5. Spleen, Liver and Pancreas, Biliary ducts and Gallbladder (75).pptx
72
een, Pancreas, Liver and biliary sys Learning Objectives Describe the anatomy of spleen and relation with the other abdominal organs Describe the position and form of the pancreas and its relationships to other abdominal organs. Describe the position of the liver, the lobes and their key anatomical relations. Explain the peritoneal reflections of the liver. Describe the gall bladder and bile ducts.
Transcript of 5. Spleen, Liver and Pancreas, Biliary ducts and Gallbladder (75).pptx
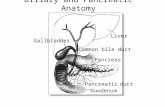
Liver and Pancreas
Spleen, Pancreas, Liver and biliary systemLearning ObjectivesDescribe the anatomy of spleen and relation with the other abdominal organs
Describe the position and form of the pancreas and its relationships to other abdominal organs.
Describe the position of the liver, the lobes and their key anatomical relations. Explain the peritoneal reflections of the liver.
Describe the gall bladder and bile ducts.SpleenLargest lymphatic organs
Serves as a blood reservoir, storing RBCs and platelets.
Ovoid, purplish, pulpy mass . Measurements1 inch thick, 3 inches wide, 5 inches long, and 7 ounces weight.
SpleenLocated in the left upper abdominal quadrant or hypochondrium.
Related to left 9th - 11th ribs and separated by the diaphragm and the costodiaphragmatic recess.
Long axis lies along the shaft of the 10th rib.
SurfacesDiaphragmatic surface: ConvexVisceral surface: Concave
BordersSuperiorInferiorAnterior
Ends:AnteriorPosterior (medial)
Relations of the spleen Anteriorly: Stomach.
Posteriorly: Left part of the diaphragm, which separates it from the pleura, lung, and ribs 9 -11.
Inferiorly: Left colic flexure.
Medially: Left kidney.
Peritoneal relation:Entirely surrounded by peritoneum except at the splenic hilumSplenic hilum: related to tail of the pancreas and constitutes the left boundary of the omental bursa.Spleen contacts the posterior wall of the stomach and is connected to its greater curvature by the gastrosplenic ligament and to the left kidney by the splenorenal ligament.
Splenorenal ligaments, containing splenic vessels, are attached to the hilum of the spleen on its medial aspect .
Splenic artery:Largest branch of the celiac trunk
Tortuous course posterior to the omental bursa, anterior to the left kidney, and along the superior border of the pancreas.
Divides into five or more branches that enter the hilum between the layers of the splenorenal ligament.
Splenic vein
Joined by the Inf. Mesenteric vein
Runs posterior to the body and tail of the pancreas
Unites with the Sup. Mesenteric Vein posterior to the neck of the pancreas to form the portal vein.
Splenic lymphatic vesselsLeave the lymph nodes in the splenic hilum
Pass along the splenic vessels to the pancreaticosplenic lymph nodes .
Lymph nodes relate to the posterior surface and superior border of the pancreas.
Pancreaticosplenic lymph nodesRupture of the Spleen and SplenectomySevere blows on the left side may fracture one or more of these ribs, resulting in sharp bone fragments that can lacerate the spleen.
Cause the thin capsule and overlying peritoneum of the spleen to burst, disrupting its soft parenchyma or pulp (ruptured spleen).
Profuse bleeding (intraperitoneal hemorrhage) and shock.
Repair of a ruptured spleen difficult; consequently, splenectomy (removal of the spleen) is often performed to prevent the person from bleeding to death.
Sub-total (partial) splenectomy, when possible, is followed by rapid regeneration.
Even total splenectomy usually does not produce serious effects, especially in adults, because most of its functions are assumed by other reticuloendothelial organs (e.g., the liver and bone marrow).SplenomegalyResulting from, for example, granulocytic leukemia (high leukocyte and white blood cell count), or some forms of hemolytic or granulocytic anemias, may enlarge
Spleen usually not palpable in the adult
Generally, if its lower edge can be detected when palpating below the left costal margin at the end of inspiration , it is enlarged about three times of its normal size.
Splenic Enlargement
Pathologically enlarged spleen extends downward and medially along the long axis.
Left colic flexure and the phrenicocolic ligament prevent a direct downward enlargement of the organ.
Accessory Spleen(s):
One or more small accessory spleens may form near the splenic hilum
May be embedded partly or wholly in the tail of the pancreas, between the layers of the gastrosplenic ligament, in the infracolic compartment in the mesentery, or in close proximity to the ovary or testis .
Common (10%), are usually small (approximately 1 cm in diameter, but range from 0.2 to 10 cm), and often resemble a lymph node.
Awareness of the possible presence of an accessory spleen is important because if not removed during splenectomy, the symptoms that indicated removal of the spleen (e.g., splenic anemia) may persist.
Accessory SpleenNormal spleenSplenic Needle Biopsy and Splenoportography:
The relationship of the costodiaphragmatic recess of the pleural cavity to the spleen is clinically important. This potential space descends to the level of the 10th rib in the midaxillary line.
Its existence must be kept in mind when doing a splenic needle biopsy, or when injecting radiopaque material into the spleen for visualization of the portal vein (splenoportography).
If care is not exercised, this material may enter the pleural cavity, causing pleuritis (inflammation of the pleura).
PancreasMixed gland: exocrine and an endocrine in nature.
Exocrine portion produces enzymes
Endocrine portion produces the hormones insulin and glucagon by the pancreatic islets (islets of Langerhans)
PancreasSoft and lobulated structureLies in the epigastrium and the left upper quadrant. Crosses the transpyloric planeSituated on the posterior abdominalRetroperitoneal organParts: head, neck, body, and tail
Head:
Disc shaped
Lies within the concavity of the duodenum.
Uncinate process: a part of the head extends to the left behind the superior mesenteric vessels
Neck:Constricted portion of the pancreas
Connects the head to the body.
Lies in front of the beginning of the portal vein and the origin of the superior mesenteric artery from the aorta.
Body:Runs upward and to the left across the midline.
Triangular in cross section.
Tail:Passes forward in the splenicorenal ligament
Related to the hilum of the spleen.
Relations of the Pancreas:Anteriorly:From right to left:Transverse colon and the attachment of the transverse mesocolon
Lesser sac
Stomach.
Relations of the Pancreas:Posteriorly: From right to left: Bile ductPortal and Splenic veinsInferior vena cavaAortaOrigin of the superior mesenteric arteryLeft psoas muscleLeft suprarenal glandLeft kidneyHilum of the spleen
Pancreatic DuctsMain duct of the pancreas begins in the tail and runs the length of the gland, receiving numerous tributaries on the way.
Main pancreatic duct and the bile duct unite to form the short, dilated hepatopancreatic ampulla (of Vater)
Hepatopancreatic ampulla opens into the second part of the duodenum at about its middle on the major duodenal papilla.
Pancreatic DuctsAccessory duct of the pancreas:
Occasionally present
Drains the upper part of the head
Opens into the duodenum a short distance above the main duct on the minor duodenal papilla.
Frequently communicates with the main duct.
ArteriesSplenicSuperior and inferior pancreaticoduodenal
Veinsdrain into the portal system.
Lymph Drainage
The efferent vessels ultimately drain into the celiac and superior mesenteric lymph nodes.Nerve Supply:The nerves of the pancreas are derived from the vagus and abdominopelvic splanchnic nerves passing through the diaphragm.
Pancreatic secretion is primarily mediated by secretin and cholecystokinin, hormones formed by the epithelial cells of the duodenum and upper intestinal mucosa under the stimulus of acid contents from the stomach.
Diagnosis of Pancreatic Disease
Pain from the pancreas is commonly referred to the back.
Inflammation of the pancreas can spread to the peritoneum forming the posterior wall of the lesser sac and may leads to adhesions and the closing off of the lesser sac to form a pseudocyst.Trauma of the PancreasSudden blow to the abdomen occurs, can compress and tear the pancreas against the vertebral column or may damage during splenectomy
Damaged pancreatic tissue releases activated pancreatic enzymes that produce the signs and symptoms of acute peritonitis.Cancer of the Head of the Pancreas and the Bile Duct:cancer of the head of the pancreas often causes obstructive jaundice.
Blockage of the Hepatopancreatic Ampulla and Pancreatitis
A gallstone lodge in the constricted distal end of the ampulla, where it opens at the summit of the major duodenal papilla. In this case, both the biliary and pancreatic duct systems are blocked and neither bile nor pancreatic juice can enter the duodenum.
Bile may back up and enter the pancreatic duct, usually resulting in pancreatitis (inflammation of the pancreas).
These two pictures were taken with the endoscope. A large cholesterol stone (white arrow) is released from a wire basket into the duodenum (left picture).
Endoscopic view of an ampullary carcinoma.PancreatectomiesIn the treatment of some people with chronic pancreatitis, most of the pancreas is removed, a procedure called pancreatectomy.
Anatomical relationships and the blood supply of the head of the pancreas, bile duct, and duodenum make it impossible to remove the entire head of the pancreas .
Usually a rim of the pancreas is retained along the medial border of the duodenum to preserve the duodenal blood supply.Accessory Pancreatic TissueMay develop in the stomach, duodenum, ileum, or an ileal diverticulum
Most common sites: stomach and duodenum.
May contain pancreatic islet cells that produce glucagon and insulin.
A little accessory pancreas situated in the greater curvature of the antrum.Liver
Largest gland in the body
Weight: 1500 g.
Occupies almost all of the right hypochondrium and epigastrium and extends into the left hypochondrium.
Surfaces, Peritoneal Reflections, and Relationships of the Liver
Convex diaphragmatic surface (anterior, superior, and some posterior)
Flat or even concave visceral surface (posteroinferior)
Both surfaces separated anteriorly by the inferior border.
Subphrenic recesses:Superior extensions of the peritoneal cavity (greater sac).
Exist between diaphragm and the anterior and superior aspects of the diaphragmatic surface of the liver.
Separated into right and left recesses by the falciform ligament
Extends between the liver and the anterior abdominal wall.
Portion of the supracolic compartment of the peritoneal cavity immediately inferior to the liver is the subhepatic space.
Hepatorenal recess (hepatorenal pouch; Morison pouch):
Posterosuperior extension of the subhepatic space
Lying between the right part of the visceral surface of the liver and the right kidney and suprarenal gland.
Gravity-dependent part of the peritoneal cavity in the supine position; fluid draining from the omental bursa flows into this recess.
Communicates anteriorly with the right subphrenic recess.
Subphrenic AbscessesA common site for pus to collect is in a subphrenic recess or space. These subphrenic abscesses are more common on the right side because of the frequency of ruptured appendices and perforated duodenal ulcers.
Because the right and left subphrenic recesses are continuous with the hepatorenal recess, pus from a subphrenic abscess may drain into one of the hepatorenal recesses, especially when patients are bedridden.
A subphrenic abscess is often drained by an incision inferior to, or through, the bed of the 12th rib.
An anterior subphrenic abscess is often drained through a subcostal incision located inferior and parallel to the right costal margin.Diaphragmatic surface:Covered with visceral peritoneum, except posteriorly in the bare area of the liver, where it lies in direct contact with the diaphragm.
The bare area: demarcated by the reflection, as the upper and lower layers of the coronary ligament. These layers meet on the right to form the right triangular ligament.
Near the apex (the left extremity) of the liver, the anterior and posterior layers of the left part of the coronary ligament meet to form the left triangular ligament .
Inferior vena cava traverses a deep groove for the vena cava within the bare area of the liver.
Visceral surface:Covered with peritoneum, except at the fossa for the gallbladder and the porta hepatis
Porta hepatis: a transverse fissure where the vessels (portal vein, hepatic artery, and lymphatic vessels), the hepatic nerve plexus, and hepatic ducts that supply and drain the liver enter and leave it.
Visceral surface relations:Right side of the anterior aspect of the stomach.
Superior part of the duodenum Lesser omentum (extends into the fissure for the ligamentum venosum).
Gallbladder (fossa for gallbladder).
Right colic flexure and right transverse colon (the colic area).
Right kidney and suprarenal gland (the renal and suprarenal areas).
Two sagittal fissures, linked centrally by the transverse porta hepatis, form the letter H on the visceral surface.
Right sagittal fissure: continuous groove formed anteriorly by the fossa for the gallbladder and posteriorly by the groove for the vena cava.
Left sagittal fissure: continuous groove formed anteriorly by the fissure for the ligamentum teres or round ligament, and posteriorly by the fissure for the ligamentum venosum.
Round ligament of the liver: fibrous remnant of the left umbilical vein.
Contents of the Falciform ligament: round ligament and small paraumbilical veins. Ligamentum venosum: fibrous remnant of the fetal ductus venosus, which shunted blood from the umbilical vein to the IVC, short-circuiting the liver.
Anatomical Lobes of the LiverTwo topographical (anatomical) lobes and two accessory lobes: Caudate and quadrate lobes (parts of the anatomic right lobe).
Caudate lobe is so-named not because it is caudal in position (it is not) but because it often gives rise to a tail in the form of an elongated papillary process .
A caudate process extends to the right, between the IVC and the portal hepatis, connecting the caudate and right lobes .
Vascular segments : subdivided into four divisions and then into eight surgically resectable hepatic segments, each served independently by a secondary or tertiary branch of the portal triad.
Blood Vessels of the Liver
Portal vein: brings 75-80% of the blood to the liver.
Hepatic artery: accounting for only 20-25% of blood received by the liver.
Hepatic Veins: formed by the union of collecting veins that in turn drain the Central veins of the hepatic parenchyma, open into the IVC.
Rupture of the LiverThe liver is easily injured because it is large, fixed in position, and friable (easily crumbled). Often a fractured rib that perforates the diaphragm tears the liver. Because of the liver's great vascularity and friability, liver lacerations often cause considerable hemorrhage and right upper quadrant pain. In such cases, the surgeon must decide whether to remove foreign material and the contaminated or devitalized tissue by dissection or to perform a segmentectomy.Aberrant Hepatic ArteriesA more common variety of right or left hepatic artery that arises as a terminal branch of the hepatic artery proper may be replaced in part or entirely by an aberrant (accessory or replaced) artery arising from another source.
The most common source of an aberrant right hepatic artery is the SMA (Fig. A).
The most common source of an aberrant left hepatic artery is the left gastric artery (Fig.B).
Lymphatic drainage of the Liver
Superficial lymphatics drain to the hepatic lymph nodes scattered along the hepatic vessels and ducts in the lesser omentum.
Efferent lymphatic vessels from the hepatic nodes drain into celiac lymph nodes, which in turn drain into the chyle cistern.
A few lymphatic vessels follow different routes:
From the posterior surface of the left lobe toward the esophageal hiatus of the diaphragm to end in the left gastric lymph nodes.
From the anterior central diaphragmatic surface along the falciform ligament to the parasternal lymph nodes.
Along the round ligament of the liver to the umbilicus and lymphatics of the anterior abdominal wall.Hepatomegaly
Marked temporary engorgement stretches the fibrous capsule of the liver, producing pain around the lower ribs, particularly in the right hypochondrium.
Diseases that produce hepatic engorgement such as congestive heart failure, bacterial and viral diseases such as hepatitis cause liver enlargement, or hepatomegaly.
Inferior edge may be readily palpated below the right costal margin and may even reach the pelvic brim in the right lower quadrant of the abdomen.
Liver is a common site of metastatic carcinoma.Cancer cells may also pass to the liver from the thorax, especially from the right breast, because of the communications between thoracic lymph nodes and the lymphatic vessels draining the bare area of the liver. Cirrhosis of the LiverProgressive destruction of hepatocytes (parenchymal liver cells) in hepatic cirrhosis and replacement of them by fat and fibrous tissue.
Alcoholic cirrhosis, the most common of many causes of portal hypertension
Fibrous tissue surrounds the intrahepatic blood vessels and biliary ducts, making the liver firm, and impeding the circulation of blood through it (portal hypertension).
The treatment of advanced cirrhosis may include the surgical creation of a portosystemic or portocaval shunt, anastomosing the portal and systemic venous systems.Liver BiopsyHepatic tissue may be obtained for diagnostic purposes by liver biopsy.
The needle is commonly directed through the right 10th intercostal space in the midaxillary line.
Before the physician takes the biopsy, the person is asked to hold his or her breath in full expiration to reduce the costodiaphragmatic recess and to lessen the possibility of damaging the lung and contaminating the pleural cavity.Biliary DuctsConvey bile from the liver to the duodenum.
Bile is produced continuously by the liver and stored and concentrated in the gallbladder, which releases it intermittently when fat enters the duodenum.
Bile emulsifies the fat, so that it can be absorbed in the distal intestine.
Biliary Ducts:Hepatocytes secrete bile into the bile canaliculi formed between them.
The canaliculi drain into the small interlobular biliary ducts and then into large collecting bile ducts of the intrahepatic portal triad, which merges to form the right and left hepatic ducts.
Biliary DuctsThe right and left hepatic ducts drain the right and left (parts of the) liver, respectively.
Shortly after leaving the porta hepatis, the right and left hepatic ducts unite to form the common hepatic duct, which is joined on the right side by the cystic duct to form the bile duct and conveys the bile to the duodenum.
Bile Duct: (formerly, common bile duct)Forms by the union of the cystic duct and the common hepatic duct.
Length: 5 to 15 cm
Bile Duct:The bile duct descends posterior to the superior part of the duodenum and lies in a groove on the posterior surface of the head of the pancreas. On the left side of the descending part of the duodenum, the bile duct comes into contact with the main pancreatic duct. These ducts run obliquely through the wall of this part of the duodenum, where they unite to form the hepatopancreatic ampulla, the dilation within the major duodenal papilla.
Bile Duct:The distal end of the ampulla opens into the duodenum through the major duodenal papilla.
The circular muscle around the distal end of the bile duct is thickened to form the sphincter of the bile duct.
When the sphincter contracts, bile cannot enter the ampulla and the duodenum; hence bile backs up and passes along the cystic duct to the gallbladder for concentration and storage.
The arteries supplying the bile duct include:
Proximal part of the duct by the Cystic artery
Middle part of the duct by the Right hepatic artery
Retroduodenal part of the duct by the Posterior superior pancreaticoduodenal artery and Gastroduodenal artery.
VEINS:From the proximal part of the bile duct and the hepatic ducts usually enter the liver directly.
Posterior superior pancreaticoduodenal vein drains the distal part of the bile duct and empties into the portal vein or one of its tributaries.Lymphatic:Pass to the cystic lymph nodes near the neck of the gallbladder, the node of the omental foramen, and the hepatic lymph nodes.
Efferent lymphatic vessels from the bile duct pass to the celiac lymph nodes.GallbladderPear-shaped
7-10 cm long
Lies in the fossa for the gallbladder on the visceral surface of the liver.
Capacity: 50 mL
Peritoneum completely surrounds the fundus of the gallbladder and binds its body and neck to the liver.
Hepatic surface of the gallbladder attaches to the liver by connective tissue of the fibrous capsule of the liver.
Parts :Fundus Wide end, projects from the inferior border of the liverLocated at the tip of the right 9th costal cartilage in the mid-clavicular line.BodyContacts the visceral surface of the liver, the transverse colon, and the superior part of the duodenum.Neck:Narrow and taperedDirected toward the porta hepatisMakes an S-shaped bendJoins the cystic duct.
Cystic duct: (3-4 cm long) connects the neck of the gallbladder to the common hepatic duct.
The mucosa of the neck spirals into the spiral fold (spiral valve).
The spiral fold helps keep the cystic duct open; thus bile can easily be diverted into the gallbladder when the distal end of the bile duct is closed by the sphincter of the bile duct and/or hepatopancreatic sphincter, or bile can pass to the duodenum as the gallbladder contracts.
The cystic duct: passes between the layers of the lesser omentum, usually parallel to the common hepatic duct, which it joins to form the bile duct.The cystic artery, supplying the gallbladder and cystic duct , commonly arises from the right hepatic artery in the angle between the common hepatic duct and the cystic duct (cystohepatic triangle). Variations occur in the origin and course of the cystic artery .
The cystic veins, draining the neck of the gallbladder and cystic duct, enter the liver directly or drain through the portal vein to the liver, after joining the veins draining the hepatic ducts and upper bile duct . The veins from the fundus and body of the gallbladder pass directly into the visceral surface of the liver and drain into the hepatic sinusoids.
The lymphatic drainage of the gallbladder is to the hepatic lymph nodes, often through cystic lymph nodes located near the neck of the gallbladder.
Efferent lymphatic vessels from these nodes pass to the celiac lymph nodes.
The nerves to the gallbladder and cystic duct pass along the cystic artery from the celiac nerve plexus (sympathetic and visceral afferent [pain] fibers), the vagus nerve (parasympathetic), and the right phrenic nerve (actually somatic afferent fibers).
Parasympathetic stimulation causes contractions of the gallbladder and relaxation of the sphincters at the hepatopancreatic ampulla.
However, these responses are generally stimulated by the hormone cholecystokinin (CCK), produced by the duodenal walls (in response to the arrival of a fatty meal) and circulated through the bloodstream.Infundibulum of the GallbladderIn diseased states of the gallbladder, a dilation or pouch appears at the junction of the neck of the gallbladder and the cystic duct. This pouch is called the infundibulum of the gallbladder (Hartmann pouch).
When this pouch is large, the cystic duct arises from its upper left aspect, not from what appears to be the apex of the gallbladder.
Gallstones commonly collect in the infundibulum. Mobile GallbladderThe gallbladder has a short mesentery in approximately 4% of people.
Such gallbladders are subject to vascular torsion and infarction (sudden insufficiency of arterial or venous blood supply).
GallstonesCommon sites for impaction :
Infundibulum of the gallbladder, another common.
Hepatic and Cystic ducts.
Distal end of the hepatopancreatic ampulla
Causes biliary colic (intense, spasmodic pain).
Pain develops in the epigastric region
Later the pain shifts to the right hypochondriac region at the junction of the 9th costal cartilage and the lateral border of the rectus sheath, indicated by the linea semilunaris.
Gallstones in the DuodenumImpacted gallstone in its duct may develop adhesions with adjacent viscera.
May ulcerate the tissue boundaries between the gallbladder and superior part of the duodenum and the transverse colon are most likely to develop a fistula: cholecystenteric fistula.
The fistula would enable a large gallstone, incapable of passing though the cystic duct, to enter the alimentary tract .
A large gallstone entering the small intestine in this way may become trapped at the ileocecal valve, producing a bowel obstruction (gallstone ileus).
Cholecystectomy
The cystic artery most commonly arises from the right hepatic artery in the cystohepatic triangle (Calot triangle).
Cystohepatic triangle: BoundedInferiorly: Cystic ductMedially: Common hepatic ductSuperiorly: Inferior surface of the liver
Thank you