Uncertainty in measurement for 43 biochemistry ... LTCV PBQ.pdf · try, this is particularly...
12
Clin Chem Lab Med 2015; aop Gladys Matar*, Bernard Poggi, Roland Meley, Chantal Bon, Laurence Chardon, Karim Chikh, Anne-Claude Renard, Catherine Sotta, Jean-Christophe Eynard, Regine Cartier and Richard Cohen Uncertainty in measurement for 43 biochemistry, immunoassay, and hemostasis routine analytes evaluated by a method using only external quality assessment data DOI 10.1515/cclm-2014-0942 Received September 24, 2014; accepted February 19, 2015 Abstract Background: International organizations require from medical laboratories a quantitative statement of the uncertainty in measurement (UM) to help interpret patient results. The French accreditation body (COFRAC) recom- mends an approach (SH GTA 14 IQC/EQA method) using both internal quality control (IQC) and external quality assessment (EQA) data. The aim of this work was to vali- date an alternative way to quantify UM using only EQA results without any need for IQC data. This simple and practical method, which has already been described as the long-term evaluation of the UM (LTUM), is based on linear regression between data obtained by participants in EQA schemes and target values. We used it for 43 routine analytes covering biochemistry, immunoassay, and hemo- stasis fields. Methods: Data from 50 laboratories participating in Pro- BioQual (PBQ) EQA schemes over 25 months were used to obtain estimates of the median and 90th percentile LTUM and to compare them to the usual analytical goals. Then, the two UM estimation methods were compared using data from 20 laboratories participating in both IQC and EQA schemes. Results: Median LTUMs ranged from 2.9% (sodium) to 16.3% (bicarbonates) for biochemistry analytes, from 12.6% (prothrombin time) to 18.4% (factor V) for hemosta- sis analytes when using the mean of all participants, and were around 10% for immunoassays when using the peer- group mean. Median LTUMs were, in most cases, slightly lower than those obtained with the SH GTA 14 method, whatever the concentration level. Conclusions: LTUM is a simple and convenient method that gives UM estimates that are reliable and comparable to those of recommended methods. Therefore, proficiency testing (PT) organizers are allowed to provide participants with an additional UM estimate using only EQA data and which could be updated at the end of each survey. Keywords: external quality assessment; internal quality control; long-term analytical coefficient of variation; pro- ficiency testing; uncertainty in measurement. List of abbreviations: AB, accuracy bias; AFP, α-fetoprotein; AL, acceptable limit; ALAT, alanine ami- notransferase; ALP, alkaline phosphatase; ANOVA, analy- sis of variance; AP, all participant results; aPTT, activated partial thromboplastin time; ASAT, aspartate aminotrans- ferase; CB, constant bias; CEA, carcinoembryonic antigen; CK, creatine kinase; CV WL , within-laboratory coefficient *Corresponding author: Gladys Matar, ProBioQual, 9 rue Professeur Florence 69003, Lyon, France, E-mail: [email protected] Bernard Poggi and Chantal Bon: Service de Biochimie et Biologie moléculaire, Hôpital de la Croix-Rousse, Hospices Civils de Lyon, Lyon, France; and ProBioQual, Lyon, France Roland Meley: Service d’Hématologie, St Etienne, France; and ProBioQual, Lyon, France Laurence Chardon: Service de Biochimie et Biologie moléculaire, Hôpital Edouard Herriot, Hospices Civils de Lyon, Lyon, France; and ProBioQual, Lyon, France Karim Chikh: Service de Biochimie et Biologie moléculaire, Centre Hospitalier Lyon Sud, Hospices Civils de Lyon, Pierre-Bénite, France; and ProBioQual, Lyon, France Anne-Claude Renard, Catherine Sotta and Jean-Christophe Eynard: ProBioQual, Lyon, France Regine Cartier: Service de Biochimie et Biologie moléculaire, Groupement Hospitalier Est, Hospices Civils de Lyon, Bron, France; and ProBioQual, Lyon, France Richard Cohen: Service de Biochimie et Biologie moléculaire, Hôpital Edouard Herriot, Hospices Civils de Lyon, Lyon, France; Université Claude Bernard Lyon-1, ISPB Faculté de pharmacie, MATEIS UMR CNRS 5510, France; and ProBioQual, Lyon, France Authenticated | [email protected] author's copy Download Date | 3/27/15 10:16 AM
Transcript of Uncertainty in measurement for 43 biochemistry ... LTCV PBQ.pdf · try, this is particularly...

Clin Chem Lab Med 2015; aop
Gladys Matar * , Bernard Poggi , Roland Meley , Chantal Bon , Laurence Chardon , Karim Chikh ,
Anne-Claude Renard , Catherine Sotta , Jean-Christophe Eynard , Regine Cartier
and Richard Cohen
Uncertainty in measurement for 43 biochemistry, immunoassay, and hemostasis routine analytes evaluated by a method using only external quality assessment data
DOI 10.1515/cclm-2014-0942
Received September 24 , 2014 ; accepted February 19 , 2015
Abstract
Background: International organizations require from
medical laboratories a quantitative statement of the
uncertainty in measurement (UM) to help interpret patient
results. The French accreditation body (COFRAC) recom-
mends an approach (SH GTA 14 IQC/EQA method) using
both internal quality control (IQC) and external quality
assessment (EQA) data. The aim of this work was to vali-
date an alternative way to quantify UM using only EQA
results without any need for IQC data. This simple and
practical method, which has already been described as
the long-term evaluation of the UM (LTUM), is based on
linear regression between data obtained by participants in
EQA schemes and target values. We used it for 43 routine
analytes covering biochemistry, immunoassay, and hemo-
stasis fields.
Methods: Data from 50 laboratories participating in Pro-
BioQual (PBQ) EQA schemes over 25 months were used to
obtain estimates of the median and 90th percentile LTUM
and to compare them to the usual analytical goals. Then,
the two UM estimation methods were compared using
data from 20 laboratories participating in both IQC and
EQA schemes.
Results: Median LTUMs ranged from 2.9% (sodium) to
16.3% (bicarbonates) for biochemistry analytes, from
12.6% (prothrombin time) to 18.4% (factor V) for hemosta-
sis analytes when using the mean of all participants, and
were around 10% for immunoassays when using the peer-
group mean. Median LTUMs were, in most cases, slightly
lower than those obtained with the SH GTA 14 method,
whatever the concentration level.
Conclusions : LTUM is a simple and convenient method
that gives UM estimates that are reliable and comparable
to those of recommended methods. Therefore, proficiency
testing (PT) organizers are allowed to provide participants
with an additional UM estimate using only EQA data and
which could be updated at the end of each survey.
Keywords: external quality assessment; internal quality
control; long-term analytical coefficient of variation; pro-
ficiency testing; uncertainty in measurement.
List of abbreviations: AB, accuracy bias; AFP,
α -fetoprotein; AL, acceptable limit; ALAT, alanine ami-
notransferase; ALP, alkaline phosphatase; ANOVA, analy-
sis of variance; AP, all participant results; aPTT, activated
partial thromboplastin time; ASAT, aspartate aminotrans-
ferase; CB, constant bias; CEA, carcinoembryonic antigen;
CK, creatine kinase; CV WL
, within-laboratory coefficient
*Corresponding author: Gladys Matar, ProBioQual, 9 rue Professeur
Florence 69003, Lyon, France, E-mail: [email protected]
Bernard Poggi and Chantal Bon: Service de Biochimie et Biologie
mol é culaire, H ô pital de la Croix-Rousse, Hospices Civils de Lyon,
Lyon, France ; and ProBioQual, Lyon, France
Roland Meley: Service d ’ H é matologie, St Etienne, France ; and
ProBioQual, Lyon, France
Laurence Chardon: Service de Biochimie et Biologie mol é culaire,
H ô pital Edouard Herriot, Hospices Civils de Lyon, Lyon, France ; and
ProBioQual, Lyon, France
Karim Chikh: Service de Biochimie et Biologie mol é culaire, Centre
Hospitalier Lyon Sud, Hospices Civils de Lyon, Pierre-B é nite, France ;
and ProBioQual, Lyon, France
Anne-Claude Renard, Catherine Sotta and Jean-Christophe Eynard: ProBioQual, Lyon, France
Regine Cartier: Service de Biochimie et Biologie mol é culaire,
Groupement Hospitalier Est, Hospices Civils de Lyon, Bron, France ;
and ProBioQual, Lyon, France
Richard Cohen: Service de Biochimie et Biologie mol é culaire,
H ô pital Edouard Herriot, Hospices Civils de Lyon, Lyon, France ;
Universit é Claude Bernard Lyon-1, ISPB Facult é de pharmacie,
MATEIS UMR CNRS 5510, France ; and ProBioQual, Lyon, France
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

2 Matar et al.: Uncertainty in measurement estimates from external quality assessment
of variation; COFRAC, French accreditation body; DBMS,
database management system; EQA, external quality
assessment; EUROLAB, European Federation of National
Associations of Measurement, Testing, and Analyti-
cal Laboratories; FSH, follicle stimulating hormone;
FT3, free triiodothyronine; FT4, free thyroxine; GGT,
γ -glutamyltransferase; GUM, guide to the expression of
uncertainty in measurement; IFCC, International Federa-
tion of Clinical Chemistry and Laboratory Medicine; ILAC,
International Laboratory Accreditation Cooperation;
IOLM, International Organization of Legal Metrology; IQC,
internal quality control; ISO, International Organization
for Standardization; hCG, human chorionic gonadotropin;
LCV, long-term analytical coefficient of variation; LDH,
lactate dehydrogenase; LH, luteinizing hormone; LTB,
long-term bias; LTUM, long-term uncertainty in measure-
ment; PB, proportional bias; PBQ, ProBioQual; PG, peer
group; ProT, prothrombin time; PSA, prostate-specific
antigen; PT, proficiency testing; RE, random error; SE, sys-
tematic error; SH GTA 14, COFRAC Accreditation Technical
Guide for UM; s WL
, within-laboratory standard deviation;
TE, total error; TSH, thyroid stimulating hormone; um,
standard uncertainty in measurement; UM, uncertainty in
measurement (or expanded uncertainty in measurement
for a 95% level of confidence).
Introduction The National Institute of Standards and Technology speci-
fies that: “ a measurement result is complete only when accompanied by a quantitative statement of its uncertainty. The uncertainty is required in order to decide if the result is adequate for its intended purpose and to ascertain if it is consistent with other similar results ” [1] . In clinical chemis-
try, this is particularly important to ensure that test results
are fit for their clinical purpose and do not compromise
patient care. The uncertainty in measurement (UM) could,
thereby, be used to assess the quantitative performances
of analytical procedures [2] . Thus, medical laboratories
are expected to estimate the uncertainty for test measure-
ments, especially since many international organizations,
such as International Federation of Clinical Chemistry
and Laboratory Medicine (IFCC) [3] , International Labora-
tory Accreditation Cooperation (ILAC) [4] , International
Organization of Legal Metrology (IOLM) [5] and Interna-
tional Organization for Standardization (ISO) [6, 7] [ISO
17025 (2005) and ISO 15189 (2012)], required it. According
to the ISO 15189 (2012) 5.5.1.4 standard: “ The laboratory shall determine the uncertainty of measurement for each
procedure in the analytical phase used to record the meas-ured values of patient samples ” .
In the aim to provide terminology and methodology for
expressing UM, a joint working group consisting of experts
from these and other organizations published a “ Guide to the
expression of uncertainty in measurement ” (GUM) [8] , which
establishes the general rules for evaluating and expressing
UM. The GUM presents different approaches to estimate UM
using a mathematical theory and experimental observation,
so-called “ modeling approaches ” . These methods were
compared to alternative “ empirical approaches ” in the tech-
nical report published by European Federation of National
Associations of Measurement, Testing, and Analytical Lab-
oratories (EUROLAB) [9] , which classifies these different
approaches in two categories: the intra- and inter-laboratory
approach. In the first category, estimation of the UM is based
on the GUM “ modeling approaches ” or on individual data
combinations available from reference methods and inter-
nal quality control (IQC), providing an estimation of repeat-
ability, within-laboratory reproducibility, and bias. In the
second category, the UM estimation is based on validation
method or proficiency testing (PT) data from the labora-
tory ’ s results obtained during participation in an external
quality assessment (EQA).
According to the “ empirical approaches ” , the UM is
estimated from the imprecision and the bias. The impre-
cision, in general, is quantified by the within-laboratory
reproducibility standard deviation (s WL
), or coefficient of
variation (CV WL
) obtained under within-laboratory repro-
ducibility conditions (often called “ intermediate condi-
tions ” ): different operators, reagent batches, calibrators,
or long-time repetition. The bias is quantified by the devi-
ations of measurement results from corresponding refer-
ence values. Thus, a combination of the intralaboratory
and the interlaboratory approaches is possible using IQC
data to estimate the imprecision (s WL
), and the EQA labora-
tory ’ s results to estimate the bias. This combined method
was suggested in the EUROLAB Technical report, and
recommended in the SH GTA 14 [10] , the technical guide
for the UM estimation, published by COFRAC (the French
accreditation body) in 2011.
As the UM is used to assess the performances of quan-
titative analytical procedures, Meijer et al. [11] proposed to
express the UM as the long-term analytical performance
(LTUM) of a laboratory using only its EQA results over a
long period of time. The imprecision is then expressed by
the long-term analytical CV (LCV) and the deviation of the
laboratory ’ s result from the measurand assigned value is
determined by the long-term bias (LTB).
In order to provide participants with an estimate of the
UM by a different method and to allow the PT organizer to
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

Matar et al.: Uncertainty in measurement estimates from external quality assessment 3
include UM estimation in the reports established at the end
of each survey, we quantified the LTUM of a large panel of
routine analytes assayed in a medical laboratory. We used
data of 50 laboratories participating in ProBioQual (PBQ)
EQA programs in biochemistry, immunoassay, and hemo-
stasis over a long period of time (25 months). Moreover,
data from 20 laboratories participating in both IQC and
EQA schemes were used to compare the LTUM and the SH
GTA 14 (IQC/EQA) UM estimation methods and to point out
the advantages and the drawbacks of each approach.
Materials and methods ProBioQual
PBQ (http://www.probioqual.com) is a French non-profi t, non-gov-
ernmental association established in 1972 by biologists to promote
training and quality control in medical laboratories. As a PT provider,
PBQ proposes six IQC and 26 EQAs in biochemistry, immunology,
hematology, serology, and drug tests, including over 200 diff erent
analytes. Thus, almost 1700 international medical laboratories par-
ticipate in at least one of these programs, allowing an assessment of
their analytical procedures.
Survey specimens and laboratories
Laboratories received, per year, human sera lyophilized specimens
(24 for biochemistry, or 12 for immunoassay), or 16 human citrated
plasmas lyophilized specimens for hemostasis EQA schemes. Intra-
and inter-vials homogeneity tests results showed that lyophilization
procedure was successfully applied but the recovery of this procedure
was not tested. All survey samples were shipped at room temperature
and then stored in the laboratories at 2 ° C/8 ° C until reconstitution.
Simulation tests on the survey specimens have proved their stability
during all the shipment process. According to an established sched-
ule, the participants processed each specimen as if it was a patient
sample, using routine methods to determine the concentration of
each measurand. The main commercial methods, reagents and
devices used by the laboratories to assess the EQA schemes samples
are listed in the Table 1 . Aft er results submission on the PBQ website,
under anonymous laboratory code number, statistical evaluation
was performed according to the ISO guideline 13528 (2005) [12] , as
it is recommended in the PT-specifi c standard ISO 17043 (2010) [13] .
The ISO 13528 (2005) robust algorithm A was applied to calculate the
mean of submitted results, which was used as the consensus value.
No further statistical analysis of outliers was performed. The iterative
process was terminated when the mean and CV estimates were sta-
ble and the percentage of values modifi ed then did not exceed 15%.
Thereby, two consensus values were determined: the fi rst one was
the mean of all participants ’ results (AP) and the second was that of
laboratories using the same assay type of method, the same reagents
and the same device, forming a peer group (PG). A minimum of six
participants was required to apply the robust algorithm. The labora-
tories received a PT report including the results of all participants,
with an individual evaluation of the laboratory performance. PBQ
provided advice on the interpretation of the statistical analysis and
comments on participants ’ performance.
Each laboratory participating to PBQ EQA Schemes had an
anonymous code number. The laboratories participating to this study
were selected randomly from the beginning, the middle, and the end
of our anonymous code number list. The new ones had the latest
numbers and the older had the fi rst numbers. Like that, the selected
laboratories represented experienced and non-experienced labora-
tory in our EQA schemes. Fift y laboratories participating in PBQ bio-
chemistry (915 participants in 2013), immunoassay (892 participants
in 2013) or hemostasis (848 participants in 2013) EQA schemes over
25 months (January 2011 until January 2013) were selected to test the
LTUM method estimation. This prolonged period of time was suffi -
cient to take into account a number of PT surveys covering a wide
concentration range of measurands, hence allowing a real long-term
analytical performance evaluation. Since these programs did not
have the same survey frequency (weekly, monthly, or 2-monthly),
between eight and 45 results were included in the evaluation of the
LTUM for each laboratory. For the comparison between LTUM and SH
GTA 14 (IQC/EQA) methods, data from 20 laboratories participating
in both IQC (153 and 170 participants in biochemistry and hemostasis
2013 IQC schemes, respectively) and EQA programs, were used over
the same period of time.
LTUM method
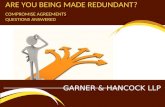
The LTUM method used the linear regression model (y = bx + a), as
described by Meijer et al. [11] , to express the laboratory value (y) as
a function of the target value (x), where b is the slope and a is the
intercept point ( Figure 1 ). The total error (TE) is presented in Figure 1
as the diff erence between each data point (the laboratory value) and
the identity line y = x (the target value). Thus, it could be assimilated to
the accuracy bias (AB) or to the UM. The TE is composed of a random
error (RE) and a systematic error (SE), itself composed of a constant
(CB) and a proportional biases (PB). The RE corresponds to the disper-
sion of the data points around the regression line caused by routine
operating conditions variability (as multiple calibrators and reagent
batches, multiple operators, equipment maintenance, etc.) over the
EQA period of time, and is quantifi ed by the LCV. SE is represented
by the deviation of the regression line from the identity line and cor-
responds to the LTB. The CB (vertical distance between parallel and
identity lines on Figure 1) is equal to the intercept a of the regression
line at every level within the concentration range. It could be due to
the so-called “ matrix-eff ect ” . The PB is represented, at each concen-
tration level, by the diff erence between the regression and parallel
lines. Its intensity increases with concentration level and could be due
to calibration errors. The LCV and the LTB represent the two compo-
nents of the UM, which could be determined as follows [11] :
2 2UM 1.96 um 1.96 LCV LTB= × = × + (1)
y/xs
LCVx
=
(2)
2 2 2
x
n 1(b 1) s ( y x )
nLTBx
− ⋅ − ⋅ + −=
(3)
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

4 Matar et al.: Uncertainty in measurement estimates from external quality assessment
Tabl
e 1 :
Bio
che
mis
try,
he
mo
sta
sis
an
d i
mm
un
oa
ss
ay
ma
in c
om
me
rcia
l m
eth
od
s a
nd
de
vice
s.
AN
AL
YT
ES
ME
TH
OD
S
Bic
arb
on
ates
SP
EC
TRA
L R
EF
LEC
TOM
ETR
YV
itros
Dev
ice
UV
EN
ZY
MA
TIC
ME
THO
DS
PH
KIN
ETI
CS
To
tBili
rub
inE
NZ
YM
ATI
CS
ME
THO
DS
3 a
lpha
-HD
S p
hoto
met
ry
Cal
ciu
m
SP
EC
TRA
L R
EF
LEC
TOM
ETR
YV
itros
Dev
ice
SE
LEC
TIV
E E
LEC
TRO
DE
S
SP
EC
TRA
L P
HO
TOM
ETR
Y N
M-B
AP
TA
SP
EC
TRA
L P
HO
TOM
ETR
Y
O.C
RE
SO
L P
HTA
LEIN
SP
EC
TRA
L P
HO
TOM
ETR
Y A
RS
EN
AZ
O II
I
Ch
ole
ster
ol
SP
EC
TRA
L R
EF
LEC
TOM
ETR
YV
itros
Dev
ice
ES
TER
AS
E O
XY
DA
SE
PE
RO
XY
DA
SE
-
chro
mog
en.
phen
olic
(PA
P)
ES
TER
AS
E O
XY
DA
SE
PE
RO
XY
DA
SE
-
chro
mog
en.
non
phen
olic
(PA
P)
Cre
atin
ine
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
JAF
FE
-S
tand
ardi
zed
IDM
S -
Cor
rect
ed
JAF
FE
-S
tand
ardi
zed
IDM
S N
on c
orre
cted
JAF
FE
-N
on S
tand
ardi
zed
IDM
S -
Non
Cor
rect
ed
EN
ZY
MA
TIC
S M
ETH
OD
S
Iro
nS
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
e
FE
RE
NE
-D
IRE
CT
FE
RR
OZ
INE
Pho
tom
etry
Glu
cose
HE
XO
KIN
AS
E
SP
EC
TRA
L R
EF
LEC
TOM
ETR
YV
itros
Dev
ice
GO
D -
PO
D "
Trin
der"
GO
D E
LEC
TRO
DE
Mag
nes
ium
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y V
itros
Dev
ice
SP
EC
TRA
L P
HO
TOM
ETR
Y -
AR
SE
NA
ZO
SP
EC
TRA
L P
HO
TOM
ETR
Y C
ALM
AG
ITE
SP
EC
TRA
L P
HO
TOM
ETR
Y -
VA
RIE
D C
OLO
R
EN
ZY
MA
TIC
S M
ETH
OD
S
Ph
osp
hat
esS
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
e
Fer
rous
sulfa
te re
duci
ngag
ent
PH
OS
PH
OM
OLY
BD
ATE
FR
EE
RE
DU
CTI
ON
(U.V
.)
Cl/K
/Na
DIR
EC
T P
OTE
NTI
OM
ETR
Y
IND
IRE
CT
PO
TEN
TIO
ME
TRY
Tri
gly
ceri
de
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
GP
O P
AP
ME
THO
D -
mea
sure
men
t of
tot
al g
lyce
rol
Ura
te
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
UR
ICA
SE
PE
RO
XY
DA
SE
CH
RO
MO
GE
NE
DIR
.
UR
ICA
SE
PE
RO
XY
DA
SE
CH
RO
MO
GE
NE
+ A
OD
UR
ICA
SE
U.V
. -29
3 nm
DIR
EC
TE
Ure
aS
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
e
UR
EA
SE
U.V
. -ki
netic
s
UR
EA
SE
with
ELE
CTR
OD
E -
Con
duct
omet
ry
BIO
CH
EM
IST
RY
AN
AL
YT
ES
AS
SE
SS
ME
NT
SU
PP
LIE
RD
EV
ICE
SA
BB
OT
T
Dia
gn
ost
icA
rchi
tect
c80
00
Arc
hite
ct c
4000
BE
CK
MA
NU
niC
elD
xC60
0 / 6
00i
Uni
Cel
DxC
800
AU
400
/ AU
480
/ A
U 6
40/
AU
680
RO
CH
E
Dia
gn
ost
ics
Mod
ular
P -
PP
-D
P
Cob
as(c
501-
c502
)C
obas
Inte
gra
400
Cob
asIn
tegr
a80
0H
itach
i 717
SIE
ME
NS
Adv
ia16
50/1
800
Dim
ensi
on E
xLD
imen
sion
RxL
HM
D
imen
sion
Vis
ta
Dim
ensi
on X
pand
TH
ER
MO
S
CIE
NT
IFIC
Kon
elab
60/i
and
Kon
elab
Prim
e 60
/i
Kon
elab
30/i
and
Kon
elab
Prim
e 30
/i
OR
TH
O
Clin
ical
Dia
gn
ost
ic
Vitr
os5.
1 F
S
Vitr
os35
0
IMM
UN
OA
SS
AY
AN
AL
YT
ES
AS
SE
SS
ME
NT
SU
PP
LIE
RD
EV
ICE
S
AB
BO
TT
Dia
gn
osti
cA
rchi
tect
i100
0/20
00
BE
CK
MA
NU
nice
lDX
i800
-60
0i
Acc
ess/
DxI
/DxC
/Lxi
BIO
ME
RIE
UX
Vid
as
RO
CH
E D
iag
no
stic
s
Cob
as e
601
(cob
as 6
000
serie
s)
Mod
ular
E (
170)
-E
E
Cob
as e
602
(cob
as 8
000
serie
s)
Ele
csys
2010
Cob
as e
411
(cob
as 4
000
serie
s)
SIE
ME
NS
AD
VIA
Cen
taur
/Cen
taur
XP
Dim
ensi
on V
ista
Imm
ulite
2000
/ 200
0 X
Pi
TH
ER
MO
SC
IEN
TIF
ICK
rypt
or/K
rypt
orco
mpa
ct
TO
SO
H b
iosc
ien
ces
AIA
200
0
OR
TH
O C
linic
alD
iag
no
stic
sV
itros
5600
HE
MO
ST
AS
IS A
NA
LY
TE
S A
SS
ES
SM
EN
T
SU
PP
LIE
RD
EV
ICE
SM
ET
HO
DS
RE
AG
EN
TS
Inst
rum
enta
tion
L
abo
rato
ryF
RA
NC
E
AC
L E
LITE
PR
O
(700
0, 8
000,
900
0)O
PTI
CA
LD
ETE
CTI
ON
Hem
osil
Ant
ithro
mbi
nH
emos
ilA
ntith
rom
bin
liqui
deIL
Hem
osil
Fib
rinog
enC
laus
sIL
Hem
ostil
TP F
ibH
S P
lus
IL H
emos
ilR
ecom
bipl
astin
eIL
Hem
osil
AP
TT S
PIL
Hem
osil
Syn
thas
ilP
lasm
a de
ficie
nten
fac
teur
V
AC
L TO
P
RO
CH
E
Dia
gn
ost
ics
HIT
AC
HI,
MO
DU
LAR
OP
TIC
AL
DE
TEC
TIO
NA
ntith
rom
bine
C
OB
AS
, IN
TEG
RA
SIE
ME
NS
Sys
mex
CA
(CA
-500
, C
A-1
500,
CA
-700
0)O
PTI
CA
LD
ETE
CTI
ON
Ber
ichr
omA
T II
IIn
nova
nce
Ant
ithro
mbi
neP
lasm
a ex
empt
de
fact
eur V
Mul
tifib
ren
UD
ade
Thro
mbi
ne
Thro
mbo
relS
Inno
vin
(Thr
omb.
R
ecom
bina
nte)
Pat
hrom
tinS
LA
ctin
FS
SY
SM
EX
CS
(2
000/
2000
i, 21
00/2
100i
, 510
0)B
CT,
BC
S, B
CS
(X
P)
ST
AG
OS
TA, S
TA c
ompa
ct,
STA
-R, S
TA-R
E
volu
tion
VIS
CO
SIM
ETR
ICA
L D
ETE
CTI
ON
Sta
chro
mA
T II
IS
TA d
efic
ient
en f
acte
ur V
Fib
ripre
stA
utom
ate
STA
Fib
rinog
en,
Néo
plas
tine
CI
Néo
plas
tine
CI P
LUS
CK
Pre
stP
TT A
utom
ate
Cep
hasc
reen
Tri
nit
y B
iote
ch
KC
4, K
C10
, KC
40M
EC
AN
ICA
L D
ETE
CTI
ON
Trin
iclo
tFib
rinog
ène
Kit
Trin
iclo
tAut
omat
ed
AP
TTTr
inic
lotA
PTT
HS
Opt
ion
2, 4
, 8D
estin
yM
ax, D
estin
yP
lus
OP
TIC
AL
DE
TEC
TIO
NC
oag-
A-M
ate
XC
AA
NA
LY
TE
SM
ET
HO
DS
AL
AT
/ AS
AT
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y V
itros
Dev
ice
IFC
C M
ETH
OD
S w
ithP
LPIF
CC
ME
THO
DS
with
outP
LP
Am
ylas
eS
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
eN
ITR
OP
HE
NY
L P
OLY
SA
CC
HA
RID
E N
P-G
3N
ITR
OP
HE
NY
L P
OLY
SA
CC
HA
RID
E N
P-G
5/G
6/G
7
CK
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
N-A
CE
TYL-
CY
STE
INE
IF
CC
Rec
omm
anda
tion
N-A
CE
TYL-
CY
STE
INE
oth
ers
GG
T
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
NO
N-C
AR
BO
XY
L S
UB
STR
ATE
C
AR
BO
XY
L S
UB
STR
ATE
C
AR
BO
XY
L S
UB
STR
ATE
IF
CC
Rec
omm
anda
tion
LD
H
SP
EC
TRA
L R
EF
LEC
TOM
ETR
Y
V
itros
Dev
ice
PY
RU
VA
TE S
UB
STR
ATE
-D
GK
CLA
CTA
TE S
UB
STR
ATE
-IF
CC
(L--
>P)
UV
ME
THO
DS
-IF
CC
(L-
->P
)P
YR
UV
ATE
SU
BS
TRA
TE -
OTH
ER
S
LIP
AS
ES
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
eC
OLO
RIM
ETR
Y
AL
PS
PE
CTR
AL
RE
FLE
CTO
ME
TRY
Vitr
osD
evic
eA
.M.P
. TA
MP
ON
(NO
N I
FC
C/S
FB
C)
A.M
.P. T
AM
PO
N (I
FC
C/S
FB
C)
A A’
B C
Lis
t o
f b
ioch
em
istr
y m
ain
co
mm
erc
ial
me
tho
ds
(A
) a
nd
of
the
ma
in d
evi
ces
us
ed
by
the
pa
rtic
ipa
nts
to
as
se
ss
bio
che
mis
try
(A ′ )
, h
em
os
tas
is (
B)
an
d i
mm
un
oa
ss
ay
(C)
an
aly
tes
. B
es
ide
s t
he
ma
in d
evi
ces
an
d d
ete
ctio
n m
eth
od
s,
rea
ge
nts
are
lis
ted
fo
r h
em
os
tas
is a
na
lyte
s a
ss
es
sm
en
t (B
).
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

Matar et al.: Uncertainty in measurement estimates from external quality assessment 5
combined data from IQC and calibration uncertainty. However, for
convenient use in medical laboratories, the COFRAC recommends the
third one which was well described by Fisicaro et al. [14, 15] . Briefl y,
the in-house validation method or IQC data were used to determine
imprecision, and the EQA laboratory data were used to calculate bias.
Calculation could be made either using concentration values (s WL
and
bias expressed as concentration units) or using relative values (CV WL
and bias expressed as a percentage of the assigned value) for the ran-
dom and the systematic component of error, respectively. Here, both
UM terms were expressed as percentages. Applying the uncertainty
propagation law, an estimation of UM was given by the following
equations:
2 2UM 1.96 u 1.96 u(IQC) u(EQA)= × = × +
(5)
WLs
u(IQC) CV 100m
= = ×
(6)
2
2
E
| E |u(EQA) s
3
⎛ ⎞= +⎜ ⎟⎝ ⎠
(7)
where CV = coeffi cient of variation, s WL
= within-
laboratory standard deviation, m = IQC laboratory mean,
− ⎛ ⎞−= = = ×⎜ ⎟− ⎝ ⎠∑ ∑ 2
i ii i
E(%) i
i
E (%) (E (%) E(%)) y xE(%) , S , E (%) 100
n n 1 x
and n = number of laboratory EQA results.
As required, UM should be determined at two concentration
levels at least corresponding to the critical clinical limits [16] . These
limits were chosen as specifi ed by Vassault et al. [17] for biochemistry
analytes and normal and pathologic levels were determined by PBQ
for hemostasis analytes. Only the EQA control samples correspond-
ing to the same concentration range as IQC samples were selected
among those used during the 25-month surveys.
Finally, the median UMs, calculated from 20 laboratories either
by the SH GTA 14 method or by the LTUM approach, were compared
at each of the two concentration levels.
Results
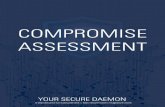
Biochemistry EQA schemes
The results of 50 laboratories participating in the PBQ
biochemistry EQA program were used to quantify LTUM
for 23 routine analytes including ions, substrates, and
enzymatic parameters, according to Equations 1 – 4. Two
different target values were considered for either that of
AP ( Figure 2 A), or that of the PG (Figure 2B), except for the
enzymatic analytes, for which only the PG target values
were taken into account because of the high dispersion
between AP results. To evaluate the performance of 50%
and 90% of the laboratories, median and 90th percentile
LTUM were calculated and compared (Figure 2) to two
analytical goals commonly used by laboratories for the
2
y/x 2
1s (y y)
(n 2 )
(x x)(y y)
(x x)
⎡ ⎤⎡ ⎤⎣ ⎦⎢ ⎥= − −⎢ ⎥− ⎣ ⎦
− −
−∑∑
∑
(4)
where um = standard uncertainty in measurement, UM = expanded
uncertainty in measurement for a 95% level of confi dence (k = 1.96
is the coverage factor), x = consensus value; x ̅ = mean value for x;
y = laboratory value; y ̅ = mean value for y; s x = standard error of x;
b = slope; s y/x
= variability of the regression line, based on the least-
squares method and n = number of laboratory EQA results.
For each of the 50 laboratories chosen as described above, LTUM
was evaluated using diff erent consensus values obtained from the
AP or PG groups. Calculation of specimen number n, LCV, LTB, um,
and expanded UM were realized by the database management sys-
tem (DBMS) generated by the 4D soft ware (V. 2012). For each survey,
any result deviating from the assigned value by > 3 standard devia-
tions of the comparison group ( | z | > 3) was identifi ed as an outlier
and discarded. This method is only valid for a normal distribution
and the number of results removed was < 3. As expected, the hypoth-
esis that data came from a normal distribution, appreciated by the
χ 2 goodness of fi t and Kolmogorov-Smirnov tests, was not rejected
when considering PG data and rejected when considering AP data
for most analytes. The LTUM evaluation was performed only when
n ≥ 8 results were available from a laboratory, except when EQA sam-
ples had to be split in two concentration levels for the comparison
study between the LTUM and SH GTA 14 methods (n ≥ 6). The reduc-
tion in the minimum data number for linear regression analysis did
not aff ect signifi cantly either the LTUM estimates or the conclusion of
this part of our study.
SH GTA 14 (IQC/EQA) method
The SH GTA 14 suggests four diff erent methods for the UM assess-
ment based on the GUM “ Modeling approach ” [8] , on data from
method validation, on combined data from IQC and EQA, and on
Regression line y = bx+ a
Identity line y=x
Consensus value x
a
EQA laboratory results y
Parallel line
RE
TESE
PB
CB
Figure 1: Linear regression model for the assessment of UM: y = bx + a.
CB, constant bias; PB, proportional bias; RE, random error; SE,
systematic error; TE, total error.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

6 Matar et al.: Uncertainty in measurement estimates from external quality assessment
validation method purpose. One was the expanded AB
defined for the medium concentration level by Vassault
et al. [17] from the state-of-the-art deduced from the expe-
rience of several French EQA organizers in 1999 and the
second was the desirable TE derived by Ricos et al. (http://
www.westgard.com/biodatabase1.htm) from biological
variations database. Analytical goals derived from the
state-of-the-art are less strict than those defined by biolog-
ical variations except for analytes whose biological vari-
ations are very high [bilirubin, iron, triglyceride, alanine
aminotransferase (ALAT), creatine kinase (CK), and
lipase]. Median AP LTUM was comprised between 2.9%
(sodium) and 16.3% (bicarbonates), while the median PG
LTUM range was 2.4% (sodium) to 13.7% (bicarbonates).
As expected, AP LTUM was higher than PG LTUM for the
majority of analytes. For some analytes (cholesterol, iron,
glucose, phosphate, potassium, sodium, and urea), close
estimates of the median LTUM were obtained whatever the
target value used. When the AP consensus mean was used
(Figure 2A), 90% or more laboratories fulfilled both LTUM
Bic
arbo
nate
s
Tot B
iliru
bin
Cal
cium
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Glu
cose
Mag
nesi
um
Pho
spha
te
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
Ure
a
19.6 23.5 4.5 4.9 13.7 17.6 19.6 9.8 11.8 11.0 6.9 3.5 15.7 13.7 15.7 16.3 13.8 6.2 6.2 7.1 12.8 6.0 6.2 10.0 5.4 3.5 2.9 10.1 6.4 8.9 23.3 24.5 9.7 9.0 10.4 18.7 12.0 10.1 13.4 8.7 5.3 4.6 15.4 13.4 15.1 4.9 26.9 2.6 1.5 9.0 8.9 30.7 7.0 4.8 10.1 5.6 0.7 26.0 12.0 15.6
Bic
arbo
nate
s
Tot B
iliru
bin
Cal
cium
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Glu
cose
Mag
nesi
um
Pho
spha
te
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
Ure
a
ALA
T
Am
ylas
e
AS
AT
CK
GG
T
LDH
Lipa
se
ALP
19.6 23.5 4.5 4.9 13.7 17.6 19.6 9.8 11.8 11.0 6.9 3.5 15.7 13.7 15.7 17.6 17.6 17.6 17.6 17.6 17.6 17.6 17.6
13.7 7.0 4.1 3.1 5.0 7.1 4.9 5.3 6.6 5.1 3.0 2.4 5.8 4.7 7.2 6.4 5.5 6.9 8.0 8.3 8.4 8.4 7.8
20.8 12.0 5.7 5.6 6.6 11.1 10.3 7.3 10.1 8.2 4.6 3.6 8.6 5.9 12.5 11.7 9.1 10.8 11.8 14.1 15.2 13.3 15.1
4.9 26.9 2.6 1.5 9.0 8.9 30.7 7.0 4.8 10.1 5.6 0.7 26.0 12,0 15,6 27.5 14.6 16.7 30.3 22.1 11.4 37.9 12.0
0%
5%
10%
15%
20%
25%
30%
35%
40% B
0%
5%
10%
15%
20%
25%
30%
35%
40% VassaultVV AB Median LTUM LL X 90th percentile LTUM Ricos TE A
Figure 2: Biochemistry analytes LTUM evaluation.
Median (50th percentile) and 90th percentile (cross point) LTUM of 50 laboratories evaluated from AP (A), or from PG (B) target values, are
compared to the Vassault et al. [17] intermediate concentration level AB, and to “ Ricos desirable TE ” (January 2014) for 23 routine analytes.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

Matar et al.: Uncertainty in measurement estimates from external quality assessment 7
were not calculated by ANOVA, the difference between
the AP-CV and the median PG-CV reflected the extent of
between PG-biases and provided a good idea of analyte
standardization. Table 2 shows that the lowest differences
were obtained for α -fetoprotein (AFP), prostate-specific
antigen (PSA), human chorionic gonadotropin (hCG),
thyroid stimulating hormone (TSH) and free triiodothy-
ronine (FT3) with the more satisfactory standardiza-
tion status at this concentration level. The UM for these
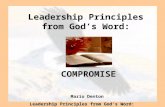
15 routine immunoassay analytes was estimated by the
LTUM method described above ( Figure 3 ). Only the PG
target value was considered here, since standardization
of immunoassays is not presently sufficiently advanced to
allow the use of the AP consensus mean without greatly
overestimating LTB and, hence, AP LTUM. Except for FT3
and free thyroxine (FT4), intra- and inter-individual varia-
tions are high, leading to a desirable TE (Figure 3) between
21% [CA 15-3, follicle stimulating hormone (FSH)] and
46% (CA 19-9). The AB established from the state-of-the-
art for these analytes was also very high, reaching values
between 24% and 29%. The median PG LTUMs were
around 10% and did not exceed 12.5%, widely below both
state-of-the-art and biological variation analytical goals.
This is confirmed by the LTUM 90th percentile showing
that over 90% laboratories fulfilled analytical goals for
the majority of analytes, except for FT3 and FT4, which
are very finely regulated in vivo and for TSH.
Hemostasis EQA schemes
Five hemostasis analytes [antithrombin, factor V, fibrin-
ogen, prothrombin time (ProT), and activated partial
thromboplastin time (aPTT)] were selected to determine
LTUM by using 50 laboratory results oncoming from their
participation in the PBQ hemostasis EQA scheme. As pre-
viously, biological variation analytical goals were found
in the Ricos et al. database (http://www.westgard.com/
biodatabase1.htm), except for factor V. Since the hemo-
stasis analytical goals derived from the state-of-the-art
are not presently defined, we decided to compare median
LTUM estimates to the acceptable limits (AL) set at PBQ
by expert biologists in charge of the hemostasis EQA
scheme. Median LTUMs were between 12.6% (ProT) and
18.4% (factor V) when the AP consensus value was used
( Figure 4 A) and between 6.4% (aPTT) and 17.1% (factor
V) when the PG consensus value was used (Figure 4B).
Except for aPTT, the use of the PG consensus mean lowered
slightly median LTUM. Apart from fibrinogen, both LTUM
analytical goals were not met by the majority of the 50
laboratories when the AP consensus value was used.
analytical goals for total bilirubin, iron, phosphate, potas-
sium, triglyceride, urate, and urea; for calcium and chlo-
ride, both analytical goals were satisfied only by < 50%
laboratories; for cholesterol, creatinine, glucose, and
magnesium, the state-of-the-art LTUM analytical goal was
fulfilled by about 90% laboratories, but < 50% laborato-
ries reached the biological variation analytical goal; lastly
for sodium, according to its very low biological variation,
the state-of-the-art analytical goal was met by 50% labo-
ratories and the biological variation analytical goal by
far < 50% laboratories. When using PG consensus value
(Figure 2B), even more laboratories reached the two ana-
lytical goals since LTUM was lower for most analytes; for
enzymes, almost all laboratories fulfilled the state-of-the-
art analytical goal while the biological variation goal, was
reached by > 90% laboratories for ALAT, amylase, aspar-
tate aminotransferase (ASAT), CK, γ -glutamyltransferase
(GGT), lipase and by 70% laboratories for lactate dehydro-
genase (LDH) and alkaline phosphatase (ALP).
Immunoassay EQA schemes
A representative example of results obtained during one
immunoassay EQA 2013 survey for 15 routine analytes,
including tumor markers and hormones, is given Table 2 .
Although the between- and within-method variability
Table 2 : An example of results obtained during one immunoassay
EQA survey (2013).
Analyte n n PG AP consensus mean
AP CV, %
MedianPG CV, %
AFP, kUI/L 640 13 70.5 9 5
CEA, μ g/L 666 13 17.5 12 5
CA 125, kU/L 607 13 44.2 12 5
CA 15-3, kU/L 630 13 30.4 15 6
CA 19-9, kU/L 634 13 34.3 21 7
PSA, μ g/L 795 14 5.0 8 5
Free PSA, μ g/L 616 15 0.54 17 6
FSH, UI/L 667 12 26.7 12 4
LH, UI/L 732 12 16.2 14 5
hCG, UI/L 1081 17 31.1 9 6
Prolactin, mUI/L 578 14 507 16 6
TSH, mUI/L 918 14 4.56 8 4
Free T3, pmol/L 734 12 5.19 11 7
Free T4, pmol/L 828 12 17.0 11 6
Estradiol, pmol/L 738 14 563 13 8
AP consensus mean and CV: mean and CV calculated from the n
values using the ISO 13528 (2005) robust algorithm A. n, number of
values; n PG, number of peer groups for each analyte; median PG
CV, median of the n peer group CVs.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

8 Matar et al.: Uncertainty in measurement estimates from external quality assessment
AF
P
CA
125
CA
15-
3
CA
19-
9
CE
A
Est
radi
ol
FS
H
hCG
LH
PS
A
Fre
e P
SA
Pro
lact
in
Fre
e T
3
Fre
e T
4
TS
H
!! 23.5 27.4 27.4 29.4 23.5 29.4 29.4 29.4 29.4 29.4 29.4 29.4 29.4 29.4 !! 11.6 11.0 10.7 11.1 12.5 11.8 9.7 10.4 9.6 11.3 12.4 11.4 11.6 10.8 10.6
22.0 18.3 15.5 20.1 18.2 25.8 15.8 19.0 19.5 22.4 18.8 19.3 20.0 14.4 31.1 21.9 35.4 20.8 46.3 24.7 26.9 21.2 27.9 33.6 29.4 11.3 8.7 23.7
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50% assaultVV AB Median LTUM 90th percentile LTUM Ricos TE
Figure 3: Immunoassay analytes LTUM evaluation.
Median (50th percentile) and 90th percentile (cross point) LTUM of 50 laboratories evaluated from the peer group (PG) target values are
compared to the Vassault et al. [17] intermediate concentration level AB, and to “ Ricos desirable TE ” (January 2014) for 15 tumor markers
and hormones.
Even when PG consensus value was used, the situation
was improved only for aPTT and ProT LTUM compared to
PBQ AL, but not with Ricos TE. For factor V, both AP LTUM
(18.4%) and PG LTUM (17.1%) were higher than the only
existing analytical goal (PBQ AL 12%). Figure 4 shows the
relative importance of the two components (LCV and LTB)
of AP and PG LTUM expressed as percentages. For aPTT,
LTB decreased from 79% (AP) to 25% (PG), for ProT from
44% (AP) to 21% (PG), and for fibrinogen from 31% to 19%
(Figure 4C, D). These three tests are chronometric, so the
coagulation time depends on reagent types and detection
methods, which could explain the LTB decrease when
considering PG instead of AP consensus value. In con-
trast, factor V and antithrombin AP and PG LTB percent-
ages were almost the same (about 10%), in keeping with
the closeness of AP and PG LTUM (Figure 4C, D). However,
LCV percentages were very high for antithrombin and
for factor V (about 90%), indicating the heterogeneity of
within-laboratory assay conditions. Thus, the ratio LCV/
LTB (with LTB calculated from AP consensus mean) could
be considered as a measure of the relevance of applying
AP or PG consensus value for bias estimation.
SH GTA 14/LTUM comparison
In order to compare the COFRAC recommended method
(SH GTA 14 IQC/EQA) to the LTUM approach, data from
20 laboratories, participating to both PBQ IQC and EQA
schemes in biochemistry and hemostasis, were used to
estimate the UM of 19 routines analytes. For immunoas-
says, comparison between the two UM method assess-
ments was impossible because of insufficient IQC data.
The within-laboratory CV (Equation 6) was estimated for
each of 20 laboratories from 10 to 15 results sent monthly
and cumulated over the 25-month period, at two concen-
tration levels close to the upper and the lower limits of the
reference range (biochemistry analytes) or corresponding
to normal and pathological levels (hemostasis analytes).
The SH GTA 14 UM and the LTUM were evaluated for each
concentration level, using the AP or PG target value.
For biochemistry analytes, SH GTA 14 UM was higher
or similar to LTUM ( Figure 5 ) whatever the consen-
sus mean (AP or PG) used. A slight decrease of UM was
observed when the PG consensus mean was used instead
of the AP consensus mean.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

Matar et al.: Uncertainty in measurement estimates from external quality assessment 9
For hemostasis analytes, AP SH GTA 14 UM was slightly
higher than AP LTUM, except for aPTT, at a normal level
whereas they were very similar at a pathological level
( Figure 6 ). When PG target value was considered instead
of AP results, SH GTA 14 UM and LTUM decreased for all
the analytes, particularly for aPTT, at both concentration
levels.
Discussion The aim of this work was to validate a simple and practical
method of calculating the UM applicable to medical labo-
ratories using only EQA results without any need for IQC
data. For this purpose, we estimated LTUM for 43 routine
analytes using data from our EQA schemes and compared
it to analytical goals commonly used in laboratory medi-
cine (state-of-the-art and biological variations). This esti-
mation was then evaluated by comparison with a method
based on a combination of IQC and EQA results and rec-
ommended by COFRAC: the SH GTA 14 approach.
The LTUM approach is based on linear regression
between laboratory data and comparison group means.
Furthermore, the regression line parameters (slope and
intercept) are estimations of proportional and constant
biases respectively, allowing the use of control samples
at different concentration levels. The quality of these
estimates is better as the number of degrees of freedom
(number of EQA samples minus two) increases. Con-
versely with the SH GTA 14 method, control samples must
be sorted according to their concentration level in order to
avoid UM overestimation [s E term in Equation 7 represent-
ing standard deviation of bias] due to PB if concentration
units are used for calculation, or to CB if relative values
(percentages) are used. Here, we observed an overestima-
tion of SH GTA 14 UM mainly at a low concentration level
(data not shown) when s WL
and bias (expressed in concen-
tration units) were used compared to UM obtained when
relative values (CV WL
and bias expressed as a percentage
of the target value) were applied. This observation sug-
gests the preponderance of a PB component in the EQA
data processed.
0%
5%
10%
15%
20%
B
0%
5%
10%
15%
20%Median LTUM PBQ AL Ricos TEA
0%10%20%30%40%50%60%70%80%90%
100%
Antithromb III Factor V Fibrinogen ProT aPTT
D
0%10%20%30%40%50%60%70%80%90%
100%
Antithromb III Factor V Fibrinogen ProT aPTT
LTB LCV C
Antithromb III Factor V Fibrinogen ProT aPTT
13.4% 18.4% 13.4% 12.6% 18.1%
12.0% 12.0% 12.0% 10.0% 10.0%
8.3% - 13.6% 5.3% 4.5%
Antithromb III Factor V Fibrinogen ProT aPTT
12.8% 17.1% 11.1% 9.2% 6.4%
12.0% 12.0% 12.0% 10.0% 10.0%
8.3% - 13.6% 5.3% 4.5%
Figure 4: Hemostasis analytes LTUM.
Median LTUMs of 50 laboratories evaluated from AP (A), or PG (B) consensus values are compared to PBQ AL and to “ Ricos desirable TE ”
(January 2014). Contribution of the two LTUM components (LTB, LCV) for AP (C) and PG (D) results, expressed as percentages. ProT is
expressed in % and aPTT in seconds.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

10 Matar et al.: Uncertainty in measurement estimates from external quality assessment
0%
5%
10%
15%
20%
25%
PG LTUM low concentration level PG SH GTA 14 low concentration level
0%
5%
10%
15%
20%
25%
PG LTUM high concentration level PG SH GTA 14 high concentration level
0%
5%
10%
15%
20%
25%
AP LTUM low concentration level AP SH GTA 14 low concentration level
A
Bic
arbo
nate
s
Tot B
iliru
bin
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
16.5 20.9 7.9 8.2 19.4 12.5 5.2 3.3 10.4 6
19.7 17.6 7.2 8.8 21.4 12.8 5.5 4.4 14.2 7.3
B'
Bic
arbo
nate
s
Tot B
iliru
bin
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
ALA
T
AS
AT
CK
GG
T
17.9 7.7 4.4 5.5 6.8 6.1 3.3 3.5 6.7 5.4 6.8 6.3 8.0 6.8
18.9 11.9 5.0 7.8 10.7 7.7 4.4 4.0 10.0 6.0 10.4 8.7 13.2 9.2
Bic
arbo
nate
s
Tot B
iliru
bin
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
ALA
T
AS
AT
CK
GG
T
14.0 12.5 3.9 5.9 9.8 8.0 3.7 2.6 6.8 4.2 8.7 9.3 14.6 10.0
18.8 15.6 5.5 7.9 13.6 11.0 4.5 3.9 12.9 6.1 13.9 10.2 16.6 10.1
A'
0%
5%
10%
15%
20%
25%
AP LTUM high concentration level AP SH GTA 14 high concentration level
B
Bic
arbo
nate
s
Tot B
iliru
bin
Chl
orid
e
Cho
lest
erol
Cre
atin
ine
Iron
Pot
assi
um
Sod
ium
Trig
lyce
ride
Ura
te
18.7 17.2 6.9 8.9 12.3 9.4 3.9 4.3 11.0 6.3
22.5 15.2 7.4 9.4 17.0 9.4 5.4 4.3 12.4 8.9
Figure 5: SH GTA 14/LTUM comparison.
Median UMs of 20 laboratories for 14 routine biochemistry analytes determined by SH GTA 14 and LTUM methods at low (left) and high
(right) concentration level, using AP (A and B) and PG (A ′ and B ′ ) results from their participation to PBQ IQC and EQA schemes.
Several assumptions are necessary for the validity of
the LTUM estimation: linearity between EQA laboratory
values and target values, equality of variance in the con-
centration range explored (homoscedasticity) and com-
mutability of the control samples.
The LTUM method has the advantage of fully taking
into account the evolution of the bias as a function of con-
centration. However, it provides a single estimate of the
variability of the regression line (s y/x
) for the whole con-
centration range explored by the control samples while
the trend of standard deviation to vary with concentration
is well known (increase for biochemistry and immunoas-
say analytes and decrease for coagulation parameters).
Therefore, the estimation of the variance obtained by this
method could be reliable only for analytes whose clini-
cally relevant concentration range is limited. Otherwise,
for hormones such as hCG or TSH, it will be necessary to
regroup control samples according to their concentration
level as in the case of the SH GTA 14 method. As expected,
our results (Figures 5 and 6) showed no significant differ-
ence between LTUM at low and high concentration levels.
In addition, UM values obtained by the two methods
tested are very similar indicating that heteroscedasticity
is not a limiting factor when applying the LTUM method to
biochemistry and hemostasis routine measurands.
Another important condition to demonstrate the
potential of this UM estimate approach is the commut-
ability of EQA samples with those of patients. Only in
this case, the bias estimate will be reliable reflecting the
discrepancies between measurement procedures and not
the matrix related bias. Indeed, the most desirable PT/
EQA programs are those that use commutable samples
with target values assigned by a reference method (cat-
egories 1 and 2 in reference [18] ). Although fresh samples
of human origin are distributed in some of our programs,
data used in this study came only from processed (mostly
lyophilized and spiked or diluted to adjust the concentra-
tion levels) and therefore likely non-commutable control
materials. IQC samples, used for the SH GTA 14 method,
must also be commutable to provide the best estimate of
within laboratory precision. So in order to validate the
estimation of the UM by the method proposed here, it is
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

Matar et al.: Uncertainty in measurement estimates from external quality assessment 11
necessary to characterize control samples with respect
to their commutability. This could be done by comparing
their behavior to a representative panel of patient samples
for combinations of the most used measurement pro-
cedures as described in the CLSI document EP30-A [19] .
A limit of our study is that the commutability of control
samples was not tested and therefore a matrix related bias
could not be excluded for some diagnostic systems. In this
case, all methods relying on EQA/IQC data to estimate the
systematic component of TE, are likely to give incorrect
UM values. For this reason, the LTUM estimates presently
provided to participants in PBQ EQA schemes only use the
peer group target values. An alternative could be to use
the GUM “ Modeling approach ” which is a method less
prone to this drawback but more difficult to implement in
medical laboratories. However, our main goal in this work
was not to obtain a reliable estimate of bias but to test a
convenient method for calculating the UM and to compare
it to a recommended method which also requires the com-
mutability of samples.
At last, the UM estimate is tightly dependent on the
choice of the target value as shown by the different values
observed when the homogeneous group (PG) mean is
used instead of the mean of AP. Of course, the use of a TE
estimate based on APs rather than on peer group EQA data
is more appropriate to obtain valid conclusions regarding
the suitability of routine methods for meeting TE goals
for interpretation of patient results. However, the present
standardization status of some analytes (tumor markers)
requires the use of the same method (in the same labora-
tory) for the monitoring of patients and justifies our bias
estimation by comparison to the peer group. Furthermore,
the UM estimates obtained using both references were in
close agreement for many measurands except those for
which standardization status is still a matter of concern
(enzymes, immunoassays).
In conclusion, this study allowed validation of UM
calculation by a simple method that uses only the results
of EQA schemes. It provided estimates comparable to
methods recommended by official bodies and enabled biol-
ogists to compare estimates obtained by different methods.
As an EQA organizer, we provide all participants at the end
of each survey, since January 2014, with an estimate of UM
by this method using data from control samples assayed
0%
5%
10%
15%
20%
25%
Fibrinogen ProT aPTT
PG LTUM normal level PG SH GTA 14 normal level
0%
5%
10%
15%
20%
25%
Fibrinogen ProT aPTT
AP LTUM normal level AP SH GTA 14 normal level
0%
5%
10%
15%
20%
25%
Fibrinogen ProT aPTT
AP LTUM pathologic level
AP SH GTA 14 pathologic level B
11.3% 12.4%
15.6% 14.8%
15.9% 15.7%
A
11.7% 13.0%
11.8%
14.6%
19.6%
16.6%
A'
9.8%
12.5% 10.8% 11.6%
6.7%
9.5%
0%
5%
10%
15%
20%
25%
Fibrinogen ProT aPTT
PG LTUM pathologic level PG SH GTA 14 pathologic level
B'
9.5% 11.7%
9.2%
11.8%
5.7%
9.3%
Figure 6: SH GTA 14/LTUM comparison for hemostasis analytes.
Median UMs of 20 laboratories for three hemostasis analytes estimated by the SH GTA 14 and LTUM approaches at normal and pathologic
levels from AP (A and B) and PG (A ′ and B ′ ) results.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM

12 Matar et al.: Uncertainty in measurement estimates from external quality assessment
during the current year and the previous 2 years. The accu-
mulation of results over time for a large panel of analytes
and a great number of clinical laboratories will allow better
appreciation of its advantages and disadvantages.
Author contributions: All the authors have accepted
responsibility for the entire content of this submitted
manuscript and approved submission.
Financial support: None declared.
Employment or leadership: None declared.
Honorarium: None declared.
Competing interests: The funding organization(s) played
no role in the study design; in the collection, analysis, and
interpretation of data; in the writing of the report; or in the
decision to submit the report for publication.
References 1. Guidelines for evaluating and expressing the uncertainty of NIST
measurement results. NIST Technical Note 1994:1297.
2. White GH, Farrance I. Uncertainty of measurement in quantitative
medical testing a laboratory implementation guide. AACB Clin
Biochem Rev 2004;25(Suppl):S124.
3. Fuentes AX. Uncertainty of measurement in clinical microbiology.
In: eJIFCC 2004;13. Available from: http://www.ifcc.org/ifccfiles/
docs/130401006.pdf . Accessed November 2004.
4. International Laboratory Accreditation Cooperation (ILAC). ILAC
G-2:1994. Available from: http://www.ilac.org . Accessed Novem-
ber 2004.
5. Guide to the expression of uncertainty in measurement. Geneva:
International Organization for Standardization (ISO), 1993.
6. ISO 17025: General requirements for the competence of testing
and calibration laboratories. Geneva: International Organization
for Standardization (ISO), 2005.
7. ISO 15189: Medical laboratories – particular requirements for
quality and competence. Geneva: International Organization for
Standardization (ISO), 2012.
8. Evaluation of measurement data – Guide to the expression of
uncertainty in measurement. JCGM 100:2008.
9. Measurement uncertainty revisited: alternative approaches to
uncertainty evaluation. European Federation of National Asso-
ciations of Measurement, Testing and Analytical Laboratories,
EUROLAB. Technical Report No. 1/2007.
10. SH GTA 14: Technical guide for accreditation for the uncertainty
measurement assessment in medical biology. Available from:
http://www.cofrac.fr . Accessed 2011.
11. Meijer P, de Maat MP, Kluft C, Haverkate F, van Houwelingen
HC. Long-term analytical performance of hemostasis field
methods as assessed by evaluation of the results of an external
quality assessment program for antithrombin. Clin Chem
2002;48:1011 – 5.
12. ISO 13528: Statistical methods for use in proficiency testing by
interlaboratory comparisons. Geneva: International Organiza-
tion for Standardization (ISO), 2005.
13. ISO 17043: Conformity assessment – general requirements
for proficiency testing. Geneva: International Organization for
Standardization (ISO), 2010.
14. Fisicaro P, Amarouche S, Lalere B, Labarraque G, Priel M.
Approaches to uncertainty evaluation based on proficiency
testing schemes in chemical measurements. Accred Qual Assur
2008;13:361 – 6.
15. Amarouche, S, Priel M, De Graeve J. Exploiting proficiency test-
ing results, a new alternative to the evaluation of uncertainties:
application in medical biology: dosage of glucose in human
plasma. Workshop on the Impact of Information Technology in
Metrology. BIPM-PTB, Berlin, 2007.
16. SH GTA 06: Technical guide for accreditation: quality assess-
ment in medical biology. Available from: http://www.cofrac.fr .
Accessed 2012.
17. Vassault A, Grafmeyer D, de Graeve J, Cohen R, Beaudonnet A,
Bienvenu J. Analyses de biologie m é dicale: sp é cifications et
normes d ’ acceptabilit é à l ’ usage de la validation de techniques.
Ann Biol Clin 1999;57:685 – 95.
18. Miller WG, Jones GR, Horowitz GL, Weykamp C. Proficiency test-
ing/external quality assessment: current challenges and future
directions. Clin Chem 2011;57:1670 – 80.
19. CLSI. Characterization and qualification of commutable refer-
ence materials for laboratory medicine; CLSI document EP30-A.
Wayne, PA: Clinical and Laboratory Standards Institute, 2010.
Authenticated | [email protected] author's copyDownload Date | 3/27/15 10:16 AM