

Sudden cardiac-death-1215093819502124-8
67
Sudden Cardiac Death Sudden Cardiac Death Rosco Gore Rosco Gore
-
Upload
dr-khalid-hasan-khan -
Category
Documents
-
view
26 -
download
0
Transcript of Sudden cardiac-death-1215093819502124-8
Sudden Cardiac DeathSudden Cardiac Death
Rosco GoreRosco Gore
DefinitionDefinition
The natural death from cardiac The natural death from cardiac causes, heralded by abrupt loss of causes, heralded by abrupt loss of consciousness within 1 hour of the consciousness within 1 hour of the onset of an acute change in onset of an acute change in cardiovascular status. cardiovascular status.
Epidemiology Epidemiology
300,000 cases per year300,000 cases per year 1-2/10001-2/1000 Bimodal distributionBimodal distribution
CausesCauses
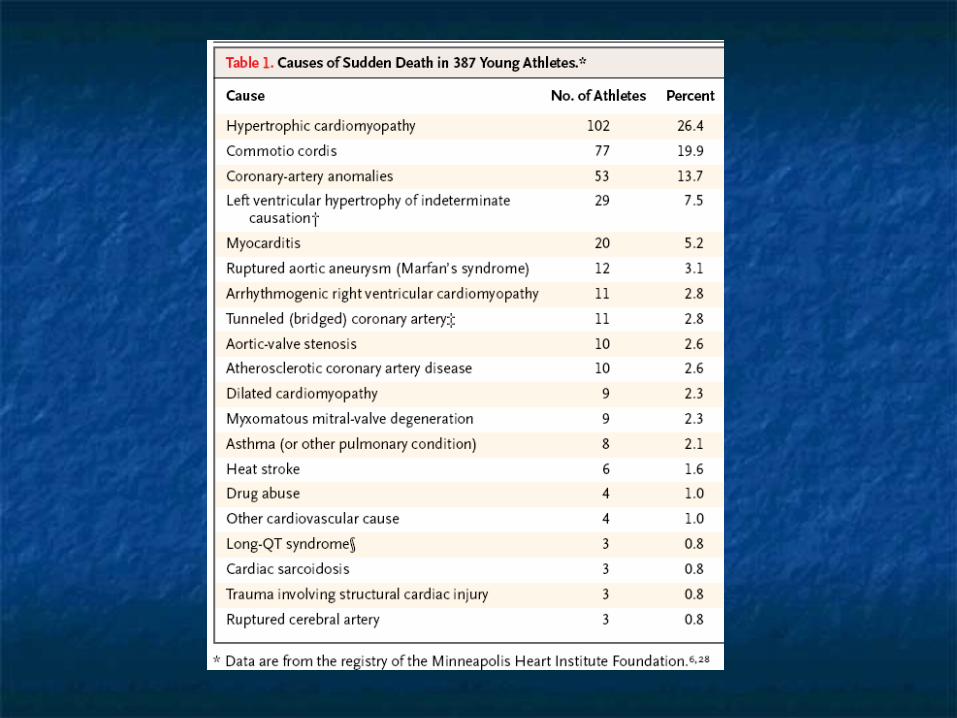
Long QT SyndromeLong QT Syndrome Brugada SyndromeBrugada Syndrome Hypertrophic Cardiomyopathy Hypertrophic Cardiomyopathy Arrhythmogenic Right Ventricular Arrhythmogenic Right Ventricular
Dysplasia Dysplasia Commotio Cordis Commotio Cordis Coronary AnomalyCoronary Anomaly
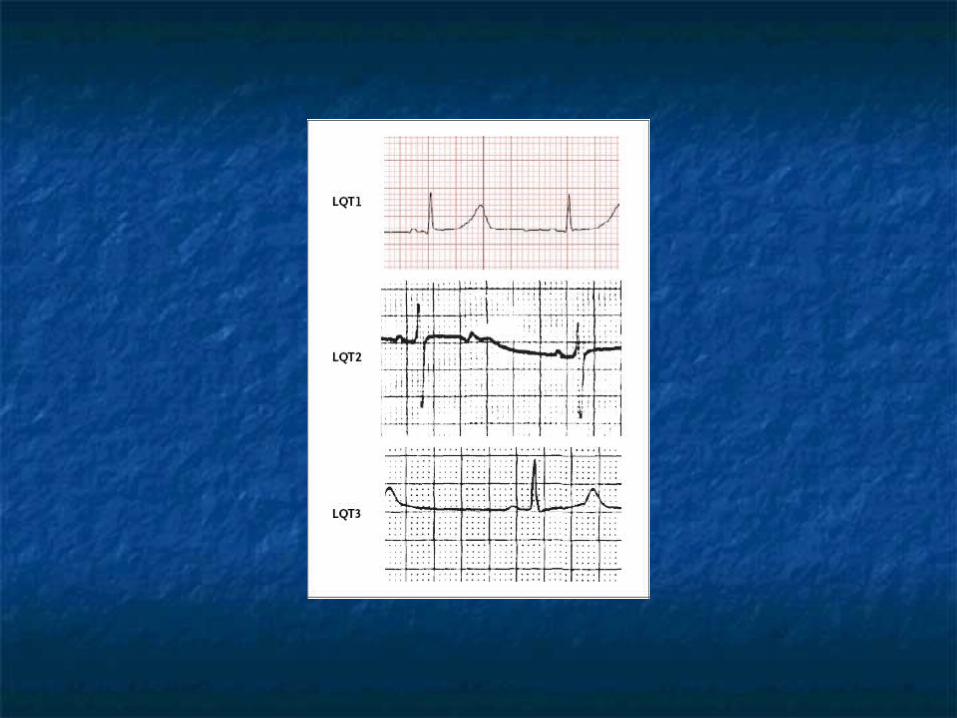
Long QT SyndromeLong QT Syndrome
Autosomal Dominate- Romano-WardAutosomal Dominate- Romano-Ward Autosomal Recessive- Jervell and Autosomal Recessive- Jervell and
Lange-NielsenLange-Nielsen AcquiredAcquired 1/10,0001/10,000
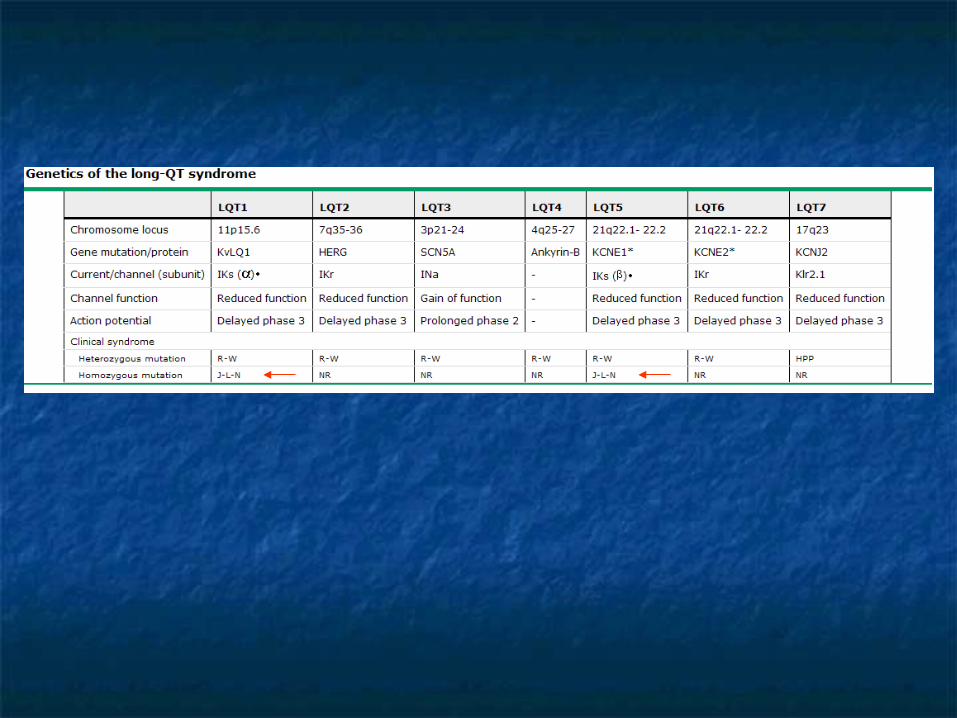
GeneticsGenetics
Underlying mutations determine Underlying mutations determine phenotypic expressionphenotypic expression
Variable penetranceVariable penetrance Compound mutationsCompound mutations
PresentationPresentation
Palpitations, Presyncope, Syncope, Palpitations, Presyncope, Syncope, Seizures, or Cardiac arrestSeizures, or Cardiac arrest
Asymptomatic prolonged QTcAsymptomatic prolonged QTc Referred by family membersReferred by family members Has a predilection for younger Has a predilection for younger
patientpatient
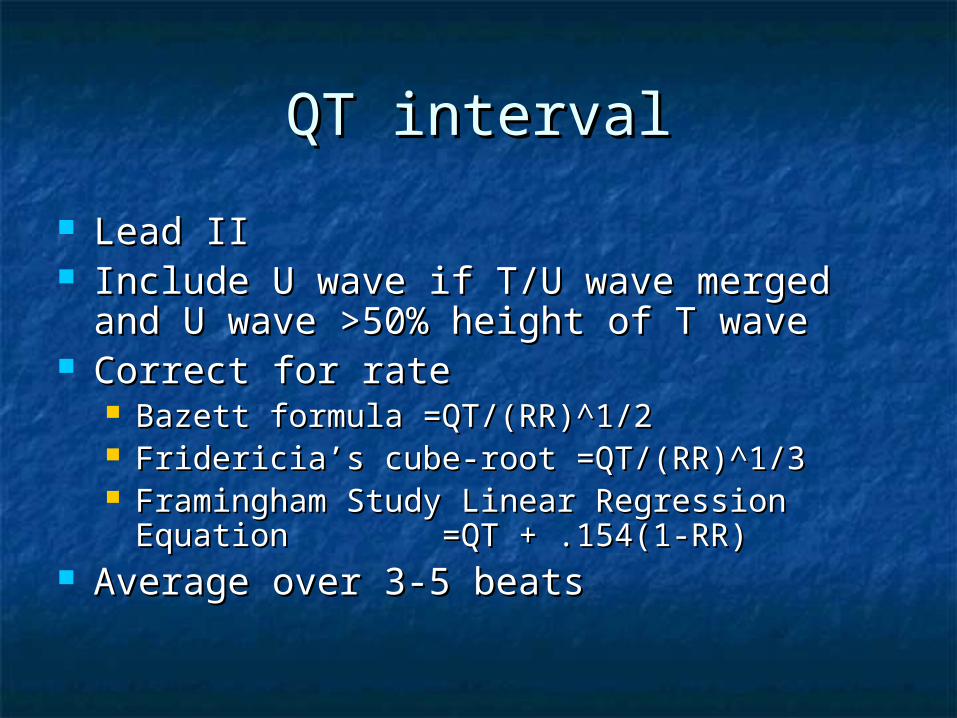
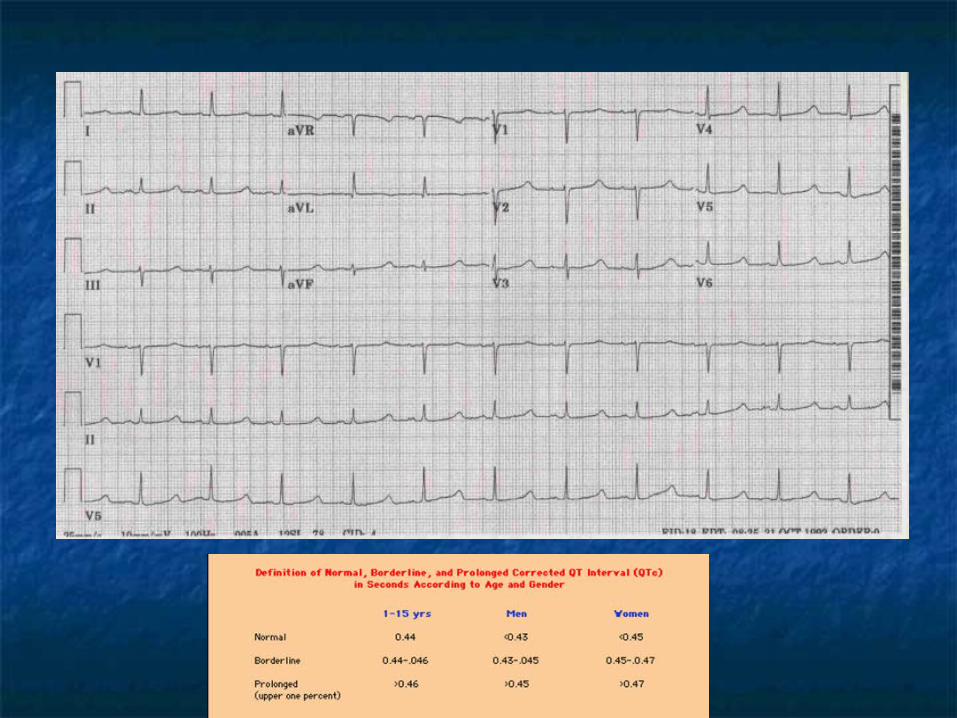
QT intervalQT interval
Lead IILead II Include U wave if T/U wave merged and U Include U wave if T/U wave merged and U
wave >50% height of T wavewave >50% height of T wave Correct for rateCorrect for rate
Bazett formula =QT/(RR)^1/2Bazett formula =QT/(RR)^1/2 Fridericia’s cube-root =QT/(RR)^1/3Fridericia’s cube-root =QT/(RR)^1/3 Framingham Study Linear Regression Equation Framingham Study Linear Regression Equation
=QT + .154(1-RR) =QT + .154(1-RR) Average over 3-5 beatsAverage over 3-5 beats
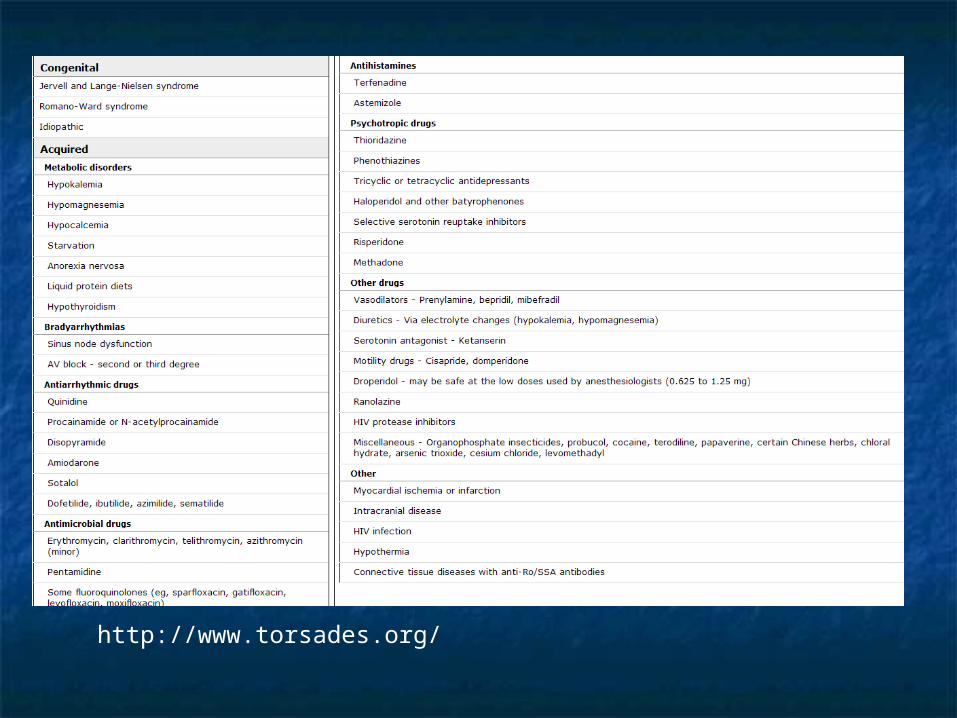
http://www.torsades.org/
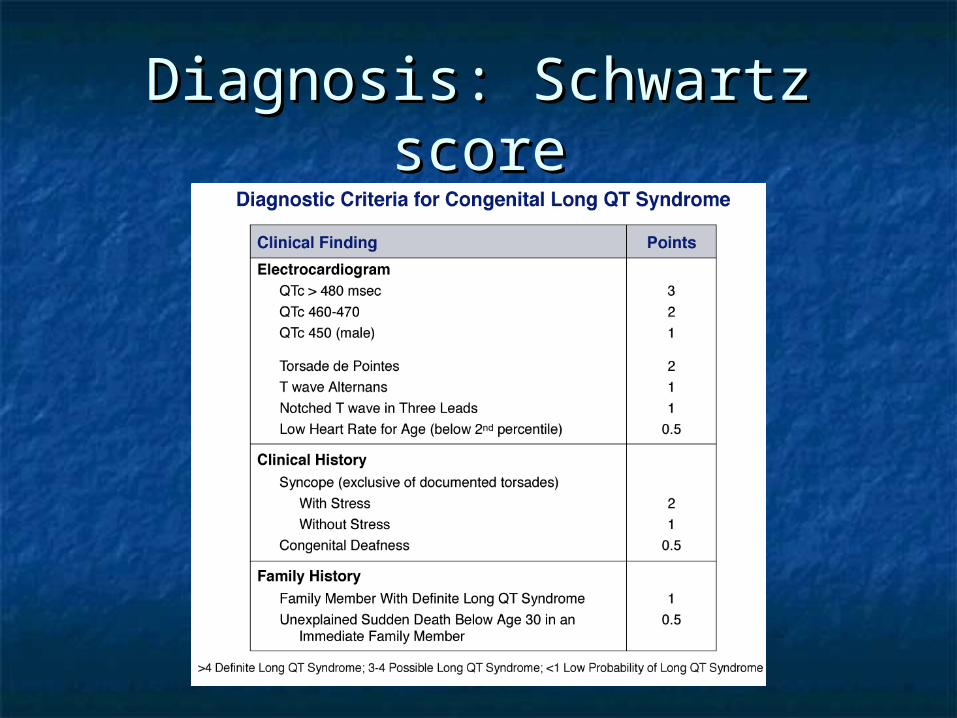
Diagnosis: Schwartz scoreDiagnosis: Schwartz score
PrognosisPrognosis
Events increase w/ increasing QTcEvents increase w/ increasing QTc
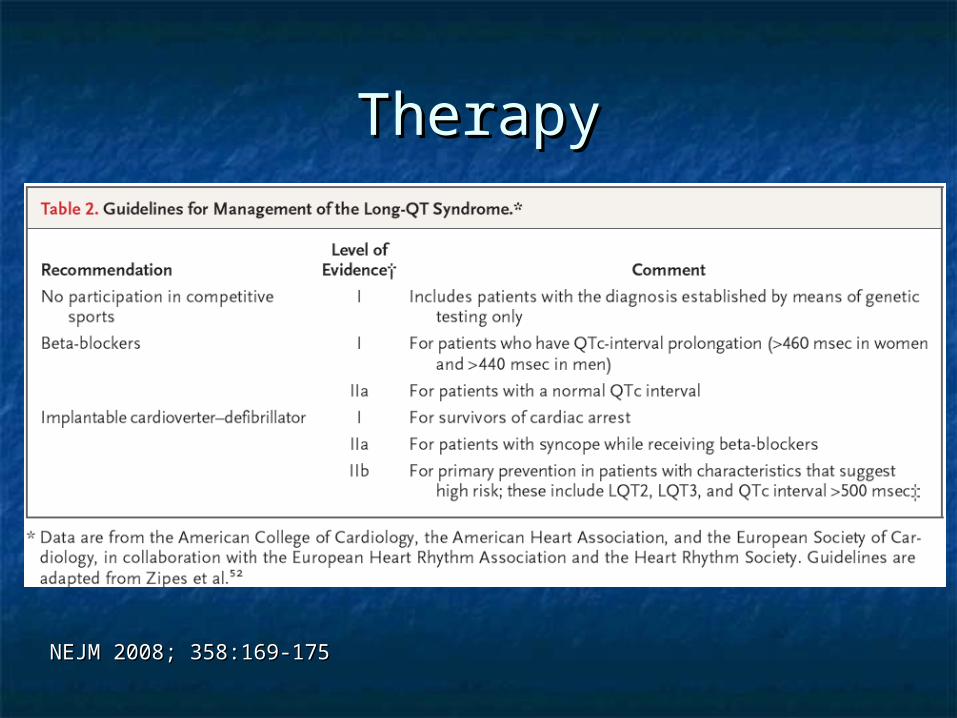
TherapyTherapy
NEJM 2008; 358:169-175NEJM 2008; 358:169-175
Brugada SyndromeBrugada Syndrome
Autosomal dominate defect in Autosomal dominate defect in cardiac Na channels- variable cardiac Na channels- variable expressionexpression
0.4% US population0.4% US population Male predominanceMale predominance Average age of Dx=41Average age of Dx=41
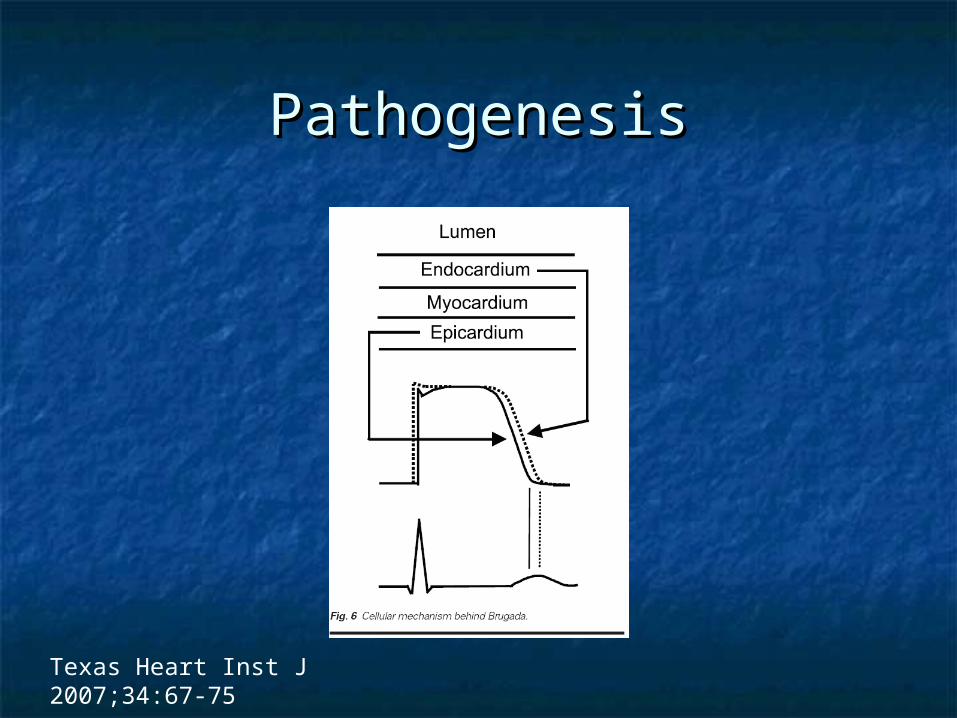
PathogenesisPathogenesis
Texas Heart Inst J 2007;34:67-75
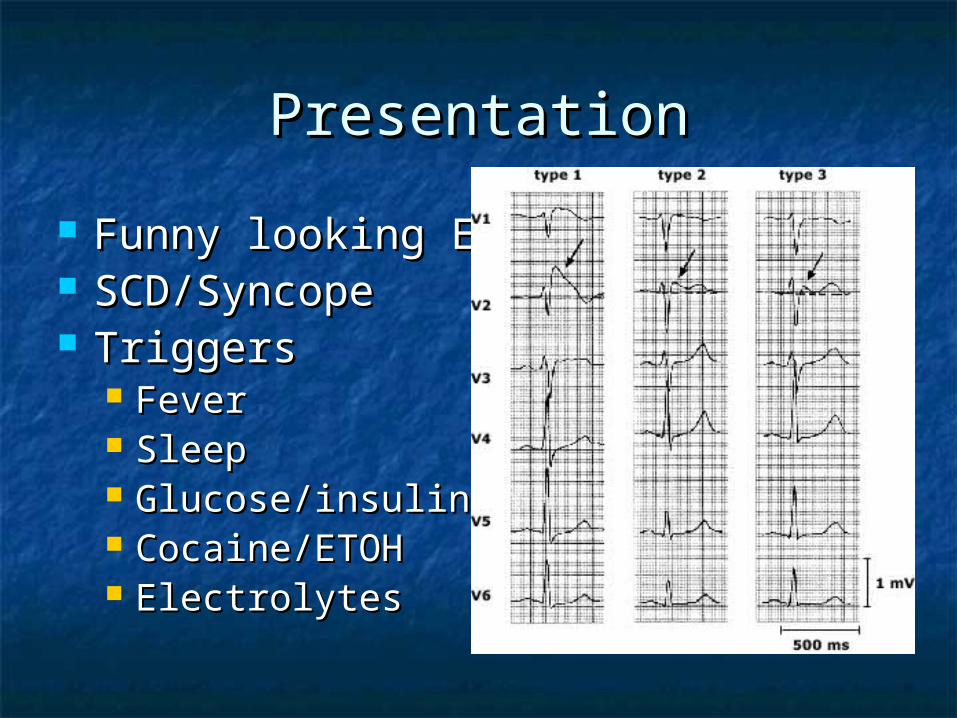
PresentationPresentation
Funny looking EGKsFunny looking EGKs SCD/Syncope SCD/Syncope TriggersTriggers
FeverFever SleepSleep Glucose/insulinGlucose/insulin Cocaine/ETOHCocaine/ETOH ElectrolytesElectrolytes
Unmasking AgentsUnmasking Agents
Na channel blockersNa channel blockers Calcium Channel blockersCalcium Channel blockers Beta blockersBeta blockers NitratesNitrates TricyclicsTricyclics SSRISSRI
DiagnosisDiagnosis
Type I ST pattern + one ofType I ST pattern + one of Documented ventricular fibrillation Documented ventricular fibrillation Self-terminating polymorphic ventricular Self-terminating polymorphic ventricular
tachycardia (VT) tachycardia (VT) Family history of sudden cardiac death at <45 years Family history of sudden cardiac death at <45 years Type 1 ST segment elevation in family members Type 1 ST segment elevation in family members Electrophysiologic inducibility of VT Electrophysiologic inducibility of VT Unexplained syncope suggestive of a Unexplained syncope suggestive of a
tachyarrhythmia tachyarrhythmia Nocturnal agonal respiration Nocturnal agonal respiration
Type II or III pattern + conversion to type I Type II or III pattern + conversion to type I +one of the above+one of the above
PrognosisPrognosis
SCD or VFSCD or VF SyncopeSyncope Type I patternType I pattern
TreatmentTreatment
ACC/AHA- AICDACC/AHA- AICD Class I- Pt w/ previous cardiac arrestClass I- Pt w/ previous cardiac arrest Class IIa- Pt w/ previous syncopeClass IIa- Pt w/ previous syncope Class IIa- Pt w/ previous VTClass IIa- Pt w/ previous VT
Quinidine and hydroguinidineQuinidine and hydroguinidine
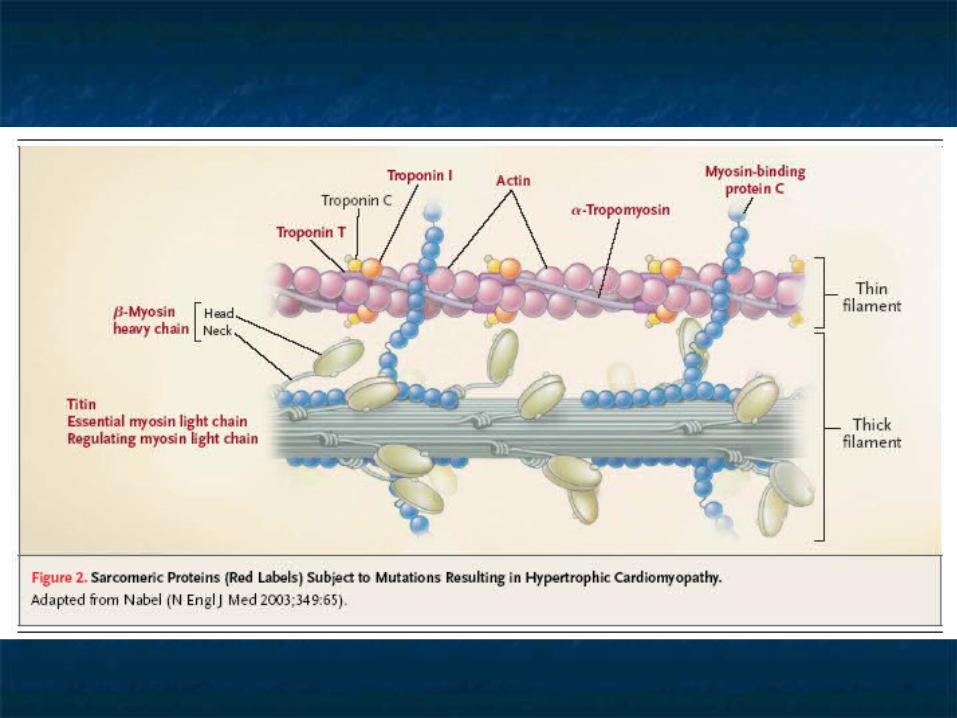
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
AD defect in the myocardial AD defect in the myocardial contractile proteinscontractile proteins
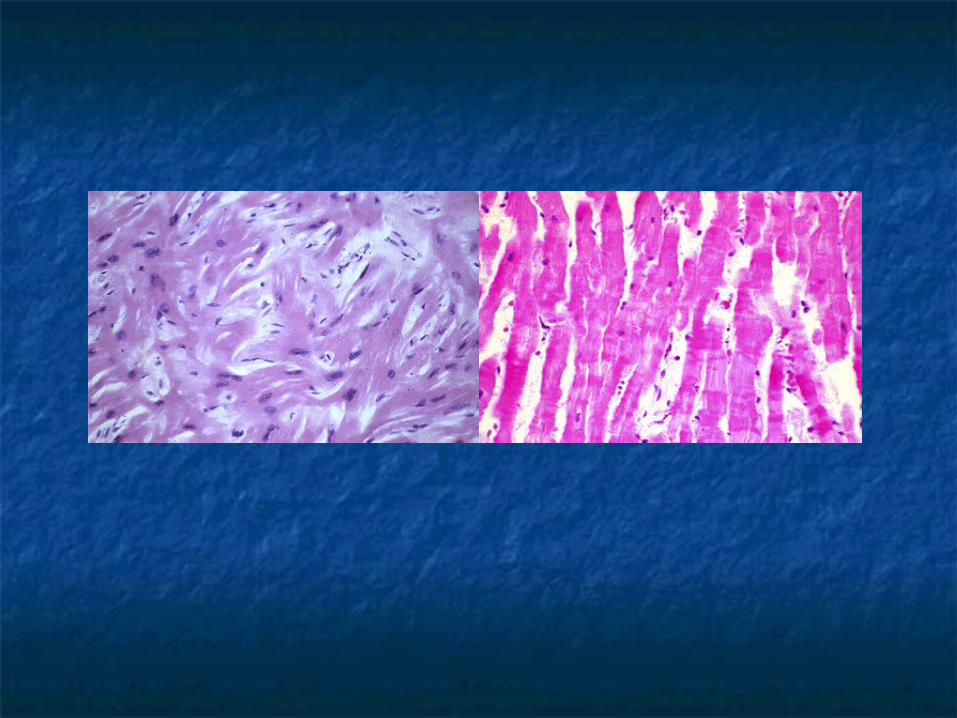
Defective sarcomers->Myocyte Defective sarcomers->Myocyte dissaray->…Ventricular hypertrophydissaray->…Ventricular hypertrophy
0.16-0.29% US population0.16-0.29% US population
PresentationPresentation
SCDSCD DOEDOE SyncopeSyncope Heart failureHeart failure Chest PainChest Pain PalpitationPalpitation AsymptomaticAsymptomatic
Physical ExamPhysical Exam
Systolic Crescendo-decrescendo Systolic Crescendo-decrescendo murmur LLSB/apexmurmur LLSB/apex
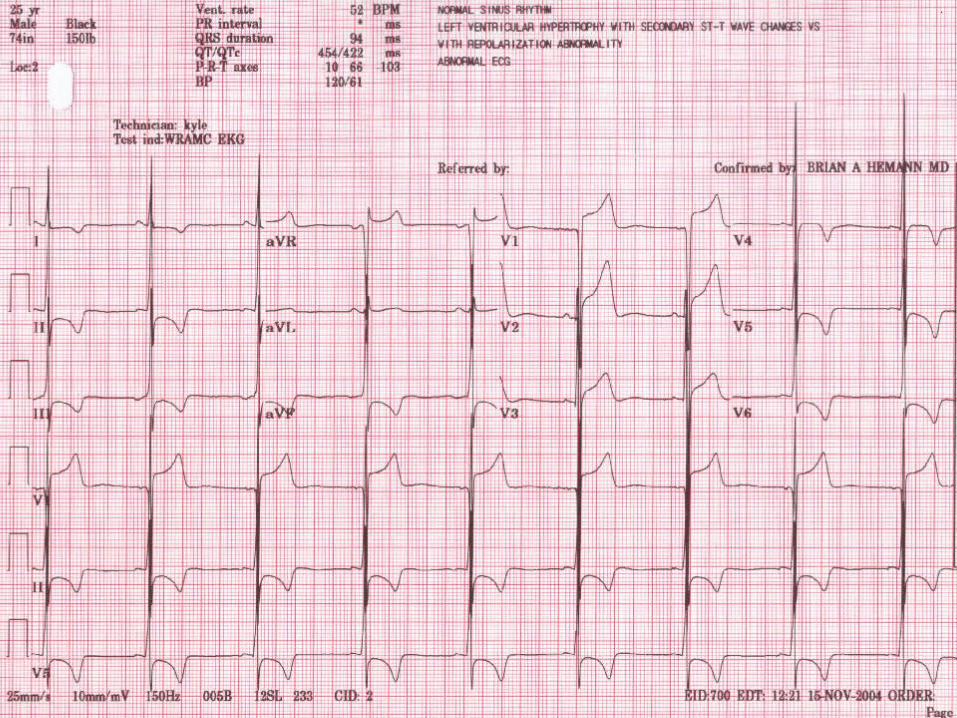
Decreases w/ squatting, hand dripDecreases w/ squatting, hand drip Increase w/ standingIncrease w/ standing Bifid pulsesBifid pulses EKG-LVHEKG-LVH
Ventricular ArrhythmiasVentricular Arrhythmias
Contributing factorsContributing factors Myocardial hypertrophyMyocardial hypertrophy Myocardial disarrayMyocardial disarray Myocardial fibrosisMyocardial fibrosis Myocardial ischemiaMyocardial ischemia Autonomic disturbanceAutonomic disturbance
SCDSCD 1% annual incidence1% annual incidence
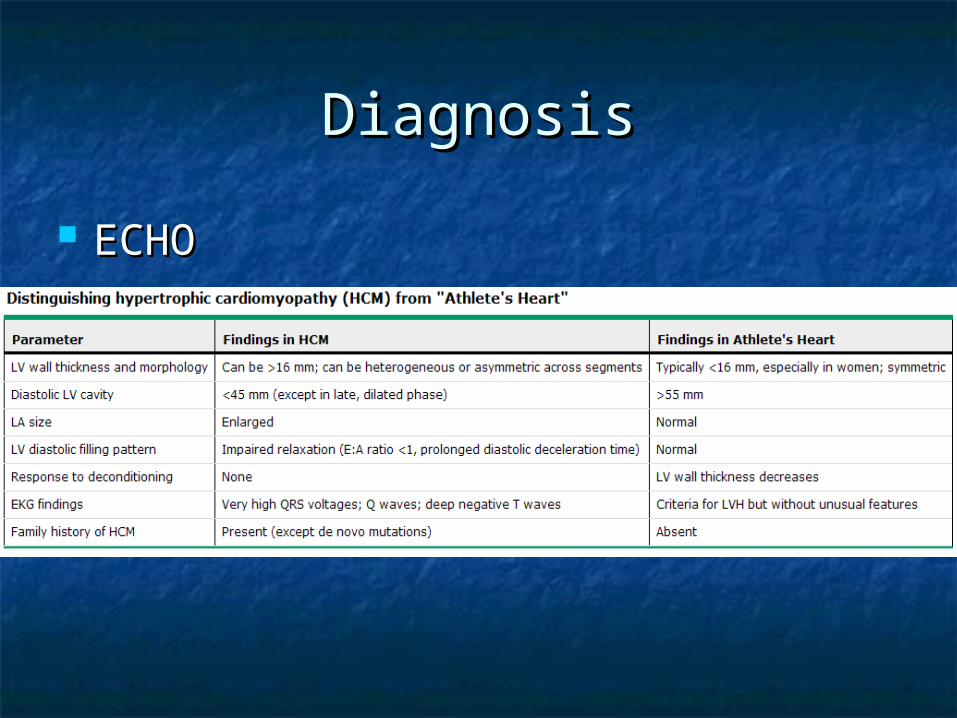
DiagnosisDiagnosis
ECHOECHO
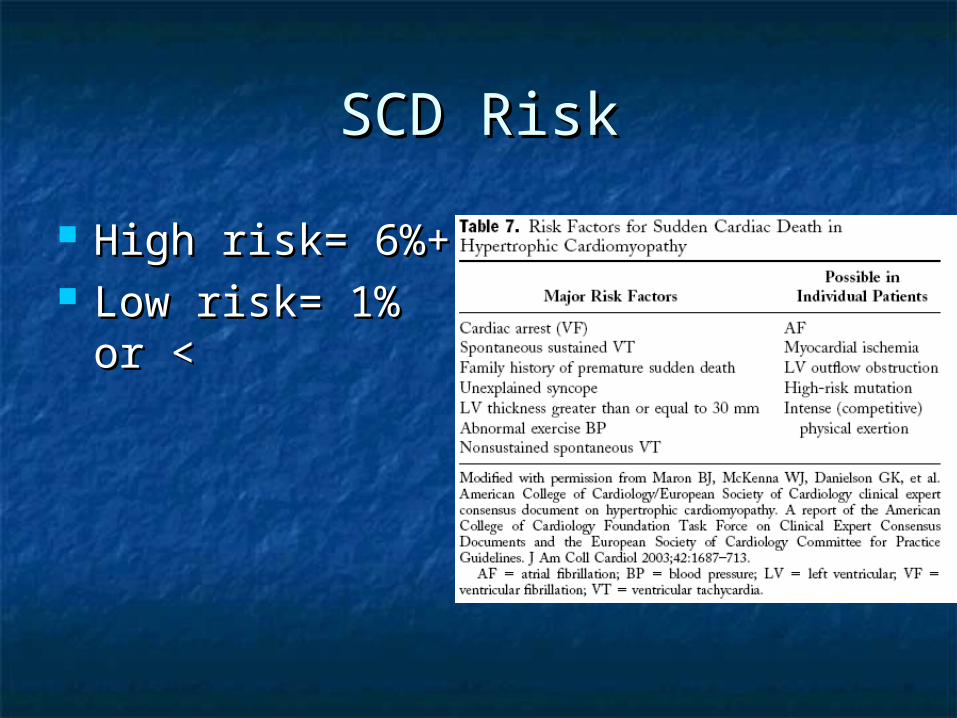
SCD RiskSCD Risk
High risk= 6%+High risk= 6%+ Low risk= 1% or Low risk= 1% or
<<
TreatmentTreatment
PharmocologicPharmocologic VerapamilVerapamil Beta blockersBeta blockers DisopyramidDisopyramid
ICDICD Class I- h/o sustained VT/VFClass I- h/o sustained VT/VF One or more major risk factorOne or more major risk factor
Ablation/SurgeryAblation/Surgery
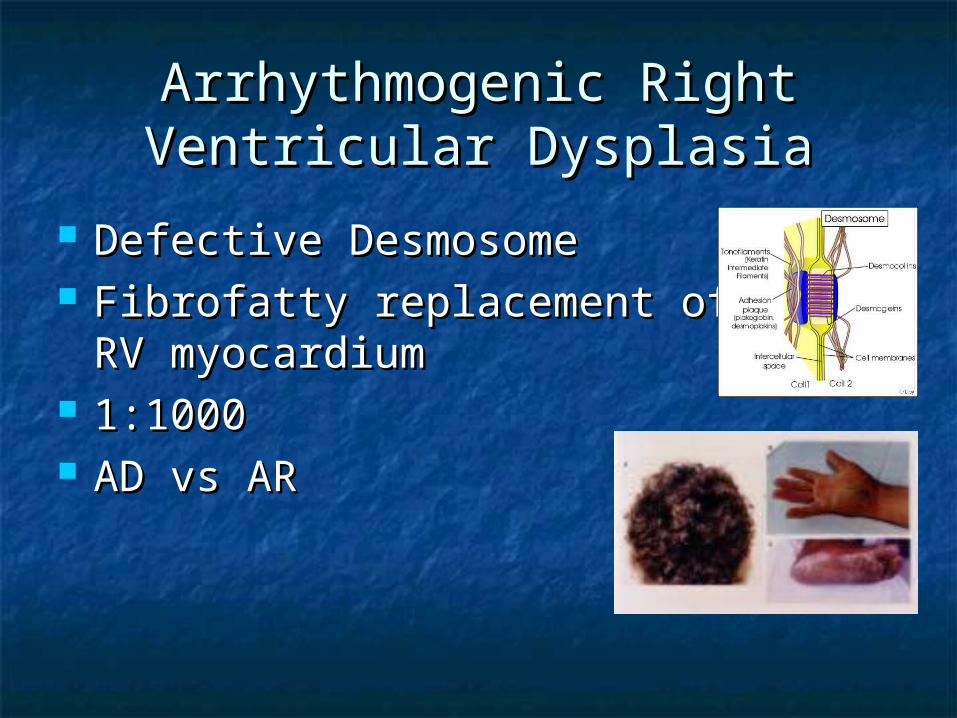
Arrhythmogenic Right Arrhythmogenic Right Ventricular DysplasiaVentricular Dysplasia
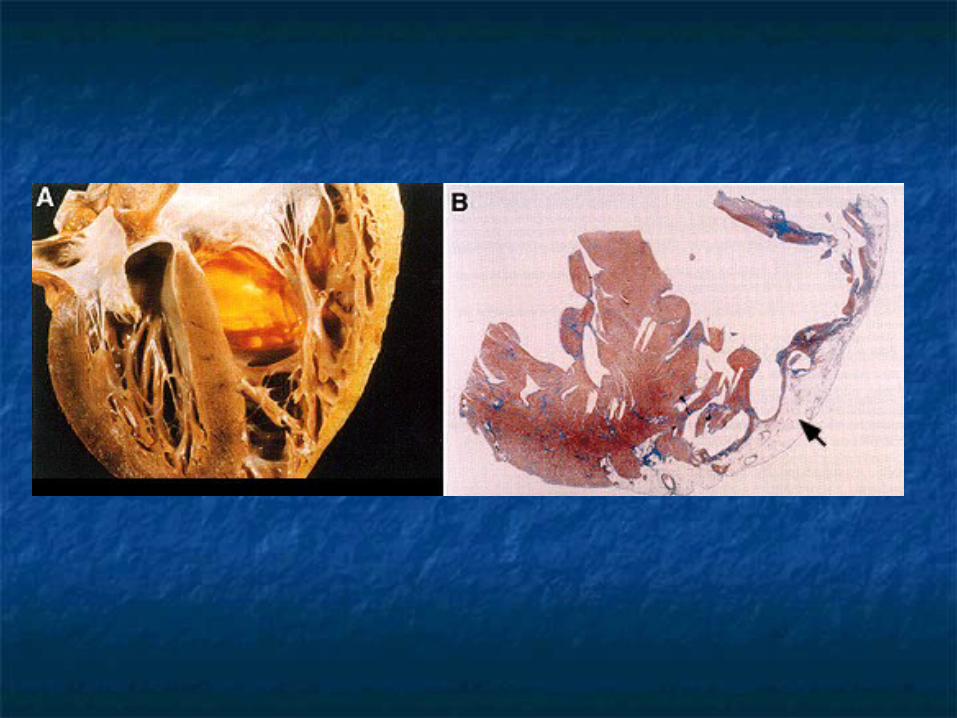
Defective DesmosomeDefective Desmosome Fibrofatty replacement of the RV Fibrofatty replacement of the RV
myocardiummyocardium 1:10001:1000 AD vs ARAD vs AR
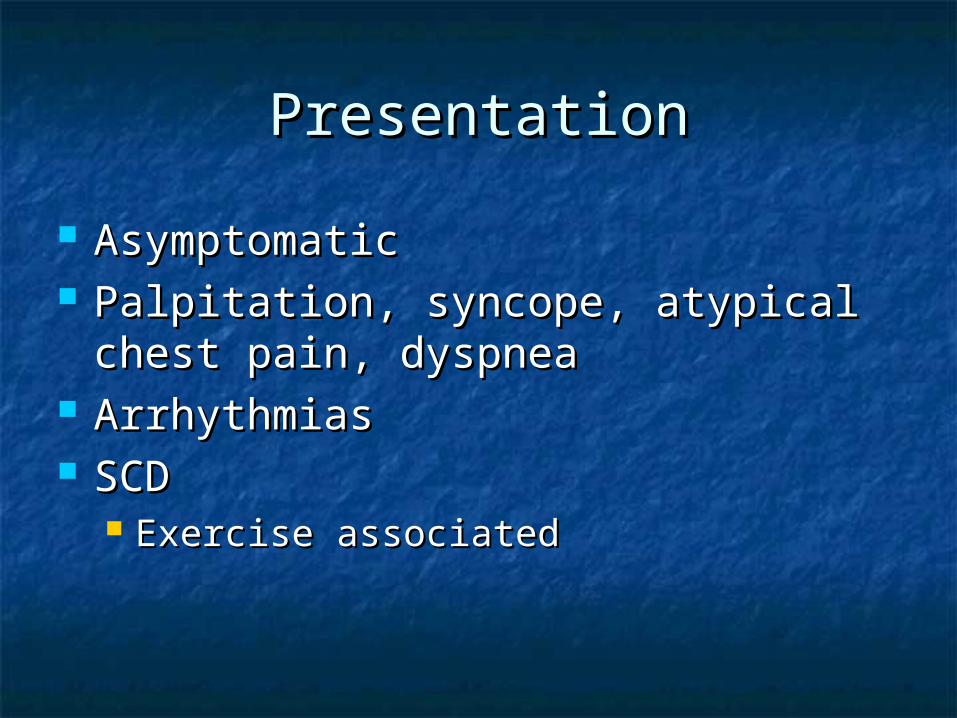
PresentationPresentation
AsymptomaticAsymptomatic Palpitation, syncope, atypical chest Palpitation, syncope, atypical chest
pain, dyspneapain, dyspnea ArrhythmiasArrhythmias SCDSCD
Exercise associatedExercise associated
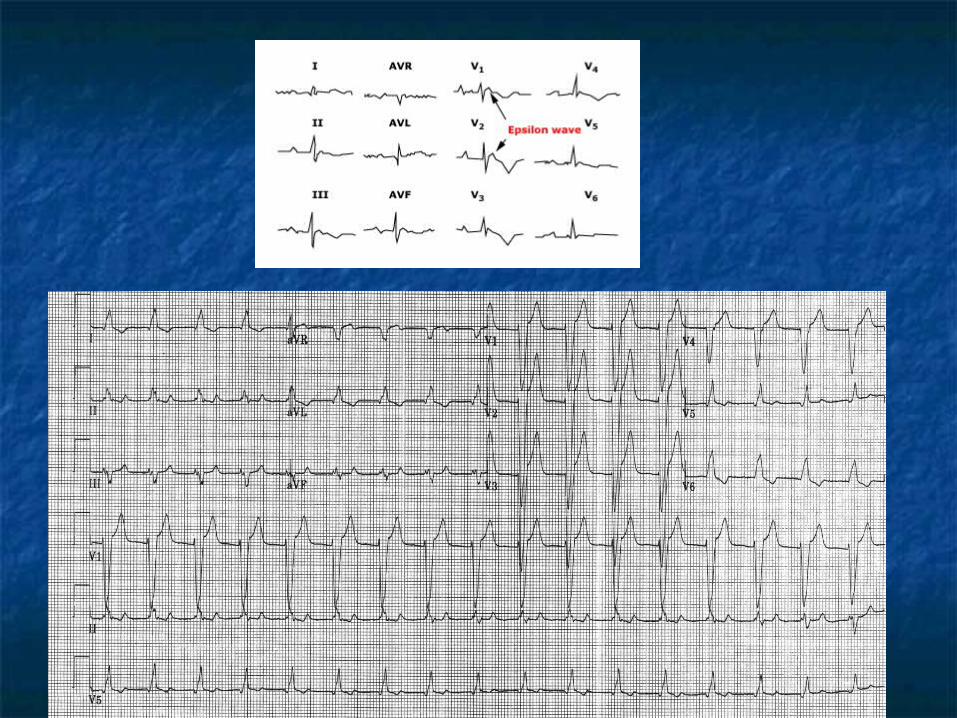
DiagnosisDiagnosis
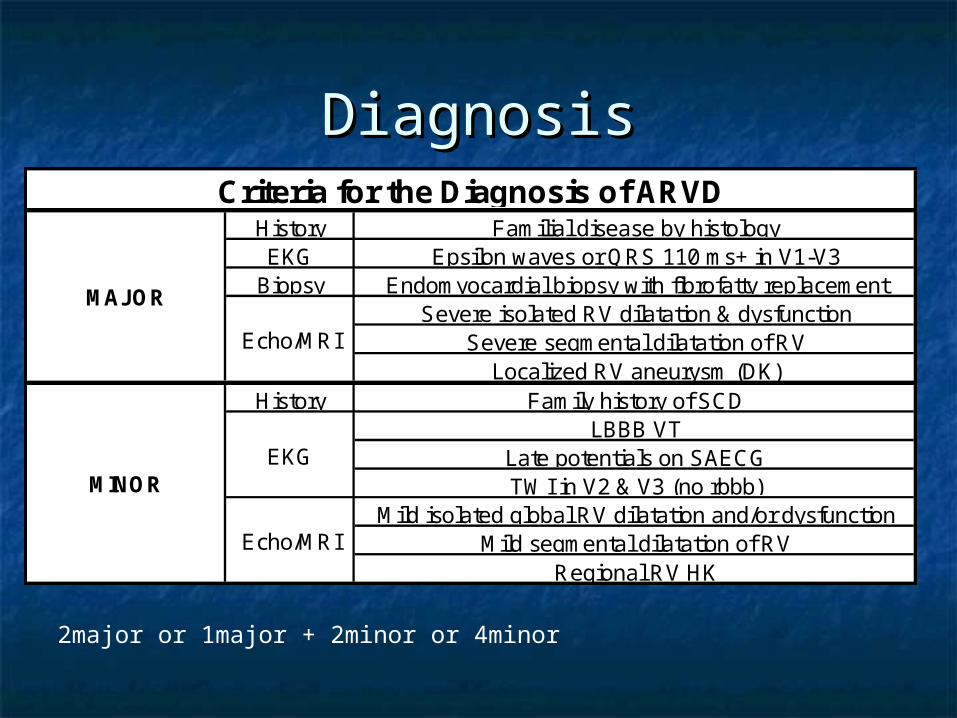
History Familial disease by histologyEKG Epsilon waves or QRS 110 ms+ in V1-V3
Biopsy Endomyocardial biopsy with fibrofatty replacementSevere isolated RV dilatation & dysfunction
Severe segmental dilatation of RVLocalized RV aneurysm (DK)
History Family history of SCDLBBB VT
Late potentials on SAECGTWI in V2 & V3 (no rbbb)
Mild isolated global RV dilatation and/or dysfunctionMild segmental dilatation of RV
Regional RV HKEcho/MRI
MINOR
Criteria for the Diagnosis of ARVD
MAJOR
Echo/MRI
EKG
2major or 1major + 2minor or 4minor
TreatmentTreatment
ICD: ICD: Class I: History of sustained VT/VFClass I: History of sustained VT/VF Class IIa: extensive disease, LV Class IIa: extensive disease, LV
involvement, family members w/ SCD, involvement, family members w/ SCD, syncopesyncope
Amiodarone or Sotalol-Class IIAAmiodarone or Sotalol-Class IIA Ablation-Class IIAAblation-Class IIA
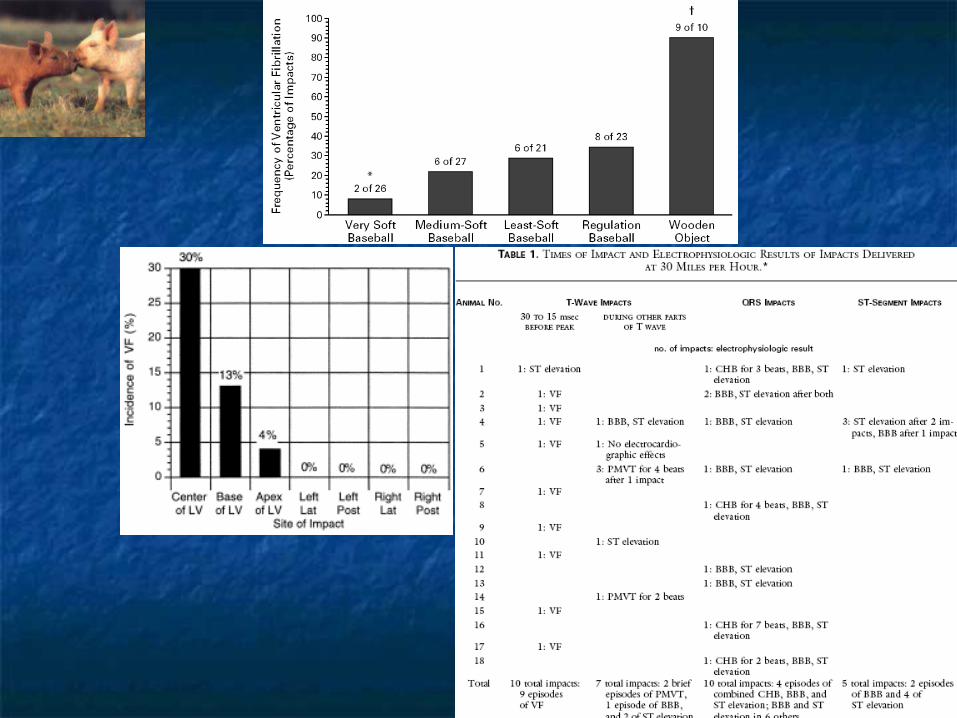
Commotio Cordis Commotio Cordis
SCD due to low-impact precordial SCD due to low-impact precordial traumatrauma
Male predominance, young ageMale predominance, young age High mortalityHigh mortality Probability related to speed, time, Probability related to speed, time,
hardness of object and location of hardness of object and location of impactimpact

Commotio cordisCommotio cordis
TreatmentTreatment CPRCPR ShockShock
PreventionPrevention Safety baseballsSafety baseballs Chest protectorsChest protectors
Follow upFollow up EKGEKG HolterHolter EchoEcho
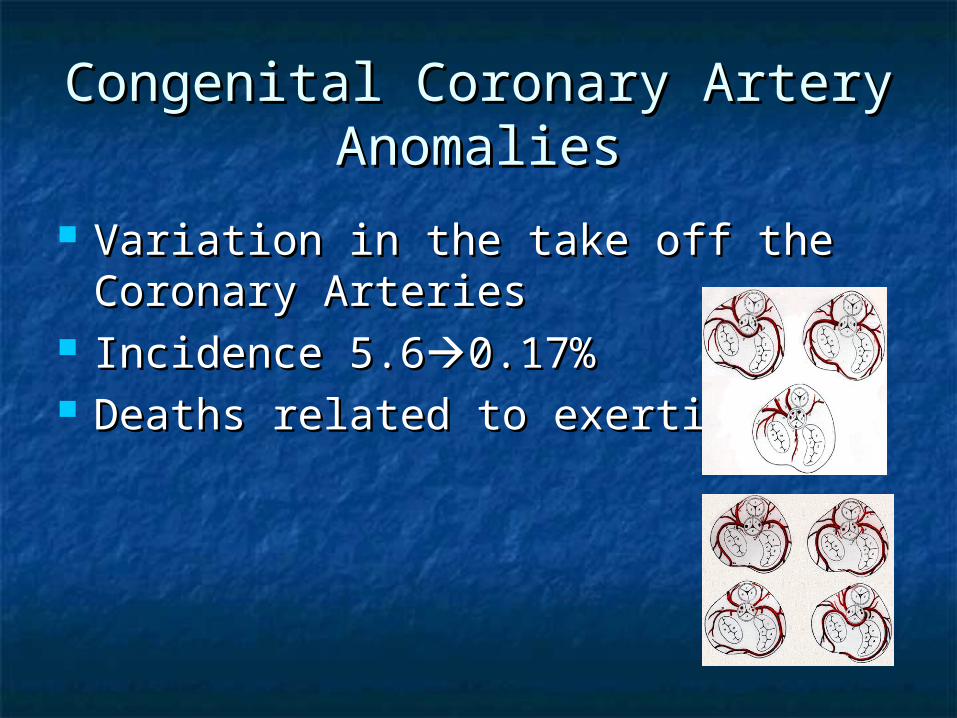
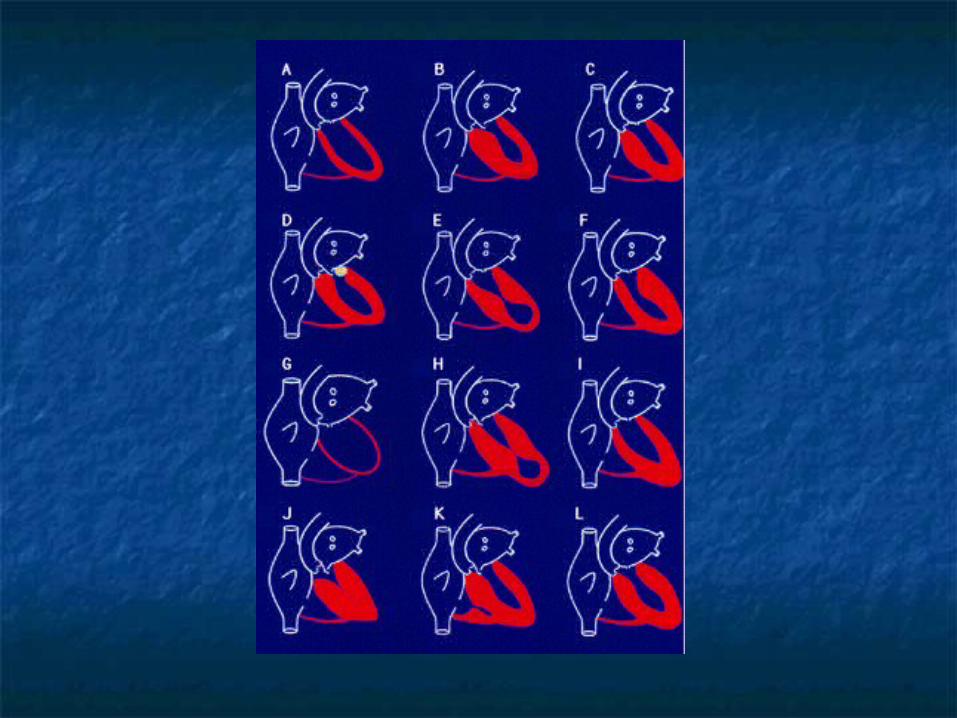
Congenital Coronary Artery Congenital Coronary Artery AnomaliesAnomalies
Variation in the take off the Coronary Variation in the take off the Coronary ArteriesArteries
Incidence 5.6Incidence 5.60.17%0.17% Deaths related to exertionDeaths related to exertion
PresentationPresentation
AnginaAngina Atypical chest painAtypical chest pain SyncopeSyncope PalpitationPalpitation DizzinessDizziness SCDSCD
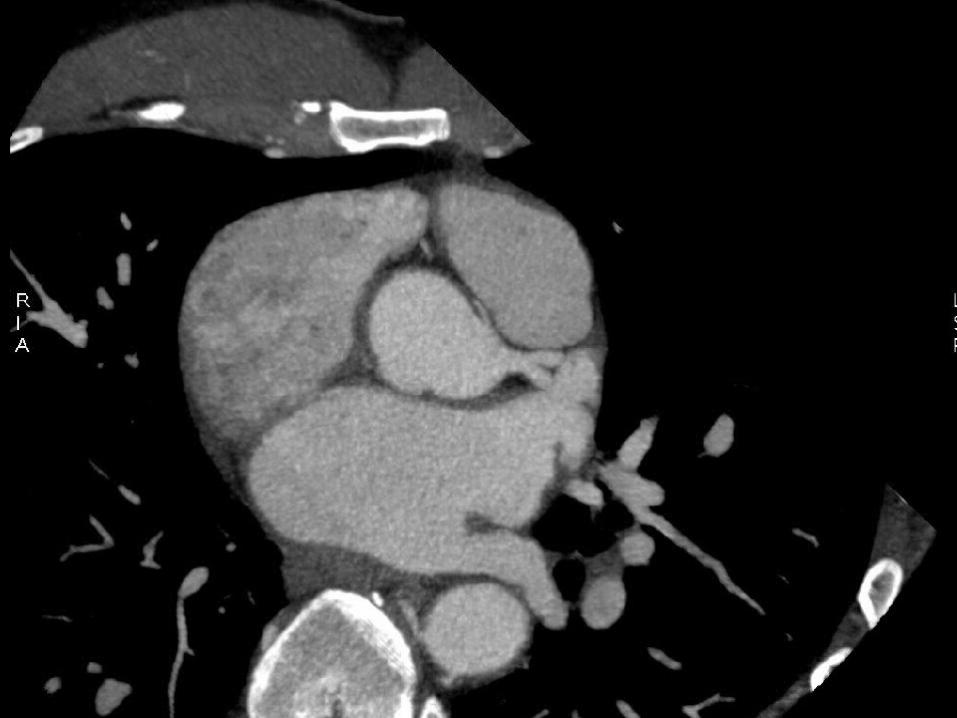
PathophysiologyPathophysiology
Compression between the pulmonary Compression between the pulmonary artery and aortaartery and aorta
Acute angle take offAcute angle take off Myocardial necrosisMyocardial necrosis
DiagnosisDiagnosis
ECHOECHO Cardiac MRICardiac MRI CT angiographyCT angiography Cardiac CathCardiac Cath
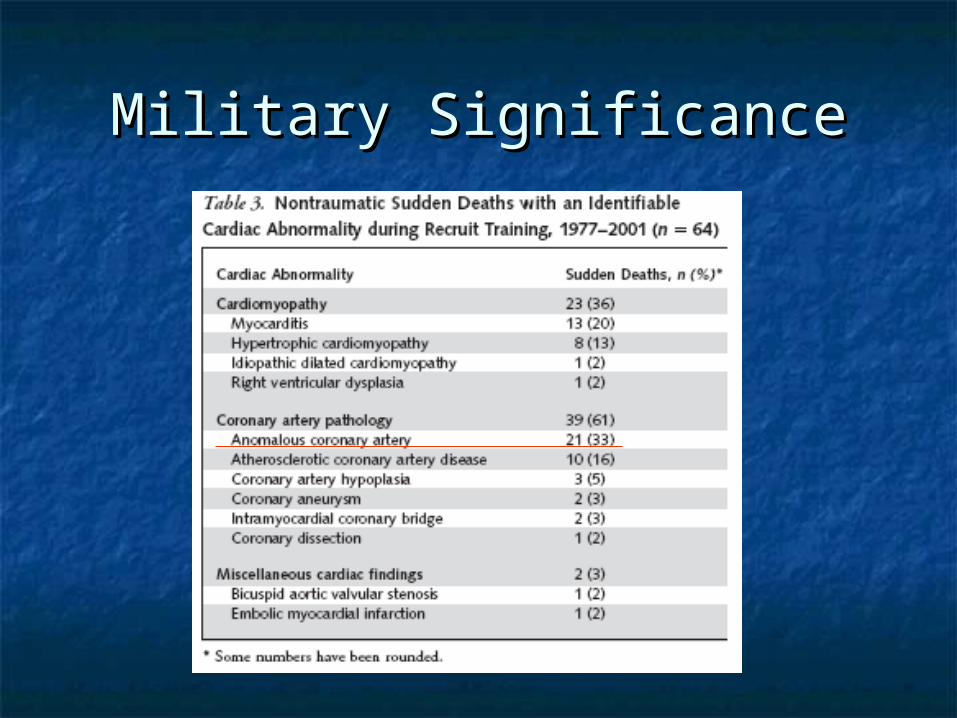
Military SignificanceMilitary Significance

TreatmentTreatment
Beta BlockersBeta Blockers SurgerySurgery Coronary StentsCoronary Stents Avoid strenuous activitiesAvoid strenuous activities
What do you call 2 orthopedic surgeons reading an EKG?
A double blind study!!!!
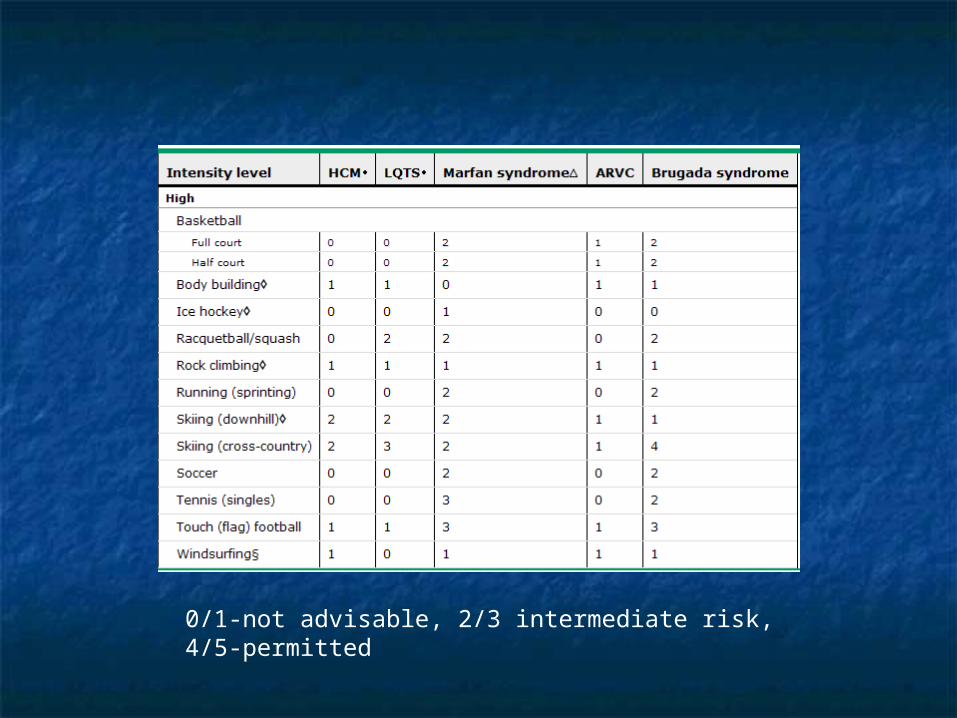
0/1-not advisable, 2/3 intermediate risk, 4/5-permitted
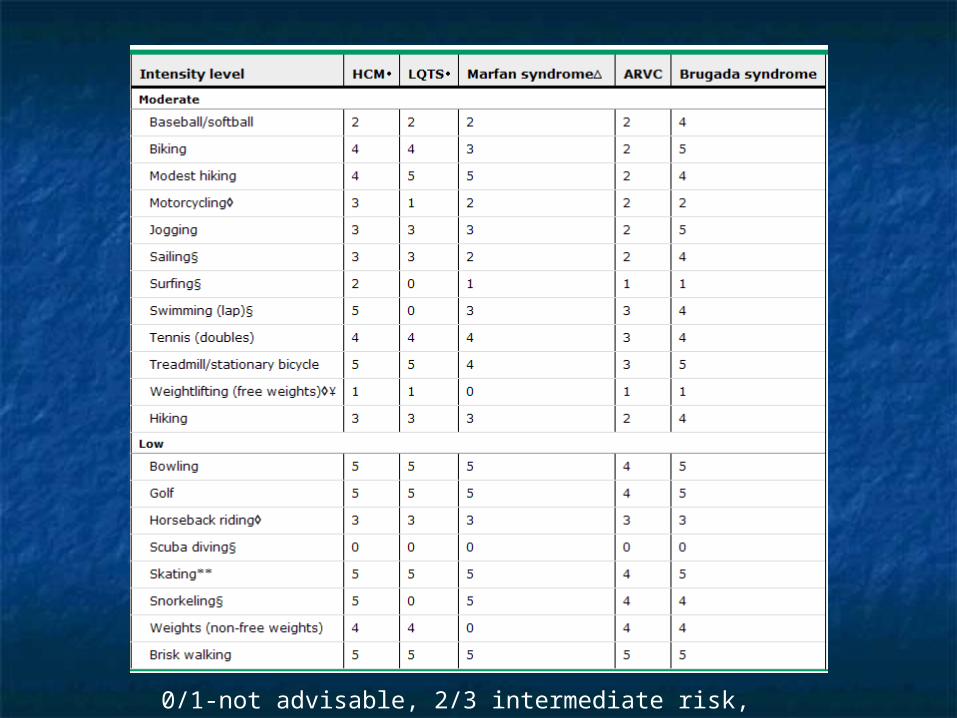
0/1-not advisable, 2/3 intermediate risk, 4/5-permitted
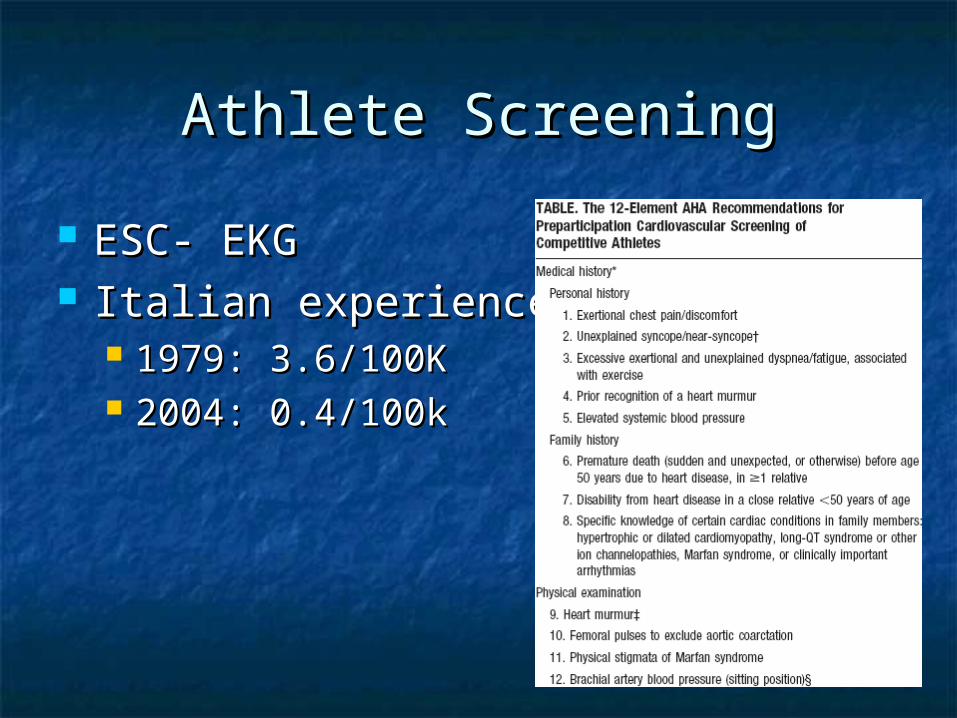
Athlete ScreeningAthlete Screening
ESC- EKGESC- EKG Italian experienceItalian experience
1979: 3.6/100K1979: 3.6/100K 2004: 0.4/100k2004: 0.4/100k
A 32-year-old man is seen for an annual physical examination. There is no personal or family history of cardiovascular disease or symptoms. On physical examination, S1 and S2 are normal and there is an S4 present. There is a grade 2/6 crescendo-decrescendo systolic murmur heard best at the lower left sternal border. The murmur does not radiate to the carotid arteries. Valsalva maneuver increases the intensity of the murmur, and moving from a standing position to a squatting position, performing a passive leg lift while recumbent, and performing isometric handgrip exercises decreases the intensity. Rapid upstrokes of the peripheral pulses are present.
A Mitral valve prolapse
B Hypertrophic cardiomyopathy
C Atrial septal defect
D Ventricular septal defect
E Aortic stenosis
A 32-year-old man is seen for an annual physical examination. There is no personal or family history of cardiovascular disease or symptoms. On physical examination, S1 and S2 are normal and there is an S4 present. There is a grade 2/6 crescendo-decrescendo systolic murmur heard best at the lower left sternal border. The murmur does not radiate to the carotid arteries. Valsalva maneuver increases the intensity of the murmur, and moving from a standing position to a squatting position, performing a passive leg lift while recumbent, and performing isometric handgrip exercises decreases the intensity. Rapid upstrokes of the peripheral pulses are present.
A Mitral valve prolapse
B Hypertrophic cardiomyopathy
C Atrial septal defect
D Ventricular septal defect
E Aortic stenosis
A 23-year-old man is evaluated for palpitations that occur during exercise. He is otherwise healthy and takes no medications. Both the physical examination and the resting electrocardiogram are normal. A stress test demonstrates sustained monomorphic ventricular tachycardia at 201/min at peak exercise. There were no ischemic changes until the arrhythmia developed. The ventricular tachycardia had a left bundle and inferior axis morphology and terminated spontaneously after 7 minutes of rest. An echocardiogram is normal, and an MRI shows no abnormalities in the right or left ventricles.
What is the most likely etiology of ventricular tachycardia in this patient?
A Coronary spasm
B Idiopathic
C Arrhythmogenic right ventricular cardiomyopathy
D Infiltrative heart disease
E Anomalous origin of the coronary arteries
A 23-year-old man is evaluated for palpitations that occur during exercise. He is otherwise healthy and takes no medications. Both the physical examination and the resting electrocardiogram are normal. A stress test demonstrates sustained monomorphic ventricular tachycardia at 201/min at peak exercise. There were no ischemic changes until the arrhythmia developed. The ventricular tachycardia had a left bundle and inferior axis morphology and terminated spontaneously after 7 minutes of rest. An echocardiogram is normal, and an MRI shows no abnormalities in the right or left ventricles.
What is the most likely etiology of ventricular tachycardia in this patient?
A Coronary spasm
B Idiopathic
C Arrhythmogenic right ventricular cardiomyopathy
D Infiltrative heart disease
E Anomalous origin of the coronary arteries
A: ARVD
B: Goldwire’s space re-entry vehicle
C: Spaceballs hat hair
A: ARVD
B: Goldwire’s space re-entry vehicle
C: Spaceballs hat hair