Title · Web viewAntibiotic loaded cement beads are commonly used for the treatment of biofilm...
44
Effects of Loading Concentration, Blood and Synovial Fluid on Antibiotic Release and Anti-Biofilm Activity of Bone Cement Beads Devendra Dusane a, * ,† , Scott Diamond b, *, Cory Knecht b, *, Nicholas Farrar c, *, Casey Peters d , Robert Howlin e , Matthew Swearingen a , Jason Calhoun f , Roger D. Plaut g , Tanya Nocera c , Jeffrey Granger h , Paul Stoodley a,h a Department of Microbial Infection and Immunity, The Ohio State University, Columbus, Ohio 43210 b Department of Medicine, The Ohio State University, Columbus, Ohio 43210 c Department of Biomedical Engineering, The Ohio State University, Columbus, Ohio 43210 d Department of Biochemistry, The Ohio State University, Columbus, Ohio 43210 e Centre for Biological Sciences, Faculty of Natural & Environmental Sciences & Institute for Life Sciences, University of Southampton, Southampton, UK f Department of Muscoskeletal Sciences, Spectrum Health Medical Group, Grand Rapids, Michigan 1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Transcript of Title · Web viewAntibiotic loaded cement beads are commonly used for the treatment of biofilm...
Effects of Loading Concentration, Blood and Synovial Fluid on Antibiotic
Release and Anti-Biofilm Activity of Bone Cement Beads
Devendra Dusane a,*,†, Scott Diamond b,*, Cory Knecht b,*, Nicholas Farrar c,*, Casey Peters d,
Robert Howlin e, Matthew Swearingen a, Jason Calhoun f, Roger D. Plaut g, Tanya Nocera c,
Jeffrey Granger h, Paul Stoodley a,h
a Department of Microbial Infection and Immunity, The Ohio State University, Columbus,
Ohio 43210
b Department of Medicine, The Ohio State University, Columbus, Ohio 43210
c Department of Biomedical Engineering, The Ohio State University, Columbus, Ohio 43210
d Department of Biochemistry, The Ohio State University, Columbus, Ohio 43210
e Centre for Biological Sciences, Faculty of Natural & Environmental Sciences & Institute for
Life Sciences, University of Southampton, Southampton, UK
f Department of Muscoskeletal Sciences, Spectrum Health Medical Group, Grand Rapids,
Michigan
g Division of Bacterial, Parasitic, and Allergenic Products, Center for Biologics Evaluation
and Research, Food and Drug Administration, Silver Spring, MD 20993
h Department of Orthopaedics; The Ohio State University, Columbus, Ohio 43210
† E-mail address: [email protected]
* Equal contribution
1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
ABSTRACT
Antibiotic loaded cement beads are commonly used for the treatment of biofilm related
orthopaedic periprosthetic infections; however the effects of antibiotic loading and exposure
of beads to body fluids on release kinetics are unclear. The purpose of this study was to
determine the effects of (i) antibiotic loading density (ii) loading amount (iii) material type
and (iv) exposure to body fluids (blood or synovial fluid) on release kinetics and efficacy of
antibiotics against planktonic and lawn biofilm bacteria. Short-term release into an agar gel
was evaluated using a fluorescent tracer (fluorescein) incorporated in the carrier materials
calcium sulfate (CaSO4) and poly methyl methacrylate (PMMA). Different fluorescein
concentrations in CaSO4 beads were evaluated. Mechanical properties of fluorescein-
incorporated beads were analyzed. Efficacy of the antibiotics vancomycin (VAN) or
tobramycin (TOB) alone and in combination was evaluated against planktonic and lawn
biofilms of bioluminescent strains of Staphylococcus aureus and Pseudomonas aeruginosa.
Zones of inhibition (ZOI) were measured visually and using an in-vivo imaging system
(IVIS). The influence of body fluids on release was assessed using CaSO4 beads that
contained fluorescein or antibiotics and were pre-coated with human blood or synovial
fluid. The spread from the beads followed a square root of time relationship in all cases. The
loading concentration had no influence on short-term fluorescein release and pre-coating of
beads with body fluids did not affect short-term release or antibacterial activity. Compared to
PMMA, CaSO4 had a more rapid short term rate of elution and activity against planktonic
and lawn biofilms. This study highlights the importance of considering antibiotic loading and
packaging density when investigating the clinical application of bone cements for infection
management.
Running title: Short-term antibiotic release and anti-biofilm efficacy from bone cement
beads
2
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
Keywords: periprosthetic infection; biofilm; bone cement; antibiotic release; zone of
inhibition
1. Introduction
Orthopaedic periprosthetic joint infections (PJI) are difficult to treat with systemic
antibiotic therapy and can lead to severe complications such as removal of the implant with
functional loss of the affected body part or life-threatening conditions [1, 2]. The extent of
infection depends upon several factors, such as health of the patient, length of time of
infection and condition of local soft tissues.
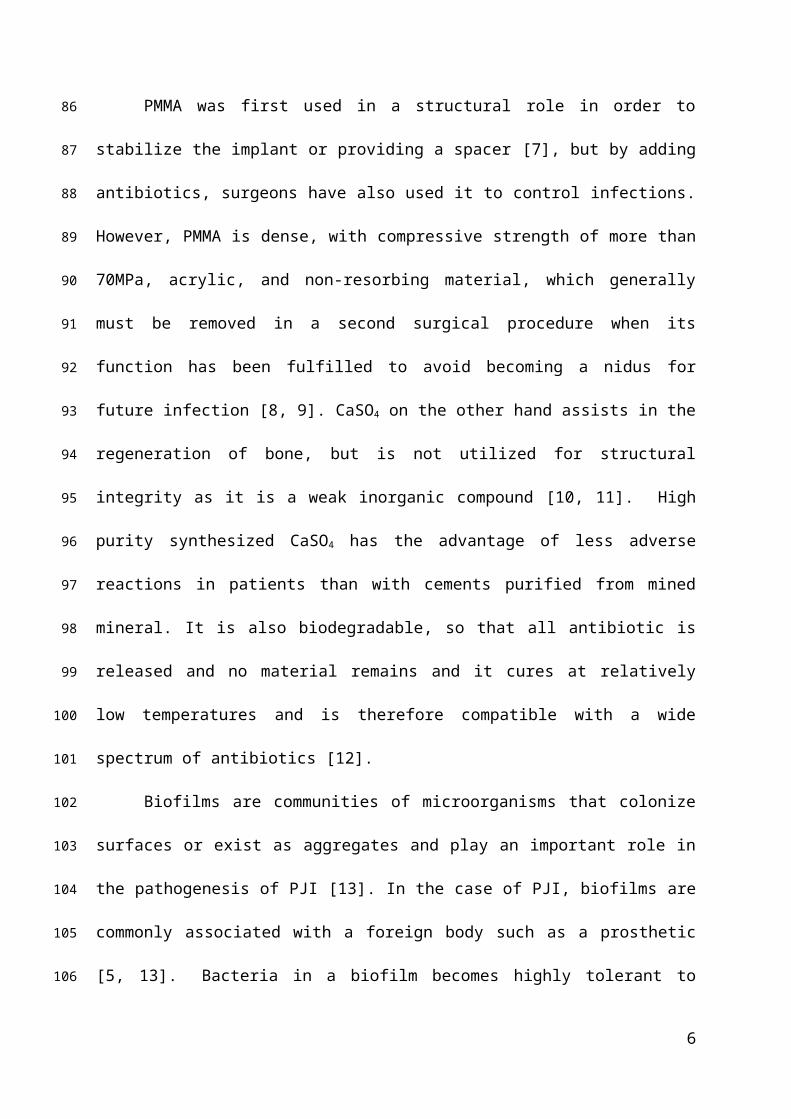
Antibiotic-loaded bone cement beads are a commonly-used option functioning to fill
the dead space and managing infection for the treatment of PJI [3, 4] (Fig. 1). Beads are
made directly in the operating room from poly (methyl) methacrylate (PMMA) or mineral
based formulations such as calcium sulfate (CaSO4) [4-6].
Fig. 1. Surgical site of infection showing antibiotic loaded calcium sulfate (CaSO4) beads.
PMMA was first used in a structural role in order to stabilize the implant or providing
a spacer [7], but by adding antibiotics, surgeons have also used it to control infections.
3
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
However, PMMA is dense, with compressive strength of more than 70MPa, acrylic, and non-
resorbing material, which generally must be removed in a second surgical procedure when its
function has been fulfilled to avoid becoming a nidus for future infection [8, 9]. CaSO4 on the
other hand assists in the regeneration of bone, but is not utilized for structural integrity as it is
a weak inorganic compound [10, 11]. High purity synthesized CaSO4 has the advantage of
less adverse reactions in patients than with cements purified from mined mineral. It is also
biodegradable, so that all antibiotic is released and no material remains and it cures at
relatively low temperatures and is therefore compatible with a wide spectrum of antibiotics
[12].
Biofilms are communities of microorganisms that colonize surfaces or exist as
aggregates and play an important role in the pathogenesis of PJI [13]. In the case of PJI,
biofilms are commonly associated with a foreign body such as a prosthetic [5, 13]. Bacteria
in a biofilm becomes highly tolerant to antibiotics as compared to the planktonic phenotype,
therefore localized antibiotics delivery is needed to provide sustained high concentrations of
antibiotics, that cannot be achieved systemically [14, 15].
However, to achieve these concentrations, whether incorporating the required dose of
antibiotics in few beads or distributing the dose in multiple beads to provide better release
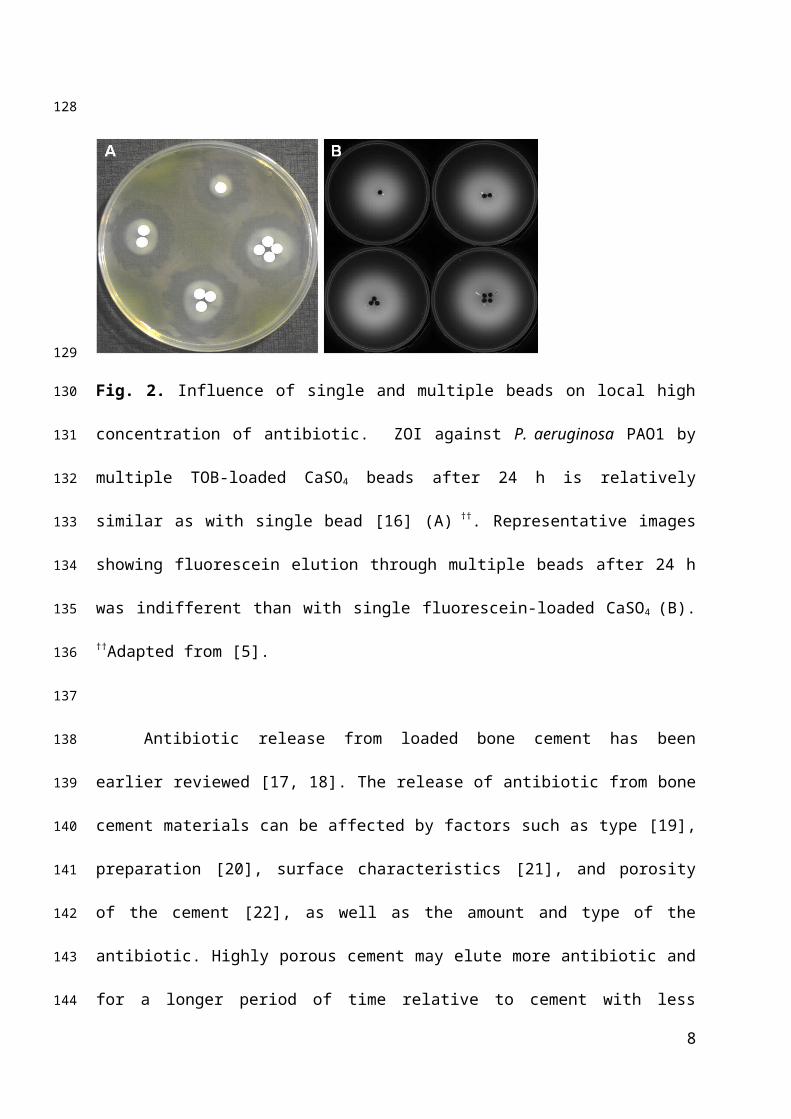
and efficacy is unclear. In a previous study, we reported that the zone of inhibition of
Pseudomonas aeruginosa PAO1 from CaSO4 carrier beads loaded with tobramycin (TOB)
was similar regardless of whether beads were placed singly or in groups of 2, 3 or 4 (Fig. 2A)
[5]. This is important since it shows that in diffusion limited environment, such as might be
found in periprosthetic tissue or quiescent fluid, that the packing density of the beads is an
important consideration in providing adequate coverage of the infected area. Further, multiple
beads placed together also provide a multiplicity of antibiotic at a specific location.
Moreover, when the release is diffusion limited for an absorbable material in which all
4
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
antibiotic will be released it might be expected that the higher bead density would provide
longer coverage.
Fig. 2. Influence of single and multiple beads on local high concentration of antibiotic. ZOI
against P. aeruginosa PAO1 by multiple TOB-loaded CaSO4 beads after 24 h is relatively
similar as with single bead [16] (A) ††. Representative images showing fluorescein elution
through multiple beads after 24 h was indifferent than with single fluorescein-loaded CaSO4
(B). ††Adapted from [5].
Antibiotic release from loaded bone cement has been earlier reviewed [17, 18]. The
release of antibiotic from bone cement materials can be affected by factors such as type [19],
preparation [20], surface characteristics [21], and porosity of the cement [22], as well as the
amount and type of the antibiotic. Highly porous cement may elute more antibiotic and for a
longer period of time relative to cement with less porosity [23]. The porous cement material
such as CaSO4 is a better antibiotic carrier material than PMMA for local delivery of
antibiotics [5]. In a recent study by Chang et al (2014) it was shown that adding antibiotics
(such as vancomycin, amphotericin B) powder in distilled water before mixing with bone
cement significantly improves the efficiency of antibiotic release than same dose of antibiotic
5
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
powder [24]. However, the ultimate compressive strength of the beads was significantly
reduced in specimens containing liquid antibiotics.
Release of antibiotic from bone cement has previously been reported and measured in
phosphate buffered saline (PBS) by estimating the zone of inhibition [25] or by using HPLC
[26] or LC-MS [27]. However, the diffusion of antibiotics from a carrier bead into
surrounding soft tissue and quiescent joint fluid is a diffusion limited environment and the
degree of penetration of an antibiotic into the infected site is an important determinant of
therapeutic success [4, 28]. We have earlier reported the use of agar diffusion method to
analyze the zone of inhibition [5] and extended these observations to study the importance of
antibiotic loading density, loading amount, material type and exposure to body fluids on
release kinetics and efficacy of antibiotics against planktonic and lawn biofilm bacteria. The
agar method allows understanding how antibiotics might spread into the surrounding tissues
as we can monitor the elution distance, antibacterial effects and preserve the gradients that
are likely to develop in vivo in areas that are diffusion limited. The diffusion limited agar
technique therefore becomes relevant and clinically important.
To investigate the release kinetics of diffusion from beads into a surrounding gel in
real time we used fluorescein dye tracer which has previously been used as a surrogate to
study antibiotic release based on its hydrophilic characteristics [16]. In the clinical setting,
antibiotic-loaded beads immediately come into contact with the body fluids, such as blood
and synovial fluid that may influence the properties and release from the beads. We
hypothesized that exposure to these body fluids influences the release kinetics of antibiotic
from antibiotic-loaded orthopaedic cements. Calcium is a known clotting factor and it is
possible that blood clots that form around the beads may also influence release of antibiotics.
This might be disadvantageous (by trapping antibiotics within the beads) or advantageous
6
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
(slowing down the release to increase the period over which the beads may effectively release
antimicrobial concentrations inhibitory to the cells).
Therefore the purpose of the present study was to determine whether (i) the bone
cements PMMA and high purity synthetic CaSO4 hemihydrate would have different elution
kinetics and efficacy against planktonic and biofilm bacteria, (ii) the release kinetics of
antibiotics from CaSO4 beads was dependent on the loading concentration and (iii) if
exposure to human blood or synovial fluid influenced the release kinetics and antibiotic
efficacy. To track release, we used an agar model to simulate release into a surrounding
viscous medium by diffusion alone, using fluorescein as a tracer and the extinction of activity
in biofilm lawns grown from bioluminescent strains of Staphylococcus aureus and
Pseudomonas aeruginosa, two common PJI pathogens.
2. Materials and methods
2.1. Preparation of bone cement beads with fluorescein
CaSO4 (Stimulan Rapid Cure, Biocomposites Inc, NC, USA) and PMMA
(PALACOS® R, Zimmer, IN, USA) powders were weighed, and the corresponding volume of
respective liquid (sterile water for Stimulan Rapid Cure and methyl methacrylate, N,N-
dimethyl-p-toluidine in case of PALACOS R) was added and mixed for 30 to 60s to form a
homogeneous paste. The paste was then spread onto a flexible rubber mold (Biocomposites
Ltd) to make hemispherical beads of 4.8 mm diameter. The beads were left undisturbed to set
for 1 h. After the beads solidified, the molds were flexed by hand in a torsional motion to
remove the beads which were loosened from the mold and dropped in sterile petriplate and
stored at room temperature until use. Control beads were prepared without fluorescein.
Fluorescein (Fluka, USA) was incorporated into beads in the amounts of 1.0 g per 10cc pack
(20.0 g) of CaSO4 or 2.33 g per 40.0 g of PMMA were prepared. One pack of Stimulan
7
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
contains 20.0 g of powder and 6 mL of liquid, which upon mixing yields 23.8 g of set
cement. The mass of one set 4.8 mm bead was 97 ± 4 (n=4) mg so that one pack would
theoretically make approximately 245 beads. With 1.0 g of fluorescein per pack of Stimulan,
the average weight of fluorescein per bead was 3.92 mg and made approximately 250 beads.
When 1.0 g of fluorescein was mixed into a Stimulan pack, each bead was infused with 4.2%
(by weight) of fluorescein. Similarly for PMMA, one pack of PALACOS containing 40.0 g
of powder and 20 mL of liquid that made 53.2 g of set cement. The average mass of a single
4.8 mm bead was 59 ± 8 (n=4) mg, so that one pack could potentially make up to 900 set
beads. The mass of an individual bead and the total number of beads that could be made per
pack were used to calculate the amount of additive (fluorescein or antibiotic) on a per-bead
basis to account for density differences between the two materials.
In order to analyze the effect of number of beads on release of fluorescein, single or
multiple CaSO4 beads (1−4) containing fluorescein (1.0 g per 10cc pack of CaSO4, Stimulan
Rapid Cure, Biocomposites) were placed on 1% agar (Fig. 2B). Using fluorescein, similar
elution characteristics were observed as in case of TOB when single and multiple beads were
used (Fig. 2A-B). Furthermore, in order to investigate the effect of loading density on elution
kinetics, various concentrations of fluorescein-containing beads were also prepared. The
weights of fluorescein used were 0.125, 0.25, 0.5, 1.0, 2.0 and 4.0 g per 10cc pack of CaSO4.
Amounts above 4.0 g per 10cc pack of CaSO4 were not used, since at higher amounts the
beads did not set well.
2.2. Elution kinetics of fluorescein through bone cement beads
CaSO4 and PMMA beads containing fluorescein were placed on 1% pure agar
(Sigma, USA) plates using sterile forceps. The plates were incubated at 37°C, and at different
time intervals (0−8 h) fluorescent images were captured using a gel documentation system
8
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
(Gel Doc™ XR Bio-Rad). The images were analyzed using a freeware program, Fiji
(Fiji.sc/fiji). Images at various time points were aligned to create a set of images that were
normalized to pixel size. Plate diameter was used to set the scale to pixel ratio, the images
were stacked and automatic intensity threshold was applied to determine fluorescein elution
distance. The fluorescein release experiments were performed in triplicate.
2.3. Mechanical properties of cement beads
Increasing the concentration of antibiotics can impair the setting and mechanical
properties of the bone cements [15, 29]. Weakening of cement material is of high concern,
thus in order to avoid mechanical weakening, low concentration of the compound is usually
recommended [15, 30]. The strength of beads containing fluorescein was measured using the
compression test. A bead was placed between two parallel plates and was crushed with a
constant strain. The test frame (100Q Series Mechanical Test Frame, Test Resources) was
activated by turning on the device and running a compressive test profile with a constant
positional change in the parallel plates. After optimizing the strain, 1 mm/min was selected
due to the uniformity and consistency of the load (Newtons) as a function of time (seconds).
The top compression plate was manually lowered until it was flush with the top point of the
spherical section of the bead, and this position was set to zero. Upon initiation of the constant
strain, the threaded top shaft was forced into the apex of the bead, and the force was
measured in real-time by the load cell. The plots of load as a function of time were
transmitted from the test frame to a laptop using WinCom™. Load as a function of time for a
CaSO4 bead was plotted where the bead exhibited a clear first crack point, which was termed
its ultimate compressive strength. Thus, the applied force recorded was when the
microstructure of the bead began to permanently deform (termed as the first crack strength).
9
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
Maximum load values of the impregnated beads were exported to Excel and compared to
their respective control beads.
Fluorescein-impregnated CaSO4 beads were compressed until their ultimate
compressive strengths were observed on the plots of applied load as a function of time.
Student t-tests were performed on each of the concentrations of fluorescein compared to the
non-impregnated bead.
2.4. Preparation of CaSO4 and PMMA beads impregnated with antibiotics
The efficacy of antibiotic-impregnated bone cements was measured by preparing
beads in a similar way as mentioned for fluorescein. Briefly, CaSO4 (20.0 g per pack) or
PMMA (40.0 g per pack) beads with or without the antibiotic(s) [vancomycin hydrochloride
(VAN; Fluka USA) 1.0 g per pack of cement powder or tobramycin sulphate (TOB; Sigma-
Aldrich) 240 mg per pack of cement powder] were prepared. The loading amount of
antibiotic (VAN) per bead in CaSO4 was 3.9 mg and TOB was 0.97 mg. PMMA had 3.47 mg
of VAN and 0.9 mg of TOB per bead [14]. The percent weight of antibiotic impregnated
bead was normalized based on 1.0 g antibiotic added to a 10cc pack of Stimulan per the
manufacturer's recommendation. The levels of antibiotic addition were representative of
levels reported in the literature [5]. The powders were evenly blended with or without the
antibiotics and beads were prepared as described earlier. Controls consisted of beads with no
antibiotic (negative control) and plates with no beads (positive control). All the experiments
were performed in triplicate.
2.5. Bacteria and growth conditions
Bioluminescent strains of Staphylococcus aureus SAP231 [31] and Pseudomonas
aeruginosa Xen41 (PerkinElmer, USA) were used. S. aureus SAP231 is a multidrug resistant
10
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
strain (MRSA) of pulsed-field gel electrophoresis type USA300 containing an integrated
plasmid carrying luxBADCE, [31] whereas P. aeruginosa Xen41 is a P. aeruginosa PAO1
luminescent strain that harbors the luxCDABE cassette inserted in a constitutively expressed
manner [32, 33]. These bacteria were cultured in brain heart infusion (BHI) and lysogeny
broth (LB) respectively (Sigma Aldrich, USA).
2.6. Determination of MIC of VAN and TOB against bacteria
The MIC of antibiotics (VAN and TOB) was determined using the E-test strip
method. S. aureus SAP231 or P. aeruginosa Xen41 was grown in the appropriate growth
media overnight and diluted 100 times. The diluted culture was spread (100 µL) onto freshly
prepared BHI or LB agar plates, and E-test strips (BioMerieux, KY, USA) were placed on the
surface of the plates. The plates were incubated for 24 h at 37°C, and the MIC was
determined based on the area of no growth corresponding to the lowest antibiotic
concentration [34].
2.7. Inhibition of planktonic bacterial growth using antibiotic eluting beads
Agar diffusion assays were used to determine release and inhibitory activity of
antibiotics from the beads (CaSO4 or PMMA) over time. For inoculating the agar plates, a
colony of bacteria was removed from a cultured petri dish to culture overnight at 37°C in 15
mL BHI or LB broth for respective bacterial cultures. The grown culture was diluted to an
optical density (OD) corresponding to ~106 cells/mL and plated on respective BHI or LB
solid agar media. The antibiotic-loaded beads containing VAN, TOB or combinations (VAN
+ TOB) were placed in the center of the plates immediately after inoculation. The plates were
incubated at 37oC at 5% CO2 for 24 h. Images of the plates were taken, and the diameter of
the zones of inhibition (ZOI) formed around the beads was measured using Vernier calipers
11
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
and the in-vivo imaging system (IVIS). Measurements of ZOI were taken 24 h after
placement of the bead. Assays were performed in experimental triplicate and the ZOI data
were expressed as the mean ± standard error.
2.8. Killing pre-existing lawn biofilms using antibiotic eluting beads
Bacterial cultures were spread on respective agar media as described earlier for
planktonic bacterial growth and were incubated for 24 h at 37°C. CaSO4 or PMMA beads
with or without antibiotics were placed onto pre-grown lawn biofilms of S. aureus SAP231 or
P. aeruginosa Xen41 on respective agar plates. Images of the plates were taken and the area
around the antibiotic beads showing the dark zone where bioluminescence was suppressed by
the spreading antibiotic under IVIS imaging system was measured and designated as the
“zone of inactivation” (ZOIn). The ZOIn formed around the beads was measured every 24 h
following placement of the bead on the plate. The spread of inactivation was measured as the
radius of the dark circle. The distance was plotted as a power law relationship function of the
square root of time to linearize the data (all R2 > 0.90). The slope (power law constant) was
used as a comparative release rate coefficient.
Swabs from the inner and outer zones for both PMMA and CaSO4 beads placed on the
lawn biofilm were collected and spread on fresh agar plates to determine whether the
bacterial cells in the zone of inactivation had been killed. Assays were performed in
experimental triplicate and the ZOIn data were expressed as the mean ± standard error.
The colony forming units (CFU/cm2) were calculated from the 24 h grown cultures on
the agar plates. Agar plugs from different areas of the plates containing S. aureus or P.
aeruginosa (24 h grown) were immersed in sterile PBS, homogenized, serially diluted and
plated on respective growth media. The counts for S. aureus and P. aeruginosa were 1.33 ×
12
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
107 and 1.21 × 106 CFU/cm2 respectively. One tailed student’s t-test was used to compare
between CaSO4 and PMMA beads.
2.9. Influence of host factors on release kinetics
To determine whether host factors influence fluorescein release, we used human
blood and bovine synovial fluid (Lampire Biological Laboratories, PA). Blood from healthy
human donors was collected in accordance with the approved IRB protocol 2015H0121.
Individual beads (with or without fluorescein) were placed in wells of a 96-well microtitre
plate and fresh unadulterated blood (~200 µL) was immediately added to the well after
collection. In addition to unadulterated blood which formed a clot on the beads we also
exposed beads to heparinized blood. Similarly, bovine synovial fluid (~200 µL) was added to
the microtitre plate wells containing fluorescein in CaSO4 beads. The beads were removed
after 20 min and were placed on the surface of 1% agar plates using sterile forceps. The
plates were incubated for 24 h at 37°C and every hour fluorescent images were collected and
processed using Fiji.
2.10. Influence of host factors on antibacterial activity
To compare the effect of unadulterated human blood and bovine synovial fluid on the
ZOI, CaSO4 beads with and without TOB antibiotic (240 mg in 10cc pack) were placed in
microtitre plate wells and fresh blood from healthy donors (~200 µL) was immediately
added. The beads were removed after ensuring blood clots and coats around the beads (20
min) and were placed on the surface of P. aeruginosa spread LB agar plates. The beads were
inserted inside the agar surface, plates were incubated at 37°C, and images (using camera and
IVIS) were collected after 24 h.
13
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305

3. Results
3.1. Short-term release from bone cements
Fluorescein was used as a tracer compound to study short-term release (8 h) through
1% agar using varying concentration of fluorescein-impregnated CaSO4 beads. Fluorescence
intensity increased over time along the radial distance travelled (Fig. 3A-B).
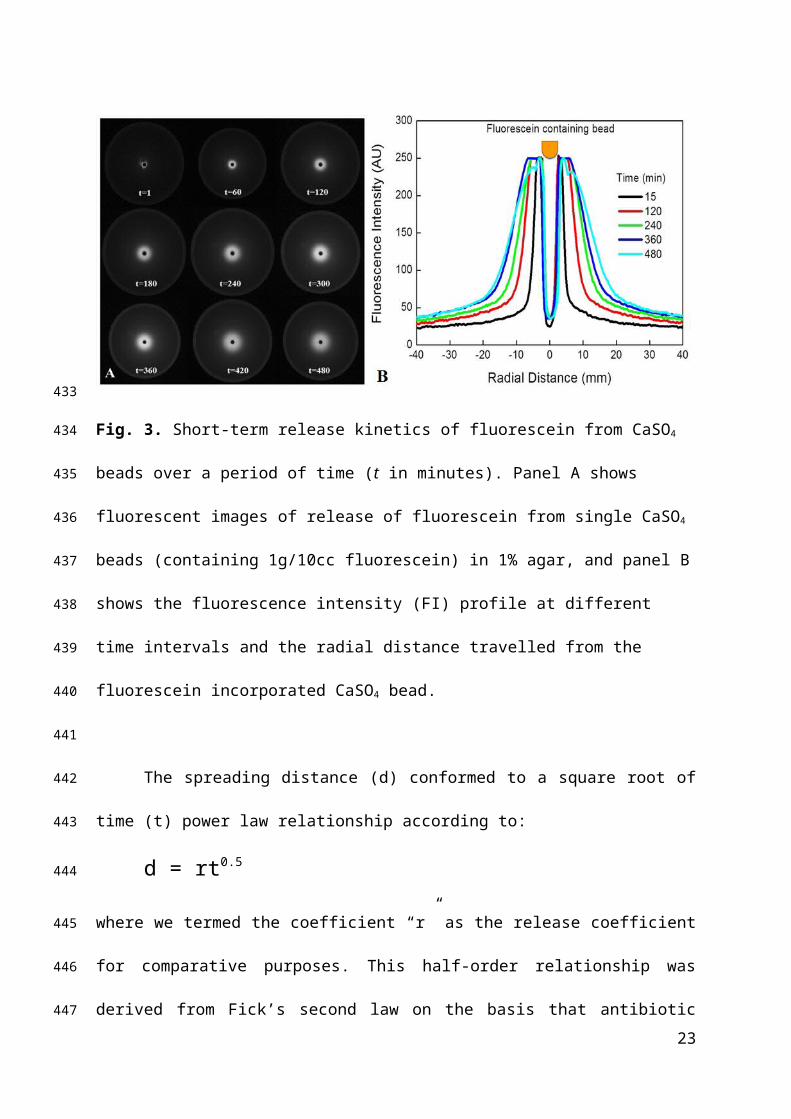
Fig. 3. Short-term release kinetics of fluorescein from CaSO4 beads over a period of time (t in
minutes). Panel A shows fluorescent images of release of fluorescein from single CaSO4
beads (containing 1g/10cc fluorescein) in 1% agar, and panel B shows the fluorescence
intensity (FI) profile at different time intervals and the radial distance travelled from the
fluorescein incorporated CaSO4 bead.
The spreading distance (d) conformed to a square root of time (t) power law
relationship according to:
d = rt0.5
where we termed the coefficient “r” as the release coefficient for comparative purposes. This
half-order relationship was derived from Fick’s second law on the basis that antibiotic elution
14
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
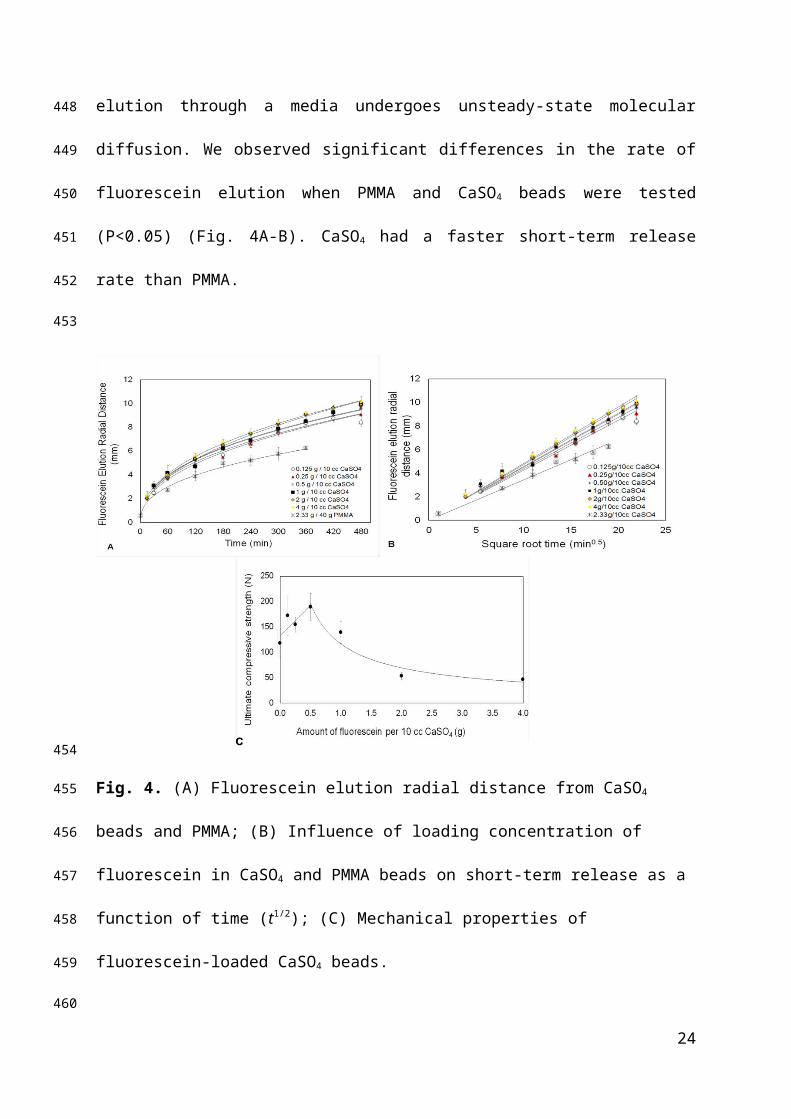
through a media undergoes unsteady-state molecular diffusion. We observed significant
differences in the rate of fluorescein elution when PMMA and CaSO4 beads were tested
(P<0.05) (Fig. 4A-B). CaSO4 had a faster short-term release rate than PMMA.
Fig. 4. (A) Fluorescein elution radial distance from CaSO4 beads and PMMA; (B) Influence
of loading concentration of fluorescein in CaSO4 and PMMA beads on short-term release as a
function of time (t1/2); (C) Mechanical properties of fluorescein-loaded CaSO4 beads.
3.2. Mechanical properties of fluorescein-containing CaSO4 beads
Initially, the ultimate compressive strength of the CaSO4 beads strength increased
with fluorescein weights of upto 0.5 g (Fig. 4C). However, at weights of 2.0 g and 4.0 g of
fluorescein, the beads were significantly weakened. Above 4.0 g, the beads did not set.
Previous reports with PMMA bone cement showed no significantly change as the antibiotics
15
323
324
325
326
327
328
329
330
331
332
333
334
335
336

are eluted and the percentage drop compressive strength was much higher with larger
amounts of antibiotics [35, 36].
3.3. Determination of minimum inhibitory concentration
The MIC of both VAN and TOB against S. aureus SAP231 was 2.0 µg/mL. For P.
aeruginosa Xen41, the MIC of TOB was 1.5 µg/mL. VAN had no effect on the growth of P.
aeruginosa.
3.4. Inhibition of planktonic bacteria by antibiotic elution through beads
CaSO4 beads demonstrated faster killing than PMMA beads against both P.
aeruginosa and S. aureus (Table 1). The ZOI was measured surrounding CaSO4 beads loaded
with or without VAN or TOB on agar plates. ZOI by CaSO4 loaded with TOB against P.
aeruginosa was larger (41 ± 0.6 mm) than against S. aureus (30.6 ± 0.8 mm). Moreover,
VAN had lower ZOI (23.9 ± 0.8) against S. aureus than did TOB (Table 1).
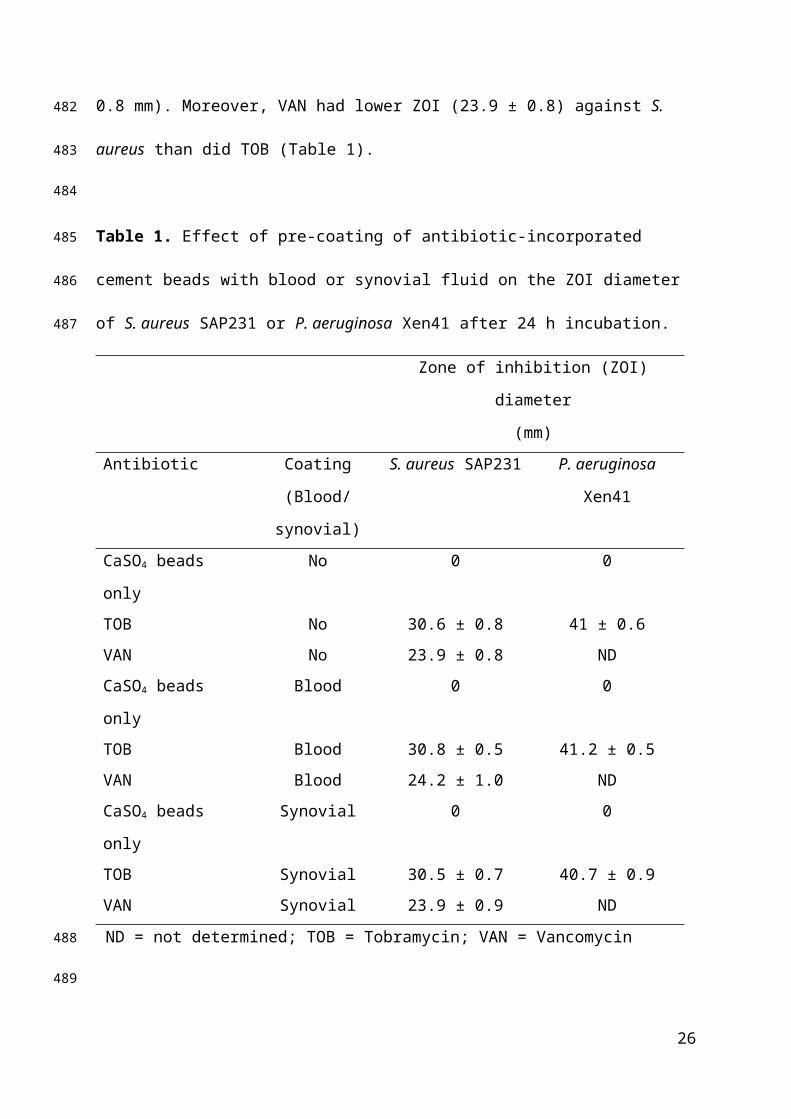
Table 1. Effect of pre-coating of antibiotic-incorporated cement beads with blood or synovial
fluid on the ZOI diameter of S. aureus SAP231 or P. aeruginosa Xen41 after 24 h incubation.
Zone of inhibition (ZOI) diameter
(mm)
Antibiotic Coating
(Blood/synovial)
S. aureus SAP231 P. aeruginosa Xen41
CaSO4 beads only No 0 0
TOB No 30.6 ± 0.8 41 ± 0.6
VAN No 23.9 ± 0.8 ND
CaSO4 beads only Blood 0 0
TOB Blood 30.8 ± 0.5 41.2 ± 0.5
VAN Blood 24.2 ± 1.0 ND
CaSO4 beads only Synovial 0 0
16
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
TOB Synovial 30.5 ± 0.7 40.7 ± 0.9
VAN Synovial 23.9 ± 0.9 ND
ND = not determined; TOB = Tobramycin; VAN = Vancomycin
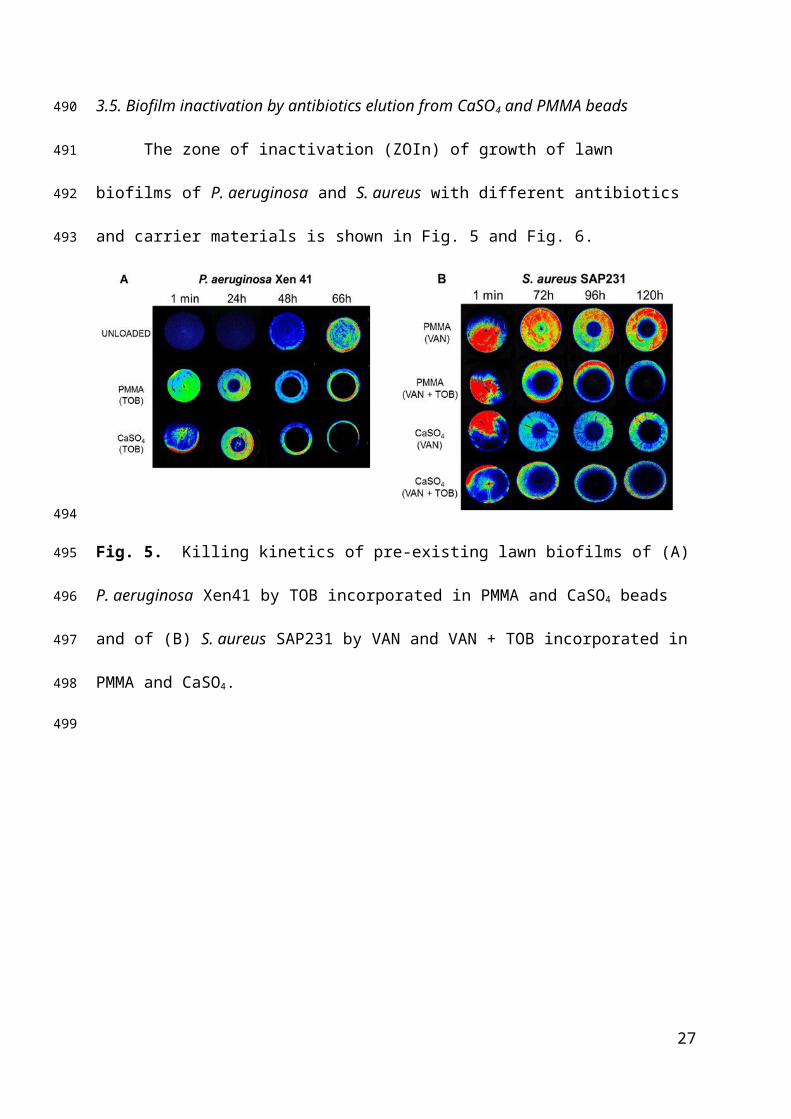
3.5. Biofilm inactivation by antibiotics elution from CaSO4 and PMMA beads
The zone of inactivation (ZOIn) of growth of lawn biofilms of P. aeruginosa and S.
aureus with different antibiotics and carrier materials is shown in Fig. 5 and Fig. 6.
Fig. 5. Killing kinetics of pre-existing lawn biofilms of (A) P. aeruginosa Xen41 by TOB
incorporated in PMMA and CaSO4 beads and of (B) S. aureus SAP231 by VAN and VAN +
TOB incorporated in PMMA and CaSO4.
17
354
355
356
357
358
359
360
361
362
363
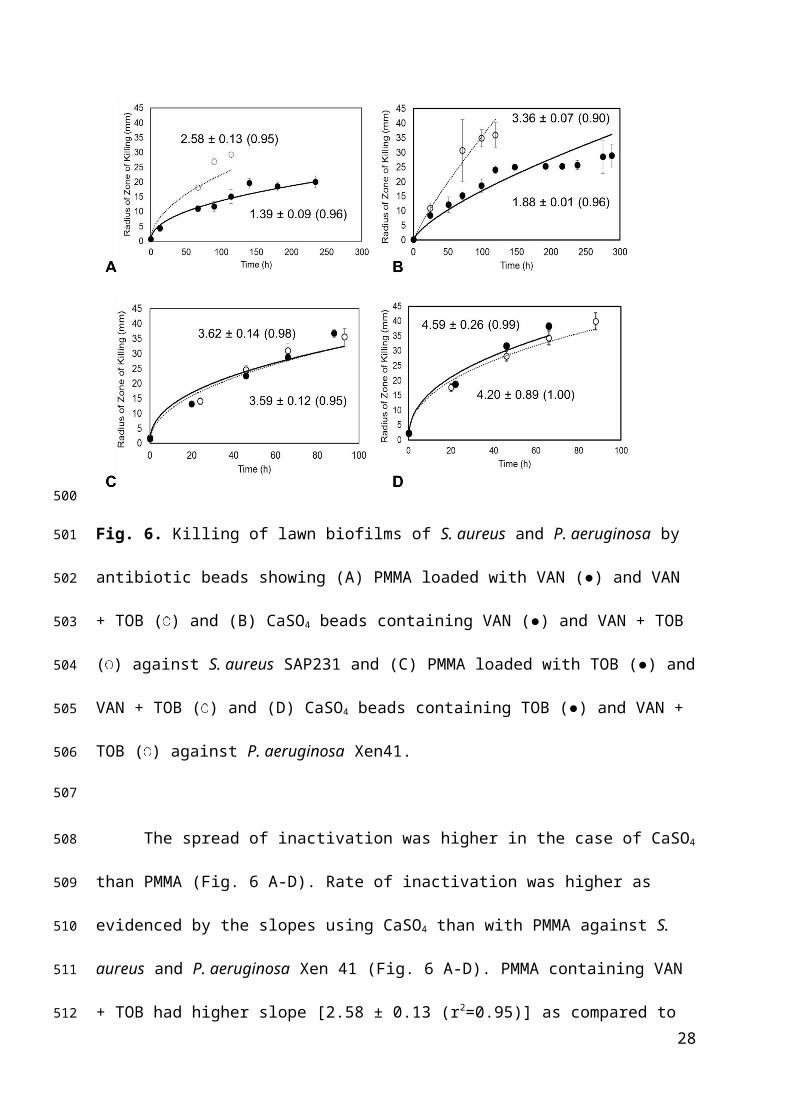
Fig. 6. Killing of lawn biofilms of S. aureus and P. aeruginosa by antibiotic beads showing
(A) PMMA loaded with VAN (●) and VAN + TOB ( ) and (B) CaSO4 beads containing
VAN (●) and VAN + TOB ( ) against S. aureus SAP231 and (C) PMMA loaded with TOB
(●) and VAN + TOB ( ) and (D) CaSO4 beads containing TOB (●) and VAN + TOB ( )
against P. aeruginosa Xen41.
The spread of inactivation was higher in the case of CaSO4 than PMMA (Fig. 6 A-D).
Rate of inactivation was higher as evidenced by the slopes using CaSO4 than with PMMA
against S. aureus and P. aeruginosa Xen 41 (Fig. 6 A-D). PMMA containing VAN + TOB
had higher slope [2.58 ± 0.13 (r2=0.95)] as compared to VAN alone [1.39 ± 0.09 (r2=0.96)]
against S. aureus suggesting increased rate of inactivation. CaSO4 on the other hand had
higher rate of inactivation with VAN + TOB [3.36 ± 0.07 (r2=0.90)] than VAN alone [1.88 ±
0.01 (r2=0.96)] against S. aureus. Against P. aeruginosa, the zone of inactivation with
PMMA containing TOB [3.59 ± 0.12 (r2=0.95)] was comparable with TOB + VAN [3.62 ±
18
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
0.14 (r2=0.98)]. Similarly, the difference was non-significant with CaSO4 containing TOB
antibiotic [4.59 ± 0.26 (r2=0.99)] and TOB + VAN [4.20 ± 0.89 (r2=1.00)].
The spread rate constants were higher for CaSO4 (P<0.05) than for PMMA,
demonstrating a faster release rate. TOB + VAN significantly increased the spread rate of
inactivation of lawn biofilms in the case of S. aureus from both cements than VAN alone,
suggesting a possible synergistic effect of the two antibiotics. However, the combination of
antibiotics had no significant effect on increasing the ZOIn with either of the cement
materials against P. aeruginosa (Fig. 6 C-D).
Areas within the ZOIn were swabbed from plates with P. aeruginosa and S. aureus
lawns containing antibiotic beads after day 3. S. aureus showed viable cells present in the
ZOIn with both cement beads containing antibiotics, whereas no growth of P. aeruginosa
Xen41 in the ZOIn was observed. Although this suggests complete eradication of P.
aeruginosa biofilms with antibiotics VAN and/or TOB, a longer antibiotic contact time may
be required to eradicate S. aureus SAP231.
3.6. Body fluids do not influence release from bone cement
The rate of elution of fluorescein from PMMA when coated with blood was
significantly slower (P<0.05) than with no fluids (Fig. 7). Heparinized blood had no influence
on the short-term (8 h) elution of fluorescein from CaSO4 (P˃0.05, data not shown).
19
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
Fig. 7. Release efficiency of fluorescein from CaSO4 (●) and PMMA (▲) beads coated with
or without blood ( ) or synovial fluid ( ).
3.7. Body fluids do not influence ZOI
Antibiotic-incorporated CaSO4 beads had the same ZOI regardless of whether they
were uncoated or were coated with blood or synovial fluid (Fig. 8 A-B).
Fig. 8. White light (A) and no light (luminescence) (B) images showing the influence of
blood or synovial fluid on ZOI of antibiotic (tobramycin) against the bioluminescent strain of
P. aeruginosa Xen41 after 24 h.
20
398
399
400
401
402
403
404
405
406
407
408
409

The ZOI by TOB in the absence of body fluids was 41 ± 0.6 mm against P.
aeruginosa Xen41 and 30.6 ± 0.8 mm against S. aureus SAP231 (Table 1). VAN showed a
ZOI of 23.9 ± 0.8 mm against S. aureus. In the presence of blood or synovial fluid, the ZOI
for TOB against S. aureus was 30.8 ± 0.5 or 30.5 ± 0.7 mm respectively, whereas for VAN
the ZOI was 24.2 ± 1.0 or 23.9 ± 0.9 mm respectively. Against P. aeruginosa, the ZOI with
TOB was 41 ± 0.6 that was statistically non-significant (P=0.39) when the beads were coated
with blood (41.2 ± 0.5mm) and synovial fluid (40.7 ± 0.9 mm) suggesting no influence of
body fluids on antibacterial activity.
4. Discussion
The delivery of local antibiotics for the management of musculoskeletal infection has
become increasingly popular [17, 37]. Initial high local concentration of antibiotic is
beneficial to eradicate resistant bacteria and biofilms that may be present at the site of
infection, even after debridement. High local concentrations of antibiotics facilitate diffusion
to avascular areas. These areas could remain inaccessible to systemic antibiotics and
organisms that are resistant to drug concentrations achieved by systemic antibiotic. Due to the
higher localized drug concentrations from antibiotic-loaded beads, these resistant organisms
may be more susceptible [37-39]. Fluorescein sodium, a freely water soluble and hydrophilic
compound was used as a fluorescent tracer for elution kinetic studies [16]. In this study,
fluorescein-loaded CaSO4 had a greater short-term rate of elution than PMMA (Fig. 4A-B).
The higher rate of elution could be due to differences in micropore structure and the
absorbable feature of CaSO4 as compared to the non-absorbable PMMA [5, 14].
Present and previous studies have shown that packing density is important when
considering the use of antibiotics in bone cements (PMMA and CaSO4) [5, 14], highlighting
the importance that initial release of antibiotics into a tissue or fluid may not be strongly
21
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
influenced by concentration. However, it is important that the packing density is adequate to
ensure spatial distribution of the antibiotic, particularly in areas that are diffusion-limited. If
impregnated CaSO4 beads initially release at the same rate regardless of antibiotic
concentration, it can be concluded that the higher the concentration of antibiotic, the longer
the bead will elute. Though, at high antibiotic impregnation, faster degradation may ensue
due to changes in the mechanical structure and properties of the bone cement beads [15, 29,
40] may lead to faster degradation. It is evident that the low concentration of fluorescein in
CaSO4 increases the short term ultimate compressive strength. At 2.0 g and 4.0 g (per 10cc)
fluorescein, CaSO4 became increasingly brittle and harder to mix, thus forming weaker beads.
When 1.0 g of fluorescein was incorporated in CaSO4, no difference in the ultimate
compressive strength was observed (Fig. 4C). Interestingly, even at 4.0 g there was little
influence of the mechanical strength on short-term release kinetics, even though the
significantly weaker strength suggested changes to the microstructure.
Biofilms are of major concern in PJI infections [13]. Due to the link between the
biofilm phenotype and the establishment of periprosthetic infection, additional studies were
undertaken to determine how effective antibiotic-loaded beads were at killing planktonic and
preformed lawn biofilms. Vancomycin and tobramycin were utilized because these two
antibiotics are commonly used in the treatment of PJI [5, 14]. Vancomycin is a popular
antibiotic due to its potential to prevent Gram-positive bacterial infections, which are mostly
due to methicillin resistant S. aureus (MRSA) [41]. Tobramycin is effective against both S.
aureus and the opportunistic pathogen, P. aeruginosa. When incorporated in a porous carrier
material (CaSO4) the short-term release and efficacy of antibiotics was significantly enhanced
as compared to PMMA. Our study showed that there was a faster initial release from CaSO4
beads than PMMA, as evidenced by the ZOIn and fluorescein spreading patterns (Fig. 4 and
5). This suggests higher killing of lawn biofilms from antibiotic-impregnated CaSO4 beads
22
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
(Fig. 6), which is consistent with the previous reports [5, 39, 42]. Furthermore, in previous
studies, delivery of vancomycin resulted in low release efficiency when delivered using non-
biodegradable materials such as PMMA [43, 44]. The lower antibiotic release from PMMA
could be because of the compact matrix capable of taking up only small quantities of
dissolution fluid into its outermost layers [23, 45]. Gradually, the dissolution fluid can
penetrate the bone cement to dissolve antibiotics within superficial regions of the bone
cement and fails to reach the interior of the bone cement. For example, gentamicin was only
released from the outer 100 μm of PMMA bone cement [45]. CaSO4 on the other hand is
more porous and absorbable than PMMA [5, 42, 46], therefore results in higher rate of
elution of antibiotics. The sustained release of antibiotics from bone cements is largely
affected by the penetration of fluids into the polymer matrix. Host factors such as in-vivo
interaction of the beads with blood, synovial fluid or clotting at the site of surgery could
affect the release and efficacy of antibiotics. Therefore considering the clinical relevance, the
influence of blood and synovial fluid on release kinetics and antibiotic activity from CaSO4
and PMMA beads was studied. Blood and synovial fluid showed no significant effects on
short term release kinetics or antibiotic activity.
All the elution studies in the present investigation were performed by assessing
diffusion into a solid hydrogel agar medium instead of the aqueous ‘infinite medium’
solution. In this case, the advantage of agar method for understanding how antibiotics might
spread into the surrounding tissue is two-fold since the elution distance and antibacterial
effects can be easily monitored, and it preserves the gradients that are likely to develop in-
vivo in areas that are diffusion-limited. However, there are certain limitations of this study,
wherein this is an in-vitro study, and did not evaluate the in-vivo elution kinetics or in-vivo
inhibition of bacterial biofilms. These issues will be examined in future studies with more
focus on clinical applications.
23
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
Antibiotic-infused bone cements are promising materials in fighting and preventing
PJIs. A greater short term rate of elution and antibiotic efficacy was observed with CaSO4
beads as compared to PMMA. Interestingly, this was independent of the loading density and
was not affected by exposure to body fluids. This study highlights the importance of
considering antibiotic loading and packaging density when investigating the clinical
application of bone cements for infection management.
Acknowledgements
We thank Biocomposites Ltd. for providing the Stimulan.
Figure Legends
Fig. 1. Surgical site of infection showing antibiotic loaded calcium sulfate (CaSO4) beads.
Fig. 2. Influence of single and multiple beads on local high concentration of antibiotic. ZOI
against P. aeruginosa PAO1 by multiple TOB-loaded CaSO4 beads after 24 h is relatively
similar as with single bead [16] (A) ††. Representative images showing fluorescein elution
through multiple beads after 24 h was indifferent than with single fluorescein-loaded CaSO4
(B). ††Adapted from [5].
Fig. 3. Short-term release kinetics of fluorescein from CaSO4 beads over a period of time (t in
minutes). Panel A shows fluorescent images of release of fluorescein from CaSO4 beads in
1% agar, and panel B shows the fluorescence intensity (FI) profile at different time intervals
and the radial distance travelled from the fluorescein incorporated CaSO4 bead.
Fig. 4. (A) Fluorescein elution radial distance from CaSO4 beads and PMMA; (B) Influence
of loading concentration of fluorescein in CaSO4 and PMMA beads on short-term release as a
function of time (t1/2); (C) Mechanical properties of fluorescein-loaded CaSO4 beads.
24
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
Fig. 5. Killing kinetics of pre-existing lawn biofilms of (A) P. aeruginosa Xen41 by TOB
incorporated in PMMA and CaSO4 beads and of (B) S. aureus SAP231 by VAN and VAN +
TOB incorporated in PMMA and CaSO4.
Fig. 6. Killing of lawn biofilms of S. aureus and P. aeruginosa by antibiotic beads showing
(A) PMMA loaded with VAN (●) and VAN + TOB ( ) and (B) CaSO4 beads containing
VAN (●) and VAN + TOB ( ) against S. aureus SAP231 and (C) PMMA loaded with TOB
(●) and VAN + TOB ( ) and (D) CaSO4 beads containing TOB (●) and VAN + TOB ( )
against P. aeruginosa Xen41.
Fig. 7. Release efficiency of fluorescein from CaSO4 (●) and PMMA (▲) beads coated with
or without blood ( ) or synovial fluid ( ).
Fig. 8. White light (A) and no light (luminescence) (B) images showing the influence of
blood or synovial fluid on ZOI of antibiotic (tobramycin) against the bioluminescent strain of
P. aeruginosa Xen41 after 24 h.
REFERENCES
[1] S.M. Kurtz, E. Lau, J. Schmier, K.L. Ong, K. Zhao, J. Parvizi, Infection burden for hip and knee arthroplasty in the United States, The Journal of arthroplasty, 23 (2008) 984-991.[2] S.M. Kurtz, E. Lau, H. Watson, J.K. Schmier, J. Parvizi, Economic burden of periprosthetic joint infection in the United States, The Journal of arthroplasty, 27 (2012) 61-65.e61.[3] D.N. Fish, H.M. Hoffman, L.H. Danziger, Antibiotic-impregnated cement use in U.S. hospitals, American journal of hospital pharmacy, 49 (1992) 2469-2474.[4] D.A. Wininger, R.J. Fass, Antibiotic-impregnated cement and beads for orthopedic infections, Antimicrobial agents and chemotherapy, 40 (1996) 2675-2679.[5] S.J. McConoughey, R.P. Howlin, J. Wiseman, P. Stoodley, J.H. Calhoun, Comparing PMMA and calcium sulfate as carriers for the local delivery of antibiotics to infected surgical sites, Journal of biomedical materials research. Part B, Applied biomaterials, 103 (2015) 870-877.[6] C.L. Nelson, The current status of material used for depot delivery of drugs, Clinical orthopaedics and related research, (2004) 72-78.[7] A.E. Gross, The role of polymethylmethacrylate bone cement in revision arthroplasty of the hip, The Orthopedic clinics of North America, 36 (2005) 49-54, vi.
25
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523524
525526527528529530531532533534535536537538539540541
[8] O.S. Kluin, H.C. van der Mei, H.J. Busscher, D. Neut, Biodegradable vs non-biodegradable antibiotic delivery devices in the treatment of osteomyelitis, Expert opinion on drug delivery, 10 (2013) 341-351.[9] S. Gitelis, G.T. Brebach, The treatment of chronic osteomyelitis with a biodegradable antibiotic-impregnated implant, Journal of orthopaedic surgery (Hong Kong), 10 (2002) 53-60.[10] A.S. Coetzee, Regeneration of bone in the presence of calcium sulfate, Archives of otolaryngology (Chicago, Ill. : 1960), 106 (1980) 405-409.[11] K.A. al Ruhaimi, Effect of calcium sulphate on the rate of osteogenesis in distracted bone, International journal of oral and maxillofacial surgery, 30 (2001) 228-233.[12] J.Y. Ferguson, M. Dudareva, N.D. Riley, D. Stubbs, B.L. Atkins, M.A. McNally, The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis: a series of 195 cases, The bone & joint journal, 96-b (2014) 829-836.[13] V.K. Aggarwal, M.R. Rasouli, J. Parvizi, Periprosthetic joint infection: Current concept, Indian Journal of Orthopaedics, 47 (2013) 10-17.[14] B.M. Howlin RP, Webb JS, Cooper JJ, Aiken SS, Stoodley P, Antibiotic-loaded synthetic calcium sulfate beads for prevention of bacterial colonization and biofilm formation in periprosthetic infections, Antimicrobial agents and chemotherapy, 59 (2015) 111-120.[15] G. Lewis, S. Janna, Estimation of the optimum loading of an antibiotic powder in an acrylic bone cement: gentamicin sulfate in SmartSet HV, Acta orthopaedica, 77 (2006) 622-627.[16] S.N. A. Seidlitz, B. Semmling, S. Petersen, T. Reske, W. Schmidt, N. Grabow, K. Sternberg, W. Weitschies, In vitro estimation of drug loss during the implantation procedure of drug-eluting stents Biomedical Engineering, 57 (2012) 403-406.[17] W.A. Jiranek, A.D. Hanssen, A.S. Greenwald, Antibiotic-loaded bone cement for infection prophylaxis in total joint replacement, The Journal of bone and joint surgery. American volume, 88 (2006) 2487-2500.[18] A. Bistolfi, G. Massazza, Vern, #233, E. , Mass, #232, A. , D. Deledda, S. Ferraris, M. Miola, F. Galetto, M. Crova, Antibiotic-Loaded Cement in Orthopedic Surgery: A Review, ISRN Orthopedics, 2011 (2011) 8.[19] K.E. Marks, C.L. Nelson, E.P. Lautenschlager, Antibiotic-impregnated acrylic bone cement, The Journal of bone and joint surgery. American volume, 58 (1976) 358-364.[20] M.J. Askew, M.F. Kufel, P.R. Fleissner, Jr., I.A. Gradisar, Jr., S.J. Salstrom, J.S. Tan, Effect of vacuum mixing on the mechanical properties of antibiotic-impregnated polymethylmethacrylate bone cement, Journal of biomedical materials research, 24 (1990) 573-580.[21] B.A. Masri, C.P. Duncan, C.P. Beauchamp, N.J. Paris, J. Arntorp, Effect of varying surface patterns on antibiotic elution from antibiotic-loaded bone cement, The Journal of arthroplasty, 10 (1995) 453-459.[22] A.S. Baker, L.W. Greenham, Release of gentamicin from acrylic bone cement. Elution and diffusion studies, The Journal of bone and joint surgery. American volume, 70 (1988) 1551-1557.[23] M.J. Penner, B.A. Masri, C.P. Duncan, Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement, The Journal of arthroplasty, 11 (1996) 939-944.[24] Y.H. Chang, C.L. Tai, H.Y. Hsu, P.H. Hsieh, M.S. Lee, S.W. Ueng, Liquid antibiotics in bone cement: an effective way to improve the efficiency of antibiotic release in antibiotic loaded bone cement, Bone & joint research, 3 (2014) 246-251.
26
542543544545546547548549550551552553554555556557558559560561562563564565566567568569570571572573574575576577578579580581582583584585586587588589590
[25] C.M. Stevens, K.D. Tetsworth, J.H. Calhoun, J.T. Mader, An articulated antibiotic spacer used for infected total knee arthroplasty: a comparative in vitro elution study of Simplex and Palacos bone cements, Journal of orthopaedic research : official publication of the Orthopaedic Research Society, 23 (2005) 27-33.[26] J. Jackson, F. Leung, C. Duncan, C. Mugabe, H. Burt, The use of bone cement for the localized, controlled release of the antibiotics vancomycin, linezolid, or fusidic acid: effect of additives on drug release rates and mechanical strength, Drug delivery and translational research, 1 (2011) 121-131.[27] S.S. Aiken, J.J. Cooper, H. Florance, M.T. Robinson, S. Michell, Local release of antibiotics for surgical site infection management using high-purity calcium sulfate: an in vitro elution study, Surgical infections, 16 (2015) 54-61.[28] T. Rimmele, E. Boselli, D. Breilh, S. Djabarouti, J.C. Bel, R. Guyot, M.C. Saux, B. Allaouchiche, Diffusion of levofloxacin into bone and synovial tissues, The Journal of antimicrobial chemotherapy, 53 (2004) 533-535.[29] G. Lewis, Properties of antibiotic-loaded acrylic bone cements for use in cemented arthroplasties: a state-of-the-art review, Journal of biomedical materials research. Part B, Applied biomaterials, 89 (2009) 558-574.[30] A.D. Hanssen, M.J. Spangehl, Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements, Clinical orthopaedics and related research, (2004) 79-85.[31] M.C. Plaut RD, Prabhakara R, Merkel TJ, Stibitz S, Stably Luminescent Staphylococcus aureus Clinical Strains for Use in Bioluminescent Imaging, PloS one, 8 (2013) 3.[32] T. Babrowski, C. Holbrook, J. Moss, L. Gottlieb, V. Valuckaite, A. Zaborin, V. Poroyko, D.C. Liu, O. Zaborina, J.C. Alverdy, Pseudomonas aeruginosa virulence expression is directly activated by morphine and is capable of causing lethal gut derived sepsis in mice during chronic morphine administration, Annals of Surgery, 255 (2012) 386-393.[33] G.S. Hirt H, Antimicrobial peptide GL13K is effective in reducing biofilms of Pseudomonas aeruginosa., Antimicrobial agents and chemotherapy, 57 (2013) 4903-4910.[34] R.P. Rennie, L. Turnbull, C. Brosnikoff, J. Cloke, First Comprehensive Evaluation of the M.I.C. Evaluator Device Compared to Etest and CLSI Broth Microdilution for MIC Testing of Aerobic Gram-Positive and Gram-Negative Bacterial Species, Journal of clinical microbiology, 50 (2012) 1147-1152.[35] R.E. Duey, A.C. Chong, D.A. McQueen, J.L. Womack, Z. Song, T.A. Steinberger, P.H. Wooley, Mechanical properties and elution characteristics of polymethylmethacrylate bone cement impregnated with antibiotics for various surface area and volume constructs, The Iowa orthopaedic journal, 32 (2012) 104-115.[36] M.G. Ficklin, K.A. Kunkel, J.T. Suber, P.D. Gerard, M.P. Kowaleski, Biomechanical evaluation of polymethyl methacrylate with the addition of various doses of cefazolin, vancomycin, gentamicin, and silver microparticles, Veterinary and comparative orthopaedics and traumatology : V.C.O.T, 29 (2016) 394-401.[37] A.D. Hanssen, Local antibiotic delivery vehicles in the treatment of musculoskeletal infection, Clinical orthopaedics and related research, (2005) 91-96.[38] A. Connaughton, A. Childs, S. Dylewski, V.J. Sabesan, Biofilm Disrupting Technology for Orthopedic Implants: What's on the Horizon?, Front Med (Lausanne), 1 (2014) 22.[39] G.W. Bowyer, N. Cumberland, Antibiotic release from impregnated pellets and beads, The Journal of trauma, 36 (1994) 331-335.[40] Y. He, J.P. Trotignon, B. Loty, A. Tcharkhtchi, J. Verdu, Effect of antibiotics on the properties of poly(methylmethacrylate)-based bone cement, Journal of biomedical materials research, 63 (2002) 800-806.
27
591592593594595596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633634635636637638639
[41] L.J. Lee SH, Baek WY, Lim JO, Regional delivery of vancomycin using pluronic F-127 to inhibit methicillin resistant Staphylococcus aureus (MRSA) growth in chronic otitis media in vitro and in vivo., J controlled release, 96 (2004) 1-7.[42] P. Udomkusonsri, S. Kaewmokul, S. Arthitvong, N. Phaochoosak, Elution profiles of cefazolin from PMMA and calcium sulfate beads prepared from commercial cefazolin formulations, The Journal of veterinary medical science / the Japanese Society of Veterinary Science, 74 (2012) 301-305.[43] B.K. Li B, Wenke JC, Guelcher SA, Sustained release of vancomycin from polyurethane scaffolds inhibits infection of bone wounds in a rat femoral segmental defect model. J Control Release., J controlled release, 145 (2010) 221-230.[44] C.J. Mader JT, Cobos J. , In vitro evaluation of antibiotic diffusion from antibiotic-impregnated biodegradable beads and polymethylmethacrylate beads. , Antimicrobial Agents and Chemotherapy. , 41 (1997) 415-418.[45] D.J. Schurman, C. Trindade, H.P. Hirshman, K. Moser, G. Kajiyama, P. Stevens, Antibiotic-acrylic bone cement composites. Studies of gentamicin and Palacos, The Journal of bone and joint surgery. American volume, 60 (1978) 978-984.[46] P. Frutos, E. Diez-Pena, G. Frutos, J.M. Barrales-Rienda, Release of gentamicin sulphate from a modified commercial bone cement. Effect of (2-hydroxyethyl methacrylate) comonomer and poly(N-vinyl-2-pyrrolidone) additive on release mechanism and kinetics, Biomaterials, 23 (2002) 3787-3797.
28
640641642643644645646647648649650651652653654655656657658659660661