The Role of VATS in the Diagnosis of Sarcoidosis · of these two diseases and it was stated in the...
15
1 Sarcoidosis Diagnosis | www.smgebooks.com Copyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited. Diagnosis of Sarcoidosis: Exclusion of Tubercu- losis: Diagnostic Enigma in Clinical Practice INTRODUCTION Definitive diagnosis of sarcoidosis is not possible in some cases where there are overlapping features or disease confined to one organ and requires follow up of several years to clarify. The relationship between sarcoidosis and tuberculosis (TB) remains controversial, and this enigma continues to baffle even the most astute physicians across the world. The exact distinction between these two entities is very often blurred due to similar clinical and radiological features of these two diseases and it was stated in the earliest description of it by J Huchinson in 1887 who considered it as unsual type of lupus [1]. Whether Mycobacterium tuberculosis has a role in causative aetiology of sarcoidosis is unclear despite decades of research [2]. Newer molecular methods of diagnosis may help us in future while making the diagnosis of either of these conditions with confidence. However, for the treating physician it is important to distinguish between the two entities as the treatment is diametrically opposite to each other. It is not uncommonin countries with high burden of tuberculosis to see patientsbeing treated for tuberculosis alone or for bothdiseases together due to lack of ruling in or ruling out of tuberculosis with confidence by the treating physicians. Deepak Talwar* and Arjun Khanna Pulmonary & Critical care, Metro Centre for Respiratory Diseases, India *Corresponding author: Deepak Talwar, Director & Chair, Pulmonary & Critical care, Metro Group of Hospitals, L-94, sector 11 Noida, 201301, India. Email: [email protected] Published Date: September 05, 2016 Gr up SM
Transcript of The Role of VATS in the Diagnosis of Sarcoidosis · of these two diseases and it was stated in the...

1Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Diagnosis of Sarcoidosis: Exclusion of Tubercu-losis: Diagnostic Enigma in Clinical Practice
INTRODUCTIONDefinitive diagnosis of sarcoidosis is not possible in some cases where there are overlapping
features or disease confined to one organ and requires follow up of several years to clarify. The relationship between sarcoidosis and tuberculosis (TB) remains controversial, and this enigma continues to baffle even the most astute physicians across the world. The exact distinction between these two entities is very often blurred due to similar clinical and radiological features of these two diseases and it was stated in the earliest description of it by J Huchinson in 1887 who considered it as unsual type of lupus [1]. Whether Mycobacterium tuberculosis has a role in causative aetiology of sarcoidosis is unclear despite decades of research [2]. Newer molecular methods of diagnosis may help us in future while making the diagnosis of either of these conditions with confidence. However, for the treating physician it is important to distinguish between the two entities as the treatment is diametrically opposite to each other. It is not uncommonin countries with high burden of tuberculosis to see patientsbeing treated for tuberculosis alone or for bothdiseases together due to lack of ruling in or ruling out of tuberculosis with confidence by the treating physicians.
Deepak Talwar* and Arjun KhannaPulmonary & Critical care, Metro Centre for Respiratory Diseases, India
*Corresponding author: Deepak Talwar, Director & Chair, Pulmonary & Critical care, Metro Group of Hospitals, L-94, sector 11 Noida, 201301, India. Email: [email protected]
Published Date: September 05, 2016
Gr upSM

2Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
The exact aetiology of sarcoidosis is poorly understood and still not known. Asgranulomatous inflammation plays central role in pathogenesis of sarcoidosis and variety of antigenic stimuli are believed to be responsible for it. Many clinical conditions caused by variety of organic and inorganic antigens are characterized by similar granulomatous inflammation [3] and one need to rule out such known causes prior to reaching the diagnosis of sarcoidosis, hence in high prevalence countries with tuberculosis risks of misdiagnosis and over diagnosis is more. Though initiation of inflammation in sarcoidosis has been linked to the presence of a poorly degradable antigen [4] but none has stood the test of time and scientific studies. The most plausible antigen postulated and investigated is Mycobacterium tuberculosis (MTB) [4] but ‘one disease, one cause’ is yet elusive in sarcoidosis. Hence, sarcoidosis is always a diagnosis of exclusion ( of tuberculosis ) in countries with high burden of tuberculosis which poses significant challenges from epidemiological to clinical, radiological, pathological, immunological and therapeutic overlapping findings.
EPIDEMIOLOGICAL OVERLAP Conventionally, sarcoidosis is seen typically in developed nations and tuberculosis in developing
and underdeveloped world. However, over the past few years sarcoidosis is being increasingly diagnosed in the developing countries which may be due to a relative decline in tuberculosis due to effective TB control programs or due to increasingly more recognition of sarcoidosis due to heightened awareness and better availability of radiological and bronchoscopic diagnostic methods is not well understood [5]. A large review linking the two diseases has pointed that sarcoidosis was detected more commonly once the TB prevalence decreased in the populations [6]. Surprisingly it has been noted that ethenic populations with higher incidence of TB also had a higher incidence of sarcoidosis and over a period of time the prevalence of both the diseases moves in a parallel direction [7].
CLINICAL OVERLAP Sarcoidosis and Tubeculosis have remarkable clinco-radiological similarities as both the
diseases have propensity of virtually affecting any organ or many organs at any point of time sequentially or consecutively. The usual presentation of both these diseases includes constitutional symptoms such as malaise, fatigue, anorexia, fever, joint pain etc besides organ specific presentations. The diagnosis of pulmonary tubeculosis is easy when the patient presents with hemoptysis in fibro-cavitatory disease and sputum AFB result is positive. However, this is only one end of the spectrum. Many patients present with non specific complaints and on evaluation have mediastinal lymphadenopathy with or without pulmonary infiltrates, a presentation which is well described with Sarcoidosis as well. Although, untreated tuberculosis have more signs and symptoms as compared to sarcoidosis but no rule of thumb exists as constitutional features are present in 1/3rd cases of sarcoidosis. Classical reoccurant uveitis, erythema nodosum or hepatospleenomegaly has been reported in both clinical conditions. Apical pulmonary fibrosis can occur in both conditions, although cavitation is rarer in sarcoidosis but well described. Even

3Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
findings such as exudative, lymphocytic pleural effusions, so characteristically associated with TB have been described in sarcoidois [8].The ‘footprints’ of sarcoidosis, is multisystem involvement e.g. heart, kidney, central and peripheral nervous system, liver, spleen, eye, skin and other visceral organs ( Figure 1& 2 ) but such organ involvement is seen in few patients with tuberculosis with widespread systemic dissemination, a situation practically indistinguishable from sarcoidosis [9]. Hence, confident diagnosis is needed prior to initiation of treatment. Though there is no pathogonomic clinical findings of sarcoidosis but Lofgren’s, Miculicz, Heerfordt’s syndromes orbilateral facial nerve palsy mostly requires no diagnostic work up [10] but still it would be difficult to ignore tuberculosis as a differential or associated disease in endemic regions.
Figure 1: Skin lesions in Sarcoidosis: a. raised pinkish nodular lesion b. large erythematous lesions over legs resembling EN c Nodulo-papular, reddish lesions over thigh d keloid over scar
e. erythematous, raised lesions over elbow f. raised nodular scaly psoriasis like lesions over back. All lesions on biopsy revealed NCG consistent with Sarcoidosis.

4Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 2: Eye involvement in Sarcoidosis: Chagren’s patch over eye lid, showed NCG on biopsy. b. Pars Plana exudation c. Anterior Synechiaed. Cystoid macular edema with macular scarring.
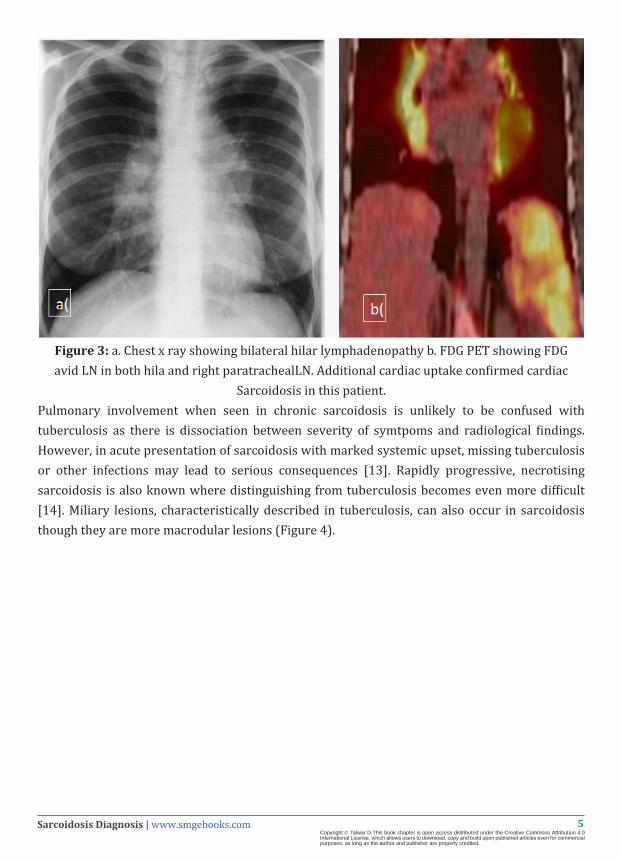
4. RADIOLOGICAL IMAGING OVERLAPBilateral hilar lymphadenopathy, the commonest clinical presentation of sarcoidosis, is also described in tuberculosis [11]. Isolated mediastinal lymphadenopathy is a frequent confusing presentation in third world as characteristic lymphnodal features are not helpful even on contrast enhanced CT scans. Although, lymph nodes in sarcoidosis are usually discrete, smooth, bilateral, symmetrical and usually not associated with central hypodensity indicating necrosis, whereas a central necrosis and asymmetric conglomerate lymph nodes are classically described in tuberculosis, but such classical findings are exception rather than rule. Neither absence of necrosis, nor size or location of LN in thorax can confidently rule out tuberculosis (Figure 3). Calcification has been reported in 53% and 46% of sarcoid and tuberculosis patients respectively [12].
5Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 3: a. Chest x ray showing bilateral hilar lymphadenopathy b. FDG PET showing FDG avid LN in both hila and right paratrachealLN. Additional cardiac uptake confirmed cardiac
Sarcoidosis in this patient.Pulmonary involvement when seen in chronic sarcoidosis is unlikely to be confused with tuberculosis as there is dissociation between severity of symtpoms and radiological findings. However, in acute presentation of sarcoidosis with marked systemic upset, missing tuberculosis or other infections may lead to serious consequences [13]. Rapidly progressive, necrotising sarcoidosis is also known where distinguishing from tuberculosis becomes even more difficult [14]. Miliary lesions, characteristically described in tuberculosis, can also occur in sarcoidosis though they are more macrodular lesions (Figure 4).

6Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 4: FDG PET/CT showing FDG avid lymphnodes in and lung lesions which on routine CT appeared fibrotic and inactive.
Thus, no clinical or radiological sign can distinguish between the two clinical entities with absolute certainty and leaves us for want of mycobacterial results.
ETIOLOGICAL OVERLAPAs the histopathological hallmark of sarcoidosis is a granuloma, an infectious, transmissible
aetiology was thought to be responsible for it [15]. Though Mycobacterium tuberculosis as the cause of does not fulfil the Koch’s postulates, but scientific data linking sarcoidosis with M tuberculosis is both impressive and controversial. The theory of infectious transmission is further strengthened by the observation that transplant recipients develop sarcoidosis after receiving organs from donors with sarcoidosis [16]. Some workers have also, demonstrated cell wall deficient bacteria, which are variably acid fast in tissue samples supposed to be sarcoid granulomas [17]. The issue is further complicated in the developing countries with high prevalence of tuberculosis, where tissue samples may have variable presence of AFB which may not represent active tuberculosis but needs to be accounted for. Hence, coexistence of both these diseases has been reported, and has lead workers to propose terms such as ‘Tuberculosis -Sarcoidosis’ [18]. As expected,

7Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
prevalence of NAAT based detection of tubercular antigens in sarcoidosis is more in countries with a higher prevalence of tuberculosis. Gupta and collegues suggested an association rather than a chance occurrence of finding positive mycobacterial NAAT results as the pooled odds for studies having a control arm were 7.32 (95% CI, 3.74–14.33).This raises the question whether to treat tuberculosis upfront at the time of diagnosis.
PATHOLOGICAL OVERLAPHistologically, both tuberculosis and sarcoidosis show granuloma- tous inflammation in tissue
samples. Pathologist usually describe multiple, discrete, well formed, non-necrotizing compact granulomas with no or minimal central necrosis in sarcoidosis but there are no specific diagnostic features of sarcoid granuloma. On the other hand, granulomas with a more florid necrotizing inflammation is commonly seen in TB. However, necrosis has been described in biopsy samples of sarcoidosis and reported in up to 35% of specimens [19]. The detection of necrosis is far less in smaller specimens such as bronchoscopic lung biopsies [20] and bigger tissue specimens obtained with cryoprobe has been shown to improve chances of showing necrosis [21]. Peribronchovascular location of granulomas is an clue to sarcoidosis as it corresponds to perilymphatic distribution of disease seen on CT scans [22]. Similarly, one can find noncaseating granulomas in tuberculosis in up to 24% of cases [23]. Though there are subtle differences in histological appearance but there are no features specific enough to differentiate the two conditions with certainty, apart from positive mycobacterial results [24].
IMMUNOLOGICAL OVERLAP In subjects with sarcoidosis there is a depressed delayed hypersensitivity manifesting as
cutaneous anergy. Tuberculin sensitivity is depressed in sarcoidosis even in the background of high prevalence of TB. This tuberculin energy is commonly utilized as a diagnostic tool and is seen in active sarcoidosis which disappears with disease inactivity and positive test suggests an alternative diagnosis [25]. A negative test at a cut-off of 10mm reaction to 5TU PPD has virtually 100% sensitivity for sarcoidosis; similarly a negative tuberculin test excludes TB infection, except in immune compromised individuals, such as those with terminal malignancies, AIDS etc. But Mantoux is negative in 90% of sarcoidosis and 35-6% in tuberculosis, further emphasising that significant overlap exists here too. Also, positive mantoux in sarcoidosis is seen either when two diseases coexist or sarcoid is in remission and seen in up to 40% in some reports [26]. Although, negative mantoux test is considered of high predictive value in sarcoidosis but in high prevalance countries it would be expected in large number of tuberculosis patients too. Hence, positive mantoux in sarcoidosis and negative montoux in tuberculosis would need more histopathological and mycobacterial results to make a confident diagnosis of one or the other condition.
Interferon gamma release assays (IGRAs) have a higher sensitivity and specificity for detecting MTB infection than the conventional TST, as they utilize antigens specific for MTB complex. A positive IGRA, just like a positive PPD response, does not mean active TB infection and cannot rule

8Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
out the diagnosis of sarcoidois [26]. IGRA is a more sensitive test than TST in healthy individuals and, unlike the depressed TST; it continue storema in positive in patients with sarcoidosis [27]. This finding has two very important implications
1. IGRA is better than TST in detecting latent TB infection in patients of sarcoidosis
2. In high prevalence settings a positive IGRA should not be a deterrent for making a diagnosis of sarcoidosis, as it merely represents an underlying latent tubercular infection reported in 29% of sarcoid patients [28].
Antibody detection tests against MTB antigens by ELISA have been studied to distinguish between tuberculosis and non tubercular diseases since 1980’s but were not very sucessful. Serum anti TB IgG were reported to be in the healthy range in sarcoidosis in contrast to much higher levels in tuberculosis [29] but no large data to support its use to distinguish two conditions especially when reactivation of tuberculosis after immunosuppressive therapy is for sarcoidosis is a major concern.
It is now postulated that the presence of mycobacterial infection or BCG vaccination in a genetically predisposed host may contribute to the development of an immune response leading to sarcoidosis [30] and may explain to some extent significant overlap in immunological investigations.
Molecular Gentics Overlap
Molecular genetic studies involving real time PCR methodology has been tested to distinguish between sarcoidosis and tuberculosis on tissue samples obtained on biopsy of involved organs for DNA of MTB but no final answer has come so far. In a study, real-time PCR qualitation and quantification of MTB DNA in sarcoidosis reported to be significantly different MTB DNA measurements from tuberculosis with no statistically significant difference from controls. Although presence of MTB DNA for IS986 area has been reported in samples of tissue from inactive tuberculosis too, it’s simple presence will not be able to distinguish between active versus latent TB and hence would not be able to solve issues in diagnosis in high TB prevalence countries. However, quantitative real time PCR assays by same authors have been shown to distinguish clearly between tuberculosis where multiple copies are demonstratable in TB but only low number copies in sarcoidosis but they used liquid paraffin fixed tissue specimens [31,33]. Hence, although role of real time PCR for detection of MTB DNA is promising but not much experience has come from developing world where the main problem of differentiation between TB and sarcoidosis lies.
Presently role of genexpert for MTB detection has not be reported in distinguishing between tuberculosis and sarcoidosis on tissue samples obtained by biopsies.

9Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Biomarkers Overlap
Need to develop useful biomarkers for diagnosis of sarcoidosis has long been recognized, being a disease where diagnosis is by exclusion and tuberculosis is the forerunner.
Serum Angiotensin Converting Enzyme
A membrane bound glycoprotein expressed by epithelial cells of many tissues but most abundent on the luminal surface of vascular endothelium, pulmonary epithelium, epitheliod cells of sarcoid granulomas, alveolar macrophages and converts angiotensn I to angiotensin II. Less than 50% of sarcoid patients ( 60% in acute and 10% in chronic cases ) have raised serum ACE levels and is also elevated in tuberculosis, lymphoma or atypical mycobacerial infections, close mimicks of sarcoidosis [34]. Normal serum ACE levels does not exclude sarcoidosis, while raised levels can only be of supportive value when clinico-radilogical findings are highly suggestive of sarcoiodsis. Also there is genetic polymorphism in ACE activity [35]. Hence, it’s of little value in distinguishing between sarcoidosis and tuberculosis. There is difference between available commercial kits to measure this value and leads to variable reference limits as well as quality issues.
Blood Gene Profiling
Significant overlap has been reported in gene expression profiles in sarcoidosis and tuberculosis due to histological similarities [36]. Differences in PMBC gene expression between sarcoidosis and tuberculosis using Algilent-014850 Whole Human Genome Microarry showed enrichment of downreglated genes involved in mitochondrial oxidative phosphorylation and translational activity compared with patients with tuberculosis [37].
Therapeutic Overlap
Treatment of two conditions is not only different but also may have harmful and potentially fatal implications if there is an error in judgement.If indeed tuberculosis is a causal factor in sarcoidosis, then this hypothesis can be further reinforced if antitubercular therapy (ATT) is useful in treatment of sarcoidosis. Data on this issue are sparse, conflicting and controversial. These trials were generally small and poorly designed [38].
HOW AND WHY SHOULD WE DISTINGUISH BETWEEN THESE TWO ENTITIES?
The clinicians are often at the cross roads trying to establish whether patient has sarcoidosis or tuberculosis. Often, owing to confusion, the patients are given ATT with steroids which is presently unacceptable in the era of heightened patient awareness and possible toxicity of therapy. This further leads to loss of faith with possiblity of litigation. Hence, clinician must make every attempt to diagnose either of these conditions with confidence and offer treatment accordingly. The highest level of confidence in diagnosis of sarcoidosis has been changed from definite diagnosis

10Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
to highly probable diagnosis of sarcoidosis by researchers realizing that absolute certainty in diagnosis of sarcoidosis is ‘NOT’ achievable [39] (Table 1).
Table 1: Diagnosis of Sarcoidosis: levels of confidence as per individual case with various clinical, radiological and histopathological evidence.
However, this is much more difficult in the developing world, where it’s difficult to exclude tuberculosis with confidence. One requires a strong clinical acumen supported by a constellation of clinical, radiological and laboratory evidence and long follow up to make a confident diagnosis of sarcoidosis (Table 2). A positive tuberculin test in a patient with suspected sarcoidosis or necrosis in granuloma need to be viewed suspiciously and requires extra thoracic evidence of systemic involvement by sarcoidosis e.g. skin, eye or kidney which adds to the level of confidence to reach the final diagnosis. Summary findings in such cases may help clinician at the time of delimma towards making highly probable diagnosis of sarcoidosis (Table 3).

11Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Table 2: Distinguishing features favoring diagnosis of Sarcoidosis or tuberculosis.
Table 3: Steps in evaluation of suspected case of Sarcoidosis.

12Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Concurrent diagnosis of tuberculosis in patients already diagnosed and treated as sarcoidosis or vice versa is even more challenging and requires demonstration of MTB on smear examination or culture or follow up of many years when final diagnosis becomes clear. Role of Nuclear Imaging tests to distinguish between Sarcoidosis versus Tuberculosis.
GALLIUM 67 SCANSClassical ‘lambda sign’( right paratracheal and bihilar lymphadenopathy) is seen in 72% and
‘panda sign’(parotid and lacrymal gland upatke) in 79% of patients and both being reported in 621%with sarcoidosis. However, they are not specific and also seen HIV, Sjogren syndrome, SLE, lymphoma and after radiation in head and neck malignancies. However, it’s not been studied in tuberculosis and hence its utility to distinguish between the two diseases cannot be stated. Currently, its diagnostic utility is only when combined with SPECT and CT and not routinely recommened.
SOMATOSTATIN ANALOGUES RECEPTOR IMAGINGThis is newer alternative to gallium scans as somatostat in receptors are expressed by
lymphocytes and macrophages and seen in sarcoidosis but also reported in other granulomatous diseases and hence not specific for sarcoidosis [40]. Although abnormal pentetriotide uptake is comparable to gallium but it’s been reported to be more in steroids treated patients [41]. However, abnormal uptake has been reported in other diseases including malignancy hence not entirely specific.
FDG PET SCANSSince granuloma contains activated macrophages and CD4-T lymphoctes and FDG is
transported in to these cells proportional to the disease activity in sarcoidosis but also in other granulomatous diseases [42]. These scans can guide occult affected organs than conventional radiographic methods and may assist in planning most acessible and active site for biopsy. Tuberculosis and lymphomas have similar FDG uptake pattern and pose diagnostic challenge. More profuse lesions in and outside the chest than expected though hints towards sarcoidosis but is not specific and sensitive enough. SUV upatke of >15 seen in sarcoisois has been reported to distinguish it from tuberculosis if mailgnacy has already been ruled out [43]. In doagnosed sarcoidosis with persistent symptoms, FDG PET/CT may show the site and presence of ongoing activity (Figure 5). Also, it helps in distinguishing from burnt out fibrosis from metabolic active disease in lungs [44] and following response to treatment [45].

13Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 5: Atypical Sarcoidosis: a. CXR showing hilar prominence b. Micro nodular random nodules on HRCT started ATT being tuberculin positive c. 2 months later developed massive left sided effusion d CT showed clearance of nodules with mediastinally mphnodes and left pleural
effusion e. medical thoracoscopy revealed multiple large nodules on parietal and visceral pleura. F. biopsy showed NCG which was also demonstrated on EBUS of sub carinal LN, confirming
Sarcoidosis and patient recovered fully on steroids for 6 months.
CONCLUSIONThe tuberculosis versus sarcoidosis debate has continued from ‘medical antiquity’. On
one extreme it has been suggested that sarcoidosis and tuberculosis are two ends of the same spectrum of granulomatous response to a mycobacterial infection, with Lofgren’s syndrome representing the hyper reactive end of the spectrum and pulmonary tuberculosis representing the opposite end. Analogous to leprosy, sarcoidosis can be thought to be the tuberculoid form of the pathological responses to mycobacteria. But there are several counter arguments to these unifying hypotheses. Probably the mycobacteria or its byproducts incite the sarcoid response in genetically predisposed individuals, which in some leads to transient mediastinal lymphadenopathy in some, and fibrosing debliating lung fibrosis in others.
The current era of genomics and proteomics is very interestig with newer markers and cytokines to distinguish between these two diseases at the molecular level would be a future.

14Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Present molecular methods however, do not distinguish dead TB bacilli from actively replicating ones and hence cannot be relied upon to make the diagnosis of TB with certainty in a patient with mediastinal lymphadenopathy, fever and malaise, who presents with a negative PPD response and have possible diagnosis of sarcoidosis. Imaging has contributed a lot in characterization of disease, its extent, activity and severity but yet lacks high diagnostic sensitivity and specificity. Histology showing NCG from one site by itself can not establish the diagnosis and hence in life diagnosis of sarcoidosis is clinico-radiological.
Since, absolute certainty in diagnosis is not possible despite all tests being done to distinguish between these two diseases, our present endevour would focus on reducing diagnostic uncertainty of one disease, so as to make optimal therapeutic decisions. Patience and surveillance in difficult and atypical cases brings answers on long follow ups.
References1. Hutchinson J. Anomalous diseases of skin and fingers: case of livid papillary psoriasis? In: Illustrations of clinical surgery. J & A
Churchill, London. 42-3.
2. Gupta D, Agarwal R, Aggarwal AN, Jindal SK. Molecular evidence for the role of mycobacteria in sarcoidosis: a meta-analysis. Eur Respir J. 2007; 30: 508-516.
3. Perez RL, Rivera-Marrero CA, Roman J. Pulmonary granulomatous inflammation: From sarcoidosis to tuberculosis. Semin Respir Infect. 2003; 18: 23-32.
4. Newman LS. Aetiologies of sarcoidosis. Eur Resp Mon 2005; 32:23–48.
5. Gupta D, Sharma OP. Sarcoidosis. In: Jindal SK, Gupta D, Shankar PS, et al., editors. Text book of pulmonary and critical care medicine. Delhi: Jaypee; 2010. pp. 1188–1216.
6. Hosoda Y, Sasagawa S, Yamaguchi T. Sarcoidosis and tuberculosis: epidemiological similarities and dissimilarities. A review of a series of studies in a Japanese work population (1941–1996) and the general population (1959–1984). Sarcoidosis Vasc Diffuse Lung Dis 2004; 21:85–93.
7. Brett GZ. Epidemiological trends in tuberculosis and sarcoidosis in a district of London between 1958 and 1963. Tubercle. 1965; 46: 413-416.
8. Joshi S, Periwal P, Dogra V, Talwar D. Sarcoidosis as unusual cause of massive pleural effusion. Respir Med Case Rep. 2015; 16: 143-145.
9. Sharma SK, Mohan A, Pande JN, Prasad KL, Gupta AK. Clinical profile, laboratory characteristics and outcome in miliary tuberculosis. QJM. 1995; 88: 29-37.
10. Govender P, Berman JS. The Diagnosis of Sarcoidosis. Clin Chest Med. 2015; 36: 585-602.
11. Woodring JH, Vandiviere HM, Fried AM, Dillon ML, Williams TD. Update: the radiographic features of pulmonary tuberculosis. AJR Am J Roentgenol. 1986; 146: 497-506.
12. Vagal AS, Shipley R, Meyer CA. Radiological manifestations of sarcoidosis. Clin Dermatol. 2007; 25: 312-325.
13. Judson MA. Advances in the diagnosis and treatment of sarcoidosis. F1000Prime Rep. 2014; 6: 89.
14. Rosen Y. Four decades of necrotizing sarcoid granulomatosis: what do we know now? Arch Pathol Lab Med. 2015; 139: 252-262.
15. Moller DR. Potential etiologic agents in sarcoidosis. Proc Am Thorac Soc. 2007; 4: 465-468.
16. Heyll A, Meckenstock G, Aul C, Söhngen D, Borchard F. Possible transmission of sarcoidosis via allogeneic bone marrow transplantation. Bone Marrow Transplant. 1994; 14: 161-164.
17. Brown ST, Brett I, Almenoff PL. Recovery of cell wall-deficient organisms from blood does not distinguish between patients with sarcoidosis and control subjects. Chest 2003; 123:413–417.
18. Shah J R. Tuberculous sarcoidosis. Lung India 2007; 24:83-6.
19. RICKER W, CLARK M. Sarcoidosis; a clinicopathologic review of 300 cases, including 22 autopsies. Am J Clin Pathol. 1949; 19: 725-749.
15Sarcoidosis Diagnosis | www.smgebooks.comCopyright Talwar D.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
20. Longcope WT, Freiman DG. A study of sarcoidosis; based on a combined investigation of 160 cases including 30 autopsies from The Johns Hopkins Hospital and Massachusetts General Hospital. Medicine. 1952; 31: 1–132.
21. Dhooria S, Sehgal IS, Aggarwal AN, Behera D, Agarwal R. Transbronchial lung biopsy with flexible cryoprobe : First case report from India. Lung India. 2016; 33: 64-68.
22. Myers JL, Tazelaar HD. Challenges in pulmonary fibrosis: 6--Problematic granulomatous lung disease. Thorax. 2008; 63: 78-84.
23. Mitchell DN, Mollar DR, Spiro SG, Wells A,editor. Sarcoidosis, 2012 London: Hoddar& Stoughton Ltd.
24. Gupta D, Chetty M, Kumar N, Aggarwal AN, Jindal SK. Anergy to tuberculin in sarcoidosis is not influenced by high prevalence of tuberculin sensitivity in the population. Sarcoidosis Vasc Diffuse Lung Dis. 2003; 20: 40-45.
25. Smith-Rohrberg D, Sharma SK. Tuberculin skin test among pulmonary sarcoidosis patients with and without tuberculosis: it’s utility for the screening of the two conditions in tuberculosis-endemic regions. Sarcoidosis Vasc Diffuse Lung Dis 2006; 23: 130–134.
26. Gupta D, Kumar S, Aggarwal AN. Interferon gamma release assays (QuantiFERON-TB Gold In Tube) in patients of sarcoidosis from a population with high prevalence of tuberculosis infection. Sarcoidosis Vasc Diffuse Lung Dis. 2011; 28: 95–101.
27. Inui N, Suda T, Chida K. Use of the QuantiFERON-TB Gold test in Japanese patients with sarcoidosis. Respir Med. 2008; 102: 313-315.
28. Vyas S, Thangakunam B, Gupta R, Michael JS, Christopher DJ. Interferon gamma release assay and tuberculin skin test positivity in sarcoidosis. Lung India. 2015; 32: 91-92.
29. Hörster R, Kirsten D, Gaede KI, Jafari C, Strassburg A. Antimycobacterial immune responses in patients with pulmonary sarcoidosis. Clin Respir J. 2009; 3: 229-238.
30. Reich JM. On the nature of sarcoidosis. Eur J Intern Med. 2012; 23: 105-109.
31. Berthet FX, Rasmussen PB, Rosenkrands I. A Mycobacterium tuberculosis operon encoding ESAT-6 and a novel low-molecular-mass culture filtrate protein (CFP-10). Microbiology 1998; 144: 3195–3203.
32. Chen ES, Wahlström J, Song Z, Willett MH, Wikén M. T cell responses to mycobacterial catalase-peroxidase profile a pathogenic antigen in systemic sarcoidosis. J Immunol. 2008; 181: 8784-8796.
33. Oswald-Richter K, Sato H, Hajizadeh R. Mycobacterial ESAT-6 and katG are recognized by sarcoidosis CD4þ T cells when presented by the American sarcoidosis susceptibility allele, DRB1#1101. J Clin Immunol 2010; 30: 157–166.
34. Lieberman J. Elevation of serum angiotensin-converting-enzyme (ACE) level in sarcoidosis. Am J Med. 1975; 59: 365-372.
35. Winterbauer RH, Belic N, Moores KD. Clinical interpretation of bilateral hilar adenopathy. Ann Intern Med. 1973; 78: 65-71.
36. Koth LL, Solberg OD, Peng JC, Bhakta NR, Nguyen CP. Sarcoidosis blood transcriptome reflects lung inflammation and overlaps with tuberculosis. Am J Respir Crit Care Med. 2011; 184: 1153-1163.
37. Maertzdorf J, Weiner J, Mollenkopf HJ, TBornot TB. Network, Bauer T, Prasse A. Common patterns and disease-related signatures in tuberculosis and sarcoidosis. Proc Natl Acad Sci U S A. 2012; 109: 7853-7858.
38. JAMES DG, THOMSON AD. The course of sarcoidosis and its modification by treatment. Lancet. 1959; 1: 1057-1061.
39. Judson MA, Baughman RP, Teirstein AS. Defining organ involvement in Sarcoidosis: the ACCESS proposed instrument. ACCESS Research Group. A case control etiologic study of Sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2014; 31: 19-27
40. Sulavik SB, Spencer RP, Palestro CJ, Swyer AJ, Teirstein AS. Specificity and sensitivity of distinctive chest radiographic and/or 67Ga images in the noninvasive diagnosis of sarcoidosis. Chest. 1993; 103: 403-409.
41. Lebtahi R, Crestani B, Belmatoug N, Daou D, Genin R. Somatostatin receptor scintigraphy and gallium scintigraphy in patients with sarcoidosis. J Nucl Med. 2001; 42: 21-26.
42. Lewis PJ, Salama A. Uptake of fluorine-18-fluorodeoxyglucose in sarcoidosis. J Nucl Med. 1994; 35: 1647-1649.
43. Mostard RL, van Kroonenburgh MJ, Drent M. The role of the PET scan in the management of sarcoidosis. Curr Opin Pulm Med. 2013; 19: 538-544.
44. Nair V, Prajapat D, Talwar D. Sarcoidosis and multiple myeloma: Concurrent presentation of an unusual association. Lung India. 2016; 33: 75-78.
45. Guleria R, Jyothidasan A, Madan K, Mohan A, Kumar R. Utility of FDG-PET-CT scanning in assessing the extent of disease activity and response to treatment in sarcoidosis. Lung India. 2014; 31: 323-330.