





Languages
Pages
Legal

M-2HEPATOBILIARY
IMAGING
Liver Gallbladder And Bile Ducts Pancreas Spleen
2013

GOALS
Review anatomy of hepato- biliary system.
Correlate imaging with pathology.
Discuss radiologic imaging options.
Choose treatment

ANATOMY / PHYSIOLOGY
Portal vein flow
Hepatic arterial flow
Hepatic vein flow
Biliary drainage

PORTAL BLOOD FLOW
CT

PORTAL VEIN
Coronal and Axial imagesCT
US

CT
US
Transverse CT sections and corresponding US

Catalano, O. A. et al. Radiographics 2008;28:359-378
HEPATIC ARTERIES

LATERAL AORTOGRAM AND CT SHOW ORIGINS OF
CELIAC ARTERY AND SMA
SMA
Celiac
Celiac
SMA

Proper hepatic
Gastroduodenal
Celiac
SMA
THE COMMON HEPATIC ARTERY BECOMES THE PROPER HEPATIC ARTERYAFTER THE GASTRODUODENAL BRANCH DESCENDS.

Arteriography of the three main branches of the celiac artery: Common Hepatic Artery, Left Gastric Artery, and Splenic Artery
Furuta T et al. Radiographics 2009;29:e37
©2009 by Radiological Society of North America
Celiac
HEART

Catalano, O. A. et al. Radiographics 2008;28:359-378
HEPATIC VEINS

HEPATIC VEINSCoronal scan

HEPATIC VEINS ENTERING IVC CT
ULTRASOUND

Catalano, O. A. et al. Radiographics 2008;28:359-378
INTRA AND EXTRAHEPATIC BILIARY TREE

Silva, A. C. et al. Radiographics 2004;24:677-687
NORMAL BILIARY ANATOMY
NORMAL HIDA SCAN

Silva, A. C. et al. Radiographics 2004;24:677-687
COMPARISON WITHMR CHOLANGIOGRAM (MRCP)

MR CHOLANGIOGRAM
OPERATIVE CHOLANGIOGRAM
COMMON BILE DUCT

GALLBLADDER
POST CHOLECYSTECTOMY
GALLBLADDER CALCULI

ERCP
MR cholangiogram shows signal from the bile and other fluids. ERCP has iodinated contrastinjected with an endoscope with the canula in the distal common bile duct.
ENDOSCOPIC RETROGRADE
Cholangio - Pancreatography

PANCREATIC ANATOMY

WHO PRESENTS FOR IMAGING?
Right upper quadrant pain
Altered laboratory data
Staging of malignancy / infection
Physical exam findings
Abdominal trauma

Differential Diagnosis:
Acute Cholecystitis/Cholelithiasis
PUD / Gastritis / Reflux
Acute hepatitis / Liver Abcess
Pancreatitis
Choledocholithiasis
ACUTE RIGHT UPPER QUADRANT PAIN

RIGHT UPPER QUADRANT PAIN
Gallstone = cholelithiasis
Common - prevalence 10%
Pain with contraction after eating

DIAGNOSIS
ULTRASOUND
Cost / Availability
Fluid background is ideal for imaging
Helpful to assess for any associated biliary dilatation or inflammatory change

CHOLELITHIASIS

Sonography is preferred as the initial imaging test of choice, with supplemental scintigraphy in problematic cases.
ACUTE CHOLECYSTITIS

CHOLECYSTITIS
With diffuse wall thickening and edema.
Ultrasound and CT demostration of edema in and around GB wall
A Sonographic Murphy’s sign is focal tenderness corresponding to the gallbladder.
Along with other ultrasound evidence of inflammation (gallbladder wall thickening, pericholecystic fluid) it helps physicians separate Acute Cholecystitis from gallstones alone.
Murphy’s Sign

IMAGING ALTERNATIVES
Nuclear medicine - HIDA
CT
X-ray
Cholangiography - MR or Endoscopic

NORMAL HIDA
ABNORMAL HIDA
Obstructed cystic duct doesn’t allow for filling of radionuclide into the GB.
HEPATO - BILIARY
SCINTIGRAM
Gall bladder
Absent Gall bladder

NORMAL GALLBLADDER
GALLSTONE
CHOLECYSTITIS
Thickened edematous gallbladder wall with cholecystitis on CT

GALLSTONES 15-30% calcify

COMPLICATIONS OF GALLSTONES
• Cystic duct obstruction Cholecystitis A
• Common bile duct obstruction Obstructive jaundice B Ascending cholangitis
• Pancreatic duct obstruction Pancreatitis C
A
B
C

Normal bile duct size
Diameter < portal diameter
Obstructed duct due to distal calculus
PV
CBD
Note dilated CBD with impacted calculus

Normal
*Note dilated bile ducts. (Low density branching structures anterior to portal veins)
The Portal vein is opacified (white) from IV contrast administration. The biliary tree is of lower density and shows as a branching structure anterior to the portal vein.

Endoscopic retrograde
Cholangiopancreatography
Normal size CBD
Dilated CBD with calculi
ERCP

SPECIAL CASES
Emphysematous cholecystitis
Acalculous cholecystitis
Gallstone ileus

EMPHYSEMATOUS CHOLECYSTITISDIABETIC PATIENTS - AIR IN WALL

ACALCULOUS CHOLECYSTITISBILIARY STASIS - FASTING / ICU PATIENTS

GALLSTONE ILEUS Small Bowel Obstruction at IC valve due to migration of
gallstones that erode into duodenum from GB.
1999 2002

ABDOMEN SCANDONE 2/12/08

SAME PATIENTABDOMEN SCAN
DONE 2/25/08

CHOLECYSTOSTOMYSKIN MARKERS
NEEDLE
POSITION
DRAIN PRESENTATION
PLACEMENT

Ultrasound – 1st
CT / HIDA – 2nd
ERCP / MRCP-- 3rd
RUQ PAINIMAGING EVALUATION

ALTERED LABORATORY DATA+-PAIN
Bilirubin - jaundice
Amylase - pancreatitis
JAUNDICE
Jaundice is a clinical finding, not a single disease entity.
Two distinct categories:
Intrahepatic biliary stasis (hepatocellular jaundice) -imaging plays little useful role
Mechanical biliary obstruction.

JAUNDICEVIRAL HEPATITIS
IMAGING- LIMITED VALUE
Acute – usually normal
helps to exclude obstruction
Chronic – increased malignancy risk

Neoplasms of the pancreas
Choledocholithiasis
Pancreatitis
Iatrogenic strictures of the biliary tree
THE MOST COMMON CAUSES OF OBSTRUCTIVE JAUNDICE
IN THE UNITED STATES

JAUNDICEBILIRUBIN
Painless Malignancy Chronic obstruction
Painful Hepatitis / liver edema Choledocholithiasis / acute obstruction
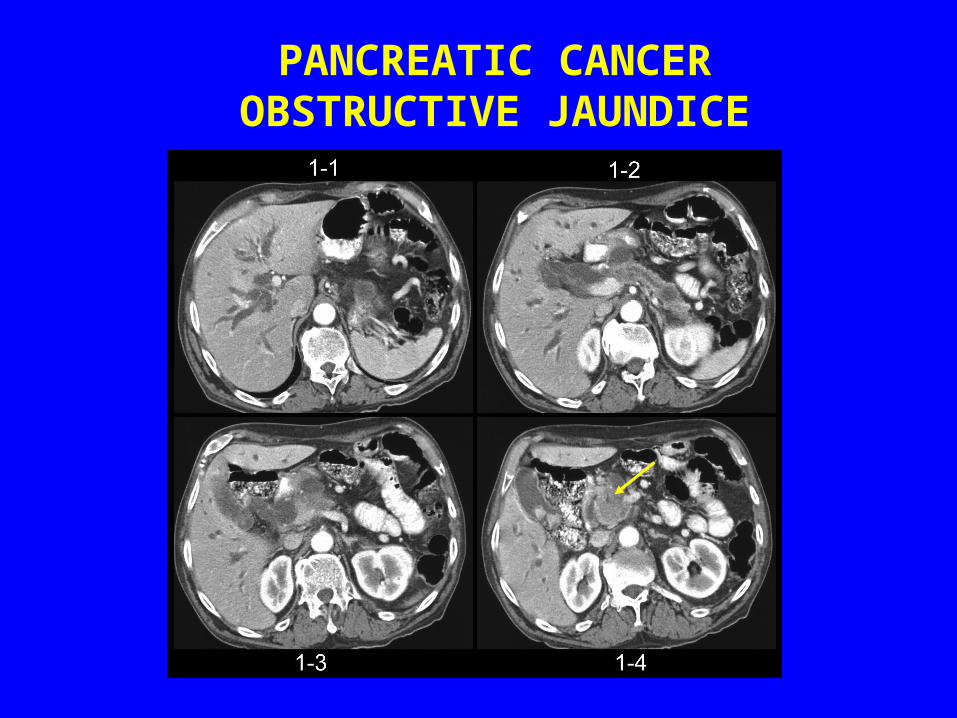
PANCREATIC CANCEROBSTRUCTIVE JAUNDICE

PALPABLE GALL BLADDER
A palpable gall bladder in an asymtomatic patient can be seen with pancreatic carcinoma due to distal obstruction (Courvoisier sign)

PANCREATITIS elevated
AMYLASE & LIPASE
Biliary calculi-obstruction Alcohol- chemical toxicity

Pseudocyst
Pain
Infection
Hemorrhage- pseudoaneurysm
Pancreatic insufficiency
COMPLICATIONS OF PANCREATITIS
Large retrogastric fluid collection is a pseudocyst related to pancreatic enzyme break down of tissue.

PANCREATIC ABSCESS

DRAINAGE OF PANCREATIC ABSCESS

STAGINGMALIGNANCY / INFECTION
Mesenteric blood flow spreads disease to liver
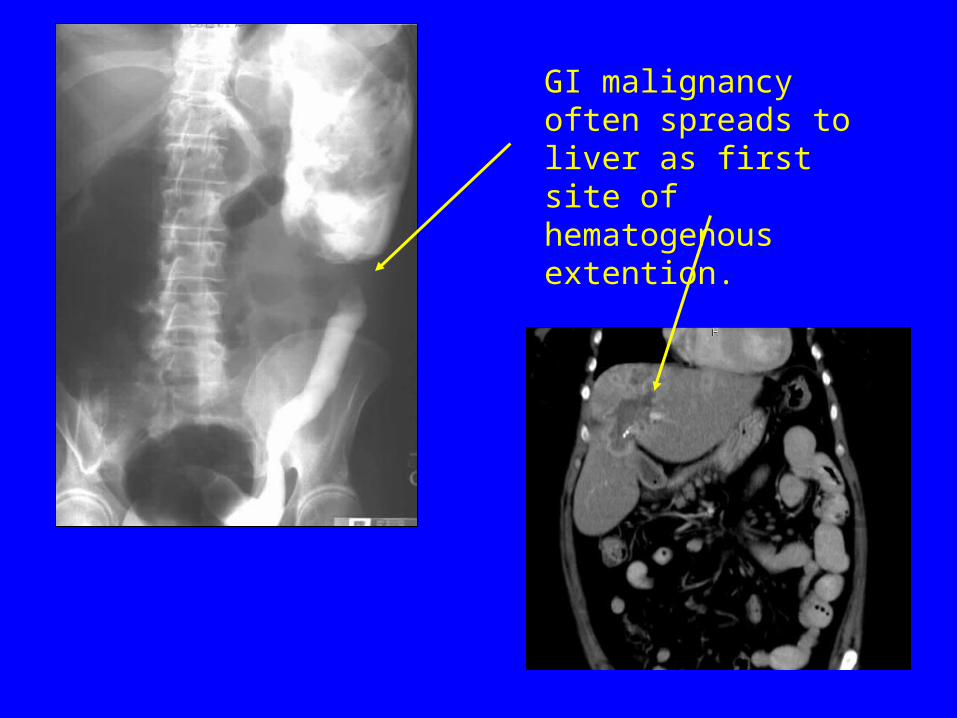
GI malignancy often spreads to liver as first site of hematogenous extention.
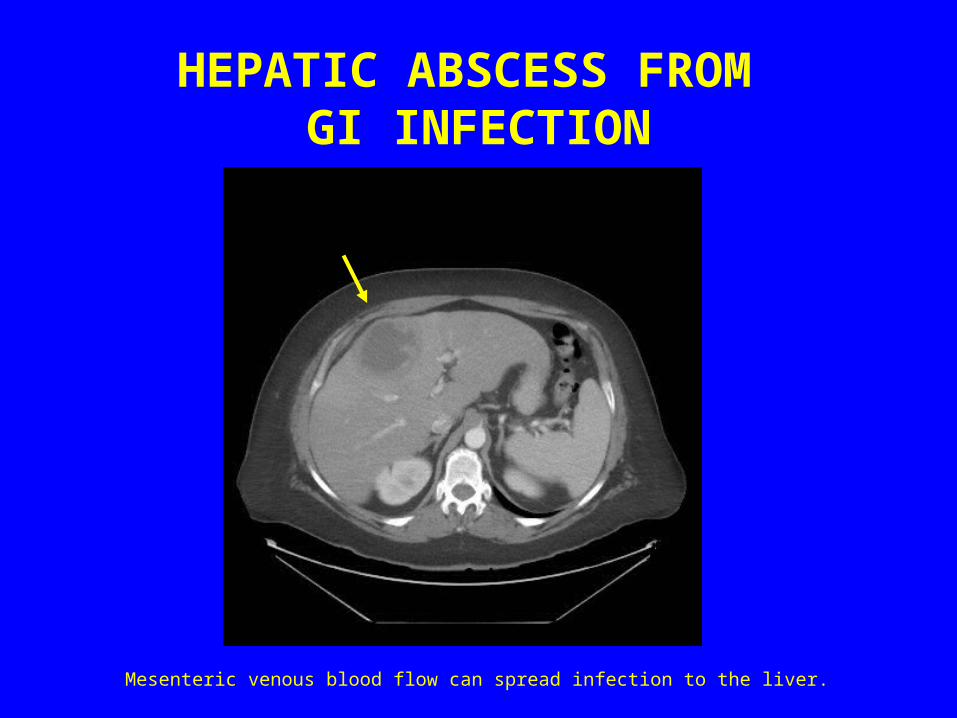
HEPATIC ABSCESS FROM GI INFECTION
Mesenteric venous blood flow can spread infection to the liver.

PALPABLE PHYSICAL EXAM FINDINGS
Enlarged liver
Enlarged spleen
Ascites - distention

PALPABLE LIVER-metastatic disease
A palpable enlarged liver edge is nonspecific but raises questions of mass or liver pathology.

ENLARGED PALPABLE SPLEEN
Enlarged spleen raises issue of lymphoproliferative diseases or infection.

SPLEEN
ENLARGED SPLEEN ON
ULTRASOUND AND CT.
*Note left kidney

Coronal scan
SPLENOMEGLY
*Note dilated splenic vein
*

Ascites displacing bowel medially on Xray
Lucent fluid at tip of liver on ultrasound
Fluid on CT
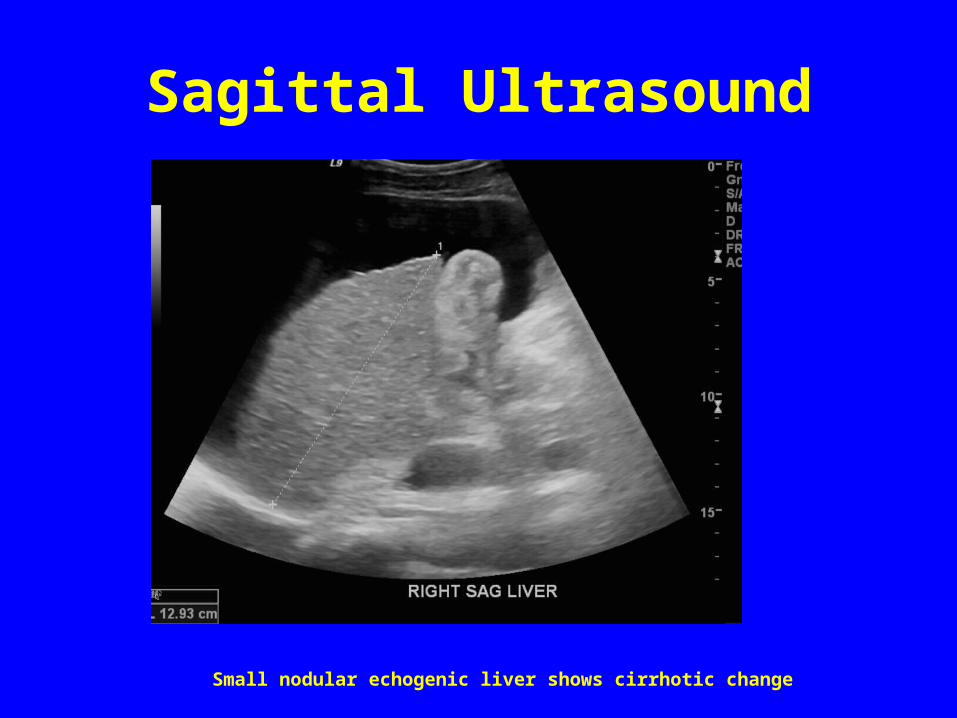
Sagittal Ultrasound
Small nodular echogenic liver shows cirrhotic change

CIRRHOSIS Portal hypertension
Here long standing cirrhosis has lead to a scarred shrunken liver. Portal hypertension resulting leads to varices and redirection of blood flow into a recanalized umbilical vein.

VARICES
Varices are at risk for hemorhage. They can be treated by embolization at GI endoscopy or vascular shunt of portal blood flow by Surgery or Radiology to decrease portal pressure.

Surgical Portocaval shunts as therapy
Side to side
Splenorenal

Interventional Radiology shunt
Hepatic vein - Portal vein
TIPSTransjugular Intrahepatic Portosystemic Shunt

TRAUMA

UNSTABLE—SURGERY
X-ray-- Chest/ Abd / Pelvis if possible
FAST SCAN-- to look for peritoneal fluid
STABLE– CT SCANNING
TRAUMA

F.A.S.T. SCAN(Focused Assessment with Sonography for Trauma)
Ultrasound survey for free peritoneal fluid

F.A.S.T. SCAN(Focused Assessment with Sonography for Trauma)
Ultrasound survey for free peritoneal fluid
Need 400-500 ccs
Not good for organ injury or bowel injury
Peritoneal Lavage is outdated
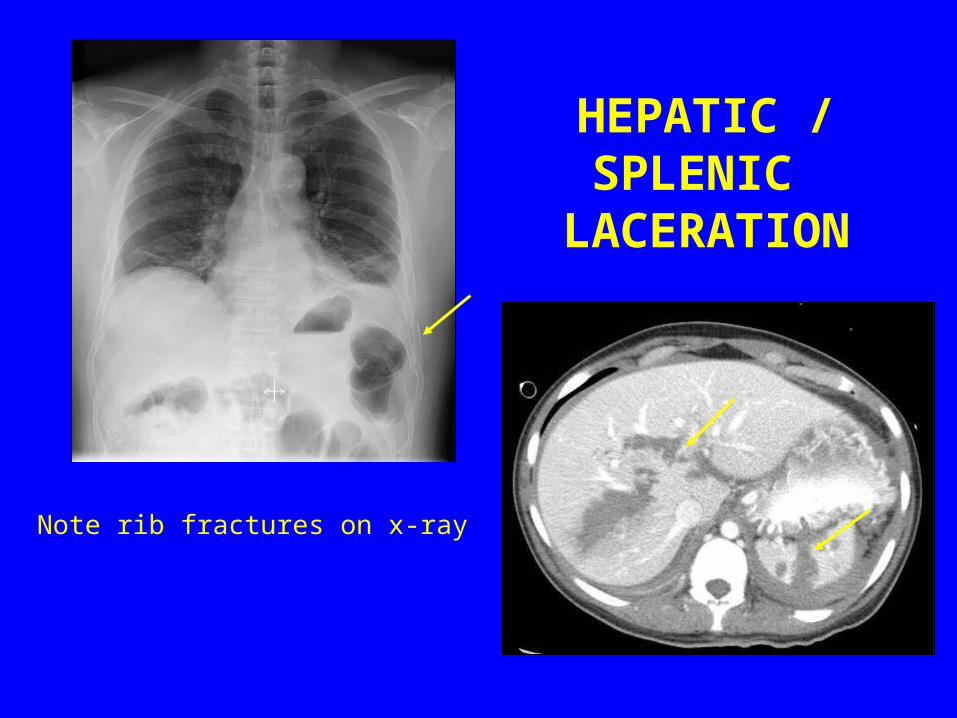
HEPATIC / SPLENIC
LACERATION
Note rib fractures on x-ray

POST TRAUMATICPANCREATITIS
SEAT- BELT INJURY
There is diffuse edema and hemorhage in adjacent tissues around the pancreas.

WHAT IMAGING POSSIBILITIES?
ULTRASOUND---GB / CBD / LIVER
Plain x-ray---ERCP
CT---PANCREAS / LIVER
Nuclear Medicine---HIDA
MR---MRCP
These are the imaging modalities and important sites of assessment

Top Related