Focus on Disorders of the Biliary Tract (Relates to Chapter 44, “Nursing Management: Liver,...
85
Focus on Disorders of the Biliary Tract (Relates to Chapter 44, “Nursing (Relates to Chapter 44, “Nursing Management: Liver, Pancreas, and Biliary Management: Liver, Pancreas, and Biliary Tract Problems” in the textbook) Tract Problems” in the textbook) Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
-
Upload
primrose-wilson -
Category
Documents
-
view
223 -
download
2
Transcript of Focus on Disorders of the Biliary Tract (Relates to Chapter 44, “Nursing Management: Liver,...

Focus on Disorders of the Biliary Tract
(Relates to Chapter 44, “Nursing (Relates to Chapter 44, “Nursing Management: Liver, Pancreas, and Biliary Management: Liver, Pancreas, and Biliary
Tract Problems” in the textbook)Tract Problems” in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

2
Gallbladder Disease
•Cholelithiasis Cholelithiasis Most common disorder of Most common disorder of
biliary systembiliary system Stones in the gallbladderStones in the gallbladder
•CholecystitisCholecystitis Inflammation of the gallbladderInflammation of the gallbladder Usually associated with Usually associated with
cholelithiasischolelithiasis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

3
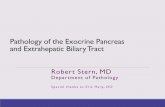
Gallbladder With Gallstones
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 44-16. Cholesterol gallstones in a gallbladder that was removed.

4
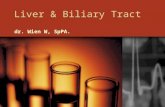
X-ray of Gallstones
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 44-17. X-ray of a gallbladder with gallstones.

5
Gallbladder Disease
•Common health problem in Common health problem in United StatesUnited States
• 8% to 10% of adults have 8% to 10% of adults have cholelithiasis.cholelithiasis.
• Incidence of cholelithiasis Incidence of cholelithiasis Higher in women, multiparous Higher in women, multiparous
women, and persons over 40 women, and persons over 40 yearsyears
Estrogen therapy ↑ riskEstrogen therapy ↑ riskCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

6
Gallbladder Disease
•Other risk factorsOther risk factors Sedentary lifestyleSedentary lifestyle Familial tendencyFamilial tendency ObesityObesity
•More common in whites than in More common in whites than in Asian and African AmericansAsian and African Americans
•↑ ↑ incidence in Navajo and Pimaincidence in Navajo and Pima
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

7
Etiology and Pathophysiology
•CholecystitisCholecystitis Most commonly associated Most commonly associated
with obstructionwith obstruction•Gallstones or biliary sludgeGallstones or biliary sludge
In absence of obstructionIn absence of obstruction•Occurs in older adults and Occurs in older adults and those who have trauma, those who have trauma, extensive burns, or recent extensive burns, or recent surgerysurgery
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

8
Etiology and Pathophysiology
•Cholecystitis causesCholecystitis causes BacteriaBacteria
•Escherichia coliEscherichia coli—Most common—Most common Other factors include Other factors include
•AdhesionsAdhesions•NeoplasmsNeoplasms•AnesthesiaAnesthesia•OpioidsOpioids
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

9
Etiology and Pathophysiology
•Cholecystitis (cont’d)Cholecystitis (cont’d) Inflammation Inflammation
•Major pathophysiologic conditionMajor pathophysiologic condition•Confined to mucous lining or Confined to mucous lining or entire wallentire wall
•Gallbladder is edematous and Gallbladder is edematous and hyperemic.hyperemic.
•May be distended with bile or pusMay be distended with bile or pus•Cystic duct may become occluded.Cystic duct may become occluded.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

10
Etiology and Pathophysiology
•CholelithiasisCholelithiasis Cause of gallstones unknownCause of gallstones unknown Develops when balance that Develops when balance that
keeps cholesterol, bile salts, keeps cholesterol, bile salts, and calcium in solution is and calcium in solution is alteredaltered•Causes include infection and Causes include infection and disturbances in metabolism of disturbances in metabolism of cholesterol.cholesterol.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

11
Etiology and Pathophysiology
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Bile in gallbladder is Bile in gallbladder is
supersaturated with supersaturated with cholesterol.cholesterol.
Precipitation of cholesterol Precipitation of cholesterol results.results.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

12
Etiology and Pathophysiology
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Other components of bile Other components of bile
that precipitate into stones that precipitate into stones includeinclude•Bile saltsBile salts•BilirubinBilirubin•CalciumCalcium•ProteinProtein
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

13
Etiology and Pathophysiology
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Stones that are primarily Stones that are primarily
cholesterol are the most cholesterol are the most common. common.
Immobility, pregnancy, and Immobility, pregnancy, and inflammatory or obstructive inflammatory or obstructive lesions of biliary system ↓ lesions of biliary system ↓ bile flow.bile flow.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

14
Etiology and Pathophysiology
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Stones may remain in Stones may remain in
gallbladder or may migrate to gallbladder or may migrate to cystic or common bile duct.cystic or common bile duct.
Cause pain as they pass Cause pain as they pass through ductsthrough ducts•May lodge in ducts and produce May lodge in ducts and produce an obstructionan obstruction
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

15
Etiology and Pathophysiology
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) If blockage occurs in cystic If blockage occurs in cystic
ductduct•Bile can continue to flow into Bile can continue to flow into the duodenum directly from the duodenum directly from liverliver
•When bile in gallbladder cannot When bile in gallbladder cannot escape stasis, may lead to escape stasis, may lead to cholecystitischolecystitis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

16
Clinical Manifestations
•Vary from Vary from Indigestion Indigestion Moderate to severe painModerate to severe pain FeverFever JaundiceJaundice
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

17
Clinical Manifestations
• Initial symptoms of acute Initial symptoms of acute cholecystitischolecystitis IndigestionIndigestion PainPain Tenderness in right upper Tenderness in right upper
quadrantquadrant
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

18
Clinical Manifestations
•Acute cholecystitisAcute cholecystitis Pain may be acute.Pain may be acute.
•May be accompanied by May be accompanied by nausea, vomiting, restlessness, nausea, vomiting, restlessness, and diaphoresisand diaphoresis
Inflammation manifestationsInflammation manifestations•LeukocytosisLeukocytosis•FeverFever
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

19
Clinical Manifestations
•Acute cholecystitis (cont’d) Acute cholecystitis (cont’d) Physical findingsPhysical findings
•Right upper quadrant Right upper quadrant tendernesstenderness
•Abdominal rigidityAbdominal rigidity
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

20
Clinical Manifestations
•Chronic cholecystitisChronic cholecystitis SymptomsSymptoms
•History of History of • Fat intoleranceFat intolerance•DyspepsiaDyspepsia•HeartburnHeartburn• FlatulenceFlatulence
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

21
Clinical Manifestations
•CholelithiasisCholelithiasis May produce severe May produce severe
symptoms or none at allsymptoms or none at all•““Silent cholelithiasis”Silent cholelithiasis”
Severity depends onSeverity depends on•Presence of obstructionPresence of obstruction•Whether or not stones moveWhether or not stones move
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

22
Clinical Manifestations
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Stones lodged in ducts or Stones lodged in ducts or
moving may cause spasm.moving may cause spasm.•Can produce severe painCan produce severe pain•Termed biliary colic, although Termed biliary colic, although more steady than colickymore steady than colicky
•Pain could be accompanied by Pain could be accompanied by tachycardia, diaphoresis, and tachycardia, diaphoresis, and prostration.prostration.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

23
Clinical Manifestations
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Pain may last an hour.Pain may last an hour.
•When it subsides, tenderness in When it subsides, tenderness in right upper quadrant develops.right upper quadrant develops.
Attacks of pain occur 3 to 6 Attacks of pain occur 3 to 6 hours after a heavy meal or hours after a heavy meal or after lying down.after lying down.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

24
Clinical Manifestations
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Total obstruction symptomsTotal obstruction symptoms
•JaundiceJaundice•Dark amber urineDark amber urine•Clay-colored stoolsClay-colored stools•PruritusPruritus
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

25
Clinical Manifestations
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Total obstruction symptoms Total obstruction symptoms
(cont’d) (cont’d) •Intolerance to fatty foodsIntolerance to fatty foods•Bleeding tendenciesBleeding tendencies•SteatorrheaSteatorrhea•No urobilinogen in urineNo urobilinogen in urine
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

26
Complications
•CholecystitisCholecystitis Gangrenous cholecysitisGangrenous cholecysitis Subphrenic abscessSubphrenic abscess PancreatitisPancreatitis CholangitisCholangitis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

27
Complications
•Cholecystitis (cont’d) Cholecystitis (cont’d) Biliary cirrhosisBiliary cirrhosis FistulaeFistulae Gallbladder ruptureGallbladder rupture
•Bile peritonitisBile peritonitis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

28
Complications
•Cholecystitis (cont’d)Cholecystitis (cont’d) Most common complications Most common complications
in older patients and those in older patients and those with diabeteswith diabetes•Gangrenous cholecystitisGangrenous cholecystitis•Bile peritonitis Bile peritonitis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

29
Complications
•Cholelithiasis Cholelithiasis CholangitisCholangitis Biliary cirrhosisBiliary cirrhosis CarcinomaCarcinoma PeritonitisPeritonitis CholedocholithiasisCholedocholithiasis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

30
Diagnostic Studies
•UltrasoundUltrasound• Laboratory testsLaboratory tests
Liver function studiesLiver function studies WBC countWBC count Serum bilirubinSerum bilirubin Serum amylaseSerum amylase
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

31
Diagnostic Studies
• ERCPERCP•Percutaneous transhepatic Percutaneous transhepatic
cholangiographycholangiography
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

32
Collaborative CareConservative Therapy
•CholecystitisCholecystitis Acute episode focus onAcute episode focus on
•Pain controlPain control•Antibiotic treatment Antibiotic treatment •Maintenance of fluid and Maintenance of fluid and electrolyte balanceelectrolyte balance
Treatment supportive and Treatment supportive and symptomaticsymptomatic
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

33
Collaborative CareConservative Therapy
•Cholecystitis (cont’d)Cholecystitis (cont’d) TreatmentTreatment
•Gastric decompressionGastric decompression• If nausea/vomiting is severeIf nausea/vomiting is severe
•AnticholinergicsAnticholinergics•↓ ↓ secretionsecretion•Counteract smooth muscle Counteract smooth muscle
spasmsspasms
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

34
Collaborative CareConservative Therapy
•Cholecystitis (cont’d)Cholecystitis (cont’d) Treatment (cont’d) Treatment (cont’d)
•NSAIDsNSAIDs•Pain managementPain management
•CholecystostomyCholecystostomy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

35
Collaborative CareConservative Therapy
•CholelithiasisCholelithiasis TreatmentTreatment
•Depends upon stage of diseaseDepends upon stage of disease•Bile acids are used to dissolve Bile acids are used to dissolve stones.stones.•Gallstones may occur.Gallstones may occur.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

36
Collaborative CareConservative Therapy
•CholelithiasisCholelithiasis TreatmentTreatment
•Two nonsurgical approaches for Two nonsurgical approaches for stone removalstone removal• ERCP with sphincterotomyERCP with sphincterotomy• Extracorporeal shock-wave Extracorporeal shock-wave
lithotripsy lithotripsy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

37
Collaborative CareConservative Therapy
•CholelithiasisCholelithiasis•ERCP with sphincterotomyERCP with sphincterotomy
• Effective in removing common bile Effective in removing common bile duct stonesduct stones
• Endoscope passed to duodenumEndoscope passed to duodenum•Sphincter of Oddi is widened. Sphincter of Oddi is widened. •Basket is used to retrieve stone.Basket is used to retrieve stone.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

38
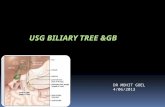
Endoscopic Sphincterotomy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 44-18. During endoscopic sphincterotomy, an endoscope is advanced through the mouth and stomach untilIts tip sits in the duodenum opposite the common bile duct. Inset, after widening the duct mouth by incising thesphincter muscle, the physician advances a basket attachment into the duct and snags the stone.

39
Collaborative CareConservative Therapy
•CholelithiasisCholelithiasis Extracorporeal shock-wave Extracorporeal shock-wave
lithotripsy lithotripsy •Used if stone is too large to Used if stone is too large to passpass
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

40
Collaborative CareSurgical Therapy
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Laparoscopic Laparoscopic
cholecystectomycholecystectomy•Treatment of choiceTreatment of choice•Removal of gallbladder through Removal of gallbladder through one to four puncture holesone to four puncture holes
•Minimal postoperative painMinimal postoperative pain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

41
Collaborative CareSurgical Therapy
•Cholelithiasis (cont’d) Cholelithiasis (cont’d) Laparoscopic Laparoscopic
cholecystectomy (cont’d) cholecystectomy (cont’d) •Discharge on day or next dayDischarge on day or next day•Injury to common bile duct is Injury to common bile duct is the main complication. the main complication.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 42

43
Collaborative CareSurgical Therapy
•Cholelithiasis (cont’d)Cholelithiasis (cont’d) Open cholecystectomy Open cholecystectomy
•Removal of gallbladder through Removal of gallbladder through right subcostal incisionright subcostal incision
•T-tube inserted into common T-tube inserted into common bile duct bile duct • Ensures patency of the duct Ensures patency of the duct •Allows excess bile to drain Allows excess bile to drain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

44
Placement of T-Tube
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 44-19. Placement of T tube. Dotted lines indicate parts removed.

45
Collaborative Care Transhepatic Biliary Catheter
•Used preoperatively inUsed preoperatively in Biliary obstructionBiliary obstruction Hepatic dysfunctionHepatic dysfunction
•Used when Used when Inoperable liver, pancreatic or Inoperable liver, pancreatic or
bile duct carcinoma obstructs bile duct carcinoma obstructs bile flowbile flow
Endoscopic drainage is Endoscopic drainage is unsuccessful.unsuccessful.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

46
Collaborative Care Transhepatic Biliary Catheter
• Inserted percutanously Inserted percutanously •Allows for decompression Allows for decompression
of obstructed extrahepatic of obstructed extrahepatic bile ductsbile ducts
•After insertion, catheter is After insertion, catheter is connected to drainage bag.connected to drainage bag.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

47
Collaborative Care Transhepatic Biliary Catheter
•Skin care Skin care Catheter insertion site Catheter insertion site
cleaned daily with antisepticcleaned daily with antiseptic Observe for bile leakage. Observe for bile leakage.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

48
Collaborative CareDrug Therapy
•Most commonMost common AnalgesicsAnalgesics
•MorphineMorphine•NSAIDsNSAIDs
AnticholinergicsAnticholinergics•AtropineAtropine
Fat-soluble vitamins (A, D, E, Fat-soluble vitamins (A, D, E, K)K)
Bile saltsBile saltsCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

49
Collaborative CareDrug Therapy
•Cholestyramine (Questran) Cholestyramine (Questran) may be given for pruritus.may be given for pruritus. Given in powdered form, Given in powdered form,
mixed with milk or juicemixed with milk or juice
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

50
Collaborative CareNutritional Therapy
•Diet modificationsDiet modifications MajorMajor
•Low saturated fat dietLow saturated fat diet•High in fiber and calciumHigh in fiber and calcium
Reduced calorie diet if obeseReduced calorie diet if obese Eat small, more frequent Eat small, more frequent
meals.meals.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

51
Collaborative CareNutritional Therapy
•Diet modifications (cont’d)Diet modifications (cont’d) After laparoscopic After laparoscopic
cholecystectomycholecystectomy•Liquids for dayLiquids for day•Light meals for several daysLight meals for several days
After incisional cholecystectomyAfter incisional cholecystectomy•Liquids to bland diet after return of Liquids to bland diet after return of bowel soundsbowel sounds
•May need to restrict fats for 4 to 6 May need to restrict fats for 4 to 6 weeksweeks
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

52
Nursing Management
•Nursing assessment Nursing assessment Subjective dataSubjective data
•Past medical historyPast medical history•Obesity, infection, cancer, Obesity, infection, cancer,
pregnancypregnancy•Medication useMedication use
• Estrogen, oral contraceptivesEstrogen, oral contraceptives•Surgical historySurgical history
•Previous abdominal surgeryPrevious abdominal surgery
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

53
Nursing ManagementNursing Assessment
•Subjective dataSubjective data Positive family historyPositive family history AnorexiaAnorexia Weight lossWeight loss IndigestionIndigestion Nausea and vomitingNausea and vomiting
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

54
Nursing ManagementNursing Assessment
•Subjective data (cont’d)Subjective data (cont’d) Fat intoleranceFat intolerance Clay-colored stoolsClay-colored stools Dark urineDark urine Pain in right upper quadrantPain in right upper quadrant PruritusPruritus
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

55
Nursing ManagementNursing Assessment
•Objective dataObjective data FeverFever RestlessnessRestlessness JaundiceJaundice TachypneaTachypnea
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

56
Nursing ManagementNursing Assessment
•Objective data (cont’d) Objective data (cont’d) TachycardiaTachycardia Abnormal liver enzymes Abnormal liver enzymes Abnormal gallbladder Abnormal gallbladder
ultrasoundultrasound
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

57
Nursing ManagementNursing Diagnoses
•Acute painAcute pain• Ineffective self-health Ineffective self-health
managementmanagement
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

58
Nursing ManagementPlanning
•Overall goalsOverall goals Relief of pain and discomfortRelief of pain and discomfort No complications No complications
postoperativelypostoperatively No recurrent attacks of No recurrent attacks of
cholecystitis or cholelithiasischolecystitis or cholelithiasis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

59
Nursing ManagementNursing Implementation
•Health promotionHealth promotion Recognize predisposing Recognize predisposing
factors in general health factors in general health screening.screening.•Disease more common in Disease more common in Native AmericansNative Americans
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

60
Nursing ManagementNursing Implementation
•Acute interventionAcute intervention Nursing objectivesNursing objectives
•Relieve painRelieve pain•Relieve nausea and vomitingRelieve nausea and vomiting•Provide comfort and emotional Provide comfort and emotional supportsupport
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

61
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) Nursing objectives (cont’d) Nursing objectives (cont’d)
•Maintaining fluid and Maintaining fluid and electrolyte balance and electrolyte balance and nutritionnutrition
•Making accurate assessmentsMaking accurate assessments•Observing for complicationsObserving for complications
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

62
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) Assess pain and administer Assess pain and administer
pain medications.pain medications. Provide clean bed, Provide clean bed,
comfortable positioning, and comfortable positioning, and oral care.oral care.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

63
Nursing ManagementNursing Implementation
•Acute intervention (cont’d) Acute intervention (cont’d) Nausea and vomitingNausea and vomiting
•May need gastric May need gastric decompression decompression
•Oral hygiene Oral hygiene •Care of naresCare of nares•Accurate intake and outputAccurate intake and output•Antiemetics Antiemetics
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

64
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) PruritusPruritus
•Relief measuresRelief measures•Baking soda or calamine lotionBaking soda or calamine lotion•Soft linenSoft linen•Control of temperatureControl of temperature•Shortening of nailsShortening of nails• Teaching patients to scratch with Teaching patients to scratch with
knuckles rather than nailsknuckles rather than nails
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

65
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) Observe for signs of Observe for signs of
obstruction.obstruction.•JaundiceJaundice•Clay-colored stoolsClay-colored stools•Dark, foamy urineDark, foamy urine•FeverFever•↑ ↑ WBCWBC•SteatorrheaSteatorrhea
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

66
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) Watch for bleeding.Watch for bleeding.
•Common sites—mucous Common sites—mucous membranesmembranes
•If presentIf present•Small-gauge needles with gentle Small-gauge needles with gentle
pressurepressure•Know patient’s prothrombin time.Know patient’s prothrombin time.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

67
Nursing ManagementNursing Implementation
•Acute intervention (cont’d)Acute intervention (cont’d) Assess for infection.Assess for infection.
•Temperature elevation with Temperature elevation with chills and jaundice may indicate chills and jaundice may indicate choledocholithiasis.choledocholithiasis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

68
Nursing ManagementNursing Implementation
•Postoperative carePostoperative care Laparoscopic cholecystectomyLaparoscopic cholecystectomy
•Monitoring for complicationsMonitoring for complications•Common problemCommon problem
•Shoulder pain from irritation of Shoulder pain from irritation of phrenic nerve and diaphragm due to phrenic nerve and diaphragm due to retained COretained CO22
•Place patient in Sims’ position.Place patient in Sims’ position.• Encourage deep breathing, Encourage deep breathing,
ambulation.ambulation.•Administer pain medications.Administer pain medications.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

69
Nursing ManagementNursing Implementation
•Postoperative care (cont’d) Postoperative care (cont’d) Incisional cholecystectomyIncisional cholecystectomy
•Maintain adequate ventilation.Maintain adequate ventilation.•Prevent respiratory Prevent respiratory complications. complications.
•Provide general postop nursing Provide general postop nursing care.care.
•If T-tube present,If T-tube present,•Maintain bile drainage.Maintain bile drainage.•Observe function and drainage.Observe function and drainage.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

70
Nursing ManagementNursing Implementation
•Ambulatory and home careAmbulatory and home care Dietary teachingDietary teaching Fat-soluble vitamin Fat-soluble vitamin
supplementssupplements Instructions to patient Instructions to patient
regarding observations regarding observations indicating obstructionindicating obstruction
Stress significance of continued Stress significance of continued health care.health care.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

71
Nursing ManagementNursing Implementation
•Ambulatory and home careAmbulatory and home care Laparoscopic cholecystectomyLaparoscopic cholecystectomy
•Home care instructionsHome care instructions•Teaching essentialTeaching essential
Open-incision cholecystectomyOpen-incision cholecystectomy•Discharged in 2 to 3 daysDischarged in 2 to 3 days•No heavy lifting for 4 to 6 weeksNo heavy lifting for 4 to 6 weeks
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

72
Nursing ManagementEvaluation
• Expected outcomesExpected outcomes Appear comfortable and Appear comfortable and
verbalize pain reliefverbalize pain relief Verbalize knowledge of Verbalize knowledge of
activity level and dietary activity level and dietary restrictionsrestrictions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

73
Gallbladder Cancer
•Primary cancer of gallbladder Primary cancer of gallbladder is uncommon.is uncommon.
•Majority are Majority are adenocarcinomas.adenocarcinomas.
•Relationship exists between Relationship exists between gallbladder cancer and gallbladder cancer and chronic cholecystitis and chronic cholecystitis and cholelithiasis.cholelithiasis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

74
Gallbladder Cancer
• Early symptomsEarly symptoms InsidiousInsidious Similar to those of Similar to those of
cholecystitis and cholecystitis and cholelithiasischolelithiasis
• Late symptomsLate symptoms Usually those of biliary Usually those of biliary
obstruction obstruction
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

75
Gallbladder Cancer
•Diagnosis and stagingDiagnosis and staging EUSEUS Transabdominal ultrasoundTransabdominal ultrasound CTCT MRIMRI MRCPMRCP
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

76
Gallbladder Cancer
•Usually not detected until Usually not detected until disease advanceddisease advanced
• If found early, can be If found early, can be curativecurative
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

77
Gallbladder Cancer
• Factors influencing Factors influencing successful surgical successful surgical outcomesoutcomes Depth of cancer invasionDepth of cancer invasion Extent of liver involvementExtent of liver involvement Presence of venous or Presence of venous or
lymphatic invasionlymphatic invasion Lymph node metastasis Lymph node metastasis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

78
Gallbladder Cancer
• If surgery is not an optionIf surgery is not an option Endoscopic stenting of biliary Endoscopic stenting of biliary
tree to reduce jaundice tree to reduce jaundice •Adjuvant therapiesAdjuvant therapies
Radiation therapyRadiation therapy ChemotherapyChemotherapy
•Poor prognosis overallPoor prognosis overall
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

79
Gallbladder Cancer
•Nursing managementNursing management Supportive careSupportive care
•NutritionNutrition•HydrationHydration•Skin careSkin care•Pain reliefPain relief
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

80
The surgical treatment of choice for the The surgical treatment of choice for the patient with symptomatic gallbladder patient with symptomatic gallbladder disease is a:disease is a:
1. Cholecystotomy.1. Cholecystotomy.2. Choledocholithotomy.2. Choledocholithotomy.3. Cholecystoduodenostomy.3. Cholecystoduodenostomy.4. Laparoscopic cholecystectomy. 4. Laparoscopic cholecystectomy.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

81
Postoperatively, a patient with an incisional Postoperatively, a patient with an incisional cholecystectomy has a nursing diagnosis of cholecystectomy has a nursing diagnosis of ineffective breathing pattern related to splinted ineffective breathing pattern related to splinted respirations secondary to a high abdominal respirations secondary to a high abdominal incision. The nursing intervention that should be incision. The nursing intervention that should be implemented first for this patient is to:implemented first for this patient is to:
1. Assess lung sounds every 2 to 4 hours.1. Assess lung sounds every 2 to 4 hours.2. Provide analgesics to relieve incisional pain.2. Provide analgesics to relieve incisional pain.3. Assist the patient to cough and deep breathe 3. Assist the patient to cough and deep breathe every hour.every hour.4. Position the patient on the operative side to 4. Position the patient on the operative side to splint the incision. splint the incision.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Case Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 82

83
Case Study
• 35-year-old woman 35-year-old woman presents to emergency presents to emergency department complaining of department complaining of acute abdominal pain.acute abdominal pain.
•She points to pain in the She points to pain in the right upper quadrant.right upper quadrant.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

84
Case Study
•She describes the pain as 7 She describes the pain as 7 out of 10.out of 10.
• Lab values show elevated Lab values show elevated WBCs and bilirubin.WBCs and bilirubin.
•Ultrasound confirms Ultrasound confirms gallstones.gallstones.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

85
Discussion Questions
1.1. What is her priority of care?What is her priority of care?
2.2. What are her treatment What are her treatment options?options?
3.3. What can you teach her What can you teach her about avoiding complications about avoiding complications or recurrences?or recurrences?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.