herapeutic Drug Monitoring Course · PDF fileherapeutic Drug Monitoring ... patient's drug...
47
Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines ــــــــــــــــــــــــــــــــــــ0 T T T Therapeutic herapeutic herapeutic herapeutic Clinical Toxicology Lines Series Dr: Dr: Dr: Dr: Maha Al Maha Al Maha Al Maha Al-Ma Ma Ma Ma Head of Dammam Poison Contro ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ـــــــــ ــــــــــــــــــــــــــــــــــــDrug Monitorin Drug Monitorin Drug Monitorin Drug Monitorin s azroua azroua azroua azroua ol Center Dr: Ahmed Dr: Ahmed Dr: Ahmed Dr: Ahmed Toxicology Consultant D ـ ـــــــــــــــــــــــــــــــــــDr: Ahmed Refat Dr: Ahmed Refat Dr: Ahmed Refat Dr: Ahmed Refat ــــــــــــــــــــــــــــAntidote Course ng ng ng ng Course Course Course Course Refat Refat Refat Refat Dammam PCC
Transcript of herapeutic Drug Monitoring Course · PDF fileherapeutic Drug Monitoring ... patient's drug...

Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines ــــــــــــــــــــــــــــــــــــــــــــ
0
TTTTherapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring
Clinical Toxicology Lines Series
Dr: Dr: Dr: Dr: Maha AlMaha AlMaha AlMaha Al----MazrouaMazrouaMazrouaMazroua
Head of Dammam Poison Control Center
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
herapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring
Clinical Toxicology Lines Series
MazrouaMazrouaMazrouaMazroua
Head of Dammam Poison Control Center
Dr: Ahmed RefatDr: Ahmed RefatDr: Ahmed RefatDr: Ahmed Refat
Toxicology Consultant Dammam PCC
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed RefatDr: Ahmed RefatDr: Ahmed RefatDr: Ahmed Refat
Antidote Courseـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
herapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring herapeutic Drug Monitoring CourseCourseCourseCourse
Dr: Ahmed RefatDr: Ahmed RefatDr: Ahmed RefatDr: Ahmed Refat
Toxicology Consultant Dammam PCC

Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines ــــــــــــــــــــــــــــــــــــــــــــ
1
Therapeutic Drug Monitoring Course
IIII---- IIIIntroductionntroductionntroductionntroduction
Therapeutic drug monitoring and pharmacogenomics are both clinical toxicology
related areas within the clinical laboratory. Although each
laboratory medicine, the two fields overlap significantly. This course provides an overview of each
of these laboratory sub-disciplines and discusses the utility, rationale, and practice of each one.
The course is intended for clinical toxicologist, clinical laboratory health care personnel and other
technologists and technicians who are responsible for monitoring, prescribing and administering
therapeutic medications.
IIIIIIII---- CCCCourse Outlineourse Outlineourse Outlineourse Outline
A: Therapeutic Drug Monitoring� Introduction
� Therapeutic Drug Monitoring Definition
� Pharmacogenomics Definition
� Basic Pharmacokinetics
� Drug Concentration Over Time
� Drug Metabolism
� Drug Elimination
� Half-life
� Bioavailability
� Protein Binding
� Protein Availability and Drug Dosing
� Other Factors Affecting Drug Absorption and Distribution
� Given what you have learned thus far, which of the follo
true?
� Steady State
� Steady State Example
� Sampling
� Peak and Trough Sampling Times
� Why TDM?
� Unexpected Concentrations
� A physician needs to prescribe a drug to a patient but the drug has a narrow therapeutic
window. He is concerned about possible toxic effects. To asse...
� TDM For All Drugs?
� When is TDM Not Useful?
� Alternative to TDM
� Examples of Drugs That are Monitored by TDM
� TDM for Antibiotics
� TDM for Anticonvulsants
� TDM for Immunosuppressants
� TDM for Cardiac Medications
� TDM for Theophylline
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
herapeutic Drug Monitoring Course
Therapeutic drug monitoring and pharmacogenomics are both clinical toxicology
related areas within the clinical laboratory. Although each is considered a sub
laboratory medicine, the two fields overlap significantly. This course provides an overview of each
disciplines and discusses the utility, rationale, and practice of each one.
ended for clinical toxicologist, clinical laboratory health care personnel and other
technologists and technicians who are responsible for monitoring, prescribing and administering
A: Therapeutic Drug Monitoring………………………………………………………………...5
Therapeutic Drug Monitoring Definition
Pharmacogenomics Definition
Drug Concentration Over Time
Protein Availability and Drug Dosing
Other Factors Affecting Drug Absorption and Distribution
Given what you have learned thus far, which of the following statements below do you think is
Peak and Trough Sampling Times
Unexpected Concentrations
A physician needs to prescribe a drug to a patient but the drug has a narrow therapeutic
concerned about possible toxic effects. To asse...
When is TDM Not Useful?
Examples of Drugs That are Monitored by TDM
TDM for Anticonvulsants
TDM for Immunosuppressants
TDM for Cardiac Medications
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Therapeutic drug monitoring and pharmacogenomics are both clinical toxicology-
is considered a sub-discipline within
laboratory medicine, the two fields overlap significantly. This course provides an overview of each
disciplines and discusses the utility, rationale, and practice of each one.
ended for clinical toxicologist, clinical laboratory health care personnel and other
technologists and technicians who are responsible for monitoring, prescribing and administering
………………………………………………………………...5
wing statements below do you think is
A physician needs to prescribe a drug to a patient but the drug has a narrow therapeutic

� � � � � � � � � � � � � � � � � � � � Clinical Toxicology Lines Clinical Toxicology Lines Clinical Toxicology Lines ــــــــــــــــــــــــــــــــــــــــــــ
2
� Albuterol is a fast-acting bronchodilator used acutely during asthma attacks. Which of the
reasons below explains why TDM for albuterol is not availab...
� Laboratory Methods
� PETINIA
� FPIA
� Chemiluminescenc
B: Pharmacogenomics…………………………………� Individualized Medicine
� Polymorphism and CYP450
� CYP450s
� CYP2D6
� Metabolizers
� Enzyme Abnormalities and Drugs
� Clinical Utility
� Warfarin Metabolism
� A person who is classified as an ultrarapid metabolizer (UM) would need of a drug metabolized
by that enzyme.
� CYP450 Induction and Inhibition
� A patient is taking cimetidine for a stomach ulcer. This drug inhibits CYP2D6. The patient is
now prescribed amphetamine for narcolepsy. Amphetamine i...
� Genotype versus Phenotype
� TDM and PGx
� The Bottom Line
C: Individualized TDM Drug Profiles
D: References:……………………………………………………………………………………...47
E: Practical Settings:
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
acting bronchodilator used acutely during asthma attacks. Which of the
reasons below explains why TDM for albuterol is not availab...
………………………………………………………………………….17
Polymorphism and CYP450
Enzyme Abnormalities and Drugs
A person who is classified as an ultrarapid metabolizer (UM) would need of a drug metabolized
CYP450 Induction and Inhibition
A patient is taking cimetidine for a stomach ulcer. This drug inhibits CYP2D6. The patient is
now prescribed amphetamine for narcolepsy. Amphetamine i...
Genotype versus Phenotype
Profiles……………………………………………………………..23
……………………………………………………………………………………...47
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
acting bronchodilator used acutely during asthma attacks. Which of the
……………………………………….17
A person who is classified as an ultrarapid metabolizer (UM) would need of a drug metabolized
A patient is taking cimetidine for a stomach ulcer. This drug inhibits CYP2D6. The patient is
……………………………………………………………..23
……………………………………………………………………………………...47

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
3
IIIIIIIIIIII---- CCCCourse ourse ourse ourse contentcontentcontentcontent
Introduction
Therapeutic drug monitoring and pharmacogenomics are both
within the clinical laboratory. Although each is
the two fields overlap significantly. In this course, we w
laboratory sub-disciplines and discuss the utility, rationale, and practice of each one.
Therapeutic Drug Monitoring Definition
Therapeutic Drug Monitoring (TDM) is a branch of clinical chemistry that specializes
measurement of medication levels in
measurements of drugs and/or their metabolites. These measurements are
patient serum samples. TDM can be contrasted with urine drug
performed to detect or monitor drug abuse or check patient compliance when a drug with high abuse
potential has been prescribed. Determining actual concentrations are less important for urine drugs of
abuse screening. Providing accurate concentrations for TDM,
concentrations provided with TDM allow clinicians to adjust medication dosages as well as
patient's drug metabolism response and their compliance or dosing regimen.
Pharmacogenomics DefinitionPharmacogenomics (usually abbreviated PGx) is the study of how variations in the human
genome affect a given individual's response
handled by a specific person given
Basic Pharmacokinetics In order to discuss TDM and PGx we need to also introduce the concept of pharmacokinetics.
Pharmacokinetics is the study of drug disposition in the body: It
the circulation, how long they remain in the blood, and how they are ultimately eliminated from the
body. TDM is the clinical assessment of a drug's pharmacokinetic properties. Physicians and
toxicologist, pharmacists often need to establish that a
concentration yet does not reach a toxic concentration.
factors that determine a drug's disposition in the body. These factors ultima
therapeutic drug monitoring.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Therapeutic drug monitoring and pharmacogenomics are both clinical toxicology
within the clinical laboratory. Although each is considered a sub-discipline within laboratory medicine,
the two fields overlap significantly. In this course, we will provide an overview of
disciplines and discuss the utility, rationale, and practice of each one.
Therapeutic Drug Monitoring Definition
Therapeutic Drug Monitoring (TDM) is a branch of clinical chemistry that specializes
measurement of medication levels in serum. TDM requires that the laboratory make quantitative
measurements of drugs and/or their metabolites. These measurements are almost always made on
patient serum samples. TDM can be contrasted with urine drug testing. Urine drug testing is usually
performed to detect or monitor drug abuse or check patient compliance when a drug with high abuse
Determining actual concentrations are less important for urine drugs of
Providing accurate concentrations for TDM, on the other hand, is essential. Serum
concentrations provided with TDM allow clinicians to adjust medication dosages as well as
patient's drug metabolism response and their compliance or dosing regimen.
Pharmacogenomics Definition Pharmacogenomics (usually abbreviated PGx) is the study of how variations in the human
genome affect a given individual's response to medications. It refers to how administered drugs will be
handled by a specific person given specific genetic mutations and polymorphisms they may have.
In order to discuss TDM and PGx we need to also introduce the concept of pharmacokinetics.
Pharmacokinetics is the study of drug disposition in the body: It concerns how and when drugs enter
remain in the blood, and how they are ultimately eliminated from the
TDM is the clinical assessment of a drug's pharmacokinetic properties. Physicians and
ists often need to establish that a drug is present at a clinically
concentration yet does not reach a toxic concentration. The next few pages will describe some of the
factors that determine a drug's disposition in the body. These factors ultimately decide the
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
clinical toxicology -related areas
discipline within laboratory medicine,
ill provide an overview of each of these
disciplines and discuss the utility, rationale, and practice of each one.
Therapeutic Drug Monitoring (TDM) is a branch of clinical chemistry that specializes in the
serum. TDM requires that the laboratory make quantitative
almost always made on
testing. Urine drug testing is usually
performed to detect or monitor drug abuse or check patient compliance when a drug with high abuse
Determining actual concentrations are less important for urine drugs of
on the other hand, is essential. Serum
concentrations provided with TDM allow clinicians to adjust medication dosages as well as assess a
Pharmacogenomics (usually abbreviated PGx) is the study of how variations in the human
to medications. It refers to how administered drugs will be
polymorphisms they may have.
In order to discuss TDM and PGx we need to also introduce the concept of pharmacokinetics.
concerns how and when drugs enter
remain in the blood, and how they are ultimately eliminated from the
TDM is the clinical assessment of a drug's pharmacokinetic properties. Physicians and clinical
drug is present at a clinically-effective
The next few pages will describe some of the
tely decide the need for

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
4
Drug Concentration Over Time
When a drug enters the body, it reaches a peak concentration
eliminated. The figure on the right shows a typical drug kinetic when a dr
Drug Metabolism
The liver plays a major role in converting lipophilic, nonpolar molecules (including drugs) to
more polar, water-soluble forms through a
modified by either phase I or phase ll reactions. These reactions are carried
classes of enzymes.
- Phase I reactions alter chemical structure by oxidation, reduction, or hydrolysis.
- Phase ll reactions conjugate drugs to create p
Drug Elimination
Most water-soluble drugs are eliminated from the b
filtration, or a combination of the two. It
soluble. When a small molecular
by simple filtration through the kidneys and it will then enter the urine. Since fatty, nonpolar
molecules do not dissolve in water they tend to accumulate in tissues or bi
Until the body can render these molecules
An alteration in renal function will have a major effect on the clearance of the drug or its active
metabolite(s). Decreased renal function
Half-life
The amount of time it takes for a drug concentration in the body to decrease by 50% is called
the drug's half-life (abbreviated t1/2).
body. Most drugs are eliminated from the body in 1 to 3 days, but some
can still be detected in the body weeks after the initial dose.
kinetic pattern for an oral drug.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Drug Concentration Over Time
When a drug enters the body, it reaches a peak concentration that starts to fall as the drug is
right shows a typical drug kinetic when a drug is given
The liver plays a major role in converting lipophilic, nonpolar molecules (including drugs) to
soluble forms through a series of enzymatic reactions. Drug molecules can be
modified by either phase I or phase ll reactions. These reactions are carried out by several important
Phase I reactions alter chemical structure by oxidation, reduction, or hydrolysis.
Phase ll reactions conjugate drugs to create products that are water-soluble.
soluble drugs are eliminated from the body through hepatic metabolism,
filtration, or a combination of the two. It makes sense that the body would aim to make a drug water
small molecular-weight compound is water soluble, it can be excreted from the blood
by simple filtration through the kidneys and it will then enter the urine. Since fatty, nonpolar
do not dissolve in water they tend to accumulate in tissues or bind strongly to proteins.
Until the body can render these molecules water-soluble, they are much less likely to be excreted.
An alteration in renal function will have a major effect on the clearance of the drug or its active
unction results in elevated serum drug concentrations.
The amount of time it takes for a drug concentration in the body to decrease by 50% is called
life (abbreviated t1/2). The longer a drug's half-life, the slower it is remov
body. Most drugs are eliminated from the body in 1 to 3 days, but some drugs with longer half
can still be detected in the body weeks after the initial dose. The figure below illustrates a typical
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
that starts to fall as the drug is
ug is given intravenously (IV).
The liver plays a major role in converting lipophilic, nonpolar molecules (including drugs) to
series of enzymatic reactions. Drug molecules can be
out by several important
Phase I reactions alter chemical structure by oxidation, reduction, or hydrolysis.
soluble.
ody through hepatic metabolism, renal
makes sense that the body would aim to make a drug water
can be excreted from the blood
by simple filtration through the kidneys and it will then enter the urine. Since fatty, nonpolar
nd strongly to proteins.
soluble, they are much less likely to be excreted.
An alteration in renal function will have a major effect on the clearance of the drug or its active
results in elevated serum drug concentrations.
The amount of time it takes for a drug concentration in the body to decrease by 50% is called
life, the slower it is removed from the
drugs with longer half-lives
The figure below illustrates a typical

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
5
Bioavailability
Bioavailability refers to the amount of drug that actually reaches
by comparing (in the same subjects) the area of the curve (AUC) that is found under the
concentration kinetic graph. This is done u
form. Then the two areas are compared. This is illustrated in the diagram on
oral drug that makes it to the circulatory system is the bioavailability of that drug.
bioavailability is 100%.
For oral medications, the bioavailability will be less than 100%,
reasons: 1- Oral drugs have slower absorption and distribution than IV
that is absorbed can depend on the status
integrity/health of the intestines, speed of the GI tract, etc.)
enzymes that are present anywhere along the GI tract.
If bioavailability is low then the
achieves the appropriate serum
IV drug and the drug takes longer to enter the circulation, clearing the drug will also
longer time.
Protein Binding
Most drugs are bound to proteins when they
considering general solubility rules of
lithium, it will easily dissolve into the aqueous environment of the
the circulation. However most drugs are complex
For drugs that are not highly soluble in
to solubilize that drug into blood. Serum contains a myriad of proteins.
Although these proteins themselves are water
they often contain lipophilic regions on them, which
drugs through the circulation.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Bioavailability refers to the amount of drug that actually reaches the circulation. It is calculated
subjects) the area of the curve (AUC) that is found under the
concentration kinetic graph. This is done using an equivalent dose of the intravenous form and oral
two areas are compared. This is illustrated in the diagram on the right. The fraction of
circulatory system is the bioavailability of that drug.
For oral medications, the bioavailability will be less than 100%, due in part to any of these
Oral drugs have slower absorption and distribution than IV drugs. 2
depend on the status of the GI tract (stomach pH, presence of food,
the intestines, speed of the GI tract, etc.). Oral drugs may be broken down by
anywhere along the GI tract.
If bioavailability is low then the oral dose needed has to be increased so that a given dose
achieves the appropriate serum concentration. Since the absorption of an oral drug is slower than an
IV drug and the drug takes longer to enter the circulation, clearing the drug will also
Most drugs are bound to proteins when they circulate in the body. This makes sense when
considering general solubility rules of chemistry. If a drug is simple, eg, an elemental salt such as
dissolve into the aqueous environment of the blood and widely distribute through
circulation. However most drugs are complex organic molecules with variable solubility in
For drugs that are not highly soluble in an aqueous environment, some carrier protein
blood. Serum contains a myriad of proteins.
Although these proteins themselves are water soluble (since they are found dissolved in
they often contain lipophilic regions on them, which can bind non-polar drugs and thus carry these
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
the circulation. It is calculated
subjects) the area of the curve (AUC) that is found under the serum
equivalent dose of the intravenous form and oral
the right. The fraction of
circulatory system is the bioavailability of that drug. For IV drugs, the
due in part to any of these
2- The amount of drug
of the GI tract (stomach pH, presence of food,
Oral drugs may be broken down by
oral dose needed has to be increased so that a given dose
Since the absorption of an oral drug is slower than an
IV drug and the drug takes longer to enter the circulation, clearing the drug will also most likely take a
circulate in the body. This makes sense when
elemental salt such as
blood and widely distribute through
organic molecules with variable solubility in water.
ome carrier protein will be needed
soluble (since they are found dissolved in blood)
polar drugs and thus carry these

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
6
Albumin is a major drug-binding protein in serum.
neutral drugs primarily bind to it.
can bind to lipoproteins. Alkaline drugs tend to bind to globulins, particularly to a globulin called alpha
1 acid glycoprotein. Only free, unbound drugs are able to bind protein drug receptors on cells and
have therapeutic effects.
An equilibrium exists in the systemic circulation between a free and protein
between a free and receptor-bound drug. This
Protein Availability and Drug Dosing
Drug-binding proteins in serum can fluctuate in disease states.
fall, as can occur in liver failure or
If this happens a new dose of drug may produce a toxic concentration of f
now lower. The image on the right illustrates the loss of equilibrium between a protein
and a free drug when drug-binding proteins are diminished.
bound may need to be adjusted in
common drugs that are highly protein
imipramine and phenytoin.
Conclusion: So far we have learned that many factors (proteinbioavailability, elimination, etc.) affect a drug's disposition in the body. Because we usually cannot safely
predict how a drug will be tolerated in a person, we use therapeutic drug monitoring (TDM) to verify that
a drug is present at an appropriate
Other Factors Affecting Drug Absorption and Distribution
In addition to protein availability, other factors may affect drug absorption and distribution in
the body as a whole or within specific
other factors.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
binding protein in serum. Albumin is an alkaline protein, so acidic and
neutral drugs primarily bind to it. If albumin binding sites become saturated, acidic and neutral drugs
Alkaline drugs tend to bind to globulins, particularly to a globulin called alpha
Only free, unbound drugs are able to bind protein drug receptors on cells and
An equilibrium exists in the systemic circulation between a free and protein
bound drug. This is illustrated in the image to the right.
Protein Availability and Drug Dosing
in serum can fluctuate in disease states. For example, if albumin levels
fall, as can occur in liver failure or nephritic syndrome, less albumin will be available for drug binding.
dose of drug may produce a toxic concentration of free drug since albumin is
The image on the right illustrates the loss of equilibrium between a protein
binding proteins are diminished. Doses of drugs that are highly protein
bound may need to be adjusted in patients with lower drug-binding protein levels.
common drugs that are highly protein-bound include thyroxine, warfarin, diazepam, heparin,
So far we have learned that many factors (protein
bioavailability, elimination, etc.) affect a drug's disposition in the body. Because we usually cannot safely
predict how a drug will be tolerated in a person, we use therapeutic drug monitoring (TDM) to verify that
nt at an appropriate.
Other Factors Affecting Drug Absorption and Distribution
In addition to protein availability, other factors may affect drug absorption and distribution in
the body as a whole or within specific sites of the body. The following table highlights some of these
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Albumin is an alkaline protein, so acidic and
saturated, acidic and neutral drugs
Alkaline drugs tend to bind to globulins, particularly to a globulin called alpha-
Only free, unbound drugs are able to bind protein drug receptors on cells and
An equilibrium exists in the systemic circulation between a free and protein-bound drug and
is illustrated in the image to the right.
For example, if albumin levels
albumin will be available for drug binding.
ree drug since albumin is
The image on the right illustrates the loss of equilibrium between a protein-bound drug
Doses of drugs that are highly protein-
binding protein levels. Examples of some
thyroxine, warfarin, diazepam, heparin,
binding, lipophilicity,
bioavailability, elimination, etc.) affect a drug's disposition in the body. Because we usually cannot safely
predict how a drug will be tolerated in a person, we use therapeutic drug monitoring (TDM) to verify that
In addition to protein availability, other factors may affect drug absorption and distribution in
following table highlights some of these

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
7
Factor Discussion
Regional blood flow
Reduced area blood flow can be seen in diabetics and enhanced blood flow can be
seen in tumors. Reduced blood flow means reduced exposure to drug.
Lipid solubility of the drug
The more lipophilic a drug is, the more likely it will enter the central nervous
system. The brain itself is a very lipid
normal web of epithelial cells in the CNS blood vessels.
blood-brain-barrier. Lipophilic drugs can cross cell membranes of this barrier more
easily than polar drugs.
The integrity of the GI tract
In a diseased gut, an orally
Age
Drug kinetics and dispositions change throughout life. In general,
drugs is reduced in the elderly.
Genetics
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
disposition.
Steady State
Most drugs are not given as a single dose but are part of a multi
physician's responsibility to prescribe a drug such that the concentration of that drug reaches a
and effective level as quickly as possible without inducing toxicity. The
clinician, if multiple doses of a drug will be given, is for both the peak and the trough
consistently within the therapeutic range.
life, it will take about 5 half-lives to
Steady State Example
If the drug Gentamicin has an elimination half
drug should reach steady state
dosing results in a 'sawtooth' pattern. Peaks correspond to the times right after the drug is taken;
troughs correspond to the times right before the
Of course a physician may want to get a patient into the therapeutic range mor
these cases a higher loading dose of drug can be prescribed initially with instructions that after the
first couple of doses, the dose should be reduced.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Reduced area blood flow can be seen in diabetics and enhanced blood flow can be
seen in tumors. Reduced blood flow means reduced exposure to drug.
solubility of the drug
The more lipophilic a drug is, the more likely it will enter the central nervous
system. The brain itself is a very lipid rich organ but there also exists a tighter
normal web of epithelial cells in the CNS blood vessels. This leads to the so called
barrier. Lipophilic drugs can cross cell membranes of this barrier more
easily than polar drugs.
The integrity of the GI tract
In a diseased gut, an orally-administered drug may not be absorbed as expected.
Drug kinetics and dispositions change throughout life. In general,
drugs is reduced in the elderly.
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
given as a single dose but are part of a multi dose regimen. It is the
physician's responsibility to prescribe a drug such that the concentration of that drug reaches a
and effective level as quickly as possible without inducing toxicity. The dosing-goal for the
clinician, if multiple doses of a drug will be given, is for both the peak and the trough
consistently within the therapeutic range. If a drug is given at intervals that are the same as its half
lives to reach steady state.
If the drug Gentamicin has an elimination half-life of 12 hours and is given every 12 hours, the
after 5 half-lives (60 hours). Notice in the diagram th
dosing results in a 'sawtooth' pattern. Peaks correspond to the times right after the drug is taken;
troughs correspond to the times right before the next dose.
Of course a physician may want to get a patient into the therapeutic range mor
dose of drug can be prescribed initially with instructions that after the
first couple of doses, the dose should be reduced.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Reduced area blood flow can be seen in diabetics and enhanced blood flow can be
seen in tumors. Reduced blood flow means reduced exposure to drug.
The more lipophilic a drug is, the more likely it will enter the central nervous
rich organ but there also exists a tighter-than
This leads to the so called
barrier. Lipophilic drugs can cross cell membranes of this barrier more
administered drug may not be absorbed as expected.
Drug kinetics and dispositions change throughout life. In general, metabolism of
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
dose regimen. It is the
physician's responsibility to prescribe a drug such that the concentration of that drug reaches a safe
goal for the prescribing
clinician, if multiple doses of a drug will be given, is for both the peak and the trough drug levels to be
If a drug is given at intervals that are the same as its half-
life of 12 hours and is given every 12 hours, the
lives (60 hours). Notice in the diagram that this kind of
dosing results in a 'sawtooth' pattern. Peaks correspond to the times right after the drug is taken;
Of course a physician may want to get a patient into the therapeutic range more quickly. In
dose of drug can be prescribed initially with instructions that after the

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
8
Sampling
Ideally, a drug level would be monitored frequently and
a detailed pharmacokinetic profile over time.
relatively infrequent clinic visits,
concentration 'snap-shot' is taken. This then requires us to ask: 'when should we collect blood in order
to best measure the serum concentration of the drug in question?'
Peak and Trough Sampling Times
A trough refers to the valley or bottom 'spike' of the
drug is taken orally the trough will be the low point of the serum concentration. It will be
period immediately before the next dose. Thus, when we want to draw a trough
before the patient is supposed to take their next dose.
concentration) the time for drawing depends
kinetics of the drug.
For oral medications One hour after drug is taken is usuall
> two hours). For IV medications: sample 15
(IM) injections: sample 30 minutes to one hour after injection
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Ideally, a drug level would be monitored frequently and consistently, providing the clinician
a detailed pharmacokinetic profile over time. In reality, serum samples are often measured only during
relatively infrequent clinic visits, meaning that many days or weeks may pass before a drug
taken. This then requires us to ask: 'when should we collect blood in order
the serum concentration of the drug in question?'
Peak and Trough Sampling Times
A trough refers to the valley or bottom 'spike' of the sawtooth pattern we saw earlier. When
drug is taken orally the trough will be the low point of the serum concentration. It will be
period immediately before the next dose. Thus, when we want to draw a trough
is supposed to take their next dose. To assess peak levels (the time of maximum
concentration) the time for drawing depends on the route of administration and the absorption
For oral medications One hour after drug is taken is usually adequate (this assumes
For IV medications: sample 15-30 minutes after injection/infusion
(IM) injections: sample 30 minutes to one hour after injection
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
consistently, providing the clinician with
In reality, serum samples are often measured only during
meaning that many days or weeks may pass before a drug
taken. This then requires us to ask: 'when should we collect blood in order
sawtooth pattern we saw earlier. When a
drug is taken orally the trough will be the low point of the serum concentration. It will be the time
period immediately before the next dose. Thus, when we want to draw a trough level we draw just
To assess peak levels (the time of maximum
on the route of administration and the absorption
y adequate (this assumes a half-life of
30 minutes after injection/infusion. For Intramuscular

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
9
Why Therapeutic Drug Monitoring TDM?
Pharmacologists determine a drug's pharmacokinetic characteristics empirically during clinical
drug trials. From these studies, they are able to determine the solubility and distribution, the average
half-life, the levels of protein binding, and the
However, every patient is unique. Changes in the gut (if the drug is taken orally), genetic
variations in the liver's metabolizing
liver) all affect how a drug will be handled by an individual. Given
important to take a measurement of the drug in serum so that we can be sure the dose given is
leading to an appropriate concentration in the body.
appropriate for a given patient.
Every drug has a sub-clinical concentration (a
achieved) and a toxic concentration (a concentration at
For some drugs, the range between the minimum
concentration is large. These drugs are thus relatively safe. Other drugs
therapeutic window and need closer
therapeutic windows, like the anticonvulsant carbamazepine (Tegretol), should be
since elevated doses can cause serious conditions such as agranulocytosis.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Why Therapeutic Drug Monitoring TDM?
Pharmacologists determine a drug's pharmacokinetic characteristics empirically during clinical
drug trials. From these studies, they are able to determine the solubility and distribution, the average
life, the levels of protein binding, and the effective concentrations needed for treatment.
However, every patient is unique. Changes in the gut (if the drug is taken orally), genetic
variations in the liver's metabolizing enzymes, and the functional status of organs (like the kidneys and
affect how a drug will be handled by an individual. Given these variables, it becomes
important to take a measurement of the drug in serum so that we can be sure the dose given is
an appropriate concentration in the body. TDM helps to ensure that a dosing regimen is
clinical concentration (a concentration at which effective therapy won't be
achieved) and a toxic concentration (a concentration at which the drug will be harmful to the
For some drugs, the range between the minimum effective concentration and the toxic
large. These drugs are thus relatively safe. Other drugs
therapeutic window and need closer monitoring. This is the role of TDM. Medications with narrow
anticonvulsant carbamazepine (Tegretol), should be
serious conditions such as agranulocytosis.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Pharmacologists determine a drug's pharmacokinetic characteristics empirically during clinical
drug trials. From these studies, they are able to determine the solubility and distribution, the average
effective concentrations needed for treatment.
However, every patient is unique. Changes in the gut (if the drug is taken orally), genetic
enzymes, and the functional status of organs (like the kidneys and
these variables, it becomes
important to take a measurement of the drug in serum so that we can be sure the dose given is
at a dosing regimen is
concentration at which effective therapy won't be
which the drug will be harmful to the patient.)
effective concentration and the toxic
have a very narrow
Medications with narrow
anticonvulsant carbamazepine (Tegretol), should be closely monitored

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
10
Unexpected ConcentrationsTDM provides a quantitative measure of the circulating concentration of a drug. The physician
determines if the dosage of the drug
If a drug concentration is determined to be outside the therapeutic range, it
the reasons listed in the table below
Factor Discussion
Noncompliance
Patients may (intentionally or unintentionally) not take the drug as prescribed. TDM
can thus help monitor
Dosing errors
The dose may have been
Malabsorption
The TDM result will reveal if the drug cannot be absorbed well through the gut and
an alternative route of
Drug interactions
Many drugs interfere
interactions will be revealed
Kidney or liver disease
Any pathology that affects elimination will cause an elevation in a drug level that
will be unmasked by TDM.
Altered protein binding
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
disposition.
Variations in the genetics of drug
the body. This is the field of pharmacogenomics that will be
Conclusion: The drug should be measured at a time corresponding to the peak concentration (not the trough). One to 2 hours after an oral dose is
should correspond to peak concentration.
injection of the drug will not represent the peak value. A drug that is given via IV
immediately, and the peak concentration of the drug would be measured
injection. A measurement that is taken just before the next dose is given represents the trough value of the
drug.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Unexpected Concentrations: TDM provides a quantitative measure of the circulating concentration of a drug. The physician
determines if the dosage of the drug needs to be adjusted based on this information.
If a drug concentration is determined to be outside the therapeutic range, it
the reasons listed in the table below.
Patients may (intentionally or unintentionally) not take the drug as prescribed. TDM
can thus help monitor compliance.
The dose may have been erroneous or inappropriate given the patient's condition.
The TDM result will reveal if the drug cannot be absorbed well through the gut and
an alternative route of administration will be needed.
Many drugs interfere with the absorption or metabolism of other drugs. These
interactions will be revealed by TDM.
Any pathology that affects elimination will cause an elevation in a drug level that
will be unmasked by TDM.
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
Variations in the genetics of drug-metabolizing enzymes can also affect drug concentrations in
pharmacogenomics that will be discussed later in the course.
The drug should be measured at a time corresponding to the peak concentration (not
the trough). One to 2 hours after an oral dose is usually sufficient time for a drug to be absorbed and
peak concentration. A drug measurement that is taken 2 to 4 hours after an IV
injection of the drug will not represent the peak value. A drug that is given via IV
immediately, and the peak concentration of the drug would be measured 15 to 30 minutes after the IV
A measurement that is taken just before the next dose is given represents the trough value of the
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
TDM provides a quantitative measure of the circulating concentration of a drug. The physician
needs to be adjusted based on this information.
If a drug concentration is determined to be outside the therapeutic range, it may be for one of
Patients may (intentionally or unintentionally) not take the drug as prescribed. TDM
erroneous or inappropriate given the patient's condition.
The TDM result will reveal if the drug cannot be absorbed well through the gut and
with the absorption or metabolism of other drugs. These
Any pathology that affects elimination will cause an elevation in a drug level that
Mutations or deletions in drug metabolizing enzymes can greatly affect a drug's
metabolizing enzymes can also affect drug concentrations in
discussed later in the course.
The drug should be measured at a time corresponding to the peak concentration (not
usually sufficient time for a drug to be absorbed and
A drug measurement that is taken 2 to 4 hours after an IV
injection of the drug will not represent the peak value. A drug that is given via IV enters the circulation
15 to 30 minutes after the IV
A measurement that is taken just before the next dose is given represents the trough value of the

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
11
TDM For All Drugs? Can all drugs benefit from TDM? Not really. For TDM to be effective and useful, one or
the following should apply:
� The effective concentration and toxic concentrations must be well
� The pharmacokinetics of the drug are known to be variable.
� The drug is given chronically.
� There is the potential for drug
� The drug exhibits high protein binding.
� The toxicity will mimic the indication for the drug; toxicity may not be visible during an exam
but will only be revealed with TDM.
� The patient is pregnant, very young, or elderly.
� Compliance or history with the drug
Unless criteria like these exist, it doesn't make much sense to perform TDM testing. Penicillin,
for example is never measured in the
chronically, it has minimal toxicity, etc.
When is TDM Not Useful?
TDM is not useful in these specific situations:
� For drugs which act intracellularly, or that need to be converted to active forms (like AZT)
� For drugs in which the effects last much longer than the serum concentrations of the drugs;
examples include Antineoplastics
� Narcotic pain medications where continued use can lead to tolerance such that the levels
needed for pain relief in one person
Alternative to TDM Some drugs are more efficiently monitored by determining their effects rather than by
measuring the serum drug level. Warfarin dosing, for example, is better monitored by
prothrombin time (PT) and International Normalized Ratio (INR). We monitor
the physiologic effect since the effects of warfarin will outlast its
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Can all drugs benefit from TDM? Not really. For TDM to be effective and useful, one or
The effective concentration and toxic concentrations must be well-defined.
The pharmacokinetics of the drug are known to be variable.
The drug is given chronically.
There is the potential for drug-to-drug interactions.
The drug exhibits high protein binding.
The toxicity will mimic the indication for the drug; toxicity may not be visible during an exam
but will only be revealed with TDM.
The patient is pregnant, very young, or elderly.
Compliance or history with the drug is poor.
Unless criteria like these exist, it doesn't make much sense to perform TDM testing. Penicillin,
for example is never measured in the serum. It has a wide therapeutic window, it is not given
chronically, it has minimal toxicity, etc.
TDM is not useful in these specific situations:
For drugs which act intracellularly, or that need to be converted to active forms (like AZT)
For drugs in which the effects last much longer than the serum concentrations of the drugs;
Antineoplastics (cancer chemotherapies) and warfarin.
Narcotic pain medications where continued use can lead to tolerance such that the levels
needed for pain relief in one person would be toxic to another person.
are more efficiently monitored by determining their effects rather than by
measuring the serum drug level. Warfarin dosing, for example, is better monitored by
prothrombin time (PT) and International Normalized Ratio (INR). We monitor
the physiologic effect since the effects of warfarin will outlast its presence in the blood.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Can all drugs benefit from TDM? Not really. For TDM to be effective and useful, one or more of
defined.
The toxicity will mimic the indication for the drug; toxicity may not be visible during an exam
Unless criteria like these exist, it doesn't make much sense to perform TDM testing. Penicillin,
serum. It has a wide therapeutic window, it is not given
For drugs which act intracellularly, or that need to be converted to active forms (like AZT)
For drugs in which the effects last much longer than the serum concentrations of the drugs;
(cancer chemotherapies) and warfarin.
Narcotic pain medications where continued use can lead to tolerance such that the levels
are more efficiently monitored by determining their effects rather than by
measuring the serum drug level. Warfarin dosing, for example, is better monitored by measuring the
warfarin by looking at
presence in the blood.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
12
Examples of Drugs That are Monitored by TDMFour major classes of drugs are frequently monitored by TDM:
1. Antibiotics
2. Anticonvulsants
3. Immunosuppressants
4. Cardiac medications
There are other drugs that are monitored by TDM that are not included in any of the above
classifications, but the majority of TDM testing
four categories.
TDM for Antibiotics Infection is obviously a very serious indication, and effective antibiotic levels must be achieved
as soon as possible. However, many
concentrations of these antibiotics need to be monitored. Having serum
high are both situations which must be avoided.
Examples of antibiotics that are monitored by TDM include:
Amikacin
Gentamicin
Tobramycin
Vancomycin
Antibiotics such as ampicillin that are readily cleared and have a wide therapeutic window are
not usually monitored by TDM.
TDM for Anticonvulsants Anticonvulsants (also known as anti
therapeutic windows. When lev
are too high can depress the central nervous system and may even lead
Examples of anticonvulsants that are monitored by TDM include:
Carbamazepine (Tegretol)
Valproic acid (Depakene)
Phenytoin (Dilantin)
Phenobarbital
Primidone (Mysoline)
TDM for ImmunosuppressantsDrugs used to inhibit the immune system are part of standard treatment after transplant
surgeries. Unfortunately, these life
high concentrations. The reason drug monitoring is used for
concentrations are adequate to suppress the immune response and prevent rejection yet not
enough to cause liver failure or severe
Examples of immunosuppressants that are monitored by TDM include:
Cyclosporine
Methotrexate (this drug is also used as an anti
Tacrolimus
Sirolimus
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Examples of Drugs That are Monitored by TDM Four major classes of drugs are frequently monitored by TDM:
There are other drugs that are monitored by TDM that are not included in any of the above
classifications, but the majority of TDM testing is performed for drugs that are included in one of thes
Infection is obviously a very serious indication, and effective antibiotic levels must be achieved
as soon as possible. However, many antibiotics also have nephrotoxic or ototoxic effects; the
antibiotics need to be monitored. Having serum concentrations too low or too
high are both situations which must be avoided.
Examples of antibiotics that are monitored by TDM include:
ampicillin that are readily cleared and have a wide therapeutic window are
Anticonvulsants (also known as anti-epileptic or anti-seizure medications) typically have narrow
therapeutic windows. When levels are too low, the risk for seizure remains present. Drug levels that
are too high can depress the central nervous system and may even lead to coma.
Examples of anticonvulsants that are monitored by TDM include:
Carbamazepine (Tegretol)
epakene)
Phenytoin (Dilantin)
Primidone (Mysoline)
TDM for Immunosuppressants Drugs used to inhibit the immune system are part of standard treatment after transplant
surgeries. Unfortunately, these life-saving drugs also cause hepatotoxicity and nephrotoxicity with
high concentrations. The reason drug monitoring is used for immunosuppressants is to ensure that
concentrations are adequate to suppress the immune response and prevent rejection yet not
enough to cause liver failure or severe immunodeficiency.
Examples of immunosuppressants that are monitored by TDM include:
Methotrexate (this drug is also used as an anti-neoplastic drug)
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
There are other drugs that are monitored by TDM that are not included in any of the above
is performed for drugs that are included in one of these
Infection is obviously a very serious indication, and effective antibiotic levels must be achieved
antibiotics also have nephrotoxic or ototoxic effects; the
concentrations too low or too
ampicillin that are readily cleared and have a wide therapeutic window are
seizure medications) typically have narrow
too low, the risk for seizure remains present. Drug levels that
to coma.
Drugs used to inhibit the immune system are part of standard treatment after transplant
and nephrotoxicity with
immunosuppressants is to ensure that
concentrations are adequate to suppress the immune response and prevent rejection yet not high

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
13
TDM for Cardiac Medications
Inotropics (drugs used to increase the
need TDM. The cardiac glycoside
Overdose can cause vomiting, diarrhea, confusion, visual
difficulty with these medications is that overdose produces the same symptoms that the
to treat. For example, procainamide is used for arrythmyia, but an overdose of procainamide can
produce an arrythmia. Thus, without TDM the physician will not kno
less, since both states can lead to the same
Examples of cardiac medications that are monitored by TDM include:
Digoxin
Digitoxin
Procainamide
N-Acetylprocainamide (NAPA)
Quinidine
TDM for Theophylline Theophylline is used as a bronchodilator for the treatment of moderate to severe asthma and
chronic obstructive pulmonary disease
TDM is needed for theophylline because the kinetics of the drug are highly variable. It has a
narrow therapeutic window, and overdose
excitability.
Clearance of the drug is increased in children, smokers, persons with cystic fibrosis, and persons
with hyperthyroidism. Elimination is
Laboratory Methods Immunoassays are the most common technique used by clinical laboratories for therapeutic
drug monitoring. Antibodies that recognize specific drugs have been developed. Although most drugs
are much too small to evoke an immune
proteins to produce antibodies that recognize drug
There are several methods that utilize the principals of immunoassay for detection and
quantification of therapeutic drugs in serum.
Some of these methods are:
• Particle-enhanced turbidimetric inhibition immunoassay (PETINIA)
• Cloned enzyme donor immunoasssay (CEDIA)
• Fluorescence Polarization Immunoassay (FPIA)
• Chemiluminescent assays
PETINIA Particle-enhanced turbidimetric inhibition immunoassay (PETINIA) is a homogeneous
competitive immunoassay.
Antibody fragments and drug
turbidity of the solution. Free drug from the
decreasing the rate of particle aggregation.
The rate of aggregation is inversely proportional to the concentration of drug in the sample.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
TDM for Cardiac Medications
Inotropics (drugs used to increase the pumping ability of the heart) and antiarrhythmics may
need TDM. The cardiac glycoside inotropics digoxin and digitoxin have narrow therapeutic windows.
Overdose can cause vomiting, diarrhea, confusion, visual disturbances, and cardiac arryhthmias. A
ulty with these medications is that overdose produces the same symptoms that the
to treat. For example, procainamide is used for arrythmyia, but an overdose of procainamide can
Thus, without TDM the physician will not know whether to give more drug or
less, since both states can lead to the same presentation.
Examples of cardiac medications that are monitored by TDM include:
Acetylprocainamide (NAPA) -the metabolite of procainamide
Theophylline is used as a bronchodilator for the treatment of moderate to severe asthma and
chronic obstructive pulmonary disease (COPD).
TDM is needed for theophylline because the kinetics of the drug are highly variable. It has a
narrow therapeutic window, and overdose can result in elevated heart rate, arrhythmia, and CNS
Clearance of the drug is increased in children, smokers, persons with cystic fibrosis, and persons
with hyperthyroidism. Elimination is slowed in congestive heart failure and in the elderly.
Immunoassays are the most common technique used by clinical laboratories for therapeutic
Antibodies that recognize specific drugs have been developed. Although most drugs
much too small to evoke an immune response, scientists can conjugate drugs to immunogenic
proteins to produce antibodies that recognize drug-specific epitopes.
There are several methods that utilize the principals of immunoassay for detection and
cation of therapeutic drugs in serum.
Some of these methods are:
enhanced turbidimetric inhibition immunoassay (PETINIA)
Cloned enzyme donor immunoasssay (CEDIA)
Fluorescence Polarization Immunoassay (FPIA)
Chemiluminescent assays
enhanced turbidimetric inhibition immunoassay (PETINIA) is a homogeneous
Antibody fragments and drug-latex particles will bind to form aggregates that increase the
turbidity of the solution. Free drug from the sample competes for the antibody fragment, thereby
decreasing the rate of particle aggregation.
The rate of aggregation is inversely proportional to the concentration of drug in the sample.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
pumping ability of the heart) and antiarrhythmics may
inotropics digoxin and digitoxin have narrow therapeutic windows.
disturbances, and cardiac arryhthmias. A
ulty with these medications is that overdose produces the same symptoms that the drug is used
to treat. For example, procainamide is used for arrythmyia, but an overdose of procainamide can
w whether to give more drug or
Theophylline is used as a bronchodilator for the treatment of moderate to severe asthma and
TDM is needed for theophylline because the kinetics of the drug are highly variable. It has a
can result in elevated heart rate, arrhythmia, and CNS
Clearance of the drug is increased in children, smokers, persons with cystic fibrosis, and persons
congestive heart failure and in the elderly.
Immunoassays are the most common technique used by clinical laboratories for therapeutic
Antibodies that recognize specific drugs have been developed. Although most drugs
response, scientists can conjugate drugs to immunogenic
There are several methods that utilize the principals of immunoassay for detection and
enhanced turbidimetric inhibition immunoassay (PETINIA)
enhanced turbidimetric inhibition immunoassay (PETINIA) is a homogeneous
latex particles will bind to form aggregates that increase the
the antibody fragment, thereby
The rate of aggregation is inversely proportional to the concentration of drug in the sample.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
14
FPIA • Fluoresence polarization immunoassay (FPIA) is also a homogenous competitive
this system, fluorescein-labeled drug competes with unlabeled drug from the patient's serum
sample for binding sites on an antibody reagent.
• The patient's sample, presumably containing the therapeutic drug that is being monitored, and
the fluorescein-labeled drug are added to a chamber containing antibody for that drug.
• The labeled and unlabeled drug will compete for binding sites on the antibody. The greater the
amount of drug in the sample, the fewer the number of binding sites that are a
labeled analyte, leaving a greater number of small, free fluorescein
solution.
• When the chamber is excited with plane polarized light, fluorescein will absorb the light and emit
it at a higher wavelength as fluores
• A small, free fluorescein-labeled drug rotates randomly and faster than it would if it were bound
to antibody, interrupting the light and leading to less emission of light.
• The larger antibody-drug-
measured plane.
• A lower level of drug in the patient's sample results in greater emission of polarized light because
there are more antibody-drug
plane. A higher level of drug
This inverse relationship between the concentration of the drug and the polarization units (signal)
is illustrated in the image below.
• FPIA assays are rapidly being replaced by higher
now rarely used.
Chemiluminescence Chemiluminescent assays use antibodies that are conjugated to enzymes, such as peroxidase or
alkaline phosphatase. These enzymes, when mixed with chemiluminescent
the visible spectrum.
A direct relationship exists between the amount of drug that is present in the sample and the
light units that are produced and
chemiluminescence are more sensitive than immunoassays that
product.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Fluoresence polarization immunoassay (FPIA) is also a homogenous competitive
labeled drug competes with unlabeled drug from the patient's serum
sample for binding sites on an antibody reagent.
The patient's sample, presumably containing the therapeutic drug that is being monitored, and
labeled drug are added to a chamber containing antibody for that drug.
The labeled and unlabeled drug will compete for binding sites on the antibody. The greater the
amount of drug in the sample, the fewer the number of binding sites that are a
labeled analyte, leaving a greater number of small, free fluorescein-labeled molecules in the
When the chamber is excited with plane polarized light, fluorescein will absorb the light and emit
it at a higher wavelength as fluorescent light.
labeled drug rotates randomly and faster than it would if it were bound
to antibody, interrupting the light and leading to less emission of light.
fluorescein complexes rotate slower and emit m
A lower level of drug in the patient's sample results in greater emission of polarized light because
drug-fluorescein complexes present to produce light in the measured
plane. A higher level of drug in the patient's sample results in a lower emission of polarized light.
This inverse relationship between the concentration of the drug and the polarization units (signal)
is illustrated in the image below.
FPIA assays are rapidly being replaced by higher-throughput chemiluminescent assays. FPIA is
Chemiluminescent assays use antibodies that are conjugated to enzymes, such as peroxidase or
enzymes, when mixed with chemiluminescent substrates, produce light in
A direct relationship exists between the amount of drug that is present in the sample and the
light units that are produced and measured by the luminometer in the instrument. Assays that use
nce are more sensitive than immunoassays that rely on the generation of a colored
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Fluoresence polarization immunoassay (FPIA) is also a homogenous competitive immunoassay. In
labeled drug competes with unlabeled drug from the patient's serum
The patient's sample, presumably containing the therapeutic drug that is being monitored, and
labeled drug are added to a chamber containing antibody for that drug.
The labeled and unlabeled drug will compete for binding sites on the antibody. The greater the
amount of drug in the sample, the fewer the number of binding sites that are available for the
labeled molecules in the
When the chamber is excited with plane polarized light, fluorescein will absorb the light and emit
labeled drug rotates randomly and faster than it would if it were bound
fluorescein complexes rotate slower and emit more light in the
A lower level of drug in the patient's sample results in greater emission of polarized light because
fluorescein complexes present to produce light in the measured
in the patient's sample results in a lower emission of polarized light.
This inverse relationship between the concentration of the drug and the polarization units (signal)
throughput chemiluminescent assays. FPIA is
Chemiluminescent assays use antibodies that are conjugated to enzymes, such as peroxidase or
substrates, produce light in
A direct relationship exists between the amount of drug that is present in the sample and the
measured by the luminometer in the instrument. Assays that use
rely on the generation of a colored

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
15
Individualized Medicine It has been said that we live in a new era of "individualized medicine" or "personalized
medicine." One of the primary drivers for this
PGx is the study of how individual variations in the human genome affect
The term "pharmacogenetics" is also used for this discipline (people in the field use both terms;
however, the term 'pharmacogenomics' is more popular).
The primary reason that individuals metabolize and respond to drugs differently is the inter
individual differences in receptor proteins and
receptor proteins and enzymes can give rise to very different responses to drugs.
mutations are referred to as variants.
Polymorphism and CYP450To discuss PGx, we must first define two terms:
1. A polymorphism is a variation in a specific gene
population. It is essentially a mutation that
2. CYP450 refers to a family of enzymes found predominantly in the liver. CYP450 enzymes
work on a variety of substrates
facilitate excretion in the urine and feces.
There are many known polymorphisms which occur in the protein sequences of CYP450
enzymes.
CYP450s Many CYP450 enzymes have been characterized, and
recognize have been worked out to a
to-date, been associated with significant polymorphisms that affect drug
CYP1A2
CYP2C9
CYP2C19
CYP2D6
CYP2D6
There has been much research on CYP450 enzymes and many papers reporting polymorphisms
with clinical significance. We can't
• It is estimated that about 25% of common drugs are metabolized b
• CYP2D6 accounts for only about 1% of all CYP450 enzymes, but it is important in the metabolism
of about 100 drugs.
• There are more than 80 genetic variants that have been described in the CYP2D6 gene. The
normal, wild-type allele displays normal
have enhanced or diminished activity.
• The variants can be grouped generally according to the resulting alterations in protein function.
• The groupings correlate with four major enzyme metabolic capacities
intermediate, extensive (normal), or ultrarapid
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
It has been said that we live in a new era of "individualized medicine" or "personalized
medicine." One of the primary drivers for this idea is the emerging field of pharmacogenomics (PGx).
PGx is the study of how individual variations in the human genome affect responses to medications.
The term "pharmacogenetics" is also used for this discipline (people in the field use both terms;
'pharmacogenomics' is more popular).
The primary reason that individuals metabolize and respond to drugs differently is the inter
individual differences in receptor proteins and enzymes that metabolize the drugs. Mutations in these
oteins and enzymes can give rise to very different responses to drugs.
mutations are referred to as variants.
Polymorphism and CYP450 To discuss PGx, we must first define two terms:
A polymorphism is a variation in a specific gene (allele) that affects at least 1% of the
population. It is essentially a mutation that occurs relatively frequently in the population.
CYP450 refers to a family of enzymes found predominantly in the liver. CYP450 enzymes
work on a variety of substrates (in this case, drugs), altering their chemical structures to
facilitate excretion in the urine and feces.
There are many known polymorphisms which occur in the protein sequences of CYP450
Many CYP450 enzymes have been characterized, and the substrates (drugs) that each can
recognize have been worked out to a large extent. The major subfamilies of CYP450 enzymes that have
date, been associated with significant polymorphisms that affect drug disposition are:
There has been much research on CYP450 enzymes and many papers reporting polymorphisms
with clinical significance. We can't discuss all CYP450s but lets consider CYP2D6 as an example:
It is estimated that about 25% of common drugs are metabolized by CYP2D6.
CYP2D6 accounts for only about 1% of all CYP450 enzymes, but it is important in the metabolism
There are more than 80 genetic variants that have been described in the CYP2D6 gene. The
type allele displays normal metabolic activity whereas some of the variant forms
have enhanced or diminished activity.
The variants can be grouped generally according to the resulting alterations in protein function.
The groupings correlate with four major enzyme metabolic capacities
intermediate, extensive (normal), or ultrarapid metabolizers.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
It has been said that we live in a new era of "individualized medicine" or "personalized
idea is the emerging field of pharmacogenomics (PGx).
responses to medications.
The term "pharmacogenetics" is also used for this discipline (people in the field use both terms;
The primary reason that individuals metabolize and respond to drugs differently is the inter-
enzymes that metabolize the drugs. Mutations in these
oteins and enzymes can give rise to very different responses to drugs. In PGx, these
(allele) that affects at least 1% of the
occurs relatively frequently in the population.
CYP450 refers to a family of enzymes found predominantly in the liver. CYP450 enzymes
drugs), altering their chemical structures to
There are many known polymorphisms which occur in the protein sequences of CYP450
the substrates (drugs) that each can
The major subfamilies of CYP450 enzymes that have
disposition are:
There has been much research on CYP450 enzymes and many papers reporting polymorphisms
discuss all CYP450s but lets consider CYP2D6 as an example:
y CYP2D6.
CYP2D6 accounts for only about 1% of all CYP450 enzymes, but it is important in the metabolism
There are more than 80 genetic variants that have been described in the CYP2D6 gene. The
metabolic activity whereas some of the variant forms
The variants can be grouped generally according to the resulting alterations in protein function.
The groupings correlate with four major enzyme metabolic capacities (phenotypes): poor,

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
16
Metabolizers When discussing PGx, we classify a person according to his/her phenotype (their metabolic
capacity for a given enzyme).
• A poor metabolizer (PM) is a person who lacks a fully
expression of the enzyme and therefore
would require lower doses of a drug that is metabolized by that enzyme. A PM
standard dose is more likely to experience unwanted side effects or toxicity. A PM can also
experience diminished effects with drugs that need to be metabolized to active compounds by
the enzyme in question.
• An ultrarapid metabolizer
polymorphism (mutation) that codes for a more
enzyme. They will eliminate the drug more quickly. A UM may be resistant to standard
treatments, and it may take some time to adjus
• An intermediate metabolizer
dysfunctional copy. The IM group is
• A person with normal enzyme activity is referred to as wild type or as an
(EM). This person should respond to
population in which most dosing regimens have been worked out
Enzyme Abnormalities and Drugs
Not all PGx is concerned with CYP450 enzymes. There are other drug
show polymorphisms and can affect the way people respond to a drug. The following is a list of
enzymes for which known mutations have been associated with
Enzymes Acetylcholinesterase
Acetylcholinesterase
Alcohol dehydrogenase
Dihydropyrimidine dehydrogenase
CYP2C9
CYP2C19
CYP2D6
Glucose-6-phosphate dehydrogenase
N-acetyltransferase
Thioprine methyltransferase
UDP-glucuronosyl transferase
Clinical Utility • The ultimate goal in measuring CYP450 function or identifying polymorphisms is to predict
effective therapeutic doses and responses
• Polymorphisms are identified using molecular techniques (allele
sequencing, hybridization assays,
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
When discussing PGx, we classify a person according to his/her phenotype (their metabolic
(PM) is a person who lacks a fully-functional enzyme or has reduced
expression of the enzyme and therefore exhibits decreased metabolism of drugs. This person
would require lower doses of a drug that is metabolized by that enzyme. A PM
dard dose is more likely to experience unwanted side effects or toxicity. A PM can also
effects with drugs that need to be metabolized to active compounds by
ultrarapid metabolizer (UM) will require a higher dose than usual since he/she has a
polymorphism (mutation) that codes for a more efficient enzyme or more expression of an
enzyme. They will eliminate the drug more quickly. A UM may be resistant to standard
treatments, and it may take some time to adjust the dosage before therapy is achieved.
intermediate metabolizer (IM) has one wild-type (normal) copy of the gene and one absent or
dysfunctional copy. The IM group is very heterogeneous.
A person with normal enzyme activity is referred to as wild type or as an extensive metabolizer
(EM). This person should respond to standard dosages of a drug. Most people are EM's. This is the
population in which most dosing regimens have been worked out in clinical
Enzyme Abnormalities and Drugs
Not all PGx is concerned with CYP450 enzymes. There are other drug-metabolizing enzymes that
affect the way people respond to a drug. The following is a list of
which known mutations have been associated with clinical effects.
Substrates (Drugs)
Alcohol Succinylcholine
Alcohol Dihydropyrimidine dehydrogenase Fluorouracil
Warfarin, phenytoin, losartanDiazepam, omeprazole (Prilosec)Many antidepressants, opioids,
phosphate dehydrogenase Aspirin, quinidine Procainamide, isoniazid
Thioprine methyltransferase 6-mercaptopurine glucuronosyl transferase Acetaminophen, tolbutamide, irinotecan
The ultimate goal in measuring CYP450 function or identifying polymorphisms is to predict
effective therapeutic doses and responses in patients.
Polymorphisms are identified using molecular techniques (allele-specific PCR, restriction digests,
sequencing, hybridization assays, bead-based systems, microarrays, pyrosequencing, et al).
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
When discussing PGx, we classify a person according to his/her phenotype (their metabolic
functional enzyme or has reduced
exhibits decreased metabolism of drugs. This person
would require lower doses of a drug that is metabolized by that enzyme. A PM who receives a
dard dose is more likely to experience unwanted side effects or toxicity. A PM can also
effects with drugs that need to be metabolized to active compounds by
r dose than usual since he/she has a
efficient enzyme or more expression of an
enzyme. They will eliminate the drug more quickly. A UM may be resistant to standard
t the dosage before therapy is achieved.
type (normal) copy of the gene and one absent or
extensive metabolizer
standard dosages of a drug. Most people are EM's. This is the
trials.
metabolizing enzymes that
affect the way people respond to a drug. The following is a list of
phenytoin, losartan Diazepam, omeprazole (Prilosec) Many antidepressants, opioids, antiarrhythmics
Acetaminophen, tolbutamide, irinotecan
The ultimate goal in measuring CYP450 function or identifying polymorphisms is to predict
specific PCR, restriction digests,
based systems, microarrays, pyrosequencing, et al).

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
17
• Although most clinical labs do not offer PGx testing, reference la
tests. For example, one reference
measures about one dozen of the most common and significant mutation sites on
This allows for detection of approximately
laboratory then generates a report
metabolizing status.
• Estimates show that 6-10% of the general population have a complete deficiency of CYP2D6, with
the prevalence of mutations varying from
Warfarin Metabolism • PGx testing for warfarin metabolism has received the most attention thus far.
• Recent studies have revealed that about half of the variations seen in
anticoagulant warfarin are due to PGx
obviously serious, with inadequate doses predisposing patients to
placing them at risk for hemorrhage.
• The United States' Food and Drug Administration (FDA) recently approved updated labeling for
Coumadin (warfarin sold by Bristol
incorporate PGx information into warfarin
warfarin products are now adding similar labeling.
• The genes involved in warfarin metabolism are CYP2C9 and vitamin K epoxide reductase complex
subunit 1 (VKOR).
• Warfarin owes its anticoagulant action to its inhibition of VKOR. This enzym
critical element for the clotting
metabolism of warfarin: CYP2C9 *2, *3, *4, *5, *6, and *11.
denoted with asterisks.)
• One-third of the patients that receive warfarin metabolize it differently than expected and
experience a higher risk of bleeding.
• Genetic testing for the two most common polymorphisms (CYP2C9*2 and *3) as well as for VKOR
may be able to reduce the variability
• Labs performing PGx testing can provide general warfarin dosing recommendations based on the
patient's genotype analysis. The lab
moderate, high, or very high sens
then help physicians calculate an appropriate starting and maintenance dose given the phenotype
of a particular person.
• For example, a patient who has one CYP2C9 normal wild
polymorphism (CYP2C9*3), and also a VKOR
sensitivity to warfarin. This patient should have frequent INR monitoring and possible
dose reduction.
• It is important to recognize that knowing a g
dose prediction; other drugs and/or
activity. Therefore, monitoring the INR is still very important.
Conclusion: A person classified as an ultrarapid m
activity of the enzyme. This means that a UM would need more of the drug to achieve a 'normal' level since he/she is
rapidly metabolizing the drug.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Although most clinical labs do not offer PGx testing, reference labs are beginning to market these
tests. For example, one reference laboratory in the Midwest that offers CYP2D6 profiling
measures about one dozen of the most common and significant mutation sites on
This allows for detection of approximately 98% of the known CYP2D6 polymorphisms. The
laboratory then generates a report which will advise the physician on the patient's drug
10% of the general population have a complete deficiency of CYP2D6, with
alence of mutations varying from <1% to as much as 21% within a given population.
PGx testing for warfarin metabolism has received the most attention thus far.
Recent studies have revealed that about half of the variations seen in
anticoagulant warfarin are due to PGx factors. The consequences of incorrect warfarin dosing are
obviously serious, with inadequate doses predisposing patients to thrombosis and higher doses
placing them at risk for hemorrhage.
ed States' Food and Drug Administration (FDA) recently approved updated labeling for
Coumadin (warfarin sold by Bristol-Myers Squibb). The new labeling suggests that physicians
incorporate PGx information into warfarin-dosing regimens for patients. Manufac
warfarin products are now adding similar labeling.
The genes involved in warfarin metabolism are CYP2C9 and vitamin K epoxide reductase complex
Warfarin owes its anticoagulant action to its inhibition of VKOR. This enzym
critical element for the clotting. There are six CYP2C9 alleles that are known to cause prolonged
metabolism of warfarin: CYP2C9 *2, *3, *4, *5, *6, and *11. (Polymorphisms in CYP450 genes are
the patients that receive warfarin metabolize it differently than expected and
experience a higher risk of bleeding.
Genetic testing for the two most common polymorphisms (CYP2C9*2 and *3) as well as for VKOR
may be able to reduce the variability associated with warfarin dosing response.
Labs performing PGx testing can provide general warfarin dosing recommendations based on the
patient's genotype analysis. The lab report will indicate whether a patient has a normal, mild,
moderate, high, or very high sensitivity to warfarin. Online calculators or handy
then help physicians calculate an appropriate starting and maintenance dose given the phenotype
For example, a patient who has one CYP2C9 normal wild-type allele (CYP
polymorphism (CYP2C9*3), and also a VKOR polymorphism is predicted to have a moderate
sensitivity to warfarin. This patient should have frequent INR monitoring and possible
It is important to recognize that knowing a genotype does not necessarily guarantee accurate
dose prediction; other drugs and/or environmental or disease factors can also alter CYP2C9
activity. Therefore, monitoring the INR is still very important.
Conclusion: A person classified as an ultrarapid metabolizer (UM) has a polymorphism that enhances the catabolic
activity of the enzyme. This means that a UM would need more of the drug to achieve a 'normal' level since he/she is
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
bs are beginning to market these
laboratory in the Midwest that offers CYP2D6 profiling
measures about one dozen of the most common and significant mutation sites on this enzyme.
98% of the known CYP2D6 polymorphisms. The
which will advise the physician on the patient's drug-
10% of the general population have a complete deficiency of CYP2D6, with
<1% to as much as 21% within a given population.
PGx testing for warfarin metabolism has received the most attention thus far.
Recent studies have revealed that about half of the variations seen in patients taking the
factors. The consequences of incorrect warfarin dosing are
thrombosis and higher doses
ed States' Food and Drug Administration (FDA) recently approved updated labeling for
Squibb). The new labeling suggests that physicians
dosing regimens for patients. Manufacturers of generic
The genes involved in warfarin metabolism are CYP2C9 and vitamin K epoxide reductase complex
Warfarin owes its anticoagulant action to its inhibition of VKOR. This enzyme recycles vitamin K, a
There are six CYP2C9 alleles that are known to cause prolonged
(Polymorphisms in CYP450 genes are
the patients that receive warfarin metabolize it differently than expected and
Genetic testing for the two most common polymorphisms (CYP2C9*2 and *3) as well as for VKOR
ed with warfarin dosing response.
Labs performing PGx testing can provide general warfarin dosing recommendations based on the
report will indicate whether a patient has a normal, mild,
itivity to warfarin. Online calculators or handy paper charts can
then help physicians calculate an appropriate starting and maintenance dose given the phenotype
type allele (CYP2C9 *1), one
polymorphism is predicted to have a moderate
sensitivity to warfarin. This patient should have frequent INR monitoring and possible warfarin
enotype does not necessarily guarantee accurate
environmental or disease factors can also alter CYP2C9
etabolizer (UM) has a polymorphism that enhances the catabolic
activity of the enzyme. This means that a UM would need more of the drug to achieve a 'normal' level since he/she is

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
18
CYP450 Induction and Inhibition
• PGx is not the only factor to consider when thinking about variation in drug responses among
different people. Although
are other big players that influence drug metabolism.
• For example, many drugs ar
produce more of a particular
For example, CYP2D6 can be inhibited by the common
fluoxetine (Prozac). Substances in food can also affect CYP450 expression or may simply compete
with a drug for metabolism. An example is grapefruit. Several organic compounds found in
grapefruit have an inhibitory action on CYP3A4.
• Since many patients are on m
change, CYP450 expression levels
• Some CYP450 inducers and inhibitors are listed in the table on the following page.
CYP450
CYP1A2
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A
Note: This is not an exhaustive listing of inducers and inhibitors.
Conclusion: Since cimetidine inhibits CYP2D6
to be metabolized as readily. Most drug interactions are like this: one drug inhibits or competes with the same
as another drug. The end result is that higher
toxicity.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
CYP450 Induction and Inhibition
the only factor to consider when thinking about variation in drug responses among
polymorphisms of drug-metabolizing enzymes are a big player, there
are other big players that influence drug metabolism.
For example, many drugs are able to induce the expression of CYP450 enzymes (cause cells to
produce more of a particular enzyme). Also, CYP450s can be inhibited by a variety of substances.
For example, CYP2D6 can be inhibited by the common medications cimetidine (Tagamet) and
etine (Prozac). Substances in food can also affect CYP450 expression or may simply compete
with a drug for metabolism. An example is grapefruit. Several organic compounds found in
grapefruit have an inhibitory action on CYP3A4.
Since many patients are on multiple medications and since dietary and environmental factors can
change, CYP450 expression levels cannot be solely predicted based on their genotype.
Some CYP450 inducers and inhibitors are listed in the table on the following page.
Inhibitor Inducer
Amiodarone Cimetidine Ciprofloxacin
Tobacco
Amiodarone Fluvastatin Isoniazid Fluconazole
RifampinSecobarbital
Cimetidine Indomethacin Ketokonazole
Prednisone
Celecoxib Cimetidine Cocaine Methadone Pentazocine
ImipramineDesipramineAmitriptyline
Disulfiram Fluoxetine
Ethanol Isoniazid
Midazolam Erythromycin Methadone
PhenobarbitalDexamethasone
: This is not an exhaustive listing of inducers and inhibitors.
CYP2D6, less amphetamine will probably need to be given since it will not be able
Most drug interactions are like this: one drug inhibits or competes with the same
lt is that higher concentrations of one, or both, drugs are present, leading to potential
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
the only factor to consider when thinking about variation in drug responses among
metabolizing enzymes are a big player, there
e able to induce the expression of CYP450 enzymes (cause cells to
enzyme). Also, CYP450s can be inhibited by a variety of substances.
medications cimetidine (Tagamet) and
etine (Prozac). Substances in food can also affect CYP450 expression or may simply compete
with a drug for metabolism. An example is grapefruit. Several organic compounds found in
ultiple medications and since dietary and environmental factors can
cannot be solely predicted based on their genotype.
Some CYP450 inducers and inhibitors are listed in the table on the following page.
Tobacco
Rifampin Secobarbital
Prednisone
Imipramine Desipramine Amitriptyline
Isoniazid Phenobarbital Dexamethasone
, less amphetamine will probably need to be given since it will not be able
Most drug interactions are like this: one drug inhibits or competes with the same CYP450
concentrations of one, or both, drugs are present, leading to potential

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
19
Genotype versus Phenotype• Genotyping can give us a definitive profile of a given CYP450 enzyme's mutations. But since there
are dozens of mutations usually
CYP450 is not always realistic.
• Without complete sequencing of the entire allele, it may not be possible to entirely rule out a
mutation in a patient who shows none of
• If we consider the number of possible mutations and the possible presence of inducing/inhibiting
substances, phenotyping for drug
• Phenotyping involves measuring the metabolism of a probe
dextromethorphan or debrisoquine can
metabolized. Both these drugs are safe and extensively metabolized by CYP2D6.
as 'probe drug testing'. By measuring t
capacity of a CYP450 enzyme can be estimated.
• Such testing is complex and tedious, however, and has not become routine in clinical laboratories.
Therefore, genotyping is likely to be the
TDM and PGx • Can we use therapeutic drug monitoring (TDM) to assess PGx?
• TDM of the drug in question can also tell us a good deal about a drug's metabolism and will also
take into account all the other
etc.) However, unlike genotyping and probe
performed during therapy, not before. So, in fact, TDM is not really used to predict therapy in PGx
but serves as a confirmation of PGx findings.
• TDM and genotyping should be considered complementary and can be used in tandem to, first,
predict and then verify appropriate serum
The Bottom Line
• In recent years PGx has not expanded and become
for this are many. One reason is
metabolism (diet, co-medications, age, organ function, etc.) to rely on a
so many variables the cost of obtaining a PGx genotype on a patient becomes hard to justify. As
genetic test prices continues to fall this will present less of a barrier in the future. Another
problem has been the lack of clinical studies that
for patients. That is, if PGx testing doesn't cause better outcomes, then it is hard for
patients to justify its cost. There are some studies which suggest, for example, that PGx testing
may reduce hospital admissions (for those
studies which clearly demonstrate that PGx testing provides
• The US Medicare/Medicaid system has also been slow to reimburse for PGx testing. Thus, it has
not been adopted by mainly labs or
• There are some drugs however for which PGx testing is becoming more popular. Some of these
drugs have such a high potential for
these drugs has become standard of
assessed before use include:
Irinotecan (where UDP
6-mercaptopurine (Thiopurine methyl transferase (TPMT) activity is assessed)
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Genotype versus Phenotype Genotyping can give us a definitive profile of a given CYP450 enzyme's mutations. But since there
usually associated with each enzyme, a complete characterization of a
CYP450 is not always realistic.
Without complete sequencing of the entire allele, it may not be possible to entirely rule out a
mutation in a patient who shows none of the more common polymorphisms.
If we consider the number of possible mutations and the possible presence of inducing/inhibiting
substances, phenotyping for drug metabolism may sound more reasonable than genotyping.
Phenotyping involves measuring the metabolism of a probe drug. For example, with CYP2D6,
dextromethorphan or debrisoquine can be given to a patient to see how well the drug is
metabolized. Both these drugs are safe and extensively metabolized by CYP2D6.
as 'probe drug testing'. By measuring the parent drug and the metabolite in urine, the metabolic
capacity of a CYP450 enzyme can be estimated.
Such testing is complex and tedious, however, and has not become routine in clinical laboratories.
Therefore, genotyping is likely to be the main tool that is used for assessing the PGx of a patient.
Can we use therapeutic drug monitoring (TDM) to assess PGx?
TDM of the drug in question can also tell us a good deal about a drug's metabolism and will also
take into account all the other variables at play (co-medications, diet, impaired organ function,
etc.) However, unlike genotyping and probe-drug testing, therapeutic drug monitoring must be
performed during therapy, not before. So, in fact, TDM is not really used to predict therapy in PGx
as a confirmation of PGx findings.
TDM and genotyping should be considered complementary and can be used in tandem to, first,
predict and then verify appropriate serum drug levels.
In recent years PGx has not expanded and become as widespread as most predicted. The reasons
for this are many. One reason is that there are just too many variables at play with drug
medications, age, organ function, etc.) to rely on a simple PGx result. With
ost of obtaining a PGx genotype on a patient becomes hard to justify. As
test prices continues to fall this will present less of a barrier in the future. Another
problem has been the lack of clinical studies that show that PGx improves morbidity an
for patients. That is, if PGx testing doesn't cause better outcomes, then it is hard for
patients to justify its cost. There are some studies which suggest, for example, that PGx testing
admissions (for those on warfarin) but to-date there are few large, powerful
studies which clearly demonstrate that PGx testing provides added benefit to patients.
The US Medicare/Medicaid system has also been slow to reimburse for PGx testing. Thus, it has
mainly labs or health systems.
There are some drugs however for which PGx testing is becoming more popular. Some of these
drugs have such a high potential for severe, lethal toxicity that PGx testing or enzyme testing for
these drugs has become standard of care. Some examples of these drugs
assessed before use include:
Irinotecan (where UDP-glucuronosyl transferase 1A1 (UGT1A1) is assessed)
mercaptopurine (Thiopurine methyl transferase (TPMT) activity is assessed)
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Genotyping can give us a definitive profile of a given CYP450 enzyme's mutations. But since there
associated with each enzyme, a complete characterization of a
Without complete sequencing of the entire allele, it may not be possible to entirely rule out a
polymorphisms.
If we consider the number of possible mutations and the possible presence of inducing/inhibiting
metabolism may sound more reasonable than genotyping.
drug. For example, with CYP2D6,
be given to a patient to see how well the drug is
metabolized. Both these drugs are safe and extensively metabolized by CYP2D6. This is referred to
he parent drug and the metabolite in urine, the metabolic
Such testing is complex and tedious, however, and has not become routine in clinical laboratories.
hat is used for assessing the PGx of a patient.
TDM of the drug in question can also tell us a good deal about a drug's metabolism and will also
medications, diet, impaired organ function,
drug monitoring must be
performed during therapy, not before. So, in fact, TDM is not really used to predict therapy in PGx
TDM and genotyping should be considered complementary and can be used in tandem to, first,
as widespread as most predicted. The reasons
that there are just too many variables at play with drug
simple PGx result. With
ost of obtaining a PGx genotype on a patient becomes hard to justify. As
test prices continues to fall this will present less of a barrier in the future. Another
show that PGx improves morbidity and mortality
for patients. That is, if PGx testing doesn't cause better outcomes, then it is hard for clinicians and
patients to justify its cost. There are some studies which suggest, for example, that PGx testing
date there are few large, powerful
added benefit to patients.
The US Medicare/Medicaid system has also been slow to reimburse for PGx testing. Thus, it has
There are some drugs however for which PGx testing is becoming more popular. Some of these
severe, lethal toxicity that PGx testing or enzyme testing for
and the enzymes that
glucuronosyl transferase 1A1 (UGT1A1) is assessed)
mercaptopurine (Thiopurine methyl transferase (TPMT) activity is assessed)

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
20
5-Fluorouricil (Dihydropyrimidine dehydrogenase (DPD) activity is assessed)
• Clopidogrel (Plavix) is another drug in which PGx testing is getting more attention. For this anti
platelet drug, CYP2C19 or platelet function
able to convert clopidogrel to its active metabolite to achieve the needed anti
• Clopidogrel (Plavix) (where CYP2C19 or platelet function is assessed)
• By knowing a patient's disposition to specific drugs, the physician should be able to sta
patient on an appropriate regimen rather
Drugs whose metabolism may prove to be problematic can be avoided, and
that are metabolized by different, unaffected enzymes can be ch
• Clinical chemists, pharmacologists, and physicians need to translate knowledge of CYP450
polymorphisms into clinically
• Dosing recommendations for PM, EM, IM and UM patients are beginning to appear in the
literature for various classes of drugs, and
pharmacogenomic testing in the development process for new drugs.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
dropyrimidine dehydrogenase (DPD) activity is assessed)
Clopidogrel (Plavix) is another drug in which PGx testing is getting more attention. For this anti
platelet drug, CYP2C19 or platelet function is often directly assessed to ensure that the patient is
able to convert clopidogrel to its active metabolite to achieve the needed anti
Clopidogrel (Plavix) (where CYP2C19 or platelet function is assessed)
By knowing a patient's disposition to specific drugs, the physician should be able to sta
patient on an appropriate regimen rather than perfecting treatment based on trial and error.
Drugs whose metabolism may prove to be problematic can be avoided, and
that are metabolized by different, unaffected enzymes can be chosen.
Clinical chemists, pharmacologists, and physicians need to translate knowledge of CYP450
polymorphisms into clinically-validated treatment algorithms.
Dosing recommendations for PM, EM, IM and UM patients are beginning to appear in the
various classes of drugs, and the FDA is encouraging the incorporation of
pharmacogenomic testing in the development process for new drugs.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
dropyrimidine dehydrogenase (DPD) activity is assessed)
Clopidogrel (Plavix) is another drug in which PGx testing is getting more attention. For this anti-
is often directly assessed to ensure that the patient is
able to convert clopidogrel to its active metabolite to achieve the needed anti-platelet effect.
By knowing a patient's disposition to specific drugs, the physician should be able to start the
than perfecting treatment based on trial and error.
Drugs whose metabolism may prove to be problematic can be avoided, and second-line therapies
Clinical chemists, pharmacologists, and physicians need to translate knowledge of CYP450
Dosing recommendations for PM, EM, IM and UM patients are beginning to appear in the
the FDA is encouraging the incorporation of

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
21
IVIVIVIV---- IIIIndividualized TDM Drugndividualized TDM Drugndividualized TDM Drugndividualized TDM Drug
Acetylsalicylic acid (Aspirin)
USUAL DOSAGE
- Adults (antiinflammatory): 45 to 60 mg/kg/day
- Children (antiinflammatory) 70 to 90 mg/kg/day
USUAL DOSING INTERVAl
- Daily dose given in four to six divided doses
TOXIC EFFECTS
- Tinnitus, headaches, vertigo, hearing loss
-Gastrointestinal, intolerance
-Bronchospasm.
-Severe chronic and acute lntoxication, central Hyperventilation, respiratory alkalosis, metabolic
acidosis ( ˃400 mg/l: ˃2.9 mmol/l),hyperglycemia (early),
TIME TO PEAK SERUM CONCENTRATION
-Salicylic acid :1 to 2 hours(formulation dependent)
TIME TO ACHIEVE STEADY STATE
- Salicylic acid: 5 to 7 days of chronic oral dosing
ELIMINATION HALF-LIFE
-Acetylsalicylic acid:15 to 30 min
-The serum half-life and volume of distribution of salisylic acid may increase with increasing dose
-Salicylic acid:-3 hours after single 250 mg dose
ROUTE OF ELIMINATION
-Acetylsalicylic acid is hydrolyzed to salicylic aci
-Salicylic acid is then metabolized to the following compounds which undergo renal elimination:
• Salicyluric acid (saturable metabollc pathway)
• Gentisic acid (first- order pathway)
• Salicyl acyl glucuronide (first
• Salicyl phenol glucuronide
PROTEIN BINDING
-50 to 90% (concentration dependent)
USUAl SAMPLING TIMES
- 1 to 3 hours after an oral dose (formulation dependent)
USUAl THERAPEUTIC RANGE
- SaLicylic acid: 150 to 300 mg/l; 1.1 t0 2.2 mmol/l (antlinflamma
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease:
• Hypoalbuminemia (decreased protein binding)
Drugs:
• Acetylsalicyilc acid can cause a conformational change in albumin's structure, resulting in
altered protein binding for other drugs
• Corticosteroids decrease steady state levels
0thers:
• Rate 0f absorptlon from stomach is pH and formulation dependent (i.e., high pH, slow
absorption)
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
ndividualized TDM Drugndividualized TDM Drugndividualized TDM Drugndividualized TDM Drug ProfilesProfilesProfilesProfiles
45 to 60 mg/kg/day
Children (antiinflammatory) 70 to 90 mg/kg/day
Daily dose given in four to six divided doses
Tinnitus, headaches, vertigo, hearing loss
Gastrointestinal, intolerance
Severe chronic and acute lntoxication, central Hyperventilation, respiratory alkalosis, metabolic
˃400 mg/l: ˃2.9 mmol/l),hyperglycemia (early), Hypoglycemia (late).
TIME TO PEAK SERUM CONCENTRATION
alicylic acid :1 to 2 hours(formulation dependent)
5 to 7 days of chronic oral dosing
30 min
life and volume of distribution of salisylic acid may increase with increasing dose
3 hours after single 250 mg dose -20 hours at higher doses
cetylsalicylic acid is hydrolyzed to salicylic acid
alicylic acid is then metabolized to the following compounds which undergo renal elimination:
Salicyluric acid (saturable metabollc pathway)
order pathway)
Salicyl acyl glucuronide (first- order pathway)
Salicyl phenol glucuronide (saturable metabolic pathway)
50 to 90% (concentration dependent)
1 to 3 hours after an oral dose (formulation dependent)
300 mg/l; 1.1 t0 2.2 mmol/l (antlinflammatory)
AFFECTING SERUM CONCENTRATIONS
Hypoalbuminemia (decreased protein binding)
Acetylsalicyilc acid can cause a conformational change in albumin's structure, resulting in
altered protein binding for other drugs
Corticosteroids decrease steady state levels of salicylates
ate 0f absorptlon from stomach is pH and formulation dependent (i.e., high pH, slow
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Severe chronic and acute lntoxication, central Hyperventilation, respiratory alkalosis, metabolic
Hypoglycemia (late).
life and volume of distribution of salisylic acid may increase with increasing dose
alicylic acid is then metabolized to the following compounds which undergo renal elimination:
Acetylsalicyilc acid can cause a conformational change in albumin's structure, resulting in
ate 0f absorptlon from stomach is pH and formulation dependent (i.e., high pH, slow

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
22
• Systemic acildosis can cause increased tissue uptake reducing the validity of serum level
concentrations
• Urinary alkalinization increases renal elimination in overdose
NOTES:
1. Half-life is longer in newborns
2 Salicylic acid is excreted unchanged in the urine only 2to 14 %
3. Therapeutic range is usually lower if the drug is used for analgesia
4. To assess risk 0f acute toxicity refer to the nomogram of Done
1978).
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Systemic acildosis can cause increased tissue uptake reducing the validity of serum level
Urinary alkalinization increases renal elimination in overdose
2 Salicylic acid is excreted unchanged in the urine only 2to 14 %
3. Therapeutic range is usually lower if the drug is used for analgesia
4. To assess risk 0f acute toxicity refer to the nomogram of Done (Done AK, Pediatrics (Suppl) 62: 890
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Systemic acildosis can cause increased tissue uptake reducing the validity of serum level
(Done AK, Pediatrics (Suppl) 62: 890-897,

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
23
Gentamicin (Cepiophal, Garamycin, Genticin, Gentisone):
USUAL DOSAGE (lV, IM)
- Loading Dose
Adults: 1 to 2 mg/kg
Children: 1 to 2 mg/kg
Neonates: 2 to 2.5 mg/kg
- Maintenance Dose
Adults: 3 to 6 mg/kg/day
Children: 4 to 10 mg/kg/day
Neonates: 2 to 7.5 mg/kg/day
USUAl DOSING INTERVAl
- Adults: given in two to four divided doses/day
- Children: given in three to six divided doses/day
- Neonates: given in one to two divided doses/day
TOXIC ETFECTS
- Nephrotoxicity .
- Ototoxicity
- Neuromuscular blockade
TIME TO ACHIEVE STEADY STATE
- Adults: ˂30 years: 2.5 to 15 hours
- Children: 2.5 to 12.5 hours of chronic dosing
- Neonates: 10 to 45 hours of chronic dosing
ELIMINATION HALF-LIFE
- Adults: ˂ 30 years 0.5 to 3 hours
- Children: 0.5 to 2.5 hours
- Neonates: 2 to 9 hours
ROUTE OF ELIMINATION
- Renal excretion 90 % unchang
- No known metabolites
PROTEIN BINDING
- ≤ 10 %
USUAl SAMPLING TIMES
- Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
- Trough: immediately before next dose
USUAl THERAPEUTIC RANGE
- Peak: 5 to 10 mg/l
- Trough: ˂2 mg/l
SELECTED FACTORSAFFECTING SERUM CONCENTRATIONS
Drugs:
• Other nephrotoxic drugs which might decrease renal function
• High concentrations of certain penicillins (e.g.,
either in vitro or in vivo especially in patients
0thers:
• Renal impairement: ↓clearance
• Dehydration: ↓volume of distribuRon
• Obesity : alters distribution
• Burn patients: ↑dosage requirement
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Cepiophal, Garamycin, Genticin, Gentisone):
2 to 2.5 mg/kg
3 to 6 mg/kg/day
4 to 10 mg/kg/day
2 to 7.5 mg/kg/day
given in two to four divided doses/day
in three to six divided doses/day
given in one to two divided doses/day
2.5 to 15 hours of chronic dosing / ˃30years: 7.5 to 75 hours of chronic dosing
2.5 to 12.5 hours of chronic dosing
10 to 45 hours of chronic dosing
30 years 0.5 to 3 hours/ ˃30years 1.5 to 15 hours
Renal excretion 90 % unchanged
Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
Trough: immediately before next dose
SELECTED FACTORSAFFECTING SERUM CONCENTRATIONS
ther nephrotoxic drugs which might decrease renal function will cause decreased clearance.
High concentrations of certain penicillins (e.g., carbenicillin) may inactivate
either in vitro or in vivo especially in patients its severely compromised renal function.
↓clearance
↓volume of distribuRon
alters distribution
↑dosage requirement
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
to 75 hours of chronic dosing
Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
cause decreased clearance.
inactivate aminoglycosides
compromised renal function.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
24
• Hypermeatbolic surgical patients:
• Cystic fibrosis : ↑ dosage requirement
Notes:
1. These are starting dosages which may exceed manufacturers
opinions of usual dosages required
infections and normal renal function.
2. In neonates the dosages should be adjusted based on patient
function.
3. Higher dosages may be necessary in select patients.
4. Dosing intervals should be adjusted based on patient response, serum concentrations, and renal function
5. Once daily dosages have been recommended. At a dosage o
concentration 0f 0.2 mg/l was found (Prins et al. 1993, Lancet 341 , 335
and monitoring may vary.
6. Assuming normal renal function.
7. Peak delayed in patients who have co
8. Usual therapeutic range will be dependent on infection organism,
the patient, and Severity of infection. Increases in trough concentrations consistent
accumulation have been associated with toxicity.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
bolic surgical patients: ↑clearance
↑ dosage requirement
These are starting dosages which may exceed manufacturers recommendations and reflect the authors
dosages required to achieve therapeutic serum concentrations
infections and normal renal function. These dosages require monitoring of serum concentrations.
In neonates the dosages should be adjusted based on patient response, serum concentrations, and renal
Higher dosages may be necessary in select patients.
Dosing intervals should be adjusted based on patient response, serum concentrations, and renal function
nce daily dosages have been recommended. At a dosage of 4 mg/kg/day once a day (q.d.) an average peak
0.2 mg/l was found (Prins et al. 1993, Lancet 341 , 335-39). Guidelines for dosage regimens
Assuming normal renal function.
Peak delayed in patients who have compromised renal function
Usual therapeutic range will be dependent on infection organism, site of infection, immunological status of
everity of infection. Increases in trough concentrations consistent
associated with toxicity.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
recommendations and reflect the authors
in patients with serious
These dosages require monitoring of serum concentrations.
concentrations, and renal
Dosing intervals should be adjusted based on patient response, serum concentrations, and renal function
4 mg/kg/day once a day (q.d.) an average peak
Guidelines for dosage regimens
site of infection, immunological status of
everity of infection. Increases in trough concentrations consistent with tissue

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
25
NETILMICIN (Netillin, Netromycin
USUAL DOSAGE (lV, IM)
- Loading Dose
Adults: 1 to 2 mg/kg
Children: 1 to 2 mg/kg
Neonates: 2 to 2.5 mg/kg
- Maintenance Dose
Adults: 4 to 86 mg/kg/day
Children: 4 to 2 mg/kg/day
Neonates: 2 to 7.5 mg/kg/day
USUAl DOSING INTERVAl
- Adults: given in two to four divided doses/day
- Children: given in three to six divided doses/day
- Neonates: given in one to two divided doses/day
TOXIC ETFECTS
- Nephrotoxicity .
- Ototoxicity
- Neuromuscular blockade
TIME TO ACHIEVE STEADY STATE
- Adults: ˂30 years-2.5 to 15 hours
- Children: 2.5 to 12.5 hours of chronic dosing
- Neonates: 10 to 45 hours of chronic dosing
ELIMINATION HALF-LIFE
- Adults: ˂ 30 years-0.5 to 3 hours
- Children: 0.5 to 2.5 hours
- Neonates: 2 to 9 hours
ROUTE OF ELIMINATION
- Renal excretion 90 % unchanged
- No known metabolites
PROTEIN BINDING
- ≤ 10 %
USUAl SAMPLING TIMES
• Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
• Trough: immediately before next dose
USUAl THERAPEUTIC RANGE
• Peak: 5 to 12 mg/l {11 to 25 umol/l}
• Trough: ˂3 mg/l { 6umol/l}
SELECTED FACTORSAFFECTING SERUM CONCENTRAT
Drugs:
• Other nephrotoxic drugs which might decrease renal function wlll cause decreased clearance.
• High concentrations of certain penicillins (e.g., carbenicillin)
either in vitro or in vivo especially in patients with
0thers:
• Renal impairement: ↓clearance
• Dehydration: ↓volume of distribuRon
• Obesity: alters distribution
• Burn patients: ↑dosage requirement
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
etromycin)
2 to 2.5 mg/kg
4 to 86 mg/kg/day
2 mg/kg/day
2 to 7.5 mg/kg/day
given in two to four divided doses/day
given in three to six divided doses/day
given in one to two divided doses/day
2.5 to 15 hours of chronic dosing / ˃30years- 7.5 to 75 hours of chronic dosing
2.5 to 12.5 hours of chronic dosing
10 to 45 hours of chronic dosing
0.5 to 3 hours/ ˃30years-1.5 to 15 hours
unchanged
Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
Trough: immediately before next dose
Peak: 5 to 12 mg/l {11 to 25 umol/l}
˂3 mg/l { 6umol/l}
SELECTED FACTORSAFFECTING SERUM CONCENTRATIONS
ther nephrotoxic drugs which might decrease renal function wlll cause decreased clearance.
High concentrations of certain penicillins (e.g., carbenicillin) may lnactivate aminoglycosides
either in vitro or in vivo especially in patients with severly compromised renal function.
↓clearance
↓volume of distribuRon
alters distribution
↑dosage requirement
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
7.5 to 75 hours of chronic dosing
Peak: 0.5 to 1 hours after the end of 30 minutes infusion {1 hour after IM dose}
ther nephrotoxic drugs which might decrease renal function wlll cause decreased clearance.
may lnactivate aminoglycosides
severly compromised renal function.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
26
• Hypermeatbolic surgical patients
• Cystic fibrosis: ↑ dosage requirement
Notes:
1. These are starting dosages which may exceed manufacturers
opinions of usual dosages required to achieve therapeutic serum concentrations
infections and normal renal function.
2. In neonates the dosages should be adjusted based on patient
function.
3. Higher dosages may be necessary in select patients.
4. Dosing intervals should be adjusted based on patient response, serum concentrations, and renal function
5. once daily dosages have been recommended. At a dosage of
peak concentration 0f 21.3 mg/l was found (see ref
monitoring may vary.
6. Assuming normal renal function.
7. Peak delayed in patients who have compromised renal function
8. Usual therapeutic range will be dependent on infection organism,
the patient, and severity of infection. Increases in trough concentrations consistent
accumulation have been associated with toxicity.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Hypermeatbolic surgical patients: ↑clearance
↑ dosage requirement
1. These are starting dosages which may exceed manufacturers recommendations and reflect the authors
dosages required to achieve therapeutic serum concentrations
normal renal function. These dosages require monitoring of serum concentrations.
2. In neonates the dosages should be adjusted based on patient response, serum concentrations, and renal
3. Higher dosages may be necessary in select patients.
sing intervals should be adjusted based on patient response, serum concentrations, and renal function
5. once daily dosages have been recommended. At a dosage of 6.6 mg/kg/day once a day (q.d.) an average
21.3 mg/l was found (see ref. 20 page 16). Guidelines for dosage regimens and
6. Assuming normal renal function.
7. Peak delayed in patients who have compromised renal function
8. Usual therapeutic range will be dependent on infection organism, site of infection,
severity of infection. Increases in trough concentrations consistent
accumulation have been associated with toxicity.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
recommendations and reflect the authors
in patients with serious
These dosages require monitoring of serum concentrations.
response, serum concentrations, and renal
sing intervals should be adjusted based on patient response, serum concentrations, and renal function.
6.6 mg/kg/day once a day (q.d.) an average
Guidelines for dosage regimens and
immunological status of
severity of infection. Increases in trough concentrations consistent with tissue

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
27
VANCOMYCIN :(Fibrantil, Vancocin
USUAL DOSAGE (lV)
- Adults: 20 to 40 mg/kg/day
- Children: 40 to 60 mg/kg/day
- Neonates: 30 mg/kg/day
USUAl DOSING INTERVAl
- Adults: given in two to four divided doses/day
- Children: given in two to four divided doses/day
- Neonates: given in two divided doses/day
TOXIC ETFECTS
- Hypersensitivity: skin rashes and anaphylaxis
- Ototoxicity
- Phlebitis and pain at site of injection
- Nephrotoxicity(rare)
TIME TO ACHIEVE STEADY STATE
- ~20 to 30 hours of chronic dosing
ELIMINATION HALF-LIFE
- Adults: 4 to 10 hours
- Children: 2 to 3 hours
- Neonates: 6 to 10 hours
ROUTE OF ELIMINATION
- renal ˃90 % unchanged in urine
PROTEIN BINDING
- 30 to 55 %
USUAl SAMPLING TIMES
- Peak: 1 hour after the end of intravenous infusion
- Trough: immediately prior to next dose
USUAl THERAPEUTIC RANGE
- Peak: 20 to 40 mg/l {14 to 28 umol/l}
- Trough: 5 to 10 mg/l { 3 to 7umol/l}
SELECTED FACTORSAFFECTING SERUM CONCENTRATIONS
- Renal disease may increase serum concentration
Notes:
- Peak delayed in patients who have compromised renal fu
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
ancocin)
40 to 60 mg/kg/day
given in two to four divided doses/day
given in two to four divided doses/day
given in two divided doses/day
ypersensitivity: skin rashes and anaphylaxis/ "Red-neck” syndrome/ Chills and fever
Phlebitis and pain at site of injection
~20 to 30 hours of chronic dosing
˃90 % unchanged in urine
Peak: 1 hour after the end of intravenous infusion
Trough: immediately prior to next dose
Peak: 20 to 40 mg/l {14 to 28 umol/l}
Trough: 5 to 10 mg/l { 3 to 7umol/l}
SELECTED FACTORSAFFECTING SERUM CONCENTRATIONS
Renal disease may increase serum concentration
Peak delayed in patients who have compromised renal function
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Chills and fever

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
28
CARBAMAZEPINE (Tegretol):
USUAL DOSAGE (lV)
- Adults: 5 to 25 mg/kg/day orally
trigeminal neuralgia}
- Children: 5to 30 mg/kg/day orally
USUAl DOSING INTERVAl
- given in two to four divided doses depending on patient tolerance
TOXIC ETFECTS
- Diplopia,blurred vision,nystagmus
- Headache,dizziness,ataxia,sedation
- Nausea,vomiting
- Hyponatremia,water intoxication
- Exacerbation of seizure frequency
- Disturbances of heart rhythm and conduction
- Hypersensitivity reaction
Time to peak serum concentration
- Quite variable .usually 4 to 8 after dosing with conventional formulations.usually more than 12
hours after a single dose with sustained release formulatins,in overdosing afte
TIME TO ACHIEVE STEADY STATE
- After 2 to 6 days of chronic oral dosing
ELIMINATION HALF-LIFE
- 6 to 25 hours {chronic dosing}
ROUTE OF ELIMINATION
- ~99% by hepatic metabolism
- ~1%execreted unchanged in urine
- The active 10,11-epoxide metabolite may
PROTEIN BINDING
- 65 to 80 %
USUAl SAMPLING TIMES
- Chronic oral dosing :trough immediately before next dose
USUAl THERAPEUTIC RANGE
- 4 to 11 mg/l{17 to 47 umol/l}
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
- Hepatic: ↓ clearance
Other
- Children: ↑ clearance / -
- Pregnancy: ↑ clearance
Drug interactions:
- Cimetidine, danazol, diltiazem,
- Fluoxeline, fluvoxamine ,
- Isoniazid,macrolide antibiotics,
- propoxyphene, verapamril,
- viloxazine
- Activated charcoaL (used in
- Barbiturates, felbamate,phenytoin
- Valproic acid, Valpromide:
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
5 to 25 mg/kg/day orally {anticonvulsant}/ 3 to 20 mg/kg/day orally
5to 30 mg/kg/day orally {anticonvulsant}
given in two to four divided doses depending on patient tolerance
Diplopia,blurred vision,nystagmus
Headache,dizziness,ataxia,sedation
Hyponatremia,water intoxication
Exacerbation of seizure frequency
rhythm and conduction
Quite variable .usually 4 to 8 after dosing with conventional formulations.usually more than 12
hours after a single dose with sustained release formulatins,in overdosing afte
After 2 to 6 days of chronic oral dosing
hours {chronic dosing}
~99% by hepatic metabolism
~1%execreted unchanged in urine
epoxide metabolite may contribute to therapeutic and toxic effects
Chronic oral dosing :trough immediately before next dose
4 to 11 mg/l{17 to 47 umol/l}
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Old age: ↓clearance
Cimetidine, danazol, diltiazem,
Isoniazid,macrolide antibiotics, ↓clearance
propoxyphene, verapamril,
Activated charcoaL (used inncases of toxicity or overdose): ↑ clearance by
Barbiturates, felbamate,phenytoin : ↑ clearance
: ↑ level of 10,11-epoxide metabolite
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
3 to 20 mg/kg/day orally {treatment of
Quite variable .usually 4 to 8 after dosing with conventional formulations.usually more than 12
hours after a single dose with sustained release formulatins,in overdosing after 24 hours
contribute to therapeutic and toxic effects
by ↓absorpRon

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
29
Notes:
1. Patients receiving concurrent treatment with barbiturates or
compared to patients on monotherapy. Treatment should be initiated with a low
one -fourth of the maintenance
doses are achieved in approximately 3 to 4 weeks.
epilepticus.
2. Sustained release formulations may a low prolongation of
3. Skin rashes are common (about 10 %). rare hypersensitivity or
lymphadenopathy, blood dyscrasias, hepatotoxicity, pneumonitis. Taken during
may increase the rate of congenital
4. At initiation of treatment. Serum drug levels may decrease
necessitating follow-up levels to verify stabilization of serum concentration.
5. Half lives are much longer (15 t0 50 hours) after a single d
children than in adults.
6. Serum drug levels may fluctuate markedly. An additional sample at time of peak may provide useful
information in some patients.
7. Lower concentrations are usually adequate for
8. Carbamazepine is an enzyme inducer and may stimulate the
such as valproic acid, cyclosporin, glucocorticoids, oral anticoagulants and
likelihood that enzyme induction
necessitate eventual dosage reduction 0f these concurrent drugs.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Patients receiving concurrent treatment with barbiturates or phenytoin generally require larger dosages
n monotherapy. Treatment should be initiated with a low dose, usually one
fourth of the maintenance dose,and lncreased gradually by about 25 % on a weekly basis
doses are achieved in approximately 3 to 4 weeks. Abrupt discontinuation of treatment may result in status
2. Sustained release formulations may a low prolongation of dosing interval.
3. Skin rashes are common (about 10 %). rare hypersensitivity or idiosyncratic reactions may include fever,
blood dyscrasias, hepatotoxicity, pneumonitis. Taken during pregnancy,
may increase the rate of congenital malformations.
4. At initiation of treatment. Serum drug levels may decrease after 1 To 3 weeks due to autoinduction,
up levels to verify stabilization of serum concentration.
5. Half lives are much longer (15 t0 50 hours) after a single dose in non-induced state. Half
6. Serum drug levels may fluctuate markedly. An additional sample at time of peak may provide useful
7. Lower concentrations are usually adequate for trigeminal neuralgia or other neuropathic syndromes.
. Carbamazepine is an enzyme inducer and may stimulate the metabolism of concurrently administered drugs
acid, cyclosporin, glucocorticoids, oral anticoagulants and steroid oral contra
likelihood that enzyme induction will gradually decrease following carbamazepine discontinuation
necessitate eventual dosage reduction 0f these concurrent drugs.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
phenytoin generally require larger dosages
dose, usually one-third to
lncreased gradually by about 25 % on a weekly basis so that full
Abrupt discontinuation of treatment may result in status
idiosyncratic reactions may include fever,
pregnancy, carbamazepine
after 1 To 3 weeks due to autoinduction,
induced state. Half-lives are shorter in
6. Serum drug levels may fluctuate markedly. An additional sample at time of peak may provide useful
trigeminal neuralgia or other neuropathic syndromes.
metabolism of concurrently administered drugs
steroid oral contraceptives. The
will gradually decrease following carbamazepine discontinuation may

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
30
PHENOBARBITAL (Phenobarbitone
USUAL DOSAGE
- Adults: 1 to 4 mg/kg/day orally
- Children: 2 to 5 mg/kg/day orally
USUAl DOSING INTERVAl
- May be given as once daily dose at bedtime
TOXIC ETFECTS
- Sedation,tiredness,fatigue,confusion
- Cognitive impairment,depression
- Irritability,hyperactivity(in children)
- Vitamin D deficiency
- Ataxia,dysarthria
- Exacerbation of seizure frequency
- Decreased libido,impotence
- Dupuytren,s contraction,shoulder stiffness
- Hypersensitivity reactions
Time to peak serum concentration
- Variable usually 1 to 3 hours after
TIME TO ACHIEVE STEADY STATE
- Adults and adolescents: 10 to 25 days of chronic oral dosing
- Infants and children: 8 to 20 days of chronic oral dosing
ELIMINATION HALF-LIFE
- Adults: ~100 hours(range 50 to 150)
- Infants and children: ~ 65 hours(range
- Newborns: 60 to 200 hours
ROUTE OF ELIMINATION
- ~70% by hepatic metabolism
- 20 to 40%execreted unchanged in urine
- No active metabolites
PROTEIN BINDING
- ~50%
USUAl SAMPLING TIMES
- Due to the long half life, fluctuations in serum drug concentration
negligible. However, when making comparative measurements, it is advisable that
time be consistent.
USUAl THERAPEUTIC RANGE
- 10 to 40 mg/l {43 to 172 umol/l}
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
- Hepatic impairment will decrease metabolism
- Moderate to severe renal impairment will decrease clearance of unchanged drug
Other
- Neonates: ↓ clearance
- Children: ↑ clearance
- Pregnancy: ↑ clearance
- Urine alkalinization: ↑clearance
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
henobarbitone):
1 to 4 mg/kg/day orally
to 5 mg/kg/day orally
May be given as once daily dose at bedtime
Sedation,tiredness,fatigue,confusion
Cognitive impairment,depression
y(in children)
Exacerbation of seizure frequency
Decreased libido,impotence
Dupuytren,s contraction,shoulder stiffness
Variable usually 1 to 3 hours after dosing
10 to 25 days of chronic oral dosing
8 to 20 days of chronic oral dosing
~100 hours(range 50 to 150)
~ 65 hours(range 40 to 130)
~70% by hepatic metabolism
20 to 40%execreted unchanged in urine
Due to the long half life, fluctuations in serum drug concentration at steady state are usually
when making comparative measurements, it is advisable that
{43 to 172 umol/l}
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Hepatic impairment will decrease metabolism
Moderate to severe renal impairment will decrease clearance of unchanged drug
↑clearance
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
at steady state are usually
when making comparative measurements, it is advisable that the sampling
Moderate to severe renal impairment will decrease clearance of unchanged drug

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
31
Drug interactions:
- chloramphenicol,dextropro
- dicoumarol,furosemide,methsuximide,
- methylphenidate,phenytoin,
- sulthiame,valproic acid
- Activated charcoal: ↑ clearance by
Notes:
1. Phenobarbital may also be used intravenously for the treatment
scheme involves a loading dose at a rate not exceeding 100 mg/min until seizures stop
mg/kg is administered. lf seizures continue, infusion can be continued at a rate of 50 mg/min until a total
dose of 20 mg/kg is reached. Sedation and respiratory
and adequate support facilities should be readily available.
2. Hypersensitivity reactions are relatively rare and may include
pregnancy, Phenobarbital may increase the rate 0f congenital malformations.
3. Longer half-lives are observed in premature newborns.
4. Some patients may be controlled at lower concentrations.
phenobarbital, chronically treated patients may tolerate, without major adverse effects, serum drug
concentrations which would be very toxic upon acute exposure. To minimi
treatment should be started at a low dosage whenever
discontinuation of treatment may result in status epilepticus.
5. Phenobarbital is present in serum of patients treated with primidone, methylphenobarbital (mephobarbital)
and eterobarbital.
6. Phenobarbital is an enzyme inducer and may stimulate the
such as valproic acid, carbamazepine, cyc
contraceptives. The likelihood that enzyme induction will gradually decrease following Phenobarbital
discontinuation may necessitate eventual dosage reduc
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
- poxyphene ,
dicoumarol,furosemide,methsuximide, ↓clearnce
methylphenidate,phenytoin,
↑ clearance by ↓absorpRon
Phenobarbital may also be used intravenously for the treatment of status epilepticus. A possible dosing
dose at a rate not exceeding 100 mg/min until seizures stop
mg/kg is administered. lf seizures continue, infusion can be continued at a rate of 50 mg/min until a total
dose of 20 mg/kg is reached. Sedation and respiratory depression occur frequently with intravenous doses
facilities should be readily available.
2. Hypersensitivity reactions are relatively rare and may include rashes, fever and eosinophilia. Taken during
may increase the rate 0f congenital malformations.
rved in premature newborns.
4. Some patients may be controlled at lower concentrations. Since tolerance develops to the sedative effects 0f
phenobarbital, chronically treated patients may tolerate, without major adverse effects, serum drug
hich would be very toxic upon acute exposure. To minimize
treatment should be started at a low dosage whenever possible and titrated upwards. Abrupt
may result in status epilepticus.
present in serum of patients treated with primidone, methylphenobarbital (mephobarbital)
6. Phenobarbital is an enzyme inducer and may stimulate the metabolism of concurrently administered drugs
such as valproic acid, carbamazepine, cyclosporine, glucocorticoids, oral anticoagulants, and steroid oral
contraceptives. The likelihood that enzyme induction will gradually decrease following Phenobarbital
cessitate eventual dosage reduction of these concurrent drugs.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
of status epilepticus. A possible dosing
dose at a rate not exceeding 100 mg/min until seizures stop or a total dose of 10
mg/kg is administered. lf seizures continue, infusion can be continued at a rate of 50 mg/min until a total
depression occur frequently with intravenous doses
rashes, fever and eosinophilia. Taken during
Since tolerance develops to the sedative effects 0f
phenobarbital, chronically treated patients may tolerate, without major adverse effects, serum drug
ze initial adverse effects,
possible and titrated upwards. Abrupt
present in serum of patients treated with primidone, methylphenobarbital (mephobarbital)
metabolism of concurrently administered drugs
losporine, glucocorticoids, oral anticoagulants, and steroid oral
contraceptives. The likelihood that enzyme induction will gradually decrease following Phenobarbital
tion of these concurrent drugs.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
32
PHENYTOIN (Dilantin, Epanutin
USUAL DOSAGE
- Adults: 3 to 6 mg/kg/day orally
- Children: 5 to 9 mg/kg/day orally
USUAl DOSING INTERVAl
- Adults: 1 or 2 daily doses formulation
- Children: 2 to 3 divided oral doses
TOXIC EFFECTS
- Nystagmus. dysarthria. diplopia, ataxia
- Cognitive dysfunction , behavioural problems
- Exacerbation of seiuzure frequency
- Encephalopathy
- Folate and vitamin D deficiency
- Coarse features, hirsutism, acne, gum hypertrophy . Hypersensitivity reactions
Time to peak serum concentration
- Usually 2 to 6 hours after oral dosing
- With sustained release formulations,peak may occur 3 to 9 hours(or even later) after dosi
TIME TO ACHIEVE STEADY STATE
- Phenytoin exhibits dose-dependent kinetics and the time to reach steady state increases with
increasing serum concentrations,
oral dosing
ELIMINATION CHARACTERISTICS
- The term half life is not a useful parameter with druqs that
pharmacokinetics. More useful terms
concentration at which rate of metabolism is half of its maximal rate (K
- Vmax 100 to 1000 mg/day
- Km 1 ro 15 mg/l (4 ro 59 umol/l)
ROUTE OF ELIMINATION
- More than 95% by hepatic metabolism
- Less than 5%execreted unchanged in urine
- No active metabolites
PROTEIN BINDING
- ~92%
USUAl SAMPLING TIMES
- Due to slow oral absorption and
state are usually relatively small;
advisable that sampling time be consistent (ideally: trough level)
USUAl THERAPEUTIC RANGE
- Adults, children, infants˃ 3months:
- Preterm,term neonates and
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
- Mononucleosis: ↑clearance
- Chronic liver disease: ↓ clearance
- Renal disease: see note 4
Other
- Neonates: ↓Clearance
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
panutin)
3 to 6 mg/kg/day orally
to 9 mg/kg/day orally
1 or 2 daily doses formulation
2 to 3 divided oral doses dependent
Nystagmus. dysarthria. diplopia, ataxia
Cognitive dysfunction , behavioural problems probably serum level related
Exacerbation of seiuzure frequency
n D deficiency
Coarse features, hirsutism, acne, gum hypertrophy . Hypersensitivity reactions
Usually 2 to 6 hours after oral dosing
With sustained release formulations,peak may occur 3 to 9 hours(or even later) after dosi
dependent kinetics and the time to reach steady state increases with
increasing serum concentrations, usually steady state is achieved after 4 to 24 days of chronic
The term half life is not a useful parameter with druqs that exhibit dose dependent
pharmacokinetics. More useful terms would be maximal rate of metabolism (V
at which rate of metabolism is half of its maximal rate (Km):
1 ro 15 mg/l (4 ro 59 umol/l)
More than 95% by hepatic metabolism
Less than 5%execreted unchanged in urine
Due to slow oral absorption and elimination ,fluctuation in serum drug concentration at steady
ually relatively small; however ,hen making comparative measurements,it is
advisable that sampling time be consistent (ideally: trough level)
3months: 10 to 20 mg/l (40 to 80 umol/l)
m,term neonates and Infants 2 weeks to 3months: 6 to 14 mg/l ( 24 to 55 umol/l)
AFFECTING SERUM CONCENTRATIONS
↑clearance
↓ clearance
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
level related
Coarse features, hirsutism, acne, gum hypertrophy . Hypersensitivity reactions
With sustained release formulations,peak may occur 3 to 9 hours(or even later) after dosing
dependent kinetics and the time to reach steady state increases with
usually steady state is achieved after 4 to 24 days of chronic
exhibit dose dependent
would be maximal rate of metabolism (Vmax) and
elimination ,fluctuation in serum drug concentration at steady
however ,hen making comparative measurements,it is
( 24 to 55 umol/l)

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
33
- Children: ↑ clearance
- Pregnancy: ↑ clearance
- Urine alkalinization: ↑clearance
Drug interactions:
- Some antacids,antineoplastics,nasogastric feeding formulas,activated charcoal,and
may reduce phenytoin absorption
- Some drugs may displace phenytoin from protein binding sites in serum,usually this results in a
decrease in total serum phenytoin concentration without change in free
concentration.relationship between total serum
- Phenylbutazone ,valproic acid,and sulfonamides may increase free phenytoin
concentration{these drugs displace phenytoin from serum binding sites and may inhibit
phenytoin metabolism}
- Vigabatrin,folic acid ,and rifampicin may decrease serum phenytoin levels
- Amiodarone,chloramphenicol,cimitidine,dextropropoxyphene,felbamate,isoniazid,methsuximid
e,methylphenidate,some phenothiazines,sulthiame,and several other drugs may increase serum
phenytoin concentration
- PhenobarbitaI may cause a transient increase d
decrease due to enzyme induction
Notes:
1. Phenytoin js usually started at a low dosage and increased
response is required loading doses may be given.
linear relationship between sodium salt and free acid(10% dosage difference),may cause
disproportionately large increase in serum drug concentration.
in status epilepticus. phennytoin may also be used intravenously for the treatment of status epilipticus.a
possible dosing scheme involves a loading dose of 18 mg/kg at a rate not exceeding 50mg/min.hypotention
and a systole may occur and adequate support facilities should be readily available.diazepam or lorazepam
are usually combined with phenytoin in the treatment of status epilepticus.intravenous maintainance doses
of phenytoin should be given in two to three divided daily dos
2. Hypersensitivity reactions are relatively rare and may include
Lymphadenopathy systemic lupus erythematosus,
pregnancy, phenytoin may increase the rate of congenita
3. For practical purposes, however,
cases,the longest values being recorded at high serum
range from 10 to 30 hours at concentration between 10 and 20 mg/l{shorter or higher values are recorded
at concentrations below or above this range respectively}
4.binding to serum proteins may decrease in conditions associated withy hypoalbuminemia
{malnutrition,nephritic syndrome
displacing agents {hyperbilirubinemia,uremia}.
salicylates, sulfonylureas and most notably,valproic acid may also displace phenytoin
and increase its free fraction.since only the unbound (free)drug is pharmacologically active,in the presence
of decreased binding the total serum phenytoin concentration may underestimate the amount of drug
which is active ,and therapeu
situations,it may be useful to measure the free concentration.a therapeutic range of 1 to 2 mg/l(4 to 8
umol/l)is suggested for free phenytoin
5. some patients may be controlled at low
6.Phenytoin is an enzyme inducer and may stimulate the metabolism of concurrently administered drugs such
as valproic acid,carbamazepines,
contraceptives
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
↑clearance
antacids,antineoplastics,nasogastric feeding formulas,activated charcoal,and
may reduce phenytoin absorption
Some drugs may displace phenytoin from protein binding sites in serum,usually this results in a
decrease in total serum phenytoin concentration without change in free
concentration.relationship between total serum concentration and response will be altered.
Phenylbutazone ,valproic acid,and sulfonamides may increase free phenytoin
concentration{these drugs displace phenytoin from serum binding sites and may inhibit
rifampicin may decrease serum phenytoin levels
Amiodarone,chloramphenicol,cimitidine,dextropropoxyphene,felbamate,isoniazid,methsuximid
e,methylphenidate,some phenothiazines,sulthiame,and several other drugs may increase serum
arbitaI may cause a transient increase due to competitive jnhibition of metabolism or a
decrease due to enzyme induction
1. Phenytoin js usually started at a low dosage and increased graduall y according to clinical response. if rapid
required loading doses may be given. dosage adjustment should be cautions due to the non
linear relationship between sodium salt and free acid(10% dosage difference),may cause
disproportionately large increase in serum drug concentration. abrupt withdrawal of treatment may result
phennytoin may also be used intravenously for the treatment of status epilipticus.a
possible dosing scheme involves a loading dose of 18 mg/kg at a rate not exceeding 50mg/min.hypotention
occur and adequate support facilities should be readily available.diazepam or lorazepam
are usually combined with phenytoin in the treatment of status epilepticus.intravenous maintainance doses
of phenytoin should be given in two to three divided daily doses
2. Hypersensitivity reactions are relatively rare and may include; Skin rashes, fever and eosinophilia.
systemic lupus erythematosus, hepatotoxicity, blood dyscrasias.
phenytoin may increase the rate of congenital malformations.
however, it can be estimated that half lives range from 20 to 100 hours in most
cases,the longest values being recorded at high serum concentrations. In infants and children,half
at concentration between 10 and 20 mg/l{shorter or higher values are recorded
at concentrations below or above this range respectively}
4.binding to serum proteins may decrease in conditions associated withy hypoalbuminemia
{malnutrition,nephritic syndrome,neonates,elderly patients,pregnancy,atc}or accumulation of endogenous
displacing agents {hyperbilirubinemia,uremia}. other drugs such many sulfonamides,
sulfonylureas and most notably,valproic acid may also displace phenytoin
and increase its free fraction.since only the unbound (free)drug is pharmacologically active,in the presence
of decreased binding the total serum phenytoin concentration may underestimate the amount of drug
which is active ,and therapeutic and toxic effects will appear at lower total concentration.in these
situations,it may be useful to measure the free concentration.a therapeutic range of 1 to 2 mg/l(4 to 8
umol/l)is suggested for free phenytoin
5. some patients may be controlled at lower concentrations .see also note 4
henytoin is an enzyme inducer and may stimulate the metabolism of concurrently administered drugs such
as valproic acid,carbamazepines, cyclosporine, glucucorticoids, oral anticoagulants and steroid oral
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
antacids,antineoplastics,nasogastric feeding formulas,activated charcoal,and sucralfate
Some drugs may displace phenytoin from protein binding sites in serum,usually this results in a
decrease in total serum phenytoin concentration without change in free
concentration and response will be altered.
Phenylbutazone ,valproic acid,and sulfonamides may increase free phenytoin
concentration{these drugs displace phenytoin from serum binding sites and may inhibit
Amiodarone,chloramphenicol,cimitidine,dextropropoxyphene,felbamate,isoniazid,methsuximid
e,methylphenidate,some phenothiazines,sulthiame,and several other drugs may increase serum
ve jnhibition of metabolism or a
graduall y according to clinical response. if rapid
dosage adjustment should be cautions due to the non-
linear relationship between sodium salt and free acid(10% dosage difference),may cause
al of treatment may result
phennytoin may also be used intravenously for the treatment of status epilipticus.a
possible dosing scheme involves a loading dose of 18 mg/kg at a rate not exceeding 50mg/min.hypotention
occur and adequate support facilities should be readily available.diazepam or lorazepam
are usually combined with phenytoin in the treatment of status epilepticus.intravenous maintainance doses
Skin rashes, fever and eosinophilia.
blood dyscrasias. taken during
it can be estimated that half lives range from 20 to 100 hours in most
concentrations. In infants and children,half-lives
at concentration between 10 and 20 mg/l{shorter or higher values are recorded
4.binding to serum proteins may decrease in conditions associated withy hypoalbuminemia
,neonates,elderly patients,pregnancy,atc}or accumulation of endogenous
other drugs such many sulfonamides, phenylbutazone,
sulfonylureas and most notably,valproic acid may also displace phenytoin from serum proteins
and increase its free fraction.since only the unbound (free)drug is pharmacologically active,in the presence
of decreased binding the total serum phenytoin concentration may underestimate the amount of drug
tic and toxic effects will appear at lower total concentration.in these
situations,it may be useful to measure the free concentration.a therapeutic range of 1 to 2 mg/l(4 to 8
henytoin is an enzyme inducer and may stimulate the metabolism of concurrently administered drugs such
oral anticoagulants and steroid oral

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
34
VALPROIC ACID (Convulex,Depakene,Epilim,O
USUAL DOSAGE
- Adults: 10 to 45 mg/kg/day orally
- Children: 10 to 60 mg/kg/day orally
USUAl DOSING INTERVAl
- Given in one to four divided doses
TOXIC EFFECTS
- Gastric irritation,nausea and vomiting
- Weight gain
- Sedation,stupor,tremor
- Thrombocytopenia
- Hepatotoxicity,pancreatitis
- Teratogenicity(neural tube defects)
- Hyperammonemia
Time to peak serum concentration
- Syrup: 0.5 to1 hour after dosing
- Capsules or plain tablets: 0.5 to 2 hours after dosing
- Enteric coated tablets: 3 to 8 hours after dosing
TIME TO ACHIEVE STEADY STATE
- After 2 to 4 days of chronic oral dosing
ELIMINATION HALF-LIFE
- Adults: 6 to 17 hours
- Infants and children: 5 to 15
- Newborns( ≤ 2months): 15 to 60 hours
ROUTE OF ELIMINATION
- About 95% by hepatic metabolism
- Less than 5%execreted unchanged in urine
- Reactive metabolites may contribute to hepatotoxicity and possibly teratogenicity
PROTEIN BINDING
- ~90%
USUAl SAMPLING TIMES
- Chronic oral dosing: trough immediately before next dose
USUAl THERAPEUTIC RANGE
- 50 to 100 mg/l(347 to 693 umol/l)
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
- Hepatic disease: see note 4
- Renal disease: see note 4
- Hypoalbuminemia: see note 4
Other
- Neonates: ↓ clearance
- Children: ↑ clearance
- Pregnancy : ↑ clearance
- Old age: see note4
Drug interactions:
- Activated charcoal, some antacids
- Salicylates: see note 4 &9
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
(Convulex,Depakene,Epilim,Orfiril)
10 to 45 mg/kg/day orally
10 to 60 mg/kg/day orally
Given in one to four divided doses
astric irritation,nausea and vomiting
eratogenicity(neural tube defects)
dosing
0.5 to 2 hours after dosing
3 to 8 hours after dosing
fter 2 to 4 days of chronic oral dosing
5 to 15 hours
15 to 60 hours
bout 95% by hepatic metabolism
Less than 5%execreted unchanged in urine
Reactive metabolites may contribute to hepatotoxicity and possibly teratogenicity
trough immediately before next dose
50 to 100 mg/l(347 to 693 umol/l)
FACTORS AFFECTING SERUM CONCENTRATIONS
see note 4
some antacids and Some antineoplastics: ↓absorpRon
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Reactive metabolites may contribute to hepatotoxicity and possibly teratogenicity

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
35
- Barbiturates, Phenytoin, Carbamazepine
- Some drugs displace valproic acid f
Notes:
1. Available in several dosage forms ,e.g.valproic acid,sodium valproate,magnesium valproate.treatment is
usually initiated with arelatively low dose and increased gradually.abrupt discontinuation of treatment may
result in status epilepticus
2. Sustained release formulations may allow prolongation of dosing interval.
3. Absorption from enteric coated tablets may be m
4. Protein binding decreases at high serum concentrations Binding mav decrease in conditions associated with
hypoalbuminemia (malnutrition, nephrotic syndrome, neonates,
accumulation of endogenous displacing agents(uremia), and concurrent treatment with displacing
such as salicylates and phenylbutazone . since only the unbound (free)drug is pharmacologically active,
the presence of decreased binding the total serum valproic acid concent
amount of drug high is active,
5. Serum drug levels may fluctuate markedly
information in some patients
6. Valproic acid is the active moiety in the serum of patients treated with divalproex sodium
valpromide (depamide)
7. Some patients with seizures that are difficult to control may benefit from concentration greater than
100mg/l without adverse effects
8. Valproic acid may inhibit the metabolic elimination of Phenobarbital,
epoxide,and lamotrigine. Valproic acid displaces phenytoin from serum protein binding sites. A favourable
(synergistic) pharmacodynamic interaction between ethosuximide and valproic acid may occur in patients
with certain types of absence seizures.
9. Salicylates may inhibit the metabolism of valproic acid in addi
these two mechanisms have opposing effects on total clearance of valproic acid
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Carbamazepine: ↑clearance
splace valproic acid from serum protein binding sites: see note4
vailable in several dosage forms ,e.g.valproic acid,sodium valproate,magnesium valproate.treatment is
initiated with arelatively low dose and increased gradually.abrupt discontinuation of treatment may
ustained release formulations may allow prolongation of dosing interval.
bsorption from enteric coated tablets may be markedly delayed by food.
rotein binding decreases at high serum concentrations Binding mav decrease in conditions associated with
(malnutrition, nephrotic syndrome, neonates, elderly patients,
us displacing agents(uremia), and concurrent treatment with displacing
such as salicylates and phenylbutazone . since only the unbound (free)drug is pharmacologically active,
the presence of decreased binding the total serum valproic acid concentration may underestimate the
and therapeutic and toxic effects will appear at lower total concentration
g levels may fluctuate markedly an additional sample at time of peak may provide useful
alproic acid is the active moiety in the serum of patients treated with divalproex sodium
ome patients with seizures that are difficult to control may benefit from concentration greater than
out adverse effects.
alproic acid may inhibit the metabolic elimination of Phenobarbital, phenytoin,
alproic acid displaces phenytoin from serum protein binding sites. A favourable
pharmacodynamic interaction between ethosuximide and valproic acid may occur in patients
with certain types of absence seizures. valproic acid may increase serum ethosuximide concentrations
alicylates may inhibit the metabolism of valproic acid in addition to displacing it from protein binding sites.
these two mechanisms have opposing effects on total clearance of valproic acid
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
see note4
vailable in several dosage forms ,e.g.valproic acid,sodium valproate,magnesium valproate.treatment is
initiated with arelatively low dose and increased gradually.abrupt discontinuation of treatment may
rotein binding decreases at high serum concentrations Binding mav decrease in conditions associated with
elderly patients, Pregnancy, etc.).
us displacing agents(uremia), and concurrent treatment with displacing drugs,
such as salicylates and phenylbutazone . since only the unbound (free)drug is pharmacologically active, in
ration may underestimate the
and therapeutic and toxic effects will appear at lower total concentration
an additional sample at time of peak may provide useful
alproic acid is the active moiety in the serum of patients treated with divalproex sodium (depakote) and
ome patients with seizures that are difficult to control may benefit from concentration greater than
phenytoin, carbamazepine-10,11-
alproic acid displaces phenytoin from serum protein binding sites. A favourable
pharmacodynamic interaction between ethosuximide and valproic acid may occur in patients
valproic acid may increase serum ethosuximide concentrations
tion to displacing it from protein binding sites.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
36
METHOTREXATE (Methotrexate LPD,
USUAL DOSAGE
- The dosage for methotrexate is widely varied,
to high dose lV therapy (1
must follow a specific treatment
USUAl DOSING INTERVAl
- Consult specific treatment protocol(see above)
TOXIC EFFECTS
- Nausea and vomiting
- Myelosuppression
- Mucositis
- Renal dysfunction
- Hepatic dysfunction
- Leukoencephalopathy
- Rash
TIME TO ACHIEVE STEADY STATE
- Approximately 12 to 24 hours of chronic dosing
ELIMINATION HALF-LIFE
- 2 to 4 hours,initial half-life
- 8 to 15 hours,terminal half-
ROUTE OF ELIMINATION
- Renal excretion 70- 90 % unchanged
- Renal excretion of methotrexate and 7
- Metabolism up to ~ 30%; major extracellular metabolite
activity; poor solubility in acidic
PROTEIN BINDING
- 50 to 60%
USUAl SAMPLING TIMES
- The sampling times for methotrexate will depend on dose,
0f the patient (consult specific treatment protocol)
of leucovorin rescue doses
USUAl TOXIC RANGE
- A usual therapeutic range for methotrexate has not been defined. The minimum cytotoxic
concentration is ~ 0.01 µmol/l.
- Serum concentrations which have been assoc
high-dose (~ 5 g/m2) infusion. when only low
24 hours ˃5 µmol/l give higher dose of
48 hours ˃ 0.5 µmol/l leucovorin or extend rescue
72 hours˃0.05 µmol/l beyond planned endpoint
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
• Renal disease
• Aciduria {urine PH˂6.5} ↓clearance
• Decreased urine flow
• Ascites, pleural effusion,
• GI obstruction
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Methotrexate LPD, Mexate):
The dosage for methotrexate is widely varied, ranging from low dose oral therapy (~ 20 mg/m
(1-12 g/m2) with leucovorin rescue. Thus, the dosage of
treatment protocol.
Consult specific treatment protocol(see above)
ausea and vomiting
pproximately 12 to 24 hours of chronic dosing
-life
90 % unchanged
enal excretion of methotrexate and 7-hydroxymethotrexate .
etabolism up to ~ 30%; major extracellular metabolite 7-hydroxy methotrexate (lit
vity; poor solubility in acidic urine)
The sampling times for methotrexate will depend on dose, duration of lnfusion and clinical status
specific treatment protocol). These are generally used to
A usual therapeutic range for methotrexate has not been defined. The minimum cytotoxic
µmol/l.
Serum concentrations which have been associated with increased risk of toxicity after a six
infusion. when only low-dose leucovorin rescue is given:
5 µmol/l give higher dose of
0.5 µmol/l leucovorin or extend rescue
0.05 µmol/l beyond planned endpoint
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
enal disease
˂6.5} ↓clearance
pleural effusion, 3rd
space fluid collection
Prolong serum half
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
low dose oral therapy (~ 20 mg/m2)
) with leucovorin rescue. Thus, the dosage of Methotrexate
hydroxy methotrexate (little cytotoxic
duration of lnfusion and clinical status
used to guide adjustment
A usual therapeutic range for methotrexate has not been defined. The minimum cytotoxic
toxicity after a six-hour
dose leucovorin rescue is given:
rolong serum half-life

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
37
• Drugs:
• Nonabsorbable antibiotics
• Concurrent or previous therap w
• Probenecid,salicylates
• NSAIDS.sulfonamides
Notes:
1.”toxicity”assignment is dependent on duration of exposure,
influenced by intensity 0f cumulative exposure prior
leucovorin dosage guidelines based on methotrexate serum concentration see
MethotrexateSerum concentration more than 24 hrs from
beginning of infusion
20 to 50 µmol/l
10 to 20 µmol/l
5 to 10 µmol/l
1 to 5 µmol/l
0.5 to 1 µmol/l
0.1 to 0.5 pmol/l
0.01 to 0.1 µmol/l
2.Methotrexate (MTX) concentrations should be monitored and leucovorin
in”high_risk” patients until serum MTX concentrations are < 0.05 µmol/l. Leucovorin
reduced, as indicated, as MTX serum concentrations decrease
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Nonabsorbable antibiotics ↓absorpRon
or previous therap with neoplastic drugs
benecid,salicylates ↓clearance
NSAIDS.sulfonamides
1.”toxicity”assignment is dependent on duration of exposure, as well as serum concentration. and is probably
intensity 0f cumulative exposure prior to measured points and beyond measured points. For
based on methotrexate serum concentration see next table.
Methotrexate erum concentration more than 24 hrs from
beginning of infusion
LeucovorinApproximate dose required
20 to 50 µmol/l 500 mg/m2 lV Q 6 hours
10 to 20 µmol/l 200 mg/m2 lV Q 6 hours
5 to 10 µmol/l 100 mg/m2 lV Q 6 hours
1 to 5 µmol/l 30 mg/m2 lV or PO Q 6 hours
to 1 µmol/l 15 mg/m2 PO Q 6 hours
pmol/l 15 mg/m2 PO Q 12 hours
µmol/l 5to 10 mg/m2 PO Q 12 hours
Methotrexate (MTX) concentrations should be monitored and leucovorin administration should be continued
until serum MTX concentrations are < 0.05 µmol/l. Leucovorin
MTX serum concentrations decrease
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
↓absorpRon
ith neoplastic drugs
as well as serum concentration. and is probably
beyond measured points. For
next table.
Leucovorin
pproximate dose required
lV or PO Q 6 hours
PO Q 12 hours
administration should be continued
until serum MTX concentrations are < 0.05 µmol/l. Leucovorin dosages may be

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
38
THEOPHYLLINE (Aminophylline,T
USUAL DOSAGE
Loading dosage
• No prior theophylline administration
• Prior theophylline administration,
in an Emergency without symptoms of Intoxication
Maintenance dosage
• Adults(healthy nonsmokers)
• Adults(smokers)
• Adults(cardiac decompensation a
• Children(˃9 years;healthy)
• Children(1 to 9 years)
• Infants(4 to 52 weeks)
• Neonates
Chronic dosage
• Adults(healthy nonsmokers)
• Adults(smokers)
• Adults(cardiac decompensation a
• Adolescents(12 to 16 years)
• Children(9 to 12 years)
• Children(1 to 9 years)
• Infants(6 to 51 weeks)
• Neonates(premature or normal)
USUAl DOSING INTERVAl
- Intravenous
- Loading doses 0f theophylline should be infused over 30 min .
- Maintenance doses of theophylline should be calculated for a
adriinistered as a continous intravenous
- Oral therapy
- Dosing intervals will vary dependent upon product formulation,
elimination rate. ln case of chronic
- However, the following will provide guidelines for dosage intervals
Total daily dosage
Rapid Release
Sustained Release: Children
Adults
TOXIC EFFECTS
- Nausea , vomiting ,diarrhea,insomnia,headache
- Irritability,nervousness
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
(Aminophylline,Theo-dur,theo 24):
oading dosage Theophylline dosage
administration In previous 24 hours 5 mg/kg IV over 30 min
Prior theophylline administration, Obtain serum concentration;
Emergency without symptoms of Intoxication.
2mg/kg IV over 30 min
dosage Theophylline
Infusion Rate (mg/kg/hour)
Adults(healthy nonsmokers) 0.4
Adults(smokers) 0.6
(cardiac decompensation and/or liver dysfunction 0.2
0.7
0.8
0.008
Neonates 0.13
dosage Theophylline dosage
Adults(healthy nonsmokers) 10
Adults(smokers) 15
(cardiac decompensation and/or liver dysfunction 4
Adolescents(12 to 16 years) 18
Children(9 to 12 years) 20
Children(1 to 9 years) 24
Infants(6 to 51 weeks) 0.3
Neonates(premature or normal) 3.0
0f theophylline should be infused over 30 min .
of theophylline should be calculated for a 24 hour period and then
adriinistered as a continous intravenous infusion starting 30 to 60 min after loading dose
Dosing intervals will vary dependent upon product formulation, age of patient, and
elimination rate. ln case of chronic dosage sustained release formulations are commonly used.
, the following will provide guidelines for dosage intervals
Given in divided Doses
elease 3 to 4
Adults
2 to 3
1 to 2
ausea , vomiting ,diarrhea,insomnia,headache
rritability,nervousness
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
Theophylline dosage
5 mg/kg IV over 30 min
2mg/kg IV over 30 min
Theophylline Infusion Rate (mg/kg/hour)
0.4
0.6
0.2
0.7
0.8
0.008 (age in weeks+0.021)
0.13
Theophylline dosage
10-15
15-18
4-8
18
20
24
0.3 (age in weeks+8)
3.0
24 hour period and then
infusion starting 30 to 60 min after loading dose
age of patient, and patients
dosage sustained release formulations are commonly used.
Given in divided Doses

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
39
- Seizures,sinus tachycardia,
Time to peak serum concentration
- This is dependent upon product formulation, since sustained
prolonged time to "peak", compared to conventional products (about 3 to 8 hours longer)
TIME TO ACHIEVE STEADY STATE
- Adults: ~2 to 3 days of chronic oral dosing
- Children: ~1 to 2 days of chronic oral dosing
- Infants: ~1 to 5 days of chronic oral dosing
- Newborn: ~120 hours of chronic oral dosing
- Premature neonates: ~150 hours of chronic oral dosing
RATE OF ELIMINATION
- Adults(healthy ,nonsmokers)
- Adults(healthy,smokers)
- Adults(liver cirrhosis): 10 to 56 hours
- Children: 4 hours(range 2 to 10)
- Infants(4 to 52 weeks):
- Neonates:
• Premature: 30 hours
• Normal newborn
RATE OF ELIMINATION
- Hepatic metabolism th
metabolite in newborn
- Renal excretion of less than 10% unchanged drug (greater in newborn)
PROTEIN BINDING
- 55 to 66% (healthy adults)
- ~36%(neonates,adults with liver
USUAl SAMPLING TIMES
- Intravenous
• Prior to intravenous infusion .
• 30 min after completion of loading dose to measure adequacy of dose .
• 4 to 6 hours after beginning continous infusion therapy (presteady state but used
to establish trend) or befor
- Oral, Peak
• 2 hours after administration of a product with rapid release properties
• 4 to 8 hours after administration of a product with sustained release properties
- Oral, Trough
• Immediately
USUAl THERAPEUTIC RANGE
- Asthma (bronchodilator)8 to 20 mg/l
- Neonatal apnea 6 to 11 mg/l
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
• Disease
• Fever associated with upper
• Cor pulmonale
• Acute pulmonary edema
• Hepatic cirrhosis
• Cardiac decompensation
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
,sinus tachycardia, cardiac arrhythmias, cerebral hypoxia, cardiorespiratory collapse
This is dependent upon product formulation, since sustained release products have a very
prolonged time to "peak", compared to conventional products (about 3 to 8 hours longer)
~2 to 3 days of chronic oral dosing
~1 to 2 days of chronic oral dosing
~1 to 5 days of chronic oral dosing
~120 hours of chronic oral dosing
~150 hours of chronic oral dosing
,nonsmokers): 9hours(range 3 to 12)
Adults(healthy,smokers): 4 hours
10 to 56 hours
4 hours(range 2 to 10)
: 3 to 14 hours
30 hours
ormal newborn: 24 hours
the renal execresion of relatively inactive metabolites,
metabolite in newborn
of less than 10% unchanged drug (greater in newborn)
55 to 66% (healthy adults)
~36%(neonates,adults with liver cirrhosis)
Prior to intravenous infusion .
30 min after completion of loading dose to measure adequacy of dose .
6 hours after beginning continous infusion therapy (presteady state but used
to establish trend) or before next infusion
hours after administration of a product with rapid release properties
to 8 hours after administration of a product with sustained release properties
before next oral dose
(bronchodilator)8 to 20 mg/l: (44 to 111 µmol/l)
apnea 6 to 11 mg/l: (33 to 61 µmol/l)
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
ever associated with upper respiratory illness
pulmonale
Acute pulmonary edema ↓clearance
Cardiac decompensation
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
cardiorespiratory collapse
release products have a very
prolonged time to "peak", compared to conventional products (about 3 to 8 hours longer)
relatively inactive metabolites, caffeine is a
30 min after completion of loading dose to measure adequacy of dose .
6 hours after beginning continous infusion therapy (presteady state but used
hours after administration of a product with rapid release properties
to 8 hours after administration of a product with sustained release properties
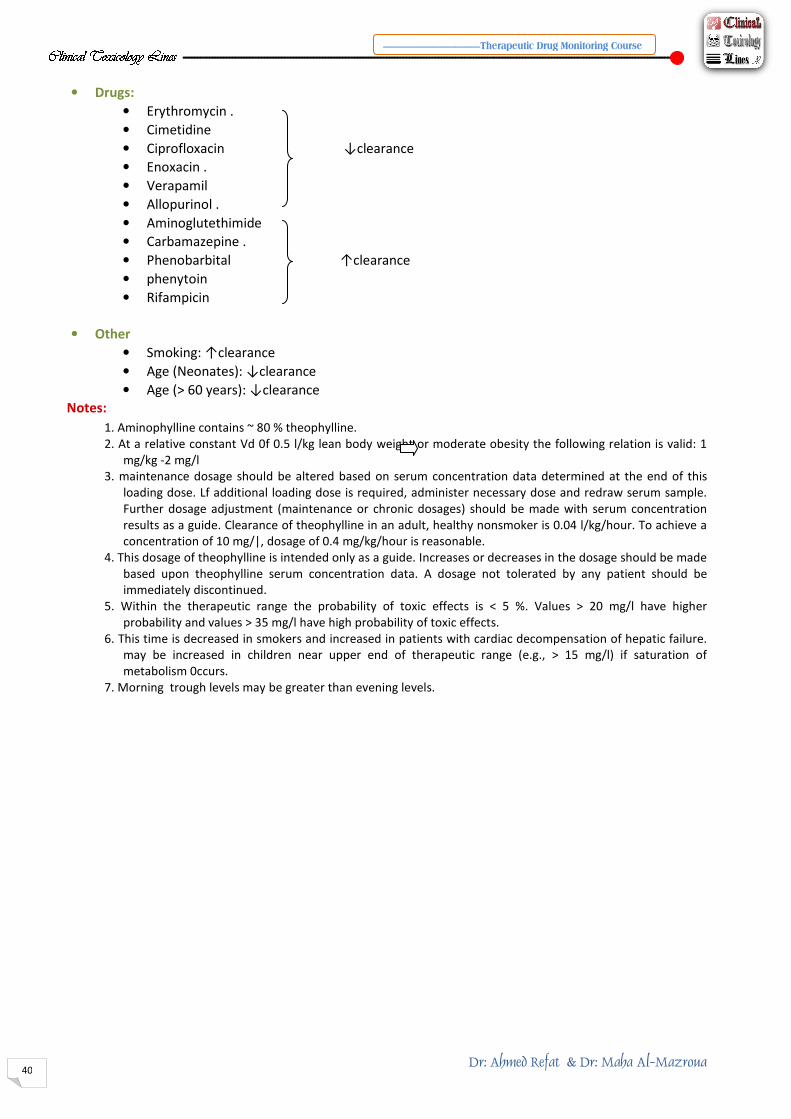
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
40
• Drugs:
• Erythromycin .
• Cimetidine
• Ciprofloxacin
• Enoxacin .
• Verapamil
• Allopurinol .
• Aminoglutethimide
• Carbamazepine .
• Phenobarbital
• phenytoin
• Rifampicin
• Other
• Smoking: ↑clearance
• Age (Neonates): ↓clearance
• Age (> 60 years): ↓clearance
Notes:
1. Aminophylline contains ~ 80 % theophylline.
2. At a relative constant Vd 0f 0.5 l/kg lean body weight or moderate
mg/kg -2 mg/l
3. maintenance dosage should be al
loading dose. Lf additional loading dose is required, administer necessary dose and redraw serum sample.
Further dosage adjustment (maintenance or chronic dosages) should be made with se
results as a guide. Clearance of theophylline in an adult, healthy nonsmoker is 0.04 l/kg/hour. To achieve a
concentration of 10 mg/|, dosage of 0.4 mg/kg/hour is reasonable.
4. This dosage of theophylline is intended only as a guide.
based upon theophylline serum concentration data. A dosage not
immediately discontinued.
5. Within the therapeutic range the probability of toxic effects is
probability and values > 35 mg/l have high probability of toxic effects.
6. This time is decreased in smokers and increased in patients
may be increased in children near upper end of ther
metabolism 0ccurs.
7. Morning trough levels may be greater than evening levels.
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Ciprofloxacin ↓clearance
Phenobarbital ↑clearance
↓clearance
↓clearance
1. Aminophylline contains ~ 80 % theophylline.
2. At a relative constant Vd 0f 0.5 l/kg lean body weight or moderate obesity the following relation is valid: 1
3. maintenance dosage should be altered based on serum concentration data determined at the end of this
loading dose. Lf additional loading dose is required, administer necessary dose and redraw serum sample.
Further dosage adjustment (maintenance or chronic dosages) should be made with se
results as a guide. Clearance of theophylline in an adult, healthy nonsmoker is 0.04 l/kg/hour. To achieve a
concentration of 10 mg/|, dosage of 0.4 mg/kg/hour is reasonable.
4. This dosage of theophylline is intended only as a guide. Increases or decreases in the dosage should be made
upon theophylline serum concentration data. A dosage not tolerated by any patient sh
5. Within the therapeutic range the probability of toxic effects is < 5 %. Values >
> 35 mg/l have high probability of toxic effects.
6. This time is decreased in smokers and increased in patients with cardiac decompensation of hepatic failure.
increased in children near upper end of therapeutic range (e.g., > 15 mg/l) if saturation of
7. Morning trough levels may be greater than evening levels.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
obesity the following relation is valid: 1
data determined at the end of this
loading dose. Lf additional loading dose is required, administer necessary dose and redraw serum sample.
Further dosage adjustment (maintenance or chronic dosages) should be made with serum concentration
results as a guide. Clearance of theophylline in an adult, healthy nonsmoker is 0.04 l/kg/hour. To achieve a
reases or decreases in the dosage should be made
tolerated by any patient should be
< 5 %. Values > 20 mg/l have higher
with cardiac decompensation of hepatic failure.
(e.g., > 15 mg/l) if saturation of

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
41
DOGOXIN (Lanoxin):
USUAL DOSAGE
- Loading dosage (rapid digitalizing)
Oral
• Adults and children > 10 years
• Children (2 to 10 years):
• infants (1 to 24 months):
• Neonates (0 to 4 weeks):
• Administer in 3 to 4 divided doses over 24 hours
- Intravenous
• Use approximately 0.8 x the oral loading dose.
30 minutes (at least 4 hour inter
the first or second dose; use the actual amount administered to calculate the maintenance
dose
- Maintenance dosage
• Adults
-Normal renal function
-Renal failure: see note 2 and table below
• Children(2 to 10 years)
• Infants(1 to 24 months):
• Neonates(0 to 4 weeks):
• Adjust on the basis of the final loading dose and estimated renal
fibrillation, on the basis of heart rate.
clearance, are shown in the table below:
Creatinine clearance(ml/min)
100
50
25
10
0
USUAl DOSING INTERVAl
• Once daily for adult patients receiving
0.25 mg/day. Divide the dose
• If there are gastrointestinal side effects, such as nausea, anorexia
• Divide the dose into 2 or 3 daily doses for paediatric patients
TOXIC EFFECTS
• Caraiac:
- Ventricular dysrhythmias, including multifocal PVC, ventricular tachycardia
- A V block, accelerated A
- Sinus bradycardia or complete SA block
- Atrial fibrillation with slow ventricular rate .
• Gastrointestinal:
- Anorexia, nausea, vomiting, diarrhea
• Neuroiogical:
- Headache, fatigue, malaise, disturbance of color vision
Time to peak serum concentration
• Intravenous:
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
(rapid digitalizing)
Adults and children > 10 years: 12 to 20 µg/kg
o 10 years): 10 to 40 µg/kg
onths): 20 to 40 µg /kg
Neonates (0 to 4 weeks): 20 to 30 µg/kg
Administer in 3 to 4 divided doses over 24 hours
Use approximately 0.8 x the oral loading dose. Administer in 3 to 4 divided doses over 5 to
minutes (at least 4 hour intervals). 0mit doses if these are signs of digoxin toxicity after
first or second dose; use the actual amount administered to calculate the maintenance
ormal renal function: 125 to 500 µg/day PO
see note 2 and table below
Children(2 to 10 years): 8 to 10 µg/kg/day PO
Infants(1 to 24 months): 14 to 18 µg/kg/day PO
Neonates(0 to 4 weeks): 8 to 10 µg/kg/day PO
Adjust on the basis of the final loading dose and estimated renal function and, in atrial
fibrillation, on the basis of heart rate. Suggested maintenance doses, based on creatinine
are shown in the table below:
reatinine clearance(ml/min) Fraction of loading dose
0.33
0.25
0.20
0.16
0.14
nce daily for adult patients receiving < 0.2S mg/day and twice daily for patients receiving >
0.25 mg/day. Divide the dose
f there are gastrointestinal side effects, such as nausea, anorexia or dianhea.
the dose into 2 or 3 daily doses for paediatric patients
dysrhythmias, including multifocal PVC, ventricular tachycardia
A V block, accelerated A-V junctional rhythms.
Sinus bradycardia or complete SA block.
Atrial fibrillation with slow ventricular rate .
Anorexia, nausea, vomiting, diarrhea
, fatigue, malaise, disturbance of color vision
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
3 to 4 divided doses over 5 to
vals). 0mit doses if these are signs of digoxin toxicity after
first or second dose; use the actual amount administered to calculate the maintenance
function and, in atrial
doses, based on creatinine
raction of loading dose
daily for patients receiving >
or dianhea.
dysrhythmias, including multifocal PVC, ventricular tachycardia.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
42
Peak concentration is usually reached immediately after
does not accurately reflect tissue digoxin concentration and thus pharmacological effect
(see usual sampling times).
• Oral:
Peak concentration following oral therapy is usually reached
ln 60 to 90 minutes after administration (see also above,
TIME TO ACHIEVE STEADY STATE
• Normal renal function: ~ 5 to 7 days of chronic dosing
• Reduced renal function: ~
ELIMINATION HALF-LIFE
• Adults mean 40 hours, range 20 to 50 hours
• Premature neonates 56 to 88 hours .
• Full term neonates 35 to 42 hours .
• lnfants 18 to 33 hours .
• Children ~ 12 to 24 hours
ROUTE OF ELIMINATION
• Renal 75 to 80 % excreted unchanged .
• Hepatic ~ 30 % (may be increased substantially in patients
PROTEIN BINDING
• ~20%
USUAl SAMPLING TIMES
• 8 to24 hours after dose administered(better correlation of serum and tissue concentrations)
USUAl THERAPEUTIC RANGE
• 0.8 to 2.0 µg/l (1.0 to 2.6 nmol/l)
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
• renal disease
• Sever,uncompensated heart failure
Drugs:
• Spironolactone
• Liquid antacids and kaolin
• Quinidine, amiodarone
Notes:
1. The preferred method of administering the loading dose is
loading dose by this route. lntravenous loading is generally reserved for patients
with life-threatening tachyarrhythmias responsive to the
patient and renal function. For patients with severe renal impairment
of the range to compensate for a reduction in the volume 0f distribution.
digitalizing is not necessary and treatment is started with the maintenance dose.
2. ln adults with renal failure, maintenance dose regimen should
3.The dosing intervals listed are only guidelines. Each patient
based on age, clinical response, and renal function.
4. For serum concentrations to best reflect cardiac activity, serum
equilibrium between serum and tissue. The time t
8 to 12 hours.
5. Depends on renal function e.g., up to 120 hours in renal failure.
6. There are other factors which do not affect digoxin serum concentrations,
effect of digoxin, for example hypokalemia, hypomagnesemia, hypercalcemia,
These may act by affecting myocardial
tablets. The user is referred to pharmacology tex
7. Acetyldigoxin is rapidly and totally converted to digoxin.
equivalent dose of diqoxin.
8. Bioavailability of digoxin products is highly variable (70 to
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Peak concentration is usually reached immediately after administration. However, this
curately reflect tissue digoxin concentration and thus pharmacological effect
(see usual sampling times).
Peak concentration following oral therapy is usually reached
ln 60 to 90 minutes after administration (see also above, intravenous).
5 to 7 days of chronic dosing
~ Greater than 7 days,depending upon degree of reduction
Adults mean 40 hours, range 20 to 50 hours
Premature neonates 56 to 88 hours .
Full term neonates 35 to 42 hours .
Renal 75 to 80 % excreted unchanged .
Hepatic ~ 30 % (may be increased substantially in patients with renal impairment)
8 to24 hours after dose administered(better correlation of serum and tissue concentrations)
0.8 to 2.0 µg/l (1.0 to 2.6 nmol/l)
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Sever,uncompensated heart failure
↓clearance
Spironolactone
Liquid antacids and kaolin-pectin preparations ↓absorpRon
uinidine, amiodarone: ↑serum concentraRon
method of administering the loading dose is orally, and the majority of patients receive their
by this route. lntravenous loading is generally reserved for patients
threatening tachyarrhythmias responsive to the drug. The dose varies, depending upon the age of the
and renal function. For patients with severe renal impairment chose a loading dose at the low end
for a reduction in the volume 0f distribution. ln most clinical situations rapid
and treatment is started with the maintenance dose.
2. ln adults with renal failure, maintenance dose regimen should be adjusted to individual patient requirments.
3.The dosing intervals listed are only guidelines. Each patient should have a dosing interval selected individually
age, clinical response, and renal function.
4. For serum concentrations to best reflect cardiac activity, serum samples should be taken when digoxin is in
serum and tissue. The time to equilibrium following either oral or lV digoxin is usually
5. Depends on renal function e.g., up to 120 hours in renal failure.
6. There are other factors which do not affect digoxin serum concentrations, but do affect the pharmacological
for example hypokalemia, hypomagnesemia, hypercalcemia, and acid
These may act by affecting myocardial sensitivity to digoxin or by affecting the oral absorption of digx
tablets. The user is referred to pharmacology texts for fulI lists of these factors.
7. Acetyldigoxin is rapidly and totally converted to digoxin. Methyldigoxin is converted to about 50 % of an
8. Bioavailability of digoxin products is highly variable (70 to 100 %) depending on the formulation.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
administration. However, this
curately reflect tissue digoxin concentration and thus pharmacological effect
intravenous).
reater than 7 days,depending upon degree of reduction
with renal impairment)
8 to24 hours after dose administered(better correlation of serum and tissue concentrations)
↓clearance
orally, and the majority of patients receive their
, depending upon the age of the
chose a loading dose at the low end
ln most clinical situations rapid
be adjusted to individual patient requirments.
ave a dosing interval selected individually
samples should be taken when digoxin is in
oral or lV digoxin is usually
but do affect the pharmacological
and acid- base balance.
ting the oral absorption of digxxin
Methyldigoxin is converted to about 50 % of an
n the formulation.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
43
CYCLOSPORIN A (Sandimmun):
USUAL DOSAGE
• Starting doses: (Monotherapy)10 to 15 mg/kg/day
• Chronic maintenance doses:~2 to 6mg/kg/day
• Autoimmune disease: 2.5 to 5 mg/kg/day
USUAl DOSING INTERVAl
• Adults:once or twice daily
• Children:may require three times daily dosing
TOXIC EFFECTS
• Renal dysfunction/raised serum creatinine .
• Hepatic impairment, hypertension , hypomagnesaemia .
• Hypertrichosis, gum hyperplasia
Time to peak serum concentration
• ~3 hours after oral adminstration
TIME TO ACHIEVE STEADY STATE
• 3 to 5 days of chronic dosing
ELIMINATION HALF-LIFE
• Adults: 15 hours(range 4 to 50).
• Children: 9 hours(range 3 to 20)
ROUTE OF ELIMINATION
• Hepatic: ˃90% excreted in bile,
• Renal: ~ 6 % ˂0.1 % as unchanged drug
• Major metabolites: AM1,AM4N,AM9
PROTEIN BINDING
• 98 to 99 %
USUAl SAMPLING TIMES
• Pre-dose,normally about 12 or 24 hours after the last dose
USUAl THERAPEUTIC RANGE
• induction therapy {approx.
• Maintenance therapy: 100 to 250 µg/l .
• Values refer to whole blood specific measurements.
• Therapeutic range varies dependent upon organ transplanted.
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Disease
• Hepatic impairement reduces cyclosporin clearance and prolongs the elimination half
• Diarrhea and inflammatory bowel disorders reduce oral absorption.
Drugs:
• Ketoconazole .
• Erythromycin .
• Diltiazem . ↑
• Verapamil
• Nicardipine .
• rifampicin .
• isoniazlde .
• Phenytoin . ↓
• Phenobarbital .
• Carbamazepine
Notes:
1. Doses vary widely, depending upon the indication for cyclosporin,
co-prescription of other immunosuppressive drugs. lt is common practice for
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
onotherapy)10 to 15 mg/kg/day - (Compination therapy)7 to 10 mg/kg/day
hronic maintenance doses:~2 to 6mg/kg/day
2.5 to 5 mg/kg/day
Adults:once or twice daily
Children:may require three times daily dosing
enal dysfunction/raised serum creatinine .
Hepatic impairment, hypertension , hypomagnesaemia .
Hypertrichosis, gum hyperplasia
~3 hours after oral adminstration
3 to 5 days of chronic dosing
15 hours(range 4 to 50).
9 hours(range 3 to 20)
90% excreted in bile,˂1% as unchanged drug
˂0.1 % as unchanged drug
AM1,AM4N,AM9
dose,normally about 12 or 24 hours after the last dose
therapy {approx. < 3 months after transplantation) 150 to 350 µg/l .
100 to 250 µg/l .
refer to whole blood specific measurements.
range varies dependent upon organ transplanted.
SELECTED FACTORS AFFECTING SERUM CONCENTRATIONS
Hepatic impairement reduces cyclosporin clearance and prolongs the elimination half
Diarrhea and inflammatory bowel disorders reduce oral absorption.
↑Cyclosporin concentrations
erapamil
↓Cyclosporin Concentration
Phenobarbital .
Doses vary widely, depending upon the indication for cyclosporin, the time following transplantation and the
of other immunosuppressive drugs. lt is common practice for cyclosporin dosage to be
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
ompination therapy)7 to 10 mg/kg/day
after transplantation) 150 to 350 µg/l .
Hepatic impairement reduces cyclosporin clearance and prolongs the elimination half-life
the time following transplantation and the
cyclosporin dosage to be

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
44
adjusted on the basis of blood concentration
cyclosporin measurements should be made in blood and the majority of centres follow
Concentrations in plasma or serum ar
blood sample.
2. A loading dose is not normally given. A variety of induction protocols
before transplantation, others only when adequate renal function ha
lntravenous doses are usually given in clinical settings in which
common. These include after liver transplantation, following bone marrow transplantation
with cystic fibrosis who have received a
between patients. lt may also be affected by bile acids and food. A new oral formulation
Neoral) is available, and appears to display more
current solution or gelatine capsules.
3. The dose is usually reduced on the basis of cyclosporin blood
signs of deteriorating renal function.
4. The intravenous preparation contains polyethoxylated castor oil
reactions, including anaphylaxis. lntravenous doses are approximately one
5. Patients with cystic fibrosis may require up
doses needed.
6. Blood monitoring prior to steady state may be useful to establish
7. The elimination half-life may be underestimated if blood samples
hour dosing lnterval.
8. Blood samples should not be collected via intravenous Iines
administered, as there is significant and reversible binding of the drug to the tubing.
9. Ranges apply primarily to kidney, liver and heart transplant recipients. Higher concentrations are common
using the doses associated with lung or heart
patients with triple or quadruple regimens and in patients with liver dy
variations in practice between different units.
10. High probability of toxicity at pre
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
adjusted on the basis of blood concentration measurements. The consensus recommendations are that
should be made in blood and the majority of centres follow
Concentrations in plasma or serum are lower and are affected by the temperature of separation of the
2. A loading dose is not normally given. A variety of induction protocols are used, some starting cyclosporin
others only when adequate renal function has been established,
lntravenous doses are usually given in clinical settings in which poor oral absorption is suspected or
after liver transplantation, following bone marrow transplantation
c fibrosis who have received a lung or heart/lung transplant. oral absorption varies substantially
also be affected by bile acids and food. A new oral formulation
Neoral) is available, and appears to display more consistent absorption characteristics than either the
solution or gelatine capsules.
3. The dose is usually reduced on the basis of cyclosporin blood concentration measurements and if there are
renal function.
paration contains polyethoxylated castor oil and has been associated with some adverse
anaphylaxis. lntravenous doses are approximately one third of the oral dose
5. Patients with cystic fibrosis may require up-to four times daily dosing because of the relatively large oral
6. Blood monitoring prior to steady state may be useful to establish that the patient is absorbing the drug.
life may be underestimated if blood samples are only collected durin
8. Blood samples should not be collected via intravenous Iines through which cyclosporin has been
significant and reversible binding of the drug to the tubing.
kidney, liver and heart transplant recipients. Higher concentrations are common
using the doses associated with lung or heart-lung transplantation. Lower concentrations are common in
patients with triple or quadruple regimens and in patients with liver dysfunction. However, there are wide
variations in practice between different units.
10. High probability of toxicity at pre-dose concentration > 400 µg/l during maintenance therapy.
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
The consensus recommendations are that
should be made in blood and the majority of centres follow this advice.
and are affected by the temperature of separation of the
are used, some starting cyclosporin
s been established, post-operatively.
poor oral absorption is suspected or
after liver transplantation, following bone marrow transplantation and in patients
oral absorption varies substantially
also be affected by bile acids and food. A new oral formulation (Sandimmun
ent absorption characteristics than either the
concentration measurements and if there are
and has been associated with some adverse
third of the oral dose
ng because of the relatively large oral
that the patient is absorbing the drug.
are only collected during a single 12 or 24
through which cyclosporin has been
significant and reversible binding of the drug to the tubing.
kidney, liver and heart transplant recipients. Higher concentrations are common
lung transplantation. Lower concentrations are common in
sfunction. However, there are wide
during maintenance therapy.

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
45
References • Brunton LL, Chabner BA, Knollman BC. Goodman
Therapeutics. 12th ed. McGraw
• Burtis CA, Ashwood ER, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th
ed. Philadelphia: WB Saunders;
• Deenen MJ, Cats A, Beijnen JH, Schellens
adoption of pharmacogenetics.
• Oncologist. 2011;16(6):811-
• Epstein RS, Moyer TP, Aubert RE, O Kane DJ, Xia F, Verbrugge RR, Gage BF, Teagarden JR. Warfarin
genotyping reduces hospitaliz
22; 55(25):2804-2812.
• Kaplan LA, Pesce A, Kazmierczak S. Clinical Chemistry: Theory, Analysis, Correlation. 4th ed. New
York: Mosby; 2002.
• Tanaka E, Terada M, Misawa S. Cytochrome P450 2E1: i
Pharm Ther. 2000Jun;25(3):165
• Froscher W, Eichelbaum M, Gugler B, ilildebrand G, Penin H.
• Beardsley RS, Freeman JM, Appel FA. Epilepsia 24: 330
• Lund L. Arch. Neurol.31.289
• Oellerich M, Bohm MM, Tietjen HG, Sybrecht GW. Theophyl
Staib AH, Woodcock BG,
• Rietbrock N (eds): Vieweg Verlag, Braunschweig,255
• Evans WE, Crom WR, Abromowitch M et a
• Whipple JK, Ausman RK, Franson T, Ouebbeman EJ. Crit Care
• OellerichM , Schutz E, Polzien F et al. Ther Drug Monit 16:
• Oellerich M, Burdelski M, Ringe B et al. Lancet 1.640
• Schroeder TJ, Gremse DA, Mansour ME et al. Transplant Proc.
• Oellerich M, Burdelski M, Lautz HU et al. Hepatology 14: 1029
• Koch-Weser J. NewEngl J Med 287: 227
• College of American Pathologists lnc.: T
• Kahan BD, Shaw LM, Holt D, Grevel J, Johnston A Consensus
therapeutic drug monitoring
• Shaw LM, Yatscoff RW, Bowers LD et al .Canadia
report of the consensus panel. Clin Chem 36: 1841
• Jusko WJ and D'Ambrosio R. Transplant Proc 23:2732
• Preskorn SH, and Fast GA. J Clin Psychiatry 52 (suppl): 23
• Bennett M J, Carpenter KH, Worthy E, Iilleyman JS. Clin Chem
• Matzuk MM, Shlomchik M, Shaw LM. Ther Drug Monit 13:
• Edson RS, and Terrell CL. Mayo Clin Proc 66: 1158
• Tulkens PM. Scand J Infect Dis, Suppl 74:
• Holt DW, Fashola T0A, Johnston A. immunology Letters 29:
• Oellerich M and Muller-Vahl H. Clin Pharmacokinet 9 (Suppl 1):
• Peck CC, D'Argenio DZ, Rodmas JH, Applied Pharmacokinetics:
Monitoring, 3rd edition. Evans
Vancouver, WA, (1992).
• Sawchuk RJ, Zaske DE, Cipolle BJ, Wargin WA, Strate BG Clin
• Sheiner LB, Rosenberg B,Melmon K. Computer
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Brunton LL, Chabner BA, Knollman BC. Goodman & Gilman's The Pharmacological Basis of
Therapeutics. 12th ed. McGraw-Hill, 2011.
Burtis CA, Ashwood ER, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th
ed. Philadelphia: WB Saunders; 2005.
Deenen MJ, Cats A, Beijnen JH, Schellens JH. Part 1: background, methodology, and clinical
adoption of pharmacogenetics.
-819. Epub 2011 May 31.
Epstein RS, Moyer TP, Aubert RE, O Kane DJ, Xia F, Verbrugge RR, Gage BF, Teagarden JR. Warfarin
hospitalization rates results from the MM-WES. J Am Coll Cardiol. 2010 Jun
Kaplan LA, Pesce A, Kazmierczak S. Clinical Chemistry: Theory, Analysis, Correlation. 4th ed. New
Tanaka E, Terada M, Misawa S. Cytochrome P450 2E1: it's clinical and toxicological role. J Clin
Pharm Ther. 2000Jun;25(3):165-75.
Froscher W, Eichelbaum M, Gugler B, ilildebrand G, Penin H. J Neurol 224 193201,(1981)
Beardsley RS, Freeman JM, Appel FA. Epilepsia 24: 330-335, ( 1983).
Lund L. Arch. Neurol.31.289-294,(1914).
ellerich M, Bohm MM, Tietjen HG, Sybrecht GW. Theophyl lines and other methylxanthines,
Rietbrock N (eds): Vieweg Verlag, Braunschweig,255-266, ( 1982).
Evans WE, Crom WR, Abromowitch M et al. New Engl J Med 314:471-477, (1986).
Whipple JK, Ausman RK, Franson T, Ouebbeman EJ. Crit CareMed 19: 1480-1485, (1991).
OellerichM , Schutz E, Polzien F et al. Ther Drug Monit 16:225-231 ,(1994)
Oellerich M, Burdelski M, Ringe B et al. Lancet 1.640-642,(1989).
Schroeder TJ, Gremse DA, Mansour ME et al. Transplant Proc.21 .2299-2301 ,(1989).
Oellerich M, Burdelski M, Lautz HU et al. Hepatology 14: 1029-1034,(1991)
Weser J. NewEngl J Med 287: 227- 231,(1972).
College of American Pathologists lnc.: TDM Survey, Set Z-A,Skokie,lL, USA(1991).
Kahan BD, Shaw LM, Holt D, Grevel J, Johnston A Consensus Document: Hawk's Cay meeting on
therapeutic drug monitoring of cyclosporine. Clin Chem 36. 1510- 1516, (1990).
Shaw LM, Yatscoff RW, Bowers LD et al .Canadian Consensus Meeting on cyclosporine monitoring:
panel. Clin Chem 36: 1841- 1846, (1990).
Jusko WJ and D'Ambrosio R. Transplant Proc 23:2732-2735, (1991 ).
Preskorn SH, and Fast GA. J Clin Psychiatry 52 (suppl): 23-33, (1991 ).
Bennett M J, Carpenter KH, Worthy E, Iilleyman JS. Clin Chem 30: 817, (1984).
Matzuk MM, Shlomchik M, Shaw LM. Ther Drug Monit 13:215- 219, (1991 ).
Edson RS, and Terrell CL. Mayo Clin Proc 66: 1158- 1164, (1991 ).
Tulkens PM. Scand J Infect Dis, Suppl 74: 249-257, (1991).
Holt DW, Fashola T0A, Johnston A. immunology Letters 29: 99 -103,(1991).
Vahl H. Clin Pharmacokinet 9 (Suppl 1): 61- 70 (1984).
Peck CC, D'Argenio DZ, Rodmas JH, Applied Pharmacokinetics: Principles of Therapeutic D
Monitoring, 3rd edition. Evans WE, Schentag JJ, Jusko WJ eds. Applied Therapeutics, lnc.
Sawchuk RJ, Zaske DE, Cipolle BJ, Wargin WA, Strate BG Clin Pharmacol Ther 21: 362
Sheiner LB, Rosenberg B,Melmon K. Computer Biomed Res 5: 411- 459,(1972).
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
& Gilman's The Pharmacological Basis of
Burtis CA, Ashwood ER, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th
JH. Part 1: background, methodology, and clinical
Epstein RS, Moyer TP, Aubert RE, O Kane DJ, Xia F, Verbrugge RR, Gage BF, Teagarden JR. Warfarin
WES. J Am Coll Cardiol. 2010 Jun
Kaplan LA, Pesce A, Kazmierczak S. Clinical Chemistry: Theory, Analysis, Correlation. 4th ed. New
t's clinical and toxicological role. J Clin
J Neurol 224 193201,(1981)
lines and other methylxanthines,
477, (1986).
1485, (1991).
2301 ,(1989).
Skokie,lL, USA(1991).
Document: Hawk's Cay meeting on
1516, (1990).
Meeting on cyclosporine monitoring:
30: 817, (1984).
219, (1991 ).
70 (1984).
Principles of Therapeutic Drug
WE, Schentag JJ, Jusko WJ eds. Applied Therapeutics, lnc.
Pharmacol Ther 21: 362 -369, (1977).
459,(1972).

� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � ــــــــــــــــــــــــــــــــــــــــــــ
46
• Bottger H-Ch, 0ellerich M, Sybrecht GW. Ther Drug Monit 10:
• Pryka RD, Rodvold KA, Garrison M, Rotschafer JC. Ther Drug
• 0ellerich M, Schneider B. In: Keller H, Trendelenburg Ch, eds
Clinical biochemistry, 2. Data
1989).
• Vozeh S. Clin Pharmacokinet 13: 131
• Burton ME, Ash CL, Hill Jr DP, Handy T, Shepherd MD, Vasko
694, {1991 ).
• 31.Destache CJ, Meyer SK, Bittner MJ, Hermann KG. Ther Drug
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
Dr: Ahmed Refat &
Therapeutic Drug Monitoring Courseــــــــــــــــــــــــــــــــــــــــــــ
Ch, 0ellerich M, Sybrecht GW. Ther Drug Monit 10: 280- 286, (1988).
Pryka RD, Rodvold KA, Garrison M, Rotschafer JC. Ther Drug Monit 11: 450-454, (1989).
0ellerich M, Schneider B. In: Keller H, Trendelenburg Ch, eds Curtius HCh, Both M, series eds.
Clinical biochemistry, 2. Data presentation, interpretation. Berlin: W. de Gruyter & Co. ,403
Vozeh S. Clin Pharmacokinet 13: 131 -140, (1987).
Burton ME, Ash CL, Hill Jr DP, Handy T, Shepherd MD, Vasko MR. Clin Pharmacol Ther 49: 685
31.Destache CJ, Meyer SK, Bittner MJ, Hermann KG. Ther DrugMonit 12: 419
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
& Dr: Maha Al-Mazroua
Therapeutic Drug Monitoring Course
286, (1988).
454, (1989).
Curtius HCh, Both M, series eds.
presentation, interpretation. Berlin: W. de Gruyter & Co. ,403- 423 (
lin Pharmacol Ther 49: 685-
Monit 12: 419- 426, (1990).