Drug-Eluting Stents in Angina - Home - Dialogues in ... · drug-eluting stents: a cause for...
61
233 Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008 Guest Editor - Eugene Braunwald, MD Guest Editorial Percutaneous coronary intervention: a contemporary assessment - E. Braunwald 235 Lead Article Drug-eluting coronary stents: stents and stent-ability - W. Wijns, M. Valgimigli 239 Expert Answers to Three Key Questions Medical therapy, surgery, or PCI: does (or should) the availability of drug-eluting stents influence the decision? - A. A. J. Adgey, B. M Glover, S. J. Walsh 255 Antiplatelet therapy: what to do if the patient with a drug-eluting stent needs elective noncardiac surgery? - M. Pfisterer, M. J. Zellweger, M. Filipovic, F. Nietlispach 262 What are the regulatory and economic challenges posed by drug-eluting stents? B. R. Shah, K. A. Schulman 267 Fascinoma Cardiologica Matters @ Heart: Dr Patterson and his missing gene - R. J. Bing 273 Summaries of Ten Seminal Papers - M. Valgimigli 277 Drug-Eluting Stents in Angina One-year outcomes of coronary artery bypass graft surgery versus percutaneous coronary intervention with multiple stenting for multisystem disease: a meta-analysis of individual patient data from randomised clinical trials – N. Mercado and others Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis – C. Stettler and others Clinical end points in coronary stent trials: a case for stan- dardized definitions – D. E. Cutlip and others Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern – E. Camenzind and others Are drug-eluting stents associated with a higher rate of late thrombosis than bare metal stents? Late stent thrombosis: a nuisance in both bare metal and drug-eluting stents P. W. Serruys and J. Daemen Drug-eluting stent update 2007: Part I. A survey of current and future generation drug-eluting stents: meaningful advances or more of the same? Part II: Unsettled issues – J. Daemen and P. W. Serruys Cyphering the complexity of coronary artery disease using the syntax score to predict clinical outcome in patients with three- vessel lumen obstruction undergoing percutaneous coronary intervention – M. Valgimigli and others Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study – J. Daemen and others Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization – A. V. Finn and others Balancing the risks of restenosis and stent thrombosis in bare- metal versus drug-eluting stents. Results of a decision analytic model – P. Garg and others Bibliography of One Hundred Key Papers 289
Transcript of Drug-Eluting Stents in Angina - Home - Dialogues in ... · drug-eluting stents: a cause for...

233
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Guest Editor - Eugene Braunwald, MD
Guest Editorial Percutaneous coronary intervention: a contemporary assessment - E. Braunwald 235
Lead Article Drug-eluting coronary stents: stents and stent-ability - W. Wijns, M. Valgimigli 239
Expert Answers to Three Key Questions Medical therapy, surgery, or PCI: does (or should) the availability of drug-eluting stents influence the decision? - A. A. J. Adgey, B. M Glover, S. J. Walsh 255Antiplatelet therapy: what to do if the patient with a drug-eluting stent needs elective noncardiac surgery? - M. Pfisterer, M. J. Zellweger, M. Filipovic, F. Nietlispach 262What are the regulatory and economic challenges posed by drug-eluting stents?B. R. Shah, K. A. Schulman 267
Fascinoma Cardiologica Matters @ Heart: Dr Patterson and his missing gene - R. J. Bing 273
Summaries of Ten Seminal Papers - M. Valgimigli 277
Drug-Eluting Stents in Angina
One-year outcomes of coronary artery bypass graft surgeryversus percutaneous coronary intervention with multiple stentingfor multisystem disease: a meta-analysis of individual patientdata from randomised clinical trials – N. Mercado and others
Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis – C. Stettler and others
Clinical end points in coronary stent trials: a case for stan-dardized definitions – D. E. Cutlip and others
Stent thrombosis late after implantation of first-generationdrug-eluting stents: a cause for concern – E. Camenzind and others
Are drug-eluting stents associated with a higher rate of latethrombosis than bare metal stents? Late stent thrombosis: a nuisance in both bare metal and drug-eluting stents P. W. Serruys and J. Daemen
Drug-eluting stent update 2007: Part I. A survey of current andfuture generation drug-eluting stents: meaningful advances ormore of the same? Part II: Unsettled issues – J. Daemen and
P. W. Serruys
Cyphering the complexity of coronary artery disease using thesyntax score to predict clinical outcome in patients with three-vessel lumen obstruction undergoing percutaneous coronaryintervention – M. Valgimigli and others
Early and late coronary stent thrombosis of sirolimus-elutingand paclitaxel-eluting stents in routine clinical practice: datafrom a large two-institutional cohort study – J. Daemen and others
Pathological correlates of late drug-eluting stent thrombosis: strutcoverage as a marker of endothelialization – A. V. Finn and others
Balancing the risks of restenosis and stent thrombosis in bare-metal versus drug-eluting stents. Results of a decision analyticmodel – P. Garg and others
Bibliography of One Hundred Key Papers 289

234
Avkiran M, PhD Cardiovascular Research The Rayne InstituteSt Thomas’ HospitalLondon, UK
Bassand JP, MDDept of CardiologyUniversity Hospital Jean MinjozBesançon, France
Bertrand ME, MDHôpital CardiologiqueLille, France
Bolli R, MDDivision of CardiologyUniversity of LouisvilleLouisville, KY, USA
Camm JA, MDDept of Cardiac and Vascular SciencesSt George’s University of LondonLondon, UK
Coats A, MDFaculty of MedicineUniversity of SydneySydney, Australia
Cobbe SM, MDDept of Medical CardiologyGlasgow Royal InfirmaryGlasgow, UK
Cohn JN, MDRasmussen Center for Cardiovascular Disease PreventionMinneapolis, MN, USA
Cokkinos DV, MD1st Cardiology DeptOnassis Cardiac Surgery CenterAthens, Greece
Cowie M, MD, PhDDept of Clinical CardiologyNational Heart & Lung InstituteLondon, UK
Danchin N, MDDept of CardiologyHôpital Européen Georges PompidouParis, France
Dargie HJ, MDCardiac ResearchWestern InfirmaryGlasgow, UK
Di Pasquale G, MDDpt of CardiologyMaggiore HospitalBologna, Italy
Dzau VJ, MDDuke University Medical Center & Health System DUMCDurham, NC, USA
Consulting Editors
Editors in ChiefFerrari R, MD, PhDDept of Cardiology, Arcispedale S. AnnaUniversity of Ferrara, Ferrara, Italy
Hearse DJ, BSc, PhDThe Cardiothoracic Centre, The Rayne InstituteSt Thomas’ Hospital, London, UK
Fernandez-Aviles F, MDInstitute of Hematology and Oncology, IDIBAPSHospital University Clinic of Barcelona Barcelona, Spain
Fox KM, MDDept of CardiologyRoyal Brompton HospitalLondon, UK
Fox KA, MDDept of Cardiological ResearchUniversity of EdinburghEdinburgh, UK
Fuster V, MD, PhDCardiovascular InstituteMount Sinai Medical CenterNew York, NY, USA
Hasenfuss G, MDDept of CardiologyGeorg-August UniversitätGöttingen, Germany
Hori M, MD, PhDDept of Internal Medicine and TherapeuticsOsaka University Graduate School of MedicineOsaka, Japan
Katz AM, MDUniversity of Connecticut School of MedicineFarmington, CT, USA
Komajda M, MDDept of CadiologyCHU Pitié-SalpêtrièreParis, France
Komuro I, MD, PhDDept of Cardiovascular Sciences & MedicineChiba University Graduate School of MedicineChiba, Japan
Lakatta EG, MDNational Institute on AgingGerontology Research CenterBaltimore, MD, USA
Libby P, MDCardiovascular MedicineBrigham & Women’s HospitalBoston, MA, USA
Lonn E, MDHamilton Health Sciences General SiteHamilton, Ontario, Canada
Lopez-Sendon JL, MDCCU Dept of CardiologyHospital University Gregorio MaranonMadrid, Spain
Maggioni AP, MDANMC Research CenterFirenze, Italy
Marber MS, MD, PhDCardiovascular Research The Rayne Institute St Thomas’ HospitalLondon, UK
Oto A, MDMedical Office, Hacettepe University School of MedicineAnkara, Turkey
Patrono C, MDDept of PharmacologyUniversity La SapienzaRome, Italy
Pepine CJ, MDDept of MedicineUniversity of FloridaGainesville, FL, USA
Rapezzi C, MDInstitute of CardiologyUniversity of BolognaBologna, Italy
Remme WJ, MD, PhDSticares FoundationRotterdam, The Netherlands
Rosen MR, MDDept of Pharmacology &PediatricsColumbia University College of Physicians & SurgeonsNew York, NY, USA
Ruzyllo W, MDNational Institute of CardiologyWarsaw, Poland
Ryden L, MD, PhDDept of CardiologyKarolinska University Hospital SolnaStockholm, Sweden
Schneider MD, MDBaylor College of MedicineHouston, TX, USA
Seabra-Gomes RJ, MDInstituto do CoracaoHospital Santa CruzCarnaxide, Portugal
Sechtem U, MDDept of Internal Medicine & CardiologyRobert Bosch KrankenhausStuttgart, Germany
Simoons ML, MDThoraxcenterErasmus University Medical CenterRotterdam, The Netherlands
Sleight P, MDDept of Cardiovascular MedicineJohn Radcliffe HospitalOxford, UK
Soler-Soler J, MD Dept of CardiologyHospital General Vall d’HebronBarcelona, Spain
Steg PG, MDDept of CardiologyHôpital Bichat–Claude BernardParis, France
Swedberg K, MD, PhDDept of MedicineSahlgrenska University Hospital OstraGöteborg, Sweden
Tardif JC, MDMontreal Heart InstituteMontreal, Quebec, Canada
Tavazzi L, MDDivision of CardiologyPoliclinico San Matteo IRCCSPavia, Italy
Tendera M, MD3rd Division of CardiologySilesian School of MedicineKatowice, Poland
Vanhoutte PM, MDDept of PharmacologyUniversity of Hong Kong Faculty of MedicineHong Kong, China
Widimsky P, MD, PhDVinohrady CardiocenterCharles University HospitalPrague, Czech Republic
Wijns WC, MDCardiovascular Center AalstOLV Hospital, Aalst, Belgium
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008

Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
235
Eugene Braunwald, MDTIMI Study Group - Cardiovascular Division - Brigham and Women’s Hospital - and
the Department of Medicine - Harvard Medical School - Boston, Mass - USA
t has been known for more than three centuries that chronic stable angina pectoris
is most commonly caused by narrowing of one or more epicardial arteries.
Andreas Grüntzig’s brilliant development of percutaneous transluminal coronary
angioplasty (PTCA) in 1977 to relieve coronary obstruction was the first and most
important step in the development of modern percutaneous coronary intervention
(PCI), and represents one of the triumphs of twentieth-century medicine. Coronary
revascularization by PTCA soon became a widely used and effective approach for the
treatment of angina. When compared with coronary artery bypass surgery (CABG), PCI
proved to be equally efficacious in the majority of patients. To the chagrin of cardiac
surgeons, an increasing fraction of patients with disabling chronic stable angina se-
lected PCI over surgery because it causes little discomfort and requires only a brief
hospitalization and convalescence. Furthermore, it does not exclude subsequent sur-
gery, should it be necessary.
As a result of the development of PCI, an important new specialty, interventional car-
diology, developed and interventional cardiologists quickly became the “darlings” of
both the profession and the public. In the early 1980s in North America and to a lesser
extent in Western Europe, coronary angiography and PCI were carried out in patients
with progressively less disabling angina. The “oculostenotic reflex” soon became wide-
spread, viz, if a stenosis on the coronary arteriogram was visualized, then its immediate
relief by PCI would be carried out almost reflexly by the interventional cardiologist.
However, three problems with PTCA soon emerged. The first was the development of
restenosis caused by neointimal hyperplasia of fibromuscular tissue in the dilated
coronary artery. This occurred in 35% to 40% of patients, requiring one and in some
instances multiple repeat procedures. The second problem, fortunately much less
Guest Editorial
PERCUTANEOUS CORONARY INTERVENTION: A CONTEMPORARY ASSESSMENT
I
•••
Eugene Braunwald, MD, Chairman, TIMI Study Group, 350 Longwood Avenue, 1st office floor, Boston, MA 02115, USA (e-mail: [email protected])

frequent, was the development of acute coronary occlusion secondary to procedurally
induced coronary arterial dissection and/or thrombosis of the coronary artery. This
serious complication, if not corrected immediately, would lead to acute myocardial
infarction or death, and required emergency CABG. PTCA required the “standby” of an
operating room and cardiac surgical team—obviously an expensive and inconvenient
requirement. The third problem was the growing realization that coronary atherosclerosis
is usually a multifocal, not a unifocal disease; a focal stenosis visualized angiographically
was just the tip of the iceberg. Therefore, relieving these obstructions in patients with
chronic angina, while greatly reducing or even abolishing symptoms, did not seem to
alter the natural history of the disease.
The development, in 1986, of metal stents, at first bare-metal stents (BMS), inserted
into the coronary artery following balloon angioplasty, was the second of the three
major advances of PCI, since it essentially eliminated procedural coronary occlusions.
Although BMS reduced coronary restenosis by one third, to about 20% to 25%, this
remained a stubborn residual problem that did not yield to a large number of pharma-
cologic approaches that were explored. BMS also brought with them an uncommon,
but often devastating, early complication—platelet-driven stent thrombosis. To avoid
this, dual antiplatelet therapy, ie, aspirin and a thienopyridine, first ticlopidine and
more recently clopidogrel, was required. This treatment was associated with its own
risk—bleeding that was spontaneous or which accompanied cardiac (or other) surgery.
The development of drug-eluting stents (DES) in 2001 represents the third important
advance of PCI. DES are coated by a carrier polymer and anti-inflammatory antiprolifer-
ative agents and have been successful in reducing restenosis substantially, to between
5% and 10%. DES have not eliminated the early stent thrombosis with its attendant high
risk that was noted with BMS. Indeed, it appears that late stent thrombosis, ie, between
30 days and 1 year, and very late stent thrombosis (after 1 year), may actually be more
frequent with DES than with BMS. Such late thromboses may occur because the anti-
proliferative activity of the coating, which reduces the risk of restenosis, also inhibits
reendothelialization, leaving the stent as a nidus for platelet aggregation. This compli-
cation may occur despite prolonged dual antiplatelet therapy, although patients who
develop stent thrombosis despite such therapy often exhibit hyporesponsiveness to
one or both of the antiplatelet drugs.
Moreover, patients with DES who discontinue dual antiplatelet therapy prematurely are
at especially high risk of stent thrombosis, which, like coronary occlusion after PTCA,
is associated with a very high incidence of mortality or massive nonfatal myocardial
infarction. Long-term compliance with dual antiplatelet therapy is problematic and the
need to interrupt it because of the occurrence of serious bleeding or because of refusal
of payers to continue long-term reimbursement for thienopyridines may become re-
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Guest Editorial - Braunwald
236
•••

sponsible for a growing number of DES thromboses in the future. The duration of dual
antiplatelet therapy required to minimize the risk of DES thrombosis has not yet been
determined, but probably exceeds 1 year. In addition, DES may also cause local hyper-
sensitivity reactions.
Where do we go from here? First, a rededication to meticulous deployment regardless
of the composition or configuration of the stent is necessary. Second, continued research
on DES should be strongly encouraged. New stents must steer a course between the
Scylla of inadequate reendothelialization and the Charybdis of excessive neointimal
hyperplasia. Ultimately, fully resorbable DES are likely to become standard. Formal
prospective registries to ascertain long-term outcomes of patients with newly approved
stents are essential to ensure maximum patient safety.
Second, a new look at the platelet P2Y12 component of dual antiplatelet therapy is in-
dicated. Detection of hyporesponsiveness to clopidogrel and/or aspirin with a number
of portable devices is now possible. In the not inconsiderable number of patients who
exhibit hyporesponsiveness, the doses of these drugs could be increased. Prasugrel, a
novel thienopyridine, has been shown to reduce both early and late stent thrombosis
by half, albeit at the cost of an increased risk of bleeding. This drug is now wending its
way through the regulatory process. Very potent nonthienopyridine P2Y12 blockers are
also under active investigation.
Finally, and perhaps most importantly, a reconsideration of the indications for PCI is
in order. While this procedure successfully eliminates or reduces the severity of stable
angina pectoris, PCI has never been demonstrated to improve survival or reduce the
incidence of acute myocardial infarction in these patients. Intensive medical manage-
ment of angina has improved considerably since the introduction of PCI in the 1970s,
and a trial of such therapy should be attempted before allowing the “oculostenotic
reflex” to prevail. A medical strategy could be even more important when patients with
asymptomatic or mildly symptomatic coronary obstruction are identified in increasing
numbers as multislice computed tomographic coronary angiography becomes more
widespread. Of course, if optimum medical therapy fails in a patient with severe angina,
mechanical reperfusion is required; the specific method—PCI or CABG—depends on
the coronary anatomy and left ventricular function.
The situation differs in patients with acute coronary syndromes. PCI, if carried out
without delay after the onset of symptoms in patients with ST-segment–elevation my-
ocardial infarction (STEMI) has been shown to be life saving and is now the treatment
of choice for patients with this condition. When the thrombosis occurs in a large proxi-
mal coronary artery, as is often the case, late lumen loss and restenosis may be of less
concern than when it occurs in a smaller coronary artery. Since PCI must be carried
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Guest Editorial - Braunwald
237
•••

out immediately on presentation of patients with acute STEMI, it is often difficult in the
very few minutes available to ascertain if the patient is likely to adhere to dual anti-
platelet therapy for a prolonged period. Thus, DES may not be the stents of choice in
these patients. In patients with unstable angina and non-ST-segment–elevation myo-
cardial infarction, the need for PCI is also clear, since the composite end point of death
or myocardial infarction is reduced by this procedure; DES may be quite useful in
patients with this condition.
A number of dazzling advances in cardiovascular therapeutics have occurred during the
last half century. However, none of these have been free of problems, either limitations
of efficacy and/or the development of adverse effects. All have required continuous
reassessment. PCI certainly stands tall among these advances. This issue of Dialoguesin Cardiovascular Medicine provides a thoughtful, contemporary assessment of this
important therapy.
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Guest Editorial - Braunwald
238
•••

239
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-abilityWilliam Wijns*, MD, PhD, FESC; Marco Valgimigli †, MD*Cardiovascular Center Aalst - Aalst - BELGIUM †Cardiovascular Institute - Arcispedale S. Anna - University of Ferrara - Ferrara - ITALY
Stents are endoprosthetic scaffolding devices designedto enlarge the vessel lumen, seal dissections and cre-ate a rounder, smoother channel. Their advent hassignificantly advanced the field of interventionalcardiology. Yet, metallic stents are associated withintima proliferation, causing in-stent restenosis andsubsequent need for reintervention in a substantialnumber of patients. Considerable efforts have goneinto the development of stents covered by an activecoating designed to inhibit in-stent restenosis—thedrug-eluting stent (DES). They proved to be highlyefficacious in reducing reintervention rates, but byinhibiting stent-driven intima hyperplasia, they alsodelay vascular healing after the procedure, whichexposes treated patients to the need for prolongeddual antiplatelet treatment and to the risk of delayedabrupt stent closure. Moreover, the synthetic nonbio-erodable polymer containing the drug may be an im-portant trigger of local vascular inflammation, whichmay ultimately contribute to long-term vulnerabilityof the implanted stent. Second-generation DES engi-neered with more biocompatible or even reabsorbablepolymers are being developed, which hopefully willmake DES equally safe as well as more efficaciousthan currently available bare metal stents.
HISTORICAL PERSPECTIVES
More than 30 years have passed since the beginning of clinical interventional cardiol-ogy on the occasion of the first angioplastyprocedure performed by Andreas Grüntzig
on September 16, 1977. With the launch of a new eraof device-based therapies, his legacy has translatedinto several new chapters in the history of medicine,pushing every other discipline, not just cardiovascularcare, toward less invasive forms of treatment (Figure 1,page 240).
The first patient to undergo transluminal balloon di-latation was 38 years old (the same age as Grüntzig)and had a discrete lesion in the proximal anterior descending coronary artery and disabling angina.Bernhard Meier, who as a resident in Zurich was takingcare of the patient at the time, recounts that eventhough Grüntzig told the patient that he was the firstto undergo the procedure, the patient was enthusiasticto have an alternative to bypass surgery. With all thesenior staff of the hospital in attendance, Grüntzig per-formed the procedure, and recalled1:
Keywords: coronary artery disease; interventional cardiology; angioplasty;stent; bare-metal stent; drug-eluting stentAddress for correspondence: William Wijns, MD, PhD, CardiovascularCenter Aalst, OLV Ziekenhuis, Moorselbaan 164, 9300 Aalst, Belgium(http://cardio-aalst.be; e-mail: [email protected])Dialogues Cardiovasc Med. 2008;13:239-252
Copyright © 2008 LLS SAS. All rights reserved www.dialogues-cvm.org
SELECTED ABBREVIATIONS AND ACRONYMS
BENESTENT BElgian NEtherlands STENT [trial]
BMS bare-metal stent
DES drug-eluting stent
FIM First-in-Man [trial]
MACE major adverse cardiac event
PCI percutaneous coronary intervention
SIRIUS SIRolImUS-eluting stent in de novo native coronary lesions [trial]
STRESS STress REStenosis Study

The catheter wedged the stenosis so that there was no
antegrade flow and the distal coronary pressure was very
low. To the surprise of all of us, no ST elevation, ventricular
fibrillation or even extrasystole occurred and the patient
had no chest pain. At this moment I decided not to start
the coronary perfusion with the roller pump. After the
first balloon deflation, the distal coronary pressure rose
nicely. Encouraged by the positive response, I inflated the
balloon a second time to relieve the residual gradient.
Everyone was surprised about the ease of the procedure
and I started to realize that my dreams had come true.
This patient remained free of angina, and when heunderwent repeat catheterization on September 16,1987, the anterior descending coronary artery waswidely patent. Ten years later, he remained asympto-matic and in September 1997, he performed a maxi-mal bicycle ergometric test with normal results.
In the early days of angioplasty, the guide catheterswere made of Teflon and were extremely stiff. The bal-loon catheters were of a double-lumen design with aclosed end and a short, nonmovable, and barely steer-able guidewire attached directly at the tip of the bal-loon. The catheters were high profile, and recrossingthe plaque after dilatation attempts was consideredextremely dangerous. The procedure was guided byangiographic assessment, of poor quality at the time,and by measurement of the change in pressure gradi-ent across the lesion. Pressures were measured fromthe tip of the balloon catheter and at the coronary ostium through the guide catheter. Even though theballoon catheter was high profile, which was causinga pressure gradient by itself, a significant reduction intranslesional gradient could be documented after suc-cessful dilatations. Because of the lack of steerabilityof the balloon catheter, it was necessary to achieveselective intubation or at least selective direction ofthe guide catheter toward the artery to be intubated.
In 1982, at the urging of John Simpson and others,companies began to make steerable guidewires, whichrepresented the first of a series of incremental quan-tum leaps in technology such that today, virtually allsegments of the coronary tree can be reached withoutmuch difficulty.
Soon the initial enthusiasm was tempered by the highrate of stenosis recurrence, the restenosis process, a major problem in over 30% of patients undergoingangioplasty. Numerous reports on the incidence ofrestenosis began to appear.2-4 The pathological mech-anisms of restenosis have been studied by a numberof investigators.5-9 The restenotic lesion was found tobe composed of cells very similar to smooth musclecells with a great deal of extracellular matrix.9 Variouscorrelates of restenosis were identified.10 Early ran-domized trials addressed the problem of restenosis bycomparing anticoagulation regimens, without muchsuccess.11-13 Although antiplatelet agents were effectivein preventing acute complications,14,15 none of thesestudies showed that antiplatelet or anticoagulant strate-gies influenced restenosis rates. Many other drugswere tested both in animal models and in humans.All of them eventually failed to have a significant im-pact on restenosis rates after balloon angioplasty.16
This set the stage for the development of coronarystents. Stents are endoprosthetic scaffolding devicesdesigned to enlarge the vessel lumen, seal dissections,and create a rounder, smoother channel. The first hu-man implants of coronary stents occurred in 1986. Thestent was the interwoven helical self-expanding de-sign (Wallstent), which was used by Jacques Puel inToulouse, France, and Ulrich Sigwart, in Lausanne,Switzerland. At the beginning, stents were mainly in-tended to be used as a backup after balloon angioplas-ty in cases of abrupt and/or threatened closure of the
240
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
Figure 1. Historicalphotograph of AndreasGrüntzig during aposter session at theAmerican HeartAssociation Meetings in the late seventies. He was discussing theinitial results of balloonangioplasty of athero-sclerotic coronary vessels.© American HeartAssociation.

coronary artery following balloon dilatation. Abruptvessel closure, complicating 6% to 8% of balloon an-gioplasty procedures, was associated with a 5% mor-tality, 40% rate of myocardial infarction, and 40% rateof emergency coronary artery bypass grafting.17 Notonly were stents shown to significantly reduce theseadverse events, it soon became obvious that muchmore effective and predictable dilatation results couldbe obtained.17,18 Subsequently, two landmark investi-gations proved that the systematic use of stents wasassociated with improved outcome and reduced reste-nosis rate compared with balloon angioplasty. Patientsstudied in the BElgian NEtherlands STENT study(BENESTENT)19 and the STress REStenosis Study(STRESS)20 underwent single-lesion angioplasty invessels ranging from 3 to 4 mm in diameter. The reduc-
tion in restenosis was from 42% to 32% inSTRESS and from 32% to 22% in BENESTENT.Many additional studies showed in a con-sistent manner that the use of stents wasleading to predictable initial outcome andreduced restenosis rate, both contributingto decreasing the need for reintervention ascompared with balloon angioplasty (Figure 2).
Yet, stented angioplasty has been plaguedfrom the onset by early stent thrombosis(<30 days after index procedure). Indeed,initially, stent thrombosis rates as high as24% raised serious doubts as to the viabilityof the therapy.21 Moreover, restenosis, nowspecifically due to in-stent neointimal pro-liferation of matrix and vascular smooth mus-cle cells, was not abolished by bare-metalstents (BMS), remaining at 30% to 40% with
repeat revascularization still occurring in 15% to 20%of cases. Two further major developments revolution-ized the practice and results of stented angioplasty.Paul Barragan in Marseille, and others in France, beganto use antiplatelet therapy consisting of aspirin andticlopidine instead of the cocktail of virtually all avail-able anticoagulants given so far in attempting to pre-vent stent thrombosis.22 This practice spread rapidlythroughout France and other countries. An understand-ing of the improved results with antiplatelet therapywas provided by Schomig and the group in Munich.23,24
Their study, comparing aspirin and ticlopidine therapywith warfarin therapy, demonstrated that the plateletactivation occurring with the latter was not presentwhen antiplatelet therapy alone was used. This is thelikely explanation for the reduced (sub)acute throm-
241
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
Figure 2.
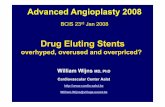
A. Upper left: À blanc picture of the right coronary arteryshows the metallic stent struts of a previously implanted drug-eluting stent (arrow) and the heavily calcified vessel walldownstream. Upper right: Contrast injection shows diffusein-stent restenosis with subocclusive luminal narrowing.Lower left: Intravascular ultrasound images inside the stent(level A) showing irregular and narrow lumen (green contours).The stent struts (thick hyperechogenic dots) have remainedapposed against the vessel wall, but neointimal tissue hasproliferated through stent struts, causing re-narrowing.Lower right: Intravascular ultrasound images recorded dis-tally (level B) show the circular and superficial calcifications,preventing penetration of ultrasound in the deeper vessel layers(shadowing effect).
B. Coronary angiography of the coronary vessel (2 projections)after overexpansion of a new drug-eluting stent deployed inside the previously implanted one, restoring a widely patentlumen.
A
B
�

242
bosis rate that has been seen in all published studiesusing antiplatelet therapy alone. These observationswere then confirmed by numerous clinical trials.25,26
During the same time period, Antonio Colombo inMilan, Italy, who was pioneering intravascular ultra-sound imaging, observed that many times stents werenot fully expanded and were in poor apposition againstthe vessel wall, potentially a risk factor for thrombosis.These features were not discernible by angiographyand his observations led to the use of high-pressurepost-stent balloon inflations for more complete expan-sion of the metallic stent struts.27
With the combined prescription of thienopyridinesand aspirin for 4 to 8 weeks,28,29 together with properstent deployment techniques,27 early stent thrombosisrates decreased to what was felt to be an unavoidableand acceptable 1% to 1.5%. Notably, it remains un-known still today what is the minimal time periodduring which it is indispensable to prescribe dual an-tiplatelet therapy after implantation of a given stenttype. Stent implantation, inherently a thrombogenicprocedure, initiates a complex interaction betweenthe blood components and the metallic surface of thestent, which includes the deposition of protein, theactivation of platelets, the complement system, andcoagulation factors. Eventually, thrombi will propagateover the surface of the stent creating a confluent en-dothelial monolayer. Modifications of the metallic stentsurface and various biologically inert surface coatings,such as carbon, platinum, phosphorylcholine, andgold have been applied to stainless-steel stents in anattempt to reduce thrombosis and restenosis, but theclinical effectiveness of these strategies has not beenproven. Instead, gold coating resulted in increasedrates of restenosis.30 Continuously ongoing efforts toreduce the �30% late in-stent restenosis rates throughvarious systemic pharmacological approaches remainedunsuccessful until local radiation, a strong antiprolif-erative therapy (vascular brachytherapy), was appliedto prevent or treat this condition.31-33
While successful in reducing restenosis, vascularbrachytherapy was the first illustration that delayedhealing might portend an increased risk of thrombosistogether with the expected reduction in neointimalproliferation and the less desirable lack of endothelial-ization. Indeed, stent thrombosis rates increased againup to 5.3%,34 and the time window of event occurrencewas extended beyond 1 year so that the initial clinicalbenefit would eventually erode as time went by, a se-quence of pathogenetic events that would repeat it-self later as radiation was replaced by cytotoxic drugs.
THE ADVENT OF DRUG-ELUTING STENTS
Considerable efforts have gone into the developmentof stents covered by an active coating designed to in-hibit in-stent restenosis—the drug-eluting stent (DES).The components of a DES can be divided into a plat-form (the stent), a carrier (usually a polymer), and anagent (a drug) to prevent restenosis. Stents are idealdelivery systems because they allow the local deliveryof the active agent to the area of vascular injury, avert-ing the need to deliver high doses systemically. Thedevelopment of a suitable carrier to transport an ap-propriate agent has been challenging, since it musthave mechanical resistance to abrasion during implan-tation, be suitable for sterilization, allow time- anddose-controlled drug release, be nonthrombogenic norbe the cause of inflammation of the vessel wall andtissue.26 Various types of coatings have been devel-oped, including phosphorylcholine, biocompatiblenonerodable, biodegradable, or bioabsorbable poly-mers, as well as ceramic layers. A drug that is success-fully eluted should inhibit the complex cascade ofevents that leads to neointimal formation after stentimplantation. The inflammatory and proliferative mech-anisms of the general tissue-healing response andspecific blood and vessel-wall components of the vas-cular reparative processes are potential targets fortherapeutic approaches aimed at reducing neointimalproliferation (Figure 3). The success of eluting devicesis highly dependent on each component of the complex,as well as on the interactions among these elements.Therefore, different DES brands will not share a classeffect, since there is a myriad of possible iterations oneach component of the drug-device combinations thatmay have significant therapeutic implications. Manyproposed devices did not work and different DES differin their ability to inhibit neointimal growth. Finally,because the results of short-term experiments in ani-mal models cannot be directly translated to humans,specific clinical trials were required in order to estab-lish the efficacy and safety for each device.
FIRST-GENERATION DRUG-ELUTING STENTS
The first positive clinical data on DES came from trialsexamining sirolimus-coated stents. Sirolimus, a natu-ral macrocyclic lactone with potent antiproliferative,anti-inflammatory, and immunosuppressive effects,acts by inhibiting the activation of the mammaliantarget of rapamycin (mTOR), ultimately causing arrestof the cell cycle (Figure 3). The Cypher sirolimus-elut-
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

243
ing stent (Cordis, Johnson & Johnson) is produced bycoating a stainless-steel stent with a thin layer of anonerodable polymer containing sirolimus. The seminalfirst implantations of slow- and fast-release sirolimus-eluting stents, in the First-in-Man (FIM) clinical study,were performed by de Souza in São Paulo, Brazil, andSerruys in Rotterdam, the Netherlands.27 Four monthsafter implantation, both formulations were associatedwith minimal neointimal hyperplasia, as measured byintravascular ultrasonography and quantitative coro-nary angiography. The slow-release formulation wassubsequently selected for clinical use. In the Brazilianstudy, intravascular ultrasonography at 4 years revealed
continued suppression of intimal hyperplasia in thegroup of 30 patients with the slow-release sirolimus-eluting stent, with an event-free survival rate of 87%.28
The results of the randomized, double-blind SIRIUStrial (SIRolImUS-eluting stent in de novo native coro-nary lesions), involving 1055 patients, were used to gainapproval of the device by the Food and Drug Admin-istration (FDA) in the United States in 2003.29 Thispivotal trial confirmed the efficacy and short-term safetyof the sirolimus-eluting stent in single, previously un-treated coronary artery lesions, with a 91% relative re-duction in angiographic restenosis compared with theotherwise identical BMS: 3.2% vs 35.4% (P<0.001).
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
Endothelial denudation
Medial dissection
Exposure of subintimalcomponents
Proliferation andmigration of vascularsmooth-muscle cells
Assembly andstabilization
of microtubes
Inhibition
InhibitionPaclitaxel
S6-ribosome
P7056 kinases
Promotion
Proliferation andmigration of vascularsmooth-muscle cells
Inhibition
PromotionInhibition
Penetration of lipid core
Stent implantation
Reaction to stent struts(macrophages, giant cells)
Activation of vascularsmooth-muscle cells
Mitogen-activatedprotein kinase
InhibitionmTOR SirolimusSirolimus- and
tacrolimus-binding protein
Downregulationof P27
MCell cycle
S
G1
G0
G2
Polymerizationof tubulin
Activation of platelets
Stent implantation
Production of cytokines,mitogens, chemotactic
factors (platelet-derivedgrowth factor β,
epidermal growth factor)
Production of tumor necrosis factor,
interleukins, chemokines,matrix metalloproteinase
angiotensin
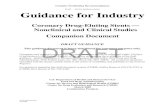
Figure 3. Mechanisms of restenosis after stent implantation and targets of therapy with sirolimus including other “limus” agents and paclitaxel. Sirolimusanalogs act through the same pathway as sirolimus. The restenosis cascade that is initiated after stent implantation is shown in green. The mechanism ofaction of sirolimus (and analogs) is shown in blue, whereas the mechanism of action of paclitaxel is shown in yellow.
Reproduced from reference 26: Serruys PW, Kutryk MJ, Ong AT. Coronary-artery stents. N Engl J Med. 2006;354:483-495. Copyright © 2006,Massachusetts Medical Society.

244
The second DES that was released on the market wasthe polymer-based paclitaxel-eluting stent. Paclitaxelis a potent antiproliferative agent that inhibits the dis-assembly of microtubules (Figure 3). A series of studies(TAXUS) were conducted to collect data on 3 iterationsof the stent platform, the Nir, the Express, and theLiberte stents (Boston Scientific). A copolymer coating(Translute, Angiotech) is used for the biphasic releaseof paclitaxel, with an initial burst in the first 2 days,followed by lower-level release for 10 days. Unlike thesirolimus-eluting stent, a considerable amount of drugis kept within the polymer (ie, not fully released). Thebiologic and clinical consequences of this specific re-lease kinetics remain elusive today. The randomizedTAXUS-IV trial, involving 1314 patients, assessed thesafety and efficacy of the slow-release paclitaxel-elutingstent in single, previously untreated lesions and ledto FDA approval in 2004.30 Nine months after stenting,the need for a repeated procedure in the treated vesselwas 4.7% in the group that received paclitaxel-elutingstents, as compared with 12.0% in the group that re-ceived BMS (P<0.001).
From the literature, the Cypher and Taxus stents ap-pear to yield similar rates of repeat revascularization,although most comparative studies suggest that theluminal preservation achieved by the Cypher stent andmeasured by coronary angiography or intravascularultrasound is slightly superior to that of the Taxusstent.31 Recent meta-analyses of all randomized com-parisons between these two stents suggest that theuse of Cypher is associated with a slightly lower needfor reintervention in the previously instrumented ves-sel as compared with Taxus.32,33
NEWER-GENERATION DRUG-ELUTING STENTS
Despite considerable reductions in angiographicrestenosis and need for repeat revascularization pro-cedures, continued attention to the safety, efficacy,and deliverability of first-generation DES has led tothe development of new antiproliferative agents withalternative stent platforms and different drug carriersystems. Numerous drug-device combinations havebeen tested, of which over 20 have received the CE(Conformité Européenne) certificate that is necessaryfor use in the European Union.34 So far, only two ofthese new-generation DES have received positive re-views by the FDA. Zotarolimus is a novel pharmacolog-ic therapy that shares similar structure and biologicactivity with the antirestenotic agent sirolimus, ie, itblocks the function of mTOR (Figure 3). The Endeavor
stent is a cobalt-based alloy stent with a phosphoryl-choline polymer loaded with zotarolimus at a doseconcentration of 10-μg/mm stent length. It has beenshown in preclinical studies that approximately 95%of zotarolimus is eluted from the stent within 15 daysof implantation, although drug concentrations withinsurrounding vascular tissue may be detected as late as30 days after stent deployment (data on file, MedtronicVascular). To date, following the pivotal ENDEAVOR IIstudy,35 4 additional clinical trials evaluating the safetyand efficacy of zotarolimus-eluting stents have beencompleted. The ENDEAVOR IV study recently com-pared the zotarolimus-eluting stent with the paclitaxel-eluting stent in 1578 patients presenting with singlede novo lesion in 2.5-3.5 diameter vessels with anoverall lesion length of less than 28 mm.36 The primaryend point of the study was target-vessel failure at 9months with a prespecified noninferiority absolutemargin of 3.8%. A subset of 328 patients underwentangiographic follow-up at 8 months. While in-stentlate loss (ie, the largest loss of lumen diameter at fol-low-up that is due to intimal hyperplasia, Figure 4) wassignificantly higher in the Endeavor stent (0.67±0.49 mmvs 0.42±0.50 mm, P<0.001), this did not translate intoa difference in terms of the primary end point (6.6%in the Endeavor vs 7.2% in the Taxus group), whichsatisfied the noninferiority end point (P<0.001 for non-inferiority of the Endeavor compared with Taxus stent.
The everolimus-eluting coronary stent system is madeavailable by two companies (Xience-V by Abbott Vascu-lar company, IL, USA and Promus by Boston Scientific,MA, USA). Xience-V is comprised of the Multilink Visionstent and a drug-eluting coating. Everolimus is blend-ed on a nonerodable polymer, coated over anothernonerodable polymer primer layer. The coating com-prises acylic- and fluoropolymers, both approved foruse in blood-contacting applications. This layer ofeverolimus-polymer matrix with a thickness of 5-6 mi-crons is applied to the surface of the stent and is loadedwith 100 μg/cm2 of everolimus with no topcoat poly-mer layer. The stent is designed to release approximate-ly 80% of the drug within 30 days after implantation.As a sirolimus analog, everolimus also inhibits mTOR(Figure 3). In the SPIRIT II trial, 300 patients were ran-domized to either everolimus- or paclitaxel-elutingstents in a 3:1 ratio. At 1 year, there was a significantdifference in terms of major adverse cardiac events(MACE) in favor of the everolimus-eluting stent (2.7%vs 9.2% P=0.04).37 These results have recently beenduplicated in the SPIRIT III study, involving 1002 pa-tients recruited in 62 clinical sites in the US, whichrecently led to a favorable FDA review.38
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

245
LATE STENT THROMBOSIS: AN ISSUE OF DELAYED VASCULAR HEALING
While all four FDA-approved DES have shown superi-ority in terms of angiographic recurrence and clinicalreintervention rates compared with uncoated stents,there is increasing evidence for both sirolimus- andpaclitaxel-eluting stents that late adverse events re-lated to abrupt stent closure (ie, late or very late stentthrombosis) are more frequent than with the use ofBMS. Most striking is the fact that abrupt thrombosismight occur at later time points (beyond 1 year), whichis reminiscent of acute coronary occlusions seen afterradiation therapy.25 These thrombosis events are rare,but clinically severe, associated with sudden death ormyocardial infarction in half of the cases.39 Absoluterates are difficult to capture because death and myo-cardial infarction can be the expression of the diseaseprocess itself. Definitions and criteria have varied fromvery specific to more inclusive, resulting in a range of
underestimated to overestimated figures.40 The mostconservative estimates indicate a 0.6% yearly incidenceup to 4 years, corresponding to an incidence densityof 1 case/100 patient years.41 Comparisons betweendevices will require the use of standardized definitions,such as provided by the Academic Research Consor-tium.42 Time will tell whether this incremental risk oflate stent thrombosis also applies to the newer-gen-eration DES, although available data up to 4 yearsfollowing implant of the Endeavor stent seem to indi-cate that no such incremental risk is present with useof this specific drug-device combination.36
Autopsy studies have shown that after BMS deploy-ment an inflammatory reaction takes place in the ves-sel wall that involves macrophages and T lymphocyteswith few B lymphocytes and giant cells.43 After implan-tation of first-generation DES, a more pronounced in-flammatory response has been described that mayoccasionally be associated with a local hypersensitivityreaction and eosinophilic infiltration. The syntheticnonbioerodable polymer containing the drug may bean important trigger of local vascular inflammation,even though the metal struts or the drug itself may par-ticipate in this phenomenon. Virmani and colleagues44
first described a case of local hypersensitivity reactionwith extensive vasculitis of intima, media, and adven-titia consisting predominantly of lymphocytes andeosinophils in a patient presenting with very late throm-bosis after sirolimus-eluting stent implantation. Histo-pathological analysis revealed aneurysmal dilatationof the vessel wall within the stented segment with ev-idence of stent malapposition and thick fibrin throm-
bus between the stent and the arterial wall. Incidenceand clinical relevance of hypersensitivity reactionsstems from a registry, with 17 of 5783 patients reportinghypersensitivity symptoms probably or certainly relat-ed to DES.45 Chronic vessel inflammation may lead topositive vessel remodeling and stent malapposition.A pooled analysis of intravascular ultrasound studiesafter sirolimus-eluting stent46 (8.5% vs 0%; P<0.05) andpaclitaxel-eluting stent47 (8.4% vs 3.5%; P<0.05) im-plantation revealed a higher incidence of incompletestent apposition with DES compared with BMS thatwas not associated with MACE in the short term. In
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
Figure 4. Left: In-stent late loss. The lumen diameter inside the stent is measured by computerized quantitative coronary angiog-raphy. The focal point of minimum lumen diameter (MLD) is identified on the immediate postimplantation angiogram (upper row,post–drug-eluting stent [DES]) and repeated on the late angiogram (typically acquired 6 to 9 months later). Late loss as the differ-ence between minimum lumen diameters (early minus late) is an angiographic metric of restenosis propensity of coronary stents.Middle: The computer searchs for the minimum diameter inside the stent as well as on the native vessel on both stent edges (about5 mm on each side). Right: In-segment late loss. Figures are representative of those observed in the SIRIUS trial (SIRolImUS-elut-ing stent in de novo native coronary lesions) after implantation of a short sirolimus-eluting stent in a 3-mm vessel.
In-stent late loss
Late loss = 0.17 mm
MLD MLD
Late loss = 0.24 mm
Post DES
Follow-up
In-segment late loss In-segment late loss

246
contrast, a study of 13 DES patients undergoing intra-vascular ultrasound before emergency percutaneouscoronary intervention (PCI) at the time of very late stentthrombosis showed a higher incidence and larger areaof incomplete stent apposition compared with a con-trol group of 144 event-free DES patients (frequency,77% vs 12%; P<0.001).48 The following pathologicalmechanisms were identified as associated or possiblycausally related to DES thrombosis: chronic inflamma-tion/hypersensitivity reaction, stenting over major sidebranches, or bifurcation stenting using the crush tech-nique, overlapping DES edges, malapposition relatedto positive arterial remodeling or incomplete stent ex-pansion, in-stent restenosis with superimposed throm-bus, resolution of mural thrombus initially jailed by stentstruts, and penetration of necrotic core by stent struts.
In a recent necropsy comparison of 23 DES cases with25 BMS cases (>30 days after the index procedure),delayed healing manifested by persistent fibrin depo-sition and incomplete reendothelialization emergedas an important discriminator between BMS and DES
(Figure 5).49 Endothelialization (27%±26% versus 66%±25% versus 90%±21%) was reduced, whereas fibrinscores (3.0%±0.9% versus 1.9%±1.1% versus 0.9%±0.8%)were increased in DES patients with late stent throm-bosis, different from both patients with patent DESand BMS. Endothelialization was nearly complete inBMS specimens examined beyond 6 months, whereasincomplete endothelialization in DES specimens per-sisted beyond 40 months. Poor stent strut coveragewas confirmed in humans by angioscopic examinationof the inner lining of the stented vessel segment.50
Several recent clinical investigations support the no-tion of reduced or dysfunctional endothelialization afterDES implantation.51-53 Normal vasodilatory responsesto various stimuli such as exercise, pacing, or intra-coronary delivery of acetylcholine were blunted or re-placed by constriction in coronary segments proximaland distal to the stented area. Functional abnormalitiestended to be more pronounced with some DES brandsthan with others.53 Finally, drugs released from thedrug-polymer combination may exert a thrombogeniceffect on their own. Paclitaxel and sirolimus have been
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
Figure 5. A 65-year-old man suffered traumatic head injury resulting in death. He had received a sirolimus-eluting stent in the proximaland a bare-metallic Bx Velocity stent (BMS) in the distal left anterior descending (LAD) coronary artery. A (Cypher) and D (Bx Velocity)are radiographs of the stented LAD segment. B shows minimal strut coverage of Cypher stent. C shows peristrut fibrin, with rare endothelialcells. E shows abundant neointima and overlying endothelium covering the BMS. F shows high power: lymphocytes are present aroundthe stent struts, with minimal fibrin. The luminal surface is covered by smooth muscle cells in a proteoglycan/collagen rich matrix.
Reproduced from reference 49: Joner M, Finn AL, Farb A, et al. Pathology of drug-eluting stents in humans: delayed healing andlate thrombotic risk. J Am Coll Cardiol. 2006;48;193-202. Copyright © 2006, Elsevier Biomedical.
A B
CypherNo endothelialization
Fibrin
Fibrin
Strut
Neointima
BxVelocityC
D E F

247
reported to enhance endothelial tissue factor expres-sion, a cell surface receptor for coagulation factor VII,the principal activator of the coagulation cascade thatactivates factors IX and X.54,55
In summary, delayed healing and impaired endothelial-ization are common features of most cases of late andvery late stent thrombosis, and represent the likelycause of this severe adverse event. In contradistinctionto the thick layer of neointima that forms after balloonangioplasty or BMS implantation, the surface cover-age on a DES may be thin and brittle or even absentand thus prone to rupture, not unlike a vulnerableplaque. It remains to be explained why sirolimus-elut-ing stents are not more susceptible to this problemthan paclitaxel-eluting stents in light of their attestedthinner neointimal coverage. Inhomogeneity of neoin-timal hyperplasia with the paclitaxel-eluting stent (thinon struts, thicker between struts) may account for this.Long-term follow-up of newer DES will be pivotal toassess the incidence of late and very late stent throm-bosis for these devices that are intended to reconcileabsence of restenosis and late safety without interfer-ing with vascular healing and endothelial function.
SYSTEMIC ANTIPLATELET THERAPY
Recognizing that the pathogenesis of late stent throm-bosis is multifactorial and the importance of localfactors, one should not underestimate the key role ofsystemic factors. Poor response to antiplatelet therapyand the many conditions causing a permanent or tran-sient increase in the propensity for arterial thrombo-sis will both contribute to an increased risk of stentthrombosis. Whether or not a patient is at increasedrisk for stent thrombosis and for how long will dependon the complex interplay between the many possiblecombinations of any of the abovementioned local andsystemic factors. With the use of first-generation DES,an empirical approach has been to prolong the durationof dual antiplatelet effect so as to match the presumedwindow of increased risk. A retrospective analysis ofthe Duke database suggested that there is possiblebenefit associated with extension of dual antiplatelettherapy from 6 months to 1 year.56 This practice is nowendorsed by international guidelines.57,58 Protagonistsargue that long-term antiplatelet therapy might havea favorable effect on the natural course of coronarypatients in whom events are also caused by systemicatherosclerosis. There are, however, several drawbacksto this approach. All subjects receive blanket therapy,while only few might actually be at risk, for a variable,device-specific time period. Presently, these individu-
als at risk who could benefit from the prolonged ther-apy cannot be identified. Under these circumstances,blanket pharmacological prevention of a rare eventmakes little sense from an epidemiological perspectiveand can simply not be cost-effective. Secondly, thisapproach weakens the weaker even further. Elderly pa-tients or patients with severe comorbidities are morelikely to be in need of noncardiac diagnostic or surgi-cal interventions that either require treatment inter-ruption or will be associated with increased complica-tion rates when performed under dual antiplatelettherapy. Thirdly, long-term dual antiplatelet therapyhas been associated with excess bleeding in all previ-ously published large trials, including the recently re-ported TRITON study.59 Finally, enforcing an obligatorylong-term systemic drug-device combination annihi-lates the fundamental promise of DES, which was basedon local delivery of tiny amounts of drug, thereforedevoid of systemic side effects. From a cost perspec-tive, one is not easily inclined to add yet another drugto the already long list of medicines that are prescribedto coronary patients. These important issues are dis-cussed in greater detail in the contribution by Pfistereret al in the present issue.
Thus for the time being, the option of extending theduration of dual antiplatelet therapy … forever (?) isempirically envisaged after implantation of first-gen-eration DES, but does not represent a true, sustainablesolution to the problem for the future. Poor respondersto antiplatelet agents obviously represent an excep-tion.60 When properly identified at the time of stent im-plantation, these patients will require a systemic solu-tion to their systemic problem, be it an increase in thedose of clopidogrel or prescription of a more potentdrug such as prasugrel.
PRECLINICAL AND CLINICAL EVALUATION OF FUTURE DRUG-ELUTING STENTS
Until the concerns with late stent thrombosis were rec-ognized, attention was primarily, if not exclusively, focused on the antirestenosis properties of DES.61,62
Today, the emphasis is placed on their efficacy-safetyratio, which appears to depend on the balance betweenthe early benefit, namely the desired antirestenosis ef-fect, and the late hazard, driven by the rare, but severe,complication of stent thrombosis. This new concept,at times called “net clinical benefit,” is increasinglyoften recommended as an appropriate, patient-drivenend point for evaluation of newer-generation devices.Much more attention will be given to safety indicators
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

during preclinical evaluation, including indices of en-dothelial coverage and functionality, nitric oxide produc-tion, or restoration of endothelial-dependent vasomo-tion. During early human evaluation, intermediatemechanistic end points that might be relevant for safety,such as the degree of endothelial coverage, are beingcollected using high definition intracoronary imagingof stent struts with Optical Coherence Tomography63
or angioscopy.50 In this way, claims regarding increasedbiocompatibility of new or bioerodable materials canbe tested at an early stage of the evaluation plan ofthese novel devices. The assessment plan that has beenapplied so far to DES has allowed robust evaluationof efficacy, rapid identification of many inefficaciousiterations, and relatively rapid patient access, at leastin Europe (Table I) (see also discussion by Shah andSchulman in this issue of Dialogues in CardiovascularMedicine). However, this approach has been primarilydevice-oriented, aiming to address the superiority orequivalence of one device versus the other. Hoping toprovide the data that would justify the replacement ofthe old (cheap) by the new (expensive) device, mosttrials failed to ask which patient or lesion subset wouldbenefit the most. Physicians felt compelled to extrap-olate the outstanding results obtained in selectedpopulations to all-comers. As a result, much is knownabout the findings of DES in those who needed themthe least (on-label use). Limited randomized data orobservational data of lesser quality derived from post-marketing surveillance registries only provided weakevidence to support the use of DES in patients andlesion subsets needing them the most (the so-calledoff-label use). Given today’s knowledge base, differentrecommendations can be formulated.64 After the ini-tial FIM confirmation of adequate preclinical findings,pivotal randomized trials of novel drug-device combi-nations should focus on more challenging patient and
lesion subsets that are representative of clinical prac-tice. Long-term safety data from properly poweredstudy populations can then be acquired during an ini-tial phase of conditional approval. There are manynew or future candidate DES hoping to achieve recon-ciliation between powerful efficacy and retained safety.
Among the many options, one could mention theeverolimus-eluting stent37,38 and the Resolute zotaro-limus-eluting stent65; both are using durable, as wellas more biocompatible, polymers. Other options haveincorporated biodegradable polymers, namely the bio-limus-A9 eluting program that was applied to severalstent platforms66 or the sirolimus-eluting device usingthe modified stent platforms in which the drug is re-leased from tiny reservoirs. Several research teamsare developing fully biodegradable stents in combina-tion with drug elution.67,68 The objective is to providethe necessary mechanical scaffold and prevention ofrestenosis for a finite period of time after which thevessel would regain its natural state, without leavingbehind a permanent implant and the appended down-sides. This concept would be devoid of many currentlyfaced issues such as chronic inflammation, delayedvessel healing, disturbed vasomotion or incompatibilitywith radiation-based or magnetic resonance imagingand later bypass surgery.
All these novel options, some of which have reachedan advanced stage of clinical evaluation, are indicativeof the wide spectrum of higher effectiveness in com-bination with increased biocompatibility that will even-tually be achievable with the future generations of DES.How the availability of DES will continue to impacton treatment choices for patients with coronary arterydisease is discussed by Adgey et al in the present issueof Dialogues in Cardiovascular Medicine.
248
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
1st generation• Preclinical
• First-in-Man (FIM)
• (Dose-response & kinetics)
• Pivotal randomized trial
Superiority vs BMSPowered for combined clinical/
angiographic end points • Complex lesion/patient subset • Real-life registry
2nd generation• Preclinical
• First-in-Man (FIM)
• (Dose-response & kinetics)
• Pivotal randomized trial
Noninferiority vs 1st DESPowered for angiographic efficacy end
points • Complex lesion/patient subset • Real-life registry
EVALUATION PATHWAYS FOR DES
Table I. Preclinical and clinical evaluationscheme of drug-eluting stents (DES). New drug-device combinations are tested for noninferiorityagainst first-generation DES (Cypher or Taxus).The Endeavor stent has been tested for superiorityagainst bare-metal stent (BMS) and noninferiorityagainst both Cypher and Taxus. None of the pub-lished stent trials are powered for clinical outcome(death, nonfatal myocardial infarction). The valueand limitations of these evaluation schemes arediscussed in the contribution by Shah andSchulman in this issue.

249
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli
REFERENCES
1. Hurst JW.
History of Cardiac Catheterization.
New York, NY: McGraw-Hill; 1985.
2. Meier B, King SB 3rd, Gruentzig AR, et al.
Repeat coronary angioplasty.
J Am Coll Cardiol. 1984;4:463-466.
3. Leimgruber PP, Roubin GS, Hollman J, et al.
Restenosis after successful coronary angioplasty in patients withsingle-vessel disease.
Circulation. 1986;73:710-717.
4. Mercado N, Boersma E, Wijns W, et al.
Clinical and quantitative coronary angiographic predictors ofcoronary restenosis. A comparative analysis from the balloon-to-stent era.
J Am Coll Cardiol. 2001;38:645-652.
5. Gravanis MB.
The enigma of restenosis after percutaneous transluminal coronaryangioplasty.
Am J Cardiovasc Pathol. 1988;2:1-5.
6. Gravanis MB, Roubin GS.
Histopathologic phenomena at the site of percutaneous translumi-nal coronary angioplasty: the problem of restenosis.
Hum Pathol. 1989;20:477-485.
7. Karas SP, Santoian EC, Gravanis MB.
Restenosis following coronary angioplasty.
Clin Cardiol. 1991;14:791-801.
8. Johnson DE, Hinohara T, Selmon MR, Braden LJ,Simpson JB.
Primary peripheral arterial stenoses and restenoses excised bytransluminal atherectomy: a histopathologic study.
J Am Coll Cardiol. 1990;15:419-425.
9. Austin GE, Ratliff NB, Hollman J, Tabei S, Phillips DF.
Intimal proliferation of smooth muscle cells as an explanation forrecurrent coronary artery stenosis after percutaneous transluminalcoronary angioplasty.
J Am Coll Cardiol. 1985;6:369-375.
10. Ryan TJ, Faxon DP, Gunnar RM, et al.
Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American HeartAssociation Task Force on Assessment of Diagnostic and TherapeuticCardiovascular Procedures (Subcommittee on Percutaneous Trans-luminal Coronary Angioplasty).
Circulation. 1988;78:486-502.
11. Thornton MA, Gruentzig AR, Hollman J, King SB 3rd,Douglas JS.
Coumadin and aspirin in prevention of recurrence after translumi-nal coronary angioplasty: a randomized study.
Circulation. 1984;69:721-727.
12. Ellis SG, Roubin GS, Wilentz J, Douglas JS Jr, King SB,3rd.
Effect of 18- to 24-hour heparin administration for prevention ofrestenosis after uncomplicated coronary angioplasty.
Am Heart J. 1989;117:777-782.
13. Urban P, Buller N, Fox K, Shapiro L, Bayliss J,Rickards A.
Lack of effect of warfarin on the restenosis rate or on clinical out-come after balloon coronary angioplasty.
Br Heart J. 1988;60:485-488.
14. Wilentz JR, Sanborn TA, Haudenschild CC, Valeri CR,Ryan TJ, Faxon DP.
Platelet accumulation in experimental angioplasty: time courseand relation to vascular injury.
Circulation. 1987;75:636-642.
15. Barnathan ES, Schwartz JS, Taylor L, et al.
Aspirin and dipyridamole in the prevention of acute coronarythrombosis complicating coronary angioplasty.
Circulation. 1987;76:125-134.
16. Douglas JS Jr.
Pharmacologic approaches to restenosis prevention.
Am J Cardiol. 2007;100:10K-6K.
17. Detre K, Holubkov R, Kelsey S, et al.
One-year follow-up results of the 1985-1986 National Heart,Lung, and Blood Institute’s Percutaneous Transluminal CoronaryAngioplasty Registry.
Circulation. 1989;80:421-428.
18. Schomig A, Kastrati A, Mudra H, et al.
Four-year experience with Palmaz-Schatz stenting in coronary angioplasty complicated by dissection with threatened or presentvessel closure.
Circulation. 1994;90:2716-2724.
19. Serruys PW, de Jaegere P, Kiemeneij F, et al.
A comparison of balloon-expandable-stent implantation with balloonangioplasty in patients with coronary artery disease. BenestentStudy Group.
N Engl J Med. 1994;331:489-495.
20. Fischman DL, Leon MB, Baim DS, et al.
A randomized comparison of coronary-stent placement and balloonangioplasty in the treatment of coronary artery disease. StentRestenosis Study Investigators.
N Engl J Med. 1994;331:496-501.

21. Serruys PW, Strauss BH, Beatt KJ, et al.
Angiographic follow-up after placement of a self-expanding coronary-artery stent.
N Engl J Med. 1991;324:13-17.
22. Barragan P, Sainsous J, Silvestri M, et al.
Ticlopidine and subcutaneous heparin as an alternative regimenfollowing coronary stenting.
Cathet Cardiovasc Diagn. 1994;32:133-138.
23. Schomig A, Neumann FJ, Kastrati A, et al.
A randomized comparison of antiplatelet and anticoagulant therapyafter the placement of coronary-artery stents.
N Engl J Med. 1996;334:1084-1089.
24. Gawaz M, Neumann FJ, Ott I, May A, Schomig A.
Platelet activation and coronary stent implantation. Effect of anti-thrombotic therapy.
Circulation. 1996;94:279-285.
25. Schuhlen H, Hadamitzky M, Walter H, Ulm K,Schomig A.
Major benefit from antiplatelet therapy for patients at high risk foradverse cardiac events after coronary Palmaz-Schatz stent place-ment: analysis of a prospective risk stratification protocol in theIntracoronary Stenting and Antithrombotic Regimen (ISAR) trial.
Circulation. 1997;95:2015-2021.
26. Serruys PW, Kutryk MJ, Ong AT.
Coronary-artery stents.
N Engl J Med. 2006;354:483-495.
27. Sousa JE, Costa MA, Abizaid A, et al.
Sirolimus-eluting stent for the treatment of in-stent restenosis: aquantitative coronary angiography and three-dimensional in-travascular ultrasound study.
Circulation. 2003;107:24-27.
28. Sousa JE, Costa MA, Abizaid A, et al.
Four-year angiographic and intravascular ultrasound follow-up ofpatients treated with sirolimus-eluting stents.
Circulation. 2005;111:2326-2329.
29. Moses JW, Leon MB, Popma JJ, et al.
Sirolimus-eluting stents versus standard stents in patients withstenosis in a native coronary artery.
N Engl J Med. 2003;349:1315-1323.
30. Stone GW, Ellis SG, Cox DA, et al.
A polymer-based, paclitaxel-eluting stent in patients with coronaryartery disease.
N Engl J Med. 2004;350:221-231.
31. Morice MC, Colombo A, Meier B, et al.
Sirolimus- vs paclitaxel-eluting stents in de novo coronary arterylesions: the REALITY trial: a randomized controlled trial.
JAMA. 2006;295:895-904.
32. Stettler C, Wandel S, Allemann S, et al.
Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis.
Lancet. 2007;370:937-948.
33. Schomig A, Dibra A, Windecker S, et al.
A meta-analysis of 16 randomized trials of sirolimus-eluting stentsversus paclitaxel-eluting stents in patients with coronary arterydisease.
J Am Coll Cardiol. 2007;50:1373-1380.
34. Silber S, Borggrefe M, Böhm M, et al.
Positionspapier der DGK zur Wirksamkeit und Sicherheit vanMedikamente freisentzenden Koronarstents (DES).
Der Kardiologe. 2007;1:84-111.
35. Fajadet J, Wijns W, Laarman GJ, et al.
Randomized, double-blind, multicenter study of the Endeavor zotarolimus-eluting phosphorylcholine-encapsulated stent for treat-ment of native coronary artery lesions: clinical and angiographicresults of the ENDEAVOR II trial.
Circulation. 2006;114:798-806.
36. US FDA/CDRH: New Device Approval—EndeavorZotarolimus-Eluting stent.
http://www.fda.gov/cdrh/pdf6/p060033b.pdf – AccessedSeptember 5, 2008.
37. Serruys PW, Veldhof S, Dorange C, et al.
One year clinical follow-up of the XIENCE V Everolimus-elutingstent system in the treatment of patients with de novo native coro-nary artery lesions: the SPIRIT II study.
EuroInterv. 2007;3:315-320.
38. US FDA/CDRH: New Device Approval—Xience-VEverolimus Eluting Coronary Stent System.
www.fda.gov/ohrms/dockets/ac/07/slides/Presentation.pdf.Accessed September 5, 2008.
39. Kuchulakanti PK, Chu WW, Torguson R, et al.
Correlates and long-term outcomes of angiographically provenstent thrombosis with sirolimus- and paclitaxel-eluting stents.
Circulation. 2006;113:1108-1113.
40. Mauri L, Hsieh W, Massaro JM, et al.
Stent thrombosis in randomized trials of drug-eluting stents.
N Engl J Med. 2007;356:1020-1029.
250
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

251
41. Daemen J, Wenaweser P, Tsuchida K, et al.
Early and late coronary stent thrombosis of sirolimus-eluting andpaclitaxel-eluting stents in routine clinical practice: data from alarge two-institutional cohort study.
Lancet. 2007;369:667-678.
42. Cutlip DE, Windecker S, Mehran R, et al.
Academic Research Consortium. Clinical endpoins in coronarystent trials: a case for standardized definitions.
Circulation. 2007;115:2344-2351.
43. Farb A, Sangiorgi G, Carter AJ, et al.
Pathology of acute and chronic coronary stenting in humans.
Circulation. 1999;99:44-52.
44. Virmani R, Guagliumi G, Farb A, et al.
Localized hypersensitivity and late coronary thrombosis secondaryto a sirolimus-eluting stent: should we be cautious?
Circulation. 2004;109:701-705.
45. Nebeker JR, Virmani R, Bennett CL, et al.
Hypersensitivity cases associated with drug-eluting coronary stents:a review of available cases from the Research on Adverse DrugEvents and Reports (RADAR) project.
J Am Coll Cardiol. 2006;47:175-181.
46. Ako J, Morino Y, Honda Y, et al.
Late incomplete stent apposition after sirolimus-eluting stent implan-tation: a serial intravascular ultrasound analysis.
J Am Coll Cardiol. 2005;46:1002-1005.
47. Mintz GS, Weissman NJ.
Intravascular ultrasound in the drug-eluting stent era.
J Am Coll Cardiol. 2006;48:421-429.
48. Cook S, Wenaweser P, Togni M, et al.
Incomplete stent apposition and very late stent thrombosis afterdrug-eluting stent implantation.
Circulation. 2007;115:2426-2434.
49. Joner M, Finn AV, Farb A, et al.
Pathology of drug-eluting stents in humans: delayed healing andlate thrombotic risk.
J Am Coll Cardiol. 2006;48:193-202.
50. Kotani J, Awata M, Nanto S, et al.
Incomplete neointimal coverage of sirolimus-eluting stents: angio-scopic findings.
J Am Coll Cardiol. 2006;47:2108-2111.
51. Togni M, Windecker S, Cocchia R, et al.
Sirolimus-eluting stents associated with paradoxic coronary vaso-constriction.
J Am Coll Cardiol. 2005;46:231-236.
52. Hofma S, Van der Giessen W, Van Dalen B, et al.
Indication of long-term endothelial dysfunction after sirolimus-eluting stent implantation.
Eur Heart J. 2006;27:166-170.
53. Hamilos MI, Ostojic M, Beleslin B, et al.
Differential effects of drug-eluting stents on local endothelium-dependent coronary vasomotion.
J Am Coll Cardiol. 2008;51:2123-2129.
54. Steffel J, Latini RA, Akhmedov A, et al.
Rapamycin, but not FK-506, increases endothelial tissue factor expression: implications for drug-eluting stent design.
Circulation. 2005;112:2002-2011.
55. Stahli BE, Camici GG, Steffel J, et al.
Paclitaxel enhances thrombin-induced endothelial tissue factor expression via c-Jun terminal NH2 kinase activation.
Circ Res. 2006;99:149-155.
56. Eisenstein EL, Anstrom KJ, Kong DF, Shaw LK, et al.
Clopidogrel use and long-term clinical outcomes after drug-elutingstent implantation.
JAMA. 2007;297:159-168.
57. Spencer B. King, III, Sidney C. Smith Jr, John W.Hirshfeld Jr, et al.
2007 Focused Update of the ACC/AHA/SCAI 2005 GuidelineUpdate for Percutaneous Coronary Intervention. A Report of theAmerican College of Cardiology/American Heart Association TaskForce on Practice Guidelines: 2007 Writing Group to Review NewEvidence and Update the ACC/AHA/SCAI 2005 Guideline Updatefor Percutaneous Coronary Intervention, Writing on Behalf of the2005 Writing Committee.
Circulation. 2008;117:261-295.
58. Silber S, Albertsson P, Avilés FF, et al.
Guidelines for percutaneous coronary interventions. The Task Forcefor Percutaneous Coronary Interventions of the European Societyof Cardiology.
Eur Heart J. 2005;26:804-847.
59. Wiviott SD, Braunwald E, McCabe CH, et al.
Prasugrel versus clopidogrel in patients with acute coronary syn-dromes. TRITON-TIMI 38 Investigators.
N Engl J Med. 2007;357:2001-2015.
60. Bonello L, Camoin-Jau L, Aques S, et al.
Adjusted clopidogrel loading doses according to vasodilator-stimu-lated phosphoprotein phosphorylation index decrease rate of majoradverse cardiovascular events in patients with clopidogrel resistance:a multicenter randomized prospective study.
J Am Coll Cardiol. 2008;51:1404-1411.
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

252
61. Camenzind E, Steg PG, Wijns W.
Stent thrombosis late after implantation of first-generation drug-eluting stents. A cause for concern.
Circulation. 2007;115:1440-1455.
62. Serruys PW, Daemen J.
Late stent thrombosis. A nuisance in both bare-metal and drug-eluting stens.
Circulation. 2007;115:1433-1439.
63. Matsumoto D, Shite J, Shinke T, et al.
Incomplete neointimal coverage of sirolimus-eluting stents: angio-scopic findings.
Eur Heart J. 2007;28:961-967.
64. Daemen J, Simoons ML, Wijns W, et al.
Meeting Report ESC Forum on Drug Eluting Stents, EuropeanHeart House, Nice, 27-28 September 2007.
Eur Heart J. 2008. Nov 26 [Epub ahead of print].
65. Meredith I, Worthley S, Whitbourn R, et al.
The next-generation Endeavor Resolute stent: 4-month clinicaland angiographic results from the Resolute first-in-man trial.
EuroInterv. 2007;3:50-53.
66. Chevalier B, Serruys PW, Silber S, et al.
Randomized comparison of Nobori, Biolimus A9 drug-elutingcoronary stent with a Taxus, paclitaxel-eluting coronary stent inpatients with stenosis in native coronary arteries: the Nobori 1 trial.
EuroInterv. 2007;2:426-434.
67. Tanimoto S, Serruys PW, Thuesen L, et al.
Comparison of in vivo acute stent recoil between the bioabsorbableeverolimus-eluting coronary stent and the everolimus-eluting cobaltchromium coronary stent: insights from the ABSORB and SPIRITtrials.
Catheter Cardiovasc Interv. 2007;70:515-523.
68. Erbel R, Di Mario C, Bartunek J, et al.
Temporary scaffolding of coronary arteries with bioabsorbablemagnesium stents: a prospective, non-randomised multicentre trial.
Lancet. 2007;369:1869-1875.
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting coronary stents: stents and stent-ability - Wijns and Valgimigli

253
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents?
B. R. Shah, K. A. Schulman
Antiplatelet therapy: what to do if the patient with a drug-eluting stent needs elective noncardiac surgery?
M. Pfisterer, M. J. Zellweger, M. Filipovic, F. Nietlispach
Expert Answers to Three Key Questions
Medical therapy, surgery, or PCI: does (or should) the availability of drug-eluting stents influence the decision?
A. A. J. Adgey, B. M. Glover, S. J. Walsh
1
Drug-Eluting Stents in Angina
2
3

here is considerable debateregarding the benefits of op-timal medical therapy in pa-tients with stable angina who
may constitute up to 85% of patientsundergoing percutaneous coronaryintervention (PCI) in the US.1 TheClinical Outcomes Utilizing Revas-cularization and AGgressive drugEvaluation (COURAGE) trial in pa-tients with stable coronary arterydisease compared all-cause deathsor nonfatal myocardial infarction
(MI) in >2000 patients randomizedto either optimal medical therapywith or without PCI.2 There was nodifference in either the primary endpoint for either group (over a me-dian of 4.6 years). Although therewas no difference in the frequencyof angina at 5 years, one third of pa-tients in the optimal medical ther-apy group subsequently underwenta revascularization procedure. There-fore, the results of this study sup-port the role of PCI in symptom re-lief in patients with stable coronaryartery disease. It should also benoted that patients who are knownto improve prognostically from revas-cularization were not included in
While optimal medical therapyimproves prognosis in a significantnumber of patients with stable coro-nary artery disease (CAD), revas-cularization either by percutaneouscoronary intervention (PCI) orcoronary artery bypass grafting(CABG) is often required. This maybe to reduce symptoms and/or im-prove prognosis in certain subgroupsusing PCI. Drug-eluting stents(DES) have been shown to reducein-stent restenosis and target-vesselrevascularization compared withbare-metal stents. This has led tothe hypothesis that outcomes aftermultivessel coronary stenting withDES might be comparable to sur-gical revascularization for some pa-tient groups. We review the evidencefor medical therapy in CAD, andassess when patients should be con-sidered for PCI or CABG, DES,and the risks associated with DESimplantation.
T
Keywords: stable coronary artery disease;revascularization; drug-eluting stent;sirolimus; paclitaxelAddress for correspondence:Professor A. A. Jennifer Adgey, ConsultantCardiologist, Royal Victoria Hospital,Grosvenor Rd, Belfast BT12 6BA, NorthernIreland, United Kingdom(e-mail: [email protected])Dialogues Cardiovasc Med. 2008;13:255-261
255Copyright © 2008 LLS SAS. All rights reserved www.dialogues-cvm.org
Medical therapy, surgery, or PCI: does (or should)the availability of drug-eluting stents influence the decision?A. A. Jennifer Adgey*, MD, FRCP; Ben M. Glover*, MD, MRCP; Simon J. Walsh†, MD, MRCP*Royal Victoria Hospital - Belfast - Northern Ireland - UK; †Craigavon Area Hospital - Portadown - Northern Ireland - UK
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
WHAT EVIDENCE DO WEHAVE FOR MEDICAL
THERAPY, CABG, OR PCI?
SELECTED ABBREVIATIONS AND ACRONYMS
BARI Bypass Angioplasty RevascularizationInvestigation
BMS bare-metal stent
CABG coronary artery bypass grafting
CASS Coronary Artery Surgery Study
COURAGE Clinical Outcomes Utilizing Revascularizationand AGgressive drug Evaluation
DES drug-eluting stent
LMCA left main coronary artery
MASS II Medicine, Angioplasty, or Surgery Study–2
MI myocardial infarction
NSTEMI non-ST-segment–elevation myocardial infarction
PCI percutaneous coronary intervention
POBA plain old balloon angioplasty

this trial such as those with ongo-ing unstable symptoms, prognosti-cally unfavorable stress tests, leftmain stem disease, and multivesseldisease with significant left ventricu-lar dysfunction. It is therefore rea-sonable to postulate that CABGwould not have led to a significantsurvival benefit either, over modernoptimal medical therapy for the pop-ulation who were investigated. Inthe Medicine, Angioplasty, or Sur-gery Study–2 (MASS II) study therewas no survival benefit for eitherPCI or coronary artery bypass graft-ing (CABG) above medical therapyover 1 year when lower-risk patientswere treated.3
Of those undergoing PCI in the UK,in approximately 50% it is associat-ed with acute coronary syndromes4
and the results of COURAGE donot apply to these patients (<2% ofCOURAGE patients had CanadianCardiovascular Society (CCS) class 4angina at presentation).5
As with any population of patientswith coronary disease, there is aspectrum of patients who will re-quire revascularization by either PCIor CABG for symptom reduction orto improve prognosis. For the ma-jority of these patients, there areno overwhelming data to supporteither strategy at present. Ultimate-ly, some patients are not suitablefor either modality of revasculariza-tion due to technical limitations or severe comorbidity. In addition,those with stable symptoms do notrequire revascularization either prog-nostically or for symptomatic bene-fit and do well with medical therapy.Physicians must help make choicesfor individual patients on the clini-cal information, the available evi-dence, and the wishes of the patient.
Up-to-date evidence demonstratingimproved prognosis of CABG overoptimal medical management is
limited. Many studies were carriedout before the development andwidespread use of contemporarytreatments and also modern surgicaltechniques. It should be remem-bered that the initial results of theCoronary Artery Surgery Study(CASS) demonstrated no survivalbenefit for surgery over medicaltherapy over a 5-year period in pa-tients with normal ventricular func-
tion.6 The largest reported compari-son of CABG over optimal medicaltherapy is a collaborative meta-anal-ysis of 7 randomized trials of stablecoronary artery disease patients.7
This demonstrated a reduction inmortality at both 5 years and 10years in patients who underwentCABG (Figure 1), although the over-all survival benefit was only 4.3months over 10 years for the wholepopulation.8 Unsurprisingly, thegreatest mortality reduction occurredin patients with triple-vessel disease,left main coronary artery (LMCA)stenosis and impaired left ventricu-lar (LV) function. It is often forgottenthat these data cannot be consid-ered as contemporary, given that
none of the patients were routinelytreated with drugs such as statins,angiotensin-converting enzyme(ACE) inhibitors, thienopyridines,or β-blockers in the setting of sig-nificant left ventricular dysfunction.
The survival advantage for CABGover medical therapy in patientswith significant LMCA stenosis isgenerally accepted and also ap-
plied to LMCA equivalents (>70%ostial left anterior descending andleft circumflex).8 At present, histor-ical rather than contemporary trialdata continue to drive practice to-ward surgical revascularization forpatients with reduced LV function(ejection fraction >30% and <50%)and for those with diabetes. Thosewith severe impairment of LV func-tion (ejection fraction <30%) arerarely entered into surgical trials.
Direct comparisons between PCIand CABG are also hindered by alack of contemporary evidence. Thelong-term results of the Bypass An-gioplasty Revascularization Investi-gation (BARI) study demonstrate a
256
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others
CABG n = 1324
Medicine n = 1325
0.00
0.10
0.20
0.30
0.40
0.50
Time from randomization (years)
Cum
ula
tive
mort
ality
rate
0 2 4 6 8 10 12
Figure 1. Cumulative total mortality from all studies comparing coronary arterybypass grafting (CABG) versus medical therapy.
Modified from reference 8: Eagle KA, Guyton RA, Davidoff R. ACC/AHA 2004guideline update for coronary artery bypass surgery: Summary article: A report ofthe American College of Cardiology/American Heart Association Task Force onPractice Guidelines. J Am Coll Cardiol. 2004;44:1146-1154. Copyright © 2004,Elsevier Biomedical.

significant survival advantage forpatients with diabetes undergoingCABG.9 Despite, in this trial, thecomparison of angioplasty andCABG, there is almost identicallong-term survival in nondiabeticpatients. While it is accepted thatthere is a clear need for an increasein repeated revascularization withbare-metal stents (BMS) comparedwith CABG, there are no clear ben-efits in survival for the vast majorityof patients who undergo surgicalrevascularization.10
Relatively recent studies have alsodocumented no benefit of surgery forreducing major adverse cardiovas-cular events with CABG over PCI.11
Furthermore, there are no long-termdifferences in survival for CABG pa-tients compared to those treatedby PCI in the Arterial Revascular-ization Therapies Study [ARTS],12
ERACI II (not an acronym),13 or theMASS II studies.14 A recent compre-hensive meta-analysis of almost10 000 patients in randomized stud-ies comparing these revasculariza-tion strategies (CABG versus PCIboth with or without coronary stents)reaches the same conclusion: CABGconfers no survival benefit for thepatients enrolled in these trials.15
It may be that over a very long pe-riod of time (greater than 10 years)any advantages of CABG are lostprogressively due to worsening graftdisease. As graft failure increaseswith time, clinical events will un-doubtedly increase and it seemsreasonable to assume that mortalitywill also accelerate as this occurs.
Current guidelines advocate anearly invasive strategy for the ma-jority of patients with non-ST-seg-ment–elevation acute coronary syn-dromes, especially those at highestrisk.16 While a symptom-driven con-servative strategy may be warrantedin some patients with a stabilized
non-ST-segment–elevation myocar-dial infarction (NSTEMI), there issufficient evidence of a reduction indeath, MI, or hospitalization in thelong-term to support early consid-eration of revascularization for pa-tients with non-ST-segment–eleva-tion acute coronary syndromes.17
In general, patients with these formsof acute coronary syndromes will beat increased risk of future cardiacevents. Those with LMCA disease,diabetics with multivessel disease,and patients with significant leftventricular systolic dysfunction (al-though severe dysfunction precludessurgery) will usually be consideredfor CABG. Of those, patients withsevere comorbidities will usuallybe referred for PCI as they are un-suitable for CABG due to an unac-ceptable operative risk. A largeproportion of patients do not fallinto these categories, and whererevascularization is indicated, it ismost frequently performed by PCI.
Contemporary trial data that specifi-cally compare outcomes for patientswith non-ST-segment elevationacute coronary syndromes managedmedically, by PCI or surgery are lack-ing. The Veterans’ Affairs AnginaWith Extremely Serious OperativeMortality Evaluation (AWESOME)trial found comparable survival withCABG and PCI for those at high op-erative risk at 3 years follow up.18
All patients had ongoing unstableischemia and one third of the pa-tients had had an MI within 7 daysof randomization. Interestingly, justover half the PCI patients had stentsdeployed. Similarly, the ArterialRevascularization Therapy Study(ARTS), which compared PCI withCABG also included �1/3 of patientswith unstable angina, found identi-cal 3-year survival rates withoutstroke or MI in addition.19 Both stud-ies reported more repeat revascu-larization procedures with PCI.
DRUG-ELUTING STENTS: A BALANCED VIEW OF
THE EVIDENCE IN 2008
The use of intracoronary stents hasbeen routine in clinical practice forover a decade. It is widely acceptedthat these improve clinical out-comes over plain old balloon an-gioplasty (POBA), principally by reducing early acute vessel closureand subsequently restenosis of tar-get lesions. This results in a reducedneed for repeat revascularizationprocedures compared with POBA.However, with BMS there is still asignificant incidence of neointimalproliferation, vessel lumen compro-mise, and recurrent angina. This hasbeen reported to result in a revas-cularization rate of 10% to 25% with-in 1 year of PCI (BMS) in the UK.20
In order to reduce this problem,stents coated with an antiprolifera-tive agent have been developed:drug-eluting stents (DES). Many tri-als have now been carried out thatdemonstrate a highly significantreduction in in-stent restenosis andthe need for target-vessel revascu-larization when DES are comparedwith BMS.21,22
In-stent thrombosis, although muchless common than in-stent resteno-sis, generally results in an acute MIand also has a significant mortality.Historically, this complication oc-curred with BMS before reendothe-lialization had occurred and it isless common in BMS 4 weeks afterimplantation. Recently, it has be-come apparent that there is a small,but significant, increased risk ofvery late stent thrombosis associat-ed with DES. This is mainly attrib-uted to incomplete reendothelial-ization of these devices, althoughthere may be additional pathophys-iological mechanisms involved(such as chronic inflammation as-sociated with the stent coating).Beyond the first year after DES im-
257
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others

plantation there is an accumula-tion of very late stent thrombosisevents at around 0.4% to 0.6% perannum.23 The increased event ratesin DES patients were unmasked af-ter 18 months of follow-up in theseminal DES studies.24 Overall, interms of mortality and MI, the late
incidence of stent thrombosis withDES is counteracted by previouslyunrecognized thrombotic eventsand the increased risks of in-stentrestenosis in BMS (Figure 2).25,26 Itis now apparent that BMS resteno-sis is associated with a significantnumber of MIs. Therefore, while late
thrombotic events result in an ex-cess of adverse events with DES, itis important to remember that thebenefit conferred by these devicesis a large reduction in target-vesselrevascularization and that they donot lead to less major clinical events(death or MI).
258
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others
Figure 2. A comparison of the evidence for drug-eluting stents versus bare-metal stents for: (A) Major adverse cardiac events (MACE); (B) In-stent restenosis;(C) Mortality (all-cause); (D) Subacute thrombosis.
Reproduced from reference 26: Melikian N, Wijns W. Drug-eluting stents: a critique. Heart. 2008;94:145-152. Copyright © 2008, BMJ PublishingGroup Ltd & British Cardiovascular Society.
RAVELSIRIUSB-SIRIUSC-SIRIUSFUTURE 1/1SES-SMARTSCANDSTENTDIABETESENDEAVOR II Sirolimus 0.28, P < 0.001
7/12044/53314/1753/503/4912/1295/1639/8044/598
34/118117/52540/17711/508/5840/12848/15929/8088/599
17/1281/3110/11827/22671/66214/15239/5173/2436/21984/560
35/1383/303/5959/270130/6527/3848/5126/2651/227120/567
DES BMS
SCORETAXUS IASPECTTAXUS IITAXUS IVELUTESDELIVERPATENCYTAXUS VITAXUS V Paclitaxel 0.62, P < 0.001
Odds ratio
MACEDES
betterBMSbetter
Heterogeneity P < 0.001 Total 0.46, P < 0.001
0 0.2 1.02 4 7
RAVELSIRIUSB-SIRIUSC-SIRIUSFUTURE 1/1SES-SMARTSCANDSTENTDIABETESENDEAVOR II Sirolimus 0.14, P < 0.001
0/16631/3509/1521/442/4612/1233/1636/8040/298
30/114128/35366/15623/4413/4760/11351/15929/80103/302
26/21094/4966/940/308/10028/26652/66218/13738/2288/21
74/207167/49238/1043/2915/5559/270173/6527/3448/2146/17
Restenosis
DES BMS
TAXUS VITAXUS VSCORETAXUS IASPECTTAXUS IITAXUS IVELUTESDELIVERPATENCY Paclitaxel 0.35, P < 0.001
Odds ratio
DESbetter
BMSbetter
Heterogeneity P < 0.001 Total 0.25, P < 0.001
0 2 1 4
RAVELSIRIUSB-SIRIUSC-SIRIUSFUTURE 1/1SES-SMARTSCANDSTENTDIABETESENDEAVOR II Sirolimus 1.42, P = 0.30
2/1207/5332/1750/501/490/1291/1631/807/598
2/1184/5251/1770/500/582/1281/1592/803/599
5/1280/311/1180/2269/6621/1521/5170/240/2193/560
0/1380/300/592/2708/6520/384/5121/2620/2275/567
DES BMS
SCORETAXUS IASPECTTAXUS IITAXUS IVELUTESDELIVERPATENCYTAXUS VITAXUS V Paclitaxel 0.74, P = 0.37
Odds ratio
Death (all causes)DES
betterBMSbetter
Heterogeneity P = 0.65 Total 1.02, P= 0.92
10 1 60
0/1202/5332/1751/501/491/1291/1633/598
0/1184/5250/1771/500/584/1285/1597/599
13/1280/314/1185/2264/6621/1522/5170/241/2194/560
1/1380/300/590/2705/6521/382/5120/263/2274/567
RAVELSIRIUSB-SIRIUSC-SIRIUSSES-SMARTSCANDSTENTENDEAVOR II Sirolimus 0.47, P = 0.05
Subacute thrombosis
DES BMS
SCORETAXUS IASPECTTAXUS IITAXUS IVELUTESDELIVERPATENCYTAXUS VITAXUS V Paclitaxel 1.24, P = 0.53
Odds ratio
DESbetter
BMSbetter
Heterogeneity P= 0.27 Total 0.62, P= 0.44
0 10 1 60
A B
C D

In view of these findings, most cur-rent clinical practice is based on theclinical scenario. In acute MI (wherethere is increased thrombogenicity),there are still concerns regardinglate stent thrombosis with DES im-plantation. Ongoing randomizedstudies will shed further light onthe use of DES in these patients. Insmaller vessels, longer lesions, andpatients with diabetes mellitus,where the risk of in-stent restenosisis high, and in patients who havealready had an episode of BMS in-stent restenosis, there is a clear ad-vantage of DES. DES are also fre-quently used for treating otherlesions such as LMCA disease, bifur-cation lesions, chronic total occlu-sions, and saphenous vein grafts,despite the lack of availability of ro-bust randomized clinical trial data.27
These lesions are all known to beat high risk of restenosis and it isreasonable to postulate that DESwould lead to significant benefitsfor these patients over BMS.
Several drugs have now been inves-tigated on different stent platformsand/or with different polymer coat-ings (that may have biological ef-fects of their own that are distinctfrom the eluted drug).28 The moststudied drugs to date are sirolimusand paclitaxel. Investigations arecurrently ongoing with these drugsas well as with stents coated withzotarolimus, everolimus, tacrolimusand other novel agents.
At present, the cost-benefit of DESis a hotly contested debate. Thissubject is currently being examinedin the United Kingdom by the Na-tional Institute of Clinical Excel-lence. Evidence continues to accu-mulate that the cost of DES (atpresent prices) may well be in excessof the benefits that are conferred topatients and thus health care sys-tems. DES are most cost-effective forpatients when the risk of restenosis
is highest. This is particularly thecase in those with 2 or 3 risk fac-tors for restenosis, ie, small vessels(<3.0 mm in diameter), long lesions(>20 mm), and in diabetics.29
DOES (OR SHOULD) THE AVAILABILITY OF
DRUG-ELUTING STENTSINFLUENCE THE
DECISION?
The reality of clinical medicine isthat randomized controlled trialscannot provide answers to all of ourclinical dilemmas. There are cir-cumstances where, on the basis ofcurrent evidence and practice guide-lines, CABG is the preferred methodof revascularization. Until there aredata to the contrary, patients withLMCA disease and diabetics withmultivessel disease and left ventric-ular dysfunction should be consid-ered for surgery when it is clinicallyfeasible.
As discussed previously, the majori-ty of studies of patients who wererandomized to CABG or PCI withBMS consistently demonstrate nodifference in outcomes for death ormajor adverse cardiovascular eventsin the medium or long term. How-ever, there is a very clear risk of increased repeat revascularizationprocedures with PCI using BMScompared with CABG.9-15,19
It is apparent that DES will greatlyreduce this complication. We alreadyknow that these devices are highlyeffective at preventing in-stentrestenosis and subsequent target-vessel revascularization on the basisof large-scale multicenter random-ized controlled trials that have en-rolled many thousands of patients.There are already some nonran-domized data to show that thesedevices confer these benefits topatients with multivessel diseasewho are also treatable by CABG.30
Furthermore, as we strive to achievecomplete revascularization for thesepatients, we will be treating longer,more complex lesions in smallervessels and a significant proportionof patients will be diabetics. Theseare the patients who have most togain from DES use. The forthcom-ing randomized studies (SYNTAXand FREEDOM [not acronyms]) willprovide robust scientific evidencethat reflects best medical care aswell as contemporary interventionaland surgical practice. These studieswill help to answer which patientsare best served by either procedure.
DES are clearly needed for patientswith multivessel disease and theiravailability is important when in-terventionalists consider the besttreatment option for their patients.Furthermore, the second-genera-tion of these devices is likely to bemore biocompatible and/or absorb-able. It is likely that further improve-ments in DES technology will furtherreduce the risk of late thromboticevents and improve the benefitsoffered by DES. The availability ofDES is important for our patientsand should influence the decisionregarding the mode of revascular-ization for patients who require thistreatment.
CONCLUSION
In summary, DES are a safe and effective technology. These devicesare effective for reducing in-stentrestenosis and target-vessel revas-cularization after PCI. BMS resteno-sis is not a benign phenomenonand there is a clear need for DESuse in certain patients. This efficacycomes at a small risk of very latestent thrombosis, although prevent-ing events that would otherwise beassociated with BMS offsets thisrisk over the long term. DES do notproduce an excess number of deathsor MIs up to 4 years. These devices
259
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others

260
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others
are a relatively expensive technolo-gy when cost-benefit ratios are ex-amined for universal use duringpercutaneous revascularization pro-cedures. The next generation of DESwill be specifically designed to ob-viate the risk of late thromboticevents and may lead to further ben-efits over BMS if this goal can beachieved.
REFERENCES
1. Feldman DN, Gade CL, Slotwiner AJ, et al.
Comparison of outcomes of percutaneouscoronary interventions in patients of threeage groups (<60, 60 to 80, and >80 years)(from the New York State AngioplastyRegistry).
Am J Cardiol. 2006;98:1334-1339.
2. Boden WE, O'Rourke RA, Teo KK,et al.
Optimal medical therapy with or withoutPCI for stable coronary disease.
N Engl J Med. 2007;356:1503-1516.
3. Hueb W, Soares PR, Gersh BJ, et al.
The medicine, angioplasty, or surgery study(MASS-II): a randomized, controlled clinicaltrial of three therapeutic strategies for mul-tivessel coronary artery disease: one-yearresults.
J Am Coll Cardiol. 2004;43:1743-1751.
4. Gershlick A, Thomas M.
PCI or CABG: which patients and at whatcost?
Heart. 2007;93;1188-1190.
5. Boden WE, O’Rourke RA, Teo KK,et al.
The evolving pattern of symptomatic coro-nary artery disease in the United Statesand Canada: baseline characteristics of theClinical Outcomes Utilizing Revasculariza-tion and Aggressive Drug Evaluation(COURAGE) trial.
Am J Cardiol. 2007;99:208-212.
6. CASS principal investigators andtheir associates.
Coronary Artery Surgery Study (CASS): a randomized trial of coronary artery bypasssurgery. Survival data.
Circulation. 1983;68;939-950.
7. Yusuf S, Zucker D, Passamani E,et al.
Effect of coronary artery bypass graft sur-gery on survival: overview of 10-year resultsfrom randomized trials by the Coronary artery Bypass Graft Surgery Trialists Collab-oration.
Lancet. 1994;344:563-570.
8. Eagle KA, Guyton RA, Davidoff R.
ACC/AHA 2004 guideline update for coro-nary artery bypass surgery: Summary article:A report of the American College of Cardiol-ogy/American Heart Association Task Forceon Practice Guidelines.
J Am Coll Cardiol. 2004;44:1146-1154.
9. BARI Investigators.
Seven-year outcome in the bypass angio-plasty revascularization investigation(BARI) by treatment and diabetic status.
J Am Coll Cardiol. 2000;35:1122-1129.
10. Berger PB, Velianou JL, Vlachos HA, et al.
Survival following coronary angioplastyversus coronary artery bypass surgery inanatomic subsets in which coronary arterybypass surgery improves survival comparedwith medical therapy. Results from theBypass Angioplasty Revascularization Inves-tigation (BARI).
J Am Coll Cardiol. 2001;38:1440-1449.
11. SoS Investigators.
Coronary artery bypass surgery versus per-cutaneous coronary intervention with stentimplantation in patients with multivesselcoronary artery disease (the Stent or Surgerytrial): a randomized controlled trial.
Lancet. 2002;360:965-970.
12. Serruys PW, Ong ATL, van Herwerden LA, et al.
Five-year outcomes after coronary stentingversus bypass surgery for the treatment ofmultivessel disease: the final analysis of theArterial Revascularisation Therapies Study(ARTS) randomised trial.
J Am Coll Cardiol. 2005;46:575-581.
13. Rodriquez AE, Baldi J,Fernandez Pereira C, et al.
Five-year follow-up of the Argentine ran-domized trial of coronary angioplasty withstenting versus coronary bypass surgery inpatients with multivessel disease (ERACI II).
J Am Coll Cardiol. 2005;46:582-588.
14. Hueb W, Lopes NH, Gersh BJ, et al.
Five year follow up of the Medicine, Angio-plasty, or Surgery Study (MASS II): a ran-domised controlled clinical trial of 3 thera-peutic strategies for multivessel coronaryartery disease.
Circulation. 2007;115:1082-1089.
15. Bravata DM, Gienger AL,McDonald KM, et al.
Systematic review: the comparative effective-ness of percutaneous coronary interventionsand coronary artery bypass graft surgery.
Ann Intern Med. 2007;147:703-716.
16. Anderson JL, Adams CD,Antmann EM, et al.
ACC/AHA 2007 Guidelines for the Manage-ment of Patients With Unstable Angina/Non_ST-Elevation Myocardial Infarction:Executive Summary: A Report of the Amer-ican College of Cardiology/American HeartAssociation Task Force on Practice Guide-lines (Writing Committee to Revise the 2002Guidelines for the Management of PatientsWith Unstable Angina/Non_ST-ElevationMyocardial Infarction): Developed in Col-laboration with the American College ofEmergency Physicians, the Society for Car-diovascular Angiography and Interventions,and the Society of Thoracic Surgeons: En-dorsed by the American Association of Car-diovascular and Pulmonary Rehabilitationand the Society for Academic EmergencyMedicine.
Circulation. 2007;116;803-877.
17. Bavry AA, Kumbhani DJ, Rassi AN,et al.
Benefit of early invasive therapy in acutecoronary syndromes: a meta-analysis ofcontemporary randomized clinical trials.
J Am Coll Cardiol. 2006;48:1319-1325.
18. Morrison DA, Sethi G, Sacks J,et al.
Percutaneous coronary intervention versuscoronary artery bypass graft surgery for pa-tients with medically refractory myocardialischemia and risk factors for adverse out-

261
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Medical therapy, surgery, or PCI and drug-eluting stent availability - Adgey and others
comes with bypass: a multicenter, random-ized trial. Investigators of the Departmentof Veterans Affairs Cooperative Study #385,the Angina With Extremely Serious Opera-tive Mortality Evaluation (AWESOME).
J Am Coll Cardiol. 2001;38:143-149.
19. Serruys PW, Unger F, Sousa JE,et al.
Comparison of coronary artery bypass sur-gery and stenting for the treatment of mul-tivessel disease.
N Engl J Med. 2001;344:1117-1124.
20. National Institute for Health andClinical Excellence.
Ischaemic heart disease—coronary arterystents (review): appraisal consultation doc-ument. Drug-eluting stents for the treatmentof coronary artery disease (part review ofNICE technology appraisal guidance 71,2007).
www.nice.org.uk. Accessed September9, 2008.
21. Fajadet J, Morice MC, Bode C, et al.
Maintenance of long-term clinical benefitwith sirolimus-eluting coronary stents: three-year results of the RAVEL trial.
Circulation. 2005;111:1040-1044.
22. Weisz G, Leon MB, Holmes DR Jr,et al.
Two-year outcomes after sirolimus-elutingstent implantation: results from the Sirolimus-Eluting Stent in de Novo Native CoronaryLesions (SIRIUS) trial.
J Am Coll Cardiol. 2006;47:1350-1355.
23. Serruys PW, Daemen J.
Late stent thrombosis: a nuisance in bothbare metal and drug-eluting stents.
Circulation. 2007;115;1433-1439.
24. Lasala JM, Stone GW, Dawkins KD,et al.
An overview of the TAXUS Express, pacli-taxel-eluting stent clinical trial program.
J Interv Cardiol. 2006;19:422-431.
25. Stettler C, Wandel S, Allemann S,et al.
Outcomes associated with drug-eluting andbare-metal stents: a collaborative networkmeta-analysis.
Lancet. 2007;370;937-948.
26. Melikian N, Wijns W.
Drug-eluting stents: a critique.
Heart. 2008;94:145-152.
27. Colombo A, Chieffo A.
Drug-Eluting Stent Update 2007. Part III:Technique and unapproved/unsettled indica-tions (left main, bifurcations, chronic totalocclusions, small vessels and long lesions,saphenous vein grafts, acute myocardial in-farctions, and multivessel disease).
Circulation. 2007;116;1424-1432.
28. Daemen J, Serruys PW.
Drug-Eluting Stent Update 2007: Part I: A survey of current and future generationdrug-eluting stents: meaningful advancesor more of the same?
Circulation. 2007;116;316-328.
29. Tu JV, Bowen J, Chiu M, et al.
Effectiveness and safety of drug-eluting stentsin Ontario.
N Engl J Med. 2007;357:1393-1402.
30. Serruys PW, Ong ATL, Morice MC,et al.
Arterial Revascularization Therapies Studypart II—Sirolimus-eluting stents for thetreatment of patients with multivessel de novocoronary artery lesions.
EuroInterv. 2005;1:147-156.

he drugs on drug-elutingstents (DES) are supposed tolimit the “overshoot” woundhealing process (smooth mus-
cle cell proliferation and endothe-lialization) after balloon injury tothe coronary artery vessel wall, andthereby to prevent restenosis. Thedelayed healing process after DESexposes the stent struts for a longerperiod of time to circulating bloodwith the danger of inducing throm-botic processes in these stentedsegments. Therefore, dual antipla-telet drug therapy has been intro-duced and shown to be beneficialto prevent early stent thrombosis.Accordingly, dual antiplatelet ther-apy was proposed by label pre-scription from 1 month after bare-
metal stents (BMS) to 3 months af-ter sirolimus-eluting and 6 monthsafter paclitaxel-eluting stents.More recently, it was recognizedthat this healing process may takeeven longer than 6 months and thatthere is inhomogeneity of this heal-ing process even within a singlepatient or vessel.1 This is the basisfor late or very late (after 6 to 12months) stent thrombosis. TheBAsel Stent Kosten-EffektivitätsTrial–LAte Thrombotic Events(BASKET-LATE) study showed forthe first time in a randomized pros-pective observational trial that theselate stent thromboses are clinicallyrelevant after DES implantation, al-though rare and significantly morefrequent than after BMS implanta-tion.2 Between month 7 and 18 afterstenting, they led to 4.9% of throm-botic events versus only 1.3% afterBMS (P=0.01). Importantly, latestent thrombosis presented in 88%as death or myocardial infarction(MI), indicating serious clinical con-sequences of this late complication(Figure 1).
In BASKET-LATE, these late stentthrombosis events occurred afterstopping clopidogrel, and thereforethe question arose whether evenlonger dual antiplatelet therapymay prevent these events. Unfortu-nately, no randomized controlledtrial has been performed so far to
Drug-eluting stents (DES) reducerestenosis, but carry a small riskof late stent thrombosis. Dual an-tiplatelet therapy is the treatmentof choice after DES implantation.Early discontinuation of this thera-py, eg, in patients in need of non-cardiac surgery, is an importantrisk factor for stent thrombosis witha high risk of death or myocardialinfarction. Therefore, such surgeryshould be delayed for up to 12months. If it cannot be, one has tobalance risks and benefits of con-tinued antiplatelet therapy. Gener-ally, the risk of stopping dual anti-platelet therapy in the perioperativeperiod appears higher than to per-form surgery on continued therapy,except for brain surgery. We discussevidence-based data that go intothis risk-benefit analysis and how tomanage these situations practically.
Antiplatelet therapy: what to do if the patient with a drug-eluting stent needs elective noncardiac surgery?Matthias Pfisterer*, MD, FACC, FESC, FAHA; Michael J. Zellweger*, MD; Miodrag Filipovic†, MD; Fabian Nietlispach*, MD*Division of Cardiology and †Anesthesiology - University Hospital Basel - Basel - SWITZERLAND
T
Keywords: drug-eluting stent; antiplatelettherapy; noncardiac surgery; stent thrombo-sis; myocardial infarctionAddress for correspondence:Matthias Pfisterer, MD, Professor ofCardiology, Head, Department ofCardiology, University Hospital, CH-4031Basel, Switzerland(e-mail: [email protected])Dialogues Cardiovasc Med. 2008;13:262-266
262Copyright © 2008 LLS SAS. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
SELECTED ABBREVIATIONSAND ACRONYMS
BASKET- BAsel Stent Kosten- LATE Effektivitäts Trial–
LAte Thrombotic Events
BMS bare-metal stent
CURE Clopidogrel in Unstableangina to prevent Re-current Events [trial]
DES drug-eluting stents
MI myocardial infarction
PREMIER PREterax in albuminu- ria rEgRession

answer this question. An observa-tional registry study from the DukeClinical Research Institute suggest-ed that there was a better 2-yearoutcome if DES patients were stillon dual antiplatelet therapy after12 months.3 This led to recommen-dations by the Food and Drug Ad-ministration and new EuropeanSociety of Cardiology guidelines to
use dual antiplatelet therapy afterDES implantation for 12 months in patients not at increased risk ofbleeding. The notion that dual an-tiplatelet therapy may in fact pre-vent these late stent thrombosisevents is, however, questioned byobservations from two large pros-pective registry findings showingthat late stent thrombosis occurs inabout 25% of patients despite dualantiplatelet therapy,4 and that inmultivariate analysis dual antipla-telet therapy cessation is a predictorof such events only within the first6 months, but not thereafter.5 Still,most interventional cardiologistsseem to follow at present the recom-mendation to use dual antiplatelettherapy at least for 12 months.
WHAT IF ELECTIVE NONCARDIAC SURGERY
IS NEEDED?
There is no question that emer-gency surgery, if indicated, has to beperformed in patients with DES onthe current treatment, which willbe dual antiplatelet therapy withinthe first 12 months after stenting.
However, if elective surgery is pro-posed as is the case in at least 5%of patients for prostate surgery, hipreplacement, etc, the question willbe whether dual antiplatelet therapycan/should be stopped prematurelyor whether surgery can/should bepostponed and how long. Thismeans that the risk of bleeding dur-ing surgery on dual antiplatelettherapy has to be balanced againstthe risk of stent thrombosis follow-ing premature discontinuation ofdual antiplatelet therapy. The Amer-ican College of Cardiologists/Amer-ican Heart Association (ACC/AHA)guidelines suggest, based on ex-pert opinions, postponing surgeryfor at least 12 months in patientswith DES.6
BLEEDING RISK IN NONCARDIAC SURGERY ON
ANTIPLATELET THERAPY
Unfortunately, there are no largescale randomized controlled trialsto asses the bleeding risk in theseprocedures with and without anti-platelet therapy. The AntithromboticTrialists Collaboration determineda rate of spontaneous bleeding ondual antiplatelet therapy of 0.7% to1.13% (relative risk increase of 37%)compared with aspirin alone7 andthis was 2.7% to 3.7% (27% increasein relative risk) in the Clopidogrelin Unstable angina to prevent Re-current Events (CURE) trial.8 A largemeta-analysis of more than 400studies assessing the impact of as-pirin alone on preoperative bloodloss showed an increased hemor-rhagic risk of aspirin by a factor of1.5, however, without increases insurgical morbidity or mortality.9
Therefore, it seems documentedthat antiplatelet therapy does in-crease perioperative surgical bleed-ing by at least 50%, with, however,mostly minor bleedings, but thatsurgical outcomes, morbidity, andmortality are not significantlychanged, except for intracranialsurgery.
RISK OF WITHDRAWAL OFANTIPLATELET THERAPY
IN DES PATIENTS
In order to avoid excessive periop-erative bleeding, surgeons and anes-thesiologists usually ask for with-drawal of antiplatelet therapy beforesurgery. However, this is associatedwith several risks by itself: there isa certain rebound effect, even afterstopping aspirin, and aspirin with-drawal was associated with a 3 timeshigher cardiac complication rate ina meta-analysis of 50 279 second-ary prevention patients (odds ratio[OR] 3.14; P=0.0001).10 This risk washigher (OR 89.8) in patients after
263
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting stents and noncardiac surgery - Pfisterer and others
Figure 1. Early (within the initial 6 months) and late (months 7 to 18) cardiac death/myocardialinfarction (MI) in drug-eluting stent (DES)-treated patients versus bare-metal stent (BMS)-treatedpatients. There was a significant benefit in these events after DES vs BMS treatment in the initial6 months, but the contrary was true in the following 12 months.
Modified from reference 2: Pfisterer M, Brunner-La Rocca HP, Buser PT, et al; BASKET-LATEInvestigators. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-elutingstents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48:2584-2591. Copyright © 2006, Elsevier Biomedical.
0.00
0.02
0.04
0.06
0.08
Follow-up (months)
Months 0-6Dual antiplatelet therapy
Months 7-18Aspirin only
Death
/Nonfa
tal M
I
BMS
DES
P = 0.13
BMS
DES
P = 0.02
0 2 4 6 8 10 12 14 16 18

264
stenting and the delay betweenstopping aspirin and these throm-botic events was 10 to 14 days.9,10
In the PREterax in albuMInuriarEgRession (PREMIER) registry,premature stopping of clopidogrelwas associated with a 9-fold in-creased mortality within 1 year,11 in-dicating the high mortality in suchpatients. This increased bleedingrisk is also seen in coronary arterybypass grafting on dual antiplatelettherapy.12
After stent implantation, the risk ofantiplatelet therapy discontinuationseems to be different early, ie, with-in the first 6 (to 12) months, andthereafter. There are numerous stud-ies documenting the catastrophiceffect of early stopping of clopido-grel or even dual antiplatelet ther-apy.12,13 Independent predictors ofearly stent thrombosis (ie, withinthe initial 6 to 12 month after stent-ing) were identified as small vesselstenting, stenting of bifurcation le-sions, patients with diabetes or renal failure, a suboptimal angio-graphic result, and early cessationof dual antiplatelet therapy.14-19 Incontrast, the relation between dualantiplatelet therapy and late or verylate stent thrombosis seems lessclear after 6 to 12 months. Stentthrombosis and related clinicalevents may occur during this latephase despite continued antiplatelettherapy. In addition, no clusteringof the occurrence of stent thrombo-sis events was noted after stoppingclopidogrel, neither in BASKET-LATE2 nor in the Berne-Rotterdamregistry.4 Stopping clopidogrel wasno predictor of stent thrombosisafter 6 months in another Italian-German study.5 Acute coronarysyndrome seems to be the only in-dependent predictor of stent throm-bosis after 6 to 12 months.2,4,5 Thus,whereas there is strong evidencefor the danger of stopping dual an-tiplatelet therapy during the initial
6 months after DES placement, thisis much less clear and even ques-tioned after (6 to) 12 months. Thisled to a ACC/AHA Task Force state-ment warning not to stop dual an-tiplatelet therapy prematurely.20
HOW SHOULD DES PATIENTS IN NEED
OF NONCARDIAC SURGERY BE MANAGED?
In front of a patient with a DES inneed of noncardiac surgery, the firstquestion will always be whethersurgery cannot be delayed up to af-ter the initial 6—or preferably 12months—after DES implantation,when the risk of stent thrombosis islower. If that is possible, then stop-ping clopidogrel after 12 months isan option and surgery may be per-formed on aspirin alone. Still, therisk for late stent thrombosis re-mains and exposes the patient to a somewhat higher risk of cardiacevents compared with the generalpopulation.21 If postponing surgeryis not possible, one has to balancethe risks of surgical bleedings ondual antiplatelet therapy againstthose of stent thrombosis after pre-mature stopping of dual antiplatelettherapy. In view of the data show-ing that surgical bleeding rates areincreased by at least 50% withoutsignificantly altering overall surgicaloutcomes and the possibility ofmanaging perioperative bleedingcomplications by transfusions ofred blood cells or fresh thrombo-cytes on the one hand, and the cat-astrophic clinical outcomes of pe-rioperative stent thrombosis withup to greater than 80% death or MIrisk, which can only partly be man-aged by risky coronary reinterven-tions on the other hand, the recom-mendation has to be to carry outsurgery on continued dual antiplate-let therapy. In other words, the risksof stopping dual antiplatelet therapyin the perioperative period appear
generally higher than to performsurgery on continued therapy. Tak-ing into account the prothromboticenvironment during or after surgery,the current ACC/AHA Guidelineseven suggest continuing clopidogrelperioperatively beyond 1 year inhigh-risk patients (eg, patients withprevious stent thrombosis, afterleft main coronary artery stenting,after multivessel stenting, afterstenting of the last remaining ves-sel).6 However, this benefit-risk bal-ance is different for brain surgeryor surgery close to the spinal cord;here it may be mandatory to stopantiplatelet therapy.
Obviously, surgery on dual antiplate-let therapy has to be planned welland performed by a skilled surgical,anesthesiological, and intensivecare team aware of possible bleed-ing complications and how to man-age them. This means, in the ab-sence of antidotes to antiplateletdrugs, that fresh thrombocytes haveto be available immediately to stopbleeding if necessary. However, be-cause this treatment carries a riskof side effects per se, fibrinogensubstitution may be considered asan alternative. All patients withcoronary artery disease being oper-ated on are at increased surgicalrisk and this is true despite previ-ous successful revascularization.22
In fact, the value of preoperativerevascularization as a general rulehas been questioned and is notgenerally recommended.23 There-fore, these patients need specialelectrocardiographic and cardiacmonitoring and evidence of tran-sient or persistent perioperative is-chemia has to be taken seriously,with immediate consultation with acardiologist. This implies that suchsurgery is performed most safely inhospitals with interventional car-diac facilities. General anesthesia,compared with regional anesthesia,leads to an even more prothrom-
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting stents and noncardiac surgery - Pfisterer and others

botic state24 and thereby enhancesthe risk of coronary complications.However, spinal or epidural anes-thesia is generally considered to becontraindicated in the presence ofdual antiplatelet therapy. If dual an-tiplatelet therapy had to be stoppedas in neurocranial surgery, it shouldbe reinstated as quickly as possi-ble after surgery. Unfortunately, he-parins will not prevent stent throm-bosis from occurring and there areno data showing that glycoproteinIIb/IIIa inhibitors may serve periop-eratively to “bridge” a critical phasewithout oral antiplatelet drugs.20
REFERENCES
1. Finn AV, Joner M, Nakazawa G,et al.
Pathological correlates of late drug-elutingstent thrombosis: strut coverage as a markerof endothelialization.
Circulation. 2007;115:2435-2441.
2. Pfisterer M, Brunner-La Rocca HP,Buser PT, et al; BASKET-LATE Inves-tigators.
Late clinical events after clopidogrel discon-tinuation may limit the benefit of drug-elut-ing stents: an observational study of drug-eluting versus bare-metal stents.
J Am Coll Cardiol. 2006;48:2584-2591.
3. Eisenstein EL, Anstrom KJ, Kong DF, et al.
Clopidogrel use and long-term clinical out-comes after drug-eluting stent implantation.
JAMA. 2007;297:159-168.
4. Daemen J, Wenaweser P, Tsuchida K, et al.
Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-elutingstents in routine clinical practice: data froma large two-institutional cohort study.
Lancet. 2007;369:667-678.
5. Airoldi F, Colombo A, Morici N,et al.
Incidence and predictors of drug-eluting stentthrombosis during and after discontinuationof thienopyridine treatment.
Circulation. 2007;116:745-754.
6. Fleisher LA, Beckman JA, Brown KA, et al.
ACC/AHA 2007 guidelines on perioperativecardiovascular evaluation and care for non-cardiac surgery: a report of the AmericanCollege of Cardiology/American Heart As-sociation Task Force on Practice Guidelines(Writing Committee to Revise the 2002Guidelines on Perioperative CardiovascularEvaluation for Noncardiac Surgery): devel-oped in collaboration with the AmericanSociety of Echocardiography, American So-ciety of Nuclear Cardiology, Heart RhythmSociety, Society of Cardiovascular Anesthe-siologists, Society for Cardiovascular An-giography and Interventions, Society forVascular Medicine and Biology, and Societyfor Vascular Surgery.
Circulation. 2007;116:e418-e499.
7. Antithrombotic Trialists’ Collabo-ration.
Collaborative meta-analysis of randomisedtrials of antiplatelet therapy for preventionof death, myocardial infarction, and strokein high risk patients.
BMJ. 2002;324:71-86.
8. Yusuf S, Zhao F, Mehta SR,Chrolavicius S, Tognoni G, Fox KK.
Effects of clopidogrel in addition to aspirinin patients with acute coronary syndromeswithout ST-segment elevation.
N Engl J Med. 2001;345:494-502.
9. Burger W, Chemnitius JM, Kneissl GD, Rucker G.
Low-dose aspirin for secondary cardiovas-cular prevention—cardiovascular risks afterits perioperative withdrawal versus bleedingrisks with its continuation—review andmeta-analysis.
J Intern Med. 2005;257:399-414.
10. Biondi-Zoccai GG, Lotrionte M,Agostoni P, et al.
A systematic review and meta-analysis onthe hazards of discontinuing or not adheringto aspirin among 50,279 patients at risk forcoronary artery disease.
Eur Heart J. 2006;27:2667-2674.
11. Spertus JA, Kettelkamp R, Vance C, et al.
Prevalence, predictors, and outcomes of pre-mature discontinuation of thienopyridinetherapy after drug-eluting stent placement:results from the PREMIER registry.
Circulation. 2006;113:2803-2809.
12. Purkayastha S, Athanasiou T,Malinovski V, et al.
Does clopidogrel affect outcome after coro-nary artery bypass grafting? A meta-analysis.
Heart. 2006;92:531-532.
13. Iakovou I, Schmidt T, Bonizzoni E,et al.
Incidence, predictors, and outcome ofthrombosis after successful implantation ofdrug-eluting stents.
JAMA. 2005;293:2126-2130.
14. Cheneau E, Leborgne L, Mintz GS,et al.
Predictors of subacute stent thrombosis: results of a systematic intravascular ultra-sound study.
Circulation. 2003;108:43-47.
15. Cutlip DE, Baim DS, Ho KK, et al.
Stent thrombosis in the modern era: a pooledanalysis of multicenter coronary stent clini-cal trials.
Circulation. 2001;103:1967-1971.
16. Fujii K, Carlier SG, Mintz GS, et al.
Stent underexpansion and residual referencesegment stenosis are related to stent throm-bosis after sirolimus-eluting stent implanta-tion: an intravascular ultrasound study.
J Am Coll Cardiol. 2005;45:995-998.
17. Hausleiter J, Kastrati A, Mehilli J,et al.
Predictive factors for early cardiac eventsand angiographic restenosis after coronarystent placement in small coronary arteries.
J Am Coll Cardiol. 2002;40:882-889.
18. Ong AT, McFadden EP, Regar E,de Jaegere PP, van Domburg RT,Serruys PW
Late angiographic stent thrombosis (LAST)events with drug-eluting stents.
J Am Coll Cardiol. 2005;45:2088-2092.
265
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting stents and noncardiac surgery - Pfisterer and others

19. McFadden EP, Stabile E, Regar E,et al.
Late thrombosis in drug-eluting coronarystents after discontinuation of antiplatelettherapy.
Lancet. 2004;364:1519-1521.
20. Grines CL, Bonow RO, Casey DE Jr, et al.
Prevention of premature discontinuation ofdual antiplatelet therapy in patients withcoronary artery stents: a science advisoryfrom the American Heart Association, Amer-ican College of Cardiology, Society for Car-diovascular Angiography and Interventions,American College of Surgeons, and Amer-ican Dental Association, with representationfrom the American College of Physicians.
Circulation. 2007;115:813-818.
21. Schouten O, van Domburg RT,Bax JJ, et al.
Noncardiac surgery after coronary stenting:early surgery and interruption of antiplatelettherapy are associated with an increase inmajor adverse cardiac events.
J Am Coll Cardiol. 2007;49:122-124.
22. Back MR, Stordahl N,Cuthbertson D, Johnson BL,Bandyk DF.
Limitations in the cardiac risk reductionprovided by coronary revascularization priorto elective vascular surgery.
J Vasc Surg. 2002;36:526-533.
23. Eagle KA, Berger PB, Calkins H,et al.
ACC/AHA guideline update for perioperativecardiovascular evaluation for noncardiacsurgery—executive summary: a report of theAmerican College of Cardiology/AmericanHeart Association Task Force on PracticeGuidelines (Committee to Update the 1996Guidelines on Perioperative CardiovascularEvaluation for Noncardiac Surgery).
J Am Coll Cardiol. 2002;39:542-553.
24. Rosenfeld BA, Beattie C,Christopherson R, et al; PerioperativeIschemia Randomized AnesthesiaTrial Study Group.
The effects of different anesthetic regimenson fibrinolysis and the development of post-operative arterial thrombosis.
Anesthesiology. 1993;79:435-443.
266
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Drug-eluting stents and noncardiac surgery - Pfisterer and others

hen coronary angio-plasty was introducedin the late 1970s, itushered in the mod-
ern age of cardiology. However, thelong-term success of balloon an-gioplasty was hindered by high ratesof reocclusion of treated vessels. Theintroduction of bare-metal stents—essentially metal scaffolds used toprevent reocclusion in arteries aftersuccessful angioplasty—was de-scribed as the golden age of inter-ventional cardiology. However, theAchilles heel of bare-metal stentswas the high rate of in-stent throm-bosis, and it was not until the im-portance of dual antiplatelet therapywith aspirin and thienopyridines(such as clopidogrel or ticlopidine)was discovered that coronary stentswere widely adopted. But this dis-covery did not totally resolve con-cerns about high restenosis rates,which could only be overcome withrestenting or brachytherapy (andeven then with limited success).
When the first drug-eluting stentwas approved in the United States bythe Food and Drug Administration(FDA), cardiologists heralded thenew technology as a breakthroughfor the treatment of coronary arterydisease.1,2 Drug-eluting stents wererapidly adopted into clinical prac-tice (Figure 1, page 268), and it wasestimated at one time that morethan 80% of coronary stents used inthe United States were drug-elutingstents.3 However, concerns among
researchers about late stent throm-bosis leading to myocardial infarc-tion and possible cardiovascular-related death began to make theheadlines.4 Researchers were alsoconcerned about the widespreadoff-label use of drug-eluting stents(ie, for scenarios that had yet to beformally tested or approved by theFDA).5 Compounding these concernswere longer-term medical data sug-gesting that drug-eluting stentshad no significant impact on theoccurrence of myocardial infarctionand death compared with alterna-tive medical or surgical therapies.6
THE FDA APPROVALPROCESS
The modern FDA was conceived bythe Federal Food, Drug, and Cos-metic Act of 1938, a Congressionalmandate prompted by several deathsrelated to sulfanilamide that hadbeen compounded as an elixir us-ing diethylene glycol. This lethalcombination was brought to marketwithout clinical testing, and the in-cident exposed deficiencies in theFood and Drugs Act of 1906, whichdid not require safety studies fornew drugs.7 The 1938 legislation is largely credited with the currentoperating framework of the FDA. Itwas the first legislation to requiredrug labeling with adequate direc-tions for safe use. The act mandatedpremarket approval of all new drugsand required manufacturers todemonstrate safety to the FDA be-
Medical devices are complex thera-peutics that pose unique regulatory,ethical, legal, and financial chal-lenges. Drug-eluting stents wereheralded initially as a breakthroughin the treatment of coronary arterydisease. However, later revelationsabout the safety and efficacy ofdrug-eluting stents would high-light challenges in the regulatoryapproval of medical devices. In thispaper, we discuss a few key issuesthat arose from debates about drug-eluting stents: Are trials for medicaldevices adequately designed to ex-amine long-term safety? What arethe ethics of phase 1 research formedical devices when long-termcomplications are unknown? Whatare the intellectual property rightsissues for medical technology?How do payment systems createincentives that encourage overuseof medical devices?
What are the regulatory and economic challengesposed by drug-eluting stents? Bimal R. Shah*, MD; Kevin A. Schulman*†, MD*Duke Clinical Research Institute - Duke University School of Medicine - Durham, NC - USA†Health Sector Management Program - The Fuqua School of Business - Duke University - Durham, NC - USA
W
Keywords: drug-eluting stent; ethics; research; health care economics and organizations; FDAAddress for correspondence:Kevin A. Schulman, MD, Center forClinical and Genetic Economics, Duke Clinical Research Institute, PO Box 17969, Durham, NC 27715, USA; (e-mail: [email protected] Cardiovasc Med. 2008;13:267-272
267Copyright © 2008 LLS SAS. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008

fore selling their drug products.However, the act did not includeprovisions for the oversight of med-ical devices.8
A series of medical device injuriesin the late 1960s and early 1970s,and a 1970 report from the NationalHeart and Lung Institute document-ing over 10 000 injuries and 731deaths linked to medical devices,once again prompted Congress toact. The Medical Device Amend-
ments of 1976 gave the FDA the au-thority to regulate medical devicesbased on the complexity and per-ceived risk of the device. The legis-lation was later criticized for givingthe FDA little power to require man-ufacturers to report failures or ad-verse events. This power to man-date postmarket surveillance andreporting of device-related injuriesand deaths was granted to the FDAby the Safe Medical Devices Act of1990 and the Medical Device Amend-
ments of 1992.9 With the enactmentof these provisions, 224 197 device-related injuries, malfunctions, anddeaths were reported in 2006 alone.10
DEVICE APPROVAL IN THE EUROPEAN UNION
The European Union has a differentregulatory approval model than theUnited States, but the structure ofclinical research for medical devicesis similar in the two markets. To
obtain approval to market and sella device in the European Unionwithout meeting the testing require-ments of each member state, devicemakers must receive a ConformitéEuropéenne (CE) mark certifying thatthe product meets European Unionhealth, safety, and environmentalrequirements. CEs are issued byindependent, private commercialentities called “notified bodies,”which are regulated and audited byrelevant regulatory bodies in the
member states. Device companiescan choose from more than 50 noti-fied bodies in the European Union,resulting in competition among thenotified bodies, which are viewedas less bureaucratic and more nim-ble than the FDA. Nevertheless, be-cause of the variety among notifiedbodies, device approval can be vari-able and fragmented and can resultin the approval of devices and drugsthat have not received approval inthe United States. Unlike the UnitedStates, where a manufacturer mustprove to the FDA both safety andefficacy, the European Union re-quires only that the manufacturerdemonstrate that the device is safeand operates as the manufacturerintended.11
REGULATORY APPROVALFOR DRUG-ELUTING
STENTS
Cordis Corporation’s Cypher siro-limus-eluting stent received a CEmark in April 2002 for “treatment of de novo coronary artery lesions(less than or equal to 30 mm inlength) in native coronary arterieswith reference diameters rangingfrom 2.25 to 5.0 mm” based ondata from 238 patients enrolled inEurope and Latin America.12 InApril 2003, the FDA approved thesame device for “improving coronaryluminal diameter in patients withsymptomatic ischemic disease dueto discrete de novo lesions of thelength �30 mm in native coronaryarteries with a reference vessel diam-eter of �2.5 mm to �3.5 mm. Long-term outcome (beyond 12 months)for this permanent implant is un-known at present.” The FDA letter ofapproval also required clinical out-comes through 5 years post-proce-dure on at least 80% of patients inthe clinical trial used for approvalof the device, plus information on2000 patients with the device im-planted after the approval.13
268
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents? - Shah and Schulman
Figure 1. Estimated number of discharges in the United States from 1993 through 2005 for percuta-neous transluminal coronary angioplasty (ICD-9-CM codes 36.01, 36.02, and 36.05), insertion ofbare-metal stent (36.06), and insertion of drug-eluting stent (36.07).Note: Before October 2002, ICD-9-CM code 36.06 applied to insertion of any coronary stent. Therefore,there is likely some overlap in discharge estimates for bare-metal stents and drug-eluting stents in 2002.
Data Source: National Inpatient Sample, Healthcare Cost and Utilization Project (HCUP), Agencyfor Healthcare Research and Quality, US Department of Health and Human Services.
0
100 000
200 000
300 000
400 000
500 000
600 000
700 000
800 000
900 000
Year
Percutaneous transluminal coronary angioplastyInsertion of bare-metal stentInsertion of drug-eluting stent
Dis
charg
es
(weig
hte
d),
No.
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005

Three months after the approval,Cordis issued a letter to informhealth professionals of the possibil-ity stent thrombosis could occurshortly after implantation and rec-ommended that professionalschoose the appropriate stent size,appropriate patients, correct anti-platelet regimen, and proper tech-niques for stent deployment.14 InOctober 2003, the FDA released apreliminary public health notifica-tion of more than 290 reports ofsubacute stent thrombosis associ-ated with the Cypher stent. Morethan 60 reports were associatedwith death, and the remaining re-ports were associated with injuriesrequiring medical or surgical inter-vention. The FDA acknowledgedthat it did not have sufficient datato establish rates for these events,to compare drug-eluting stents withbare-metal stents, or to describe adefinable cause for the events.15 Bythis time, Cordis had distributedmore than 450 000 Cypher stentsworldwide. Despite the warningsignals, the FDA approved BostonScientific’s Taxus paclitaxel-elutingstent in March 2004.16
In the spring of 2006, conflictingstudy results presented at a meet-ing of the European Society of Car-diology fueled concerns about thesafety of drug-eluting stents.4,17 Toaddress these issues, the FDA’sCirculatory System Devices AdvisoryPanel convened a group of regula-tors, research physicians, and pa-tient and industry representativesin December 2006. At the end of a2-day conference, the panel con-cluded that drug-eluting stents wereassociated with a decrease in theneed for repeat cardiac catheteri-zation compared with bare-metalstents, but noted an increase in thefrequency of stent thrombosis, themagnitude of which was unknown,but was clearly higher with off-labeluse. The panel concluded that dual
antiplatelet therapy be continuedfor at least 1 year based in part onrecent data on this issue, but theexact duration was still unknown.18
REGULATORY ISSUES
The approval of drug-eluting stentswas predicated on the premise ofefficacy (reduced total revascular-ization rates) and safety (no stentthrombosis or deaths) in both theUnited States and the EuropeanUnion. The approval process appli-cation for the Cypher stent involvedapproximately 1000 patients (withfewer for the European Union ap-proval) in two studies with narrowlydefined inclusion criteria. However,at the time these trials were con-ducted, the populations of patientsreceiving stents were much broad-er than what the approved labelingincluded and, more importantly, ex-cluded.19 Although the participantshad been randomly assigned, thesmall number of carefully selectedpatients resulted in approvals in-formed by underpowered studieswith low event rates, essentiallymissing any ability to detect rare,serious complications such as stentthrombosis. By the time safety sig-nals began to emerge, over a halfmillion of the devices had been im-planted worldwide.
In its approval letter for the firstdrug-eluting stent, the FDA high-lighted areas of limited data for thenew technology: more complex le-sions and patients, the duration ofclopidogrel, and the impact on hardend points. These deficiencies in theapproval data would later emergeas the areas of concern regardingthe safety and efficacy of drug-elut-ing stents. The FDA correctly iden-tified the issues at the outset, butneither the United States nor Euro-pean Union regulatory authoritiesrequired the manufacturers to pro-duce additional data or align their
postmarket surveillance to mitigatethe concerns as the stents enteredbroader clinical use. When the con-cerns became widespread, the agen-cies were forced to react to anecdot-al reports and pooled studies withinsufficient primary data.
The medical device industry focuseson incremental and continuous im-provement processes on a smallerrange of products with perceivedlower risk with each iteration. Tobetter gauge safety in the approvalprocess, the challenge for medicaldevice manufacturers is to balancelarger trials and longer follow-upwith the costs and burdens of doingso. Balancing patient safety withexpected market returns, the $220billion global medical device marketcould be expected to invest in morerigorous trials if the current reim-bursement incentive structure ispreserved.20 Furthermore, devicemanufacturers could test iterativeor even new products on more en-riched patient populations to bettersimulate real-world clinical use andoutcomes. Such a requirementwould allow for better assessmentof product safety and efficacy andwould allow regulatory agencies to make a more informed approvaldecisions.
OFF-LABEL USEAND POSTMARKET
SURVEILLANCE
Regulators in the United States andthe European Union do not explic-itly regulate physician behavior orapprove the procedures by whichdevices are implanted. Furthermore,even when a physician uses a de-vice off-label, the manufacturer isabsolved of product liability.21 As aresult, once a therapy is approved,it can be used in clinical scenariosthat fall outside the guidelines forwhich it was approved with almostno liability to the manufacturer,
269
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents? - Shah and Schulman

meanwhile directly increasing themarket for which the product willbe used. The large percentage ofoff-label use of drug-eluting stentsalarmed many, with some estimatesas high as 80% at the peak of drug-eluting stent use in the UnitedStates.22 For a therapy with well-defined labeling, the rapidity andnature by which these devices weretaken up by the interventional car-diology community raises questionsabout how clinical trial data aredisseminated and assimilated intobroader clinical practice and therole of marketing practices of devicemanufacturers. With such a largeproportion of patients receivingdrug-eluting stents off-label, findinga comparator group to further as-sess safety and efficacy in clinical-ly enriched populations becomesmore difficult. Also, the increasedoff-label use of any medical therapymakes it difficult to determine ifadverse events are inherent to thetherapy or due to inappropriate usein inappropriate populations.23
Postmarket surveillance registriesmandated by regulators can be usedto monitor the safety of an approvedtherapy, particularly in populationsand clinical scenarios not represent-ed in the original clinical studies.However, experience with drug-elut-ing stents exemplifies the rapidityof medical technology developmentand the limitations of the currentregulatory framework to adequatelymonitor both existing and newtechnologies and their iterations in clinical practice. Currently, post-market surveillance is conductedusing some combination of man-dated postmarket surveillance reg-istries, national registries, claimsdata, and regulatory reporting sys-tems, and each has inherent limi-tations. A centralized, systematicregistry using an easily accessibleelectronic database including de-vice make and model information
and medication data could be usedas a real-time clinical monitoringtool to alert regulators, manufactur-ers, and providers of safety signals.
Feedback could also be provided toidentify safety and efficacy trends inthe clinical use of a newly approvedtherapy. The initial capital costs ofsuch a system would not be insignif-icant; however, once implemented,the marginal cost for each addition-al patient tracked and monitoredwould be minimal and could befunded by a public-private partner-ship to the benefit of providers,manufacturers, and regulators.
ETHICAL CONSIDERATIONS
An overriding issue for any new de-vice or drug is the ethics of the in-formed consent process for first-in-human studies. More than 75% ofphase 1 clinical trials are performedoutside of the United States, be-cause regulatory barriers add sig-nificant costs to the developmentprocess.11 As a result, many of thesetrials are conducted in emergingmarkets where participants may findit attractive to participate in a trialto receive free or discounted carethat they would not receive other-wise. Moreover, most intracoronarydevice therapies are permanent and,by definition, removable only byextreme measures. Concerns aboutstent thrombosis emerged almost7 years after the phase 1 drug-elut-ing stent trials were completed,making it nearly impossible to re-move the devices if there had beena more significant risk of morbidityor mortality. As a result, patientswho participated in phase 1 trialscould have suffered a much graverscenario, particularly those whoseaccess to medical care and resourceswas limited. There must be equi-poise in the testing of any new ther-apy, but the rapid adoption of many
medical devices presents a chal-lenge in how to address problemswith permanent indwelling devicesthat cannot be easily extracted.
Other issues with phase 1 trials aresubjects’ perceptions of the trade-off between device safety and thera-peutic outcome.24 The trade-off islikely different than that ascribedto phase 1 research for oncologytherapeutics, as stents confer nomortality benefit. Unlike explainingthe risk of death to a patient, it isunclear how patients would valuethe trade-off between the need fortarget vessel revascularization andstent thrombosis, where the mor-tality rate for the latter is unclear.
INTELLECTUAL PROPERTY ISSUES
Medical devices are subject to thesame intellectual property andpatent protections afforded to oth-er technologies. For example, inFebruary 2008, a Texas jury ruledthat Boston Scientific’s drug-elutingstent infringed on a patent by a ra-diologist issued in 1997. The origi-nal patent described how facturesin bones could be healed if a thin,flexible material with small porescould allow the flow of large mole-cules in and out of the injured bone,also describing how this methodcould apply to stents to control thedelivery of drugs to a blood vesselwall.25 Also, Cordis’ parent company,Johnson & Johnson, sued Medtronicfor patent infringement, which re-sulted in a countersuit.26 In otherparts of the world, patents for drugsand devices are loosely regulated,allowing entrepreneurs and busi-nesses in local markets to manu-facturer and sell copycat productswithout paying royalties or licens-ing fees. Given the significant lossof revenue or royalties from infringe-ment of intellectual property, manu-facturers and entrepreneurs spend
270
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents? - Shah and Schulman

significant resources to protect anddefend these rights, and this costmust be considered in the devel-opment of any novel technology.
REIMBURSEMENT AND ECONOMICS
Little data exist on the diffusion ofmedical technology into medicalpractice and the barriers and incen-tives that affect adoption. However,with the approval of drug-elutingstents in the United States and theEuropean Union, the devices weredisseminated into the market rap-idly despite costing two to threetimes more than their bare-metalcounterparts. This rapid adoptioncould be explained in part by thereimbursement climate in the Unit-ed States. In an unprecedentedmove, the Centers for Medicare &Medicaid Services (CMS) approvedreimbursement of the incrementalcost of the use of a single drug-elut-ing stent compared to the use ofbare-metal stents.27 Prior to thisdecision, a new medical technologywas only reimbursed by CMS afterit had been used on the market andthe prospective annual reimburse-ment scale was adjusted on the ba-sis of review of retrospective costdata for specific diagnosis-relatedgroups. In practice, this resulted in an increase in payment 2 yearsafter market entry (unless the tech-nology qualified for special reim-bursement consideration under atechnology pass-through program).However, by creating a favorablereimbursement climate, CMS en-couraged rapid adoption of drug-eluting stents.
The price of drug-eluting stents wasjustified initially by a reduction inthe need for repeat revasculariza-tion for restenosis (although initialmodels suggested that drug-elutingstents would not save money andmight actually add costs to the sys-
tem).28 However, this benefit ex-tends to only 10% to 15% of pa-tients, making it difficult to predictwhich patients are at risk for reste-nosis and for whom the increasedcost would be justified. The truevalue of drug-eluting stents dependson the perspective taken. For pa-tients, increased costs for drug-elut-ing stents could be justified by thepotential reduction in events andrepeat revascularization for resteno-sis. This perspective would be sharedby physicians, but could be offset bydecreased revenue from perform-ing fewer procedures. Before theMedicare fee schedule change, hos-pitals were in crisis over the poten-tial diffusion of drug-eluting stents.However, after the payment policychanged, their incentives to impedethe dissemination of the technologyevaporated.
CONCLUSIONS
Medical devices can provide im-proved quality of life and longevityto many patients. Device technolo-gies are rapidly evolving and al-most as rapidly being adopted inclinical practice. However, the caseof drug-eluting stents illustratesthe complex risk-benefit trade-offfor new devices. The informed con-sent process for phase 1 researchin developing countries places adisproportionate burden of long-term complications of permanent,indwelling devices in populationswith limited access to health careand resources. Moreover, differingregulatory schemes for premarketapproval reflect differences in re-quirements for demonstration ofclinical efficacy, safety, and post-market surveillance. Reimbursementsystems can accelerate or moderateadoption of approved devices. Takentogether, these issues highlight thecomplexities and challenges ofbringing new medical technologiesinto clinical practice.
REFERENCES
1. Morice MC, Serruys PW, Sousa JE,et al.
A randomized comparison of a sirolimus-eluting stent with a standard stent for coro-nary revascularization.
N Engl J Med. 2002;346:1773-1780.
2. Stone GW, Ellis SG, Cox DA, et al.
A polymer-based, paclitaxel-eluting stent inpatients with coronary artery disease.
N Engl J Med. 2004;350:221-231.
3. Colombo A, Corbett SJ.
Drug-eluting stent thrombosis: increasinglyrecognized but too frequently overemphasized.
J Am Coll Cardiol. 2006;48:203-205.
4. Iakovou I, Schmidt T, Bonizzoni E,et al.
Incidence, predictors, and outcome of throm-bosis after successful implantation of drug-eluting stents.
JAMA. 2005;293:2126-2130.
5. Laskey WK, Yancy CW, Maisel WH.
Thrombosis in coronary drug-eluting stents:report from the meeting of the CirculatorySystem Medical Devices Advisory Panel ofthe Food and Drug Administration Centerfor Devices and Radiologic Health, Decem-ber 7-8, 2006.
Circulation. 2007;115:2352-2357.
6. Shaw LJ, Berman DS, Maron DJ,et al.
Optimal medical therapy with or withoutpercutaneous coronary intervention to reduceischemic burden: results from the ClinicalOutcomes Utilizing Revascularization andAggressive Drug Evaluation (COURAGE)trial nuclear substudy.
Circulation. 2008;117:1283-1291.
7. Ballentine C.
Taste of raspberries, taste of death: the 1937elixir sulfanilamide incident.
FDA Consum. June 1981. Available at:http://www.fda.gov/oc/history/elixir.html.Accessed September 10, 2008.
8. Food and Drug Administration.
History of the FDA: The 1938 Food, Drug,and Cosmetic Act.
US Food and Drug Administration Web site.Available at: http://www.fda.gov/oc/history/historyoffda/ section2.html. AccessedSeptember 10, 2008.
271
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents? - Shah and Schulman

9. Maisel WH.
Safety issues involving medical devices: im-plications of recent implantable cardioverter-defibrillator malfunctions.
JAMA. 2005;294:955-958.
10. FY 2006 CDRH Annual Report.
US Food and Drug Administration Web site.Available at: http://www.fda.gov/cdrh/annual/fy2006/index.html. AccessedSeptember 10, 2008.
11. Kaplan AV, Baim DS, Smith JJ,et al.
Medical device development: from prototypeto regulatory approval.
Circulation. 2004;109:3068-3072.
12. Cordis Corporation.
First drug-eluting stent treatment for coro-nary artery disease available in Europe[press release].
Cordis Corporation; April 15, 2002.Available at: http://www.cordis.com/active/crdus/en_US/html/cordis/downloads/press/2002FirstDrugEluting.pdf. AccessedSeptember 10, 2008.
13. Food and Drug Administration.
New device approval: CYPHERTM Sirolimus-eluting Coronary Stent—P020026. US Foodand Drug Administration Web site. June 10,2003; Available at: http://www.fda.gov/cdrh/mda/docs/p020026.html.
14. Cordis Corporation.
Health professional letter from Cordis Corporation. July 7, 2003. Available at:http://www.fda. gov/bbs/topics/news/cordis_ltr.pdf.
15. Food and Drug Administration.
FDA Public Health Web Notification: Infor-mation for Physicians on Sub-acute Throm-boses (SAT) and Hypersensitivity Reactionswith Use of the Cordis CYPHERTM CoronaryStent. US Food and Drug AdministrationWeb site; October 29, 2003. Available at:http://www. fda.gov/cdrh/safety/cypher.html. Accessed September 10, 2008.
16. Food and Drug Administration.
New Device Approval: TAXUSTM Express2TMPaclitaxel-Eluting Coronary Stent System—P030025US Food and Drug AdministrationWeb site; September 9, 2004. Available at:http://www. fda.gov/cdrh/mda/ docs/ p030025.html. Accessed September 10, 2008.
17. Pfisterer M, Brunner-La Rocca HP,et al.
Late clinical events after clopidogrel dis-continuation may limit the benefit of drug-eluting stents: an observational study ofdrug-eluting versus bare-metal stents.
J Am Coll Cardiol. 2006;48:2584-2591.
18. Eisenstein EL, Anstrom KJ, KongDF, et al.
Clopidogrel use and long-term clinical out-comes after drug-eluting stent implantation.
JAMA. 2007;297:159-168.
19. Food and Drug Administration.
New Device Approval: CYPHERTM Sirolimus-eluting Coronary Stent—P020026.
US Food and Drug Administration Web site;June 10, 2003. Available at: http://www.fda.gov/cdrh/mda/ docs/p020026.html.Accessed September 10, 2008.
20. AdvaMed.
AdvaMed strongly supports efforts to expandmarket access for U.S. products abroad[press release].
February 2, 2007. Available at: http://www.advamed.org/MemberPortal/About/NewsRoom/NewsReleases/2007/02-02-2007-accessforproducts.html. AccessedSeptember 10, 2008.
21. Riegel v Medtronic, Inc.
128 SCt 999 (2008).
22. Harrington RA, Ohman EM.
The enigma of drug-eluting stents: hope,hype, humility, and advancing patient care.
JAMA. 2007;297:2028-2030.
23. Krucoff MW, Boam A, Schultz DG.
Drug-eluting stents “deliver heartburn”: Howdo we spell relief going forward?
Circulation. 2007;115:2990-2994.
24. Rasiel EB, Weinfurt KP,Schulman KA.
Can prospect theory explain risk-seeking behavior by terminally ill patients?
Med Decis Making. 2005;25:609-613.
25. Feder BJ.
Boston Scientific loses patent suit but plansto appeal.
New York Times. February 13, 2008: C10.
26. Cordis Corporation.
Jury finds Cordis patents infringed by BostonScientific stents [press release].
Cordis Corporation; June 21 2005. Availableat: http://www.cordis.com/active/crdus/en_US/html/cordis/downloads/press/Cordis_InfBy_ BSC_PR_062105a.pdf.Accessed September 10, 2008.
27. Scully T.
Medicare Payment Advisory Commissioncomment on “Changes to the HospitalOutpatient Prospective Payment System andCalendar Year 2003 Payment Rates; andChanges to Payment Suspension for UnfiledCost Reports.”
October 4, 2002. Available at: http://www.medpac.gov/publications/other_ reports/100402_opps_CW_comment.pdf.Accessed September 10, 2008.
28. Ryan J, Cohen DJ.
Are drug-eluting stents cost-effective? It de-pends on whom you ask.
Circulation. 2006;114:1736-1743.
272
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
What are the regulatory and economic challenges posed by drug-eluting stents? - Shah and Schulman

Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
273
t has been said that death andtaxes are inevitable and dreadedevils. As scientists we can add athird, the writing of a grant pro-
posal. Why is the business of writinga grant proposal so disliked? There area number of reasons: the principal in-vestigator, as he is called to lower hisself-esteem, must compress his ideasinto a mold which has been ordainedby the granting agencies; he must ex-press his ideas in an idiom with whichhe may not be familiar; he must bemindful that he must please the re-viewers, whose scientific interest andexperience may be that of a competi-tor; he must realize that the reviewers,in order to appear intelligent, mustfind fault with his application; finallyto be successful, the proposal shoulddeal with a subject of current interest,not necessarily his own. A scientistwho can wrap his ideas into the mantleof sophistication, without interferingor competing with the reviewers’ terri-tory, is endowed with the specific gene
of grantsmanship. The location of thisgene is not known and it has as yet notbeen cloned. This gene can be absentin great scientists and the defect iscompatible with scientific excellence.
An example is Clair C. Patterson (1922-1995). The Archives of the CaliforniaInstitute of Technology possess in theirfiles an interview with Clair C. Patter-son who was a member of the divisionof geology and planetary science atthe California Institute of Technology.Despite his missing gene he was agreat scientist. His scientific life washighly successful, although he was con-genitally unable to get his work fund-ed. His scientific career is a triumphof will over an inborn genetic defect.
Patterson was born in Iowa, attendedGrinnell College, moved to the Univer-sity of Iowa, and then to the Universityof Chicago to work on the Manhattan(Atomic Bomb) project. He transferredto Oakridge, Tennessee, to continue
on the Manhattan project, where hebecame familiar with mass spectrom-etry, a technique which became thebasis of his future research. He alsobecame acquainted with HarrisonBrown, the geophysicist who was in-terested in meteorites to define theelemental abundance of the solar sys-tem. Harrison Brown, his mentor andchief, had worked on the concept thatlead in iron meteorites was the kindthat existed in the solar system whenit was first formed. Patterson was ablein 1953 to measure the isotopic com-position of primordial lead, from whichhe determined the age of the earth:“But we could do it because the iso-topic composition of the lead waschanging—it was dynamic becauseuranium was decaying all the time andthere were three radioactive progeni-tors of three different isotopes in thislead that were being added all the time
I
Matters @ HeartDr Patterson and his missing gene
Richard J. Bing, MDProfessor of Medicine - USC (Em) - Director of Experimental Cardiology - Huntington Medical Research Institute
Visiting Professor in Chemistry - California Institute of Technology - Calif - USA
Clair C. Patterson. Photo taken ca. 1989. © The Caltech Institute Archives.
Adapted from: Richard J. Bing, MD. Past Truthand Present Poetry: Medical Discoveries and thePeople Behind Them. First published as a series inHeart News and Views (News Bulletin of the Inter-national Society for Heart Research). The essaysare now available as a collection published underthe same title in 2006, by TFM PUBLISHINGLTD Nr. Shrewsbury ISBN 1903378443. By kind permission of Heart News and Views(www.ishrworld.org) and TFM PUBLISHING LTD(www.tfmpublishing.com).
Address for correspondence: Richard J. Bing,MD, Director, Experimental Cardiology, Em,HMRI - Huntington Medical Research Institute,99 N Cl Molino Avenue, Pasadena, CA 91011,USA (e-mail: [email protected])
Dialogues Cardiovasc Med. 2008;13:273-275
Practical guides for the perplexed investigator now abound. Courtesy of
National Science Foundation.

the earth was there. The proportions oflead and uranium and thorium wouldchange for millions and hundreds ofmillions of years at different areas, andthe lead within would have a differentisotopic composition and you couldtrack this. You could follow it.” Thiswork also led to his second discovery,the contamination of the earth withlead; he estimated the lead concentra-tion in blood of many Americans tobe over 100 times that of the naturallevel and within a factor of two of theaccepted limit for lead poisoning. Hediscovered that leaded gasoline waspartially responsible. This finding didnot endear him to the oil industry,
which quickly withdrew funding. Thisgot Patterson in trouble, particularlysince he also published a warning onthe amount of lead entering the foodchain.
The first symptom produced by themissing gene for grantsmanship ap-peared when Patterson, after gettinghis PhD, asked for funds to measurethe age of the earth and get the leadout of the meteorite. “So I wrote a littleproposal to the U.S. Atomic EnergyCommission—since they had financedus for work that led up to this. Theyturned me down, because they werenot interested in measuring the age
of the earth.” His chief rewrote theproposal in his name; “You know, heis very good in explaining things topeople in a nonscientific way—so he wrote the darn thing. Boom. I wasawarded a fellowship, a postdoc.” Ap-parently Dr Harrison Brown's genomefully expressed the gene for grants-manship!
Patterson then wanted to study theevolution of the earth by determiningthe isotopic composition of lead inrocks. His request for funding was notapproved: “they were trying to provethat I was wrong.” Again his chief cameto the rescue and obtained moneyfrom the Atomic Energy Commission;he told them that there was enoughuranium in rocks, so they would getenough to use it in an atomic genera-tor. Apparently this sales pitch was suc-cessful. Patterson bemoans his inabili-ty to please the granting agencies. Hewrote a paper stating that lead is com-ing from leaded gasoline: “When theystopped my research they went aroundand tried to stop all my funding.”
How did Patterson compensate for hismissing gene? He would go to otheruniversities and submit joint cooper-ative proposals. Others would writethe proposals and his name would
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Dr Patterson and his missing gene - Bing
274
How old is the earth? “Clock on the Earth.”Created by John S. Dykes, July 1, 1998.
© Images.com /Corbis.
Geophysicist HarrisonBrown in laboratoryexamining samples.Photo taken inMarch 1948 byWallace Kirklandfor LIFE. © TimeInc. /Getty Images.
“Measles figure” illustrating lead levels in prehistoric person (left), modern person from in-dustrialized regions (middle), and minimum amount to cause classical lead poisoning (right).Each dot represents 0.3 mg Pb/70 kg person. Drawn by Clair Patterson. © The CaltechInstitute Archives.

be on the joint proposal and part ofthe money would come to him. As he wrote: “I have been turned downthroughout the years. If I wrote a pro-posal with science—down, no way out.”
Recently I received a pamphlet from amedical school, which proudly reportsan advance in their rating, becauseresearch grants had increased by mil-lions of dollars. Their pride is justified;bad research is usually not funded, a good application has to be well or-ganized and sophisticated. And yet—there is the case history of Dr Patter-son and others like him with the miss-
ing gene. There are also those whohave a brilliant idea, not yet clothedin the mantle of sophistication! Theonly solution for those with this miss-ing gene is to hitch their scientificwagon to someone whose genome isintact. Otherwise there is only the sat-isfaction that goes with the creationof a new idea. Alas, there is no dollarsign attached!
The author expresses his appreciation for thehelp and encouragement from the Archives of
the California Institute of Technology. Allquotations are from an interview with Dr
Patterson held at the California Institute ofTechnology in March 1995. The Caltech Archives
have issued permission for publication.
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Dr Patterson and his missing gene - Bing
275
Missing gene—Big deal! Clair Patterson receiving the Tyler Prize in1995, awarded for “environmental science, energy, andmedicine confer-ring great benefitupon mankind.” © The CaltechInstitute Archives.

277Copyright © 2008 LLS SAS. All rights reserved
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
One-year outcomes of coronary artery bypass graft surgery versus percutaneous
coronary intervention with multiple stenting for multisystem disease…
N. Mercado and others. J Thorac Cardiovasc Surg. 2005
1Drug-eluting stent update 2007: Part I.
A survey of current and future generation drug-eluting stents: meaningful advances
or more of the same? Part II: Unsettled issuesJ. Daemen and P. W. Serruys. Circulation. 2007
6
Outcomes associated with drug-eluting and bare-metal stents:
a collaborative network meta-analysisC. Stettler and others. Lancet. 2007
2
Early and late coronary stent thrombosis ofsirolimus-eluting and paclitaxel-eluting stents
in routine clinical practice…J. Daemen and others. Lancet. 2007
8
Drug-Eluting Stents in AnginaSummaries of Ten Seminal Papers
Marco Valgimigli, MDArcispedale S. Anna - University of Ferrara - Corso Giovecca 203 - 44100 Ferrara - ITALY
(e-mail: [email protected])
Dialogues Cardiovasc Med. 2008;13:277-287
4Stent thrombosis late after implantation of first-generation drug-eluting stents:
a cause for concernE. Camenzind and others. Circulation. 2007
9Pathological correlates of
late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization
A. V. Finn and others. Circulation. 2007
Balancing the risks of restenosis and stent thrombosis in bare-metal
versus drug-eluting stents. Results of a decision analytic modelP. Garg and others. J Am Coll Cardiol. 2008
10
Cyphering the complexity of coronary artery disease using the
Syntax score to predict clinical outcome...M. Valgimigli and others. Am J Cardiol. 2007
7
Are drug-eluting stents associated with a higherrate of late thrombosis than bare metal stents?
Late stent thrombosis: a nuisance in both bare metal and drug-eluting stents
P. W. Serruys and J. Daemen. Circulation. 2007
5
Clinical end points in coronary stent trials: a case for standardized definitions
D. E. Cutlip and others. Circulation. 2007
3
Selection of seminal papers by William Wijns, MD, PhD, FESC
Cardiovascular Center Aalst - Aalst - Belgium
Highlights of the years by Ian Mudway, MDLung Biology - Division of Life Sciences - Franklin Williams Building
150 Stamford Street - London SE1 9NN - UK
www.dialogues-cvm.org

278
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
ith the advent of a safe and progressivelymore effective percutaneous coronary intervention (PCI) for coronary artery disease (CAD) as apposed to traditionalcoronary artery bypass grafting (CABG),
the choice as to the best revascularization strategy formultivessel disease patients remains today still very chal-lenging. Many previous meta-analyses have pooled togeth-er available randomized controlled studies comparingpercutaneous versus surgical revascularization in such pa-tient populations. However, they are limited by inclusionof patients treated with balloon angioplasty, with use ofbare-metal stents restricted to bailout situations. The results of trials that antedated the stent era are not reflec-tive of the current practice of coronary revascularizationbecause coronary stents are nowadays implanted in ap-proximately 90% or more of all procedures and adjunctivepharmacologic therapy with glycoprotein IIb/IIIa inhibitorsis frequently used.
This systematic overview based on individual patient datafrom recent clinical trials comparing angioplasty with mul-tiple stenting against CABG surgery thus provides the cli-nician caring for patients with multivessel disease withmeaningful treatment effect estimates regarding the advan-tages and drawbacks of each treatment strategy. The au-thors created an individual patient database composed of4 trials (Arterial Revascularization Therapies Study [ARTS],Stent or Surgery [SOS] trial, Argentine Randomized Trial ofPercutaneous Transluminal Coronary Angioplasty VersusCoronary Artery Bypass Surgery in Multivessel Disease–2[ERACI-2], and Medicine, Angioplasty, or Surgery Study–2[MASS-2]) that compared percutaneous coronary inter-vention with multiple bare-metal stenting (N=1518) versusCABG (N=1533). One year after the initial procedure, PCIwith multiple stenting and coronary artery bypass graftsurgery provided a similar degree of protection againstdeath, myocardial infarction, or stroke for patients withmultisystem disease. Repeat revascularization proceduresremain high after PCI, but the difference with CABG surgeryhas narrowed in the era of bare-metal stenting. In particu-lar, the observed gap with CABG surgery has narrowed
from approximately 30% reported in the pre-stent era toapproximately 14% in the present report.
While this analysis is largely consistent with the data re-ported by single studies comparing PCI versus CABG andthe results showed in previous meta-analyses, there aresome outstanding considerations, which should be keptin mind when interpreting the data. The main limitationof this meta-analysis is the relatively short follow-up peri-od limited to 1 year. Long-term (5-year) follow-up of thiscohort of patients is planned and will likely be reportedsoon. It is also likely that the patients included may rep-resent a selected population of low-to-moderate risk patients with multisystem disease, thus limiting the gen-eralizability of the results to more complex subsets of pa-tients. Finally, the use of drug-eluting stents may signifi-cantly impact on the performance of PCI versus CABG inthis patient population. With unrestricted use of drug-eluting stents, the difference in reintervention disfavoringthe PCI approach may further be reduced without affect-ing the overall composite of death, myocardial infarction,or stroke. This is what has been shown in the ARTS II studyin which 606 multivessel disease patients undergoingtreatment with sirolimus-eluting stents were comparedwith historical results obtained in the CABG arm of ARTS I.The SYNTAX study (SYNergy between PCI with TAXus andcardiac surgery) compared in a prospective randomizedmanner multiple DES implantation versus CABG in patientswith 3-vessel disease and/or left main stem-stenosis. The1-year primary end point results of this study were present-ed at the European Society of Cardiology annual congressin September 2008.
One-year outcomes of coronary artery bypass graft surgery versus percutaneous coronary intervention with multiple stentingfor multisystem disease: a meta-analysis of individual patientdata from randomized clinical trialsN. Mercado, W. Wijns, P. W. Serruys, U. Sigwart, M. D. Flather, R. H. Stables, W. W. O’Neill, A. Rodriguez, P. A. Lemos, W. A. Hueb, et al J Thorac Cardiovasc Surg. 2005;130:512-519
w
King Fahd of Saudi Arabia dies at the age of 83and Crown Prince Abdullah accedes to the throne;
Cuban singer Ibrahim Ferrer, vocalist of the Buena Vista Social Club, dies aged 78 years; and Phil Mickelson wins the 2005 PGA Championship
2005

279
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
he long-term safety of the first two polymer-based drug-eluting stents (DES) approved bythe US Food and Drug Administration (FDA)—a sirolimus-eluting stent and a paclitaxel-eluting stent—is a matter of intense and on-
going debate, with some studies reporting increased ratesof death, myocardial infarction, or late stent thrombosiscompared with bare-metal stents (BMS). These studies were,however, hampered by the small number of patients, limit-ed durations of follow-up, or observational study designs.
Network meta-analyses allow a unified, coherent analysisof all randomized controlled trials that have compared ei-ther of the two DES with BMS or the two DES head-to-head, while fully respecting randomization. The authorsset up a collaborative group of investigators who providedtrial data based on standardized definitions of outcomesand performed a network meta-analysis. Thirty-eight trials(18 023 patients) were included with a follow-up of up to4 years. Trialists and manufacturers were also contactedto provide additional data on clinical outcomes for 29 tri-als. This network meta-analysis showed that DES and BMSwere associated with similar rates of overall and cardiacmortality, and that use of sirolimus-eluting stents was asso-ciated with a reduction in the risk of myocardial infarctioncompared with use of BMS and paclitaxel-eluting stents.About 100 patients must receive sirolimus-eluting stents,rather than BMS or paclitaxel-eluting stents, to prevent 1 myocardial infarction over 4 years. Although there waslittle evidence of an overall increase in definite stent throm-bosis associated with DES, paclitaxel-eluting stents werefound to be associated with an increased incidence of latestent thrombosis compared with BMS and sirolimus-elut-ing stents. However, it should be emphasized that wideconfidence intervals precluded definite conclusions abouta potential increase in late stent thrombosis with sirolimus-eluting stents compared with BMS.
A secondary analysis showed a marked reduction in target-lesion revascularization with both DES, which was morepronounced for sirolimus-eluting stents than for paclitaxel-eluting stents. About 6 patients must receive a sirolimus-
eluting stent rather than a BMS to prevent 1 target lesionrevascularization over 4 years; 35 would need to receive asirolimus-eluting rather than a paclitaxel-eluting stent toprevent 1 such event. Lastly, there was little evidence ofan increased risk of mortality associated with either DESin diabetic patients, but again wide confidence intervalsprecluded definite conclusions.
This network meta-analysis integrated evidence from directand indirect comparisons while fully preserving random-ization. The considerably higher number of patients andevents in this study, compared with previous analyses re-sulted in a relevant gain in statistical precision, particularlyfor the hazard ratio of death, myocardial infarction, andstent thrombosis. Network meta-analysis makes similarassumptions to standard meta-analysis of direct within-trialcomparisons, but requires that these assumptions holdover the entire set of trials in the network, including theassumption that relative treatment effects comparing twointerventions in different trials are from the same commondistribution. The smaller the heterogeneity between trials,the more likely relative treatment effects originate fromthe same distribution. Additional assumptions are that themodel fits the data and that the network of trials is con-sistent. Importantly, all assumptions were satisfied for alloutcomes, except for stent thrombosis and target-lesionrevascularization. Critics have argued that not all bare-metalstents included in the trials perform equally well, whichmakes pooling of outcomes problematic.
T
The Roman Catholic Archbishop of Bulawayo calls for mass protests to force Zimbabwe’s
President Robert Mugabe from office; The Scout Movement celebrates its centennial;
and Angola joins OPEC
2007
Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysisC. Stettler, S. Wandel, S. Allemann, A. Kastrati, M. C. Morice, A. Schömig, M. E. Pfisterer, G. W. Stone, M. B. Leon, J. S. de Lezo, et alLancet. 2007;370:937-948

280
Eleven World Wrestling Entertainers are suspendedfor suspected steroid abuse; World Rally championColin McRae and his son are killed in a helicoptercrash in Scotland; and melting sea ice in the Arctic
Ocean opens up the Northwest Passage betweenEurope, Asia and North America
2007
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
or every clinical cardiologist and cardiovascularresearcher, this consensus article calling for stan-dardized outcome definitions in coronary stenttrials should be compulsory reading. Variabilityin end point definitions creates a formidable
barrier to the understanding of results across clinical trialsor the pooling of results for the detection of rare safetysignals. With the recognition that consistency across well-considered end point definitions is critical to this process,4 academic research organizations involved in the designand management of current drug-eluting stent (DES) clinicaltrials combined efforts in an informal collaboration termedthe Academic Research Consortium (ARC) to orchestratea set of consensus definitions for DES study end points.
While this consensus document focuses on the definitionsand standardization of all clinical cardiac and cardiovas-cular end points that may be applicable to coronary stenttrials, including death, myocardial infarction, reinterventionin the target vessel and cerebrovascular accidents, theadded value of this report is that it is the first attempt topropose a universal definition for stent thrombosis.
The ARC consensus is that both levels of evidence and tim-ing of events can be stratified to define varying degrees ofcertainty and to imply different pathophysiological mecha-nisms, respectively. The triple level of certainty classifica-tion recommended is definite, probable, and possible stentthrombosis.
Definite stent thrombosis classification requires angio-graphic or autopsy confirmation, is highly specific, and ispatterned on the definition developed when these eventswere first detected during early brachytherapy clinical trials.Although it maximizes specificity, the definite classificationmay not be sufficiently sensitive for the capture of a rela-tively rare safety event. The categories of probable andpossible stent thrombosis add such sensitivity, but the util-ity of these categories will vary depending on the qualityof data available to the adjudication committee. This isparticularly true for the least specific thrombosis category,possible, which could be assigned to all late deaths unless
sufficient detail is provided for adjudication. It is importantto avoid the dilution of a potential real difference in eventswith the use of an overly sensitive definition that may in-clude cases unlikely to represent thrombosis. The ARCrecommends the combination of adjudicated definite andprobable stent thrombosis to best characterize this aspectof DES safety; however, the reporting of definite only andoverall rates is also encouraged.
Since this report, the endorsement of this classification sys-tem for defining stent thrombosis has been widespread andconsistent by both investigator- or sponsor-driven clinicaltrials, thereby resulting in a significant improvement inour understanding on the incidence, predictors, and clinicalimplications of stent thrombosis. This very sensitive defi-nition of stent thrombosis, however, has clear limitations,which should also be acknowledged, including the fact thatit labels as potential stent thrombosis almost any vesselor stent failure or even any unexplained fatal or nonfatalcardiac event in the presence of limited available informa-tion. This may be particularly problematic in studies recruit-ing patients who have an intrinsic risk of fatal or nonfatalrecurrences, such as those with ongoing myocardial infarc-tion. In such settings, the category of possible stent throm-bosis remains questionable today. Similarly, it is likely thatthe specificity of probable and possible stent thrombosiscategories decreases over time, which may impact onstudies with long and clinical outcomes. A similar effortpertaining to appropriate end points for use in postmarket-ing surveillance registries would be welcome.
Clinical end points in coronary stent trials: a case for standardized definitions
D. E. Cutlip, S. Windecker, R. Mehran, A. Boam, D. J. Cohen, G. A. van Es, P. G. Steg, M. A. Morel, L. Mauri, P. Vranckx, et al; Academic Research Consortium
Circulation. 2007;115:2344-2351
F

281
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
t the European Society of Cardiology (ESC)/World Congress of Cardiology (WCC) inBarcelona in 2006, some of us were caughtoff guard by a plenary session combiningthree critical presentations by Edoardo Ca-
menzind, Salim Yusuf, and Alain Nordmann, who raisedserious concerns about the long-term safety profile ofdrug-eluting stents (DES). This session was dubbed the“ESC firestorm” and is very well known to all updated inter-ventional cardiologists. The criticisms and concerns regard-ing the safety profile of the first-generation DES, namely,sirolimus-eluting and paclitaxel-eluting stents, are sum-marized in this comprehensive revision of the literature.
The first section of this paper is devoted to the pathophys-iology of stent thrombosis, which is attributed to the so-called Rudolf Virchow’s triad: (i) abnormal vessel wall lining (eg, incomplete endothelialization); (ii) abnormalblood-flow pattern (eg, slow flow); and (iii) altered bloodconstituents (eg, increased blood thrombogenicity). Anyof these items alone or in combination favors intravascularthrombus formation. The connection between the anti-restenosis effect of first-generation DES and late stentthrombosis resides in the fact that antiproliferative agentssuch as sirolimus or paclitaxel inhibit intimal hyperplasiagrowth and endothelial cell proliferation, which ultimatelyprevents stent strut coverage. First-generation DES inhibitor may even abolish vessel wall healing, leaving the strutsin direct contact with flowing blood and blood elements.Complete or partial lack of reendothelialization of stentstruts and vessel wall generates a long-lasting, if not per-manent, unhealed vessel wall surface, favoring plateletadhesion and aggregation, which may eventually causethrombus formation. Moreover, the chronic inflammatoryprocess is possibly linked to the nonerodable polymer orthe eluted drug itself may trigger positive vessel remodel-ing (ie, an increase in vessel lumenal diameter over time).Widening of the coronary lumen over time may reduce bothintra-stent flow velocity and wall shear stress. Segmentalslow flow may be caused by a local intravasal abnormality(eg, aneurysm or bifurcational stenting) or a global coro-nary perfusion abnormality (eg, diastolic coronary perfusion
determined by variables such as tachycardia, increased tele-diastolic pressure, microangiopathy, distal embolization),and thereby give rise to prolonged interaction betweenvessel wall and blood constituents. According to this hy-pothesis, patients with delayed or poor stent healing afterintervention who are at increased risk for late stent throm-bosis are those who show no in-stent intima hyperplasiaat follow-up and/or positive vessel remodeling.
Thus, particularly those DES that are associated with lowerlate loss (ie, higher intima hyperplasia inhibition) may pre-dispose to higher likelihood of stent thrombosis. This hy-pothesis is challenged by several reports showing that theprobability of late and especially very late stent thrombo-sis is slightly higher with paclitaxel-eluting stents thansirolimus-eluting stents, yet negative late loss at angio-graphic follow-up is more frequently detected in the latterthan in the former. While this hypothesis remains intrigu-ing, it needs to be proven by scientific trial before beingendorsed by the cardiological community.
The second part of the article focuses on the rate of over-all death or Q-wave myocardial infarction in first-genera-tion DES vs BMS studies. The discussion emphasizes theneed for a standardized definition of major cardiovascularsafety end points and calls for a more transparent andsystematic report of long-term outcomes in these studies.This report triggered intense scrutiny of all related issuesand “carved some peepholes in the DES industry firewalls”(Cook et al, EurIntervention 2008;3:535-537).
A
News Corporation’s CEO Rupert Murdoch an-nounces a $5 billion takeover of Dow Jones & Co,
the publisher of the Wall Street Journal;Street Sense wins the 133rd Kentucky Derby;
and Floyd Mayweather Jr defeats Oscar De La Hoyain the highest grossing boxing match in history
2007
Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern
E. Camenzind, P. G. Steg, W. Wijns
Circulation. 2007;115:1440-1455

282
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
his position paper, intended as a point-by-point rebuttal to the paper by Camenzind et al,is a thorough reanalysis of the issue of earlyand late stent thrombosis (ST), starting fromthe introduction of the bare-metal stent (BMS),
through the advent of brachytherapy, and finally focusingon drug-eluting stent (DES) data.
The authors questioned the scientific value of the classictriad of Virchow (altered blood constituents, flow pattern,and endothelial lining) as an explanation for ST after DESimplantation. Discontinuation of oral antiplatelet treatment(aspirin and/or clopidogrel) is associated with proinflam-matory and prothrombotic effects in patients with coronaryartery disease, and this proved to be a risk factor for coro-nary events regardless of whether a DES was implanted ornot. The optimal duration of dual antiplatelet treatmentafter DES remains currently unknown and clopidogrel dis-continuation may be a risk factor for ST only when inter-rupted in the early phase after stenting (first 6 months),whereas there are currently no sound data in favor of moreprolonged dual antiplatelet treatment. In a limited numberof DES patients, postmortem findings show dramatic andcompelling evidence of impaired reendothelialization withuncovered stent struts in stented arteries. However, emi-nent pathologists are the first to admit that postmortemstudies have failed to evidence a common denominatorand that the number of patients treated with DES in whom“uncovered stent struts” do not lead to ST is unknown, butundoubtedly very large.
Although late acquired malapposition has been occasion-ally observed with BMS, it is more frequent with DES, andthe question remains of whether it has an unfavorableprognosis with respect to late ST. Intravascular ultrasoundstudies in randomized trials (RAVEL, SIRIUS, and E-SIRIUS),are available in 325 patients and the incidence of incom-plete stent apposition at 6 months was 25% in the sirolimus-eluting stent (SES) group vs 8.3% in the BMS group. Theauthors found no prognostic impact of incomplete stentapposition on death (2.2% with incomplete stent apposi-tion vs 5.2% without) and major adverse cardiac events
(8.9% with incomplete stent apposition vs 12.6% without)in patients treated with SES, at least in the short term. LateST was observed in only 1 of 45 patients with incompletestent apposition at a 6- to 8-month follow-up.
Finally, the authors critically reanalyzed the data present-ed at ESC 2006 by Camenzind et al during the “firestorm,”pointing out two potential methodological limitations: • The meta-analysis was derived from data published atdifferent time points of follow-up. Of note, more completedata only became available following the alarm.• Camenzind took two hard clinical end points, total deathand Q-wave myocardial infarction (MI), and disregardednon–Q-wave MI, which was indeed substantially lower inthe Cypher group. By including all MI in the analysis, noincrease in the composite of death or MI would be reachedin the SES as compared with the BMS arm.
The authors concluded that late ST occurs both with DESand BMS. However, the chronology and circumstances ofoccurrence seem quite different. With DES, late ST occurslater than with BMS and seems to appear as primary throm-bosis, whereas with BMS it may related to repeat interven-tions of the target lesion. It is not known to which extentcrossover to DES for treatment of BMS restenosis con-tributes to these events. Dedicated research is warrantedto further elucidate the role of endothelial dysfunction,malapposition, and prolonged antiplatelet therapy.Currently, second-generation DES are attempting to re-solve the problems posed so far by first-generation DES.
Are drug-eluting stents associated with a higher rate of latethrombosis than bare metal stents? Late stent thrombosis: a nuisance in both bare metal and drug-eluting stents
P. W. Serruys, J. Daemen
Circulation. 2007;115:1433-1439
T
A tsunami occurs on the northern coast of Japanfollowing a 6.9 magnitude earthquake;
French presidential candidate Nicolas Sarkozy resigns as Interior Minister to concentrate on hiscampaign; and the European Union celebrates
the 50th anniversary of its foundation
2007

283
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
art I is a comprehensive review of the past,present, and foreseeable future of drug-elutingstents (DES), whose numbers keep growing inan exponential manner. They are all loaded withdrugs that interfere with inflammation and neo-
intimal proliferation pathways. The process of restenosisis a sequence of complex events that has been only partlyelucidated over the last 2 decades. Locally acting DES pro-vide an opportunity to interfere with the various mecha-nisms responsible for each step in the restenotic cascade,and a wide variety of different agents are currently available.
The limus family is discussed first, which includes sirolimus-,everolimus-, zotarolimus-, pimecrolimus-, biolimus-, andtacrolimus-eluting stents, followed by paclitaxel-elutingstents. The new coating and new platform chapters areworth reading for those of us who want to understand whois doing what in a complex system such as DES technologynowadays. The pro-healing section is entirely devoted toa dream that has still to come true: we do have to inhibitintimal hyperplasia, but at the same time we also have topromote complete healing shortly after the implantation ofthe stent to obtain both lower late loss and an ideal safetyprofile. The so-called “endothelial progenitor cell (EPC)capture stent” which is coated with anti-CD34 monoclonalantibodies is here extensively described. EPCs are, how-ever, not only identified by the expression of CD34 antigen,so the concept of a stent, which, by binding to CD34+ cir-culating cells, is able to promote stent healing is, to someextent, conceptually misleading and still waiting for proof-of-concept evidence. Indeed, today there is no clear-cutevidence suggesting that this complex type of device ac-tually promotes quicker and more complete healing thanthe bare-metal stent, while the results in terms of lateloss are partially disappointing. The last paragraph em-phasizes the importance of elution kinetics as one of themost important variables for obtaining enduring late lossinhibition over time and for avoiding the so called late“catch-up phenomenon.”
art II is entirely devoted to unsettled issues inthe DES era. After a brief summary focusing onthe value of DES implantation as an effectivemeans to reduce late loss and subsequent tar-get-lesion revascularization as compared with
BMS, the article focuses on the pitfalls of DES.
First, DES have been shown to hamper the natural vascu-lar healing process. Second, stent underexpansion (mini-mum stent area <5.0 mm2), a factor linked to restenosis,is significantly more frequent after DES implantation.Whereas stent underexpansion is observed in 20% of allrestenotic BMS lesions, an incidence of up to nearly 70%is reported in restenotic DES lesions. This may simply re-flect a less aggressive policy of stent overexpansion afterDES implantation as compared with BMS, due to exces-sive confidence in the anticipated superior antirestenoticproperties of DES. Third, DES implantation seems to beassociated with significant impairment in endothelialfunction, which in turn has been repeatedly linked to ahigher rate of late adverse events. Fourth, recent reportshave shown a significantly lower rate of neointimal cover-age with DES (13.3% to 66%) than with BMS (90% to 100%),and subclinical thrombi tended to be more common withDES (P<0.09). These observations are pertinent to theconcerns with late stent thrombosis, which is here exten-sively discussed both in the context of on- and off-labeluse of DES as compared with BMS.
P P
New species of scallop and octopi are discoveredoff the coast of Nova Scotia; Bollywood actor
Sanjay Dutt is jailed for six years on charges of obtaining weapons from gangsters in a case
associated with the 1993 Mumbai bombings; and New Zealand launches its first commerciallyavailable biofuel, consisting of 90% petrol and
10% bioethanol derived from cows’ milk
2007
Drug-eluting stent update 2007: Part I. A survey of current andfuture generation drug-eluting stents: meaningful advances ormore of the same? Part II: Unsettled issues
J. Daemen, P. W. Serruys
Circulation. 2007;116:316-328 (Part I, issue No. 3)Circulation. 2007;116:961-968 (Part II, issue No. 8)

ince the earliest reports of coronary angiography,the extent of coronary artery narrowing has beenconsidered a primary determinant of survival inpatients with coronary artery disease. The simpledivision into one-, two-, and three-vessel disease
has provided a convenient scheme for classifying patientsand it has been extensively employed across the literature.This straightforward scoring system, however, is known tounderestimate the prognostic importance of anatomy, es-pecially in patients with complex and diffuse coronary arterydisease. The Syntax score (SXscore) was developed in thecontext of the SYNTAX trial (SYNergy between PCI withTAXus and cardiac surgery) as a comprehensive angiograph-ic tool. The score merges and tailors several previouslyvalidated scoring systems to the current era of intervention,and aims to assist in patient selection and risk-stratifica-tion for individuals with extensive coronary artery diseaseundergoing revascularization.
This report compares the predictive value of the Syntaxscore and of the modified American Heart Association(AHA) lesion classification system. The Syntax score wasapplied to 1292 lesions in 306 patients undergoing treat-ment for three-vessel disease in the Arterial Revasculariza-tion Therapies Study part II (ARTS II) to examine its rolein predicting short- and long-term incidence of major ad-verse events.
The Syntax score predicted the rate of major adverse car-diac and cerebrovascular events (MACCE), with patientsin the highest score tertile showing a significantly higherevent rate at both 30 days and 1 year. After adjustment forall potential confounders, including clinical presentationand lesion characteristics, the Syntax score remained anindependent predictor of MACCE at 1 year’s follow-up, withan almost threefold increase in the risk of events in patientsin the highest compared to two lowest score tertiles. Abetter goodness of fit was obtained when modeling the riskprovided by the Syntax score than that by the modifiedAHA lesion classification. This implies a closer relationshipbetween observed and predicted event rates when the Syn-tax score is employed. In keeping with previous analysis,
the area under the curve for the Syntax score was greaterthan the AHA score for MACCE at 30 days. Similarly, usinga time-dependent analysis, based on the c-index compu-tation, the prognostic accuracy provided by the Syntax scorewas confirmed to be significantly higher.
The ultimate goal for the Syntax score will be to discrimi-nate outcome in surgically versus percutaneously treatedpatients, in view of selecting the best revascularizationstrategy for the individual patient. The prognostic impli-cations of the Syntax score for patients with three-vesseland/or left main coronary artery disease undergoing eitherpercutaneous or surgical coronary revascularization will befurther evaluated in the ongoing trial. As soon as this data-set is available, each single item of the Syntax score willbe “weighed” according to discrepancy between observedand predicted event rate in order to further optimize cali-bration and the interaction between the global score andits single components as well as with the mode of revas-cularization applied (ie, percutaneous versus surgical).While still clearly in its early phase, the Syntax score willlikely be complemented in the future by surgical risk scores,such as the Euroscore or derived scores, to better deter-mine the optimal revascularization strategy in patients withcomplex coronary artery disease.
s
India’s Essar Group buys Canadian steelmakerAlgoma for $1.63 billion; Author Ray Bradbury
and jazz saxophonist John Coltrane receive special citations at the 2007 Pulitzer Prize awards;
and shootings at the Virginia Polytechnic Institute and State University leave 33 dead
and 29 others wounded
2007
Cyphering the complexity of coronary artery disease using the Syntaxscore to predict clinical outcome in patients with three-vessel lumenobstruction undergoing percutaneous coronary intervention
M. Valgimigli, P. W. Serruys, K. Tsuchida, S. Vaina, M. A. Morel, M. J. van den Brand, A. Colombo, M. C. Morice, K. Dawkins, B. de Bruyne, et al; ARTS II
Am J Cardiol. 2007;99:1072-1081
284
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli

285
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
his cornerstone paper stems from the institu-tional databases of two tertiary referral centersin Europe, namely, Bern and Rotterdam. Be-tween April 2002, and December 2005, 8146patients underwent percutaneous coronary
intervention in these two hospitals with either sirolimus-eluting stents (SES; n=3823) or paclitaxel-eluting stents(PES; n=4323). Angiographically documented stent throm-bosis occurred in 152 patients (incidence density 1.3 per100 person-years; cumulative incidence at 3 years 2.9%).Early stent thrombosis was noted in 91 (60%) patients, andlate stent thrombosis in 61 (40%) patients. Definite latestent thrombosis occurred steadily at a constant rate of0.6% per year up to 3 years after stent implantation. Theincidence of early stent thrombosis was similar for SES(1.1%) and PES (1.3%), but late stent thrombosis was morefrequent with PES (1.8%) than with SES (1.4%; P=0.031).At the time of stent thrombosis, dual antiplatelet therapywas being taken by 87% (early) and 23% (late) of patients(P<0.0001). Independent predictors of overall stent throm-bosis were acute coronary syndrome at presentation (hazardratio, 2.28; 95% CI, 1.29-4.03) and diabetes (2.03, 1.07-3.83).The median time to occurrence of early stent thrombosiswas 4 days (inter-quartile range [IQR], 1-6). Of the 61 latestent thrombosis cases, 36 (59%) patients developed stentthrombosis 1 year or later after stent implantation (medi-an, 451 days; IQR, 211-665). The cumulative incidence ofstent thrombosis over time showed an initial steep risewith 50% of cases occurring within 9 days, followed by analmost linear increase in the remaining events up to 3years. Notably, the absence of clopidogrel treatment didnot seem to be associated with an increased risk of totaland late stent thrombosis. The main value of this com-bined, yet retrospective analysis, consists in providingstrong and worrisome evidence that the rate of late stentthrombosis does not decrease over time at least up to 3years after drug-eluting stent (DES) implantation.
The hot issue we still need to clarify today is whether therate of very late stent thrombosis will somehow flatten atlonger-term follow-up or will this constant 0.6% rate per yearbe observed even beyond 3 to 4 years after DES implanta-
tion. Only longer-term follow-up studies will tell. Concomi-tantly, the major limitation of this analysis lies on the lackof a control group treated with bare-metal stent (BMS).Indeed, based on all randomized controlled studies con-ducted so far, it seems that the overall incidence of stentthrombosis does not differ in BMS- versus DES-treated pa-tients. Thus, it is likely that BMS implantation is associatedwith a higher risk of stent thrombosis from 5 to 12 monthsafter treatment, whereas DES use increases the likelihoodof late stent thrombosis beyond 1 year. Based on theseconsiderations, if the cumulative rate of late stent throm-bosis will keep accruing over time after DES, at very long-term follow-up, the overall stent thrombosis rate may endup being significantly higher than after BMS implantation.This may translate into a net increase in the composite of death and myocardial infarction in the DES- comparedwith BMS-treated patients at very long-term follow-up.Careful long-term clinical surveillance of all DES and BMSpatients so far recruited in randomized controlled studieswill be pivotal for this purpose. Finally, in a consistentmanner, PES was associated with slightly more late stentthrombosis than SES.
This has one major implication: even first-generation DEScannot be considered as one class of devices, and to someextent each single DES differs from the other, both in termsof efficacy and safety.
T
The Virginia General Assembly votes unanimouslyin favor of a motion expressing “profound regret”
for Virginia’s role in the promotion of slavery; Mario Chanes de Armas, one of the leaders in
the Cuban revolution, dies, aged 80 years; and “The Departed” wins four Academy Awards
including Best Picture and Best Director for Martin Scorsese at the 79th Academy Awards
2007
Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study
J. Daemen, P. Wenaweser, K. Tsuchida, L. Abrecht, S. Vaina, C. Morger, N. Kukreja, P. Jüni, G. Sianos, G. Hellige, et al
Lancet. 2007;369:667-678

286
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
olymer-based sirolimus- (Cypher) and paclitax-el-eluting (Taxus) drug-eluting stents (DES)have become a treatment of choice for patientswith symptomatic coronary artery disease un-dergoing percutaneous coronary revasculariza-
tion. Although these stents have reduced rates of restenosisand late lumen loss compared with bare-metal stents, latethrombosis, a life-threatening complication of this technol-ogy, has emerged as a major concern. Although clinicalpredictors such as withdrawal of antiplatelet therapy areknown to play a role in determining the probability of latestent thrombosis, the specific morphometric and histolog-ical parameters that significantly correlate with late throm-bosis remained largely unknown.
This study reported by Finn et al was based on analysis ofautopsy material and using a database of all patients dy-ing >30 days after Cypher or Taxus DES implantation. Itsought to determine the most powerful pathological riskfactors for late thrombosis and identify the high-risk fea-tures of DES that might be clinically assessable. The mainfinding was that nonuniform healing with DES (as indicatedby the number of uncovered struts per cross section) great-ly increases the thrombotic risk.
Previous pathological studies have shown an associationbetween lack of neointimal strut coverage and thrombusformation. Although the mechanisms by which the current-generation DES induce nonuniform incomplete healingare not fully understood, lesion characteristics, drug proper-ties, dose, and distribution, and polymer biocompatibilitytogether likely play an important role.
The underlying plaque morphology may affect the rate ofhealing when stent struts penetrate deeply into a necroticcore and are not in contact with cellular areas. Eccentricplaques may prevent uniform strut deployment, therebyincreasing local toxicity resulting from higher concentra-tions of drug and polymer. Indeed, sections with evidenceof thrombosis showed significantly lower inter-strut dis-tances, which correlated with less neointimal growth. Localconcentrations of drug are ultimately highly spacing-de-
pendent, and the variance in distance between struts am-plifies differences in concentrations, leading to biologicaleffects. Heterogeneity in loaded dose of drug varies fromstrut to strut, and greater retention of lipophilic drugs indifferent regions of plaque affects arterial drug concentra-tion and results in nonuniform healing. The relationshipbetween local drug concentrations and cellular repair isunderscored by data from overlapping versus nonoverlap-ping Cypher and Taxus stents in the rabbit iliac model.
This study was seminal in establishing a predictor of latestent thrombosis. The authors speculated that there mightbe a continuum of risk increasing with the ratio of uncov-ered to total struts per section. Using a univariate logisticregression model of occurrence of thrombus in a stent sec-tion versus ratio of uncovered to total struts per section,they showed that in a stent with 30% uncovered struts, theodds ratio for thrombus is 9.0 (95% confidence interval[CI], 3.5 to 22.0) compared with a stent with complete cov-erage. Based on this postulation, many groups around theworld are now evaluating, in vivo, using optimal coherencetomography, the predictive value of uncovered struts toidentify upfront patients at high risk for very late stentthrombosis,. This may have relevant implications for long-term management, including intensification and/or tailor-ing of antiplatelet treatment to protect patients from po-tential catastrophic consequences. Prospective studies tovalidate these pathologic findings in vivo are warranted.
Pathological correlates of late drug-eluting stent thrombosis:strut coverage as a marker of endothelialization
A. V. Finn, M. Joner, G. Nakazawa, F. Kolodgie, J. Newell, M. C. John, H.K. Gold, R. Virmani
Circulation. 2007;115:2435-2441
P
UK Prime Minister Tony Blair announces he willstep down from office on the 27th of June 2007;
Malietoa Tanumafili II, Samoa’s Head of State, dies,aged 94; and Canada defeats Finland 4-2 to win
the 2007 World Hockey Championship in Moscow
2007

287
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Summaries of Ten Seminal Papers - Valgimigli
ecisions regarding percutaneous coronaryintervention (PCI) for obstructive coronarydisease have become increasingly challeng-ing for patients and physicians since the ob-servation of delayed stent thrombosis with
drug-eluting stents (DES). The main risk attributable tobare-metal stenting (BMS) was restenosis, requiring repeatrevascularization—a risk that largely ended within 1 yearafter stenting. Beyond this period, events attributable tothe stent were rare. In particular, in-stent thrombotic com-plications occurred in <1% of patients, almost exclusivelywithin the first month after BMS implantation. By limitingneointimal hyperplasia within the stent, the current gener-ation of DES has reduced the relative risk of restenosis by50% to 70%. However, there is concern that DES might beassociated with increased risks of delayed stent thrombosis.
In this study, the authors sought to quantify the degree towhich current uncertainty in the rate of very late thromboticcomplications after DES implantation would affect thechoice of one stent type versus the other. Because boththe absolute risk and duration of risk of stent thrombosisafter DES implantation are uncertain, the authors used theMarkov model of decision analysis to define what thresholdof incremental risk of thrombosis with DES would outweighthe benefits of reduced restenosis in clinical practice. Theyfound, on the basis of the best data currently available, thatthe DES strategy was preferred for a prototypical PCI pa-tient under the assumption of no difference in the rates of(very) late stent thrombosis. Although the benefit was smallin absolute terms (0.014 QALYs, or quality-adjusted lifeyears gained), this gain is plausible given the time-limitednature of the restenosis process and the absence of long-term mortality benefit associated with restenosis avoid-ance in most studies. This finding was confirmed to be ro-bust, on the basis of probabilistic sensitivity analysis, whichtakes into account a range of plausible probabilities ratherthan relying on fixed estimates alone. Nonetheless, theauthors also found their results to be highly sensitive to theabsolute risk and duration of risk for late stent thrombosis,leading to uncertainty about optimal decision over a rangeof risk that is plausible on the basis of current data. In par-
ticular, for a prototypical patient, the authors found thateven a small excess risk of very late stent thrombosis(>0.14%/year over 4 years) would be sufficient to negateany advantage of DES over BMS in terms of mean quality-adjusted life expectancy. Furthermore, if the at-risk periodextended beyond 4 years, the incremental annual risk thatcould be tolerated was even smaller.
Whether the true risk of very late thrombosis with existingDES exceeds this risk is uncertain at present. Most likely,the risk depends on stent type and patient/lesion subsets.Restenosis risks can be predicted with reasonable precisionin overall populations and according to well-understoodpatient and lesion-based factors, because restenosis wasa frequent occurrence over the past decade of practice. Incontrast, stent thrombosis risks have only recently beenstudied with similar rigor. Although pooled analyses ofrandomized trials of the two approved DES platforms to4 years of follow-up have not shown significant differences inrisk of thrombosis between DES and BMS, the confidenceintervals of these estimates are wide, suggesting that up toa 1.4% absolute risk difference at 4 years cannot be excluded.
In other terms, on the basis of a decision analytic modelincorporating the best data currently available, the authorsfound that even a small (<1%) incremental risk in throm-bosis with DES was sufficient to outweigh the benefit ofrestenosis prevention and favors BMS use for the overallPCI population. This analysis argues against the systematicuse of first-generation DES in all cases; instead DES shouldbe preferentially used in patient/lesion subsets with a highlikelihood of restenosis when treated with BMS.
Balancing the risks of restenosis and stent thrombosis in bare-metal versus drug-eluting stents. Results of a decision analytic model
P. Garg, D. J. Cohen, T. Gaziano, L. Mauri
J Am Coll Cardiol. 2008;51:1844-1853
d
Silvio Berlusconi is sworn in as the Italian PrimeMinister for his fourth term in office; a pro-Europecoalition wins the Serbian parliamentary election;
and a magnitude 7.9 earthquake hits China’sSichuan province, with at least 22 000 casualties
2008

289Copyright © 2008 LLS SAS. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Awata M, Kotani J, Uematsu M, et al. Serial angioscopic evidence of incomplete neointimal coverage aftersirolimus-eluting stent implantation: comparison with bare-metalstents.
Circulation. 2007;116:910-916.
Brilakis ES, Banerjee S, Berger PB. Perioperative management of patients with coronary stents.
J Am Coll Cardiol. 2007;49:2145-2150. Review.
Brunner-La Rocca HP, Kaiser C, Pfisterer M; Targeted stent use in clinical practice based on evidence from theBASKET Investigators. Basel Stent Cost Effectiveness Trial (BASKET).
Eur Heart J. 2007;28:719-725.
Buonamici P, Marcucci R, Migliorini A, et al. Impact of platelet reactivity after clopidogrel administration on drug-eluting stent thrombosis.
J Am Coll Cardiol. 2007;49:2312-2317.
Campo G, Valgimigli M, Gemmati D, et al. Value of platelet reactivity in predicting response to treatment andclinical outcome in patients undergoing primary coronary intervention: insights into the STRATEGY Study.
J Am Coll Cardiol. 2006;48:2178-2185.
Chen BX, Ma FY, Luo W, et al. Neointimal coverage of bare-metal and sirolimus-eluting stentsevaluated with optical coherence tomography.
Heart. 2008;94:566-570.
Chen MS, John JM, Chew DP, Lee DS, Ellis SG, Bhatt DL. Bare-metal stent restenosis is not a benign clinical entity.
Am Heart J. 2006;151:1260-1264.
Chieffo A, Morici N, Maisano F, et al. Percutaneous treatment with drug-eluting stent implantation versusbypass surgery for unprotected left main stenosis: a single-centerexperience.
Circulation. 2006;113:2542-2547.
Chieffo A, Park SJ, Valgimigli M, et al. Favorable long-term outcome after drug-eluting stent implantationin nonbifurcation lesions that involve unprotected left main coronaryartery: a multicenter registry.
Circulation. 2007;116:158-162.
Cosgrave J, Melzi G, Biondi-Zoccai GG, et al. Drug-eluting stent restenosis the pattern predicts the outcome.
J Am Coll Cardiol. 2006;47:2399-2404.
Daemen J, Kukreja N, van Twisk PH, et al. Four-year clinical follow-up of the rapamycin-eluting stent evaluatedat Rotterdam cardiology hospital registry.
Am J Cardiol. 2008;101:1105-1111.
Bibliography of One Hundred Key Papersselected by William Wijns*, MD, PhD, FESC and Marco Valgimigli†, MD
*Cardiovascular Center Aalst - Aalst - BELGIUM - (e-mail: [email protected])†Cardiovascular Institute - Arcispedale S. Anna - University of Ferrara - Ferrara - ITALY
Drug-Eluting Stents in Angina

Dibra A, Kastrati A, Mehilli J, et al; Paclitaxel-eluting or sirolimus-eluting stents to prevent restenosis ISAR-DIABETES Study Investigators. in diabetic patients.
N Engl J Med. 2005;353:663-670.
Eisenberg MJ. Drug-eluting stents: the price is not right.
Circulation. 2006;114:1745-1754.
Eisenstein EL, Anstrom KJ, Kong DF, et al. Clopidogrel use and long-term clinical outcomes after drug-elutingstent implantation.
JAMA. 2007;297:159-168.
Elezi S, Dibra A, Folkerts U, et al. Cost analysis from two randomized trials of sirolimus-eluting stentsversus paclitaxel-eluting stents in high-risk patients with coronaryartery disease.
J Am Coll Cardiol. 2006;48:262-267.
Elezi S, Dibra A, Mehilli J, et al. Vessel size and outcome after coronary drug-eluting stent placement:results from a large cohort of patients treated with sirolimus- orpaclitaxel-eluting stents.
J Am Coll Cardiol. 2006;48:1304-1309.
Fajadet J, Wijns W, Laarman GJ, et al; Randomized, double-blind, multicenter study of the EndeavorENDEAVOR II Investigators. zotarolimus-eluting phosphorylcholine-encapsulated stent for
treatment of native coronary artery lesions: clinical and angio-graphic results of the ENDEAVOR II trial.
Circulation. 2006;114:798-806.
Galløe AM, Thuesen L, Kelbaek H, et al; Comparison of paclitaxel- and sirolimus-eluting stents in everyday SORT OUT II Investigators. clinical practice: the SORT OUT II randomized trial.
JAMA. 2008;299:409-416.
Gerber R, Colombo A. Does IVUS guidance of coronary interventions affect outcome? A prime example of the failure of randomized clinical trials.
Catheter Cardiovasc Interv. 2008;71:646-654.
Grines CL, Bonow RO, Casey DE Jr, et al; American Heart Prevention of premature discontinuation of dual antiplatelet therapy Association; American College of Cardiology; Society for in patients with coronary artery stents: a science advisory from theCardiovascular Angiography and Interventions; American American Heart Association, American College of Cardiology, College of Surgeons; American Dental Association; Society for Cardiovascular Angiography and Interventions,American College of Physicians. American College of Surgeons, and American Dental Association
with representation from the American College of Physicians.
J Am Coll Cardiol. 2007;49:734-739.
Hamon M, Biondi-Zoccai GG, Malagutti P, et al. Diagnostic performance of multislice spiral computed tomographyof coronary arteries as compared with conventional invasive coronary angiography: a meta-analysis.
J Am Coll Cardiol. 2006;48:1896-1910.
Hannan EL, Racz M, Holmes DR, et al. Comparison of coronary artery stenting outcomes in the eras beforeand after the introduction of drug-eluting stents.
Circulation. 2008;117:2071-2078.
Hannan EL, Wu C, Walford G, et al. Drug-eluting stents vs. coronary-artery bypass grafting in multivessel coronary disease.
N Engl J Med. 2008;358:331-341.
Holmes DR Jr, Kereiakes DJ, Laskey WK, et al. Thrombosis and drug-eluting stents: an objective appraisal.
J Am Coll Cardiol. 2007;50:109-118. Review.
290
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Holmes DR Jr, Teirstein P, Satler L, et al; Sirolimus-eluting stents vs vascular brachytherapy for in-stentSISR Investigators. restenosis within bare-metal stents: the SISR randomized trial.
JAMA. 2006;295:1264-1273.
Hong MK, Mintz GS, Lee CW, et al. Late stent malapposition after drug-eluting stent implantation: an intravascular ultrasound analysis with long-term follow-up.
Circulation. 2006;113:414-419.
Hwang CW, Levin AD, Jonas M, Li PH, Edelman ER. Thrombosis modulates arterial drug distribution for drug-elutingstents.
Circulation. 2005;111:1619-1626.
Iakovou I, Schmidt T, Bonizzoni E, Ge L, et al. Incidence, predictors, and outcome of thrombosis after successfulimplantation of drug-eluting stents.
JAMA. 2005;293:2126-2130.
Jaffe R, Strauss BH. Late and very late thrombosis of drug-eluting stents: evolvingconcepts and perspectives.
J Am Coll Cardiol. 2007;50:119-127.
Joner M, Finn AV, Farb A, et al. Pathology of drug-eluting stents in humans: delayed healing andlate thrombotic risk.
J Am Coll Cardiol. 2006;48:193-202.
Kaiser C, Brunner-La Rocca HP, et al; Incremental cost-effectiveness of drug-eluting stents compared withBASKET Investigators. a third-generation bare-metal stent in a real-world setting:
randomised Basel Stent Kosten Effektivitäts Trial (BASKET).
Lancet. 2005;366:921-929. Erratum in: Lancet. 2005;366:2086.
Kandzari DE, Leon MB, Popma JJ, et al; Comparison of zotarolimus-eluting and sirolimus-eluting stents inENDEAVOR III Investigators. patients with native coronary artery disease: a randomized
controlled trial.
J Am Coll Cardiol. 2006;48:2440-2447.
Kastrati A, Dibra A, Spaulding C, et al. Meta-analysis of randomized trials on drug-eluting stents vs. bare- metal stents in patients with acute myocardial infarction.
Eur Heart J. 2007;28:2706-2713.
Kastrati A, Mehilli J, Pache J, et al. Analysis of 14 trials comparing sirolimus-eluting stents with bare-metal stents.
N Engl J Med. 2007;356:1030-1039.
Kelbaek H, Terkelsen CJ, Helqvist S, et al. Randomized comparison of distal protection versus conventionaltreatment in primary percutaneous coronary intervention: the drugelution and distal protection in ST-elevation myocardial infarction(DEDICATION) trial.
J Am Coll Cardiol. 2008;51:899-905.
Kereiakes DJ, Wang H, Popma JJ, et al. Periprocedural and late consequences of overlapping Cyphersirolimus-eluting stents: pooled analysis of five clinical trials.
J Am Coll Cardiol. 2006;48:21-31.
Kim YH, Ahn JM, Park DW, et al. EuroSCORE as a predictor of death and myocardial infarction afterunprotected left main coronary stenting.
Am J Cardiol. 2006;98:1567-1570.
291
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Kimura M, Mintz GS, Carlier S, et al. Outcome after acute incomplete sirolimus-eluting stent appositionas assessed by serial intravascular ultrasound.
Am J Cardiol. 2006;98:436-442.
Kimura M, Mintz GS, Weissman NJ, et al. Meta-analysis of the Effects of paclitaxel-eluting stents versus bare-metal stents on volumetric intravascular ultrasound in patientswith versus without diabetes mellitus.
Am J Cardiol. 2008;101:1263-1268.
Krucoff MW, Kereiakes DJ, Petersen JL, et al; A novel bioresorbable polymer paclitaxel-eluting stent for theCOSTAR II Investigators Group. treatment of single and multivessel coronary disease: primary results
of the COSTAR (Cobalt Chromium Stent With Antiproliferative forRestenosis) II study.
J Am Coll Cardiol. 2008;51:1543-1552.
Laarman GJ, Suttorp MJ, Dirksen MT, et al. Paclitaxel-eluting versus uncoated stents in primary percutaneouscoronary intervention.
N Engl J Med. 2006;355:1105-1113.
Lagerqvist B, James SK, Stenestrand U, Lindbäck J, Long-term outcomes with drug-eluting stents versus bare-metal stentsNilsson T, Wallentin L; SCAAR Study Group. in Sweden.
N Engl J Med. 2007;356:1009-1019.
Liistro F, Fineschi M, Angioli P, et al. Effectiveness and safety of sirolimus stent implantation for coronaryin-stent restenosis: the TRUE (Tuscany Registry of Sirolimus forUnselected In-Stent Restenosis) Registry.
J Am Coll Cardiol. 2006;48:270-275.
Lotrionte M, Biondi-Zoccai GG, et al. Meta-analysis appraising high clopidogrel loading in patients undergoing percutaneous coronary intervention.
Am J Cardiol. 2007;100:1199-1206. Review.
Lüscher TF, Steffel J, Eberli FR, et al. Drug-eluting stent and coronary thrombosis: biological mechanismsand clinical implications.
Circulation. 2007;115:1051-1058.
Mackman N. Triggers, targets and treatments for thrombosis.
Nature. 2008;451:914-918. Review.
Marroquin OC, Selzer F, Mulukutla SR, et al. A comparison of bare-metal and drug-eluting stents for off-labelindications.
N Engl J Med. 2008;358:342-352.
Marzocchi A, Saia F, Piovaccari G, et al. Long-term safety and efficacy of drug-eluting stents: two-year resultsof the REAL (REgistro AngiopLastiche dell'Emilia Romagna)multicenter registry.
Circulation. 2007;115:3181-3188.
Mauri L, Hsieh WH, Massaro JM, Ho KK, D'Agostino R, Stent thrombosis in randomized clinical trials of drug-eluting stents.Cutlip DE. N Engl J Med. 2007;356:1020-1029.
Mehta RH, Leon MB, Sketch MH Jr; The relation between clinical features, angiographic findings, andENDEAVOR II Continued Access Registry. the target lesion revascularization rate in patients receiving the
Endeavor zotarolimus-eluting stent for treatment of native coronaryartery disease: an analysis of ENDEAVOR I, ENDEAVOR II, ENDEAVOR II Continued Access Registry, and ENDEAVOR III.
Am J Cardiol. 2007;100:62M-70M.
292
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Melikian N, Wijns W. Drug-eluting stents: a critique.
Heart. 2008;94:145-152. Review.
Mintz GS, Weissman NJ. Intravascular ultrasound in the drug-eluting stent era.
J Am Coll Cardiol. 2006;48:421-429.
Miyazawa A, Ako J, Hongo Y, et al; Comparison of vascular response to zotarolimus-eluting stent versusENDEAVOR III Investigators. sirolimus-eluting stent: intravascular ultrasound results from
ENDEAVOR III.
Am Heart J. 2008;155:108-113.
Morice MC, Colombo A, Meier B, et al; Sirolimus- vs paclitaxel-eluting stents in de novo coronary arteryREALITY Trial Investigators. lesions: the REALITY trial: a randomized controlled trial.
JAMA. 2006;295:895-904.
Morice MC, Serruys PW, Barragan P, et al. Long-term clinical outcomes with sirolimus-eluting coronary stents:five-year results of the RAVEL trial.
J Am Coll Cardiol. 2007;50:1299-1304.
Ong AT, Daemen J, van Hout BA, et al. Cost-effectiveness of the unrestricted use of sirolimus-eluting stentsvs. bare metal stents at 1- and 2-year follow-up: results from theRESEARCH Registry.
Eur Heart J. 2006;27:2996-3003.
Ormiston JA, Serruys PW, Regar E, et al. A bioabsorbable everolimus-eluting coronary stent system for patientswith single de-novo coronary artery lesions (ABSORB): a prospective open-label trial.
Lancet. 2008;371:899-907.
Palmerini T, Marzocchi A, Marrozzini C, et al. Comparison between coronary angioplasty and coronary artery bypass surgery for the treatment of unprotected left main coronaryartery stenosis (the Bologna Registry).
Am J Cardiol. 2006;98:54-59.
Park DW, Yun SC, Lee SW, et al. Long-term mortality after percutaneous coronary intervention withdrug-eluting stent implantation versus coronary artery bypass surgery for the treatment of multivessel coronary artery disease.
Circulation. 2008;117:2079-2086.
Pfisterer M, Brunner-La Rocca HP, Buser PT, et al; Late clinical events after clopidogrel discontinuation may limit theBASKET-LATE Investigators. benefit of drug-eluting stents: an observational study of drug-eluting
versus bare-metal stents.
J Am Coll Cardiol. 2006;48:2584-2591.
Pinto DS, Stone GW, Ellis SG, et al; Impact of routine angiographic follow-up on the clinical benefitsTAXUS-IV Investigators. of paclitaxel-eluting stents: results from the TAXUS-IV trial.
J Am Coll Cardiol. 2006;48:32-36.
Pinto Slottow TL, Waksman R. Overview of the 2007 Food and Drug Administration CirculatorySystem Devices Panel meeting on the endeavor zotarolimus-elutingcoronary stent.
Circulation. 2008;117:1603-1608.
Pocock SJ, Lansky AJ, Mehran R, et al. Angiographic surrogate end points in drug-eluting stent trials: a systematic evaluation based on individual patient data from 11 randomized, controlled trials.
J Am Coll Cardiol. 2008;51:23-32.
293
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Price MJ, Endemann S, Gollapudi RR, et al. Prognostic significance of post-clopidogrel platelet reactivity assessed by a point-of-care assay on thrombotic events after drug-eluting stent implantation.
Eur Heart J. 2008;29:992-1000.
Reicher B, Poston RS, Mehra MR, et al. Simultaneous “hybrid” percutaneous coronary intervention andminimally invasive surgical bypass grafting: feasibility, safety, andclinical outcomes.
Am Heart J. 2008;155:661-667.
Rodriguez AE, Maree AO, Mieres J, et al. Late loss of early benefit from drug-eluting stents when comparedwith bare-metal stents and coronary artery bypass surgery: 3 yearsfollow-up of the ERACI III registry.
Eur Heart J. 2007;28:2118-2125.
Ryan J, Cohen DJ. Are drug-eluting stents cost-effective? It depends on whom you ask.
Circulation. 2006;114:1736-1743.
Schömig A, Dibra A, Windecker S, et al. A meta-analysis of 16 randomized trials of sirolimus-eluting stentsversus paclitaxel-eluting stents in patients with coronary arterydisease.
J Am Coll Cardiol. 2007;50:1373-1380. Review.
Serruys PW, Daemen J, Morice MC, et al; . Three-year follow-up of the ARTS-II—Sirolimus-eluting stents forARTS II Investigators the treatment of patients with multivessel coronary artery disease.
EuroInterv. 2007;3:450-459.
Serruys PW, Sianos G, Abizaid A, et al. The effect of variable dose and release kinetics on neointimal hyperplasia using a novel paclitaxel-eluting stent platform: the Paclitaxel In-Stent Controlled Elution Study (PISCES).
J Am Coll Cardiol. 2005;46:253-260.
Seung KB, Park DW, Kim YH, et al. Stents versus coronary-artery bypass grafting for left main coronary artery disease.
N Engl J Med. 2008;358:1781-1792.
Sianos G, Papafaklis MI, Daemen J, et al. Angiographic stent thrombosis after routine use of drug-elutingstents in ST-segment elevation myocardial infarction: the importanceof thrombus burden.
J Am Coll Cardiol. 2007;50:573-583.
Siqueira DA, Abizaid AA, Costa J de R, et al. Late incomplete apposition after drug-eluting stent implantation:incidence and potential for adverse clinical outcomes.
Eur Heart J. 2007;28:1304-1309.
Spaulding C, Daemen J, Boersma E, Cutlip DE, A pooled analysis of data comparing sirolimus-eluting stents withSerruys PW. bare-metal stents.
N Engl J Med. 2007;356:989-997.
Spaulding C, Henry P, Teiger E, et al; Sirolimus-eluting versus uncoated stents in acute myocardial TYPHOON Investigators. infarction.
N Engl J Med. 2006;355:1093-1104;
Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, and outcomes of premature discontinuationof thienopyridine therapy after drug-eluting stent placement: resultsfrom the PREMIER registry.
Circulation. 2006;113:2803-2809.
294
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Steigen TK, Maeng M, Wiseth R, et al; Randomized study on simple versus complex stenting of coronaryNordic PCI Study Group. artery bifurcation lesions: the Nordic bifurcation study.
Circulation. 2006;114:1955-1961.
Steinberg DH, Pinto Slottow TL, et al. Impact of in-stent restenosis on death and myocardial infarction.
Am J Cardiol. 2007;100:1109-1113.
Stone GW, Ellis SG, Colombo A, et al. Offsetting impact of thrombosis and restenosis on the occurrence ofdeath and myocardial infarction after paclitaxel-eluting and bare-metal stent implantation.
Circulation. 2007;115:2842-2847.
Stone GW, Ellis SG, O'Shaughnessy CD, et al; Paclitaxel-eluting stents vs vascular brachytherapy for in-stent resteno-TAXUS V ISR Investigators. sis within bare-metal stents: the TAXUS V ISR randomized trial.
JAMA. 2006;295:1253-1263.
Stone GW, Midei M, Newman W, Sanz M, et al; Comparison of an everolimus-eluting stent and a paclitaxel-elutingSPIRIT III Investigators. stent in patients with coronary artery disease: a randomized trial.
JAMA. 2008;299:1903-1913.
Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronarystents.
N Engl J Med. 2007;356:998-1008.
Svilaas T, Vlaar PJ, van der Horst IC, et al. Thrombus aspiration during primary percutaneous coronaryintervention.
N Engl J Med. 2008;358:557-567.
Taggart DP, Kaul S, Boden WE, et al. Revascularization for unprotected left main stem coronary arterystenosis stenting or surgery.
J Am Coll Cardiol. 2008;51:885-892.
Togni M, Eber S, Widmer J, et al. Impact of vessel size on outcome after implantation of sirolimus-eluting and paclitaxel-eluting stents: a subgroup analysis of theSIRTAX trial.
J Am Coll Cardiol. 2007;50:1123-1131.
Tu JV, Bowen J, Chiu M, et al. Effectiveness and safety of drug-eluting stents in Ontario.
N Engl J Med. 2007;357:1393-1402.
Valgimigli M, Campo G, Arcozzi C, et al. Two-year clinical follow-up after sirolimus-eluting versus bare-metal stent implantation assisted by systematic glycoprotein IIb/IIIaInhibitor Infusion in patients with myocardial infarction: resultsfrom the STRATEGY study.
J Am Coll Cardiol. 2007;50:138-145.
Valgimigli M, Campo G, Percoco G, et al; Multicentre Comparison of angioplasty with infusion of tirofiban or abciximabEvaluation of Single High-Dose Bolus Tirofiban vs and with implantation of sirolimus-eluting or uncoated stents forAbciximab With Sirolimus-Eluting Stent or Bare Metal acute myocardial infarction: the MULTISTRATEGY randomized Stent in Acute Myocardial Infarction Study trial.(MULTISTRATEGY) Investigators. JAMA. 2008;299:1788-1799.
Valgimigli M, van Mieghem CA, Ong AT, et al. Short- and long-term clinical outcome after drug-eluting stent implantation for the percutaneous treatment of left main coronary artery disease: insights from the Rapamycin-Eluting and TaxusStent Evaluated At Rotterdam Cardiology Hospital registries (RESEARCH and T-SEARCH).
Circulation. 2005;111:1383-1389.
295
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers

Van Beusekom HM, Saia F, Zindler JD, et al. Drug-eluting stents show delayed healing: paclitaxel more pronounced than sirolimus.
Eur Heart J. 2007;28:974-979.
Van der Hoeven BL, Liem SS, Jukema JW, et al. Sirolimus-eluting stents versus bare-metal stents in patients withST-segment elevation myocardial infarction: 9-month angiographicand intravascular ultrasound results and 12-month clinical outcome results from the MISSION! Intervention Study.
J Am Coll Cardiol. 2008;51:618-626.
Van Mieghem CA, Cademartiri F, Mollet NR, et al. Multislice spiral computed tomography for the evaluation of stentpatency after left main coronary artery stenting: a comparison withconventional coronary angiography and intravascular ultrasound.
Circulation. 2006;114:645-653.
Vermeersch P, Agostoni P, Verheye S, et al. Randomized double-blind comparison of sirolimus-eluting stent versus bare-metal stent implantation in diseased saphenous veingrafts: six-month angiographic, intravascular ultrasound, andclinical follow-up of the RRISC Trial.
J Am Coll Cardiol. 2006;48:2423-2431.
Vermeersch P, Agostoni P, Verheye S, et al; DELAYED Increased late mortality after sirolimus-eluting stents versus RRISC (Death and Events at Long-term follow-up AnalYsis: bare-metal stents in diseased saphenous vein grafts: results from Extended Duration of the Reduction of Restenosis In the randomized DELAYED RRISC Trial.Saphenous vein grafts with Cypher stent) Investigators. J Am Coll Cardiol. 2007;50:261-267.
Wessely R, Kastrati A, Mehilli J, Dibra A, Pache J, Randomized trial of rapamycin- and paclitaxel-eluting stents withSchömig A. identical biodegradable polymeric coating and design.
Eur Heart J. 2007;28:2720-2725.
Williams DO, Abbott JD, Kip KE; DEScover Investigators. Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug-eluting stents: report of theDEScover Registry.
Circulation. 2006;114:2154-2162.
Windecker S, Remondino A, Eberli FR, et al. Sirolimus-eluting and paclitaxel-eluting stents for coronary revas-cularization.
N Engl J Med. 2005;353:653-662.
Wiviott SD, Braunwald E, McCabe CH, et al; Intensive oral antiplatelet therapy for reduction of ischaemic eventsTRITON-TIMI 38 Investigators. including stent thrombosis in patients with acute coronary syndromes
treated with percutaneous coronary intervention and stenting in theTRITON-TIMI 38 trial: a subanalysis of a randomised trial.
Lancet. 2008;371:1353-1363.
Yamaguchi T, Terashima M, Akasaka T, et al. Safety and feasibility of an intravascular optical coherence tomography image wire system in the clinical setting.
Am J Cardiol. 2008;101:562-567.
296
Dialogues in Cardiovascular Medicine - Vol 13 . No. 4 . 2008
Bibliography of One Hundred Key Papers