Angioplastía del TCI: El Papel de la Imagen IntracoronariaAngioplastía del TCI: El Papel de la...
44
Angioplastía del TCI: El Papel de la Imagen Intracoronaria Mauricio G. Cohen, MD, FACC Associate Professor of Medicine, Director Cardiac Cath Lab @DrMauricioCohen #RadialFirst
Transcript of Angioplastía del TCI: El Papel de la Imagen IntracoronariaAngioplastía del TCI: El Papel de la...

Angioplastía del TCI: El Papel de la Imagen Intracoronaria
Mauricio G. Cohen, MD, FACC
Associate Professor of Medicine,
Director Cardiac Cath Lab
@DrMauricioCohen
#RadialFirst

Disclosure Statement of Financial Interest
Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or
affiliation with the organization(s) listed below.
Affiliation/Financial Relationship Company
Grant/Research Support
Consulting Fees/Honoraria Abiomed / Terumo Medical / Medtronic /
Merit Medical / The Medicines Company
Major Stock Shareholder/Equity Accumed
Royalty Income None
Ownership/Founder None
Intellectual Property Rights None
Other Financial Benefit None

Circ Cardiovasc Interv. 2016;9:e003700
Major Adverse Cardiac Events
7 RCTs
3192 patients
IVUS associated with larger post-PCI MLD,
and greater reduction in the diameter stenosis

Circ Cardiovasc Interv. 2016;9:e003700
Cardiovascular Mortality
Myocardial Infarction
TLR
Stent Thrombosis 0.49 (0.24–0.99) 0.04
0.60 (0.43–0.84) 0.003
0.52 (0.26–1.02) 0.06
0.46 (0.21–1.00) 0.05
OR (95% CI) p value

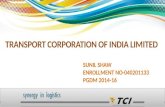
ADAPT DES: How IVUS changed the procedure?
38
23 22
13
7 8
0
10
20
30
40
50
Larger stentor balloon
Higherinflationpressure
Longer stent Incompleteexpansion
Incompleteapposition
Additionalstent
Pati
en
ts, %
Post Dilation
Operator changed the PCI strategy in 74% (2484/3349) of patients
IVUS used:
• before PCI only 7%
• after PCI only 30%
• before and after PCI 63%
Witzenbichler B et al.
Circulation 2014;129:463-470
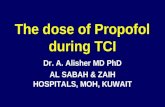
“All-comers” study of 8,583 patients to determine the frequency,
timing, and correlates of stent thrombosis and adverse clinical
events after DES. IVUS utilized in 3349 patients (39%)

Definite/P
robable
ST
(%
)
Time in Months
3361 3260 3182 3065 1791
5221 5019 4886 4713 2279
Number at risk:
IVUS Used
IVUS Not Used
P = 0.004
HR: 0.47 [95% CI: 0.28, 0.80]
0.55%
1.16%
0
1
2
0 6 12 18 24
IVUS Used
No IVUS Used
Witzenbichler B et al. Circulation. 2014;129:463-470
Relationship Between IVUS Use and Definite/Probable Stent
Thrombosis Within 2 Years

Case Presentation
• 74 yo woman, DM, HTN, DLP, CKD III, Obesity (BMI 44)
2008: BKA of the left / right iliac stent
2015: Lateral wall MI – PCI of LCx
• Current presentation: NSTEMI
• Diffuse 2 mm down sloping ST segment depression
• Troponin 0.3, GFR 33 (Cr 1.44), Hb 12.5, Plts 144
• Small R radial artery, 2.5-3 mm L radial artery
• STS PROM 4.042%
• CT surgery said NO


Diagnostic
Cath
Syntax Score 29

Left Main Disease – Rules
• Heart Team discussion - Guidelines
• Stenting strategy
Location: ostium, shaft and/or bifurcation
Understanding of bifurcation stenting techniques
• Imaging is critical: IVUS or OCT
• Focus on access safety
Transradial access with slender 7-in-6
Transfemoral for support
• Pelvis CT to assess iliofemoral vessel size
• Ultrasound guided access with micropuncture

Recommendations for LM Revascularization
Levine G, et al. J Am Coll Cardiol. 2011;58:44-122
Windecker S, et al. Eur Heart J. 2014;35:2541-619
United States Europe
PCI CABGLow
SxScore 0-22 IIa B I B
Intermediate
SxScore 23-32 IIb B I B
High
SxScore >32 III B I B
PCI CABGLow
SxScore 0-22 I B I B
Intermediate
SxScore 23-32 IIa B I B
High
SxScore >32 III B I B

8,1
10,8
15
8,3
12,7 12,4
0
2
4
6
8
10
12
14
16
SS 0-22 SS 23-32 SS >33
PCI CABG
Head SJ et al. Lancet 2018; 391: 939–48
Left Main Disease
All Cause Mortality11 Trials 1·02 (0·77–1·34)
P= 0·91
1·20 (0·94–1·51)
P= 0·14
1·52 (1·15–2·02)
P=0·0029
Mortality According to
Syntax Score
Pinteraction
0·21

Relative Risk Reduction with PCI
vs. CABG in the EXCEL TrialProcedure
Early Peri-procedure
Stone GW et al. N Engl J Med 2016;375:2223-2235
-50%
-38%
-58%
-75%
-86% -87%-100%
-90%
-80%
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
Str
oke
MI
Ble
ed
ing
Rena
l fa
ilure
Pro
lon
ged
intu
bation
Arr
hyth
mia
s
**
*
*
**
*P<0.05
Short Term Outcomes

Pre-stent deployment assessment of lesion
characteristics, calcification, and size for LM
Disease feature Studied cutoff
Plaque characterization Thin cap fibroadenoma, fibrotic,
lipid-rich, or calcified
Minimal luminal area (MLA) < 6 mm2
Lesion calcification requiring
atherectomy
> 270°
Landing zone evaluation Ideally, < 50% stenosis and without
lipid-rich plaque.

IVUS to Guide the LM Intervention
de la Torre Hernandez J et al. JACC CV Int 2014;7:244–54
Pooled analysis of 4 registries in Spain – 2 propensity-matched
groups of 1010 pts (505 x 2) with and without IVUS
IVUS No IVUS P
Overall, n 505 505
MACE (Death, MI, TLR) 14.4 22.2 0.006
- Death 7.4 13.0 0.01
- Cardiac 3.3 6.0 0.07
- MI 4.5 6.5 0.4
- TLR 7.7 6.3 0.7
Stent thrombosis (def/prob) 0.6 2.2 0.04
Subgroup with distal lsns, n 221 226
Cardiac death, MI, TLR 11.0 19.0 0.03
Distal lsns + 2 stents, n 63 62
Cardiac death, MI, TLR 16.7 41.0 0.02
MACEAdj HR (95%CI) =
0.70 (0.52–0.99)
P = 0.04
Days
Surv
ival (%
)
IVUS
No IVUS
100
90
80
70
60
0 200 400 600 800 1000 1200
Slide Courtesy: Gregg Stone


EXCEL Trial: IVUS-Guided PCI
in 690/935 pts (74%)
Pre and Post-Stenting
Post-Stenting Only
Pre-Stenting Only
43.2%
39.1%
16.4%
Maehara A. TCT 2016

EXCEL: Change in LM stenting by IVUS
YESNO
51.7%
N=357
48.3%
N=333
• Used larger balloon: 30% (107)
• Post-dilated: 29% (102)
• Used higher pressure: 17% (62)
• Treated stent under-expansion: 16% (57)
• Led to provisional 1 stent strategy rather
than planned 2 stents: 11% (41)
• Led to planned 2 stent strategy rather
than provisional 1 stent: 9% (33)
Maehara A. TCT 2016

*IDR: ischemia driven revascularization
IVUS MSA tertiles (range)Low: 4.4-
8.7 (n=172)
Inter: 8.8-
10.9 (n=169)
High:
11.0-17.8
(n=163)
P
L vs I
P
L vs H
Death/MI/stroke 19.4% (32) 16.1% (26) 9.6% (15) 0.45 0.01
Death/MI/stroke/IDR* 26.6% (44) 23.8% (39) 18.3% (29) 0.66 0.08
All cause death 13.8% (22) 10.0% (16) 5.2% (8) 0.34 0.01
Cardiovascular death 7.4% (12) 4.8% (8) 4.0% (6) 0.39 0.16
MI 10.5% (17) 8.2% (13) 3.7% (6) 0.49 0.02
Stroke 1.8% (3) 1.2% (2) 2.1% (3) 0.66 0.98
Stent thrombosis (D/P) 3.1% (5) 1.2% (2) 0.0% (0) 0.26 0.03
Left main IDR 12.0% (19) 8.3% (13) 8.8% (14) 0.30 0.41
Non-TV IDR 1.9% (3) 3.3% (5) 1.3% (2) 0.48 0.65
3-Year Outcomes by LM Minimal Stent Area
Maehara A. TCT 2016

Conclusions of EXCEL IVUS Substudy
• In the EXCEL trial, 73% of PCI cases were performed
using IVUS guidance. In the half of IVUS guidance cases,
the procedure was changed by the IVUS findings.
• After treatment with CoCr-EES, a small final MSA of the
left main coronary artery measured by IVUS was strongly
associated with death, MI and stent thrombosis during
long-term follow-up.
Maehara A. TCT 2016

• 11.4% with ISR at 9 months
• 33.8% with underexpansion of one segment
• Angiographic ISR 24.1% with underexpansion
vs. 5.4% without underexpansion.
• Although acute malapposition was observed in
28 pts, malapposition was not related to MACE
at follow-up.
LAD
ostium
LCX ostiumPOC
Proximal
LM 8mm2
Criteria for Underexpansion
Kang et al. Circulation Cardiovasc Interv. 2011;4:562-9

MACE98.1%
90.2%
Months after Initial Procedure
Eve
nt F
ree
Su
rviv
al R
ate
(%
)
P<0.001
100
Log-rank test
Underexpansion (+)
Underexpansion (-)
No. at risk
Underexpansion (+)
Underexpansion (-)
133
260
131
260
126
255
121
246
75
129
90
80
70
60
50
40
0 6 12 18 24
TLR
98.5%
90.9%
Months after Initial Procedure
Eve
nt F
ree
Su
rviv
al R
ate
(%
)
P=0.001
100
Log-rank test
Underexpansion (+)
Underexpansion (-)
No. at risk
Underexpansion (+)
Underexpansion (-)
133
260
131
260
126
255
121
246
75
129
90
80
70
60
50
40
0 6 12 18 24
MACE-free and TLR-free Survival
Kang et al. Circulation Cardiovasc Interv. 2011;4:562-9

• Strut protrusion into the aorta was seen in 68%, with a
protrusion length of 3.4±1.7mm
• Incomplete stent ostial coverage seen in 23%, with uncovered
ostial length of 2.3±1.3mm and residual plaque burden of
38±12%
• Acute malapposition seen 18.8%
• Only 1.2% of LMCA developed ostial restenosis; and not
related to strut protrusion or ostial coverage or acute
malapposition
Kang et al. Am J Cardiol 2013;111:1401-7
n=199 (Left main)
When treating an ostial or proximal lesion with a DES, the
decision of whether to protrude the proximal end of the stent or
leave the ostium uncovered does not appear to be critical

Algorithm for LM Bifurcation PCI
Rab T, et al. JACC Interv 2017;10:849–65
• Provisional stenting of side branch (usually LCx)
• Culotte: narrow angle, similar vessel diameters of
LAD and LCX
• DK Crush: narrow or wide angle, dissimilar vessel
diameters.
• DK crush better than Culotte, provisional
• TAP: wide angle, dissimilar vessel diameters
• T-stent: wide angle
• V-stent: Y bifurcation – Unstable patients
• Simultaneous kissing stents: patient unable to
tolerate ischemia
• Tryton Stent: Non DES

Chen, S-L et al. J Am Coll Cardiol 2017;70:2605–17
Kandzari D et al. Circ Cardiovasc Interv. 2018;11:e007007
DK Crush VDouble Kissing and Double Crush Versus Provisional T Stenting Technique
Stenting Technique N=529
Provisional stent 65.2%
Sidebranch balloon 70.7%
Sidebranch stent 22.1%
Planned 2-stent 34.8%
T-stent 51.1%
Culotte 23.3%
EXCEL Trial
14,4 21,20
5
10
15
20
25
MACE 3 yrs
Provisional 2-Stent
HR 0.51, 95%CI 0.32, 0.82, adjusted P<0.005

Kandzari DE et al. Circ Cardiovasc Interv. 2018;11:e007007
77
Number at risk:
73 72 69 67 67 64264 246 242 238 233 227 218105 90 88 86 85 83 8278 70 69 64 61 60 55
14.3%
19.2%
13.8%
23.3%
0
5
10
15
20
25
30
Time (Months)
0 6 12 18 24 30 36
Provisional 1-stent and 2 SBs with DS ≥50%
Planned 2-stents and 2 SBs with DS ≥50%
Provisional 1-stent and 0-1 SB with DS ≥50%
Planned 2-stents and 0-1 SB with DS ≥50%
De
ath
, s
tro
ke
or
MI (%
)
HR [95% CI =
0.56 [0.32, 0.99]
P = 0.04
HR [95% CI =
0.71 [0.34, 1.48]
P = 0.36
Provisional 1-Stent vs. Planned 2-Stents
For LM Distal Bifurcation Disease (n=529)

Almost all bifurcation lesions, including the
distal LM bifurcation, can be safely treated by
radial artery access using a 6 Fr guiding catheter.
EuroIntervention 2016;12:38-46

Lesion Preparation: 1.5 Rota Burr

IVUS post Rotational Atherectomy


LAD stenting with short main branch
protrusionResolute
2.75 x 30 mm
LAD

LAD stent
balloon crush
NC 3.5 x 12 mm
LCx

Side (LAD) Branch wire recrossing

First kissing
balloon inflation
• NC 3.5 x 12 mm - LCx
• NC 2.5 x 15 mm - LAD

Side branch wire is removed
Main branch (LCx) stenting
across the Side Branch
Resolute 3.5 x38 mm

POT
Proximal
optimization
technique

Second side branch
wire recrossing
through the main
branch stent and the
crushed SB stent

Second kissing
balloon inflation
• NC 3.5 x 12 mm - LCx
• NC 2.5 x 15 mm - LAD

Re-POT
Re–proximal
optimization
techniqueNC 4.0 x 12 mm

IVUS

Final Result

Access and Hemostasis #ldTRA

Ahn et al. BMC Cardiovascular Disorders (2016) 16:49

Unprotected LM PCI
• Heart Team endorsement
• Use your best stent, endorsed by data
• Always imaging
• Knowledge of devices and bifurcation techniques
Provisional stenting is preferred DKCRUSH
• Access:
Consider radial slender techniques. Usually 7-in-6
Femoral access for support Ultrasound & Micropuncture& Preclose