Advanced Biomedical Imaging
54
Advanced Biomedical Imaging Dr. Azza Helal Dr. Azza Helal A. Prof. A. Prof. of Medical Physics of Medical Physics Faculty of Medicine Faculty of Medicine Alexandria University Alexandria University Lecture 8 Lecture 8 Isotope scans, Radiation Isotope scans, Radiation unites unites & & Radiation hazards Radiation hazards
description
Lecture 8 Isotope scans, Radiation unites & Radiation hazards. Advanced Biomedical Imaging. Dr. Azza Helal A. Prof. of Medical Physics Faculty of Medicine Alexandria University. Isotope scans. - PowerPoint PPT Presentation
Transcript of Advanced Biomedical Imaging

Advanced Biomedical Imaging
Dr. Azza HelalDr. Azza HelalA. Prof.A. Prof. of Medical Physics of Medical Physics
Faculty of MedicineFaculty of MedicineAlexandria UniversityAlexandria University
Lecture 8Lecture 8Isotope scans, Radiation unites Isotope scans, Radiation unites
& & Radiation hazardsRadiation hazards

Isotope scansIsotope scans

Isotopes: nuclei with same no of protons but different no of neutrons. 6C12, 6C13, may be stable or unstable
Unstable nuclei (radioactive) have some unbalance in number of protons & neutrons. It has excess energy redistributed among nucleons.
To achieve a state of low energy, one of particle may gain enough energy to escape from nucleus.
Ejection of a particle changes the nucleus from one form to another. This is referred as decay or radioactivity
Isomers: nuclei with same no of protons and neutrons but different energy states. Tc99m, Tc99.

Modes of decay α β γ
β- decay Excess of neutrons Electron (beta particle) ejected from the nucleusβ+ decay.
Excess of protons Positron ejected from the nucleus
α decay Excess of nucleons (heavy nuclei) Nucleus ejects alpha particle (helium)
γ decay• γ rays are emitted during any radioactive decay

Isotope T1/2 Decay Isotope T1/2 Decay
Kr81m 13sec IT Tc99m 6hrs IT
Th201 73hr EC Xe133 5days γ & B
I123 13hr EC I131 8days B-
G67 78hr EC F18 110 min B+
TT1/21/2 of different atoms. of different atoms.
Half life time (T1/2 ) is the time required for a given nuclei to decay to ½ of its original value.

Radiopharmaceuticals:
Combination of Radionuclides with chemical
compounds (pharmaceuticals)
Once administered to the patient, it can
localize to specific organs allowing diagnosis
of a disease based on the cellular function
rather than the anatomy.

Radiopharmaceuticals (desirable properties):
Short t1/2 (few hours)
Decay to stable daughter,
Emits γ rays (isomeric transition)
Emits mono-energy γ rays (50-300) (150Kev).
So 99mTc is the best one.
– Radiation exposure is low:
It has a short t1/2 (6hrs)
Emits γ ray allowing small amounts to be detected.
Its quick decay into the less radioactive 99Tc.

Technetium-99m generator (technetium cow)
it is used to extract 99mTc from decaying of 99Mo.
99Mo is used as:
– has a t1/2 of 66 hr
– easily transported to hospitals where it decays to 99mTc (t1/2 6hr, inconvenient for transport).
Mo99 decays to pertechnetate. Pulling normal saline solution through the column of 99Mo elutes the soluble 99mTc, resulting in Na pertechnetate which is then injected to the patient.

After a wk, generator is
replaced.

Uses of Tc99m:
99Mo → 99mTc + β− (in generator)
99mTc → 99Tc + γ (in patient)
Na pertechnetate is used for imaging of tissues as thyroid, gastric mucosa & salivary glands.
it can be labeled to a wide variety of compounds e.g. – HMPAO for cerebral imaging.– HIDA for billiary studies. – MAG3 for renal studies. – DTPA for lung ventilation studies – Diphosphonate for bone imaging.

Precautions FOR handling radionuclides:
Segregation:
separated area for preparation, storage, injection,
patient to wait & image, temporary storage of waste.
patient is considered as a source of external radiation.
Follow inverse square low to decrease the exposure.
The room should be with continuous floor, glass
painted wall and formica topped benches.
Simple mixing with the compound to be labeled at
room temperature, use shielded syringes to transfer.

Personal protection:
Use the three important factors for protection, time, distance & barriers.
Time should be as short as possible (no eat, drink….) Distance from the source should be as long as possible
so use long handle forceps Barriers used as: Lead shielded generators, bottle & syringes Lead glass barriers. Special containers for transport water proof surgical gloves, cover cuts and abrasion,

Patient protection:
Check activity, avoid contamination, deal with the spills, vomiting, incontinence.
if there is contamination:
– Mop the floor with absorbent pads and seal the swabs in plastic bags & continue cleaning and monitor to check that the dose is low.
– If necessary cordon off the area or cover it with
impervious sheet till sufficient decay has occurred.

Disposal of the waste:
Contaminated materials are treated as waste.
Gaseous waste vent to atmosphere, aqueous waste diluted with water via designated sink
solid waste are placed in designated sack for disposal by incineration.
Contaminated cloths and bedding is bagged & stored in a secure protected area until sufficiently decayed.

Dose to the patient: increases in proportion to:
– Activity and the fraction taken up by the
organ.
– Effective t1/2 in the organ.
– not affected by scan time / number of images
Decrease the dose to the patient:
Drinking a lot of water
Empty the bladder to reduce dose to gonads
Avoid contamination

Gamma imaging
While X ray, CT and MRI isolate anatomic changes in the body, gamma imaging is capable of detecting areas of molecular biology detail even prior to anatomic change.
This is by counting the radioactivity and its distribution in the organ.
Isotope scans

Gamma camera components (scintillation counter):Gamma camera components (scintillation counter):
Gantry (collimator,detector crystal & photomultiplier tube in evacuated glass envelope) & data analysis computer.
Gantry is connected to computer & both control operation of the camera, acquisition and storage of images.
Collimator: lead disk with many holes separated by septa to absorb most gamma rays not parallel to collimator..
NAI crystal is connected to 100 photomultiplier
photomultiplier components: photocathode, 10-12 dynodes and anode.

When a gamma ray interacts in the crystal, it produces light which strikes photocathode producing low energy electrons. These electrons are focused and accelerated by the dynodes until about one million reach the anode.
Size of pulse which emerges from anode is α to number of electrons which are ejected from photocathode which is α to amount of light in turn α to energy which was absorbed from gamma-ray photon by the crystal.
A computer is used with gamma camera to electronically process these signals



Gamma Camera Planar ImagingGamma Camera Planar Imaging
single projection viewno image reconstruction is required

Tomography with radionuclideTomography with radionuclide

It includes SPECT (Single Photon Emission CT) & PET (Positron Emission Tomography).
Both rely on similar principles to produce images:
– use of radioactive tracer & detection of gamma rays.– tracer is chemically combined with biologically active
molecule.– waiting period for active molecule to be concentrated in
tissues of interest– then the patient is placed in the imaging scanner.
– During scan a record of tissue concentration is made as tracer decays

Differences between SPECT & PETDifferences between SPECT & PET

SPECT PET
Tracer Na pertechnotate
99mTc )6Hrs(
Flurodeoxyglucose (FDG)Fluorine-18
)110 min(
Production Generator Cyclotron
Detection site Decay Annihilation
Detector crystal One large
NaIMultiple
bismuth germinate
Camera Rotating Stationary
Collimator Present Absent
Detect Blood flow & Metabolic activity
Glucose uptake &Metabolic activity
Resolution Lower Higher
Cost Less High

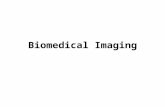
Single head SPECT
Double head SPECT Triple head SPECT

)PET(
30.000
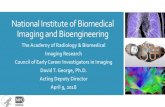
F18 undergoes positron emission decay. After traveling up to a few mm positron encounters an electron producing a
pair of annihilation photons moving in opposite directions and detected.

PET CT images show metastases to left supraclavicular lymph node a and to liver b

Differences between X-ray Imaging Differences between X-ray Imaging &&
Isotope scansIsotope scans

X-ray Imaging Isotope scansSource of radiation External (X-ray) Internally (Gamma rays)
Imaging Anatomical Physiological function
Image shows2-D or 3-D of a
structure3-D distribution of a
radionuclide
Scan Particular section More organ or tissue
specific
Delivered doseSpecific to examined
area
Most tissues receive some dose, but target or organ
excretes the highest dose.
Factors affect patient dose Mention them in X ray
& CT?Mention them?
Number of images& patient dose
Increase pt dose No effect
absorbed dose increases with Mention the factors? Mention the factors?
Exposure to radiation + +

Radiation unitesRadiation unites

Roentgen: an exposure dose
It is amount of x or gamma rays which produce ionisation of 1cc of dry air producing ion pair carrying + & -ve charge each carries one esu.
RAD: Radiation Absorbed Dose:
It is the energy deposited/unit mass (100ergs/ gm) by any type of ionizing radiation in any medium due to excitation & ionization
Gy = 100 RAD.

Biological effect of a given absorbed dose of any
type of radiation will not be of same magnitude as
effect of same absorbed dose of anther radiation.
Also it differs in different tissues
For the same dose to the organ, alpha or neutron
radiation will cause greater harm compared with
gamma rays, x rays, or electrons because the
ionization events produced by alpha or neutron
radiation will be much more closely spaced.

The absorbed dose The absorbed dose is multiplied by a radiation weighting factor wR (equivalent dose)(equivalent dose) & tissue
weighting factor wT (difference in tissue sensitivities) ((Effective dose)
Rem (Roentgen equivalent man): Effective dose
Amount of any type of radiation which produces same biological effect as one RAD of x or
gamma ray.Sievert (Sv)= 100Rem
Accounts for different tissues sensitivities. It measures radiation & organ damage.

Tissue wT Gonads 0.2
Red bone marrow 0.12 Colon 0.12 Lung 0.12
Stomach 0.12 Bladder 0.05 Breast 0.05 Liver 0.05
Oesophagus 0.05 Thyroid 0.05
Skin 0.01 Bone surfaces 0.01
Remainder 0.05 Total 1.00
Radiation type. wR Photons 1
Electrons 1 Neutrons 5 – 20
Energetic Protons 5 Alpha particles and
Fission nuclei 20
Dr Azza Helal
Equivalent dose= absorbed dose X wR
Effective dose= absorbed dose X wR X wT

Unites of radioactivity
Curie
Radioactivity of a sample which decays at a rate of 3.7X1010 dis/sec
Becquerel
Radioactivity of a sample which decays at a rate of one dis/sec
Ci=37GBq

Radiation hazardsRadiation hazards

Plain Film X Rays
Single Radiographs Effective Dose, mrem (mSv) Skull (PA or AP)1 3 (0.03)
Skull (lateral)1 1 (0.01)
Chest (PA)1 2 (0.02)
Chest (lateral)1 4 (0.04)
Chest (PA and lateral)5 6 (0.06)
Thoracic spine (AP)1 40 (0.4)
Thoracic spine (lateral)1 30 (0.3)
Lumbar spine (AP)1 70 (0.7)
Lumbar spine (lateral)1 30 (0.3)
Abdomen (AP)1 70 (0.7)
Abdomen6 53 (0.53)
Pelvis (AP)1 70 (0.7)
Pelvis or hips6 83 (0.83)
Bitewing dental film6 0.4 (0.004)
Limbs and joints6 6 (0.06)

Doses Received Undergoing an Entire Procedure
Complete Exams Effective Dose, mrem (mSv) Intravenous Pyelogram (kidneys, 6 films)1 250 (2.5)
Barium swallow (24 images, 106 sec fluoroscopy)1 150 (1.5)
Barium meal (11 images, 121 sec fluoroscopy)1 300 (3.0)
Barium follow-up (4 images, 78 sec fluoroscopy)1 300 (3.0)
Barium enema (10 images, 137 sec fluoroscopy)1 700 (7.0)
CT head1 200 (2.0)
CT chest1 800 (8.0)
CT abdomen1 1,000 (10)
CT pelvis1 1,000 (10)
CT (head and chest)5 1,110 (11)
PTCA (heart study)6 750-5,700 (7.5-57)
Coronary angiogram6 460-1,580 (4.6-15.8)
Mammogram6 13 (0.13)
Lumbar spine series6 180 (1.8)
Thoracic spine series6 140 (1.4)
Cervical spine series6 27 (0.27)


Typical Doses from Nuclear Medicine Exams
Nuclear Medical Scan Activity, mCi (MBq)
Radiopharmaceutical Effective Dose, mrem (mSv)
Brain2 20 (740) 99mTc DTPA 650 (6.5)
Brain3 50 (1,850) 15O water 170 (1.7)
Brain4 20 (740) 99mTc HMPAO 690 (6.9)
Hepatobiliary2 5 (185) 99mTc SCO 370 (3.7)
Bone2 20 (740) 99mTc MDP 440 (4.4)
Lung Perfusion/Ventilation2
5 & 10 (185 & 370)
99mTc MAA & 133Xe 150 (1.5)
Kidney2 20 (740) 99mTc DTPA 310 (3.1)
Kidney3 20 (740) 99mTc MAG3 520 (5.2)
Tumor2 3 (110) 67Ga 1,220 (12.2)
30 (1,100) 99mTc sestimibi 890 (8.9) Heart3
30 (1,100) 99mTc pertechnetate 1,440 (14.4)
2 (74) 201Tl chloride 1,700 (17) Heart4
30 (1,100) 99mTc tetrofosmi 845 (8.45)
Various3 10 (370) 18F FDG 700 (7.0)

Irradiation of the foetus results from:– Placental transfer.
– External irradiation from radioactivity in the mother's organs and tissues.
Since radionuclides in maternal tissues contribute to foetal dose so foetal dose can be reduced by:
– Maternal hydration and frequent voiding – Using smaller administered activities and
longer imaging times

Estimated Fetal Radiation Dose Based on "Typical" Exposure Values
Fetal Dose mrem, (mSv) Study
Early Pregnancy 3-Month 6-Month 9-Month AP Pelvis 144 (1.44) 131 (1.31) 127 (1.27) 157 (1.57)
PA Pelvis 40 (0.40) 16 (0.16) 232 (2.32) 100 (1.00)
Lateral Pelvis 53 (0.53) 32 (0.32) 48 (0.48) 52 (0.52)
AP T-Spine (wide FOV) 1.8 (0.018) 1.1 (0.011) 6.9 (0.069) 13 (0.13)
AP T-Spine (narrow) 1.2 (0.012) 0.8 (0.008) 4.6 (0.046) 8.9 (0.089)
Lateral T-Spine 0.6 (0.006) 0.6 (0.006) 1.7 (0.017) 3.2 (0.032)
AP Lumbar Spine 225 (2.25) 197 (1.97) 394 (3.94) 926 (9.26)
Lat Lumbar Spine 113 (1.13) 62 (0.62) 84 (0.84) 85 (0.85)
11 mSvmSv

Doses from Nuclear Medicine Exams for the Fetus
Nuclear Medical Scan
Activity, mCi (MBq)
Radiopharmaceutical Early Pregnancy Fetal Dose, mrem (mSv)
Bone 20 (740) 99mTc MDP 460 (4.6)
Lung Perfusion 5.5 (200) 99mTc MAA 56 (0.56)
0.8 (30) 123I NaI 60 (0.6) Thyroid
0.015 (0.55) 131I NaI 4 (0.04)
Tumor 5 (190) 67Ga Citrate 1,800 (18
Lung Ventilation 30 (1,100) 133Xe Gas 0.54 (0.0054)
Heart 1.5 (55) 201Tl chloride 530 (5.3)
20 (740) 99mTc MAG3 1,400 (14) Kidney
20 (740) 99mTc DTPA 900 (9)
Heart 30 (1,100) 99mTc sestimibi 1,700 (17)
Liver 9.5 (350) 99mTc disofenin / mebrofenin
600 (6)
5.4 (200) 99mTc White Blood Cells 76 (0.76) Infection
0.5 (20) 111In White Blood Cells 260 (2.6)
Liver/Spleen 8 (300) 99mTc Sulfur Colloid 54 (0.54)
Bone 20 (740) 99mTc HDP 390 (3.9)
Brain/Thyroid 30 (1,100) 99mTc Pertechnetate 1,200 (12)
Heart/blood flow 25 (930) 99mTc Red Blood Cells 600 (6.0)

Summary of Recommendations for Radiopharmaceuticals Excreted in the Breast Milk8 Administered
Pharmaceutical Activity, mCi (MBq)
Counseling?* Advisory
67Ga Citrate 5.0 (185) Yes Cessation 99mTc DTPA 20 (740) No 99mTc MAA 4 (148) Yes 12 hr 99mTc Pertechnetate 30 (1,110) Yes 48 hr 131I NaI 150 (5,550) Yes Cessation 51Cr EDTA 0.05 (1.85) No 99mTc IDA agents 8 (300) No 99mTc Glucoheptonate 20 (740) No 99mTc HAM 8 (300) No 99mTc MIBI 30 (1,110) No 99mTc MDP 20 (740) No 99mTc PYP 20 (740) No 99mTc Red Blood Cells in vivo 20 (740) Yes 12 hr 99mTc Red Blood Cells in vitro 20 (740) No 99mTc Sulfur Colloid 12 (444) No 111In White Blood Cells 0.5 (18.5) No 123I NaI 0.4 (14.8) Yes Cessation** 123I OIH 2 (74) No 123I mIBG 10 (370) Yes 48 hr 125I OIH 0.01 (0.37) No 131I OIH 0.3 (11.1) No 99mTc DTPA Aerosol 1 (37) No 99mTc MAG3 10 (370) No 99mTc White Blood Cells 5 (185) Yes 48 hr 201Tl Chloride 3 (111) Yes 96 hr

Nursing mothers must be counseled about the need to interrupt / discontinue breast feedingPumped milk may be refrigerated and used after the radioactivity has decayed
Complete cessation of breast feeding:
Ga-67 citrate
I-131 sodium iodide therapy
Interruption of breast feeding for 12 hours:
Tc-99m macroaggregated albumin
Tc-99m–labeled RBCs (in vivo labeling)
In-111–labeled WBCs
Interruption of breast feeding for 24 hours:
Tc-99m pertechnetate
I-123 metaiodobenzylguanidine
Tc-99m–labeled WBCs
Interruption of breast feeding for 168 hours:
Tl-210 chlorided

Early effects
– Whole body
– Partial body
– gonadalLate effects
Acute radiation syndrome
Teratogenic effects
Effect of radiation on the body

Radiation protectionRadiation protection

Radiation protection
To be sure that the dose received by person is small as possible so that the consequent damage
never constitute a significant hazards to the heath of irradiated person.
Maximum permissible dose (MPD)
The dose which is not expected to cause any detectable body injury for the person during his life time and till his 3rd generation.

Radiation exposures divided into 3 categories:
– Occupational exposure. (2Rem/yr, 20 mSvmSv).
– Medical exposure, (special group), persons work in controlled area (1.5Rem/yr)
– Public exposure 1/10 occupational exposure.
– Pregnant worker 1msv Pregnant worker 1msv
– Dose to embryo 5 mSv = 0.5 rem in 9mthDose to embryo 5 mSv = 0.5 rem in 9mth

Radiation detectors:
• Radiation survey meter
(Geiger Muller counter)
2. Personnel Monitoring
1. Film badge: permanent records, cheap, not accurate, hard processing, over exposure not detected at once
2. TLD : accurate, small, used in in vivo dosimetry, no permanent records, more expensive, over exposure not
detected at once. 3.Pocket dosimeter: over exposure detected at once,
expensive, no permanent records

Personnel Monitoring devices

Radiation Protection & Exposure Control
Time– Reduce the time spent near a radiation source
Distance– Inverse square law
– Radiation intensity is 1/distance 2
– NCRP recommends that personnel should stand at least 2m from x-ray tube and patient and behind a shielded barrier
Shielding