A Case Report of Familial Sudden Cardiac Death...Sudden cardiac death (SCD) is usually from cardiac...
3
Central Bringing Excellence in Open Access JSM Clinical Case Reports Cite this article: Feng W (2016) A Case Report of Familial Sudden Cardiac Death. JSM Clin Case Rep 4(3): 1103. *Corresponding author Wei Feng, Puyan District Community Health Center, Hangzhou, China, Email: Submitted: 18 May 2016 Accepted: 01 July 2016 Published: 06 July 2016 Copyright © 2016 Feng ISSN: 2373-9819 OPEN ACCESS Keywords • Familial • Sudden cardiac death • Implantable cardioverter defibrillators • Heredity Case Report A Case Report of Familial Sudden Cardiac Death Wei Feng* Puyan District Community Health Center, China Abstract The annual incidence of sudden cardiac death (SCD) in the general population is 0.1%. SCDs in the young are mainly caused by genetic heart disorders which can lead to inherited arrhythmia syndromes, such as long QT, short QT and Brugada syndromes. One of the most effective therapies for this disease is implantable cardioverter defibrillators (ICD). In this article, we reported a case of 46 years old patient with repeated syncope. Investigation of the family history we found a familial SCDs and the members died in 28.5 years old on average and all of them were male. ABBREVIATIONS SCD: Sudden Cardiac Death; ICD: Implantable Cardioverter Defibrillators; ECG: Electrocardiograms; EEG: Electroencephalogram CASE PRESENTATION Abstract of history The patient was a 46 years old woman. Admission at Nov 12, 2008. Chief complaint: Repeated syncope for 12 years. She felt dizzy and became unconsciousness after injecting penicillin 12 years ago. Before syncope, she denied headache, nausea, vomiting, dyspnea and palpitation. During syncope, her eyes rolled back, and all four extremities were stiff. She denied convulsions, foaming at the mouth, and rash. All the symptoms lasted for 1 minute and she recovered, without any sequela. The occurrence of syncope had no relationship with time, place, posture and feeding. In the last 12 years, this symptom happened for 5 times. The patient had seek medical services and all of the electrocardiograms (ECG) were normal. The 24h ambulatory electroencephalogram (EEG) was normal. The 24h ambulatory electrocardiogram demonstrated: second degree atrioventricular block. Physical examination T 37.1 °C, P 60/min, R 18/min, BP 116/70 mmHg. She was well developed and moderately nourished. Her face was ruddy and the skin was not stained yellow. No cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. No pitting edema. Superficial lymph nodes were not found enlarged. No bulge and no abnormal impulse or thrills in precordial area. The point of maximum impulse was at 5th left intercostal space and inside of the mid clavicular line. No pericardial friction sound. Border of the heart was normal. Heart sounds were strong without splitting. Cardiac rhythm was regular. No pathological murmurs. Respiratory movement was bilaterally symmetric with the frequency of 18/min. thoracic expansion and tactile fremitus were symmetric bilaterally. No pleural friction fremitus. Resonance was heard during percussion. No abnormal breath sound was heard. No wheezes. No rales. The abdomen was flat and soft. No bulge or depression. No abdominal wall varicosis. Gastralintestinal type or peristalses were not seen. Tenderness was obvious around the navel and in upper abdomen. There was not rebound tenderness on abdomen or renal region. Liver and spleen was untouched. No masses. Fluid thrill was negative. Shifting dullness was negative. Borhorygmus was not heard. No vascular murmurs. No articular swelling. Physiological reflexes were existent without any pathological ones. Hospital course ECG and EEG were normal. From echocardiography, it demonstrated that the patient’s heart function was at a normal lever (EF 72.1%). All of the chambers were at a general size (LA 2.91cm, LVIDd 4.75cm), and the thickness of myocardium was not aberrant (IVSd0.94cm, IVS/LVPW0.92). The result manifested that the patient didn’t have any visible cardiomyopathy (Figure 1). During the coronary arteriography, all of the coronary arteries were smooth, and it indicated that the patient didn’t have coronary atherosclerotic heart disease (Figure 2). The ambulatory electrocardiogram indicated: sinus rhythm, with 27 ventricular premature beats and the average rate was 85/ min. All of the blood test, cranial magnetic resonance imaging (MRI), and echocardiogram were normal. When the patient was sitting in the hospital, she felt dizzy and chest distress, the holter recorded as torsade de pointes (TDP) (Figure 3). Then she received an implantable cardioverter defibrillator (ICD). The patient followed yearly, and no event happened. Family history review The patient’s father died at 35 years old. Her son died at 21 years old, just two months earlier than she admitted into the hospital. What’s more, in her family, six persons were sudden
Transcript of A Case Report of Familial Sudden Cardiac Death...Sudden cardiac death (SCD) is usually from cardiac...

CentralBringing Excellence in Open Access
JSM Clinical Case Reports
Cite this article: Feng W (2016) A Case Report of Familial Sudden Cardiac Death. JSM Clin Case Rep 4(3): 1103.
*Corresponding authorWei Feng, Puyan District Community Health Center, Hangzhou, China, Email:
Submitted: 18 May 2016
Accepted: 01 July 2016
Published: 06 July 2016
Copyright © 2016 Feng
ISSN: 2373-9819
OPEN ACCESS
Keywords•Familial•Sudden cardiac death•Implantablecardioverterdefibrillators•Heredity
Case Report
A Case Report of Familial Sudden Cardiac DeathWei Feng*Puyan District Community Health Center, China
Abstract
The annual incidence of sudden cardiac death (SCD) in the general population is 0.1%. SCDs in the young are mainly caused by genetic heart disorders which can lead to inherited arrhythmia syndromes, such as long QT, short QT and Brugada syndromes. One of the most effective therapies for this disease is implantable cardioverter defibrillators (ICD). In this article, we reported a case of 46 years old patient with repeated syncope. Investigation of the family history we found a familial SCDs and the members died in 28.5 years old on average and all of them were male.
ABBREVIATIONSSCD: Sudden Cardiac Death; ICD: Implantable
Cardioverter Defibrillators; ECG: Electrocardiograms; EEG: Electroencephalogram
CASE PRESENTATIONAbstract of history
The patient was a 46 years old woman. Admission at Nov 12, 2008. Chief complaint: Repeated syncope for 12 years. She felt dizzy and became unconsciousness after injecting penicillin 12 years ago. Before syncope, she denied headache, nausea, vomiting, dyspnea and palpitation. During syncope, her eyes rolled back, and all four extremities were stiff. She denied convulsions, foaming at the mouth, and rash. All the symptoms lasted for 1 minute and she recovered, without any sequela. The occurrence of syncope had no relationship with time, place, posture and feeding. In the last 12 years, this symptom happened for 5 times. The patient had seek medical services and all of the electrocardiograms (ECG) were normal. The 24h ambulatory electroencephalogram (EEG) was normal. The 24h ambulatory electrocardiogram demonstrated: second degree atrioventricular block.
Physical examination
T 37.1 °C, P 60/min, R 18/min, BP 116/70 mmHg. She was well developed and moderately nourished. Her face was ruddy and the skin was not stained yellow. No cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. No pitting edema. Superficial lymph nodes were not found enlarged. No bulge and no abnormal impulse or thrills in precordial area. The point of maximum impulse was at 5th left intercostal space and inside of the mid clavicular line. No pericardial friction sound. Border of the heart was normal. Heart sounds were strong without splitting. Cardiac rhythm was regular. No pathological murmurs. Respiratory movement was bilaterally symmetric
with the frequency of 18/min. thoracic expansion and tactile fremitus were symmetric bilaterally. No pleural friction fremitus. Resonance was heard during percussion. No abnormal breath sound was heard. No wheezes. No rales. The abdomen was flat and soft. No bulge or depression. No abdominal wall varicosis. Gastralintestinal type or peristalses were not seen. Tenderness was obvious around the navel and in upper abdomen. There was not rebound tenderness on abdomen or renal region. Liver and spleen was untouched. No masses. Fluid thrill was negative. Shifting dullness was negative. Borhorygmus was not heard. No vascular murmurs. No articular swelling. Physiological reflexes were existent without any pathological ones.
Hospital course
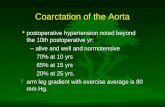
ECG and EEG were normal. From echocardiography, it demonstrated that the patient’s heart function was at a normal lever (EF 72.1%). All of the chambers were at a general size (LA 2.91cm, LVIDd 4.75cm), and the thickness of myocardium was not aberrant (IVSd0.94cm, IVS/LVPW0.92). The result manifested that the patient didn’t have any visible cardiomyopathy (Figure 1). During the coronary arteriography, all of the coronary arteries were smooth, and it indicated that the patient didn’t have coronary atherosclerotic heart disease (Figure 2). The ambulatory electrocardiogram indicated: sinus rhythm, with 27 ventricular premature beats and the average rate was 85/min. All of the blood test, cranial magnetic resonance imaging (MRI), and echocardiogram were normal. When the patient was sitting in the hospital, she felt dizzy and chest distress, the holter recorded as torsade de pointes (TDP) (Figure 3). Then she received an implantable cardioverter defibrillator (ICD). The patient followed yearly, and no event happened.
Family history review
The patient’s father died at 35 years old. Her son died at 21 years old, just two months earlier than she admitted into the hospital. What’s more, in her family, six persons were sudden

CentralBringing Excellence in Open Access
Feng (2016)Email:
JSM Clin Case Rep 4(3): 1103 (2016) 2/3
to getting positive findings by taking the 24h ambulatory electrocardiograms. Meanwhile, in the patient’s family, all the members with sudden death are male. Three in the elder generation, average age is 34.7, the morbidity is 60%; two in the same generation, average age is 23, the morbidity is 18.75%; one in filial generation and the age is 21 year old, the morbidity is 5.56%. We suspect that the disease has a certain genetic predisposition. The age of sudden death has been advanced from the generations, it may regard as “genetic anticipation”. Otherwise, with the marriage of different ethnic groups, the incidence of family members continues to decline. Owing to the normal ECGs, the patient may be suffering from a peculiar disease that different from long QT syndrome and Brugada syndrome.
Sudden cardiac death (SCD) is usually from cardiac causes, heralded by abrupt loss of consciousness within one hour of the onset of acute symptoms [1-3]. Sudden loss of consciousness is the primary manifestation and “unexpected” is a sign of it. Although some SCD patients with pre-existing heart disease may have been found in advance, but the form and time of death is Unpredictable [4]. More than 80% of the pathogeny is coronary artery disease. In addition, non-ischemic cardiomyopathy, cardiac insufficiency is also high-risk factor of SCD [5].
SCD is an important public health problem, and it is found that a genetic tendency while studying of the risk factors and the cause of SCD. In a case-control study, over 500 cases, in Seattle, a family history of SCD was found to be an independent risk factor for the onset of SCD [6]. Paris prospective study I [7] for more than 7000 men who were followed up for 23 years indicated: the history of sudden death of parents is an independent risk factor, and three tips demonstrated the role of hereditary: 1. The increasing fatalness of SCD is discrete with the increasing
Figure 1 The echocardiography results of the patient.
Figure 2 The coronary arteriography results of the patient.
Figure 3 The ECG results when the patient felt dizzy and chest distress.
Figure 4 The family tree of the patient.
death, two in the first degree relatives, two in the second degree relatives and the rest in the third degree relatives, all of them were male, and the average age is 28.5. In addition, five persons had symptom, such as, dizzy, chest distress, palpitation with no fainting (Figure 4).
DISCUSSION All of the ECGs of the patient before were normal; with
the 24h ambulatory electrocardiogram was a little aberrant by ventricular premature beats. But it is fatal that developed into malignant arrhythmia at the onset of syncope. Accordingly, it is easier to make missed diagnosis by using ordinary ECGs for a screening method of these patients. Even though, it is unlikely

CentralBringing Excellence in Open Access
Feng (2016)Email:
JSM Clin Case Rep 4(3): 1103 (2016) 3/3
Feng W (2016) A Case Report of Familial Sudden Cardiac Death. JSM Clin Case Rep 4(3): 1103.
Cite this article
risk of myocardial infarction. 2. The research objects die at the same age as their parents for the similar reason. 3. When both of parents were sudden death, the relative risk of SCD of offspring is 9.4 times, and the relative risk of SCD of the offspring is 1.8 times while one of the parents was sudden death. In patients with abnormal ECGs before the onset of the disease, as long QT syndrome [8-10] and Brugada syndrome [11-12], or other primary or hereditary ion-channel disease, the pathogenesis and genetic characteristics have long been known and studied. Take long QT syndrome (LQTS), for example, in the early 90’s of the last century, four loci were found on 11, 3, 7 and 4 chromosome [13-15], then using cloning technology, KCNQ1 was found as one of the LQT1 genes on chromosome 11 [16], and soon discovered the KCNH2, and gene mutations in KCNE1 and the KCNE2 on chromosome 21. But for those who have normal ECGs and cardiac structure, there is still a risk of sudden death due to genetic factors. Based on a large scale investigation of African Americans, a genetic mutation of cardiac sodium channel (SCN5A) was found (carrying rate=13.2%), it may still be a tendency to SCD, even though the gene was not found to exhibit a typical long QT syndrome [17]. In 1978, Coumel et al., reported the ventricular tachycardia [18], occurs in structural integrity heart, which was caused by the mental strain. The patients suffering from this disease characterize with normal ECGs and cardiac structure, but easy to sudden death, especially repeated occurs in activity and intravenous injection of catecholamines was. It is regard as Catecholaminergic polymorphic ventricular tachycardia (CPVT) [19]. In December 2000, Priori et al., confirmed in 4 CPVT patients with RyR2 gene mutation, and proved that CPVI is one kind of autosomal dominant disease with normal representation [20,21].
From the family tree Figure (4), we suspect that the incidence of patients with a certain genetic quality. The genetic quality has a certain relationship with gender, most probably, X-linked inheritable disease [22]. In order to find more patients and validate our suspicion, we suggest collecting blood samples of all families to analyze DNA. Due to personal reasons, the patient refused our proposal. However, the implantation of ICD can effectively treat malignant arrhythmia, which makes us be more confidence in the prognosis of the patient.
REFERENCES1. Ingles J, Semsarian C. Sudden cardiac death in the young: a clinical
genetic approach. Intern Med J. 2007; 37: 32-37.
2. Sen-Chowdhry S, McKenna WJ. Sudden cardiac death in the young: a strategy for prevention by targeted evaluation. Cardiology. 2006; 105: 196-206.
3. Sarkozy A, Brugada P. Sudden cardiac death and inherited arrhythmia syndromes. J Cardiovasc Electrophysiol. 2005; 16: 8-20.
4. Myerburg RJ, Castellanos A. Cardiac arrest and sudden cardiac death. In: Zipes DP, Libby P, Bonow RO, editors. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 7th edn. Elsevier Saunders Company, Philadelphia, PA. 2004: 865-908.
5. Huikuri HV, Castellanos A, Myerburg RJ. Sudden death due to cardiac arrhythmias. N Engl J Med. 2001; 345: 1472-1482.
6. Friedlander Y, Siscovick DS, Weinmann S, Austin MA, Psaty BM, Lemaitre RN, et al. Family history as a risk factor for primary cardiac
arrest. Circulation. 1998; 97: 155-160.
7. Jouven X, Desnos M, Guerot C, Ducimetière P. Predicting sudden death in the population: the Paris Prospective Study I. Circulation 1999; 99: 1978-1983.
8. Goldenberg I, Zareba W, Moss AJ. Long QT Syndrome. Curr Probl Cardiol. 2008; 33: 629-694.
9. Medeiros-Domingo A, Iturralde-Torres P, Ackerman MJ. Clinical and genetic characteristics of long QT syndrome. Rev Esp Cardiol. 2007; 60: 739-752.
10. Ching CK, Tan EC. Congenital long QT syndromes: clinical features, molecular genetics and genetic testing. Expert Rev Mol Diagn. 2006; 6: 365-374.
11. Napolitano C, Priori SG. Brugada syndrome. Orphanet J Rare Dis. 2006; 14; 1-35.
12. Herbert E, Chahine M. Clinical aspects and physiopathology of Brugada syndrome: review of current concepts. Can J Physiol Pharmacol. 2006; 84: 795-802.
13. Keating M, Atkinson D, Dunn C, Timothy K, Vincent GM, Leppert M. Linkage of a cardiac arrhythmia, the long QT syndrome, and the Harvey ras-1 gene. Science. 1991; 252: 704-706.
14. Jiang C, Atkinson D, Towbin JA, Splawski I, Lehmann MH, Li H, et al. Two long QT syndrome loci map to chromosomes 3 and 7 with evidence for further heterogeneity. Nat Genet. 1994; 8: 141-147.
15. Schott JJ, Charpentier F, Peltier S, Foley P, Drouin E, Bouhour JB, et al. Mapping of a gene for long QT syndrome to chromosome 4q25-27. Am J Hum Genet. 1995; 57: 1114-1122.
16. Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, VanRaay TJ, et al. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet. 1996; 12: 17-23.
17. Splawski I, Timothy KW, Tateyama M, Clancy CE, Malhotra A, Beggs AH, et al. Variant of SCN5A sodium channel implicated in risk of cardiac arrhythmia. Science. 2002; 297: 1333-1336.
18. Coumel P, Fidelle J, Lucet V. Catecholaminergic-induced severe ventricular arrhythmias with Adam-Stokes syndrome in children: Report of four cases. Br Heart J. 1978; 40: 28-37.
19. Leenhardt A, Lucet V, Denjoy I, Grau F, Ngoc DD, Coumel P. Catecholaminergic polymorphic ventricular tachycardia in children 7-year follow-up of 21 patients. Circulation. 1995; 91: 1512-1519.
20. Postma AV, Denjoy I, Kamblock J, Alders M, Lupoglazoff JM, Vaksmann G, et al. Catecholaminergic polymorphic ventricular tachycardia: RYR2 mutations, bradycardia, and follow up of the patients. J Med Genet. 2005; 42: 863-870.
21. Francis J, Sankar V, Nair VK, et al. Priori SG. Catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2005; 2: 550-554.
22. Towbin JA. Molecular genetic basis of sudden cardiac death. Pediatr Clin North Am. 2004; 51: 1229-1255.
23. Ding L, Hua W, Niu H, chen K, Zhang S. Primary prevention of sudden cardiac death using implantable cardioverter defibrillators. Europace. 2008; 10: 1034-1041.
24. Santini M, Lavalle C, Ricci RP. Primary and secondary prevention of sudden cardiac death: who should get an ICD? Heart. 2007; 93: 1478-1483.