Cardiovascular Outcomes in Patients with Drug Eluting Stents ...

TitIbPtTn
FCStrcaAc�
2
Journal of the American College of Cardiology Vol. 53, No. 18, 2009© 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00P
Use of Drug-Eluting Stentsin Acute Myocardial InfarctionA Systematic Review and Meta-Analysis
Somjot S. Brar, MD, Martin B. Leon, MD, Gregg W. Stone, MD, Roxana Mehran, MD,Jeffrey W. Moses, MD, Simerjeet K. Brar, BS, George Dangas, MD, PHD
New York, New York
Objectives The primary aim of the analysis was to compare outcomes by stent type for death, myocardial infarction (MI), targetvessel revascularization (TVR), and stent thrombosis in randomized trials of ST-segment elevation myocardial infarc-tion (STEMI). A secondary analysis was performed among registry studies.
Background It is not known whether there are differences in outcomes between drug-eluting stents (DES) and bare-metalstents (BMS) for STEMI.
Methods We searched MEDLINE, EMBASE, the Cochrane Library, and Internet sources for articles comparing outcomes be-tween DES and BMS among patients with STEMI between January 2000 and October 2008. Randomized controlledtrials and registries including patients 18 years of age and older receiving a DES or BMS were included. We extractedvariables related to the study design, setting, participants, and clinical end points.
Results Thirteen randomized trials were identified (N � 7,352). Compared with BMS, DES significantly reduced TVR (relativerisk [RR]: 0.44; 95% confidence interval [CI]: 0.35 to 0.55), without increasing death (RR: 0.89; 95% CI: 0.70 to 1.14),MI (RR: 0.82; 95% CI: 0.64 to 1.05), or stent thrombosis (RR: 0.97; 95% CI: 0.73 to 1.28). These observations weredurable over 2 years. Among 18 registries (N � 26,521), DES significantly reduced TVR (RR: 0.54; 95% CI: 0.40 to0.74) without an increase in MI (RR: 0.87, 95% CI: 0.62 to 1.23). Death was significantly lower in the DES groupwithin 1 year of the index percutaneous coronary intervention, but there were no differences within 2 years (p � 0.45).
Conclusions The use of DES appears safe and efficacious in randomized trials and registries of patients with STEMI. The DES sig-nificantly reduce TVR compared with BMS, without an increase in death, MI, or stent thrombosis within 2 years of theindex procedure. (J Am Coll Cardiol 2009;53:1677–89) © 2009 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2009.03.013
PmoCtaaai
rDFr
M
Smv
he aim of primary percutaneous coronary intervention (PCI)s to rapidly achieve complete myocardial reperfusion. Al-hough balloon angioplasty can restore TIMI (Thrombolysisn Myocardial Infarction) flow grade 3, stents provide addedenefit by reducing the risk of reocclusion and reinfarction afterCI (1,2). Whether additional benefit can be achieved with
he use of drug-eluting stents (DES) remains undetermined.he primary benefit of DES is a marked reduction in reste-osis; whether this should be a consideration during primary
rom the Center for Interventional Vascular Therapy, Columbia University Medicalenter, and the Cardiovascular Research Foundation, New York, New York. Dr.omjot Brar receives research grant support from Boston Scientific. Dr. Leon is onhe scientific advisory board of Abbott, Boston Scientific, and Medtronic. Dr. Stoneeceives research support from Boston Scientific, Abbott Vascular, and The Medi-ines Company. Dr. Mehran is a speaker/consultant to Cordis, Abbott, Medtronic,nd Boston Scientific (all modest, �$10,000). Dr. Moses is a speaker for Cordis,bbott, and Boston Scientific (all modest, �$10,000). Drs. Dangas is a speaker/
onsultant to Cordis, Abbott, Medtronic, and Boston Scientific (all modest,$10,000).
cManuscript received January 27, 2009; revised manuscript received February 25,
009, accepted March 2, 2009.
CI remains unknown. Patients with ST-segment elevationyocardial infarction (STEMI) were excluded from the piv-
tal SIRIUS (Sirolimus-Eluting Stent in de Novo Nativeoronary Lesions) and TAXUS IV (Paclitaxel-Eluting Stent)
rials that led to Food and Drug Administration (FDA)pproval of these devices, and DES for primary PCI remainsn “off-label” use (3,4). Recent reports have raised concernsbout the relative safety of DES, in particular for off-label use,ncluding STEMI (5–8).
We performed a systematic review and meta-analysis ofandomized controlled trials (RCTs) reporting outcomes ofES versus bare-metal stents (BMS) in patients with STEMI.or comparison, we also performed an analysis from available
egistry studies to determine outcomes in a “real-world” setting.
ethods
tudy objectives and design. The primary aim of theeta-analysis was to compare the outcomes of DES
ersus BMS in randomized trials of STEMI. The out-
omes of interest were mortality, myocardial infarction
SATsH
msrSd2a2ltFpOd
tFDfcdpitwwOs
1678 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
(MI), target vessel revasculariza-tion (TVR), and stent thrombo-sis defined according to the studyprotocols. We also performed asecondary analysis for death, MI,TVR, and stent thrombosis foridentified registry studies.Study search strategy. UsingMedline, EMBASE, and theCochrane Library, we performedsearches for possible abstractsusing various combinations ofthe terms “myocardial,” “infarc-tion,” “acute,” “elevation,” “drug,”“stent,” and “eluting” in the ab-stract/title. Two reviewers (S.S.B.and S.K.B.) identified articles eli-gible for further review by per-forming a screen of abstracts andtitles. If a study was deemed rele-vant, the manuscript was obtainedand reviewed. We also searchedconference proceedings for the
cientific Sessions of the American College of Cardiology,merican Heart Association, Transcatheter Cardiovascularherapeutics, and the European Society of Cardiology. Web
ites, including cardiosource.com, TCTMD.com, the-eart.org, and escardio.org, were also searched for relevant
Figure 1 Flow Chart of Meta-Analysis
DES � drug-eluting stent(s); FDA � Food and Drug Administration; STEMI � ST-se
Abbreviationsand Acronyms
BMS � bare-metal stent(s)
CI � confidence interval
DES � drug-eluting stent(s)
MI � myocardial infarction
NNT � number needed totreat
PCI � percutaneouscoronary intervention
RCT � randomizedcontrolled trial
RD � risk difference
RR � relative risk
STEMI � ST-segmentelevation myocardialinfarction
TIMI � Thrombolysis InMyocardial Infarction
TVR � target vesselrevascularization
aterials. Review articles and prior meta-analysis of theubject were sought (9–11). The references of these wereeviewed for additional possible studies.tudy identification. We searched through the previouslyescribed data sources for possible studies from January 1,000, to October 30, 2008. These dates were thought to beppropriate as the first DES was not FDA approved until003. The search was not limited to the English-languageiterature. We performed text searches for studies that methe following criteria: 1) direct comparison between eitherDA-approved DES (Cypher or Taxus) and a BMS inatients with STEMI; 2) reporting of outcomes beforectober 30, 2008; and 3) reporting of the incidence of
eath.The final search identified 31 studies, 13 randomized
rials, and 18 registries, which directly compared 1 of the 2DA-approved DES to BMS (Fig. 1).ata extraction. We extracted pre-specified data elements
rom each trial, including study design, stent type, sampleharacteristics, pharmacologic strategy, duration of clopi-ogrel therapy, sample size, outcome measures, primary endoint, and other study characteristics. The number of eventsn each trial were extracted, when available, on the basis ofhe intention-to-treat approach. If TVR was not reported,e used target lesion revascularization instead. All outcomesere defined according to the protocol definition (see thenline Appendix for end point definitions). For registry
tudies we used adjusted treatment effects whenever possi-
elevation myocardial infarction.
gment
Randomized Controlled Trials
Table 1 Randomized Controlled Trials
BASKET-AMI(32)
DEDICATION-AMI(29)
Di Lorenzoet al.(21)
HAAMU- STENT(22)
MISSION(30)
MULTI-STRATEGY(28)
PASSION(24)
SELECTION(26)
SESAMI(25)
STRATEGY(27)
TYPHOON(23)
HORIZONS-AMISTENT(31)
Diazde la Llera
et al.(33)
No. screened — 1,687 — 213 575 1,030 1,037 — 423 — 2,019 3,602 150
No. enrolled 217 626 270 164 376 745 619 80 320 175 712 3,006 120
Mean follow-up,months
18 8 12 17 12 8 12 7 12 24 12 12 12
Clopidogrelduration,months
6 12 6 12 12 3 6 9 12 3 6 6 9
Stent type SES, PES SES, PES SES, PES PES SES SES PES PES SES SES SES PES SES
Timing, h — �12 — �12 — �12* �12 �12 �12 �12* �12 �12 �12
GP IIb/IIIa, % 65% 96% — 100% — 100% 27% 100% 75% 100% 72% 50% 100%
Symptom toballoon, min
— 200 — — — 196 180 201 240 180 230 222 174
No. of centers 1 2 — 1 1 16 2 1 1 1 48 123 1
Rescue PCI, % — — — 45% — 0% — 0% 18% 0% — — 18%
LAD culprit, % — 41% — 44% 55% 43% 50% 50% 50% 45% 46% 43% 43%
Age, yrs, mean — 62 64 63 59 63 61 60 61 63 59 60 64
Female, % — 27% — 28% 22% 25% 24% 18% 19% 27% 22% 23% 21%
Diabetes, % — 10% — — — 15% 11% 12% 21% 14% 16% 16% 16%
Primary endpoint
Death, MI,TVR andstroke
�70% ST-segmentresolution90 min afterPCI
Death, MI,TVR,andstroke
In-segmentlate loss
In-segmentlate loss
Death, MI, TVR Death,MI,TLR
Neointimalhyperplasiaby IVUS
Binaryrestenosis
Death, MI, stroke,and binaryrestenosis
TVF† Death, MI,stroke, andST
Death, MI,TLR
*Up to 24 h was permitted with evidence of ongoing ischemia; †composite of target vessel revascularization (TVR), recurrent infarction, or target vessel-related death at 1 year..AMI � acute myocardial infarction; GP � glycoprotein; IVUS � intravascular ultrasound; LAD � left anterior descending artery; MI � myocardial infarction; PCI � percutaneous coronary intervention; PES � paclitaxel�eluting stent(s); SES � sacrolimus-eluting stent(s);
ST � stent thrombosis; TLR � target lesion revascularization; TVF � target vessel failure.
1679JACC
Vol.53,No.18,2009Brar
etal.
May
5,2009:1677–89DES
inAM
I:M
eta-Analysis

boadSlmsttoitcB
iarea
ts
sdeaswssws
bgerae
1680 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
le. When a study reported follow-up at 1 and 2 years,utcomes for both time periods were abstracted. Twouthors (S.S.B. and S.K.B.) independently extracted all trialata (kappa 0.95).tatistical analysis. From the abstracted data, we calcu-
ated the relative risk (RR) using the inverse varianceethod for each study outcome to allow for pooling of
imilar outcomes. For the randomized trials, we also reporthe outcomes as the absolute risk difference (RD), becausehis conveys both the absolute magnitude and the directionf effect. Furthermore, the number needed to treat (NNT)s easily calculated from this measure (NNT � 1/RD). Inhis analysis, a negative RD indicates an advantage for DESompared with BMS. In contrast, a positive RD means thatMS is favored over DES.The average effects for the outcomes and 95% confidence
ntervals (CI) were obtained using a random effects model,s described by DerSimonian and Laird (12). We chose theandom effects method because of its conservative summarystimate and incorporating between and within study vari-
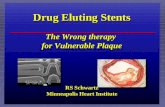
Figure 2 Outcomes in Randomized Trials
Size of data markers indicates the weight of the study: (A) mortality; (B) myocardrevascularization (TVR); and (D) stent thrombosis. BMS � bare-metal stent(s); CI
nce. To assess heterogeneity of RRs across trials, we used b
he Cochrane Q statistic (a p value �0.1 was consideredignificant) and the I2 statistic.
Sensitivity analyses were performed to assess the effects ofelected measures of study quality and clinical factors oneath, MI, TVR, and stent thrombosis. The influence ofach study was estimated by deleting each in turn from thenalysis and noting the degree to which the effect size andignificance of the treatment effect changed. This analysisas performed for each study outcome. We considered a
tudy influential if the exclusion of it changed our conclu-ion or the effect estimate by at least 20%. Meta-regressionas used to evaluate predictors of death, MI, and TVR by
tent type.Using regression techniques, we explored the relationship
etween baseline risk, defined as the TVR rate in the BMSroup, and the treatment effects. The absolute risk differ-nce was modeled as a weighted linear function of the TVRate in the BMS group. Because of the limitations of thispproach, we then applied a bivariate multilevel randomffects model for the binomial outcomes (13–15). The
rction; (C) target vesseldence interval; DES � drug-eluting stent(s). Continued on next page.
ial infa� confi
ivariate model had distinct random effects for the DES and

BNav
ppraaeapi
01MSst(S
R
EtT4tpesT2trimt(SIcv
1681JACC Vol. 53, No. 18, 2009 Brar et al.May 5, 2009:1677–89 DES in AMI: Meta-Analysis
MS groups. The model was constructed using ProcLMIXED in SAS (SAS Institute, Cary, North Carolina)
nd yielded maximum likelihood estimates for between trialariance in each treatment group.
Funnel plots were used to assess for the presence ofublication and other reporting biases by plotting therecision (inverse of the standard error) against the log riskatio. Using the Begg and Mazumdar rank correlation (16)nd Egger’s linear regression (17) method, we examined thessociation between the study size and estimated treatmentffects. The Duval and Tweedie (18) nonparametric trimnd fill method was used to obtain symmetry in the funnellot and to determine the impact of hypothetical negative ormputed studies on the pooled estimate.
The p value threshold for statistical significance was set at.05 for effect sizes. Analyses were conducted in STATA0.0 (Stata Corp., College Station, Texas), Comprehensiveeta-analysis 2.0 (Biostat, Englewood, New Jersey), and
AS version 9.2 (SAS Institute, Cary, North Carolina). Thetudy was performed in accordance with the recommenda-ions set forth by the Quality of Reporting of Meta-AnalysisQUOROM) and the Meta-Analysis of Observational
Figure 2 Continued
tudies in Epidemiology (MOOSE) work groups (19,20). M
esults
ligible studies. Table 1 lists the study characteristics forhe 13 randomized trials selected for inclusion (21–33).hese trials yielded a cumulative total of 7,352 patients,,515 of whom were randomly assigned to DES and 2,837o BMS. In 3 of the trials, both the sirolimus- and theaclitaxel-eluting stents were used; in 4 trials, the paclitaxel-luting stent was used; and in 6 studies, sirolimus-elutingtents were used. The mean ages ranged from 59 to 63 years.he frequency of diabetes mellitus ranged from 10% to1%. The left anterior descending artery was identified ashe culprit vessel in 41% to 55% of the patients. Allandomized patients received aspirin (at least 75 mg)ndefinitely and clopidogrel loading (300 to 600 mg). The
inimum duration of clopidogrel therapy ranged from 6o 12 months for all studies except 2: the STRATEGYSingle High-Dose Bolus Tirofiban and Sirolimus-Elutingtent vs Abciximab and Bare Metal Stent in Myocardialnfarction) trial and the MULTISTRATEGY (Multi-entre Evaluation of Single High-Dose Bolus Tirofibans Abciximab With Sirolimus-Eluting Stent or Bare
etal Stent in Acute Myocardial Infarction Study) trial

rtMd(4t0Rfws
BDtHfreat0tmivewtea4pscitcM(Dc(bnehsDTdI(po
BCi��T
twdwgroaorvoclSfpTii((gh
(
1682 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
equired a minimum duration of 3 months of clopidogrelherapy.
ortality. All 13 randomized trials reported mortalityata. There were 288 events among the 7,352 patients3.9%). The incidence in the DES group was 3.7% (167 of,515), and in the BMS group it was 4.3% (121 of 2,837);he corresponding pooled RR for DES versus BMS was.89 (95% CI: 0.70 to 1.14; p � 0.36) (Fig. 2A). The pooledD between the groups was �0.4%, nonsignificantly in
avor of DES (95% CI: �1.4% to 0.5%; p � 0.38). Thereas no evidence of statistical heterogeneity among these
tudies (p heterogeneity � 0.48).There were 2 trials with a nonsignificant RD in favor of
MS, the DEDICATION-STENT (Drug Elution andistal Protection During Percutaneous Coronary Interven-
ion in ST Elevation Myocardial Infarction) trial and theAAMU-STENT (Helsinki Area Acute Myocardial In-
arction Treatment Re-Evaluation) trial. The former was aandomized comparison of the paclitaxel- or sirolimus-luting stents versus BMS. Major adverse cardiac events—composite of death, MI, and target lesion revasculariza-
ion—was lower in the DES group (8.9% vs. 14.4%, p �.001), driven by a reduction in target lesion revasculariza-ion with DES (5.1% vs. 13.1%, p � 0.001). Cardiacortality and overall mortality were nonsignificantly greater
n the DES group, 4.2% versus 1.6% (p � 0.09) and 5.1%ersus 2.6% (p � 0.14), respectively. However, this differ-nce in death could not be attributed to stent thrombosis,hich was identical in the 2 arms. The HAAMU-STENT
rial randomly allocated 164 patients to either a paclitaxel-luting stent or BMS; the trial was underpowered forssessment of clinical end points. Mortality at 1 year was.9% in the BMS group compared with 9.8% in theaclitaxel-eluting stent group, a difference that was notignificant (p � 0.23). Consistent with a practice that isommon in some European countries, 45% of the patientsn the HAAMU-STENT trial were treated with a facili-ated PCI approach, a treatment strategy that remainsontroversial.
I. There were 261 events among the 7,352 participants3.6%). The incidence of MI was 3.4% (153 of 4,515) in theES group and 3.8% (108 of 2,837) in the BMS group; the
orresponding pooled RR for DES versus BMS was 0.8295% CI: 0.64 to 1.05; p � 0.12) (Fig. 2B). The pooled RDetween the groups was �0.4% (95% CI: �1.3% to 0.3%),onsignificantly in favor of DES (p � 0.19). There was novidence of statistical heterogeneity between studies (peterogeneity � 0.92). The point estimates for any giventudy did not reach statistical significance in favor of eitherES or BMS.VR. Among the 13 selected randomized trials, the inci-ence of TVR was lower with DES compared with BMS.n 9 of the studies, the reduction was statistically significantFig. 2C). There were 569 TVR events among the 7,352articipants (7.7%). The incidence of TVR was 5.3% (241
f 4,515) in the DES group and 11.5% (328 of 2,837) in theMS group; the corresponding pooled RR was 0.44 (95%I: 0.35 to 0.55; p � 0.001), yielding a 56% risk reduction
n TVR with DES. The pooled RD between groups was7.0%, significantly in favor of DES (95% CI: �9.2% to4.7%; p � 0.001). The NNT with a DES to prevent 1VR was 14 patients (95% CI: 11 to 21).We explored whether the baseline risk of patients in each
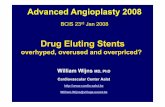
rial was related to the magnitude of the treatment benefitith DES for TVR. Baseline risk or the control rate wasefined as the TVR event rate in the BMS group. Aeighted regression analysis for the TVR rate in the BMSroup showed that the benefit of DES was greater in higherisk groups (p � 0.001) (Fig. 3). Because of the limitationsf this approach, namely regression to the mean, we appliedbivariate random-effects mixed model for the binomial
utcome. The estimated residual variance given the controlate was 0.0106, and was considerably smaller than theariance of the treatment effect, 0.1280. In summary, 92%f the variation in the treatment effects was explained by theontrol rate; so the variation in the treatment effect wasargely explained by variation in the baseline risk.tent thrombosis. All 13 randomized trials reported the
requency of stent thrombosis (Fig. 2D). Among 7,352atients, there were 194 stent thrombosis events (2.6%).he incidence of stent thrombosis was 2.7% (120 of 4,515)
n the DES group and 2.6% (74 of 2,837) in the BMS groupn the first year; the corresponding relative risk was 0.9695% CI: 0.72 to 1.30; p � 0.81). The pooled RD was 0.1%95% CI: �0.8% to 0.6%), not significantly different betweenroups (p � 0.79). There was no evidence of statisticaleterogeneity among the trials (p heterogeneity � 0.95).Four trials reported outcomes beyond the first year
22,24,27,32). There was no difference in the effect for stent
Figure 3 Relationship Between Baseline Risk and RiskDifference for TVR in Randomized Controlled Trials
Relationship between baseline risk (target vessel revascularization [TVR] ratein the bare-metal stent [BMS] group) and risk difference for TVR in randomizedcontrolled trials. The plot shows the regression of baseline risk on the risk dif-ference. A negative risk difference favors drug-eluting stents, whereas a posi-tive risk difference favors BMS. The size of each circle relates to the weight ofeach trial. p � 0.001.

t(C0Sr
dMcs
o
R
A
1683JACC Vol. 53, No. 18, 2009 Brar et al.May 5, 2009:1677–89 DES in AMI: Meta-Analysis
hrombosis between the first and the second year after PCIp � 0.99). In the second year, the RD was �0.6% (95%I: �2.3% to 1.1%; p � 0.51); the corresponding RR was.78 (95% CI: 0.38 to 1.67; p � 0.52).ensitivity and influence analysis. We also examined theobustness of the findings among the randomized studies to
Figure 4 Stratified Analyses of Randomized Trials
The pooled estimates are reported as risk difference. Abbreviations as in Figure 2
egistry Studies
Table 2 Registry Studies
Study, Author (Ref. #) Year Stent Type
LongestFollow-Up(Months) Outcomes
Lemos et al. (49) 2004 SES 10 Death, MI, TVR,
Cheneau et al. (37) 2005 SES 6 Death, MI, TVR,
Newell et al. (40) 2006 SES 6 Death, MI, TVR,
Percoco et al. (41) 2006 SES 12 Death, MI, TVR,
Nakamura et al. (50) 2006 SES, PES 36 Death, ST
Bose et al. (36) 2007 SES, PES 19 Death, MI, TVR,
GRACE (51) 2007 SES, PES 24 Death
Kupferwasser et al. (38) 2007 SES, PES 12 Death, MI, TVR,
Vagaonescu et al. (35) 2007 SES, PES 24 Death
Mauri et al. (39) 2008 SES, PES 24 Death, MI, TVR
Romano et al. (42) 2008 SES, PES 12 Death, MI, TVR,
Slottow et al. (43) 2008 SES, PES 12 Death, MI, TVR,
Vlaar et al. (44) 2008 SES, PES 24 Death, MI, TVR
Hannan et al. (45) 2008 SES, PES 18 Death, MI
Shishehbor et al. (46) 2008 SES, PES 24 Death, TVR
Jensen et al. (47) 2008 SES, PES 24 Death, MI, TVR
Brodie et al. (48) 2008 SES, PES 24 Death, MI, TVR,
Kukreja et al. (34) 2008 SES, PES 36 Death, MI, TVR,
bbreviations as in Table 1.
ifferent assumptions in a sensitivity analysis for mortality,I, TVR, and stent thrombosis (Fig. 4). The overall effect
alculated by either a random or fixed effects model yieldedimilar overall estimates for each of the end points.
We then performed stratified analysis across a numberf key study characteristics and clinical factors. Method-
N (DES/BMS)No. of
CentersAge, yrs(Mean)
Female(%)
Diabetes(%)
LADCulprit
(%)
369 (186/183) 1 59 23 11 55
607 (103/504) 1 67 22 25 39
306 (156/150) 1 63 30 16 38
,617 (205/1,412) 13 64 26 19 52
,838 (1,450/388) 8 68 23 32 46
188 (170/18) 1 60 29 21 39
,298 (569/1,729) �10 — — — —
261 (131/130) 1 65 25 23 43
,174 (2,217/2,957) �10 63 32 26 —
,421 (1,227/1,194) �5 62 31 18 41
370 (120/250) 1 61 26 25 42
240 (120/120) 1 63 36 40 —
,093 (536/557) 1 64 32 18 43
,926 (1,154/772) �10 58 28 14 43
480 (240/240) 1 61 34 18 42
,756 (783/2,973) 3 63 27 9 44
,839 (1,292/548) 8 60 27 19 34
,738 (1,207/531) 1 59 21 10 52
.
ST
ST
ST
ST 1
1
ST
2
ST
5
2
ST
ST
1
1
3
ST 1
ST 1

ostdctomWlfsdm
ecosf
rHctct(0RS(S1rac
sy
1684 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
logical quality was assessed in terms of trial size andingle-center versus multicenter trial design. By trial size,he estimated treatment effect was similar for small (�20eaths) and large (�20 deaths) studies. The 8 single-enter studies indicated greater benefit for DES than didhe 5 multicenter studies, but confidence intervals widelyverlapped. All 13 trials reported methods for conceal-ent of allocation; only 1 trial was double blinded (33).hile studies varied in length of follow-up, that had
ittle effect on estimates. With up to 24 months ofollow-up, there was no difference in death, MI, TVR, ortent thrombosis between DES and BMS. Lastly, theuration of clopidogrel therapy, �6 months versus �6onths, had little effect on estimates.The influence of each study was estimated by deleting
ach in turn from the analysis; there was no significanthange in the pooled treatment effect for death, MI, TVR,r stent thrombosis. There continued to be no evidence oftatistical heterogeneity across trials. In influence analysis
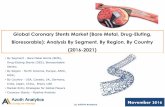
Figure 5 Outcomes in Registry Studies
Size of data markers indicates the weight of the study: (A) death within 1 year antarget vessel revascularization (TVR) within 1 year and within 2 years; and (D) stenas in Figure 2. Continued on next page.
or TVR, the NNT to prevent 1 TVR event with DES 0
anged from 13 to 16 patients. Lastly, omission of theORIZONS-AMI (Harmonizing Outcomes With Revas-
ularization and Stents in Acute Myocardial Infarction)rial, the largest trial in the series, did not appreciablyhange our findings. The RRs (95% CI) for death, MI, stenthrombosis, and TVR in the absence of this trial were 0.820.63 to 1.07), 0.82 (0.59 to 1.13), 0.99 (0.69 to 1.43), and.40 (0.32 to 0.49), respectively.egistry studies. We identified 18 registry studies ofTEMI where the outcomes were reported by stent typeTable 2) (34–51). There were 26,521 patients withTEMI, of whom 11,866 were treated with DES and4,656 with BMS. Mortality data were available from all 18egistries. Data on myocardial infarction and TVR werevailable from 14 registries. Eleven studies reported out-omes beyond 1 year.
The pooled treatment effect for mortality yielded aignificant 32% reduction in mortality with DES within 1ear of the index PCI (RR: 0.68; 95% CI: 0.54 to 0.88; p �
n 2 years; (B) myocardial infarction (MI) within 1 year and within 2 years; (C)mbosis within 1 year and within 2 years. RR � relative risk; other abbreviations
d withit thro
.01) (Fig. 5A). However, the mortality difference within 2

yb1GrwoSsSGr(Dtbmn
ab(sd
saCs0
l(tPdtnttaeatutp
1685JACC Vol. 53, No. 18, 2009 Brar et al.May 5, 2009:1677–89 DES in AMI: Meta-Analysis
ears of the index PCI was no longer statistically significantut remained in favor of DES (RR: 0.89; 95% CI: 0.64 to.22; p � 0.45). Among the observational studies, only theRACE (Global Registry of Acute Coronary Events)
egistry reported a statistically significant excess of mortalityith DES. The GRACE registry is a multinational registryf �30,000 patients with acute coronary syndromes. TheTEMI cohort from the GRACE registry represented amall percentage of the full registry; of 2,269 patients withTEMI, only 569 were treated with DES. In contrast toRACE, several large registries have observed a significant
eduction in mortality with DES at 1 and 2 years35,39,45,47). Among these registries, the RR in favor ofES ranged from 0.59 to 0.68 (p � 0.01). Also, most of
he heterogeneity between studies could be accounted fory the GRACE registry; in its absence, heterogeneity,easured as I2, decreased from 86% to 6% (p heteroge-
eity � 0.39).The pooled RR (95% CI) for myocardial infarction within 1
nd 2 years from the index PCI was not significantly differentetween DES and BMS groups at 0.87 (0.62 to 1.23) and 0.960.81 to 1.13), respectively (Fig. 5B). There was no evidence oftatistical heterogeneity among the registry studies for myocar-
Figure 5 Continued
ial infarction (p heterogeneity � 0.10). f
TVR was significantly reduced with DES in the registrytudies (Fig. 5C). Within 1 year of the index PCI, DES wasssociated with a 46% reduction in TVR (RR: 0.54; 95%I: 0.40 to 0.74; p � 0.01). By 2 years, there remained a
ignificant reduction in TVR with DES (RR: 0.71; 95% CI:.61 to 0.83; p � 0.01).Stent thrombosis within 1 year of the index PCI was
ower with DES (RR: 0.52; 95% CI: 0.31 to 0.88; p � 0.01)Fig. 5D), whereas there was no difference between stentypes at 2 years (RR: 0.94; 95% CI: 0.60 to 1.45; p � 0.77).ublication bias. Visual inspection of the funnel plot foreath did not reveal asymmetry in RCTs (Fig. 6A). In support,he Begg rank correlation test and Egger’s regression test wereot statistically significant (p � 0.39 and p � 0.52, respec-ively). However, on visual inspection, there was asymmetry inhe funnel plot in the registry studies (Fig. 6B). Given thesymmetry in the funnel plot on visual inspection, we furtherxplored any potential bias using the Duval and Tweedie trimnd fill method. In this analysis, the asymmetric studies fromhe left-hand side of the funnel plot are trimmed to locate thenbiased effect, and then the plot is filled by reinserting therimmed studies on the left as well as their imputed counter-arts to the right of the mean effect, producing a symmetric
unnel plot. The analysis incorporating 8 hypothetical or
il
D
TpprSr0stnsEs2wamltri
wrufapStLa
bhgajbTgrSstctastBpr
cwptdaDooFatra
itofprsa
1686 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
mputed studies showed the pooled estimates for death were noonger significant in the registry studies.
iscussion
his meta-analysis of 13 randomized trials, which com-ared outcomes of DES and BMS in 7,352 randomizedatients, suggests that DES use significantly decreasesestenosis compared with BMS use in patients withTEMI. The DES use yielded a relative and absoluteeduction in TVR of 56% and �7.0%, respectively (p �.001). Treatment of 13 patients with a DES in the STEMIetting could prevent 1 restenosis event within the studiedime frame. The analysis also suggests that this benefit doesot come at the expense of increased death, reinfarction, ortent thrombosis within 2 years of the index PCI.fficacy of DES. The efficacy and safety of DES are largely
upported by the analysis of 18 registry studies, including6,521 patients with STEMI. Among the registries, thereas also a statistically significant reduction in TVR without
n increase in death, MI, or stent thrombosis. However, theagnitude of the reduction in TVR with DES was slightly
ess compared with that of the randomized trials; the RR inhe registries and randomized trials were 0.54 and 0.44,espectively. These differences likely reflect the use of DES
Figure 6 Publication Bias
Funnel plot with pseudo 95% confidence limits for assessment of publicationbias for mortality among (A) randomized controlled trials and (B) registry stud-ies. Open circles represent original studies. Solid circles represent hypotheti-cal or imputed studies. Open diamonds represent the pooled treatment effectsfrom the original studies. The solid diamonds and vertical lines represent thepooled treatment effects incorporating the imputed studies.
n a broader, more complex, and heterogeneous population r
ith STEMI in the registry studies, more reflective ofeal-world experiences. These differences may also be attrib-ted to selection bias and unknown or unmeasured con-ounders. The �7.0% absolute reduction in TVR with DESmong the randomized trials is slightly less compared toatients undergoing PCI for indications other thanTEMI. In the pivotal TAXUS-IV and SIRIUS (Study ofhe Sirolimus-Eluting Stent in De Novo Native Coronaryesions) trials, the absolute reduction in TVR was �8.3%nd �12.5%, respectively.
The reduction in the TVR rate with DES also appears toe related to the population baseline risk. In studies withigher baseline risk, measured as the TVR rate in the BMSroups, the magnitude of benefit was greater with DES. Inbivariate meta-analysis, as previously described, the ma-
ority of the variation in the treatment effects was explainedy the baseline risk or the TVR rate in the BMS groups.hese findings are consistent with those of prior reports ofreater magnitude of benefit with DES in patients at higherisk for restenosis (52–55).afety of DES. The benefit of DES against restenosishould be balanced against the risk of adverse events, stenthrombosis in particular. Stent thrombosis remains a seriousomplication, associated with increased morbidity and mor-ality (8,56). The use of DES in STEMI has been identifieds a predictor of stent thrombosis in some observationaltudies (7,57). However, in the present analysis, stenthrombosis does not appear to differ between DES andMS. The RR for stent thrombosis within 2 years ofrimary PCI in RCTs and registries was 0.97 and 0.94,espectively, nonsignificantly in favor of DES (p � 0.40).
For the patient with STEMI and treated emergently, itan be difficult to ascertain the likelihood of complianceith dual antiplatelet therapy, need for future surgicalrocedures, and prior bleeding complications. It is plausiblehat the clinical sequelae of noncompliance or prematureiscontinuation of dual antiplatelet therapy should manifests an increase in death, MI, and stent thrombosis, in theES group in particular (58,59). However, we did not
bserve an increase in any of these adverse events within 1r 2 years with DES across the RCTs and registries.urthermore, there was no difference in adverse eventsmong studies requiring �6 or �6 months of clopidogrelherapy. Accordingly, the results are consistent with othereports and meta-analysis of stent thrombosis in variedcute coronary syndrome settings (60).
Interestingly, there was a statistically significant decreasen mortality with use of DES in the registry studies at 1 yearhat was not apparent at 2 years. While the direction of theverall effect for mortality in the randomized trials alsoavored DES, it was not statistically significant at any timeoint. Although we used adjusted effect measures fromegistry studies when possible, residual confounding andelection bias could explain, in part, the lower mortalityssociated with DES. Moreover, the heterogeneity between
egistries for mortality and the visual asymmetry in the
ftas
cispepsaasirpfttSvmctFascalptawcothtmWtcS
DlcAtotsr
ArHrisa
C
IuBDiyt
RCMY
R
1
1
1
1
1687JACC Vol. 53, No. 18, 2009 Brar et al.May 5, 2009:1677–89 DES in AMI: Meta-Analysis
unnel plot suggesting publication bias could also explainhis potential benefit. In fact, after correction for thesymmetry in the funnel plot, there was no longer atatistically significant difference for death in the registries.
In the aggregate, the present data do not support theoncerns that use of DES in patients with STEMI mayncrease the risk of death or MI, driven in part by increasedtent thrombosis. Post-mortem studies, including those ofatients with stent thrombosis, have shown incompletendothelialization, persistent inflammation, and late mala-osition (61). While informative, these observations remainignificantly biased, given the select cohort from which theyre derived. The true incidence of these pathologic changesnd the frequency with which they lead to death, MI, ortent thrombosis remains unknown. In the absence of anncrease in adverse clinical events with DES across multipleandomized trials and registries, the incidence of theseathologic findings is likely to be low. Furthermore, theavorable clinical outcomes in the present analysis suggesthat many patients heal the stented segment and overcomehose initial pathologic disadvantages.tudy limitations. Some studies suggest that the risk ofery late stent thrombosis (�2 years from the index PCI)ay be slightly increased with the use of DES (62). The
urrent study does not address this issue adequately, givenhat only 2 studies had follow-up beyond 24 months.urthermore, data on clopidogrel adherence were unavail-ble. The random allocation of study subjects in the RCTshould have yielded, in theory, a similar incidence oflopidogrel noncompliance in both stent groups. However,mong the registries, the duration of clopidogrel therapyikely differed, with the DES group more likely treated withrolonged therapy. That could have contributed, in part, tohe improved 1-year mortality with DES in the registriesnd is consistent with a prior report on improved outcomesith prolonged clopidogrel therapy as recommended by the
urrent guidelines (58,63). Efforts directed at the educationf patients and other health care providers on the impor-ance of compliance with dual antiplatelet therapy shouldelp further improve outcomes (58,59). Meanwhile, percu-aneous therapy continues to rapidly evolve with improve-ents in stent platforms and adjunctive medical therapy.ith 5 years of planned follow-up, the HORIZONS-AMI
rial will provide valuable insight into the long-term out-omes of the paclitaxel-eluting stent in patients withTEMI (64).Although we observed that the reduction in TVR withES compared with BMS was related to underlying base-
ine risk, an association with study level covariates does notonclusively establish a relationship at the patient level.lso, the optimal method for relating baseline risk to
reatment effect remains controversial, and alternate meth-ds have been proposed (65,66). Nevertheless, using mul-iple methods, our results are in support of such a relation-hip, and are consistent with prior reports of higher rates of
estenosis in higher-risk cohorts (52,53).1
Lastly, this meta-analysis was performed at the study level.vailability of individual patient data could improve the
eliability of the findings and permit more flexible analyses.owever, a major limitation of individual patient data analyses
emains the inability to obtain patient-level data from allnvestigators, unpublished studies in particular. Therefore, theelective inclusion of studies in individual patient data meta-nalysis can introduce publication and other biases.
onclusions
n this meta-analysis of 33,873 patients with STEMI, these of DES appears safe and efficacious compared withMS across randomized trials and registries. The use ofES significantly decreased restenosis without an increase
n the incidence of death, MI, or stent thrombosis within 2ears of the index PCI. Longer-term follow-up is necessaryo determine the durability of these observations.
eprint requests and correspondence: Dr. Somjot S. Brar,enter for Interventional Vascular Therapy, Columbia Universityedical Center, 161 Fort Washington Avenue, 5th Floor, New
ork, New York 10032. E-mail: [email protected].
EFERENCES
1. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravas-cular stents to prevent occlusion and restenosis after transluminalangioplasty. N Engl J Med 1987;316:701–6.
2. Fischman DL, Leon MB, Baim DS, et al. A randomized comparisonof coronary-stent placement and balloon angioplasty in the treatmentof coronary artery disease. Stent Restenosis Study Investigators.N Engl J Med 1994;331:496–501.
3. Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versusstandard stents in patients with stenosis in a native coronary artery.N Engl J Med 2003;349:1315–23.
4. Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med2004;350:221–31.
5. Lagerqvist B, James SK, Stenestrand U, Lindback J, Nilsson T,Wallentin L. Long-term outcomes with drug-eluting stents versusbare-metal stents in Sweden. N Engl J Med 2007;356:1009–19.
6. Shuchman M. Trading restenosis for thrombosis? New questionsabout drug-eluting stents. N Engl J Med 2006;355:1949–52.
7. Sianos G, Papafaklis MI, Daemen J, et al. Angiographic stentthrombosis after routine use of drug-eluting stents in ST-segmentelevation myocardial infarction: the importance of thrombus burden.J Am Coll Cardiol 2007;50:573–83.
8. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, andoutcome of thrombosis after successful implantation of drug-elutingstents. JAMA 2005;293:2126–30.
9. De Luca G, Stone GW, Suryapranata H, et al. Efficacy and safety ofdrug-eluting stents in ST-segment elevation myocardial infarction: ameta-analysis of randomized trials. Int J Cardiol 2008;133:213–22.
0. Kastrati A, Dibra A, Spaulding C, et al. Meta-analysis of randomizedtrials on drug-eluting stents vs. bare-metal stents in patients with acutemyocardial infarction. Eur Heart J 2007;28:2706–13.
1. Pasceri V, Patti G, Speciale G, Pristipino C, Richichi G, DiSciascio G. Meta-analysis of clinical trials on use of drug-elutingstents for treatment of acute myocardial infarction. Am Heart J2007;153:749 –54.
2. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials 1986;7:177–88.
3. Van Houwelingen HC, Zwinderman KH, Stijnen T. A bivariateapproach to meta-analysis. Stat Med 1993;12:2273–84.
4. Bland JM, Altman DG. Regression towards the mean. BMJ 1994;308:1499.

1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
1688 Brar et al. JACC Vol. 53, No. 18, 2009DES in AMI: Meta-Analysis May 5, 2009:1677–89
5. Sharp SJ, Thompson SG, Altman DG. The relation between treat-ment benefit and underlying risk in meta-analysis. BMJ 1996;313:735–8.
6. Begg CB, Mazumdar M. Operating characteristics of a rank correla-tion test for publication bias. Biometrics 1994;50:1088–101.
7. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34.
8. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based methodof testing and adjusting for publication bias in meta-analysis. Biomet-rics 2000;56:455–63.
9. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.Improving the quality of reports of meta-analyses of randomisedcontrolled trials: the QUOROM statement. Quality of Reporting ofMeta-analyses. Lancet 1999;354:1896–900.
0. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observa-tional studies in epidemiology: a proposal for reporting. Meta-analysisOf Observational Studies in Epidemiology (MOOSE) group. JAMA2000;283:2008–12.
1. Di Lorenzo E, Varricchio A, Lanzillo T, et al. Paclitaxel and sirolimusimplantation in patients with acute myocardial infarction (abstr).Circulation 2005;112:U538.
2. Helsinki Area Acute Myocardial Infarction Treatment Re-Evaluation—Should the Patients Get a Drug-Eluting or Normal Stent (HAAMU-STENT). Available at: http://www.cardiosource.com/clinicaltrials/trial.asp?trialID � 1492. Accessed May 30, 2008.
3. Spaulding C, Henry P, Teiger E, et al. Sirolimus-eluting versusuncoated stents in acute myocardial infarction. N Engl J Med2006;355:1093–104.
4. Laarman GJ, Suttorp MJ, Dirksen MT, et al. Paclitaxel-eluting versusuncoated stents in primary percutaneous coronary intervention.N Engl J Med 2006;355:1105–13.
5. Menichelli M, Parma A, Pucci E, et al. Randomized trial of Sirolimus-Eluting Stent Versus Bare-Metal Stent in Acute Myocardial Infarction(SESAMI). J Am Coll Cardiol 2007;49:1924–30.
6. Chechi T, Vittori G, Biondi Zoccai GG, et al. Single-CenterRandomized Evaluation of Paclitaxel-Eluting Versus ConventionalStent in Acute Myocardial Infarction (SELECTION). J Interv Car-diol 2007;20:282–91.
7. Valgimigli M, Percoco G, Malagutti P, et al. Tirofiban andsirolimus-eluting stent vs abciximab and bare-metal stent for acutemyocardial infarction: a randomized trial. JAMA 2005;293:2109 –17.
8. Valgimigli M, Campo G, Percoco G, et al. Comparison ofangioplasty with infusion of tirofiban or abciximab and withimplantation of sirolimus-eluting or uncoated stents for acutemyocardial infarction: the MULTISTRATEGY randomized trial.JAMA 2008;299:1788–99.
9. Kelbaek H, Thuesen L, Helqvist S, et al. Drug-eluting versus baremetal stents in patients with ST-segment elevation myocardial infarc-tion: eight-month follow-up in the Drug Elution and Distal Protec-tion in Acute Myocardial Infarction (DEDICATION) trial. Circula-tion 2008;118:1155–62.
0. A Prospective Randomized Controlled Trial to Evaluate the Efficacyof Drug-Eluting Stents Versus Bare-Metal Stents for the Treatmentof Acute Myocardial Infarction (MISSION) Trial. Available at:http://www.cardiosource.com/clinicaltrials/trial.asp?trialID�1517.Accessed May 30, 2008.
1. Harmonizing Outcomes With Revascularization and Stents in AcuteMyocardial Infarction (HORIZONS-AMI Stent). Available at:http://www.cardiosource.com/clinicaltrials/trial.asp?trialID�1754.Accessed October 15, 2008.
2. Pittl U, Kaiser C, Brunner-La Rocca HP, et al. Safety and efficacy ofdrug eluting stents versus bare metal stents in the primary angioplastyof patients with acute ST-elevation myocardial infarction: a prospec-tive randomized study. Eur Heart J 2006;27:650.
3. Diaz de la Llera LS, Ballesteros S, Nevado J, et al. Sirolimus-elutingstents compared with standard stents in the treatment of patients withprimary angioplasty. Am Heart J 2007;154:164.
4. Kukreja N, Onuma Y, Garcia-Garcia H, Daemen J, van Domburg R,Serruys PW. Primary percutaneous coronary intervention for acutemyocardial infarction: long-term outcome after bare metal and drug-eluting stent implantation. Circ Cardiovasc Intervent 2008;1:103–10.
5. Vagaonescu TD, Moreyra AE, Wilson AC, Cosgrove NM, Kostis JB.
Long-term mortality in ST-T segment and non ST-T segmentmyocardial infarction after drug-eluting stents and bare metal stentsimplantation in New Jersey: the MIDAS registry. Presented at:Transcatheter Cardiovascular Therapeutics, Washington, DC:October 20–25, 2007.
6. Bose R, Gupta G, Grayburn PA, Laible EA, Kang MJ, Choi JW.Safety of drug-eluting stents in the coronary artery in ST-elevationmyocardial infarction at a single high-volume medical center. Am JCardiol 2007;100:949–52.
7. Cheneau E, Rha S, Kuchulakanti P, et al. Impact of sirolimus-eluting stents on outcomes of patients treated for acute myocardialinfarction by primary angioplasty. Cathet Cardiovasc Intervent2005;65:469 –72.
8. Kupferwasser LI, Amorn A, Kapoor N, et al. Comparison of drug-eluting stents with bare metal stents in unselected patients with acutemyocardial infarction. Cathet Cardiovasc Intervent 2007;70:1–8.
9. Mauri L, Silbaugh TS, Garg P, et al. Drug-eluting or bare-metal stentsfor acute myocardial infarction. N Engl J Med 2008;359:1330–42.
0. Newell MC, Henry CR, Sigakis CJ, et al. Comparison of safety andefficacy of sirolimus-eluting stents versus bare metal stents in patientswith ST-segment elevation myocardial infarction. Am J Cardiol2006;97:1299–302.
1. Percoco G, Manari A, Guastaroba P, et al. Safety and long-termefficacy of sirolimus eluting stent in ST-elevation acute myocardialinfarction: the REAL (Registro REgionale AngiopLastiche Emilia-Romagna) registry. Cardiovasc Drugs Therapy 2006;20:63–8.
2. Romano M, Buffoli F, Tomasi L, Corrado L, Ferrari M, Zanini R.Safety and effectiveness of drug eluting stent in patients with STelevation myocardial infarction undergoing primary angioplasty.Cathet Cardiovasc Intervent 2008;71:759–63.
3. Slottow TL, Steinberg DH, Roy P, et al. Drug-eluting stents areassociated with similar cardiovascular outcomes when compared withbare metal stents in the setting of acute myocardial infarction.Cardiovasc Revasc Med 2008;9:24–8.
4. Vlaar P, Rihal C, Singh M, et al. Safety and efficacy of drug-elutingstent for ST-segment elevation myocardial infarction in an unselectedconsecutive cohort. Cathet Cardiovasc Intervent 2008;71:764–9.
5. Hannan E, Racz M, Walford G, et al. Drug-eluting versus bare-metalstents in the treatment of patients with ST-segment elevation myo-cardial infarction. J Am Coll Cardiol Intv 2008;1:129–35.
6. Shishehbor M, Amini R, Oliveria L, et al. Comparison of drug-elutingstents versus bare-metal stents for treating ST-segment elevationmyocardial infarction. J Am Coll Cardiol Intv 2008;1:227–32.
7. Jensen LO, Maeng M, Thayssen P, et al. Two-year clinical outcomefollowing primary precutaneous coronary intervention with drug-eluting and bare metal stent in patients with ST-segment elevationmyocardial infarction. Presented at: Transcatheter CardiovascularTherapeutics, Washington, DC: October 12–17, 2008.
8. Brodie BR, Stuckey T, Downey W, et al. Outcomes with drug-eluting stents versus bare metal stents in acute ST-elevationmyocardial infarction: results from the Strategic TranscatheterEvaluation of New Therapies (STENT) Group. Cathet CardiovascInterv 2008;72:893–900.
9. Lemos PA, Saia F, Hofma SH, et al. Short- and long-term clinicalbenefit of sirolimus-eluting stents compared with conventional barestents for patients with acute myocardial infarction. J Am Coll Cardiol2004;43:704–8.
0. Nakamura S, Bae J, Cahyadi YH, Udayachalerm W, Tresukosol D,Tansuphaswadikul S. Three-year follow-up of patients with ST-segment evelation acute myocardial infarction treated with sirolimus-eluting stent and paclitaxel-eluting stent: multicenter registry in Asia(abstr). Am J Cardiol 2006;98:76M.
1. Steg PG. Increased all-cause mortality at 2 year follow-up after PCIwith drug-eluting stents vs bare metal stents in acute coronarysyndromes: the GRACE registry experience. Presented at: EuropeanSociety of Cardiology, September 4, 2007: Vienna, Austria.
2. Garg P, Normand SL, Silbaugh TS, et al. Drug-eluting orbare-metal stenting in patients with diabetes mellitus: results fromthe Massachusetts Data Analysis Center Registry. Circulation2008;118:2277– 85.
3. Azzarelli S, Amico F, Galassi AR, Giacoppo M, Argentino V, FiscellaA. Two-year clinical follow up of coronary drug-eluting stent inpatients at high risk for coronary restenosis. J Invas Cardiol 2008;20:
62–6.
5
5
5
5
5
5
6
6
6
6
6
6
6
Ka
F
1689JACC Vol. 53, No. 18, 2009 Brar et al.May 5, 2009:1677–89 DES in AMI: Meta-Analysis
4. Sabate M, Jimenez-Quevedo P, Angiolillo DJ, et al. Randomizedcomparison of sirolimus-eluting stent versus standard stent for percu-taneous coronary revascularization in diabetic patients: the Diabetesand Sirolimus-Eluting Stent (DIABETES) trial. Circulation 2005;112:2175–83.
5. Kirtane AJ, Ellis SG, Dawkins KD, et al. Paclitaxel-eluting coronarystents in patients with diabetes mellitus: pooled analysis from 5randomized trials. J Am Coll Cardiol 2008;51:708–15.
6. Chechi T, Vecchio S, Vittori G, et al. ST-segment elevation myocar-dial infarction due to early and late stent thrombosis a new group ofhigh-risk patients. J Am Coll Cardiol 2008;51:2396–402.
7. de la Torre-Hernandez JM, Alfonso F, Hernandez F, et al. Drug-eluting stent thrombosis: results from the multicenter Spanish registryESTROFA (Estudio ESpanol sobre TROmbosis de stents FArmaco-activos). J Am Coll Cardiol 2008;51:986–90.
8. Brar SS, Kim J, Brar SK, et al. Long-term outcomes by clopidogrelduration and stent type in a diabetic population with de novo coronaryartery lesions. J Am Coll Cardiol 2008;51:2220–7.
9. Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, andoutcomes of premature discontinuation of thienopyridine therapy afterdrug-eluting stent placement: results from the PREMIER registry.Circulation 2006;113:2803–9.
0. Moreno R, Fernandez C, Hernandez R, et al. Drug-eluting stentthrombosis: results from a pooled analysis including 10 randomizedstudies. J Am Coll Cardiol 2005;45:954–9.
1. Nakazawa G, Finn AV, Joner M, et al. Delayed arterial healing andincreased late stent thrombosis at culprit sites after drug-eluting stentplacement for acute myocardial infarction patients: an autopsy study.
Circulation 2008;118:1138–45. p2. Wenaweser P, Daemen J, Zwahlen M, et al. Incidence and correlatesof drug-eluting stent thrombosis in routine clinical practice. 4-yearresults from a large 2-institutional cohort study. J Am Coll Cardiol2008;52:1134–40.
3. King SB III, Smith SC Jr., Hirshfeld JW Jr., et al. 2007 focused updateof the ACC/AHA/SCAI 2005 guideline update for percutaneouscoronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J AmColl Cardiol 2008;51:172–209.
4. Mehran R, Brodie B, Cox DA, et al. The Harmonizing Outcomeswith RevasculariZatiON and Stents in Acute Myocardial Infarction(HORIZONS-AMI) trial: study design and rationale. Am Heart J2008;156:44–56.
5. Thompson SG, Smith TC, Sharp SJ. Investigating underlying riskas a source of heterogeneity in meta-analysis. Stat Med 1997;16:2741–58.
6. McIntosh MW. The population risk as an explanatory variable inresearch synthesis of clinical trials. Stat Med 1996;15:1713–28.
ey Words: stent y drug-eluting y myocardial infarction y meta-nalysis y systematic review y meta-regression.
APPENDIX
or a table on the end points analyzed by trial,
lease see the online version of this article.