Therapuetic drug monitoring
40
Jordan university of science and Technology –Department of medical laboratory sciences Therapeutic Drug Monitoring TDM Sarah Jaradat
-
Upload
sarah-jaradat -
Category
Health & Medicine
-
view
175 -
download
0
Transcript of Therapuetic drug monitoring

Jordan university of science and Technology –Department of medical laboratory sciences
Therapeutic Drug Monitoring TDM
Sarah Jaradat

Drug definition
• In Pharmacology , a drug is "a chemical substance used in the treatment, cure, prevention, or diagnosis of disease or used to otherwise enhance physical or mental well-being. Drugs may be prescribed for a limited duration, or on a regular basis for chronic disorders.

Forms Of Drugs In The Blood
• A drug in blood exists in two forms bound and unbound.
• Protein binding can influence the drug's biological half-life in the body.
• The bound portion may act as a reservoir from which the drug is slowly released as the unbound form.

Binding of drug to globulin
02-12-20104 KLECOP, Nipani

Basic And Acidic Drugs
• Weak acids efficiency absorbed in the stomach.
• Weak basics preferentially absorbed in the intestine.
• Since albumin is alkalotic, acidic and neutral drugs will primarily bind to albumin.
• If albumin becomes saturated, then these drugs will bind to lipoprotein. Basic drugs will bind to the acidic α1 acid glycoprotein.

Therapeutic drug monitoring
• Involves the analysis, assessment and evaluation of circulating concentrations of drugs in serum, plasma, or whole blood.
• The purpose of TDM is to ensure that the medication dose is at therapeutic range and not toxic.
• Medications dosage differ between each patient based on metabolic process.
• Therapeutic range is narrow for some drugs• below range: drug not effective
• above rang: drug toxic
• TDM can be used to : • To ensure maximal therapeutic benefit.
• To ensure minimal toxic adverse effects.
• For patient not responding to drug therapy.

Indications of TDM
• The consequences of overdosing and under dosing are serious.
• There is a small difference between a therapeutic and toxic dose.
• There is a change in the patient's physiologic state that may unpredictably affect circulating drug concentrations.
• A drug interaction may be occurring.
• TDM helps in monitoring patient compliance.

Routes Of Administration

Routes Of Administration
• For a drug to express a therapeutic benefit, it must be at the appropriate concentration at its site of action.
• Measuring drug concentration at the site of action would be ideal.
• Unfortunately, for most drugs, this cannot be done.
• The circulatory system offers a convenient route that can effectively deliver most drugs to its site of action
• The goal of most therapeutic regimens is to acquire a blood, plasma, or serum concentration that has been correlated with an effective concentration at the site of action

Factors That Influence The Circulating Concentration Of An Orally Drug :
• Formulation of the drug : tablets and capsules require dissolution.
• Most of the drugs absorbed by passive diffusion (So the drug must be in hydrophobic state).
• Weak acids efficiency absorbed in the stomach.
• Weak bases preferentially absorbed in the intestine.
• Changes in Intestinal motility , Stomach pH, Food or other drugs affect absorption.
• Absorption affected also by ; age , pregnancy , and pathological conditions.
Biological effect
• A drug is effective when it binds to a specific receptor in the target tissue.
• TDM assumes that serum levels are proportional to the intercellular tissue bind capacity of the drug.
• Drug utilization in the body is influenced by:• Absorption
• Distribution
• Metabolism
• Excretion

Pharmacokinetics (PK) Vs pharmacodynamics (PD)

Pharmacokinetic
PK - What the body does to the drug?
Absorption; distribution, metabolism, excretion (ADME)
Include measurement of drug concentrations in the blood or
plasma (serum)
Pharmacodynamic
PD - What the drug does to the body?
Drug concentration at the site of action or in the plasma is related to a magnitude of effect
Include clinical or laboratory measurements such arterial
blood pressure in patients with hypertension, or INR in patients treated with oral anticoagulants

Absorption
• The efficiency of drug absorption from GIT is dependent on many factors: Tablets and capsules require dissolution before being absorbed.
Liquid solutions are more rapidly absorbed.
Weak acids are efficiently absorbed in the stomach.
Weak bases are absorbed in the intestine.
Changes in intestinal motility, pH, inflammation, as well as food or other drugs may dramatically change absorption characteristics.

15
Absorption
• All substances, including drugs, absorbed from the intestine enter the hepatic portal system.
• certain drugs are subjected to significant hepatic uptake and metabolism (first-pass metabolism).
Absorption ma y be changed with age, pregnancy and pathologic conditions.
first-pass effect (also known as first-pass metabolism or
presystemic metabolism) is a phenomenon of drug
metabolism whereby the concentration of a drug is greatly reduced before it
reaches the systemic circulation


Distribution
• The free fraction of circulating drugs is subjected to diffusion out of the vasculature to the interstitial.
• The ability of the drug to leave the circulation is dependent on lipid solubility:
Hydrophobic drugs easily traverse cellular membrane i.e. adipose and nerve cells.
Polar but not ionized cross cell membrane but do not sequester.
Ionized drugs diffuse out of the vasculature at a slow rate.
• Volume of distribution index Vd used to describe the distribution characteristic of a drug :
Vd = D/Ct
Vd volume of distribution index ( liters).
D intravenous injected dose ( grams or mg)
Ct concentration in plasma (g/L or mg/L )
Hydrophobic drugs have high Vd , ionized have small Vd.

Drug Elimination
• Drugs can be cleared from the body by various mechanisms. Independent of the clearance mechanism, decreases in the serum
concentration of drugs most often occurs as first order process “ exponential rate of loss”.
this implies that the rate of change of drug concentrations over time varies continuously in relation to the concentration of drug.
• Hepatic metabolism or renal filtration, or a combination of the two, eliminates most drugs.
• Functional changes in these organs may result in changes in the rate of elimination.
• Half-life represents the time needed for the serum concentration to decrease by one half.


• Most drugs are xenobioticsSubstances not normally found within human system, yet capable of entering biochemical
pathways intended for endogenous substances.
• The biochemical pathway responsible for a large portion of drug metabolism is the hepatic mixed function oxidase "MFO" system.
• There are many enzymes involved in MFO system divided into 2 phases:1. Phase I produce reactive intermediates.
2. Phase II conjugations of functional groups to these reactive sites, the products are water soluble.
** Functional groups such as glutathione, glycine, phosphate and sulfate.
Metabolic Clearance

Renal Clearance
• Kidneys are the primary excretory organ.
• In Renal disease Other excretory organs or pathway become involved such as: biliary tract, lungs and sweat glands.
• H2O soluble drugs excrete faster than insoluble.
• Decreases in glomerular filtration rate directly results in increased serum half-life and concentration, aminoglycosides antibiotics and cyclosporine are examples of drugs with this behavior.

• Most drugs are not administered as a single bolus but
are delivered on a scheduled basis (e.g., once every
8 hours). With this type of administration, serum a drug
oscillates between a maximum (peak drug level) and a
minimum (trough drug level).
• The goal of a multiple dosage regimen is to achieve a
trough that is in the therapeutic range and a peak that
is not in the toxic range. Evaluation of this oscillating
function cannot be done immediately after initiation of a
scheduled dosage regimen. About seven doses are
required before a steady state oscillation is acquired.

Sample Collection• Timing of specimen collection is the single most important
factor in TDM.Collaborate with nursing & phlebotomy staff for appropriate timing
Trough concentration : right before next dose
Peak concentration : one hour post administration of dose (Verify drug protocol).
• Specimen TypeSerum: no gel
Plasma: Heparinized EDTA, Citrated, Oxalated not acceptable
Whole Blood
Saliva.

Factor Affecting Drug Protein Binding
1. factor relating to the drug :a) Physicochemical characteristic of drug.
b) Concentration of drug in the body.
c) Affinity of drug for a particular component.
2. factor relating to the protein and other binding component :a) Physicochemical characteristic of the protein or binding component.
b) Concentration of protein or binding component.
c) Number of binding site on the binding site.
3. drug interaction .
4. patient related factor.

Drugs commonly measured
A. Cardiac medications (digoxin)
B. Antibiotics (amikacin, gentamicin, vancomycin)
C. Antiepileptic drugs (phenobarbital)
D. Psychoactive Drugs (lithium)
E. Immunosuppressants (Cyclosporine)
F. Antineoplastics (Methotrexate)

Drug Groups: Cardio-active
• Digoxin
• Cardiac glycoside used in the treatment of Congestive heart failure.
• Serum concentrations greater than 2 ng/mL can cause adverse effects such as nausea, vomiting, visual disturbances and cardiac effects such as premature ventricular contraction.
• Serum levels peak between 2 and 3 hours after an oral dose.

Drug Groups: Cardio-active (2)
• Quinidine
• Used to treat cardiac arrhythmic problems
• Inhibits sodium and potassium channels
• Prevents arrhythmias, atrial flutter and fibrillation
• Procainamide
• Used to treat cardiac arrhythmic situations
• Blocks sodium channels
• Affects cardiac muscle contraction
• Often measured with NAPA(N-Acetyl procainamide)
Drug Groups: Antibiotics
• Aminoglycosides• Used to treat infections with gram-negative bacteria that are resistant to
less toxic antibiotics
• Inhibits protein synthesis of the micro-organism
• Examples include: gentamycin, tobramycin, amikacin and kanamycin
• Vancomycin• Used to treat infections with more-resistant gram-positive cocci and bacilli
• Inhibits cell wall synthesis
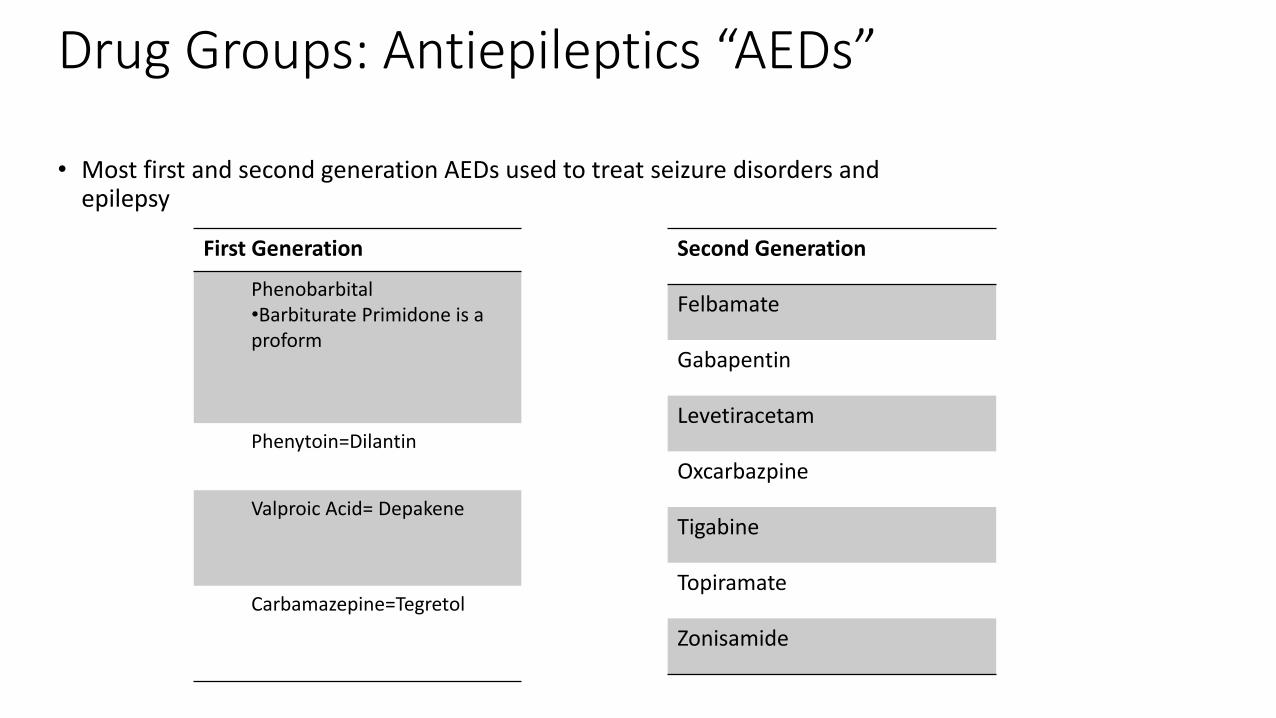
Drug Groups: Antiepileptics “AEDs”
• Most first and second generation AEDs used to treat seizure disorders and epilepsy
Second Generation
Felbamate
Gabapentin
Levetiracetam
Oxcarbazpine
Tigabine
Topiramate
Zonisamide
First Generation
Phenobarbital•Barbiturate Primidone is a proform
Phenytoin=Dilantin
Valproic Acid= Depakene
Carbamazepine=Tegretol

Drug Groups: Psychotherapeutic
• Used to treat manic depression (bipolar disorder)• Lithium
• Tricyclic Antidepressants “TCAs”
• Clozapine

Drug Group: Antiasthmatic
• Used to treat neonatal breathing disorders or respiratory disoders of adults or children, like asthma
• Examples include theophylline and theobromine

Drug Group: Immunosuppressive
• Monitoring of this group of drugs important to prevent organ rejection (host-versus-graft)
• Used to treat autoimmune disease
• Examples• Cyclosporine
• Whole blood is the specimen of choice, since it sequesters in the RBC
• Tacrolimus (Prograf)• Prevents rejection of liver and kidney transplants

Drug Group: Antineoplastics
• Inhibit RNA or DNA synthesis of tumor cells, leading to cell death
• Methotrexate• Inhibits DNA synthesis
Drug Group: Antihypertensive
• Used in treatment of high blood pressure
• Dilate blood vessels
• Sodium nitroprusside• Used for short-term control of hypertension

TDM ASSAY METHODOLOGIES
• ELISA: highly automated, rapidturnaround, moderate sensitivity but fewassays available, heterogenous.
• RIA: high sensitivity but long turnaround,many interferences, heterogenous, radiation hazards
• FPIA” fluorescence polarization immunoassay “:
highly automated, rapid turnaround,many assays available, stability of reagentsand calibration curves, moderate sensitivity,homogenous• HPLC: highest sensitivity, most assays
available, least expensive but long turnaround,requires highly trained personnel

Drug Time to steady state Sampling time Therapeutic range (mg/L)
AminoglycosidesAmikacin Adults
(< 30 y): ~ 2.5-15 h Peak 0.5-1 h after IV infusion Peak 15-25, Trough< 5Kanamycin (> 30 y): ~ 7.5-75 h (1 h after IM)Gentamicin Children: ~ 2.5-12.5 hDibekacin Neonate: ~ 10-45 h NetilmicinTobramicin Streptomycin 10-15 h Peak 1-2 h after IM Peak 15-40
Trough < 5
AntineoplasticsMethotrexate 12-24 h Depend on dose & 24 h > 5 umol/L
duration of infusion 48 h > 0.5 umol/L72 h > 0.05 umol/L
ImmunosuppressantsCyclosporine 1 d Day 3 or 4 of therapy, then 100-200 ug/L
twice weekly for few weeks and reduce to every 1-2 mo

Drug Time to steady state Sampling time Therapeutic range (mg/L)
AntiarrhythmicsDisopyramide 1-2 d Trough 2-5Lidocaine 1 h after LD 2 h after LD 1.5-5
5-10 h (no LD) 6-12 h (no LD) Procainamide/NAPA
Adult (no LD) Immediately after IV LD Procainamide 4-10: normal renal 15-25 h 2 h after start of IV infusion, NAPA 6-20: renal insuff 30-65 h once more during 24 h period
Oral: peak (1-4 h) and troughQuinidine 2 d Trough 2-5
Cardiac GlycosidesDigitoxin 1 mo 8-24 h 13-25 ug/L Digoxin 5-7 d 8-24 h 0.9-2.2 ug/L
May be longer in renal insufficiency

Drug Time to steady state Sampling time Therapeutic range
(mg/L)AntiepilepticsCarbamazepine 2-6 d Trough 4-10Ethosuximide 1-2 wk Any time 40-100Phenobarbital 3 wk Any time 15-40Phenytoin 7 d 2-4 h 10-20
Valproate 2-3 d Trough 50-100
BronchodilatorsTheophylline Adult: 2 d IV: 30 min after IV LD 10-20
Children: 1-2 d : 4-6 h after beginning therapyInfants: 1-5 d : 12-18 h after beginning therapyNewborn: 120 h Oral: peak Premy: 150 h 2 h after rapid release prep
4 h after sustained release prep

Drug Time to steady state Sampling time Therapeutic range (mg/L)
AnalgesicsAspirin 1-5 d 1-3 h 150-300 (antiinflam.)
250-400 (rheumatic fev)Paracetamol 4 h postingestion > 200toxicity 12 h postingestion > 50
Psychoactive DrugsAmitriptyline 3-8 d Trough 150-250 ug/LImipramine 2-5 d Trough 150-250 ug/LNortriptyline 4-20 d Trough 50-150 ug/LLithium 3-7 d Trough 0.6-1.2 mEq/L