
Atypische HUS en Complement - nvkc.nl · Atypische HUS en Complement ... acute renal failure Use of...
53
Atypische HUS en Complement Inzicht in pathologie en diagnostiek Nicole van de Kar, MD, PhD. Pediatric Nephrology Radboud University Nijmegen Medical Centre
Transcript of Atypische HUS en Complement - nvkc.nl · Atypische HUS en Complement ... acute renal failure Use of...

Atypische HUS en Complement Inzicht in pathologie en diagnostiek
Nicole van de Kar, MD, PhD.Pediatric Nephrology
Radboud University Nijmegen Medical Centre

Atypische HUS (aHUS) en Complement
• HUS – Thrombotische Microangiopathie
• Oorzaken HUS
• aHUS• Kliniek• Pathogenese• Diagnostiek• Therapie

Volkskrant June 7th, 2011

WHO update 21th of July 2011


Hemolytic uremic syndrome (HUS)
• Clinical features:• Hemolytic anemia
• Abnormal breakdown of red blood cells
• Thrombocytopenia• Low platelet count
• Acute renal failure
• Spectrum • HUS – MPGN - C3 glomerulopathy• HUS – TTP – maligne hypertension

HUS: Cause of clinical features
• Damaged endothelium leads to coagulation � blood vessels in glomerulus get obstructed with thrombi
� Less filtration by glomerulus � acute renal failure
� Use of thrombocytes � thrombopenia
� Damaged erythrocytes � hemolytic anemia

HUS: Blood picture
Normal erythrocytes Schistocytes in HUS

HUS is a thrombotic micro-angiopathy (TMA)
Normal glomerulus TMA

���
Etiology of thrombotic microangiopathy



Atypical HUS
• ‘No diarrhea’……• Age at onset of disease from childhood until adulthood
• Poor prognosis• Severe hypertension• End Stage Renal Disease (ESRD): 50%• Many relapses seen• Mortality: 25%
• Genetic background� complement system� coagulation

Atypical HUS
• Strong association between aHUS and mutations in the complement system:� Opsonisation of infected cells (recognition)� Activation and chemotaxis of leukocytes� Induction of cell lysis by incorporation of Membrane Attack Complex� Interaction met e.g. coagulation� Stimulation of B-cells� Transcription of several genes� Removal of apoptitic debris� Protection against auto-immunity

Classical Pathway
520
170 -
155
450 –
360
420
400 –
350
300 -
225
120 Million
years ago
Lectin Pathway
Alternative Pathway
Acquired Immunity
Complement: an Ancient Immune- and Defense System
15 Adapted from Fujita T, Nature Rev Immunol 2, 346-353, 2002.

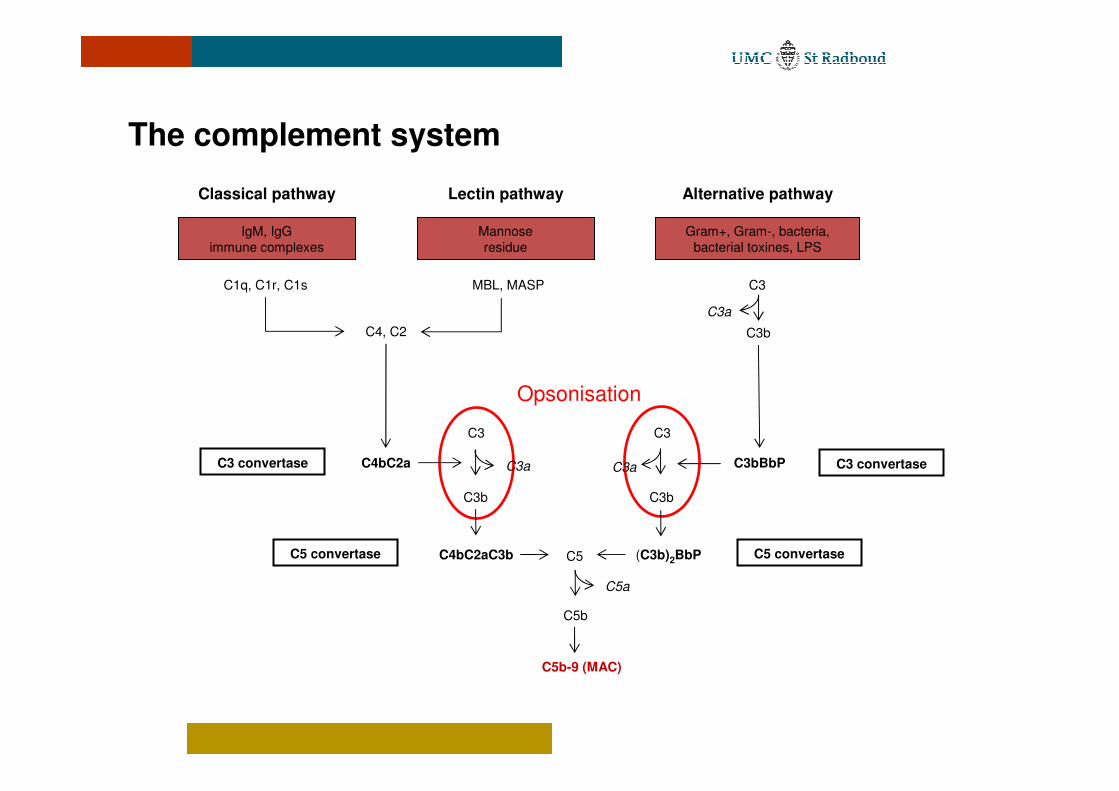
The complement system
Classical pathway Lectin pathway Alternative pathway
IgM, IgGimmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxines, LPS
C1q, C1r, C1s MBL, MASP C3
C4, C2 C3b
C3a
(C3b)2BbP
C3
C3b
C3aC4bC2aC3 convertase
C4bC2aC3bC5 convertase
C3bBbP C3 convertase
C5 convertase
C5b-9 (MAC)
C5
C5b
C5a
C3
C3b
C3a

The complement system
Classical pathway Lectin pathway Alternative pathway
IgM, IgGimmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxines, LPS
C1q, C1r, C1s MBL, MASP C3
C4, C2 C3b
C3a
(C3b)2BbP
C3
C3b
C3aC4bC2aC3 convertase
C4bC2aC3bC5 convertase
C3bBbP C3 convertase
C5 convertase
C5b-9 (MAC)
C5
C5b
C5a
C3
C3b
C3a
Activation and chemotaxis leukocytes
The complement system
Opsonisation
Classical pathway Lectin pathway Alternative pathway
IgM, IgGimmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxines, LPS
C1q, C1r, C1s MBL, MASP C3
C4, C2 C3b
C3a
(C3b)2BbP
C3
C3b
C3aC4bC2aC3 convertase
C4bC2aC3bC5 convertase
C3bBbP C3 convertase
C5 convertase
C5b-9 (MAC)
C5
C5b
C5a
C3
C3b
C3a

The complement system
Classical pathway Lectin pathway Alternative pathway
IgM, IgGimmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxines, LPS
C1q, C1r, C1s MBL, MASP C3
C4, C2 C3b
C3a
(C3b)2BbP
C3
C3b
C3aC4bC2aC3 convertase
C4bC2aC3bC5 convertase
C3bBbP C3 convertase
C5 convertase
C5b-9 (MAC)
C5
C5b
C5a
C3
C3b
C3a
Membrane Attack Complex

Complement system
Classical pathway Lectine pathway Alternative pathway
IgM, IgGImmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxine, LPS
C1q, C1r, C1s MBL, MASP C3
C4, C2
C4bC2a
C3 convertase
C3
C3b
C4bC2aC3b
C5 convertase
C3b
C3bBbP
C3 convertase
C3
(C3b)2BbP
C5 convertase
C3a
C3b
C3a
C3a
C5
C5b
C5a
C5b-9 (MAC)
Factor B
Factor H
Factor I
MCP

aHUS and the complement system
Classical pathway Lectin pathway Alternative pathway
IgM, IgGimmune complexes
Mannose residue
Gram+, Gram-, bacteria, bacterial toxines, LPS
C1q, C1r, C1s MBL, MASP
C4, C2
(C3b)2BbP
C3
C3b
C3aC4bC2aC3 convertase
C4bC2aC3bC5 convertase
C3bBbP
C5 convertase
C5b-9 (MAC)
C5
C5b
C5a
C3
C3b
C3a
Factor B
Factor D
Bb
Ba
C3
C3bC3a
X
Factor H
Factor I
MCP
�
CFHR1/3
� -FH
DAF

Pathogenesis
Adapted from Jokiranta et al. Mol Immunol 2007
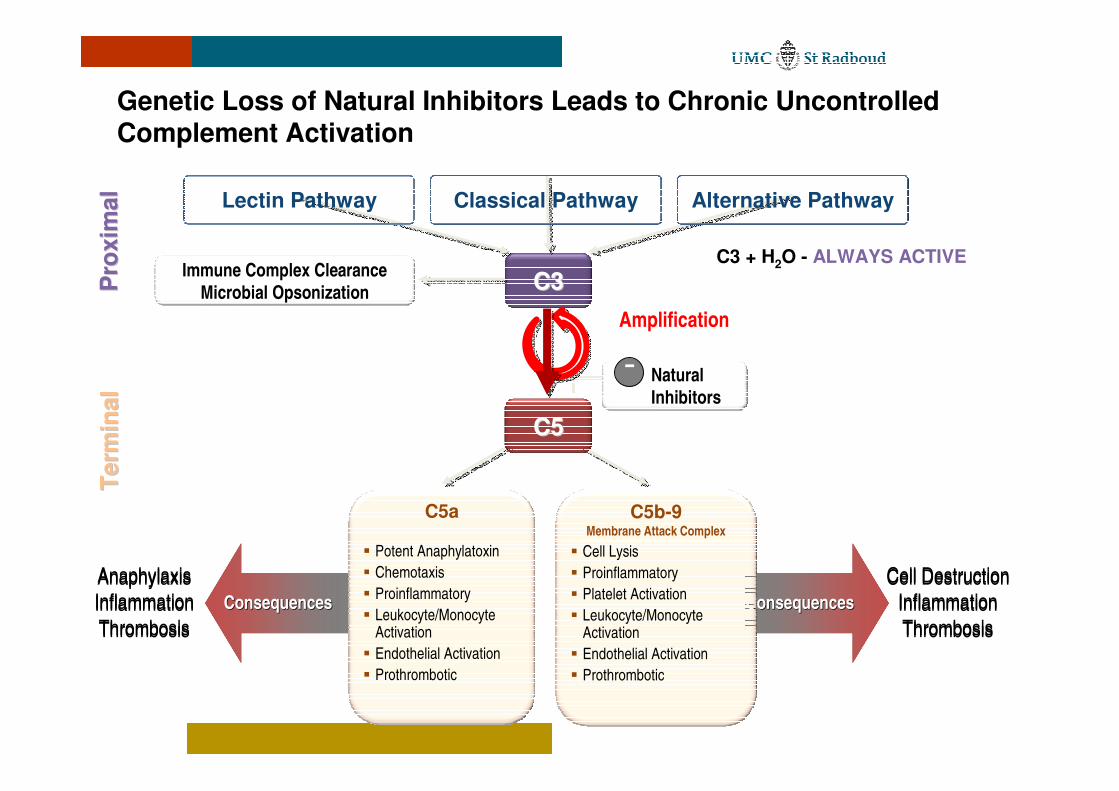
Cell DestructionInflammationThrombosis
Cell DestructionInflammationThrombosis
ConsequencesConsequencesConsequencesConsequences
Genetic Loss of Natural Inhibitors Leads to Chronic UncontrolledComplement Activation
Pro
xim
alP
roxi
mal
Term
inal
Term
inal
C3C3
C5C5
C5a
� Potent Anaphylatoxin� Chemotaxis� Proinflammatory� Leukocyte/Monocyte
Activation� Endothelial Activation� Prothrombotic
C5b-9 Membrane Attack Complex
� Cell Lysis� Proinflammatory � Platelet Activation� Leukocyte/Monocyte
Activation� Endothelial Activation� Prothrombotic
Amplification
Natural Inhibitors
Immune Complex ClearanceMicrobial Opsonization
AnaphylaxisInflammationThrombosis
AnaphylaxisInflammationThrombosis
C3 + H2O - ALWAYS ACTIVE
Lectin Pathway Alternative PathwayClassical Pathway
-

Chronic Uncontrolled Complement Activation Causes Platelet, Endothelium, Leukocyte Activation and Leads to Inflammation and Systemic Small Vessel Occlusion
Adapted from Desch et al JASN. 2007; 18:2457-60. Licht C et al Blood 2009 114:4538-4545. Noris et al NEJM. 2009; 361: 1676-87. Stahl et al Blood 2008; 111(11)5307-15. Morigi et al J Immunol 2011 ePub 3 June
Endothelial Activation
Platelet
PlateletActivation
LeukocyteActivation
ChronicChronicUncontrolledUncontrolledComplementComplement
ActivationActivation
Endothelial swelling and disruption
Platelet consumption
Mechanical hemolysis
Blood clot formation
Vessel occlusion
Inflammation
Ischemia
Hypoxia
Plateletaggregation
Antibodies against factor H
• Found in 6 - 10% aHUS, mostly young children• Block the C terminal recognition domain of CFH• Majority homozygeous deletion CFHR1-CFHR3
• Newcastle cohort n=142 (Moore et al, Blood 2010;115:379-387)
• 13 / 142 (1-11y) antibodies CFH• 10 / 13 no copies CFHR1• In 5 patients: 1x CFH, 1x CFI, 1x MCP, 2x C3

Antibodies against factor H

27
aHUS: a disorder of complement regulation
Antibodiesagainst FH
28
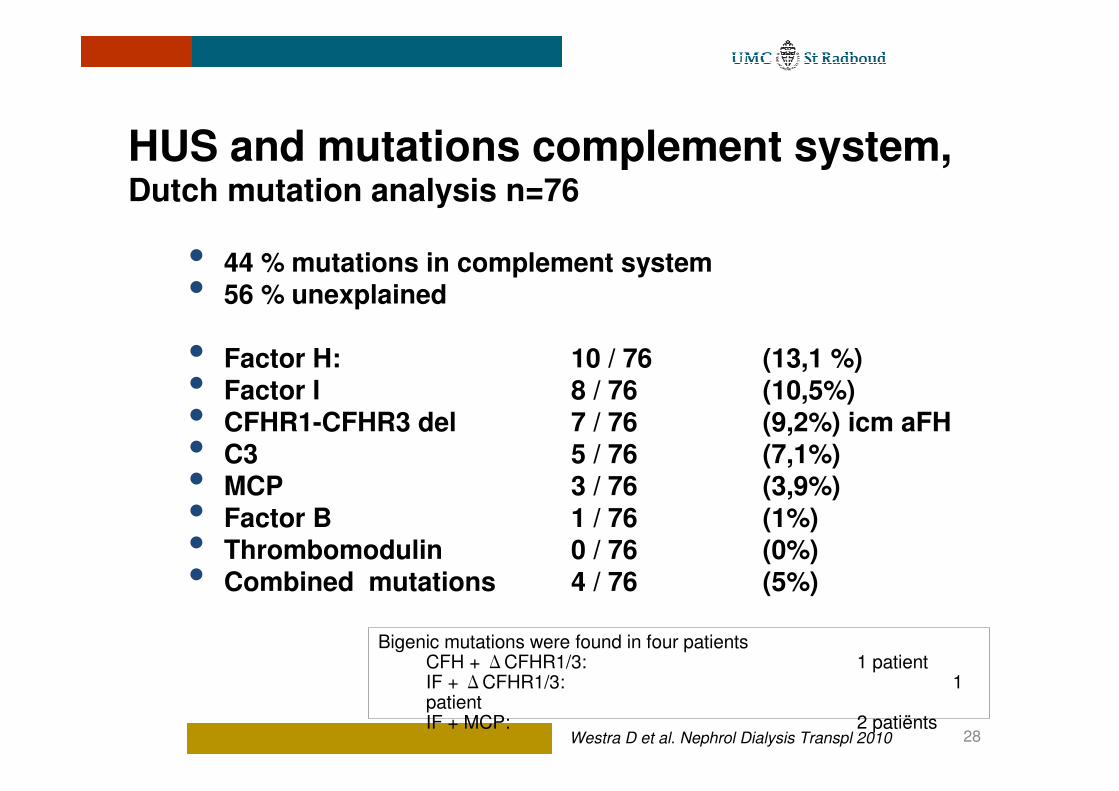
HUS and mutations complement system,Dutch mutation analysis n=76
• 44 % mutations in complement system• 56 % unexplained
• Factor H: 10 / 76 (13,1 %)• Factor I 8 / 76 (10,5%)• CFHR1-CFHR3 del 7 / 76 (9,2%) icm aFH• C3 5 / 76 (7,1%) • MCP 3 / 76 (3,9%)• Factor B 1 / 76 (1%)• Thrombomodulin 0 / 76 (0%)• Combined mutations 4 / 76 (5%)
Bigenic mutations were found in four patientsCFH + �CFHR1/3: 1 patientIF + �CFHR1/3: 1 patientIF + MCP: 2 patiënts
Westra D et al. Nephrol Dialysis Transpl 2010

29
Role of genetic complement abnormalities in HUS and their impact on clinical phenotype. Noris M et al, CJASN 2010
• 273 patients aHUS / non-STEC HUS
• CFH 65 / 273 (24%)• MCP 18 / 273 (6,6%)• CFI 10 / 273 (3,7%)• C3 12 / 273 (4,4%)• THBD 13 / 273 (4,7%)• CFH Ab 8 / 273 (3%)• No mutation 130/ 273 (48%)

30
Study Caprioli et al, Blood 2006;108:1267-1279

Penetrance of disease
• Incomplete penetrance is described (40-50%)1,2 �
• Combination of mutations, risk haplotypes and SNPs• Complement trigger to unmask regulatory defects
1 Kavanagh et al. Annu Rev Med. 2008
2 Noris et al. N Engl J Med. 2009
Impact of mutations in complement genes
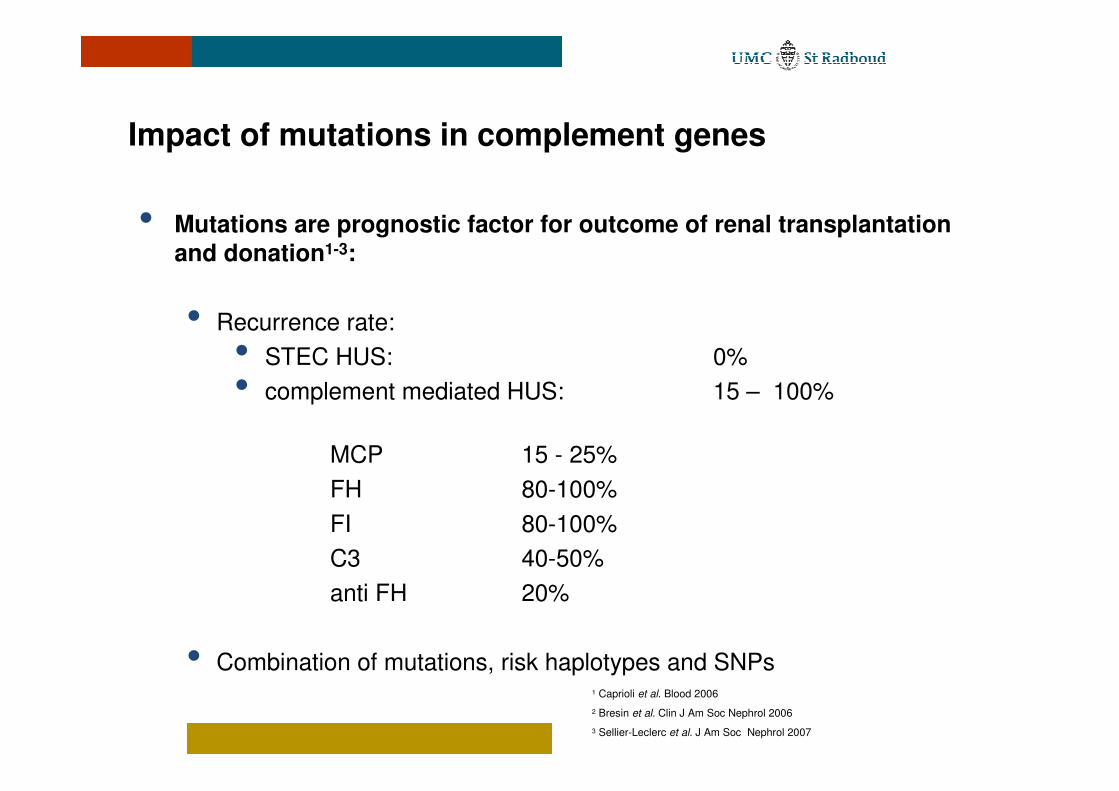
• Mutations are prognostic factor for outcome of renal transplantation and donation1-3:
• Recurrence rate:• STEC HUS: 0%• complement mediated HUS: 15 – 100%
MCP 15 - 25%FH 80-100%FI 80-100%C3 40-50%anti FH 20%
• Combination of mutations, risk haplotypes and SNPs1 Caprioli et al. Blood 2006
2 Bresin et al. Clin J Am Soc Nephrol 2006
3 Sellier-Leclerc et al. J Am Soc Nephrol 2007

Clinical outcome of patients with aHUS with mutations in complement genes
Waters AM et al Pediatrc Nephrol 2010

34
Treatment new aHUS patient at the moment......
• Plasma exchange• 40-60 ml/kg in the beginning daily, then 3 times a
week / titration (thrombocytes > 150.109)
• Plasma-infusion• First day 30-40 ml/kg• Thereafter 10-20 ml /kg
• Role of plasma in aHUS patients with MCP mutation?
35
Renal transplantation and aHUS (1)
• Complement analysis incl. genotyping
• No living-related donor. Donne et al Am J Kidney Dis 2002
Yes living-unrelated?Condition Tx: non-heart beating? Total ischemia time <24 hours?CAVE Acute tubular necrosis No calcineurin inhibitors first month??
• Protocol plasma exchange 4 weeks• Before transplantation• First week 5-7 days• Second week: three times a week• Third week: twice a week• Once a week
• CFH / IF liver-kidney transplantation / plasma exchange
• Eculizumab!

36Noris M, Remuzzi G, Am J Transplant 2010
Schematic presentation of transplant options in aHUS patients
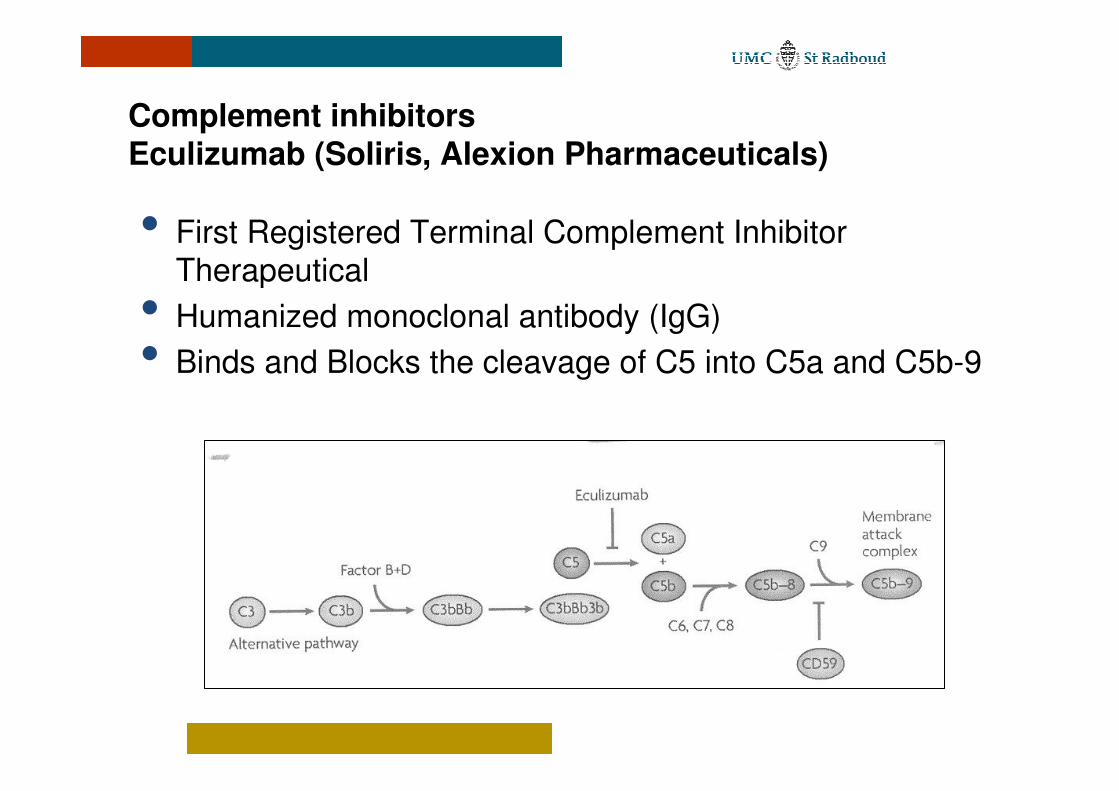
Complement inhibitorsEculizumab (Soliris, Alexion Pharmaceuticals)
• First Registered Terminal Complement Inhibitor Therapeutical
• Humanized monoclonal antibody (IgG)• Binds and Blocks the cleavage of C5 into C5a and C5b-9

Eculizumab for congenital atypical HUS in patiënt unresponse to plasma therapy (4 relapses in first 18 months, Pinf)
Gruppo RA et al, N Engl J Med 360;5:544-546,2009

Eculizumab Multinational, Multi-CenterClinical Program in aHUS (N=67)
Study C09-001(N=30)
19 Patients <18 years old
Clinical Diagnosis Clinical Diagnosis of aHUS:of aHUS:
Medical Practice Medical Practice SettingSetting
Clinical Diagnosis of aHUS With:Clinical Diagnosis of aHUS With:�� TMA (measured by platelet count, hemolysis)TMA (measured by platelet count, hemolysis)�� Organ Damage (serum creatinine Organ Damage (serum creatinine ��ULN)ULN)�� ADAMTS13 >5%; no positive STEC testADAMTS13 >5%; no positive STEC test�� No requirement for identified genetic mutationNo requirement for identified genetic mutation
RetrospectiveProspective
Long-term Extension Studies
86% (32/37) of patients continued chronic eculizumab treatment in extension studies
Study C08-003(N=20)
Adult/Adolescent
Study C08-002(N=17)
Adult/Adolescent
(26 weeks)

Prospective Studies: Eculizumab Dosing Schedule* Pretreatment Induction Phase Maintenance Phase
≥2 weeks before induction
Week�
1 2 3 4 5 6 7 8
9 and every
2 weeks thereafter
Neisseria meningitidis vaccination/ antibiotics
Eculizumab dose, mg�
900 900 900 900 1200 X 1200 X 1200
� Administration: IV infusion over 35 min every 7 d during induction and every 14 d during maintenance– Dose adjustment to every 12 days permitted
� Meningococcal prophylaxis: patients received meningococcal vaccination prior to receipt of eculizumab or received prophylactic treatment with antibiotics until 2 weeks after vaccination
*For patients <18 years of age, administration of eculizumab is based on body weight (ungoing pediatric trial)
Soliris® (eculizumab). Prescribing information. Alexion Pharmaceuticals, Inc. 2011

Eculizumab Reduced Complement Activity in All Patients
*
Chronic Uncontrolled Complement Activation
� Reduction observed in all patients after initiation of eculizumab treatment
� Reduction demonstrated as early as 1 hour after the first eculizumab dose and effect sustained through week 26
Change From Baseline to End of Study Period
Days on Eculizumab Treatment
28 84 168
C08-002C08-003

Eculizumab led to TMA Event-Free Status in80% of Patients
(N=20)
• The benefit was sustained through the entire study period (median eculizumab 62 weeks)
Four patients who did not achieve TMA event-free status did maintain a normal platelet count without PE/PI or new dialysis
Complement-Mediated TMAC08-003
• No decrease in platelet count >25% from baseline AND
• No plasma exchange/infusion AND• No new dialysis
For at least 12 consecutive weeks• In 20/20 patients:
−Elimination of PE/PI AND−No new dialysis

Conclusions: Eculizumab for Patients WithA Long Duration of Disease
Chronic eculizumab treatment resulted in sustained benefits:− Complement activity inhibition in all patients
− 80% of patients TMA-event free
− 90% of patients with hematologic normalization
− 100% of patients discontinuing PE/PI
− Rapid and sustained improvements in HRQoL
− Longer term eculizumab was well tolerated
• Similar results for patients with and without genetic mutations • Long-term improvement in renal function
− Significant, continuous, time-dependent improvement in eGFR
− Significant improvements in proteinuria
� Earlier treatment of TMA complications associated with increased likelihood of improved kidney function
C08-003
Licht C et al. ESPN Annual Meeting 2011 (Poster PS2-FRI-272); Licht C et al. ASN Annual Meeting 2011 (Poster TH-PO366)

Conclusions: Eculizumab for Patients withShorter Duration of Disease
• Chronic eculizumab treatment resulted in sustained benefits:• Complement activity inhibition in all patients• Significant and sustained increase in platelet count• 76% of patients achieved hematologic normalization• 88% of patients achieved TMA event free status• 100% of patients reduced PE/PI• 4/5 (80%) of patients eliminated dialysis with sustained eculizumab
• Similar improved outcomes were observed in patients with or without identified genetic mutations
• Continuous improvement in renal function• Significant, continuous, time-dependent improvement in eGFR• Significant improvements in proteinuria
• Earlier treatment of TMA complications associated with increasedlikelihood of improved kidney function
C08-002
Loirat C et al. ESPN Annual Meeting 2011 (Poster PS2-FRI-273); Greenbaum et al. ASN Annual Meeting 2011 (Poster TH-PO367)

• No meningococcal infection2
• All patients remain alive2
• Similar safety profile as observed in long-term PNH use3
(N=20)
Upper respiratory tract infectionb 8 (40)
Diarrhea 6 (30)
Adverse events, n (%)*1 5 (25)
Abdominal pain 4 (20)
Headache 4 (20)
Pharyngolaryngeal pain 4 (20)
Anemia 3 (15)
Cough 3 (15)
Nausea 3 (15)
Pain in extremity 3 (15)
Vertigo 3 (15)
Vomiting 3 (15)
Leukopenia 2 (10)
Urinary tract infection 2 (10)
Fatigue 1 (5)
Insomnia 1 (5)
Peripheral edema 1 (5)
Pyrexia 1 (5)
Adverse EventsSafetyC08-003

WarningWARNING: SERIOUS MENINGOCOCCAL INFECTIONS
See full prescribing information for complete boxed warning
Life-threatening and fatal meningococcal infections have occurred in patients treated with Soliris. Meningococcal infection may become rapidly life-threatening or fatal if not recognized and treated early.•Comply with the most current Advisory Committee on Immunization Practices (ACIP) recommendations for meningococcal vaccination in patients with complement deficiencies.
•Immunize patients with a meningococcal vaccine at least 2 weeks prior to administering the first dose of Soliris, unless the risks of delaying Soliris therapy outweigh the risks of developing a meningococcal infection. (See Serious Meningococcal Infections for additional guidance on the management of the risk of meningococcal infection.)
•Monitor patients for early signs of meningococcal infections, and evaluate immediately if infection is suspected.Soliris is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS). Under the Soliris REMS prescribers must enroll in the program (5.2). Enrollment in the Soliris REMS program and additional information are available by telephone: 1-888-SOLIRIS (1-888-765-4747).
Please see full prescribing information for SOLIRIS® (eculizumab).Soliris® [package insert]. Alexion Pharmaceuticals, Inc.; 2011.
AHUS patient at the moment
• Diagnosis in time and start adequate treatment in time
•Plasmapheresis,Plasmainfusions•Eculizumab
• Finance• Need for development guidelines use eculizumab!!!!!
• Genetic analysis complement genes / auto-antibodies against FH
•Avoiding triggers for endothelial activation

Wat nu?....De Uitdaging !!
• 82.000 – 500.000 euro / jaar• Wie nu eculizumab ?• Rol van plasmaferese ? • Tijdstip start eculizumab, rondom Tx?• Hoe lang?? Levenslang?
• Richtlijnen / voorwaarden opstellen• Diagnose afhankelijk etiologie / Plasmatherapie
• Landelijke registratie volwassenen / kinderen HUS

aHUS: a disorder with many risk factors


AHUS patient at the moment
• Dysregulation of complement• Normal serum C3,C4,FH,FI does not rule out
complement dysregulation• Diagnosis in time and start adequate treatment in
time•Plasmapheresis,Plasmainfusions•Eculizumab
• Finance• Need for development guidelines use eculizumab!!!!!
• Genetic analysis complement genes / auto-antibodies against FH
•Avoiding triggers for endothelial activation

Symposium
“Pathogenesis and Treatment of atypical HUS”
www.VTEC2012.org
��� �������� ��� �������


















