AF1
41
emedicine.medscape.com eMedicine Specialties > Cardiology > Arrhythmias Atrial Fibrillation Lawrence Rosenthal, MD, PhD, Associate Professor of Medicine, Director, Section of Cardiac Electrophysiology and Pacing, Fellowship Director of Clinical Cardiac Electrophysiology, Department of Internal Medicine, Division of Cardiovascular Medicine, University of Massachusetts Memorial Medical Center David D McManus, MD, Assistant Professor of Medicine, Cardiac Electrophysiology Section, Cardiology Division, University of Massachusetts Medical Center Updated: Jun 1, 2010 Introduction Background Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by disorganized atrial electrical activity and progressive deterioration of atrial electromechanical function. Electrocardiographic manifestations of atrial fibrillation include absence of sinus P waves; rapid oscillations (or fibrillatory [f] waves) that vary in amplitude, frequency, and shape; and an irregular ventricular response. Atrial fibrillation is the most common arrhythmia encountered in clinical practice (see Media file 1) and is a significant public health problem in the United States. Atrial fibrillation affects more than 2.2 million Americans and almost 5% of the population older than 69 years. The prevalence of atrial fibrillation increases dramatically with age. Atrial fibrillation is associated with known cardiovascular risk factors such as hypertension, coronary artery and valvular heart disease, heart failure (HF) and diabetes mellitus. [1 ] Data from the Framingham heart study show that atrial fibrillation is associated with a 1.5- to 1.9-fold higher risk of death, which is in part due to the strong association between atrial fibrillation and thromboembolic events. [2 ] While patients can be asymptomatic, many experience a wide variety of symptoms, including palpitations, dyspnea, fatigue, dizziness, angina, and decompensated heart failure. In addition, atrial fibrillation can be associated with hemodynamic dysfunction, tachycardia-induced cardiomyopathy, and systemic thromboembolism. Overall, approximately 15-25% of all strokes in the United States (75,000/y) can be attributed to atrial fibrillation. Known risk factors for stroke in patients with atrial fibrillation include male sex, valvular heart disease (rheumatic valvular disease), heart failure, hypertension, and diabetes. Additional risk factors, such as advanced age and prior history of stroke, diabetes, and hypertension, place patients with preexisting atrial fibrillation at even higher risk for further comorbidities such as stroke (see Table 1). [3 ] Table 1. Risk Factors for Stroke in Patients with Nonvalvular Atrial Fibrillation Risk Factors Relative Risk Prior stroke or TIA 2.5 History of hypertension 1.6 Heart failure and/or reduced left ventricular function 1.4 Advanced age 1.4 Diabetes 1.7 Coronary artery disease 1.5 Patients with rheumatic heart disease and atrial fibrillation have an even higher risk for stroke (17-fold). At least 4 large clinical trials have clearly demonstrated that anticoagulation with warfarin decreases the risk of stroke by 50-80%. Unlike most cardiovascular diseases, the prevalence of atrial fibrillation is increasing in the United States and worldwide. Atrial fibrillation is frequently encountered in both the inpatient and outpatient settings. Primary therapeutic goals include rate control, maintenance of sinus rhythm, and prevention of thromboembolism. For related information, see Medscape's Atrial Fibrillation Resource Center. Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print 1 of 41 6/13/2010 6:30 PM
-
Upload
jessica-fedriani -
Category
Documents
-
view
8 -
download
0
Transcript of AF1

emedicine.medscape.com
eMedicine Specialties > Cardiology > Arrhythmias
Atrial Fibrillation
Lawrence Rosenthal, MD, PhD, Associate Professor of Medicine, Director, Section of Cardiac Electrophysiology and Pacing, Fellowship Director of
Clinical Cardiac Electrophysiology, Department of Internal Medicine, Division of Cardiovascular Medicine, University of Massachusetts Memorial Medical
Center
David D McManus, MD, Assistant Professor of Medicine, Cardiac Electrophysiology Section, Cardiology Division, University of Massachusetts Medical
Center
Updated: Jun 1, 2010
Introduction
Background
Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by disorganized atrial electrical activity and progressive
deterioration of atrial electromechanical function. Electrocardiographic manifestations of atrial fibrillation include absence of sinus P
waves; rapid oscillations (or fibrillatory [f] waves) that vary in amplitude, frequency, and shape; and an irregular ventricular response.
Atrial fibrillation is the most common arrhythmia encountered in clinical practice (see Media file 1) and is a significant public health
problem in the United States. Atrial fibrillation affects more than 2.2 million Americans and almost 5% of the population older than 69
years. The prevalence of atrial fibrillation increases dramatically with age. Atrial fibrillation is associated with known cardiovascular risk
factors such as hypertension, coronary artery and valvular heart disease, heart failure (HF) and diabetes mellitus.[1 ]
Data from the Framingham heart study show that atrial fibrillation is associated with a 1.5- to 1.9-fold higher risk of death, which is in part
due to the strong association between atrial fibrillation and thromboembolic events.[2 ]While patients can be asymptomatic, many
experience a wide variety of symptoms, including palpitations, dyspnea, fatigue, dizziness, angina, and decompensated heart failure. In
addition, atrial fibrillation can be associated with hemodynamic dysfunction, tachycardia-induced cardiomyopathy, and systemic
thromboembolism.
Overall, approximately 15-25% of all strokes in the United States (75,000/y) can be attributed to atrial fibrillation. Known risk factors for
stroke in patients with atrial fibrillation include male sex, valvular heart disease (rheumatic valvular disease), heart failure, hypertension,
and diabetes. Additional risk factors, such as advanced age and prior history of stroke, diabetes, and hypertension, place patients with
preexisting atrial fibrillation at even higher risk for further comorbidities such as stroke (see Table 1).[3 ]
Table 1. Risk Factors for Stroke in Patients with Nonvalvular Atrial Fibrillation
Risk Factors Relative Risk
Prior stroke or TIA 2.5
History of hypertension 1.6
Heart failure and/or reduced left ventricular function 1.4
Advanced age 1.4
Diabetes 1.7
Coronary artery disease 1.5
Patients with rheumatic heart disease and atrial fibrillation have an even higher risk for stroke (17-fold). At least 4 large clinical trials
have clearly demonstrated that anticoagulation with warfarin decreases the risk of stroke by 50-80%.
Unlike most cardiovascular diseases, the prevalence of atrial fibrillation is increasing in the United States and worldwide. Atrial
fibrillation is frequently encountered in both the inpatient and outpatient settings. Primary therapeutic goals include rate control,
maintenance of sinus rhythm, and prevention of thromboembolism.
For related information, see Medscape's Atrial Fibrillation Resource Center.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
1 of 41 6/13/2010 6:30 PM

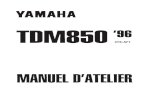
Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves are not
discernible.
Pathophysiology
While the precise mechanisms that cause atrial fibrillation are incompletely understood, atrial fibrillation appears to require both an
initiating event and a permissive atrial substrate. Significant discoveries in the last decade have highlighted the importance of focal
pulmonary vein triggers, but alternative and nonmutually exclusive mechanisms have also been evaluated. These include multiple
wavelets, mother waves, fixed or moving rotors, and macro-reentrant circuits. In a given patient, multiple mechanisms may be present
at any given time. The automatic focus theory and the multiple wavelet hypothesis appear to have the best supportive data.
A focal origin of atrial fibrillation is supported by several experimental models showing that atrial fibrillation persists only in isolated
regions of atrial myocardium. This theory has garnered considerable attention recently as studies have demonstrated that a focal
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
2 of 41 6/13/2010 6:30 PM

source of atrial fibrillation can be identified in humans and that isolation of this source can eliminate atrial fibrillation.
The pulmonary veins appear to be the most frequent source of these automatic foci, but other foci have been demonstrated in several
areas throughout the atria. Cardiac muscle in the pulmonary veins appears to have active electrical properties similar, but not
identical, to those of atrial myocytes. Heterogeneity of electrical conduction around the pulmonary veins is theorized to promote reentry
and sustained atrial fibrillation. Thus, pulmonary vein automatic triggers may provide the initiating event and heterogeneity of conduction
may provide the sustaining event in many patients with atrial fibrillation.
The multiple wavelet hypothesis proposes that fractionation of wavefronts propagating through the atria results in self-perpetuating
“daughter wavelets.” In this model, the number of wavelets is determined by the refractory period, conduction velocity, and mass of
atrial tissue. In this model, increased atrial mass, shortened atrial refractory period, and delayed intra-atrial conduction increase the
number of wavelets and promote sustained atrial fibrillation. This model is supported by data from patients with paroxysmal atrial
fibrillation demonstrating that widespread distribution of abnormal atrial electrograms predicts progression to persistent atrial
fibrillation.[4 ]Intra-atrial conduction prolongation has also been shown to predict recurrence of atrial fibrillation.
[5 ]Together, these data
highlight the importance of atrial structural and electrical remodeling in the maintenance of atrial fibrillation.
Atrial fibrillation shares strong epidemiologic associations with other cardiovascular diseases such as heart failure, coronary artery
disease, valvular heart disease, diabetes mellitus and hypertension.[1 ]These factors have been termed upstream risk factors, but the
relationship between comorbid cardiovascular disease and atrial fibrillation is incompletely understood and more complex than this
terminology implies. The exact mechanisms via which cardiovascular risk factors predispose to atrial fibrillation are not fully understood
but are under intense investigation. Catecholamine excess, hemodynamic stress, atrial ischemia, atrial inflammation, metabolic stress,
and neurohumoral cascade activation are all purported to promote atrial fibrillation.
Frequency
United States
Atrial fibrillation affects more than 2.2 million Americans. One in 4 individuals 40 years of age and older will develop atrial fibrillation
during their lifetime.[6 ]Atrial fibrillation can occur in the absence of comorbidities, as it does in 10-15% of cases of atrial fibrillation (lone
atrial fibrillation). However, atrial fibrillation is often associated with other cardiovascular diseases, including hypertension; heart failure;
diabetes; ischemic heart disease; and valvular, dilated, hypertrophic, restrictive, and congenital cardiomyopathies.[6 ]
Atrial fibrillation can be triggered after cardiac surgery and is associated with pulmonary disease, thyrotoxicosis, acute ethanol
intoxication, and electrolyte imbalance. Given the almost epidemic proportions of patients with atrial fibrillation, clinicians should be
aware of the multiple mechanisms and triggers for atrial fibrillation. Correcting the underlying disorder is often necessary to
successfully treat atrial fibrillation.
Mortality/Morbidity
Atrial fibrillation is associated with increased morbidity and mortality, in part due to the risk of thromboembolic disease in atrial fibrillation
and its associated risk factors. Disruption of normal atrial electromechanical function in atrial fibrillation leads to blood pooling and
blood stasis. This, in turn, can lead to development of thrombus, most commonly in the left atrial appendage. Dislodgement of a clot
can lead to embolic phenomena, including stroke.
One of the major management decisions in atrial fibrillation (and atrial flutter) is determining the risk of stroke and appropriate
anticoagulation regimen for low-, intermediate-, and high-risk patients. For each anticoagulant, the benefit in terms of stroke reduction
must be weighed against the risk of serious bleeding.
Most clinicians agree that the risk-benefit ratio of warfarin therapy in low-risk patients with atrial fibrillation is not advantageous (due to
the increased risk of a significant bleed versus the risk of stroke in low-risk patients). Warfarin therapy has, however, been shown to be
beneficial in higher-risk patients with atrial fibrillation. A target international normalized ratio (INR) of 2-3 is traditionally used in this cohort
as this limits the risk of hemorrhage, while providing protection against thrombus formation.
The appropriate treatment regimen for patients with atrial fibrillation at intermediate risk is controversial. In this population, the clinician
should assess risk factors for thromboembolic disease, patient preference, risk of bleeding, risk of falls or trauma, and likelihood of
medication adherence. Warfarin is also superior to clopidogrel or a combination of clopidogrel and aspirin in the prevention of embolic
events in higher-risk patients. A new class of oral direct thrombin inhibitors are in the late stages of clinical trial or pending approval and
may be as effective and as safe as warfarin in higher-risk nonvalvular atrial fibrillation.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
3 of 41 6/13/2010 6:30 PM

Several risk factor assessment algorithms have been developed to aid the clinician in decision-making regarding anticoagulation in
atrial fibrillation. The CHADS2 index[7 ](Cardiac failure, Diabetes, Stroke [or S2 = TIA]) is the most widely used of these algorithms. The
CHADS2 index uses a point system to determine yearly thromboembolic risk. Two points are assigned for a history of stroke or TIA,
and one point is given for age over 75 or a history of hypertension, diabetes, or heart failure. The predictive value of this scoring
system was evaluated in 1733 elderly patients with nonvalvular atrial fibrillation aged 65-95 who were not given warfarin at hospital
discharge. Although high scores were associated with an increased rate of stroke, few patients had a score greater than 5 or a score of
0 (see Table 2).
Table 2. Adjusted Stroke Rate in Patients with Nonvalvular Atrial Fibrillation not Treated with Anticoagulation
CHADS2 Score Adjusted Stroke Rate (%/y)
0 1.9
1 2.8
2 4.0
3 5.9
4 8.5
5 12.5
6 18.2
Recommendations for anticoagulation for patients with nonvalvular atrial fibrillation are based on 2006 ACC/AHA/ESC task force
guidelines on the management of patients with atrial fibrillation[8 ](see Table 3).
Table 3. Recommendations for Antithrombotic Therapy in Patients with Nonvalvular Atrial Fibrillation
Risk Category Recommended Therapy
No risk factors Aspirin 81-325 mg daily
One moderate-risk factor Aspirin 81-325 mg daily or warfarin (INR 2-3)
Any high-risk factor or more than 1 moderate-risk factor Warfarin (INR 2-3)
High-risk factors include prior stroke, TIA, and systemic thromboembolism.
Moderate-risk factors include age older than 75 years, hypertension, heart failure, left ventricular function <35%, and diabetes mellitus.
Risk factors of unknown significance include female gender, age 65-74 years, coronary artery disease, and thyrotoxicosis.
Age
Atrial fibrillation is strongly age-dependent, affecting 4% of individuals older than 60 years and 8% of persons older than 80 years. The
rate of ischemic stroke among elderly patients not treated with warfarin averages approximately 5% per year.
Clinical
History
Initial evaluation of the patient with new-onset atrial fibrillation should focus on the patient's hemodynamic stability. An effort should also
be made to evaluate for potential comorbid diseases that contribute to initiation or maintenance of atrial fibrillation. Immediate electrical
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
4 of 41 6/13/2010 6:30 PM

cardioversion should be considered for patients with hemodynamic collapse or evidence of cardiac ischemia.
Initial history
Clinical type of atrial fibrillation should be documented (paroxysmal, persistent, or permanent)
Type, duration, and frequency of symptoms should be assessed
Precipitating factors should be assessed (ie, exertion, sleep, caffeine, alcohol use)
Modes of termination should be assessed (ie, vagal maneuvers)
Prior antiarrhythmics and rate-controlling agents used should be documented
Presence of underlying heart disease should be assessed
Any previous surgical or percutaneous atrial fibrillation ablation procedures should be documented
Physical
The physical examination is helpful in determining underlying causes and sequelae of atrial fibrillation. An initial examination of the
patient with new-onset atrial fibrillation should attend particularly to their hemodynamic stability.
Vital signs: Heart rate, blood pressure, respiratory rate, and oxygen saturation are particularly important in evaluating
hemodynamic stability and adequacy of rate control in atrial fibrillation.
Head and neck: May reveal exophthalmos, thyromegaly, elevated jugular venous pressures, or cyanosis. Carotid artery bruits
suggest peripheral arterial disease and increase the likelihood of comorbid CAD.
Pulmonary: May reveal evidence of heart failure (ie, rales or pleural effusion). Wheezes or diminished breath sounds are
suggestive of underlying pulmonary disease (ie, chronic obstructive pulmonary disease or asthma).
Cardiac: The cardiac examination is central to the physical examination of the patient with atrial fibrillation. A displaced point of
maximal impulse or S3 suggest ventricular enlargement and elevated left ventricular pressure. A prominent P2 points to the
presence of pulmonary hypertension. Thorough palpation and auscultation are necessary to evaluate for valvular heart disease
or cardiomyopathy.
Abdomen: Ascites, hepatomegaly or hepatic capsular tenderness suggest right ventricular failure or intrinsic liver disease.
Lower extremities: Examination of the lower extremities may reveal cyanosis, clubbing or edema. Assessment of peripheral
pulses may lead to the diagnosis of peripheral arterial disease or diminished cardiac output.
Neurologic: Evidence of prior stroke and increased reflexes is suggestive of hyperthyroidism.
Causes
Atrial fibrillation is strongly associated with established cardiovascular risk factors and advancing age. Hypertension, diabetes, and
coronary artery disease promote atrial fibrillation. Structural heart disease, including valvular and congenital heart disease, is also
associated with atrial fibrillation. Acute pulmonary processes, acute or chronic alcohol use (ie, holiday or Saturday night heart, also
known as alcohol-related cardiomyopathy), illicit drug use (ie, stimulants, methamphetamines, cocaine) and hyperthyroidism also
increase the risk of atrial fibrillation. Patients undergoing cardiothoracic or esophageal surgery are another population at risk for atrial
fibrillation. In all, 20-40% of these patients experience postoperative atrial fibrillation. Certain poorly defined genetic factors may also
contribute to an individual's propensity to develop atrial fibrillation.
Hemodynamic stress: Increased intra-atrial pressure results in atrial electrical and structural remodeling and predisposes to
atrial fibrillation. Mitral or tricuspid valve disease and left ventricular dysfunction are the most common causes of increased atrial
pressure. Systemic or pulmonary hypertension also commonly predispose to atrial pressure overload. Intracardiac tumors or
thrombi are rare causes of increased atrial pressure.
Atrial ischemia: Coronary artery disease can infrequently lead directly to atrial ischemia and atrial fibrillation. More commonly,
severe ventricular ischemia leads to increased intra-atrial pressure and atrial fibrillation.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
5 of 41 6/13/2010 6:30 PM

Inflammation: Myocarditis and pericarditis may be idiopathic or may occur in association with the following:
Collagen vascular diseases
Viral or bacterial infections
Cardiac, esophageal, or thoracic surgery
Drug use: Stimulants, alcohol, and cocaine can trigger atrial fibrillation.
Endocrine disorders: Hyperthyroidism and pheochromocytoma have been associated with atrial fibrillation.
Neurologic: Intracranial processes such as subarachnoid hemorrhage or stroke can also precipitate atrial fibrillation.
Familial atrial fibrillation: History of parental atrial fibrillation appears to confer increased likelihood of atrial fibrillation (and
occasional family pedigrees of atrial fibrillation are associated with defined ion channel abnormalities, especially sodium
channels).[9 ]
Differential Diagnoses
Atrial Flutter
Atrial Tachycardia
Atrioventricular Nodal Reentry Tachycardia (AVNRT)
Paroxysmal Supraventricular Tachycardia
Wolff-Parkinson-White Syndrome
Other Problems to Be Considered
Digoxin toxicity
Hyperthyroidism
Pulmonary disease
Cardiac ischemia secondary to rapid ventricular rate
Workup
Laboratory Studies
An electrocardiogram (ECG) should be obtained to establish the diagnosis of atrial fibrillation; look for pre-excitation; determine
heart rate; and evaluate for left ventricular hypertrophy, bundle-branch block, or prior MI. The ECG is also useful to follow the QT
and QRS intervals of patients receiving anti-arrhythmic medications for atrial fibrillation.
Complete blood count, thyroid, hepatic, and renal function panels are often helpful, especially when ventricular rate is difficult to
control.
A toxicology screen or ethanol level may be appropriate to rule out acute intoxication.
Imaging Studies
Transthoracic echocardiogram (TTE)
Evaluate for valvular heart disease
Evaluate atrial and ventricular chamber and wall dimensions
Estimate ventricular function and evaluate for ventricular thrombi
Estimate pulmonary systolic pressure (pulmonary hypertension)
Evaluate for pericardial disease
Transesophageal echocardiogram (TEE)
Evaluate for left atrial (LA) thrombus (particularly in the LA appendage)
To guide cardioversion (if thrombus is seen, cardioversion should be delayed)
When TEE is planned, the concurrent use of TTE may increase cost without providing significant additional information.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
6 of 41 6/13/2010 6:30 PM

Computed tomography (CT) or magnetic resonance imaging (MRI): If atrial fibrillation ablation is planned, then 3-dimensional
imaging technologies (CT scan or MRI) are often helpful to evaluate atrial anatomy. Imaging data can be processed to create
anatomic maps of the left atrium and pulmonary veins.
Chest radiography: May help evaluate lung parenchyma and pulmonary vasculature in the appropriate clinical context.
Other Tests
Electrocardiogram
ECG findings usually confirm the diagnosis of atrial fibrillation.
The ventricular rate is typically irregular.
Discrete P waves are absent; instead, undulating fibrillatory (f) waves are present (see Media file 1).
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
7 of 41 6/13/2010 6:30 PM

Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves
are not discernible.
Six-minute walk test or exercise test
Six-minute walk or exercise testing can help assess the adequacy of rate control.
Exercise testing can exclude ischemia prior to treatment of patients with Class Ic drugs and can be used to reproduce
exercise-induced atrial fibrillation.
Holter monitoring or event recording: Helpful to establish diagnosis and evaluate rate control.
Electrophysiology study
May help identify the mechanism of a wide-QRS-tachycardia.
May help identify a predisposing arrhythmia.
May help identify sites for curative ablation or AV node ablation.
Procedures
Electrical cardioversion
Direct-current (DC) cardioversion is synchronized to the R wave to prevent a shock from being delivered during the vulnerable
phase of the T wave. This reduces the likelihood of inducing ventricular fibrillation.
Elective DC cardioversion is used to restore sinus rhythm if patients are anticoagulated adequately with a therapeutic
international normalized ratio (INR) and remain in atrial fibrillation.
In most patients, the procedure can be performed safely in an outpatient setting.
Administration of either moderate sedation (according to sedation guidelines) or general anesthesia is necessary for patient
comfort and safety during elective atrial fibrillation cardioversion.
Defibrillating patches can be positioned in several locations, including the right anterior chest and left posterior position (left of
the spine). This position allows the defibrillation vector to include the atria. Standard placement in the anterior and lateral
positions is also acceptable.
A high initial success rate should be expected. Some patients remain in sinus rhythm only transiently and quickly revert back to
atrial fibrillation. If initially unsuccessful, check patch placement and consider use of an anti-arrhythmic such as ibutilide (see
Medication section) to reduce the defibrillation threshold and increase the likelihood of cardioversion. Use of defibrillators with
biphasic waveforms have consistently been demonstrated to be more efficacious in converting atrial fibrillation to sinus
rhythm.[10 ]
Patients with atrial fibrillation of less than 48 hours' duration may be considered for immediate cardioversion as the risk of
thromboembolic sequelae from cardioversion in these patients is small.
If the precise duration of the atrial fibrillation cannot be determined or if duration of atrial fibrillation is longer than 48 hours, TEE
should be used to guide cardioversion. Alternatively, if the patient is able to tolerate atrial fibrillation, anticoagulation for 4 weeks
can circumvent the need for TEE prior to cardioversion.
Regardless of long-term anticoagulation strategy or duration of atrial fibrillation, administration of anticoagulation with heparin or
enoxaparin is recommended prior to cardioversion.
Body habitus and urgency can be used to guide shock energy. An obese patient with a large anteroposterior diameter will
probably require higher energy (ie, 360 J monophasic). A thinner person may require lower energy (200 J). Required energies
are always lower with biphasic waveforms (100-200 J).
Two sets of patches can be used to successfully cardiovert patients in whom a single maximal shock with 1 set of patches fails.
Two external defibrillators and 2 sets of defibrillation patches are required. Vectors are crossed so that 1 set of patches is
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
8 of 41 6/13/2010 6:30 PM

placed anteriorly left of the sternum and posteriorly right of the spine. The second set of patches is placed anteriorly right of the
sternum and posteriorly left of the spine. The 2 defibrillators may be activated simultaneously, in synchronized fashion, or with a
slight delay after the first discharge. This method may succeed when a single set of patches fails.
Internal cardioversion is also possible but must be performed in the electrophysiologic laboratory. Intracardiac catheters can be
positioned in the right atrium and in the coronary sinus. Synchronized shocks are then delivered between the 2 catheters, with
energies from 1-100 J. Alternatively, a defibrillating current may be passed between a single intracardiac catheter (right atrium,
coronary sinus) and a single cutaneous patch placed anteriorly or posteriorly.
In patients with an implantable cardioverter-defibrillator, device-delivered shock, synchronized to the QRS complex, may be
used to attempt cardioversion of atrial fibrillation. Rarely, external cardioversion of patients with an implanted device can result in
device damage, and device function should generally be re-evaluated following external cardioversion.
Chemical cardioversion
Hemodynamically stable patients with atrial fibrillation can be converted to sinus rhythm using oral or intravenous agents. Oral
dosing of Class Ic agents [flecainide (300 mg) or propafenone (450-600 mg)] has been shown to be efficacious in patients with
atrial fibrillation of shorter duration (<7 d).[11 ]
These drugs require monitoring for side-effects (ie, ventricular tachycardia and
heart failure). Coadministration of an AV-nodal blocking agent (ie, beta-blocker or nondihydropyridine calcium channel blocker)
is generally recommended to prevent conversion to atrial flutter with rapid ventricular response.
While inpatient loading of Class Ic agents is not required for those without structural heart disease, it is frequently practiced. Use
of flecainide and propafenone is contraindicated in patients with structural heart disease (left ventricular hypertrophy or prior
myocardial infarction), baseline QRS or QT prolongation (QTc longer than 460 ms) or in those receiving concomitant
antiarrhythmic therapy.
Intravenous procainamide (Class Ia, <18 mg/kg/h) or ibutilide (Class III, 1 mg over 15 m) may also be used for chemical
cardioversion of atrial fibrillation or to increase likelihood of successful electrical cardioversion. Both of these agents should only
be used in a highly monitored, inpatient setting. These drugs predispose to ventricular tachycardia and they should not be used
in those with significant structural heart disease, QT prolongation, or electrolyte abnormalities. Some clinicians preadminister
magnesium to attempt to reduce the risk of ventricular tachycardia. Frequent monitoring of blood pressure, heart rate, and
telemetry are advised.
Oral dosing of other Class III agents (dofetilide, amiodarone) may also be used for chemical cardioversion or to increase the
likelihood of successful electrical cardioversion. Sotalol is not generally recommended for chemical cardioversion. Amiodarone
can be initiated as outpatient therapy in the appropriate clinical context (in patients without structural heart disease or other
comorbidities). Initiation of dofetilide must be performed as inpatient therapy with a specified dose adjustment nomogram,
including age, renal function, and changes in QT interval. Amiodarone and dofetilide are efficacious in patients with structural
heart disease, including those with prior myocardial infarction or heart failure. Monitoring for bradycardia, electrolyte
disturbances, and QT prolongation is strongly recommended.
Staging
Several classification schemas have been proposed for the study of atrial fibrillation, but none fully accounts for all aspects of atrial
fibrillation. A number of different labels and nomenclature have been used to describe patterns of atrial fibrillation, including acute,
chronic, paroxysmal, intermittent, and permanent. The vagaries of each of these definitions make comparing the results of studies
assessing the magnitude and treatment of atrial fibrillation difficult.
Published guidelines from expert committees of the American College of Cardiology/American Heart Association and European
Society of Cardiology on the treatment of patients with atrial fibrillation suggest that atrial fibrillation be classified into 3 patterns (see
Media file 2). These include a first detectable episode, irrespective of whether it is symptomatic or self-limited, also recognizing that
there may be some uncertainty about the duration of the episode and any prior undetected episodes. Recurrent atrial fibrillation is
considered to be present when a patient has 2 or more episodes of atrial fibrillation. If atrial fibrillation terminates spontaneously, then
recurrent atrial fibrillation is designated as paroxysmal; if this arrhythmia becomes sustained, then atrial fibrillation is considered
persistent (irrespective of whether atrial fibrillation is terminated with pharmacologic therapy or electrical cardioversion).
Persistent atrial fibrillation may be either the first presentation of atrial fibrillation or the result of recurrent episodes of paroxysmal atrial
fibrillation. Patients with persistent atrial fibrillation also include patients with long-standing atrial fibrillation in whom cardioversion has not
been indicated or attempted, often leading to permanent atrial fibrillation. Permanent atrial fibrillation is recognized as the accepted
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
9 of 41 6/13/2010 6:30 PM

rhythm, and the main treatment goals are rate control and anticoagulation. While it is possible to reverse the progression from
paroxysmal to persistent and to permanent, this task can be challenging.
Classification scheme for patients with atrial fibrillation.
This classification schema pertains to cases that are not related to a reversible cause of atrial fibrillation (eg, thyrotoxicosis, electrolyte
abnormalities, acute ethanol intoxication). The occurrence of atrial fibrillation secondary to acute myocardial infarction, cardiac surgery,
pericarditis, pulmonary embolism, or acute pulmonary disease is considered separately because, in these situations, atrial fibrillation is
less likely to recur once the precipitating condition has been resolved and adequately treated.
Some patients with paroxysmal atrial fibrillation, typically younger patients, have been found to have distinct electrically active foci
within their pulmonary veins. These patients generally have many atrial premature beats noted on Holter monitoring. Isolation or
elimination of these foci can lead to elimination of the trigger for paroxysms of atrial fibrillation.
Patients can also have atrial fibrillation as a secondary arrhythmia associated with cardiac disease that affects the atria (eg,
congestive heart failure, hypertensive heart disease, rheumatic heart disease, coronary artery disease). These patients tend to be
older, and atrial fibrillation is more likely to be chronic. Paroxysmal atrial fibrillation may progress to permanent atrial fibrillation, and
aggressive attempts to restore and maintain sinus rhythm may prevent comorbidities associated with atrial fibrillation.
Persistent atrial fibrillation with an uncontrolled, rapid ventricular heart rate response can cause a dilated cardiomyopathy and can
lead to electrical remodeling in the atria (atrial cardiomyopathy). Therapy, such as drugs or atrioventricular nodal ablation and
permanent pacemaker implantation, to control the ventricular rate can improve left ventricular function and improve quality-of-life
scores.
New developments aimed at curing atrial fibrillation are being actively explored. By reducing the critical mass required to sustain
atrial fibrillation with either surgical or catheter-based compartmentalization of the atria (ie, MAZE procedure), fibrillatory wavelets
collide with fixed anatomic obstacles, such as suture lines or complete lines of ablation, thus eliminating or reducing the chance of
chronic atrial fibrillation. Some patients with focal origins of their atrial fibrillation also may be candidates for catheter ablation. Still,
much remains to be accomplished before either of these procedures is appropriate for primary treatment.
Treatment
Medical Care
Management of new-onset atrial fibrillation differs from that of long-term atrial fibrillation.
Management of New-Onset Atrial Fibrillation
The management of atrial fibrillation can be broken down into management of new-onset and long-standing atrial fibrillation. The
cornerstones of new-onset atrial fibrillation management are rate control and anticoagulation.[12 ]
The clinical decision to use a rhythm
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
10 of 41 6/13/2010 6:30 PM

control or rate control strategy requires integration of several factors, including degree of symptoms, likelihood of successful
cardioversion and presence of comorbidities. Anticoagulation is an important consideration in both new onset and long-standing atrial
fibrillation. See Media file 3.
Patient management for newly diagnosed atrial fibrillation. Subtherapeutic INR: INR <2 for 3 consecutive
weeks. Warfarin: INR target 2-3. TEE/cardioversion: low molecular weight heparin 1 mg/kg bid as a bridge
with initiation of warfarin INR 2-3.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
11 of 41 6/13/2010 6:30 PM

Restoration of sinus rhythm with regularization of the heart's rhythm improves cardiac hemodynamics and exercise tolerance. By
maintaining the atrial contribution to cardiac output, symptoms of heart failure and overall quality of life can improve. As atrial fibrillation
contributes to pathologic atrial and ventricular remodeling, restoration of sinus rhythm can slow and, in some cases, reverse atrial
dilatation and left ventricular dysfunction. For these reasons, most clinicians focus initially on maintenance of sinus rhythm and opt for a
rate control strategy only when rhythm control fails.
However, several randomized controlled trials have demonstrated that a strategy aimed at restoring (and maintaining) sinus rhythm
neither improves the survival rate nor reduces the risk of stroke in patients with atrial fibrillation.
In the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study,[13 ]
4060 subjects aged 65 years or older
whose atrial fibrillation was likely to be recurrent and who were at risk for stroke were randomized to a strategy of rhythm control
(cardioversion to sinus rhythm plus drugs to maintain sinus rhythm) versus a strategy of rate control (in which no attempt was made to
restore or maintain normal sinus rhythm). An insignificant trend toward increased mortality was noted in the rate control group, and,
importantly, no evidence suggested that the rhythm control strategy protected patients from stroke. Clinically silent recurrences of
atrial fibrillation in the rhythm control group are theorized to be responsible for the increased rates of thromboembolic events and
mortality noted in this cohort. This underscores the importance of anticoagulation in both rhythm control and rate control patients.
The AFFIRM study (and similar findings from the smaller Rate Control Versus Electrical Cardioversion [RACE] trial[14 ]
) has led to
the development of consensus guidelines that recommend an initial rate-control strategy for many asymptomatic patients with atrial
fibrillation. The ACC/AHA/ESC 2006 guidelines state that an initial rate control strategy is "reasonable" for asymptomatic or minimally
symptomatic older patients with hypertension and comorbid cardiovascular disease.[3 ]These same guidelines state that for younger
individuals, especially those without significant comorbid cardiovascular disease, an initial rhythm control strategy may be a better
approach.
Rate control
Regardless of long-term strategy chosen, control of ventricular rate is a critical component of management of new-onset atrial
fibrillation. The main determinants of the ventricular rate during atrial fibrillation are those intrinsic and extrinsic factors that influence
atrioventricular (AV) conduction. Foremost among these are the intrinsic AV nodal conduction properties. Underlying sympathetic
and parasympathetic tone also influences AV nodal conduction. Rate-controlling agents primarily act by increasing AV nodal
refractoriness.
Beta-blockers and calcium channel blockers are first-line agents for rate control in atrial fibrillation. These drugs can be
administered either intravenously or orally. They are effective at rest and with exertion. Caution should be exercised in
patients with reactive airway disease who are given beta-blockers.
Digoxin is sometimes used in the acute setting but does little to control the ventricular rate in active patients. As such, it is
rarely used as monotherapy. The therapeutic window for digoxin as monotherapy for rate control is narrow and would typically
yield toxic levels. Thus, there may be circumstances that this drug is used as adjunctive therapy to beta-blockers or calcium
channel blockers. Caution should be exercised in elderly patients and those with renal failure receiving digoxin. Digoxin is
indicated in patients with heart failure and reduced LV function.
Amiodarone has a Class IIa recommendation from the ACC/AHA/ESC for use as a rate controlling agent for patients who are
intolerant of or unresponsive to other agents. Caution should be exercised in those not receiving anticoagulation as
amiodarone can promote cardioversion.
Anticoagulation
Atrial fibrillation is recognized as a powerful risk factor for stroke. One of the most important considerations in the acute management
of atrial fibrillation is the need for anticoagulation. Acute cardioversion for atrial fibrillation carries a risk of thromboembolism unless
anticoagulation therapy is initiated prior to the procedure and continued post-procedure. Risk of thromboembolism in patients
undergoing either pharmacologic or electrical cardioversion is similar. The risk of thromboembolic events is greatest when atrial
fibrillation has been present for longer than 48 hours.
Effective anticoagulation in patients with atrial fibrillation reduces the risk of stroke 3-fold. Patients with newly diagnosed atrial
fibrillation and patients awaiting electrical cardioversion can be started on intravenous heparin (activated partial thromboplastin time
[aPTT] of 45-60 s) or low molecular weight heparin (1 mg/kg bid).
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
12 of 41 6/13/2010 6:30 PM

Patients can be concomitantly started on warfarin in an inpatient setting while awaiting a therapeutic INR value (2-3). Many practices
have developed specialized anticoagulation clinics to closely monitor INR values.
Oral direct thrombin inhibitors may represent an alternative to warfarin in a higher-risk population with nonvalvular atrial fibrillation, but
no agents in this class are currently approved in the United States.
In the highest-risk population (eg, atrial fibrillation with valvular heart disease or prior embolic cerebrovascular accident) bridging
anticoagulation with heparins may be required in the periprocedural period.
Cardioversion
Cardioversion may be performed electively or emergently to restore sinus rhythm in patients with new-onset atrial fibrillation.
Cardioversion is most successful when initiated within 7 days after to onset of atrial fibrillation. The need for cardioversion may be
acute when atrial fibrillation is responsible for hypotension, heart failure, or angina.
Pharmacologic agents or direct current energy can be used to cardiovert patients with atrial fibrillation. Pharmacologic cardioversion
has the advantage of not requiring sedation or anesthesia, but the major disadvantage is the risk of ventricular tachycardia and other
serious arrhythmias.
Long-Term Management of Atrial Fibrillation
Long-term management of atrial fibrillation is focused on reducing the likelihood of atrial fibrillation recurrence, reducing atrial
fibrillation-related symptoms, control of ventricular rate, and reducing stroke risk. As discussed previously, atrial fibrillation often
results from exposure to established cardiovascular risk factors. Appropriate management of these risk factors will reduce the
likelihood of future atrial fibrillation and atrial fibrillation—related morbidity and mortality. Anticoagulation should be initiated for all
individuals with atrial fibrillation with either aspirin or warfarin except those with "lone" atrial fibrillation or contraindications. Selection of
the appropriate antithrombotic drug should be based on the risk of stroke and bleeding for a given patient. Antiarrhythmic therapy
can aid in maintenance of sinus rhythm in certain patients but requires close monitoring.
Decision-making with regard to the optimal long-term strategy for atrial fibrillation management should be based on a thorough
integration of patient-specific factors and likelihood of success. As a rule, younger patients with more severe symptoms and fewer
comorbidities tend to derive a greater benefit from a long-term focus on rhythm control. Older patients with structural heart disease
(ie, left ventricular hypertrophy, prior myocardial infarction, depressed ejection fraction, or atrial dilation) are less likely to remain in
sinus and are more likely to have serious side-effects from antiarrhythmic drugs. In this cohort, most clinicians focus on long-term
rhythm control.
Atrial fibrillation causes electrophysiologic and structural remodeling which, in turn, promotes future atrial fibrillation ("atrial fibrillation
begets atrial fibrillation"). As such, many patients with paroxysmal atrial fibrillation will progress to persistent and permanent atrial
fibrillation. The degree to which this reflects the continuing influence of underlying cardiovascular risk factors as opposed to a direct
effect of atrial fibrillation is unknown. Regardless, clinicians frequently need to reevaluate their management strategies as atrial
fibrillation burden and comorbidities increase with time.
Anticoagulation
The goal of long-term anticoagulation in atrial fibrillation is to reduce the risk of thromboembolism.
Patients in atrial fibrillation have a risk of stroke or peripheral embolism that is approximately 5 times that of people in sinus
rhythm.
Recommendations for anticoagulation for patients with nonvalvular atrial fibrillation are based on a 2006 ACC/AHA/ESC task
force on the management of patients with atrial fibrillation.[8 ]
A study by van Walraven et al determined that as patients with atrial fibrillation age, the relative efficacy of oral anticoagulation does
not decrease, whereas the efficacy of antiplatelet therapy does appear to decrease as a patient ages.[15 ]
Rate control
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
13 of 41 6/13/2010 6:30 PM

As discussed previously, several trials have validated the noninferiority of an initial rate-control strategy. Many clinicians believe,
however, that an attempt at a rhythm control strategy should be made in most patients. Older patients with comorbid cardiovascular
disease have a lower likelihood of successful long-term rhythm control and thus these patients are often managed using a
rate-control strategy. Some patients initially managed with a rhythm control strategy will experience progression to recurrent or
persistent atrial fibrillation. Clinicians often switch to a rate control strategy as the atrial fibrillation burden increases.
AV nodal blocking medications are the cornerstone of rate control in long-standing atrial fibrillation. In the absence of an
accessory pathway, oral beta-blockers, nondihydropyridine calcium channel blockers, and digoxin are effective. Generally,
coadministration of beta-blockers and calcium channel blockers is reserved for patients in whom adequate rate control
cannot be achieved using a single agent.
Digoxin can be used in sedentary patients (especially in those with heart failure) but requires close monitoring of drug levels
and renal function.
In the presence of tachycardia-mediated cardiomyopathy or inadequate ventricular rate control despite drug therapy, AV
nodal ablation and pacemaker implantation can be considered.
Combinations of rate control medications (eg, beta-blocker and digoxin) may be superior to individual agents in some
patients.
Amiodarone may contribute to ventricular rate control. On the other hand, antiarrhythmia agents may organize atrial fibrillation
of a slower atrial flutter that can then conduct 1:1 from atrium to ventricle. Particularly with class Ic agents, maintenance of
effective AV nodal rate control is essential in most patients.
Every effort should be made to assess effectiveness of rate control both at rest and with exertion, especially in those patients who
primarily experience exertional atrial fibrillation-related symptoms. Twenty-four hour Holter monitoring or exercise-treadmill testing
can be helpful in evaluating heart rate variability. Adequate rate control can be defined as a heart rate of 60-80 bpm at rest and
90-115 bpm with moderate exercise.
Rhythm control
Maintenance of sinus rhythm requires treatment of cardiovascular risk factors and any underlying disorder (ie, hyperthyroidism) that
may have triggered atrial fibrillation. As discussed previously, several antiarrhythmic drugs (flecainide, propafenone, dofetilide,
amiodarone) have established efficacy in the pharmacologic conversion of atrial fibrillation to sinus rhythm.
A study by Doyle and Ho determined that amiodarone, as a part of a strategy to achieve sinus rhythm, appears safe and effective in
patients with persistent atrial fibrillation. However, intolerable adverse effects were more common in amiodarone than placebo or
rate control drug.[16 ]
Several distinct agents, most notably sotalol, dofetilide, and dronedarone, are used for the long-term maintenance of sinus rhythm.
Sotalol is efficacious but, like other Class III drugs, requires close monitoring of the QT interval and serum electrolytes. Unlike
dofetilide and amiodarone, sotalol is contraindicated in patients with structural heart disease and heart failure. Dofetilide is
efficacious in maintaining sinus rhythm but requires admission to a hospital in a monitored setting for initiation. The drug is renally
cleared and dosing is based on glomerular filtration rate. Dronedarone has recently gained approval for the maintenance of sinus
rhythm, but its efficacy is below that of amiodarone. While safer (ie, no negative effects on thyroid, pulmonary, or liver function), it is
contraindicated in patients with Class IV heart failure and recently decompensated Class II and Class III heart failure.
Catheter ablation is an alternative to pharmacologic therapy to prevent recurrent atrial fibrillation in symptomatic patients.[17 ]
Catheter
ablation is currently being performed in select centers for paroxysmal and persistent atrial fibrillation and has become a second line
of therapy after drug failure or drug intolerance. Surgical ablation of atrial fibrillation is also an option for patients with atrial fibrillation,
especially those undergoing other cardiac surgery and in those patients in whom pharmacologic and catheter-based procedures are
ineffective or contraindicated. Atrial fibrillation ablation may be superior to AV nodal ablation and biventricular pacing in heart failure
patients but is technically difficult and demanding, and the widespread applicability of ablation in this population of patients is
uncertain.
New medical and device-based rhythm control therapies are being actively explored. Experimental and clinical data suggest that
renin-angiotensin system (RAS) antagonists and HMG-CoA-Reductase Inhibitors (statins) may decrease the incidence of atrial
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
14 of 41 6/13/2010 6:30 PM

fibrillation and increase the likelihood of successful cardioversion.[18,19,20,21 ]
Device-based therapies under research include single-
and dual-site atrial pacemakers to prevent atrial fibrillation and atrial defibrillators to rapidly restore sinus rhythm. Invasive (surgical
and catheter-based) therapies to compartmentalize the atria and localize focal triggers (in the pulmonary veins) are being evaluated
and refined. (See Surgical Care.)
Special considerations
Postoperative atrial fibrillation is common (20-30%) and perioperative beta-blockers are recommended in all patients undergoing
cardiac surgery unless contraindicated.[22 ]
Preoperative administration of amiodarone and sotalol may reduce the incidence of atrial
fibrillation in patients undergoing cardiac surgery. As such, these agents may be used as prophylactic therapy in those at high risk for
postoperative atrial fibrillation. Unless a preoperative diagnosis, most postoperative atrial fibrillation is the result of tissue irritation
and will have resolved by the sixth postoperative week.
Retrospective data suggest that atrial-based pacing (AAI, DDD modes) reduces the risk of developing atrial fibrillation and increases
the interval between episodes in patients with sick sinus syndrome.[23 ]
Surgical Care
Since its inception, surgical compartmentalization of the atria, or the MAZE procedure, has evolved as an exciting procedure with a
potential to cure atrial fibrillation. Quite simply, the atria are transected and resutured to reduce the critical mass required for the
maintenance of atrial fibrillation. Early experience shows that atrial transport is restored postoperatively and that long-term
anticoagulation is not required. The downside remains the need for an open chest procedure; however, thoracoscopic procedures may
reduce hospitalization and recovery times in the future. The surgical MAZE procedure remains an attractive procedure for patients with
atrial fibrillation who are undergoing concomitant mitral valve procedures. Its role as a primary therapy for atrial fibrillation is doubtful.
Catheter ablation has taken the following 3 paths in the attempt to cure or manage atrial fibrillation. Despite classification of their atrial
fibrillation (paroxysmal, persistent, permanent) patients undergoing catheter ablation have been shown to have less atrial fibrillation than
control groups treated with antiarrhythmic agents.[24,25,26 ]
Compartmentalization of the atria with continuous ablation lines of block
Parallel to the surgical MAZE procedure, electrophysiologists attempt to recreate surgical suture lines with
radiofrequency lesions.
The procedures tend to last many hours, and the success rates are somewhat disappointing (50-60%), with left atrial
reentrant tachycardias and left atrial flutters appearing (requiring further ablation procedures).[27 ]
This approach is
typically used for patients with more persistent atrial fibrillation.
Researchers are unsure which areas of the atria are necessary to sustain atrial fibrillation. Purely right-sided lesions are
not sufficient to eliminate atrial fibrillation, making left atrial procedures necessary. In addition, gaps in linear lesions can
be difficult to find.
Research currently focuses on catheter design to deliver linear continuous lesions. Additionally, alternative energy
sources (ie, cooled radiofrequency, lesion cessation by freezing tissue, LASER, ultrasound) may improve one's ability to
deliver transmural lesions in the left atrium.
Catheter ablation of focal triggers of atrial fibrillation
In some patients, atrial fibrillation seems to be triggered by electrically active pulmonary vein foci. These foci can trigger
the atria to fibrillate.[28 ]
Patients typically have an abundance of ectopic atrial beats noted on 24-hour Holter monitoring. Electrical isolation of
individual pulmonary veins, and thus the ectopic foci, is performed successfully at many centers, and patient selection is
key to success. A combined procedure including individual pulmonary vein isolation, as well as left atrial antrum ablation
(ie, encircling pulmonary vein pairs, sometimes connecting right and left pairs along the left atrial roof, and connection to
the mitral valve annulus) is required. The use of chest CT or MRI can be used to recreate 3-dimensional anatomy in the
left atrium, thus aiding in mapping and creating contiguous lines in the left atrium.
Complications are generally in the 3-5% range and include pulmonary vein stenosis (that can be symptomatic),
perforation, thromboembolism, and tamponade. Still, cure rates as high as 70-80% have been reported in properly
selected patients (patients with frequent atrial premature beats and episodes of paroxysmal atrial fibrillation).
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
15 of 41 6/13/2010 6:30 PM

Atrioventricular node ablation and insertion of a permanent pacemaker
AV node ablation may represent an alternative in patients with chronic atrial fibrillation and an uncontrolled ventricular
response despite aggressive medical therapy.
Catheter ablation of the AV junction permanently interrupts conduction from the atria to the ventricles.
Because the result is permanent AV block, a permanent pacemaker is required. atrial fibrillation may still exist, but the
pacemaker governs the ventricular response.
The risk of thromboembolism is unchanged, and patients still require anticoagulation; however, most patients are
relieved of their symptoms.
During the first 1-3 months, the pacing rate must be programmed in the 80- to 90-beat range to prevent TdP, which has
been reported in the literature, presumably due to slow ventricular rates and the occurrence of early after-depolarizations.
In patients with significant ventricular dysfunction and permanent ventricular pacing, a biventricular device may be
appropriate.[29 ]
Improvements in LV size and function, functional class, and quality-of-life scores have been demonstrated.[30 ]
Percutaneous closure of the left atrial appendage.
Embolic stroke in patients with nonvalvular atrial fibrillation (AF) is thought to be associated with left atrial appendage
(LAA) thrombi. Holmes and colleagues compared the efficacy and safety of percutaneous closure of the left atrial
appendage versus warfarin therapy in patients with atrial fibrillation.[31 ]
Eligible patients (n=707) were randomly assigned
in a 2:1 ratio to LAA percutaneous closure and discontinuation of current warfarin (intervention; n=463) or to warfarin
treatment (control; n=244). Follow-up at the point of 1065 patient-years showed the intervention group event rate was 3
per 100 patient-years compared with the control group of 4.9 per 100 patient-years. Probability of noninferiority of the
intervention was greater than 99.9%. Although a higher rate for adverse safety events was observed in the intervention
group, LAA may be a suitable alternative to chronic warfarin therapy for stroke prophylaxis in patients with nonvalvular
atrial fibrillation.
Roux et al studied whether empiric therapy with antiarrhythmic drugs (AAD) following atrial fibrillation (AF) ablation would decrease the
incidence of atrial arrhythmias that commonly occur following ablative therapy. Patients undergoing AF ablation were randomized to
receive empiric AAD therapy or no AAD therapy for the initial 6 weeks after ablation. Measured outcomes included atrial arrhythmias
lasting more than 24 hours; atrial arrhythmias associated with severe symptoms that required hospitalization, cardioversion, or
initiation/change of antiarrhythmic drug therapy; and intolerance to antiarrhythmic agent requiring drug cessation. Results showed AAD
treatment after AF ablation was well tolerated and reduced the incidence of clinically significant atrial arrhythmias and the need for
cardioversion or hospital admission.[32 ]
Consultations
Consultation with a cardiac electrophysiologist or knowledgeable clinician is recommended prior to antiarrhythmic drug initiation.
Diet
Diet restrictions, if any, are as appropriate for the underlying heart disease and any other comorbidities (eg, diabetes mellitus).
Medication
The goals of medical therapy for patients with atrial fibrillation are to maintain sinus rhythm, avoid the risk of complications (eg, stroke),
and minimize symptoms. Warfarin represents the cornerstone of anticoagulant therapy for patients at moderate to high-risk of
thromboembolic events.
Some patients may not be able to take anticoagulants because of contraindications or comorbidities. The ACTIVE trial studied 7554
patients with atrial fibrillation with the intent to determine if adding clopidogrel to aspirin therapy would reduce the risk for acute vascular
events (ie, stroke, myocardial infarction, non-CNS systemic embolism, or death from vascular event) in patients unable to take warfarin.
Addition of clopidogrel to aspirin reduced the risk of major vascular events (P=0.01), especially stroke (P=0.001), compared with
placebo and aspirin. Increased risk for major hemorrhage was more prevalent in the clopidogrel plus aspirin group than the placebo
and aspirin group.[33 ]
The goal of antiarrhythmic drug therapy is to reduce the duration and frequency of atrial fibrillation episodes, thus improving patient
quality of life and reducing symptoms.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
16 of 41 6/13/2010 6:30 PM

Several antiarrhythmic drugs are commonly used to prevent atrial fibrillation recurrence. Currently, the FDA has approved 6
antiarrhythmic drugs (quinidine, flecainide, propafenone, sotalol, dofetilide, dronedarone) for the treatment of atrial fibrillation. Other
antiarrhythmic agents (eg, amiodarone) are used in an off-label fashion with great clinical efficacy. Use of antiarrhythmic drugs requires
caution because they can also be proarrhythmic. These agents can exacerbate pre-existing arrhythmias and generate arrhythmia de
novo. Tachy- and brady-arrhythmias generated by these agents can be of ventricular or atrial origin. Drug-drug interactions and extra-
cardiac side effects are common. Consultation with a cardiac electrophysiologist or knowledgeable clinician is recommended prior to
antiarrhythmic drug initiation.
If maintenance of sinus rhythm is the goal, the ACA/AHA/ECC have jointly developed guidelines for the long-term antiarrhythmic
treatment in the maintenance of sinus rhythm.[3 ]The following algorithm incorporates clinical trial data on the safety and efficacy of
antiarrhythmic agents. These guidelines are intended to help clinicians tailor antiarrhythmic therapy on an individual basis for their
patients.
For patients with no evidence of structural heart disease, flecainide, propafenone, sotalol, dronedarone, or dofetilide should be
considered first-line agents. Amiodarone can be considered as alternative agents. For patients with substantial left ventricular
hypertrophy (LVH), amiodarone is considered a reasonable first-line agent. For patients with coronary artery disease, dofetilide or
sotalol are first-line therapy. Amiodarone is considered a second-line agent in this population. For patients with heart failure,
amiodarone or dofetilide are first-line agents. Dronedarone should not be used in patients with Class IV heart failure or in Class II-III
patients with recent heart failure exacerbations. See Media file 4.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
17 of 41 6/13/2010 6:30 PM

Antiarrhythmic drug algorithm for the medical management of sinus rhythm in patients with atrial fibrillation.
Current practice constraints mandate that clinicians carefully consider patient populations at low and acceptable risks for outpatient
antiarrhythmic drug initiation. Proarrhythmia is the most common adverse effect of antiarrhythmics during the loading phase. While the
proarrhythmic effect of these drugs extends into the maintenance phase, inpatient drug initiation is generally recommended in the
monitored inpatient setting, especially for those patients with structural heart disease or substantial comorbidities. Nevertheless, certain
antiarrhythmic drugs have established and acceptable safety profiles when used in outpatients without structural heart disease or other
risk factors.
Atrioventricular nodal conduction blockers
Used to slow ventricular response by slowing AV nodal conduction during atrial fibrillation or atrial flutter. Also indicated for use in
conjunction with class IA and IC antiarrhythmics, which slow atrial fibrillation/flutter rate and may cause more rapid ventricular response.
Esmolol (Brevibloc)
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
18 of 41 6/13/2010 6:30 PM

Ultra–short-acting. Selectively blocks beta1-receptors with little or no effect on beta2-receptor types. Particularly useful in patients with
elevated arterial pressure, especially if surgery is planned. Shown to reduce episodes of chest pain and clinical cardiac events
compared with placebo. Can be discontinued abruptly if necessary. Useful in patients at risk for experiencing complications from
beta-blockade, particularly those with reactive airway disease, mild-moderate LV dysfunction, and/or peripheral vascular disease. Short
half-life of 8 min allows for titration to desired effect and quick discontinuation if needed.
Dosing
Adult
250-500 mcg/kg/min for 1 min loading dose followed by a 4 min maintenance infusion of 50 mcg/kg/min
If adequate therapeutic effect not observed within 5 min, repeat loading dose and follow with maintenance infusion using increments of
50 mcg/kg/min (for 4 min); sequence may be repeated up to 4 times prn
As the desired heart rate approached, omit loading infusion and reduce incremental dose of maintenance infusion from 50 mcg/kg/min
to 25 mcg/kg/min or lower; interval between titration steps may be increased from 5 min to 10 min if needed
Pediatric
Not established; 100-500 mcg/kg administered over 1 min suggested
Interactions
Aluminum salts, barbiturates, NSAIDs, penicillins, calcium salts, cholestyramine, and rifampin may decrease bioavailability and plasma
levels of esmolol, possibly resulting in decreased pharmacologic effect; cardiotoxicity of esmolol may increase when administered
concurrently with sparfloxacin, astemizole, calcium channel blockers, quinidine, flecainide, and contraceptives; toxicity of esmolol
increases when administered concurrently with digoxin, flecainide, acetaminophen, clonidine, epinephrine, nifedipine, prazosin,
haloperidol, phenothiazines, and catecholamine-depleting agents
Contraindications
Documented hypersensitivity; uncompensated congestive heart failure, bradycardia, cardiogenic shock, and A-V conduction
abnormalities
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Beta-adrenergic blockers may mask signs and symptoms of acute hypoglycemia and clinical signs of hyperthyroidism; symptoms of
hyperthyroidism, including thyroid storm may worsen when medication is abruptly withdrawn; withdraw drug slowly and monitor patient
closely
Propranolol (Inderal)
Class II antiarrhythmic, nonselective, beta-adrenergic receptor blocker with membrane-stabilizing activity that decreases automaticity of
contractions.
Dosing
Adult
1-3 mg (under careful monitoring) IV; not to exceed 1 mg/min IV to avoid lowering blood pressure and causing cardiac standstill
Allow time for drug to reach site of action (particularly if slow circulation); administer second dose after 2 min prn; thereafter, do not
administer additional drug after desired alteration in rate or rhythm achieved; switch to 10-160 mg PO bid
Pediatric
2-4 mg/kg/d PO divided bid (1-2 mg/kg bid)
IV use not recommended; however, for arrhythmias, 0.01-0.1 mg/kg, not to exceed 1 mg/dose, by slow push has been recommended;
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
19 of 41 6/13/2010 6:30 PM

change to PO as soon as possible
Interactions
Coadministration with aluminum salts, barbiturates, NSAIDs, penicillins, calcium salts, cholestyramine, and rifampin may decrease
effects; calcium channel blockers, cimetidine, loop diuretics, and MAOIs may increase toxicity; toxicity of hydralazine, haloperidol,
benzodiazepines, and phenothiazines may increase
Contraindications
Documented hypersensitivity; uncompensated CHF; bradycardia, cardiogenic shock; AV conduction abnormalities, reactive airway
disease
Precautions
Pregnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Beta-adrenergic blockade may decrease signs of acute hypoglycemia and hyperthyroidism; abrupt withdrawal may exacerbate
symptoms of hyperthyroidism, including thyroid storm; withdraw drug slowly and monitor patient closely
Atenolol (Tenormin)
Selectively blocks beta-1 receptors with little or no effect on beta-2 types. Esmolol is excellent for use in patients at risk for
experiencing complications from beta-blockade, particularly those with reactive airway disease, mild-to-moderate LV dysfunction,
and/or peripheral vascular disease. Short half-life of 8 min allows for titration to desired effect and quick discontinuation if needed.
Dosing
Adult
Up to 200 mg PO qd
Pediatric
Not established
Interactions
Aluminum salts, barbiturates, NSAIDs, penicillins, calcium salts, cholestyramine, and rifampin may decrease bioavailability and plasma
levels, possibly resulting in decreased pharmacologic effect; cardiotoxicity may increase when administered concurrently with
sparfloxacin, astemizole (recalled from US market), calcium channel blockers, quinidine, flecainide, and contraceptives; toxicity
increases when administered concurrently with digoxin, flecainide, acetaminophen, clonidine, epinephrine, nifedipine, prazosin,
haloperidol, phenothiazines, and catecholamine-depleting agents
Contraindications
Documented hypersensitivity, CHF, pulmonary edema, cardiogenic shock, AV conduction abnormalities, heart block (without a
pacemaker), reactive airway disease
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Beta-adrenergic blockade may reduce symptoms of acute hypoglycemia and mask signs of hyperthyroidism; abrupt withdrawal may
exacerbate symptoms of hyperthyroidism and cause thyroid storm; monitor patients closely and withdraw drug slowly; during IV,
carefully monitor BP, heart rate, and ECG
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
20 of 41 6/13/2010 6:30 PM

Metoprolol (Lopressor)
Selective beta1-adrenergic receptor blocker that decreases automaticity of contractions. During IV administration, carefully monitor
blood pressure, heart rate, and ECG.
Dosing
Adult
5 mg IV for 3 doses q2-5 min; then up to 200 mg PO bid
Pediatric
Not established
Interactions
Aluminum salts, barbiturates, NSAIDs, penicillins, calcium salts, cholestyramine, and rifampin may decrease bioavailability and plasma
levels, possibly resulting in decreased pharmacologic effects; toxicity may increase with coadministration of sparfloxacin,
phenothiazines, astemizole (recalled from US market), calcium channel blockers, quinidine, flecainide, and contraceptives; may
increase toxicity of digoxin, flecainide, clonidine, epinephrine, nifedipine, prazosin, verapamil, and lidocaine
Contraindications
Documented hypersensitivity, uncompensated CHF, bradycardia, asthma, cardiogenic shock, and AV conduction abnormalities,
reactive airway disease
Precautions
Pregnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Beta-adrenergic blockade may reduce signs and symptoms of acute hypoglycemia and may decrease clinical signs of
hyperthyroidism; abrupt withdrawal may exacerbate symptoms of hyperthyroidism, including thyroid storm; monitor patient closely and
withdraw drug slowly; during IV administration, carefully monitor blood pressure, heart rate, and ECG
Digoxin (Lanoxin)
Slows sinus node and AV node via vagomimetic effect and not very effective if sympathetic tone is increased. Generally not
recommended unless depressed LV function is present.
Dosing
Adult
Loading dose: 1.5-2 mg PO/IV in divided dose over 1-2 d
Maintenance dose: 0.25 mg PO/IV qd
Pediatric
Premature neonates: 15-25 mcg/kg PO/IV divided into 3 or more doses (first dose equalling half total dose), then remaining doses
q6-8h; maintenance of 4-6 mcg/kg/d PO/IV divided bid
Neonates: 20-30 mcg/kg PO/IV divided into 3 or more doses (first dose equalling half total dose), then remaining doses q6-8h;
maintenance of 5-8 mcg/kg/d PO/IV divided bid
<2 years: 30-50 mcg/kg PO/IV divided into 3 or more doses (first dose half total dose), then remaining doses q6-8h; maintenance of
7.5-12 mcg/kg/d PO/IV divided bid
2-5 years: 25-35 mcg/kg PO/IV divided into 3 or more doses (first dose equalling half total dose), then remaining doses q6-8h;
maintenance of 6-9 mcg/kg/d PO/IV divided bid
6-10 years: 15-30 mcg/kg PO/IV divided into 3 or more doses (first dose equalling half total dose), then remaining doses q6-8h;
maintenance of 4-8 mcg/kg/d PO/IV divided bid
>10 years: 8-12 mcg/kg PO/IV divided into 3 or more doses, (first dose equalling half total dose), then remaining doses q6-8h;
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
21 of 41 6/13/2010 6:30 PM

maintenance of 2-3 mcg/kg/d PO/IV qd
Interactions
Medications that may increase levels include alprazolam, benzodiazepines, bepridil, captopril, cyclosporine, propafenone,
propantheline, quinidine, diltiazem, aminoglycosides, oral amiodarone, anticholinergics, diphenoxylate, erythromycin, felodipine,
flecainide, hydroxychloroquine, itraconazole, nifedipine, omeprazole, quinine, ibuprofen, indomethacin, esmolol, tetracycline,
tolbutamide, and verapamil
Medications that may decrease serum levels include aminoglutethimide, antihistamines, cholestyramine, neomycin, penicillamine,
aminoglycosides, oral colestipol, hydantoins, hypoglycemic agents, antineoplastic treatment combinations (including carmustine,
bleomycin, methotrexate, cytarabine, doxorubicin, cyclophosphamide, vincristine, and procarbazine), aluminum or magnesium antacids,
rifampin, sucralfate, sulfasalazine, barbiturates, kaolin/pectin, and aminosalicylic acid
Contraindications
Documented hypersensitivity, beriberi heart disease, idiopathic hypertrophic subaortic stenosis, constrictive pericarditis, carotid sinus
syndrome
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Hypokalemia may reduce positive inotropic effect of digitalis; IV calcium may produce arrhythmias in digitalized patients; hypercalcemia
predisposes patient to digitalis toxicity; hypocalcemia can make digoxin ineffective until serum calcium levels are normal; institute
magnesium replacement therapy in patients with hypomagnesemia to prevent digitalis toxicity; patients diagnosed with incomplete AV
block may progress to complete block when treated with digoxin; exercise caution in hypothyroidism, hypoxia, and acute myocarditis
Antiarrhythmics, class IA
Quinidine, procainamide, and disopyramide are IA antiarrhythmic agents used to maintain sinus rhythm. Generally, start administration
in hospital because of high risk of adverse effects. All patients treated with class IA agents should be treated concomitantly with AV
nodal blocking agents. Some patients demonstrate a slowing in atrial rate and an increase in AV conduction with rapid ventricular rates
when treated with IA agents alone. Fading as first-line drugs for atrial fibrillation.
Quinidine (Cardioquin, Quinalan, Quinidex, Quinaglute)
Of Vaughn-Williams class IA agents, only quinidine is FDA-approved for atrial fibrillation. As with all class IA agents, QRS and QTc
prolongation are main ECG manifestations. Should not be used in patients with a prolonged QTc baseline (>460 milliseconds).
Generally has fallen out of favor as a first- or second-line agent for treatment of atrial fibrillation.
Dosing
Adult
300 mg PO q8-12h
324 mg PO q8h of quinidine gluconate formulation
Pediatric
Not established
Interactions
Slows elimination of digoxin and simultaneously reduces volume of distribution, leading to increased serum digoxin level; potentiates
anticoagulant effect of warfarin
Contraindications
Prior thrombocytopenic purpura during quinidine administration; complete heart block, unless a ventricular pacemaker is present, long
QTc at baseline (>460 milliseconds), history of TdP
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
22 of 41 6/13/2010 6:30 PM

Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Renal or hepatic dysfunction causes reduction in elimination half-life of parent drug and/or metabolites; CHF causes a reduction in
apparent volume of distribution; any of these conditions can result in quinidine toxicity if dosage not appropriately reduced; perform
periodic blood counts and liver and kidney tests during long-term therapy; in general, initiate during continuous cardiac monitoring, with
careful attention to the QTc interval
Procainamide (Procanbid, Pronestyl)
Not FDA-approved for treatment of atrial fibrillation; however, many use this agent for acute cardioversion (eg, postoperatively) and
because it can be administered IV. Administered IV, useful for acute conversion and can subsequently be converted to oral dose.
Negative inotropic agent and vasodilator, and care must be taken in administering to patients with reduced LV function. Generally
considered second-line agent.
Dosing
Adult
1000-2500 mg PO q12h (Procanbid formulation) based on body weight and normal renal function; not to exceed 18 mg/kg over 1 h
with initial infusion
Procainamide and N -acetyl procainamide (NAPA) levels should be drawn after steady state reached
Pediatric
Not established
Interactions
Can expect increased levels of procainamide metabolite NAPA (a class III antiarrhythmic agent) in patients taking cimetidine, ranitidine,
beta-blockers, amiodarone, trimethoprim, and quinidine; may increase effect of skeletal muscle relaxants (eg, quinidine, lidocaine) and
neuromuscular blockers; ofloxacin inhibits tubular secretion of procainamide and may increase bioavailability; when taken concurrently
with sparfloxacin, may increase risk of cardiotoxicity
Contraindications
History of complete heart block, unless a ventricular pacemaker present; lupus erythematosus; TdP; long QTc at baseline (>460
milliseconds)
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Agranulocytosis rate of 0.5% with 20-25% mortality; weekly CBC counts recommended for first 3 mo and regularly thereafter
Renal clearance; renal insufficiency may lead to accumulations of high plasma levels and its active metabolite, NAPA
In general, initiate during continuous cardiac monitoring, with careful attention to QTc interval
Disopyramide (Norpace)
Not commonly used to treat atrial fibrillation because it has adverse anticholinergic effects and because it is a strongly negative
inotropic agent, which may precipitate CHF and cardiogenic shock in patients with reduced LV function. May be useful in vagally
mediated syncope.
Dosing
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
23 of 41 6/13/2010 6:30 PM

Adult
150 mg PO q6h
300 mg PO q12h (CR formulation)
Pediatric
<12 years: 6-20 mg/kg/d PO divided q6h
>12 years: Administer as in adults
Interactions
Phenytoin, rifampin, and phenobarbital may decrease effects; toxicity increases with erythromycin and sparfloxacin; levels of digoxin
increase
Contraindications
Documented hypersensitivity; history of complete heart block; sick sinus syndrome, cardiogenic shock; CHF; prolonged baseline QTc
(>460 milliseconds)
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Dose adjustments necessary in liver disease, renal disease, and elderly persons; anticholinergic effects can cause urinary retention
and blurred vision
In general, initiate during continuous cardiac monitoring, with careful attention to QTc interval
Antiarrhythmics, class IC
Indicated for patients with atrial fibrillation and supraventricular tachycardia without structural heart disease. Given the results of the
CAST I and II trials (increased mortality), type IC agents are generally not used in patients with concomitant LV dysfunction and/or
CAD. Applicability of CAST results to other populations (eg, patients without recent MI) is uncertain. Many specialists initiate class IC
antiarrhythmic agents in an outpatient setting for patients with paroxysmal atrial fibrillation and no associated structural heart disease.
Regardless, close patient follow-up is mandated, with frequent ECG monitoring or via transtelephonic monitoring for potential signs of
proarrhythmia.
Propafenone (Rythmol)
Shortens upstroke velocity (phase 0) of monophasic action potential. Reduces fast inward current carried by sodium ions in Purkinje
fibers and, to a lesser extent, myocardial fibers. May increase diastolic excitability threshold and prolong effective refractory period.
Reduces spontaneous automaticity and depresses triggered activity.
Indicated for documented life-threatening ventricular arrhythmias, such as sustained ventricular tachycardia. Appears to be effective in
treatment of supraventricular tachycardias, including atrial fibrillation and flutter. Not recommended in patients with less severe
ventricular arrhythmias, even if symptomatic. Use in conjunction with AV nodal blocking agents when given to patients in atrial fibrillation
because conversion to AFL with 1:1 conduction (producing fast ventricular rates) has been noted.
Dosing
Adult
150-300 mg PO tid
225, 325, 425 mg PO bid (SR formulation)
Pediatric
Not established
Interactions
Rifampin may decrease plasma levels; quinidine may increase pharmacologic effects; may increase plasma levels of beta-blockers,
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
24 of 41 6/13/2010 6:30 PM

cyclosporine, warfarin, and digoxin; CYP4502D6 inhibitors (ritonavir, cimetidine, amiodarone) may increase serum levels and
cardiotoxicity
Contraindications
Documented hypersensitivity, second- or third-degree AV block, right bundle-branch block associated with left hemiblock (bifascicular
block) or trifascicular block; concurrent use of ritonavir or amprenavir
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Caution in preexisting sinus node dysfunction, history of CHF, post MI, myocardial dysfunction, or sick sinus syndrome (exacerbates
sick sinus syndrome and causes sinus pauses or sinus arrest); reserve use for life-threatening arrhythmias only due to deaths
associated with proarrhythmic effects of class IC antiarrhythmics; highly metabolized in liver; considerable percentage of metabolites
(18-35%) excreted in urine; patients with impaired liver and renal function need careful monitoring for excessive pharmacological
effects (adjust dose); rarely, positive ANA titers are reported, are reversible upon cessation of treatment, and may even disappear with
continued therapy
Flecainide (Tambocor)
Blocks sodium and potassium channels, producing dose-related decrease in intracardiac conduction in all parts of heart. Increases
electrical stimulation of threshold of ventricle, His-Purkinje system. Shortens phase 2 and 3 repolarization, resulting in decreased action
potential duration and effective refractory period.
Indicated for treatment of paroxysmal atrial fibrillation/flutter associated with disabling symptoms and paroxysmal supraventricular
tachycardias, including AV nodal reentrant tachycardia, AV reentrant tachycardia, and other supraventricular tachycardias of unspecified
mechanism associated with disabling symptoms in patients without structural heart disease. Also indicated for prevention of
documented life-threatening ventricular arrhythmias (eg, sustained ventricular tachycardia). Not recommended in less severe ventricular
arrhythmias even if patients are symptomatic. Use in conjunction with AV nodal blocking agents when given to patients in atrial
fibrillation because conversion to AFL with 1:1 conduction (producing fast ventricular rates) can occur.
Dosing
Adult
50-150 mg PO bid
Pediatric
Not established
Interactions
May increase toxicity of digoxin; beta-adrenergic blockers, verapamil, and disopyramide may have additive inotropic effects when
coadministered; CYP4502D6 inhibitors (ritonavir, cimetidine, amiodarone) may increase serum levels and cardiotoxicity
Contraindications
Documented hypersensitivity, preexisting second- or third-degree AV block, right bundle-branch block associated with left hemiblock
(bifascicular block) or trifascicular block), unless a pacemaker is present to sustain cardiac rhythm if complete heart block occurs;
concurrent use of ritonavir or amprenavir; recent MI
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Caution in preexisting sinus node dysfunction, history of CHF, post MI, myocardial dysfunction, or sick sinus syndrome (exacerbates
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
25 of 41 6/13/2010 6:30 PM

sick sinus syndrome and causes sinus pauses or sinus arrest); reserve use for life-threatening arrhythmias only due to deaths
associated with proarrhythmic effects of class IC antiarrhythmics; adjust dose in renal or hepatic impairment; known to increase
endocardial pacing thresholds; may suppress ventricular escape rhythms
Antiarrhythmics, class III
Currently, class III antiarrhythmic agents sotalol and dofetilide are FDA-approved for use in treating atrial arrhythmias; however,
amiodarone is also widely used in maintenance of sinus rhythm in patients with atrial fibrillation. Dofetilide must be initiated in an
inpatient setting. Sotalol is also initiated in an inpatient setting.
Amiodarone (Cordarone)
Has antiarrhythmic effects that overlap all 4 Vaughn-Williams antiarrhythmic classes. Has a low risk of proarrhythmia, and any
proarrhythmic reactions generally are delayed. Used in patients with structural heart disease. Most clinicians are comfortable with
inpatient or outpatient loading with 400 mg PO tid for 1 wk because of low proarrhythmic effect, followed by weekly reductions with goal
of lowest dose with desired therapeutic benefit (usual maintenance dose for atrial fibrillation is 200 mg/d). During loading, patients must
be monitored for bradyarrhythmias.
Dosing
Adult
400 mg PO tid for 1 wk, followed by weekly reductions (goal of lowest dose with desired therapeutic benefit)
Maintenance for atrial fibrillation: 200 mg/d
Pediatric
Not established
Interactions
Increases effect and blood levels of theophylline, methotrexate, digoxin, cyclosporine, beta-blockers, and anticoagulants; cardiotoxicity
is increased by ritonavir and sparfloxacin; coadministration with calcium channel blockers may cause an additive effect and may further
decrease myocardial contractility; cimetidine may increase levels
Contraindications
Documented hypersensitivity, complete AV block and intraventricular conduction defects; patients taking ritonavir or sparfloxacin
Precautions
Pregnancy
D - Fetal risk shown in humans; use only if benefits outweigh risk to fetus
Precautions
Pulmonary toxicity has a 3-7% incidence and is dose-related, rare with doses <400 mg/d; gallium scan and lung biopsies confirm
diagnosis; discontinuation with administration of steroids is preferred; assess baseline thyroid, liver, and pulmonary functions; perform
thyroid and liver studies at regular intervals (6 mo); perform yearly chest radiographs, looking for evidence of pulmonary fibrosis;
toxicity and adverse effects are a function of daily dose and duration of therapy, making this drug less desirable in younger populations;
use with extreme caution in patients with severe pulmonary disease (can cause pulmonary fibrosis and death); regular ophthalmologist
examinations due to rare cases of optic neuritis
Sotalol (Betapace atrial fibrillation)
Class III agent with beta-blocking effects. Effective in maintenance of sinus rhythm, even in patients with underlying structural heart
disease. Inpatient loading is FDA-mandated.
Dosing
Adult
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
26 of 41 6/13/2010 6:30 PM

80 mg PO bid initially, with therapeutic goal of 120-160 mg PO bid
Pediatric
Not established
Interactions
Class IA antiarrhythmic agents, disopyramide, quinidine, procainamide; other class III agents (amiodarone) can enhance potassium
channel blocking effect and should not be given concomitantly
Contraindications
Prolonged QTc at baseline (generally >500 milliseconds); history of TdP; reactive airway disease; renal failure; electrolyte
abnormalities
Precautions
Pregnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Risk factors for sotalol-induced TdP (1.5-2%) include impaired renal function (creatinine >1.4), hypokalemia, female sex, slow heart
rates, daily dose >320 mg, history of CHF or VT/VF, and QTc >500-525 milliseconds
Dofetilide (Tikosyn)
Approved by FDA for maintenance of sinus rhythm as well as for the conversion of atrial fibrillation to sinus rhythm (approx 50%) in
patients with persistent atrial fibrillation. Has no effect on cardiac output, cardiac index, stroke volume index, or systemic vascular
resistance in patients with ventricular tachycardia, mild to moderate CHF, angina, and either normal or reduced LVEF. No evidence of
negative inotropic effect.
Dosing
Adult
125, 250, or 500 mcg PO bid; must be started in a monitored inpatient setting for 3 days by certified clinician
Dose determined by creatinine clearance (CrCl) and QTc response to initial doses
Pediatric
Not established
Interactions
Verapamil, TMP-SMZ, ketoconazole, potassium-depleting diuretics, digoxin, cimetidine, phenothiazines, triamterene, metformin,
prochlorperazine, amiloride, megestrol, and other antiarrhythmic agents may increase toxicity
Contraindications
Documented hypersensitivity; CrCl <20 mL/min; QTc >440 milliseconds at baseline and >500 milliseconds after second dose; do not
use in conjunction with trimethoprim (either alone or in combination with sulfamethoxazole), verapamil, ketoconazole, cimetidine,
megestrol, phenothiazines, TCAs, or prochlorperazine
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Tightly regulated and can be prescribed only by clinicians who register with company and have specific training; to minimize risk of
induced arrhythmia, calculations of CrCl and continuous ECG monitoring must be performed; cardiac resuscitation equipment and
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
27 of 41 6/13/2010 6:30 PM

personnel must be present; maintain potassium levels within reference range prior to and during administration
Ibutilide (Corvert)
Indicated for conversion of recent-onset atrial fibrillation or atrial flutter (3 h to 90 d). Prolongs repolarization by increasing slow inward
sodium current and by blocking delayed rectifier current with rapid onset.
Dosing
Adult
>60 kg (132 lb): 1 mg IV infusion over 10 min
<60 kg: 0.01 mg/kg IV over 10 min; second infusion of equal strength can be given 10 min after first prn
Magnesium infusion (2 g MgSO4) has been used to pretreat patients receiving ibutilide to prevent TdP
Pediatric
Not established
Interactions
Increases toxicity of quinidine and procainamide; concurrent administration with TCAs, phenothiazines, and astemizole (recalled from
US market) may prolong QT interval; toxicity of digoxin increases when administered concurrently
Contraindications
Documented hypersensitivity; history of TdP; concurrent use of other QT prolonging agents
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Of 586 patients with recent-onset atrial fibrillation or AFL who received ibutilide, 149 reported medical events related to cardiovascular
system, including sustained polymorphic VT (1.7%) and nonsustained polymorphic VT (2.7%); observe patients with continuous ECG
monitoring for at least 4 h following infusion or until QTc returns to baseline; skilled personnel and proper equipment (defibrillator and
medication for treatment of life-threatening ventricular arrhythmias) must be available during monitoring period
Patients should not be given class IA agents (quinidine, disopyramide, procainamide) or class III drugs (sotalol, amiodarone)
concomitantly with or within 4 h postinfusion because of their potential to prolong refractoriness; potential for proarrhythmia exists with
other drugs that prolong the QT interval (eg, phenothiazines, TCAs, certain antihistamines); risk of TdP higher if ventricular rate or
severely reduced LV function
Antiarrhythmic Agent, Miscellaneous
Dronedarone is an antiarrhythmic agent with properties belonging to all 4 Vaughn-Williams antiarrhythmic classes.
Dronedarone (Multaq)
Blocks sodium channels, blocks beta1-adrenergic site, and alters adenyl cyclase generation (ie, negative inotropic effects); blocks
potassium channels (eg, hERG) and therefore prolongs cardiac repolarization.
In a multinational clinical trial (n >4600), dronedarone reduced cardiovascular hospitalization or death from any cause by 24%
compared with placebo.
Indicated to reduce risk for cardiovascular hospitalization in patients with paroxysmal or persistent atrial fibrillation (AF) or atrial flutter
(AFL), with a recent episode of AF/AFL and associated cardiovascular risk factors (ie, age >70 y, hypertension, diabetes, history of
CVA, LAD >50 mm or LVEF <40%) who are in sinus rhythm or who will be cardioverted.
Dosing
Adult
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
28 of 41 6/13/2010 6:30 PM

400 mg PO bid with meals
Pediatric
Not established
Interactions
CYP3A4 substrate, moderate CYP3A4 and CYP2D6 inhibitor; P-gP inhibitor
Avoid coadministration with CYP3A4 inhibitors (eg, itraconazole, azithromycin, erythromycin, grapefruit juice) that may decrease
clearance and thereby increase dronedarone plasma levels (see Contraindications); avoid use with CYP3A4 inducers (eg, rifampin,
carbamazepine) because of increased clearance and consequent reduction in dronedarone serum levels; use with other drugs that
prolong QT interval (eg, phenothiazine, TCAs, macrolide antibiotics, class I and III antiarrhythmic agents) may cause life-threatening
arrhythmias (see Contraindications)
When coadministered with P-gP substrates (eg, digoxin), P-gP substrate bioavailability may increase (consider discontinuing P-gp
substrate or decrease P-gP substrate dose by 50%)
Coadministration increases serum levels of HMG-CoA reductase inhibitors (eg, atorvastatin), thereby increasing risk for adverse
effects (eg, myopathy); monitor serum levels of CYP3A substrates with narrow therapeutic indexes (eg, sirolimus, tacrolimus) if
coadministered
Coadministration with beta-blockers or calcium channel blockers requires lowered dose of these agents and dose should only be
increased after ECG verification of tolerability
Contraindications
Documented hypersensitivity; severe heart failure (ie, NYHA class IV) or NYHA class II-III with recent decompensation requiring
hospitalization or referral to heart failure program; second- or third-degree heart block or sick sinus syndrome (unless functioning
pacemaker in place); bradycardia <50 bpm; QTc interval >500 milliseconds (coadministration with other drugs that prolong QT interval
may cause torsade de pointes[en dash]type ventricular tachycardia); severe hepatic impairment; strong CYP3A4 inhibitors
Precautions
Pregnancy
X - Contraindicated; benefit does not outweigh risk
Precautions
Boxed warning: May cause critical adverse reactions, including death, in patients with recent severe heart failure
Common adverse reactions include diarrhea, nausea, vomiting, fatigue, and asthenia; discontinue if new or worsening heart failure
develops; monitor QT interval; hypomagnesemia and hypokalemia may increase risk for serious arrhythmic event
Anticoagulants
Used to prevent thromboembolic complications.
Heparin
Augments activity of antithrombin III and prevents conversion of fibrinogen to fibrin. Does not actively lyse but is able to inhibit further
thrombogenesis. Prevents reaccumulation of clot after spontaneous fibrinolysis. Most data related to use of unfractionated heparin.
Low–molecular-weight heparin can also be utilized
Dosing
Adult
60 U/kg IV initially, followed by maintenance infusion of 12 U/kg/h IV; target aPTT is 50-70 seconds
Pediatric
50 U/kg IV initially, followed by a maintenance infusion of 15-25 U/kg/h IV; increase dose by 2-4 U/kg/h q6-8h prn, using aPTT results
Interactions
Digoxin, nicotine, tetracycline, and antihistamines may decrease effects; NSAIDs, ASA, dextran, dipyridamole, and hydroxychloroquine
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
29 of 41 6/13/2010 6:30 PM

may increase toxicity
Contraindications
Documented hypersensitivity, subacute bacterial endocarditis, active bleeding, history of heparin-induced thrombocytopenia
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Bleeding; in neonates, preservative-free heparin is recommended to avoid possible toxicity (gasping syndrome) by benzyl alcohol,
which is used as preservative; caution in severe hypotension and shock
Enoxaparin Sodium (Lovenox)
Low molecular weight heparin. Augments activity of antithrombin III and prevents conversion of fibrinogen to fibrin. Does not actively
lyse but is able to inhibit further thrombogenesis. Prevents reaccumulation of clot after spontaneous fibrinolysis.
Dosing
Adult
1 mg/kg given as a sub cuticular injection bid assuming normal renal function;
kinetics in patients more than 100 kg not well studied
Pediatric
May be used for thromboembolic disorders
In a pilot study, 23 consecutive pediatric patients at an increased risk of bleeding with heparin were treated with subcutaneous
enoxaparin 1 mg/kg q12h with subsequent doses adjusted to achieve a 4-hour anti-factor Xa level between 0.5-1 unit/mL for various
thrombotic diseases. Six of the 7 infants (<2 mo) required (based on anti-factor Xa levels) an average dose of 1.64 mg/kg bid. 3
children required a dose reduction to 0.5 mg/kg bid. Duration of treatment ranged from 10 days or less to more than 60 days.
Thrombotic events were deep vein thrombosis, pulmonary embolism, and thrombotic complication in the CNS. No new thrombotic
events occurred and 2 patients, with previous diagnosed gastrointestinal ulcers, experienced bleeding that required transfusion
Interactions
Digoxin, nicotine, tetracycline, and antihistamines may decrease effects; NSAIDs, aspirin, dextran, dipyridamole, and
hydroxychloroquine may increase toxicity
Contraindications
Active major bleeding, hypersensitivity to enoxaparin, heparin, pork products, benzyl alcohol (multi-dose formulation),
thrombocytopenia associated with a positive test for antiplatelet antibody in the presence of enoxaparin; significant renal dysfunction
Precautions
Pregnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Bacterial endocarditis; increased risk of hemorrhage; bleeding diathesis; concomitant platelet inhibitors; increased risk of hemorrhage;
congenital or acquired bleeding disorders; increased risk of hemorrhage; diabetic retinopathy; elderly patients; potential for delayed
elimination of enoxaparin;
gastrointestinal disease, ulcerative and angiodysplastic, active or recent; increased risk of hemorrhage; hemorrhagic stroke; increased
risk of hemorrhage, heparin-induced thrombocytopenia, history of; use extreme caution; low-weight men (<57 kg) and women (<45 kg);
increased exposure to enoxaparin and increased risk for bleeding; major hemorrhage (including intracranial and retroperitoneal) or
bleeding at any site may occur; investigate any unexplained reduction in hematocrit or blood pressure; recent brain, spinal, or
ophthalmologic surgery (increased risk of hemorrhage); renal impairment; increased exposure to enoxaparin and increased risk for
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
30 of 41 6/13/2010 6:30 PM

bleeding, dosage adjustment recommended in patients with CrCl <30 mL/min; thrombocytopenia may occur, discontinue therapy if
platelet count falls below 100,000/mm; uncontrolled hypertension
Warfarin (Coumadin)
Interferes with hepatic synthesis of vitamin K–dependent coagulation factors. Used for prophylaxis and treatment of venous
thrombosis, pulmonary embolism, and thromboembolic disorders. Tailor dose to maintain INR of 2-3.
Dosing
Adult
1-20 mg/d PO qd, adjust dose to desired INR (2-3) for nonvalvular atrial fibrillation/flutter
Pediatric
0.05-0.34 mg/kg/d PO; adjust dose according to weight and desired INR
Interactions
Drugs that may decrease anticoagulant effects include griseofulvin, carbamazepine, glutethimide, estrogens, nafcillin, phenytoin,
rifampin, barbiturates, cholestyramine, colestipol, vitamin K, spironolactone, oral contraceptives, and sucralfate
Medications that may increase anticoagulant effects include oral antibiotics, phenylbutazone, salicylates, sulfonamides, chloral hydrate,
clofibrate, diazoxide, anabolic steroids, ketoconazole, ethacrynic acid, miconazole, nalidixic acid, sulfonylureas, allopurinol,
chloramphenicol, cimetidine, disulfiram, metronidazole, phenylbutazone, phenytoin, propoxyphene, sulfonamides, gemfibrozil,
acetaminophen, and sulindac
Contraindications
Documented hypersensitivity; severe liver or kidney disease; open wounds or GI ulcers; pregnancy, although AHA/ACC guidelines for
pregnant patients with mechanical valves mention that risk of thrombotic mechanical valve may be higher than risk of teratogenicity from
warfarin
Precautions
Pregnancy
D - Fetal risk shown in humans; use only if benefits outweigh risk to fetus
Precautions
Do not switch brands after achieving therapeutic response; caution in active tuberculosis or diabetes; patients with protein C or S
deficiency are at risk of developing skin necrosis
Follow-up
Further Inpatient Care
Monitor INR values of patients on warfarin (desired range 2-3). Attention to drug-drug interactions (particularly with amiodarone)
is necessary.
Monitor patients on antiarrhythmic agents for signs of proarrhythmia. Worsening liver or renal function can alter antiarrhythmic
drug clearance and may require altered antiarrhythmic drug dosing. Careful monitoring of heart rate, blood pressure, and for
physical signs of congestive heart failure is necessary. The QTc interval is also an important predictor of proarrhythmic events in
patients on type IA and III agents.
Monitor liver function, thyroid function, and lung function in patients treated with amiodarone.
Further Outpatient Care
Assessment and reassessment of thromboembolic risk is necessary.
Periodic ECG monitoring (especially when taking antiarrhythmics) and Holter monitoring are often necessary to assess for
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
31 of 41 6/13/2010 6:30 PM

paroxysmal atrial fibrillation and/or rate control.
Deterrence/Prevention
Experimental and clinical data suggest that renin-angiotensin system (RAS) antagonists and HMG-CoA reductase inhibitors
(statins) may decrease the incidence of atrial fibrillation and increase the likelihood of successful cardioversion.[10,11,12,13 ]
Fish oil preparations have been shown to reduce ventricular arrhythmias in at-risk populations (coronary artery disease) and may
also protect against atrial fibrillation.
Treatment of underlying cardiovascular risk factors such as hypertension, coronary artery disease, valvular heart disease,
obesity, sleep apnea, diabetes, and heart failure is likely to decrease the incidence of atrial fibrillation.
Prognosis
Epidemiologic studies have shown that individuals in sinus rhythm live longer than do individuals with atrial fibrillation. The
AFFIRM trial addressed whether rate control and anticoagulation are sufficient goals for asymptomatic, elderly patients. The
results showed that medical therapies aimed at rhythm control offered no survival advantage over rate control and
anticoagulation.
Atrial fibrillation likely mediates this effect on overall prognosis through its association with thromboembolic events, particularly
stroke.
Development of atrial fibrillation predicts heart failure and is associated with worse NYHA HF class.
Atrial fibrillation may cause tachycardia-mediated cardiomyopathy if adequate rate control is not established. Atrial fibrillation
may also worsen heart failure in individuals who are dependent on the atrial component of the cardiac output. Those with
hypertensive heart disease and those with valvular heart disease are particularly at high risk for developing heart failure when
atrial fibrillation occurs.
Patient Education
For excellent patient education resources, visit eMedicine's Heart Center and Stroke Center. Also, see eMedicine's patient education
articles Atrial Fibrillation, Heart Rhythm Disorders, Stroke, and Supraventricular Tachycardia.
Miscellaneous
Medicolegal Pitfalls
Proper anticoagulation is extremely important in both paroxysmal and persistent atrial fibrillation.
Anticoagulation before and after cardioversion is necessary.
Use of antiarrhythmic agents requires regular, drug-specific follow-up testing.
Special Concerns
Warfarin is contraindicated during pregnancy.
Give special consideration to patients who are noncompliant and patients who are at risk for falling. These patients may be
better off with antiplatelet agents such as aspirin.
Multimedia
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
32 of 41 6/13/2010 6:30 PM

Media file 1: Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves
are not discernible.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
33 of 41 6/13/2010 6:30 PM

Media file 2: Classification scheme for patients with atrial fibrillation.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
34 of 41 6/13/2010 6:30 PM

Media file 3: Patient management for newly diagnosed atrial fibrillation. Subtherapeutic INR: INR <2 for 3
consecutive weeks. Warfarin: INR target 2-3. TEE/cardioversion: low molecular weight heparin 1 mg/kg bid
as a bridge with initiation of warfarin INR 2-3.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
35 of 41 6/13/2010 6:30 PM

Media file 4: Antiarrhythmic drug algorithm for the medical management of sinus rhythm in patients with
atrial fibrillation.
The image on the right is a reconstructed 3-dimen...
Media file 5: The image on the right is a reconstructed 3-dimensional image of the left atrium in a patient
undergoing atrial fibrillation ablation. The figure on the left was created with a mapping catheter using
Endocardial Solutions mapping technology. It represents the endocardial shell of the left atrium and is used as
the template during left atrial ablation procedures.
References
Kannel WB, Wolf PA, Benjamin EJ, et al. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation:
population-based estimates. Am J Cardiol. Oct 16 1998;82(8A):2N-9N. [Medline].
1.
Wolf P, Abbott R, Kannel W. Atrial fibrillation as an independent risk factor for stroke: The Framingham
Study. Stroke. 1999;22:983-988.
2.
Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation:
a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the
3.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
36 of 41 6/13/2010 6:30 PM

European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the
Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the
Heart Rhythm Society. Circulation. Aug 15 2006;114(7):e257-354. [Medline].
Nakao K, Seto S, Ueyama C, et al. Extended distribution of prolonged and fractionated right atrial electrograms predicts
development of chronic atrial fibrillation in patients with idiopathic paroxysmal atrial fibrillation. J Cardiovasc
Electrophysiol. Oct 2002;13(10):996-1002. [Medline].
4.
Akyürek O, Sayin T, Dinçer I, et al. Lengthening of intraatrial conduction time in atrial fibrillation and its relation with early
recurrence of atrial fibrillation. Jpn Heart J. Sep 2001;42(5):575-84. [Medline].
5.
Lloyd-Jones DM, Wang TJ, Leip EP, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart
Study. Circulation. Aug 31 2004;110(9):1042-6. [Medline].
6.
Van Walraven WC, Hart RG, Wells GA, et al. A clinical prediction rule to indentify patients with atrial fibrillation at low risk for
stroke while taking aspirin. arch int med. 2003;163(8):936-943.
7.
Fuster V, Ryden LE, Cannom DS, et al. [ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation--
excutive summary]. Rev Port Cardiol. Apr 2007;26(4):383-446. [Medline].
8.
Fox CS, Parise H, D'Agostino RB Sr, et al. Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring. JAMA. Jun
16 2004;291(23):2851-5. [Medline].
9.
Neal S, Ngarmukos T, Lessard D, et al. Comparison of the efficacy and safety of two biphasic defibrillator waveforms for the
conversion of atrial fibrillation to sinus rhythm. Am J Cardiol. Oct 1 2003;92(7):810-4. [Medline].
10.
Sulke N, Sayers F, Lip G et al. Rhythm control and cardioversion. British Heart Journal. 2007;93:29-34.11.
Zimetbaum P, Reynolds MR, Ho KK, et al. Impact of a practice guideline for patients with atrial fibrillation on medical resource
utilization and costs. Am J Cardiol. Sep 15 2003;92(6):677-81. [Medline].
12.
Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl
J Med. Dec 5 2002;347(23):1825-33. [Medline].
13.
Hagens VE, Ranchor AV, Van Sonderen E, et al. Effect of rate or rhythm control on quality of life in persistent atrial fibrillation.
Results from the Rate Control Versus Electrical Cardioversion (RACE) Study. J Am Coll Cardiol. Jan
21 2004;43(2):241-7. [Medline].
14.
[Best Evidence] van Walraven C, Hart RG, Connolly S, Austin PC, Mant J, Hobbs FD, et al. Effect of age on stroke prevention
therapy in patients with atrial fibrillation: the atrial fibrillation investigators. Stroke. Apr 2009;40(4):1410-6. [Medline].
15.
[Best Evidence] Doyle JF, Ho KM. Benefits and risks of long-term amiodarone therapy for persistent atrial fibrillation: a
meta-analysis. Mayo Clin Proc. Mar 2009;84(3):234-42. [Medline].
16.
Jung W, Wolpert C, Esmailzadeh B, et al. Clinical experience with implantable atrial and combined atrioventricular
defibrillators. J Interv Card Electrophysiol. Jan 2000;4 Suppl 1:185-95. [Medline].
17.
[Best Evidence] Healey JS, Baranchuk A, Crystal E, et al. Prevention of atrial fibrillation with angiotensin-converting enzyme
inhibitors and angiotensin receptor blockers: a meta-analysis. J Am Coll Cardiol. Jun 7 2005;45(11):1832-9. [Medline].
18.
Fauchier L, Pierre B, de Labriolle A, et al. Antiarrhythmic effect of statin therapy and atrial fibrillation a meta-analysis of
randomized controlled trials. J Am Coll Cardiol. Feb 26 2008;51(8):828-35. [Medline].
19.
Vermes E, Tardif JC, Bourassa MG, et al. Enalapril decreases the incidence of atrial fibrillation in patients with left ventricular
dysfunction: insight from the Studies Of Left Ventricular Dysfunction (SOLVD) trials. Circulation. Jun
17 2003;107(23):2926-31. [Medline].
20.
Pedersen OD, Bagger H, Kober L, et al. Trandolapril reduces the incidence of atrial fibrillation after acute myocardial infarction
in patients with left ventricular dysfunction. Circulation. Jul 27 1999;100(4):376-80. [Medline].
21.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
37 of 41 6/13/2010 6:30 PM

Bradley D, Creswell LL, Hogue CW Jr, et al. Pharmacologic prophylaxis: American College of Chest Physicians guidelines for
the prevention and management of postoperative atrial fibrillation after cardiac surgery. Chest. Aug 2005;128(2
Suppl):39S-47S. [Medline].
22.
Anselme F, Saoudi N, Cribier A. Pacing in prevention of atrial fibrillation: the PIPAF studies. J Interv Card
Electrophysiol. Jan 2000;4 Suppl 1:177-84. [Medline].
23.
Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W. Radiofrequency ablation vs antiarrhythmic drugs as
first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. Jun 1 2005;293(21):2634-40. [Medline].
24.
Stabile G, Bertaglia E, Turco P, Zoppo F, Iuliano A, Zerbo F, et al. Role of pulmonary veins isolation in persistent atrial fibrillation
ablation: the pulmonary vein isolation in persistent atrial fibrillation (PIPA) study. Pacing Clin Electrophysiol. Mar 2009;32 Suppl
1:S116-9. [Medline].
25.
Elayi CS, Verma A, Di Biase L, Ching CK, Patel D, Barrett C, et al. Ablation for longstanding permanent atrial fibrillation: results
from a randomized study comparing three different strategies. Heart Rhythm. Dec 2008;5(12):1658-64. [Medline].
26.
Haissaguerre M, Shah DC, Jais P, et al. Electrophysiological breakthroughs from the left atrium to the pulmonary
veins. Circulation. Nov 14 2000;102(20):2463-5. [Medline].
27.
Jais P, Shah DC, Haissaguerre M, et al. Atrial fibrillation: role of arrhythmogenic foci. J Interv Card Electrophysiol. Jan 2000;4
Suppl 1:29-37. [Medline].
28.
Doshi RN, Daoud EG, Fellows C, Turk K, Duran A, Hamdan MH, et al. Left ventricular-based cardiac stimulation post AV nodal
ablation evaluation (the PAVE study). J Cardiovasc Electrophysiol. Nov 2005;16(11):1160-5. [Medline].
29.
Natale A, Zimerman L, Tomassoni G, et al. AV node ablation and pacemaker implantation after withdrawal of effective
rate-control medications for chronic atrial fibrillation: effect on quality of life and exercise performance. Pacing Clin
Electrophysiol. Nov 1999;22(11):1634-9. [Medline].
30.
Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, et al. Percutaneous closure of the left atrial appendage
versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. Aug
15 2009;374(9689):534-42. [Medline].
31.
[Best Evidence] Roux JF, Zado E, Callans DJ, Garcia F, Lin D, Marchlinski FE, et al. Antiarrhythmics After Ablation of Atrial
Fibrillation (5A Study). Circulation. Sep 22 2009;120(12):1036-40. [Medline].
32.
[Best Evidence] ACTIVE Investigators, Connolly SJ, Pogue J, Hart RG, Hohnloser SH, Pfeffer M, et al. Effect of clopidogrel
added to aspirin in patients with atrial fibrillation. N Engl J Med. May 14 2009;360(20):2066-78. [Medline].
33.
A clinical prediction rule to indentify patients with atrial fibrillation at low risk fro srtroke while taking aspirin. arch int
med. 2003;163:936-943.
34.
Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. The effect of low-dose warfarin on the risk of stroke in
patients with nonrheumatic atrial fibrillation. The Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. N Engl J
Med. Nov 29 1990;323(22):1505-11. [Medline].
35.
Chen PS, Athill CA, Wu TJ, et al. Mechanisms of atrial fibrillation and flutter and implications for management. Am J
Cardiol. Nov 4 1999;84(9A):125R-130R. [Medline].
36.
Corley SD, Epstein AE, DiMarco JP, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation
Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. Mar 30 2004;109(12):1509-13. [Medline].
37.
Damiano RJ Jr, Gaynor SL, Bailey M, et al. The long-term outcome of patients with coronary disease and atrial fibrillation
undergoing the Cox maze procedure. J Thorac Cardiovasc Surg. Dec 2003;126(6):2016-21. [Medline].
38.
de Divitiis M, Omran H, Rabahieh R, et al. Right atrial appendage thrombosis in atrial fibrillation: its frequency and its clinical
predictors. Am J Cardiol. Nov 1 1999;84(9):1023-8. [Medline].
39.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
38 of 41 6/13/2010 6:30 PM

Delfaut P, Saksena S. Electrophysiologic assessment in selecting patients for multisite atrial pacing. J Interv Card
Electrophysiol. Jan 2000;4 Suppl 1:81-5. [Medline].
40.
Ducharme A, Swedberg K, Pfeffer MA, et al. Prevention of atrial fibrillation in patients with symptomatic chronic heart failure by
candesartan in the Candesartan in Heart failure: assessment of Reduction in Mortality and morbidity (CHARM) program. Am
Heart J. May 2006;151(5):985-91. [Medline].
41.
Epstein AE, Kay GN. Finding our way through the maze. J Cardiovasc Electrophysiol. Dec 1999;10(12):1575-7. [Medline].42.
Gerstenfeld EP, Callans D, Dixit S, et al. Characteristics of patients undergoing atrial fibrillation ablation: trends over a
seven-year period 1999-2005. J Cardiovasc Electrophysiol. Jan 2007;18(1):23-8.
43.
Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation--Pharmacological Intervention in Atrial Fibrillation
(PIAF): a randomised trial. Lancet. Nov 25 2000;356(9244):1789-94. [Medline].
44.
Klein AL, Grimm RA, Murray RD, et al. Use of transesophageal echocardiography to guide cardioversion in patients with atrial
fibrillation. N Engl J Med. May 10 2001;344(19):1411-20. [Medline].
45.
Klein AL, Jasper SE, Katz WE, et al. The use of enoxaparin compared with unfractionated heparin for short-term antithrombotic
therapy in atrial fibrillation patients undergoing transoesophageal echocardiography-guided cardioversion: assessment of
Cardioversion Using Transoesophageal Echocardiography (ACUTE) II randomized multicentre study. Eur Heart
J. Dec 2006;27(23):2858-65. [Medline].
46.
Malchano ZJ, Neuzil P, Cury RC, et al. Integration of cardiac CT/MR imaging with three-dimensional electroanatomical mapping
to guide catheter manipulation in the left atrium: implications for catheter ablation of atrial fibrillation. J Cardiovasc
Electrophysiol. Nov 2006;17(11):1221-9. [Medline].
47.
Massicotte P, Adams M, Marzinotto V, et al. Low-molecular-weight heparin in pediatric patients with thrombotic disease: a dose
finding study. J Pediatr. Mar 1996;128(3):313-8. [Medline].
48.
Olshansky B, Rosenfeld LE, Warner AL, et al. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM)
study: approaches to control rate in atrial fibrillation. J Am Coll Cardiol. Apr 7 2004;43(7):1201-8. [Medline].
49.
Ryder KM, Benjamin EJ. Epidemiology and significance of atrial fibrillation. Am J Cardiol. Nov
4 1999;84(9A):131R-138R. [Medline].
50.
Shah DC. The effectiveness and timing of elective pharmacological cardioversion for paroxysmal atrial fibrillation. Eur Heart
J. Dec 1999;20(24):1768-9. [Medline].
51.
Steinberg JS, Sadaniantz A, Kron J, et al. Analysis of cause-specific mortality in the Atrial Fibrillation Follow-up Investigation of
Rhythm Management (AFFIRM) study. Circulation. Apr 27 2004;109(16):1973-80. [Medline].
52.
Weerasooriya R, Davis M, Powell A, et al. The Australian Intervention Randomized Control of Rate in Atrial Fibrillation Trial
(AIRCRAFT). J Am Coll Cardiol. May 21 2003;41(10):1697-702. [Medline].
53.
Keywords
atrial fibrillation, a fib, atrial fib, arrhythmia, AFL, supraventricular tachycardia, SVT, congestive heart failure, CHF, ventricular
tachycardia, VT, ventricular fibrillation, VF, coronary artery disease, CAD, thromboembolic stroke, uncontrolled hypertension, coronary
disease, valvular heart disease, acute pulmonary processes, acute pulmonary disease, hyperthyroidism, acute alcohol intoxication,
holiday heart, Saturday night heart, illicit narcotic abuse, drug abuse, tachycardia-induced cardiomyopathy, rheumatic heart disease,
rheumatic valvular disease, hypertension, diabetes, thromboembolism, recurrent atrial fibrillation, paroxysmal atrial fibrillation,
permanent atrial fibrillation, chronic atrial fibrillation
thyrotoxicosis, electrolyte abnormalities, acute ethanol intoxication, atrial premature beats, Holter monitoring, hypertensive heart
disease, dilated cardiomyopathy, atrial cardiomyopathy, Maze procedure, electrical cardioversion, ischemic stroke, Wolff-
Parkinson-White syndrome, hepatojugular reflex, atrial flutter
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
39 of 41 6/13/2010 6:30 PM

Contributor Information and Disclosures
Author
Lawrence Rosenthal, MD, PhD, Associate Professor of Medicine, Director, Section of Cardiac Electrophysiology and Pacing,
Fellowship Director of Clinical Cardiac Electrophysiology, Department of Internal Medicine, Division of Cardiovascular Medicine,
University of Massachusetts Memorial Medical Center
Lawrence Rosenthal, MD, PhD is a member of the following medical societies: American College of Cardiology, American Heart
Association, and Massachusetts Medical Society
Disclosure: Nothing to disclose.
Coauthor(s)
David D McManus, MD, Assistant Professor of Medicine, Cardiac Electrophysiology Section, Cardiology Division, University of
Massachusetts Medical Center
Disclosure: Nothing to disclose.
Medical Editor
Alan D Forker, MD, Professor of Medicine, Program Director of Cardiovascular Fellowship, University of Missouri at Kansas City
School of Medicine; Director, Outpatient Lipid Diabetes Research Center, MidAmerica Heart Institute of St Luke's Hospital
Alan D Forker, MD is a member of the following medical societies: Alpha Omega Alpha, American College of Cardiology, American
College of Physicians, American Heart Association, American Medical Association, American Society of Hypertension, and Phi Beta
Kappa
Disclosure: Research Grant Grant/research funds Hospital contracts to do research; I am a hospital employee with no personal
profit; Speakers Bureau Honoraria Speaking and teaching
Pharmacy Editor
Francisco Talavera, PharmD, PhD, Senior Pharmacy Editor, eMedicine
Disclosure: eMedicine Salary Employment
Managing Editor
Brian Olshansky, MD, Professor of Medicine, Department of Internal Medicine, University of Iowa College of Medicine
Brian Olshansky, MD is a member of the following medical societies: American Autonomic Society, American College of Cardiology,
American College of Chest Physicians, American College of Physicians, American College of Sports Medicine, American Federation
for Clinical Research, American Heart Association, Cardiac Electrophysiology Society, Heart Rhythm Society, and New York Academy
of Sciences
Disclosure: Guidant/Boston Scientific Honoraria Speaking and teaching; Medtronic Honoraria Speaking and teaching; Guidant/Boston
Scientific Consulting fee Consulting; Novartis Honoraria Speaking and teaching; Novartis Consulting fee Consulting
CME Editor
Amer Suleman, MD, Consultant in Electrophysiology and Cardiovascular Medicine, Department of Internal Medicine, Division of
Cardiology, Medical City Dallas Hospital
Amer Suleman, MD is a member of the following medical societies: American College of Physicians, American Heart Association,
American Institute of Stress, American Society of Hypertension, Federation of American Societies for Experimental Biology, Royal
Society of Medicine, and Society of Cardiac Angiography and Interventions
Disclosure: Nothing to disclose.
Chief Editor
Jeffrey N Rottman, MD, Professor of Medicine and Pharmacology, Director, Clinical Cardiac Electrophysiology Fellowship Program,
Vanderbilt University School of Medicine; Chief, Department of Cardiology, Nashville Veterans Affairs Medical Center
Jeffrey N Rottman, MD is a member of the following medical societies: American Heart Association and North American Society of
Pacing and Electrophysiology (NASPE)
Disclosure: Nothing to disclose.
Further Reading
© 1994-2010 by Medscape.
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
40 of 41 6/13/2010 6:30 PM

All Rights Reserved
(http://www.medscape.com/public/copyright)
Atrial Fibrillation: [Print] - eMedicine Cardiology http://emedicine.medscape.com/article/151066-print
41 of 41 6/13/2010 6:30 PM