A5 - Sudden Cardiac Death
61
Educational Background: University of Santo Tomas, 1995 Santo Tomas Univ. Hospital, 1996 Post Graduate Training: Residency Training in Internal Medicine –UP PGH Fellowship in Adult Cardiology- UP PGH Training in Clinical Cardiac Electrophysiology and Pacing -Philippine Heart Center Present Positions: Consultant, Philippine Heart Center ERDIE C. FADREGUILAN, MD FPCP, FPCC ERDIE C. FADREGUILAN, MD FPCP, FPCC
-
Upload
medhat-sabri -
Category
Documents
-
view
226 -
download
0
Transcript of A5 - Sudden Cardiac Death

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 1/61
Educational Background:University of Santo Tomas, 1995
Santo Tomas Univ. Hospital, 1996
Post Graduate Training:
Residency Training in Internal Medicine –UP PGHFellowship in Adult Cardiology- UP PGH
Training in Clinical Cardiac Electrophysiology and Pacing
-Philippine Heart Center
Present Positions:Consultant, Philippine Heart Center
ERDIE C. FADREGUILAN, MDFPCP, FPCC
ERDIE C. FADREGUILAN, MDFPCP, FPCC

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 2/61
SUDDEN CARDIAC DEATH
Erdie C. Fadreguilan, MD

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 3/61

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 4/61
SUDDEN CARDIAC DEATH
• Definition:
“Natural death due to cardiaccauses heralded by abrupt loss of consciousness within one hour of the onset of acute symptoms”

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 5/61
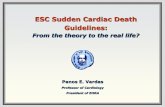
SCA- A Public Health Issue
AIDS2
Breast
Cancer1
LungCancer1
SCD3
SCD claims more
lives each year thanthese other diseasescombined:
The Facts:• Significant Killer in America
• 95% fatal without ICDprotection5 - 98% survivalwith ICD protection
• Nearly 1000 SCA deaths/day6
• ICDs are Class I indicated formost at-risk Pts7
• New guidelines clearly outline
at-risk groups7
• Studies show that ICDs arecost effective8
14,000
41,400
335,000162,500

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 6/61
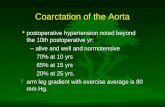
GROUP
Patients with highcoronary-risk profile
Patients with previouscoronary event
Patients with ejectionfraction <35%,congestive heart failure
Patients with previousout-of-hospital cardiacarrest
Patients with previousmyocardial infarction,low ejection fraction,and ventriculartachycardia
General population
Incidence of SCD in Specific Populationsand Annual SCD Numbers
Myerburg RJ. Circulation.1998;97:1514-1521.
300,000200,000100,0000
No. of SuddenDeathsPer Year
3025201050
Incidence of SuddenDeath(% of group)

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 7/61
What Is SCA?
• Electrical system in heart malfunctions
• Heart unexpectedly, abruptly stops beating
• Often caused by an abnormal heart rhythmcalled ventricular fibrillation (VF)
– VF accounts for half of all cardiac deaths
• Rapid, chaotic heartbeat
• Lower heart chambers, or ventricles,spasm
• Heart functioning stops
• Lack of oxygen in body, brain is dead

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 8/61
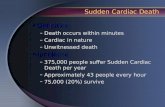
Etiology of Sudden Cardiac Death
• An estimated 13 million people had coronary heart disease (CHD) in the U.S. in 2002. 1
• Sudden death was the first manifestation of CHD in 50% of men and 63% of women.1
• CHD accounts for at least 80% of sudden cardiac deaths in Western cultures.3
1 American Heart Association. Heart Disease and Stroke Statistics2003 Update. Dallas, Tex.: American HeartAssociation; 2002.
2 Adapted from Heikki et al. N Engl J Med , Vol. 345, No. 20, 2001.
3 Myerberg RJ. Heart Disease, A Textbook of Cardiovascular Medicine. 6th ed. P. 895.
Etiology of Sudden Cardiac Death2,3
* ion-channel abnormalities, valvular or congenital heart disease, othercauses
80%Coronary
HeartDisease
15%Cardiomyopathy
5% Other*

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 9/61
SUDDEN CARDIAC DEATH
• Epidemiology– SCD due to Coronary Artery
disease: single most importantcause of death in adult population
–Ventricular Fibrillation: 75-80%–Bradyarrhythmias: minority
– SCD in the absence of CAD, CHF:
5-10% of cases

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 10/61
Arrhythmic Cause of SCD
Albert CM. Circulation. 2003;107:2096-2101.
12%Other CardiacCause
88%
ArrhythmicCause

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 11/61
PrimaryPrimary
VFVF
8%8%
Underlying Arrhythmia of Sudden CardiacArrest
Adapted from Bayés de Luna A. Am Heart J. 1989;117:151-159.
TorsadesTorsades
de Pointesde Pointes
13%13%
Bradycardia17%
VTVT
62%62%

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 12/61
Sustained Monomorphic VT
72-year-old woman with CHD

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 13/61
VF with Defibrillation (12-lead ECG)

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 14/61
Torsades de Pointes

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 15/61
SCA Survival & MortalityData
• At least 335,000 SCA deaths in the U.S.each year
• Only 5 to 10% survive first episode of SCA
• Roughly two-thirds of SCA deaths occurout-of-hospital– 5% estimated survival rate
Seidl K, Senges J. Card Electrophysiol Rev. 2003;7:5-13.
Heart Disease and Stroke Statistics 2005 Update. AHA. www.americanheart.org
Crespo EM, Kim J, Selzman KA. Am J Med Sci. 2005;329:238-246.
Zheng ZJ, et al. Circulation. 2001;104:2158-2163.
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484.

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 16/61
Cummins RO. Annals Emerg Med. 1989;18:1269-1275.
SCA Resuscitation Success vs.Time*
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9
%
Success
*Non-linear
Time (minutes)
Chance of success reduced7 - 10% each minute

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 17/61
Can SCA be Prevented?
• Research and clinical studies haveidentified several conditions that putpatients at a high risk for SCA
• Patients can be evaluated for these known
risk factors before they experience a SCA
• Treatment options are available that canprevent sudden cardiac death

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 18/61
Risk Factors for Sudden CardiacArrest
• Previous Sudden Cardiac Arrest (SCA) Event• Prior Episode of Ventricular Tachyarrhythmia
(VT)
• Previous Myocardial Infarction (MI)
• Coronary Artery Disease (CAD)• Heart Failure
• Genetic diseases
– Long QT Syndrome
–Hypertrophic Cardiomyopathy (HCM)– Brugada Syndrome
– ARVD
– SUDS

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 19/61
Myerburg RJ. Heart Disease, A Textbook of Cardiovascular Medicine, 5th ed, Vol 1.Philadelphia: WB Saunders Co;1997:ch 24.Fogoros RN. Practical Cardiac Diagnosis: Electrophysiologic Testing, 2nd ed. Blackwell Science, pp 172.The AVID Investigators. N Engl J Med. 1997;337:1576-1583.Myerburg RJ. Ann Intern Med.. 1993;119:1187-1197.Demirovic J. Progr Cardiovasc Dis. 1994;37:39-48.Friedlander Y. Circulation. 1998;97:155-160.
Sudden Cardiac Arrest Survivors
• Highest risk factor for Sudden Cardiac Arrest is
a previous SCA event
• 30 to 50% of SCA survivors will experienceanother SCA event within one year
• First-degree relatives of SCA patients have a50% higher risk of MI or primary cardiac arrest

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 20/61
Myerburg RJ. Heart Disease, A Textbook of Cardiovascular Medicine, 5th ed, Vol 1.Philadelphia: WB Saunders Co;1997:ch 24.Fogoros RN. Practical Cardiac Diagnosis: Electrophysiologic Testing, 2nd ed. Blackwell Science, pp172.The AVID Investigators. N Engl J Med. 1997;337:1576-1583.
Prior Episode of VT
• VT with syncope or a low ejection
fraction (LVEF < 40%) leads to anincreased risk of Sudden Cardiac Arrest
• The one-year risk of Sudden CardiacArrest for these patients ranges from 20to 50%

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 21/61
SCA Relationship to MI
• A previous MI can be identified in asmany as 75% of SCA patients.
• A previous MI as a single risk-factorraises the one-year risk of SCA by 5%.
• The five-year risk of SCA is 32% forpatients with all of these risk-factors:• history of MI
• non-sustained, inducible, non-suppressibleVT
• LVEF ≤ 40%
Sudden Cardiac Arrest Fast Facts. HRS. www.hrsonline.org
Risk factors for sudden cardiac death. www.heartinstitute.org.au/Community/scdMain.asp
Buxton AE, et al. N Engl J Med. 1999;341:1882-1890.
Ti D d f M t lit Ri k P t MI

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 22/61
Time Dependence of Mortality Risk Post-MIPrediction of Sudden Cardiac Death After Myocardial Infarction
in the Beta-Blocking Era1
• 700 post-MI patients;~ 95% on beta-blockers2 years after discharge.
• The epidemiologicpattern of SCD wasdifferent from thatreported in previousstudies.
–Arrhythmia events didnot concentrate earlyafter the index event;
most occurred > 18months post-MI.
1 Huikuri HV. J Am Coll Cardiol. 2003;42:652-658.
Total
Mortality
CardiacMortality
Non-SCD
SCDCumulativ e
Events(%)
18
15
12
9
6
3
18
15
12
9
6
3
20
40
60 20
40
60
Follow-Up (months) Follow-Up (months)
l i f i f C fi

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 23/61
14
11.6
8.47.89
8.2
4.9
7.2
0
2
4
6
8
10
12
14
16
1-17 mo 18 - 59 mo 60 - 119 mo > 120 mo
Conv
ICD
(n =300)
(n =283)
(n =284)
(n =292)Hazard
Ratio.98
(p = 0.92)
0.52
(p = 0.07)
0.50
(p = 0.02)
0.62
(p = 0.09)
Wilber, D. Circulation. 2004;109:1082-1084.
Relation of Time from MI to ICD Benefitin the MADIT-II Trial
Time from MI%
Mortalityf or
Each
T
imeP
eriod

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 24/61
SCD Rates in Post-MI Patientswith LV Dysfunction
2119.8
14
10
7
16 16
12 9.4
28
1820
28
0
10
20
30
TRACE CAPRICORN EMIAT MADIT MUSTT
Inducible
MUSTT
Registry
MADIT II*
Control Group Mortality at 2 year
Total Mortality
Arrhythmic Mortality
Total Mortality ~20-30%; SCDaccounts for ~50% of the total deaths.

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 25/61
“People who’ve had a heart attackhave a sudden death rate that is 4-6
times that of the general population.”1
“ People who have had a heart attackand have LV dysfunction (</=40%) havea sudden death rate that’s similar to a
CHF population.”1American Heart Association. Heart Disease and Stroke Statistics2003Update. Dallas, Tex.: American Heart Association; 2002.

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 26/61
SCD in Heart Failure 1, 2
• Despite improvements inmedical therapy, symptomatic
HF still confers a 20-25% riskof premature death in the first2.5 yrs after diagnosis.– ≈ 50% of these premature
deaths are SCD (VT/VF)1 Bardy G. The Sudden Cardiac Deatth-Heart Failure Trial
(SCD-HeFT) in Woosley RL, Singh S, ArrhythmiaTreatment and Therapy, Copyright 2000 by MarcelDekker, Inc. , pp. 323-342,
2 Sweeney MO PACE 2001;24:871-888.

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 27/61
SCA Relationship to HF
• Patients with HF are overall at 6-9 times higherrisk for SCD than general population
• As HF progresses, pump failure (rather than SCA)
becomes relatively more likely as the cause of death
• Reduced LVEF remains the single most important
risk factor for overall mortality and suddencardiac death.
Heart Disease and Stroke Statistics – 2005 Update. AHA. www. americanheart.org
S it f H t F il

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 28/61
Severity of Heart FailureModes of Death
12%
24%64%
CHF
Other
SuddenDeath(N = 103)
NYHA II
26%
15%59%
CHF
Other
SuddenDeath
(N = 103)
NYHA III
56%11%
33%
CHF
Other
SuddenDeath(N = 27)
NYHA IV SCA Pump Failure
NYHA Class II 64% 12%
NYHA Class III 59% 26%
NYHA Class IV 33% 56%

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 29/61
LVEF and SCA Incidence
Vreede-Swagemakers JJ. J Am Coll Cardiol. 1997;30:1500-1505.
LVEF
0
1
2
3
4
5
6
7
8
0-30% 31-40% 41-5 0% > 50%%
SCAV
ictims
7.5%
5.1%
2.8%
1.4%

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 30/61
SCD
•Genetic Basis
– Short QT syndrome
– Long QT Syndrome
– Brugada Syndrome
– Hypertrophic Cardiomyopathy
– Arrhythmogenic Right Ventricular Cardiomyopathy– Catecholaminergic Polymorphic Ventricular
Tachycardia
• Family history is a strong independent predictor of susceptibility to SCD

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 31/61
Schwartz PJ. Curr Probl Cardiol. 1997;22:297-351.Smith WM. Ann Intern Med. 1980;93:578-584.Garson A Jr. Circulation. 1993;87:1866-1872.
Long QT Syndrome
• Congenital disorder that may lead tounexplained syncope, seizures, and SCA
• Either asymptomatic or are prone tosymptomatic and potentially lethal arrhythmias
• 60% have a positive family history of LQTS orSCA
• Necessary to identify other family members atrisk

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 32/61
Long QT Syndrome in a 16-year-old girl

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 33/61
Myerburg RJ. Heart Disease, A Textbook of Cardiovascular Medicine. 5th ed, Vol 1.Philadelphia: WB Saunders Co; 1997:ch 24.Maron BJ. New Engl J Med. 2000;342:365-373.
Hypertrophic Cardiomyopathy
• SCD is the most common cause of death
• Prevalence is about 0.2% of the general populationand about 10% of HCM patients are considered tobe at high risk of SCA
• Over a ten year period > 50% of high-risk patients
would experience SCA
• Most common cause of SCA in athletes under age35

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 34/61
Arrhythmogenic RVDysplasia
• RV myocardium isprogressively replacedby fibrofatty tissue. LV isnormal
• LBBB morphology
• High risk of SCD if arrhythmias are leftuncontrolled
• Risk stratification isimportant
• Tx: Drugs, ICD, ablation
• Prevent arrhythmicdeath influenced byautonomic tone
Zipes and Jalife, 2001

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 35/61
Arrhythmogenic RV Cardiomyopathy

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 36/61
Brugada Syndrome
• ECG pattern of ST segmentelevation in V1 to V3 withRBBB morphology and
syncopal or sudden deathepisodes in patients withstructurally normal hearts
• Male predominance

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 37/61
Brugada Syndrome

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 38/61
Brugada Syndrome• Incidence
–Ubiquitous
–Cause of 4-12% of all sudden deaths
• Prevalence ?
• Pharmacologic maneuvers with Nablockers (Ajmaline, Flecainide,Procainamide) may unmask abnormalECG

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 39/61

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 40/61
Brugada Syndrome
• Etiology and Genetics
• SCN5A mutation
–Encodes Na channel
• Autosomal dominant pattern
• Males more prone to
phenotype (typical ECG andventricular arrhythmias)

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 41/61
Brugada Syndrome
• Na channel blockers worsenECG findings
• Isoproterenol controls
electrical storm• Prognosis and Treatment:
–Poor if left untreated
– ICD: Treatment of choice

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 42/61

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 43/61
SUDS
• 1997 Dr. KoonlaweeNademanee
• Thailand: “Lai Tai”• Japan: “Pokkuri”
• Philippines: “Bangungut”
• “Dying in their sleep”

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 44/61
SUDS
• Clinical Presentation:–Agonal respiration
–Unresponsiveness afterlabored respiration duringsleep or seizure-like
symptoms–Normal cardiac function

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 45/61
SUDS & Brugada
• No organic heart disease
• Males exclusively
•High incidence of induciblepolymorphic VT to VF
• High mortality rate
• Normalization of ECG on exercise• EP mechanism same ??

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 46/61
Treatment Options for SCA
• Defibrillation is theonly effectivetreatment for SCA
• VF tends to rapidlydeteriorate intoasystole
• Asystole cannot besuccessfully treated
with defibrillation

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 47/61
• Small devices, pectoralimplant site
• Transvenous, single incision
• Local anesthesia; conscious sedation
• Short hospital stays
• Few complications
• Perioperative mortality < 1%
• Programmable therapy options
• Single- or dual-chamber therapy
• Battery longevity up to 9 years
• 80,000 implants/year (2000 E)1
Implantable Cardioverter Defibrillator
First-line therapy for patients at risk for SCA
1Morgan Stanley Dean Witter. Investors Guide to ICDs. 2000.
Key Randomized Clinical

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 48/61
Key Randomized ClinicalTrials
Adapted from: DiMarco JP. N Engl J Med . 2003;349:1836-47. www.medscape.com
Young JB. Sudden cardiac death in heart failure. www.medscape.com
ICD therapy for the secondary prevention of SCA
Mortality
(%)
Trial N Age (yrs) Mean LVEF(%)
Follow-up(mos)
ControlTherapy
Control ICD P
AVID 1016 65 ± 10 35 18 ± 12 Amiodarone or sotalol
24.0 15.8 .02
CIDS 659 64 ± 9 34 36 Amiodarone 29.6 25.3 .14
CASH 288 58 ± 11 45 57 ± 34 Amiodarone or metoprolol
44.4 36.4 .08

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 49/61
2006 ACC/AHA/ESC Guidelines for theManagement of Ventricular Arrhythmias:
Secondary Prevention of SCD
ICD Class I Recommendation:• Patients with a history of SCA, VF,
hemodynamically unstable VT, or unexplainedsyncope
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 50/61
Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.
Patients with a previous cardiac arrest are at high risk for subsequent SCA
events but account for a small percentage of annual sudden deaths
MADIT I, MUSTT
AVID, CASH,
CIDS
SCD-HeFT,MADIT II

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 51/61
Key Randomized Clinical Trials
Adapted from: DiMarco JP. N Engl J Med. 2003;349:1836-47. www.medscape.com
Kadish A, et.al. N Engl J Med 2004;350:2151-8.
Young JB. Sudden cardiac death in heart failure. www.medscape.com
ICD therapy for the primary prevention of SCAMortality (%)
Trial N Age(yrs)
MeanLVEF (%)
Follow-up(mos)
ControlTherapy
Control ICD P
SCD-HeFT 2521 60.1 25 45.5 Optimal
MedicalTherapy
36.1 28.9 .007
MADIT 196 63 ± 9 26 27 Conventional 38.6 15.7 .009
MADIT II 1232 64 ± 10 23 20 OptimalMedicalTherapy
19.8 14.2 .007
MUSTT 704 67 ± 12 30 39 No EP-guidedtherapy 48 24 .06
DEFINITE 458 58 21 29.0±14.4 OptimalMedicalTherapy
14.1 7.9 .08
Heart Failure and Left Ventricular Dysfunction are

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 52/61
Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.
Heart Failure and Left Ventricular Dysfunction are
indicators of SCA risk
MADIT I, MUSTT
AVID, CASH,CIDS
SCD-HeFT,MADIT II
2006 ACC/AHA/ESC Guidelines for the

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 53/61
2006 ACC/AHA/ESC Guidelines for theManagement of Ventricular Arrhythmias: Primary
Prevention of SCD
ICD Class I Recommendations:• Patients with ischemic cardiomyopathy who are at least 40
days post-MI with an LVEF ≤ 30 - 40% and NYHA functionalclass II or III
• Patients with NYHA Class II-III, LVEF ≤ 30 - 35%, non-ischemiccardiomyopathy
• Patients who are at high risk of SCA due to genetic disorderssuch as long QT syndrome, Brugada syndrome, hypertrophiccardiomyopathy and arrhythmogenic right ventricular dysplasia(ARVD).
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484
2006 ACC/AHA/ESC Guidelines for the

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 54/61
2006 ACC/AHA/ESC Guidelines for theManagement of Ventricular Arrhythmias: Primary
Prevention of SCD
ICD Class II Recommendation:• Ischemic and non-ischemic patients with NYHA functional
class I, LVEF ≤ 30-35%
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484
Many methods to further risk stratify patients

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 55/61
Many methods to further risk stratify patientsrisk for SCA have been studied...
Test Objective Sensitivity
(%)
Specificity
(%)
Limitations
Echo Measurement of LVEF
55–65 75–80
HR
variability
Assessment of lowheart rate variability
38–62 75–88 Multiple non-standardized methods
EP Study Induction of VA’s 48–73 65–93 Invasive, expensive
Signal
AveragedECG
(SAECG)
Induction of latepotentials
56-68 74–81 Not useful in non-ischemic cardiomyopathy
Microvolt
T-WaveAlternans(MTWA)
Identification of
repolarizationabnormalities
77–93 37–83 Cannot be used in AF
Siddiqui A, Kowey PR. Curr Opin Cardiol. 2006;21:517-25.
Prior SG, et al. Eur Heart J, Vol 22:16:August 2001
But a reduced EFremains the singlemost important riskfactor for overallmortality and suddencardiac death.
E l ti P ti t t Ri k f SCA

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 56/61
Evaluating Patients at Risk for SCA
• Electrophysiology Studies (EPS) have been helpful
in the diagnosis of cardiac arrhythmias including:– Sinus and AV node dysfunction
– Conduction abnormalities
– Accessory pathways of conduction
– Inducibility of VT
• EPs can provide advanced treatments includingImplantable Cardioverter Defibrillators (ICDs) and
ablation therapy

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 57/61
Conclusions
• The key to SCD prevention is to identifyhigh risk patients BEFORE they have aSCA event. The majority of cases are in
patients with:
– Coronary artery disease, previous MI
– Low left ventricular ejection fraction
– Dilated cardiomyopathy and heart failure

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 58/61
INTERACTIVE SESSION
Which is NOT a recognized risk factor

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 59/61
Which is NOT a recognized risk factorfor SCD?
a. Short QT interval
b. Brugada Syndrome
c. Hypertrophic Cardiomyopathy
d. Family History of SCD
li i l t ti f SUDS

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 60/61
clinical presentation of SUDSexcept:
a. agonal respiration
b. unresponsiveness afterlabored respiration duringsleep or seizure-like
symptomsc. Depressed cardiac function

8/7/2019 A5 - Sudden Cardiac Death
http://slidepdf.com/reader/full/a5-sudden-cardiac-death 61/61
Thank You