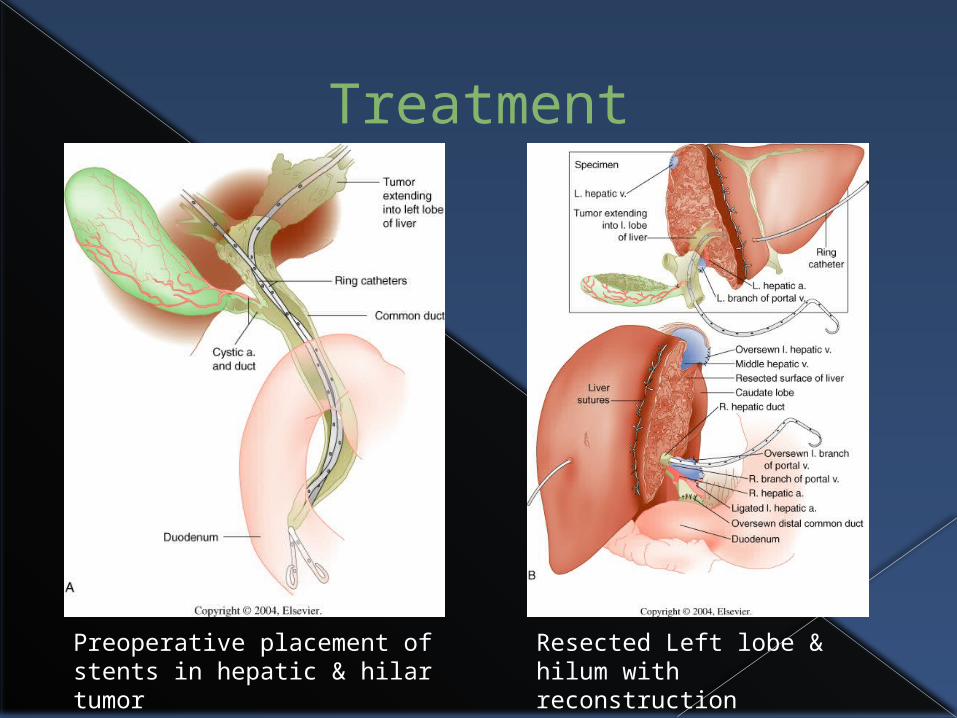
Preoperative placement of stents in hepatic & hilar tumor
Resected Left lobe & hilum with reconstruction

Prognosis
Long-term survival highly dependant on stage & treatment
For resectable intrahepatic tumors, overall 5-year 30-40%
Resectable peri-hilar tumors 10-20%
Resectable distal tumors 28-45%
Median survival for all unresectable tumors is 6-7 months
Miscellaneous Biliary Pathologies Biliary atresia
› Most common cause of persistent jaundice in newborn› Treat with hepatic portoenterostomy (Kasai procedure)
or transplantation Hemobilia
› Most cases in US due to trauma or iatrogenic injury› Diagnosis often requires arteriography› Treatment of persistent hemobilia includes
embolization or surgical ligation Benign polyps of gallbladder
› From cholesterol laden macrophages in mucosa Papilloma of bile duct
› Very rare, only ~90 cases in literature

Mirizzi Syndrome
Rare cause of biliary duct obstruction
Large stone contained within gallbladder compresses the CBD
Local spread of inflammation from gallbladder to CBD may also result in duct narrowing
The End