Zin en onzin van transfusies - hematologiecongres.nl · Rational Impact of anemia on morbidity and...
43
Transcript of Zin en onzin van transfusies - hematologiecongres.nl · Rational Impact of anemia on morbidity and...


Zin en onzin van transfusies
Sacha Zeerleder

Belangenverklaring In overeenstemming met de regels van de Inspectie van de Gezondheidszorg (IGZ)
Naam: Sacha Zeerleder
Organisatie: Academisch Medisch Centrum Amsterdam/Sanquin
☐
☐
Type van verstrengeling / financieel belang Naam van commercieel bedrijf
Ontvangst van subsidie(s)/research ondersteuning: Viropharma
Ontvangst van honoraria of adviseursfee: Viropharma, Alexion
Lid van een commercieel gesponsord ‘speakersbureau’:
Financiële belangen in een bedrijf (aandelen of opties):
Andere ondersteuning (gelieve te specificeren):
Wetenschappelijke adviesraad:
Ik heb geen 'potentiële' belangenverstrengeling
Ik heb de volgende mogelijke belangenverstrengelingen:


Separate whole blood into:
• Erytrocytes
• Plasma
• Buffycoat = “white dust” above the erythocytes
Whole blood
Preparation blood products

• Centrifugation whole blood (4400 g)
Separation whole blood

Plasma
“ Buffy coat”: leukocytes en thrombocytes
Erythrocytes
After centrifugation

Temp. Storage Prize
Erythrocytes 2-6 C 35 days € 200
Thrombocytes 20 C 5-7 days (shaker)
€ 485 (5 E)
Plasma - 30C 1 year € 172
Storage blood products

Eythrocyte (red blood cell) transfusion

• 1665: transfusion dog dog
• 1667:Denis: calf human
• 1827: Blundell: human human
• 1901: Landsteiner: ABO system
• 1930: first blood bank
• 1940: Rhesus system
Transfusion history

• Het verwijderen van een groot deel van de leukocyten door product over een filter te brengen.
Erythrocytes
• 270 mL (Ht 0.57 L/L) • <20 mL plasma • < 1 x 106 leukocytes • Shelf life 35 days at 2-6ºC • Contains 250 mg iron
Radiation 25 Gy Shelf live • 14 days • product >14 days old: 24 hrs after radiation

12
Erythrocyte consumption Dutch UMCs 2005-2014
Ee
nh
ed
en

Role of oxygen delivery
Oxygen delivery (DO2)
= cardiac output x arterial oxygen content

Oxygen delivery (DO2)
cardiac output x
arterial oxygen content
• heart rate • stroke volume
Erythropoietin hemoglobin synthesis Rightward shift of oxyhemoglobin dissociation curve → increased O2 delivery

• ABO mismatch
– incidence
– mortality
• Delayed hemolysis
• Alloimmunisation
– Ery’s
– Trombo/Leuko
• Allergic reaction
• Fever
• Volume “overload”
• TRALI
1 op 6.000-20.000
1 op 100.000-500.000
1 op 2.500
1%
10%
1-4%
0,1-1%
10-40%
1 op 5.000-10.000
Transfusion complications

To transfuse or not transfuse, that’s the question
Female, 25 years old Sportive (Polo) • progressive endometriosis • Autoimmune gastritis Fatigue, “heavy legs” when doing sports
Male, 83 years old Used to be sportive (Army, polo) • Coronary artery disease, 2 MI • Prostatic cancer- stable • Diabetes mellitus • Chronic gastritis Fatigue, shortness of breath, angina pectoris when climbing stairs
Hb = 4.9 mmol/L
Transfusion?
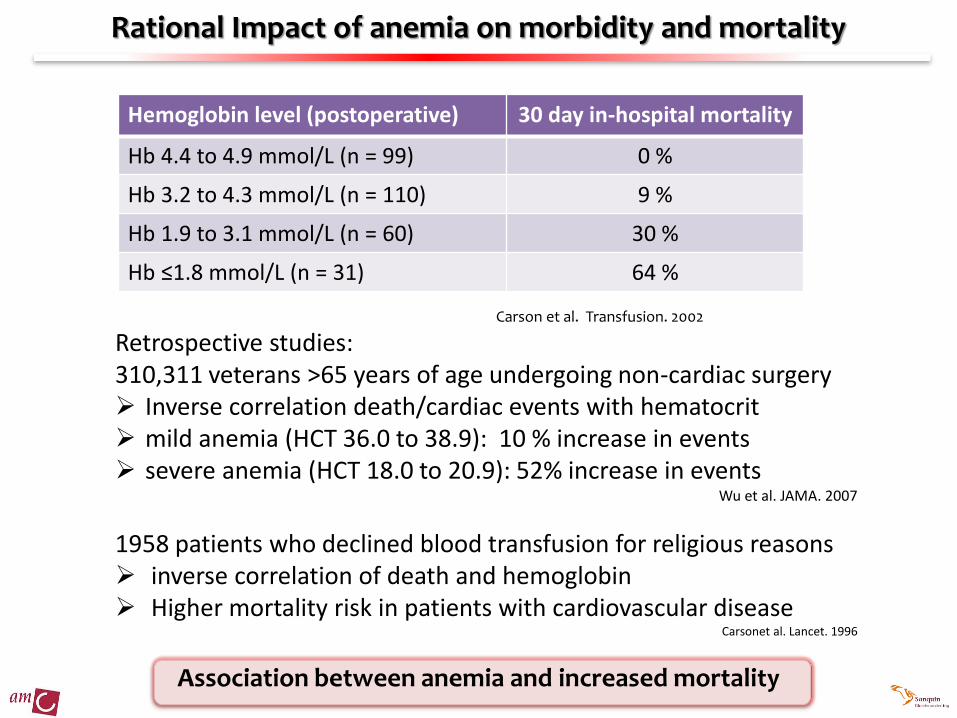
Rational Impact of anemia on morbidity and mortality
Association between anemia and increased mortality
Hemoglobin level (postoperative) 30 day in-hospital mortality
Hb 4.4 to 4.9 mmol/L (n = 99) 0 %
Hb 3.2 to 4.3 mmol/L (n = 110) 9 %
Hb 1.9 to 3.1 mmol/L (n = 60) 30 %
Hb ≤1.8 mmol/L (n = 31) 64 %
Carson et al. Transfusion. 2002
Retrospective studies: 310,311 veterans >65 years of age undergoing non-cardiac surgery Inverse correlation death/cardiac events with hematocrit mild anemia (HCT 36.0 to 38.9): 10 % increase in events severe anemia (HCT 18.0 to 20.9): 52% increase in events
Wu et al. JAMA. 2007
1958 patients who declined blood transfusion for religious reasons inverse correlation of death and hemoglobin Higher mortality risk in patients with cardiovascular disease
Carsonet al. Lancet. 1996

Rational for transfusion
association between anemia and increased mortality
Correction of anemia
What is the optimal hemoglobin threshold to correct anemia? Does transfuison improve mortality?

Optimal threshold?

Optimal threshold to correct anemia?
• American Society of Anaesthesiology • British Committee for Standards in Hematologic Australian and New
Zealand Society of Blood Transfusion • Eastern Association for Surgery of Trauma (EAST) and the American College
of Critical Care Medicine of the Society of Critical Care Medicine (SCCM) • European Society of Cardiology (ESC) • Society of Thoracic Surgeons and the Society of Cardiovascular
Anaesthesiologists • Transylvanian Blood Banking Association (Dracula) • AABB (formerly the American Association of Blood Banks) • American College of Physicians • Dutch CBO richtlijn bloedtransfusie
Hb > 6 mmol/L Transfusion not necessarily beneficial
Hb 4-6 mmol/L Beneficial effect dependent on patient’s condition
Hb < 4 mmol/L Transfusion most probably beneficial
Wang et al. Vox Sang 2010; Perioperative red blood cell transfusion. JAMA 1988; Practice Guidelines for blood component therapy: A report by the American Society of Anesthesiologists Task Force on Blood Component Therapy. Anesthesiology 1996; Murphy et al Br J Haematol 2001; Clinical Practice Guidelines: Appropriate Use of Red Blood Cells. 2001; Napolitano et al. Crit Care Med 2009; Hamm et al. Eur Heart J 2011; Ferraris et al. Ann Thorac Surg 2011; Carson et al. Ann Intern Med 2012; 157:49.

Patient condition matters
• Can the patient compensate the anemia (cardiopulmonary condition)?
• Is there evidence of acute and ongoing blood loss?
• Is there evidence for increased oxygen consumption (sepsis, fever)
• Are there any signs of atherosclerosis (heart, brain, kidney)

Dutch 4-5-6 rule
• Hb < 4 mmol/l • Acute blood loss in a healthy individual (<60 yrs)
• Hb < 5 mmol/L • Acute blood loss in a healthy individual (>60 yrs) • Acute blood loss in polytrauma • Preoperative (<60 yrs) with an expected blood loss
>500ml • Fever • Postoperative (e.g. Open heart surgery) • Mild/severe systemic disease
• Hb < 6 mmol/L • Life-threatening severe systemic disease • Inability to increase cardiac output • Septic/toxic patients • Severe long disease • Cerebrovascular diasease

Hb < 3.6 mmol/L (6 g/dL)
Transfusion recommended except in exceptional circumstances
Hb 3.6 mmol/L- 4.3 mmol/L (6 - 7 g/dL)
Transfusion generally likely to be indicated
Hb 4,3 mmol/L – 5 mmol/L (7 to 8 g/dL)
Transfusion should be considered in postoperative surgical patients, including those with stable cardiovascular disease, after evaluating the patient’s clinical status
Hb 5 mmol/L - 6.2 mmol/L (8 to 10 g/dL)
Transfusion generally not indicated, but should be considered for some populations (eg, those with symptomatic anemia, ongoing bleeding, acute coronary syndrome with ischemia)
Hb > 6.2 mmol/L (>10 g/dL)
Transfusion generally not indicated except in exceptional circumstances
AABB guideline

Is correction of anemia beneficial?

• 19 randomized clinical trials comparing • higher (liberal) versus lower (restrictive) transfusion threshold • 6264 medical and surgical patients (adults and children) • Most trials: Hb 4.3 – 6.2 mmol/L (7 and 10 g/dL)
Cochrane review: are transfusions beneficial in anemia
30 day mortality (n=4975 patients included in 11 of 19 trials)
Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012;4:CD002042. doi:10.1002/14651858.CD002042.pub3.

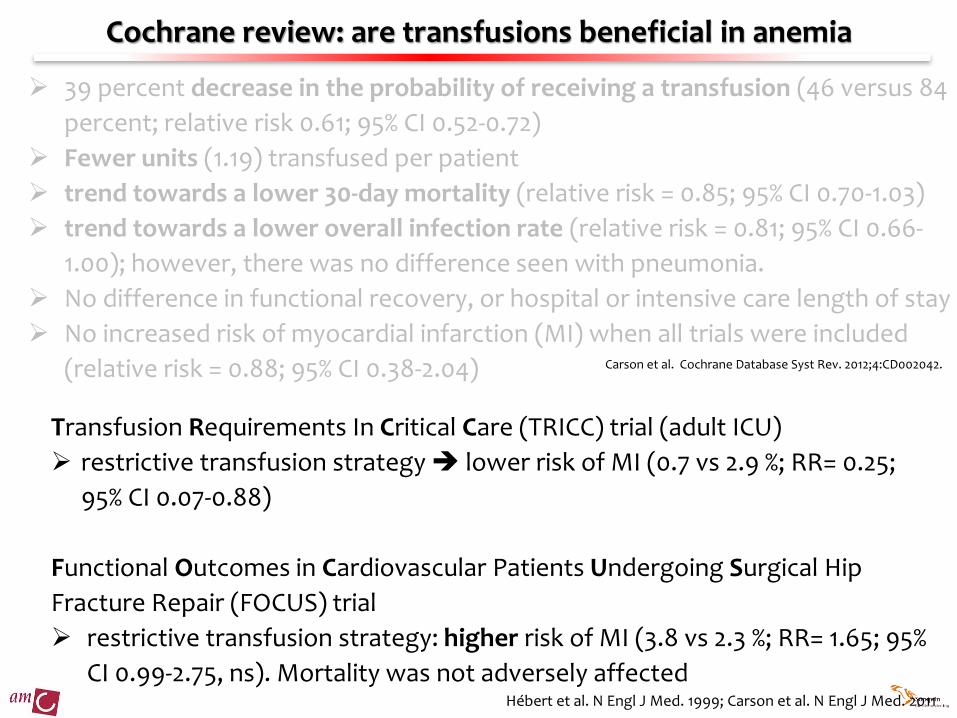
Cochrane review: are transfusions beneficial in anemia
39 percent decrease in the probability of receiving a transfusion (46 versus 84
percent; relative risk 0.61; 95% CI 0.52-0.72)
Fewer units (1.19) transfused per patient
trend towards a lower 30-day mortality (relative risk = 0.85; 95% CI 0.70-1.03)
trend towards a lower overall infection rate (relative risk = 0.81; 95% CI 0.66-
1.00); however, there was no difference seen with pneumonia.
No difference in functional recovery, or hospital or intensive care length of stay
No increased risk of myocardial infarction (MI) when all trials were included
(relative risk = 0.88; 95% CI 0.38-2.04) Carson et al. Cochrane Database Syst Rev. 2012;4:CD002042.
Cochrane review: are transfusions beneficial in anemia
39 percent decrease in the probability of receiving a transfusion (46 versus 84
percent; relative risk 0.61; 95% CI 0.52-0.72)
Fewer units (1.19) transfused per patient
trend towards a lower 30-day mortality (relative risk = 0.85; 95% CI 0.70-1.03)
trend towards a lower overall infection rate (relative risk = 0.81; 95% CI 0.66-
1.00); however, there was no difference seen with pneumonia.
No difference in functional recovery, or hospital or intensive care length of stay
No increased risk of myocardial infarction (MI) when all trials were included
(relative risk = 0.88; 95% CI 0.38-2.04) Carson et al. Cochrane Database Syst Rev. 2012;4:CD002042.
Transfusion Requirements In Critical Care (TRICC) trial (adult ICU)
restrictive transfusion strategy lower risk of MI (0.7 vs 2.9 %; RR= 0.25;
95% CI 0.07-0.88)
Functional Outcomes in Cardiovascular Patients Undergoing Surgical Hip
Fracture Repair (FOCUS) trial
restrictive transfusion strategy: higher risk of MI (3.8 vs 2.3 %; RR= 1.65; 95%
CI 0.99-2.75, ns). Mortality was not adversely affected Hébert et al. N Engl J Med. 1999; Carson et al. N Engl J Med. 2011

Potential approach in anemic patients
Asymptomatic hospitalized patient: hemodynamically stable medical/surgical patients Transfusion: Hb of 4.3 – 5 mmol/L (7 to 8 g/dL) Cardiovascular disease • asymptomatic medical patients with stable CAD: Transfusion <5 mmol/L (8 g/dL)
• symptomatic patients with coronary artery disease is guided by the symptoms and clinical judgment
• Acute coronary syndrome : nobody really knows… consider transfusion when the Hb is between 5 – 6.2 mmol/L (8 and 10 g/dL)
Oncology patient • Curative treatment: similar to medical patients • Palliative care: subjective responses to transfusion 31-70% But: Unnecessary transfusion keep patients in hospital
Carson et al. Ann Intern Med 2012; Kansagara et al. Ann Intern Med 2013; Gleeson et al. Palliat Med 1995; Sciortino et al. J Palliat Care 1993; ; Hébert et al. N Engl J Med. 1999; Carson et al. N Engl J Med. 2011

2014
2013
2012
2011
2010
2009
2008
2007
2006
0
500
1000
1500
2000
ee
nh
ed
en
RB
C (n
)
liberal restrictive
“old” rule (liberal): Hb<6.0 mmol/L: transfusion 3 EC-concentraten “new” rule (restrictive): Hb < 5.0 mmol/L: consider transfusion Hb <6.0 mmol/L with comorbidities (cardial) consider transfusion
Introduction restrictive transfusion strategy dep. Hematology AMC
Reduction of 30% ~420 products ~ 91 kEuro

To transfuse or not transfuse, that’s the question
Female, 25 years old Sportive (Polo) • progressive endometriosis • Autoimmune gastritis Fatigue, “heavy legs” when doing sports
Male, 83 years old Used to be sportive (Army, polo) • Coronary artery disease, 2 MI • Prostatic cancer- stable • Diabetes mellitus • Chronic gastritis Fatigue, shortness of breath, angina pectoris when climbing stairs
Hb = 4.9 mmol/L

Platelet transfusion

5 buffy coats pooled
• 340 mL
• 390 x 109 plts
• < 1 x 106 leucocytes
• < 5 x 109 erythrocytes
• In plasma (or PAS II)
Platelets
Apharesis platelets
• 320 mL
• 360 x109 plts
• HPA/HLA matched

platelets

removal
• Major bleeding
• Acute DIC, MAHA, TTP-HUS, HELLP
• Chronic DIC (aneurysms, malignancy, hemagiomas)
• Infection (Malaria)
• Extensive thrombosis/pulmonary embolism
• Extracorporal-/intravascular device
increased consumption
destruction • severe infection (sepsis, dengue etc) • HIT •AITP • PTP (active and passive) • drugs
sequestration •hypersplenism •hypothermia
hemodilution • fluid resuscitation • blood products
circulation
Pseudothrombocytopenia
• Clotting sample • EdTA ex-vivo aggregation • Rosette formation (leucocytes) • GpIIb/IIIa inhibitor induced clumping • Macrothrombocytes
production
• toxic/radiation • MDS/leukemia • myelophtysis • chronic liver disease • infection
Decreased production
Tc pool
Etiology of thrombocytopenia?

To transfuse or not transfuse, that’s the question
Female, 25 years old Acute myeloid leukemia
Tc = <10x109/L
Female, 25 years old polytrauma with massive bleeding
Female, 25 yrs old TTP
Tc = <10x109/L Tc = 30x109/L
Transfusion?

Endothelial cell activation/damage
Primary haemostasis fully dependent on platelets

Slichter 2004
Platelet count and efficacy primary hemostasis
Harker&Slichter, N Engl J Med 1972
Critical threshold
~10x109/L

Bleeding risk- platelet threshold?
Holler et al. 2009
Gmur et al. 1991

Platelet transfusion in clinical practice
Clinical situation/intervention Platelet trigger (x109/L)
Thrombocytopenia without bleeding 10
Thrombocytopenia plus additional factors (e.g. Fever) 20
Surgery, bleeding (WHO3) 50
Neurosurgery (incl. Opthalomological interventions), bleeding WHO4
100
Platelet transfusion: No indication or only in case of life threating conditions:
Idiopathic thrombcytopenic purpura (ITP)
Thrombotic thrombocytopenic purpura (TTP)
Disseminated intravascular coagulation (DIC)

Prophylactic vs therapeutic platelet transfusion strategy
Data not entirely clear – however, prophylactic treatment seems still reasonable

To transfuse or not transfuse, that’s the question
Female, 25 years old Acute myeloid leukemia
Tc = <10x109/L
Female, 25 years old Polytrauma with massive bleeding
Female, 25 yrs old TTP
Tc = <10x109/L Tc = 30x109/L
Transfusion?
Summary
We have some idea on when to transfuse….
There are triggers - however, patient condition matters
Erythrocyte transfusion:
• < 4 mmol/L (transfusion) and >6 mmol/L (no transfusion)
• 4-6 mmol/L? dependent on comorbidities and clinical situation
• Restrictive transfusion strategy: might be beneficial
Platelet transfusion:
Trigger for prophylactic transfusion : 10 x 109/L (20 in case of fever)




![[PPT]PEMERIKSAAN LABORATORIUM PADA ANEMIA … · Web viewPEMERIKSAAN LABORATORIUM PADA ANEMIA HEMOLITIK ELLYZA NASRUL Anemia hemolitik - Klasifikasi anemia berdasarkan morfologi anemia](https://static.fdocuments.net/doc/165x107/5c85338309d3f279718c7183/pptpemeriksaan-laboratorium-pada-anemia-web-viewpemeriksaan-laboratorium-pada.jpg)