Pulmonary Sarcoidosis

of 22
-
Upload
veeru-kuppast -
Category
Documents
-
view
16 -
download
0
description
Pulmonary Sarcoidosis
Transcript of Pulmonary Sarcoidosis
-
Pulmonary SarcoidosisJoseph P. Lynch, III, M.D.,1 Yan Ling Ma, M.D.,2 Michael N. Koss, M.D.,2
and Eric S. White, M.D.3
ABSTRACT
Sarcoidosis, a granulomatous disorder of unknown etiology, characteristicallyinvolves multiple organs. However, pulmonary manifestations typically dominate. Chestradiographs are abnormal in 85 to 95% of patients. Abnormalities in pulmonary functiontests are common and may be associated with cough, dyspnea, and exercise limitation.However, one third or more of patients are asymptomatic, with incidental abnormalities onchest radiographs. The clinical course and expression of pulmonary sarcoidosis are variable.Spontaneous remissions occur in nearly two thirds of patients. The course is chronic in upto 30% of patients. Chronic pulmonary sarcoidosis may result in progressive (sometimeslife-threatening) loss of lung function. Fatalities ascribed to sarcoidosis occur in 1 to 4% ofpatients. Although the impact of treatment is controversial, corticosteroids may be highlyeffective in some patients. Immunosuppressive, cytotoxic, or immunomodulatory agentsare reserved for patients failing or experiencing adverse effects from corticosteroids. Lungtransplantation is a viable option for patients with life-threatening disease failing medicaltherapy.
KEYWORDS: Pulmonary sarcoidosis, nonnecrotizing granuloma, necrotizing sarcoid
angiitis
The spectrum of sarcoidosis is protean, andvirtually any organ can be involved.13 Multisysteminvolvement is characteristic, but pulmonary involve-ment usually dominates.26 Skin, eyes, and peripherallymph nodes are each involved in 15 to 30% of pa-tients.13,6 Clinically signicant involvement of spleen,liver, heart, central nervous system (CNS), bone, orkidney occurs in 2 to 7% of patients.1 Asymptomaticinvolvement of these organs is far more common. Thisarticle limits discussion to pulmonary manifestations ofsarcoidosis.5
PULMONARY SARCOIDOSISAbnormalities on chest radiographs are detected in 85 to95% of patients with sarcoidosis.511 Cough, dyspnea, orbronchial hyperreactivity may be prominent in patientswith signicant endobronchial or pulmonary parenchy-mal involvement.5,12 However, 30 to 60% of patientswith sarcoidosis are asymptomatic, with incidental nd-ings on chest radiographs.5,10,13,14 The clinical course isheterogeneous. Spontaneous remissions (SRs) occur innearly two thirds of patients but the course is chronicin 10 to 30%.711,15 Chronic, progressive pulmonary
1Division of Pulmonary, Critical Care Medicine, and Hospitalists,Department of Internal Medicine, The David Geffen School ofMedicine at UCLA, Los Angeles, California; 2Department of Pathol-ogy, Keck School of Medicine, University of Southern California(USC) Los Angeles, California; 3Division of Pulmonary and CriticalCare Medicine, Department of Internal Medicine, University ofMichigan Medical School, Ann Arbor, Michigan.
Address for correspondence and reprint requests: Joseph P. Lynch,III, M.D., The David Geffen School of Medicine at UCLA, Division
of Pulmonary, Critical Care Medicine, and Hospitalists, 10833 LeConte Ave., Rm. 37-131 CHS, Los Angeles, CA 90095. E-mail:jplynch@ mednet.ucla.edu.
Sarcoidosis: Evolving Concepts and Controversies; Guest Editors,Marc A. Judson, M.D., Michael C. Iannuzzi, M.D.
Semin Respir Crit Care Med 2007;28:1;5374. Copyright# 2007by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York,NY 10001, USA. Tel: +1(212) 584-4662.DOI 10.1055/s-2007-970333. ISSN 1069-3424.
53
-
sarcoidosis may cause inexorable loss of lung functionand destruction of the lung architecture.5,16 Fatality ratesascribed to sarcoidosis range from 1 to 5%.711,13,14,1719
British investigators retrospectively reviewed 818 pa-tients with sarcoidosis (both treated and untreated).7
Forty-eight patients (5%) died, usually because ofchronic respiratory failure or cor pulmonale.20 A recentepidemiological study in the United Kingdom identied1019 cases of sarcoidosis between 1991 and 2003.20
Mortality rates at 3 and 5 years for sarcoid patientswere 5% and 7%, respectively, compared with 2% and 4%among age- and gender-matched controls without sar-coidosis. Causes of death were not reported. Swedishinvestigators followed 505 patients with sarcoidosis forup to 15 years.10 Thirty patients died (6%), but only fourdeaths were directly attributed to sarcoidosis (< 1%mortality). Huang et al reported 2.8% mortality among1090 sarcoid patients in Europe.17 A review of 775 casesof sarcoidosis in Japan reported < 1% mortality as adirect result of sarcoidosis.21 In the United States,mortality rates due to sarcoidosis were < 1% in non-referral settings11,13,14 but were higher in referral centers(likely reecting a bias selecting for more severecases).4,19,2225 In the United States, 87% of deathsattributed to sarcoidosis were secondary to pulmonarycomplications.26 By contrast, in Japan, 77% of deathsresulted from cardiac involvement.27
CLINICAL FEATURES OF PULMONARYSARCOIDOSISIn contrast to idiopathic pulmonary brosis (IPF), phys-ical ndings are usually minimal or absent in pulmonarysarcoidosis. Crackles are present in fewer than 20% ofpatients with sarcoidosis, even when radiographic inl-trates are extensive.5 Clubbing, observed in 25 to 50% ofpatients with IPF,28 is rare in sarcoidosis.5 Fatigue29 andimpaired quality of life (QOL)30 are far more commonamong patients with sarcoidosis compared with healthycontrols. The impact of sarcoidosis on QOL is discussed
in depth elsewhere in this issue by Drs. De Vries andDrent.
CHEST RADIOGRAPHIC FEATURESIN SARCOIDOSISBilateral hilar lymphadenopathy (BHL), the classicradiographic feature of sarcoidosis, is present in nearlythree quarters of patients; right paratracheal lymphnodes may be involved concomitantly.5,711 Enlarge-ment of left paratracheal, paraaortic, and subcarinallymph node groups may be detected by computed tomo-graphic (CT) scans31,32 but are not usually evident onplain chest radiographs.5 Unilateral hilar lymphadenop-athy on CT is uncommon (< 10%).33 Pulmonary paren-chymal inltrates (with or without BHL) are present in20 to 50% of patients with sarcoidosis.5,6,10 Inltratesmay be patchy or diffuse, but preferentially involve theupper and mid lung zones.5,34 Reticulonodular inl-trates, macroscopic nodules, consolidation, or masslikelesions may be evident.5 When pulmonary brosis oc-curs, volume loss, hilar retraction, and coarse linearbands may be observed on chest radiographs. Withadvanced brocystic sarcoidosis, large bullae,35,36 cysticradiolucencies,37,38 distortion,34 mycetomas,39,40 orbronchiectasis41 may be observed.
RADIOGRAPHIC CLASSIFICATIONSCHEMAThe chest radiographic staging system developed morethan 4 decades ago continues to have prognostic value.9
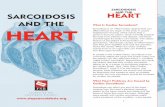
This classication schema denes the following stages:stage 0 (normal; Fig. 1); stage I (BHL without pulmo-nary inltrates; Fig. 2); stage II (BHL plus pulmonaryinltrates; Fig. 3); stage III (parenchymal inltrateswithout BHL; Fig. 4). Radiographic stage IV sarcoido-sis, encompassing extensive brosis with distortion orbullae, is not universally accepted (see Table 1). Theincidence of radiographic stages differs according to
Figure 1 Stage 0 radiographic sarcoidosis. This normal chest x-ray may be observed in 5 to 15% of cases.
54 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
geographic regions, ethnicity, and referral bias. Stage I ismost common in most series, but signicant variabilityexists (see Table 2). Most studies from Scandinavia citeda striking predominance of radiographic stage I and IIdisease,8,10 whereas some studies from the United Statesand British Isles cite a disproportionate representation ofradiographic stage III and IV disease.23,25
Although individual exceptions exist, the prog-nosis is best with radiographic stage I; intermediate withstage II; and worst with stage III or IV. SRs occur in 60to 90% of patients with stage I disease; in 40 to 70% withstage II; 10 to 20% with stage III; and 0% with stageIV.710,19,24,42 In a sentinel study in the United King-dom, Scadding followed patients with sarcoidosis for 5years.9 At the end of follow-up, 31 of 32 patients (97%)with stage I disease were asymptomatic, whereas only58% of stage II and 25% of stage III patients wereasymptomatic.9 In the United States, Siltzbach noted
similar ndings.24 In his long-term follow-up of 244patients with sarcoidosis (both treated and untreated),chest radiographs normalized in 54% of patients withstage I disease but in only 31% with stage II and 10%with stage III.24 Importantly, none of 110 patients withstage I died, whereas mortality rates were 11% with stageII and 18% with stage III disease. British investigatorsfollowed 818 patients with sarcoidosis (both treated anduntreated) and observed higher rates of radiographicresolution with stage I (59%) compared with stage II(39%) or stage III (38%) sarcoidosis.7 Swedish investi-gators followed 505 patients with sarcoidosis (bothtreated and untreated) for up to 15 years.10 At 5 yearfollow-up (both treated and untreated patients), chestradiographs had normalized in 82% of patients withstage I sarcoidosis; 68% with stage II; 37% with stageIII.10 Among 308 patients with stage I disease, 29 (9%)progressed to stage II and only ve (1.6%) progressed to
Figure 2 Stage I radiographic sarcoidosis. Bilateral hilar lymphadenopathy with clear lung elds.
Figure 3 Stage II radiographic sarcoidosis. Combined hilar lymphadenopathy and upper lung zone predominant interstitial inltrates.
PULMONARY SARCOIDOSIS/LYNCH ET AL 55
-
stage III or IV. Danish investigators followed 210patients with sarcoidosis for 1 to 10 years (both treatedand untreated).8 Among 116 patients with stage I dis-ease, chest radiographs normalized in 57%; only10 progressed to stage II; none developed stage III.Among patients with stage II, chest radiographs nor-malized in 48%; only 12% worsened. By contrast, chestradiographs normalized in only one of 10 (10%) withstage III sarcoidosis. The investigators noted that thecourse of the disease was usually dictated within the rst1 to 2 years of presentation. The vast majority (85%) ofall SRs occurred within 2 years of presentation.8 Amongpatients who remained in stage II after 2 years ofobservation, chest radiographs eventually normalized inonly 12% and worsened in 30%.8 Late relapses were rare,however, in patients exhibiting stability for the rst 2years. Only one of 63 patients (1.6%) with stage I atpresentation progressed after the second year.8 Otherstudies noted that SR occurs in 16 to 39% of patientswithin 6 to 12 months from the onset of symptoms.4244
Further, among patients who are undergoing SR, therate of late relapse is low (< 10%).4244 Genetic anddemographic factors inuence prognosis. In a study fromNew South Wales, chest radiographs normalized in
112 of 150 (75%) patients presenting with stage I or IIsarcoidosis.45 In a cohort of Japanese patients withsarcoidosis, chest radiographs cleared within 3 years in68%.46 In a cohort of 193 Spanish patients with sarcoi-dosis, chest radiographs had normalized in 78% within
Table 2 Distribution of Chest Radiographic Stages inSarcoidosis
Country, Year,# patients
X-ray Stage
0(%) I(%) II(%) III(%) IV(%)*
Sweden, 1984
(n505)103 61 25 10 1
Denmark, 1982
(n243)80.4 55 40 4.5 ND
British Isles, 2000
(n212)459 51 20 15 5
British Isles, 1983
(n818)714 56 18 11 ND
Finland, 2000
(n437)**0 44 43 13 0.4
Japan, 2000
(n457)**0 67 27 5 0
USA 1967
(n244)**0 45 39 16 ND
USA 1997
(n337)24,25,488 45 29 17 ND
USA, 1994
(n98)4420 18 27 10 25
USA 1985
(n86)1310 49 21 20 ND
USA 2001
(n736)68 40 37 10 5
*Stage IV not universally adopted.**Only included pulmonary sarcoidosis.ND, not described.
Table 1 Chest Radiographic Staging System forSarcoidosis*
Radiographic Stage Radiographic Findings
Stage 0 Normal chest x-ray (Fig. 1)
Stage I Bilateral hilar adenopathy (BHL)
Stage II BHL plus parenchymal inltrates
Stage III Parenchymal inltrates without BHL
Stage IV Irreversible scarring and distortion
*Adapted from Scadding.9
Figure 4 Stage III/IV radiographic sarcoidosis. Note the upper lung zone volume loss, upward retraction of the hilae, and tenting of thehemidiaphragms.
56 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
2 years.47 However, persistent inltrates at 2 yearspredicted a chronic or persistent course.47 In the UnitedStates, 215 patients with sarcoidosis were followedprospectively for 2 years.15 In most patients, pulmonaryfunction, x-ray stage, and dyspnea scale did not changeduring the 2 year period. Only 11 of 176 (6%) with stage0, I, or II disease progressed to stage III or IV over the2 year follow-up period. Spirometry worsened in 12%.Involvement of additional organs occurred in 50 patients(23%) during that time frame.15
Differing prognoses among studies may reectethnic, geographic, or referral biases.48 Pietinalho et alfollowed a large cohort of 437 Finnish and 457 Japanesepatients for 5 years.48 Chest radiographs normalizedwithin 1 year in 46% of Japanese but in only 16% ofFinnish patients. After 5 years, the rates of radiographicresolution were 73% and 40%, respectively (p< .001).During the 5 year period, 43 of 309 (14%) Japanesepatients and 28 of 142 (20%) Finnish patients withinitial stage I lesions progressed to higher stages inl-trates. At 5 years, among patients with initial stage IIdisease, chest radiographs had normalized in 73% ofJapanese and 36% of Finnish patients. Among patientswith initial stage III disease, chest radiographs hadnormalized by 5 years in 35% of Japanese and 24% ofFinnish patients, respectively.48
The prognosis of sarcoidosis is distinctly worseamong African Americans.4,23,25 Gottlieb et al studied337 patients with sarcoidosis, 118 of whom achieved SR(36%). Interestingly, only 8% of patients who had SRexperienced late relapse, whereas relapse rates were> 74% among patients with corticosteroid-induced re-missions.25 Importantly, sustained remissions wereachieved in 50% of Caucasians but only 20% of AfricanAmericans (p .01).
These various studies emphasize that the courseof sarcoidosis is heterogeneous and variable amongethnic groups. Identifying candidates for therapeuticintervention requires careful follow-up of clinical,radiographic, and physiological parameters. Treatment(discussed later) should be offered to patients withsevere or progressive pulmonary or extrapulmonarydysfunction.
ADDITIONAL PROGNOSTIC FACTORSAs has been mentioned, the clinical course and prognosisof sarcoidosis is inuenced by ethnic and genetic factors.Black race is associated with a higher rate of chronicprogressive disease, worse long-term prognosis, extrap-ulmonary involvement, and higher risk of relap-ses.4,7,15,22,23,25 Analysis of a cohort of 736 sarcoidpatients in the United States noted that women weremore likely to have eye and neurological involvementand erythema nodosum, whereas men were more likelyto be hypercalcemic.6 Black subjects were more likely to
have eye, liver, bone marrow, extrathoracic lymph node,and skin involvement (other than erythema nodosum).Derangements in calcium metabolism were more com-mon among white subjects.6 The inuence of humanleukocyte antigen (HLA) markers and prognosis iscontroversial.2,4952 HLA-B8 is associated with acuteinammatory features and a favorable prognosis,whereas HLA-B13 is often associated with a progressiveand protracted course.52 Some HLA patterns are asso-ciated with a good prognosis in Japanese but a poorprognosis in Italians.50,51 The inuence of genetics onprevalence and clinical expression of sarcoidosis is dis-cussed elsewhere in this issue by Dr. Iannuzzi.
Clinical features may have prognostic value.Lofgrens syndrome (i.e., BHL, erythema nodosum,polyarthritis, and fever) portends an excellent prognosis,with high rates (> 85%) of SR.7,15,42,53 Lofgrens syn-drome occurs in 30% of Caucasians with sarcoidosis, in10% of Asians, but is rare in blacks.7,22,25 Clinical factorsassociated with a worse prognosis in sarcoidosis includeage onset > 40 years7,47; hypercalcemia7; extrathoracicdisease7,22; lupus pernio7; splenomegaly47; pulmonaryinltrates on chest radiograph7,47; chronic uveitis, cysticbone lesions, nasal mucosal sarcoidosis7; lower annualfamily income.15
COMPUTED TOMOGRAPHIC SCANSHigh-resolution computed tomographic (HRCT) chestscans are superior to conventional chest radiographs indelineating parenchymal, mediastinal, and hilar struc-tures, depicting parenchymal details, and discriminatinginammation from brosis.31,34,54,55 Characteristic fea-tures of sarcoidosis on CT include mediastinal and/orhilar lymphadenopathy; nodular opacities and micronod-ules along bronchovascular bundles; predilection for midand upper lung zones; an axial distribution; pleural orsubpleural nodules; septal and nonseptal lines; conuentnodular opacities with air-bronchograms (i.e., consolida-tion); and ground-glass opacities (GGOs).34,56 Architec-tural distortion, hilar retraction, brous bands,bronchiectasis, cystic radiolucencies, bullae, and enlargedpulmonary arteries may be observed with advanced dis-ease.32,34,57,58 Multiple CT patterns or features may bepresent in individual patients and may evolve over time.34
Findings on initial CT scan have limited prognosticvalue, but certain CT features may discriminate activeinammation from brosis. Nodules, GGOs, consolida-tion, or alveolar opacities suggest granulomatous inam-mation and may reverse with therapy.59,60 By contrast,honeycomb change, cysts, coarse broad bands, distortion,or traction bronchiectasis indicate irreversible bro-sis.57,61 Despite the enhanced accuracy of CT, routineCT is not necessary or cost-effective in the managementof sarcoidosis.62 Chest CT scans may be helpful inthe following circumstances: atypical clinical or chest
PULMONARY SARCOIDOSIS/LYNCH ET AL 57
-
radiographic ndings; to detect specic complications ofthe lung disease (e.g., bronchiectasis, aspergilloma, pul-monary brosis, superimposed infection or malignancy);normal chest radiographs, but a clinical suspicion forsarcoidosis.3,34 The salient features and role of CT in themanagement of sarcoidosis are addressed elsewhere inthis issue by Dr. Wells and colleagues.
PULMONARY FUNCTION TESTSIN SARCOIDOSISAbnormalities in pulmonary function tests (PFTs) arepresent in 20% of patients with radiographic stage Isarcoidosis and in 40 to 80% of patients with parenchy-mal inltrates (stages II, III, or IV).5,7,8,6366 A restric-tive defect with reduced lung volumes [e.g., vital capacity(VC) and total lung capacity (TLC)] is characteristic.The diffusing capacity for carbon monoxide (DLCO) isthe most sensitive of the PFT parameters,66 but thedegree of impairment is less severe in sarcoidosis than inIPF.5,67 Even when chest radiographs are normal, forcedvital capacity (FVC) or DLCO is reduced in 15 to 25%and 25 to 50% of patients, respectively.63,68 Oxygenationis preserved until late in the course of sarcoidosis.5
Airow obstruction [e.g., reduced forced expira-tory volume in 1 second (FEV1) and expiratory owrates] occurs in 30 to 50% of patients with pulmonarysarcoidosis.64,66,6870 Airow obstruction may be causedby multiple mechanisms, including narrowing of bron-chial walls (via granulomatous lesions or brotic scar-ring),7173 peribronchiolar brosis,74 airway distortioncaused by pulmonary brosis,64,75 compression by en-larged lymph nodes,5 small airways disease,68,76,77 andbronchial hyperreactivity.12,66 One study of 107 patientswith newly diagnosed sarcoidosis noted a decreasedFEV1:FVC ratio in 61 patients (57%).
68 The DLCOwas reduced in 29 (27%); only seven (6%) manifestedrestriction.68 Airow obstruction was more frequentwith worsening radiographic stage. Another study of18 sarcoid patients (all of whom had reduced lungvolumes or DLCO) found that airways obstruction waspresent in all 18 when sensitive tests were employed(e.g., frequency dependence of compliance, airway re-sistance, closing volumes).77 Airow obstruction is sug-gested by CT showing bronchial mural thickening, smallairway narrowing, or patchy air trapping (mosaic patternof perfusion).7880 Patients with advanced pulmonarysarcoidosis (radiographic stages III or IV) may exhibitsevere decrements in FEV1:FVC.
64,81 Additionally, in-creased airway hyperreactivity in response to methacho-line is common in patients with sarcoidosis.8284
Clinically, this may manifest as chronic, hacking cough.In one study, 50% of patients with stage I or IIsarcoidosis exhibited bronchial hyperreactivity followingmethacholine challenge.12 A more recent series citedbronchial hyperreactivity in 46 of 80 (58%) sarcoid
patients.84 Bronchial hyperreactivity likely reects gran-ulomatous inammation involving the bronchial mu-cosa.71 Clinical bronchiectasis is a rare complication ofstage IV sarcoidosis.85
Impaired respiratory muscle function (RMF) maycontribute to dyspnea or exercise limitation in patientswith sarcoidosis.66 In a cohort of 18 sarcoid patients withnormal PFTs, inspiration muscle endurance (IME) wasimpaired compared with healthy controls, and correlatedwith symptoms and impaired QOL.86 French investi-gators studied 34 sarcoid patients and 19 controls. Reduc-tions in IME were noted in the sarcoid patients andcorrelated with impairments in health-related quality oflife (HRQOL).87 Baydur et al measured RMF by mouthinspiratory muscle pressure (PImax) and expiratory musclepressure (PEmax) in 36 sarcoid patients and 25 controls.
88
Signicant linear relationships were found between in-creasing dyspnea and decreasing RMF. Interestingly,dyspnea did not correlate with lung volumes or DLCO.
Alterations in cardiopulmonary exercise tests(CPETs) have been noted in 28 to 47% of patientswith sarcoidosis.75,8991 Typical ndings include venti-latory limitation or increased dead space volume/tidalvolume (VD/VT) or widened alveolar-arterial O2 (A-aO2) gradient with exercise.
75,89 CPET may be abnormalwhen static PFTs are normal.75,85 Miller et al performedCPET in 30 sarcoid patients with normal spirometry;DLCO was normal in 13.
75 Maximal exercise testingelicited ventilatory abnormalities in 14 (47%)75 Abnor-mal CPET (e.g., excessive ventilation to oxygen con-sumption and abnormal VD/VT) were noted in eight ofnine with a low DLCO compared with 11 of 21 with anormal DLCO. Widened A-a O2 gradient was observedprimarily in patients with low DLCO. Delobbe et alperformed CPETs in 19 sarcoid patients with normalresting PFTs (including DLCO). Compared with age-and sex-matched healthy sedentary controls, sarcoidpatients displayed reductions in maximal workload,VO2 max, tidal volume (VT), heart rate, and increasedVD/VT with exercise.
85 Another study of 20 patientswith mild pulmonary sarcoidosis noted abnormalities onCPET in nine patients (45%).89 VO2 at the anaerobicthreshold was low, and/or the rate of increase of VO2was abnormal relative to work rate or heart rate, suggest-ing a defect in cardiocirculatory function. Resting andexercise echocardiography revealed normal left ventri-cular function in all patients, but right ventriculardysfunction or hypertrophy was evident in ve. Thusabnormal response of VO2 during exercise may reectsubclinical right heart dysfunction89 or an impaired heartrate response to exercise.85
Exercise-induced desaturation correlates with re-ductions in DLCO.
75,90,92,93 In a series of 32 patientswith pulmonary sarcoidosis, DLCO < 55% had a highsensitivity (85%) and specicity (91%) in predictingexercise-induced desaturation.90 Lamberto et al reported
58 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
that alveolar membrane diffusing capacity (Dm) andDLCO were the strongest predictors of gas exchangeabnormalities during exercise.94 In contrast, lung volumesand expiratory ow rates did not correlate with exercisegas exchange.94 Arterial desaturation with exercise is rarein patients with radiographic stage I disease or preservedDLCO.
93 Arterial desaturation and DLCO correlate withthe extent and severity of sarcoidosis as assessed by CT.92
Although CPET is more sensitive than staticPFTs in predicting work and exercise capacity, thepractical value of CPET is limited. Spirometry andoximetry are usually adequate to follow the course ofthe disease. For patients with more severe disease, non-invasive 6 minute walk tests provide additional quanti-tative data.
Physiological aberrations correlate only roughlywith histological severity of the disease.74,9598 Earlystudies employing quantitative morphometric analysesnoted that physiological parameters failed to predict thehistologic severity of the disease (on open-lung biopsyspecimens).74,96,97 Although PFTs were more seriouslyderanged among patients with advanced brosis, thedegree of overlap was considerable. Further, physiolog-ical parameters cannot discriminate alveolitis (that mightbe amenable to therapy) from irreversible brosis.97,98
The extent of pulmonary physiological impair-ment correlates with severity of disease by chest radio-graphs99102 or CT scans,31,32,101,103 but correlations areimprecise. Semiquantitative scoring systems improvethe correlations between physiological parameters andHRCT.101,103105 In a seminal study, Bergin noted thatsemiquantitative scores on CT correlated inversely withFVC (r0.81) and to a lesser extent, with DLCO(r0.49).31 Drent and colleagues found that HRCTcorrelated with FEV1, FVC, DLCO, paO2max (maximalpartial pressure for oxygen), and was more sensitive thanchest radiographs in detecting pulmonary disability orabnormal gas exchange.106 However, given the imprecisecorrelations between CT and physiological parameters,direct measurement of PFTs is critical to assess theextent and degree of pulmonary functional impairment.
Specic CT ndings (e.g., thickening or irregu-larity of bronchovascular bundles, intraparenchymalnodules, septal and nonseptal lines, and focal pleuralthickening) correlate with functional impairment,whereas other features (e.g., focal consolidations,GGOs, or enlarged lymph nodes) are less important.106
The pattern of CT may reect underlying pathology.Hansell et al noted that a reticular pattern on HRCTcorrelated inversely with FVC, FEV1, FEV1:FVC, andDLCO.
107 Others afrmed that reticular and broticabnormalities on HRCT correlated modestly with phys-iological aberrations, whereas mass lesions or conuencedid not.104 Honeycomb change is most often associatedwith restriction and low DLCO, whereas bronchial dis-tortion is often associated with reduced expiratory ow
rates.58 CT patterns may evolve over time. A study ofserial CT in 40 patients with pulmonary sarcoidosisfound several distinctive evolutionary patterns.108 Mac-roscopic nodules often disappeared or decreased in size atfollow-up. In some patients, GGOs and consolidationresolved, but in others these patterns evolved into honey-combing and were associated with a decline in FVC. Aconglomeration pattern shrank and evolved into bron-chial distortion and a decline in FEV1:FVC. The salientfeatures and signicance of CT are discussed in detailelsewhere in this issue by Dr. Wells and colleagues andwill not be further addressed here.
INFLUENCE OF PULMONARY FUNCTIONON PROGNOSISPhysiological parameters at the onset do not predict long-term outcome in patients with sarcoidosis,63,109111 butmortality is higher among patients with severe physio-logical impairment.16 Sequential studies are important tofollow the course of the disease and assess response totherapy. Several studies found that VC improves morefrequently than DLCO,
63,112,113 TLC,114 or arterial oxy-genation.98 Changes in VC and DLCO are usually con-cordant; discordant changes occur in fewer than 5% ofpatients.15,98 A prospective study in the United States of193 sarcoid patients cited excellent concordance betweenchanges in FVC and FEV1.
15 Changes in FVC andFEV1 were concordant (in the same direction) in 155patients (80.3%) but were never discordant (oppositedirections). In a previous study, measurement of oxygensaturation at rest or during exercise was no more sensitivethan VC or DLCO among patients with sarcoidosis.
98
Given the variability of DLCO,63 and the expense of
obtaining lung volumes, spirometry and ow-volumeloops are the most useful and cost-effective parametersto follow the course of pulmonary sarcoidosis. Additionalstudies such as DLCO, TLC, or gas exchange have a rolein selected patients. Criteria for assessing response orimprovement have not been validated. Most investigatorsdene a change in FVC > 10 to 15% or DLCO > 20% assignicant.98,115 Responses to therapy are usually evidentwithin 6 to 12 weeks of initiation of therapy.63,116
LABORATORY FEATURESSerum angiotensin-converting enzyme (SACE) is in-creased in 30 to 80% of patients with sarcoidosis andmay be a surrogate marker of total granuloma bur-den.5,117 False-positives are noted in fewer than 20% ofpatients with other pulmonary disorders. However,SACE may be normal in patients with active disease.We believe SACE provides ancillary information whenthe activity of sarcoidosis is uncertain on clinical grounds.However, SACE should not be used in isolation todictate therapeutic interventions. Historically, the
PULMONARY SARCOIDOSIS/LYNCH ET AL 59
-
Kveim-Siltzbach skin test was used to diagnose sarcoi-dosis.118 We see no current role for the routine use of theKveim-Siltzbach skin test.2
PATHOGENESIS OF SARCOIDOSISSarcoidosis is characterized by accumulations of acti-vated T cells and macrophages at sites of disease activity(such as the lung). Sarcoid T lymphocytes belong to thehelper CD4 phenotype; rarely, CD8 lymphocytes pre-dominate.119,120 Interactions between alveolar macro-phages, CD4 T-helper (Th) cells, and a Th1-cytokinenetwork drive the granulomatous process.2 Lung T cellsfrom patients with sarcoidosis spontaneously release Th1cytokines such as interferon (IFN)-g121 and interleukin(IL)-2.122 IL-12, a product of activated macrophages,upregulates the development of Th1 cells and ampliesthe Th1 response (especially IFN-g).
123 Interleukin-18acts synergistically with IL-12 to induce release fromTh1 cells and enhances cytotoxicity of T cells.124 In-creased serum and bronchoalveolar lavage uid (BALF)levels of IL-18 were noted in patients with sarcoidosisand may be a surrogate marker of disease activity.125
Sarcoid alveolar macrophages release other cytokinesthat drive the lymphocytic alveolitis, including tumornecrosis factor (TNF)-a,126 IL-6,127 IL-15,128 mono-cyte chemotactic protein-1 (MCP-1),120 RANTES(regulated upon activation normal T cell expressed andsecreted),129 and macrophage inammatory protein(MIP)-1a and MIP-1b.130 The CC chemokines MIP-1a and MIP-1b recognize CCR5 as a cellular receptorin activated T cells and alveolar macrophages.130 MIP-1b may be important in the early (inammatory) phasesof sarcoidosis, whereas MIP-1a likely participates inlater (brotic) phases.130 CCR5 is expressed at highlevels in CD4 Th1 lymphocytes and induces increasedproduction and release of IL-1 and IFN-g.130 Down-regulation of CCR5 in advanced (brotic) stages ofsarcoidosis may indicate switch to Th2 phenotype, whichmay enhance brosis.131 Later stages of pulmonarysarcoidosis (stage III or IV) are associated with pro-gressive increases in neutrophils and eosinophils.130
Further, there is a relative reduction in CD4 and increasein CD8 lymphocytes in stage III as compared with stageI sarcoidosis.130,132.133 Other chemokines that contrib-ute to recruiting leukocytes in pulmonary sarcoidosisinclude RANTES (CCL5),129 monocyte chemotacticprotein-1 (MCP-1) (CCL2),134 the novel chemokinesingle cysteine motif (SCM)-1a (XCL-1),134 and inter-feron-g inducible protein 10 (CXCL10).135
Factors that modulate or downregulate the gran-ulomatous response have not been fully elucidated. In-creased levels of TNF-receptors (TNF-R) have beennoted in plasma and BALF in patients with sarcoido-sis.136,137 Increased expression of IL-13 (a Th2 cytokine),by sarcoid alveolar macrophages138 may attenuate or
abrogate the granulomatous response. Increased expres-sion of IL-10 in sarcoid bronchoalveolar lavage (BAL)cells has been noted in some,139,140 but not all,138 studies.Further, genetic polymorphisms may inuence the clini-cal expression and evolution of the disease. In Scandina-vian patients with pulmonary sarcoidosis, lung T cellsexpress T cell receptor (TCR) AV2S3 and the humanleukocyte antigen (HLA)-DR17 alleles.141 These lung-restricted AV2S3T cells correlated with the CD4:CD8ratio, acute disease onset, and a good prognosis.141 TheseAV2S3T cells may have a protective role against aputative sarcoid antigen. In a cohort of Dutch patients,polymorphisms in C-C chemokine receptor 2 wereassociated with Lofgrens syndrome but were notobserved in healthy controls or sarcoid patients withoutLofgrens syndrome.142 Other investigators found thatcertain HLA haplotypes were associated with acute onsetand short duration of disease and were protected againstpulmonary disease progression in Dutch and UnitedKingdom sarcoidosis patients.143,144 The inuence ofgenetics on disease susceptibility, clinical expression,and evolution of the sarcoid lesions is discussed in detailin this issue by Dr. Iannuzzi
BRONCHOALVEOLAR LAVAGE FLUID INSARCOIDOSISBAL has provided signicant insights into the patho-genesis of sarcoidosis.145 BAL in sarcoidosis demon-strates increased numbers of activated lymphocytes(typically CD4T cells), alveolar macrophages, andmyriad proinammatory cytokines and mediators.145
BAL lymphocytosis is present in > 85% of patientswith pulmonary sarcoidosis; granulocytes are normal orlow.145148 The CD4:CD8 ratio is increased in 50 to 60%of patients with sarcoidosis.145 In late phases of sarcoi-dosis, neutrophils or mast cells or both may be in-creased.82,100,149151 BAL cell proles are not specicfor sarcoidosis, but they narrow the differential diagno-sis.145,146,148 Importantly, BAL cell proles fail to predictprognosis or responsiveness to corticosteroid ther-apy.2,132,145,147,152,153 Similarly, initial BAL CD4:CD8ratios do not consistently predict outcome or responsive-ness to therapy.145 In fact, marked CD4 lymphocyticalveolitis is characteristic of Lofgrens syndrome, whichremits spontaneously in more than 85% of pa-tients.132,147,154 BAL is expensive and invasive, and wesee no clinical role for BAL in determining the need fortherapy or following response.
RADIONUCLIDE TECHNIQUESRadionuclide techniques [e.g., 67gallium citrate,155,156
scintigraphy with somatostatin analogues (111indium-penetreotide-)157,158 or technetium99m-labeled depreo-tide]159 or 18uoro-2-deoxyglucose (18FDG) positron
60 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
emission tomography (PET) scans160162 have beenemployed to diagnose or assess disease activity in sarcoi-dosis. These techniques are expensive, and clinical valuehas not been established. HRCT scans are superior toradionuclide techniques to assess inammatory and in-trathoracic involvement in sarcoidosis.103,10667Galliumscans are inconvenient (scanning is performed 48 hoursafter injection of the radioisotope) and lack prognosticvalue.163,164 However, 67Ga scans may have a role inselected patients in whom the diagnosis is difcult, suchas in cases with normal chest radiographs and featuressuggesting extrathoracic sarcoidosis [e.g., uveitis, in-volvement of the central nervous system (CNS),etc.].163 Uptake of 67Ga may identify appropriate sitesto biopsy. PET scans may demonstrate increased meta-bolic activity in patients with pulmonary sarcoido-sis,163,165,166 but the clinical value of PET is uncertain.PET has a potential role in identifying sarcoid activity atextrapulmonary sites (e.g., bone,167 cardiac,168 or neu-ral169 sites. Currently, the value of radionuclide scans inassessing intrathoracic involvement remains to be estab-lished.
DIAGNOSIS OF PULMONARYSARCOIDOSISThe histological hallmark of sarcoidosis is a necrotizinggranulomatous process, typically distributing alongbronchovascular bundles and lymphatics (Figs. 58)(discussed in depth elsewhere in this issue by Dr. Rosen).Flexible beroptic bronchoscopy (FFB) with transbron-chial lung biopsy (TBLB) is the initial diagnostic pro-cedure of choice in patients with suspected pulmonarysarcoidosis.5 Sensitivity of TBLB ranges from 60 to 90%;yields are lower with radiographic stage 0 disease.170,171
When mediastinal lymphadenopathy is present on chestCT, transbronchial needle aspiration (TBNA) biopsieswith Wang 18, 19, or 22 gauge cytology needles are
diagnostic in 63 to 90% of patients.33,172177 Typicalfeatures of sarcoidosis by cytological examination includelymphocytes, epithelioid cell granulomas, multi-nucleated giant cells with no or minimal necrosis,clusters of palisading epithelioid histiocytes, and neg-ative stains for fungi and acid-fast bacteria (AFB).33,176
In two recent studies, the combination of TBNA andTBLB had a higher yield than either procedurealone.178,179 TBNA is much less expensive than media-stinoscopic lymph node biopsy180 but requires skill.Damage to the bronchoscope may complicate TBNA,particularly when performed by individuals with limitedexperience.181
CT-guided transthoracic ne needle aspiration(FNA) with or without core needle biopsy may be usefulto diagnose malignant or benign lesions involving me-diastinal or subcarinal lymph nodes (yields up to78%).182 Complications of transthoracic FNA includepneumothoraces (10 to 60%) or hemoptysis (5 to10%).182 Endoscopic ultrasound (EUS)-guided FNAhas been used to diagnose mediastinal masses or lymphnodes, with high yield (> 90%) in patients with malig-nancy,179,183,184 but experience is limited in patients withsarcoidosis.179,185 EUS allows visualization of mediasti-nal structures, including the paraesophageal space, aor-topulmonary window, and subcarinal region.179,186 Theoptimal approach to diagnosing mediastinal lymph no-des (i.e., TBNA or CT-guided FNA) depends upon theexpertise and preference of the local institution.
Surgical biopsies are not usually required to diag-nose sarcoidosis.However,when the foregoingproceduresare not denitive, biopsy of either or both mediastinallymph nodes and lung may be warranted. This can gen-erally be done with minimally invasive procedures, such ascervical mediastinoscopy,187,188 the Chamberlain proce-dure (a parasternal minithoracotomy to biopsy aortopul-monary window or para-aortic nodes), or video-assistedthoracoscopic surgical (VATS) biopsy.189
Figure 5 Pulmonary sarcoidosis. Low-powermicroscopic viewshows the lymphangitic pattern of distribution of the granulomasso typical of sarcoid (hematoxylin and eosin (H&E), 40).
Figure 6 Pulmonary sarcoidosis showing airway involvementby nonnecrotizing epithelioid granulomas (H&E,100).
PULMONARY SARCOIDOSIS/LYNCH ET AL 61
-
SPECIFIC COMPLICATIONS OFINTRATHORACIC SARCOIDOSIS
Pulmonary Vascular Involvement in SarcoidosisClinically signicant pulmonary vascular involvement isuncommon in sarcoidosis. However, sarcoid granuloma-tous lesions follow pulmonary vessels, and incidentalhistological involvement of vessels was noted in 42 to89% of open-lung biopsies from patients with pulmonarysarcoidosis.74,190 Pulmonary arterial hypertension (PAH)was reported in 1 to 5% of patients with sarcoidosis191195
but the incidence is much higher among patients withadvanced brocystic sarcoidosis.196200 The United Net-work for Organ Sharing (UNOS) database identied 363patients with sarcoidosis listed for lung transplantation(LT) in the United States between January 1995 andDecember 2002 who had undergone right heart catheter-ization (RHC).200 This represented 73% of all listedsarcoid patients. PAH, dened as mean pulmonary
arterial pressure (mPAP) > 25 mm Hg, was present in74%; 36% had severe PAH, dened as mPAP > 40 mmHg. Importantly, PFTs did not differ between those withor without PAH. However, patients with severe PAHwere seven times more likely to require supplementaloxygen. Two previous studies found that PAH was anindependent predictor of mortality among patients withsarcoidosis listed for LT.197,199
Mechanism(s) responsible for PAH in sarcoidosisinclude hypoxic vasoconstriction192; inltration or oblit-eration of pulmonary vessels by the granulomatous,brotic response201203; and extrinsic compression ofmajor pulmonary arteries by enlarged lymph nodes.191,202
A retrospective study of 22 patients with sarcoidosis andPAH found that mPAP correlated inversely with carbonmonoxide transfer factor (TCO) but not with spirometry(e.g., FVC, FEV1).
202 In that study, ve lung explantsfrom sarcoid patients with PAH undergoing LT wereexamined. Granulomas were predominantly locatedwithin the veins, associated with occlusive venopathyand chronic hemosiderosis; arterial lesions were minor.202
The diagnosis of PAH may be difcult. Non-invasive techniques include chest CT204 and Dopplerechocardiography (DE).197 Chest CT may be useful topredict PAH in patients with parenchymal lung dis-ease.204 CT features that suggest PAH include mainpulmonary artery (PA) diameter > 29 mm; segmentalartery to bronchus ratio > 1:1 in three of four lobes204;ratio of the diameter of the main PA and of theascending aorta > 1.205 Doppler echocardiography issuperior to CT in estimating PAH but is less accuratethan RHC.197 In a cohort of 374 patients with end-stagelung disease who were being evaluated for LT, estimatesof systolic PAP (sPAP) could be made by DE in 166(44%).197 However, sPAP estimates were inaccurate(> 10 mm Hg difference) compared with RHC meas-urements. In addition, 48% of patients were misclassiedas having PAH by DE. Sensitivity, specicity, and
Figure 7 (A) Pulmonary sarcoidosis. There is intrusive involvement of the pulmonary vascular walls by granulomas, producinggranulomatous vasculitis (H&E,100). (B) Pulmonary sarcoidosis. Higher magnication view of sclerosing nonnecrotizing granulomasintruding on the wall of a vessel. Note the asteroid body within a giant cell (H&E, 200).
Figure 8 Pulmonary sarcoidosis. Pleural involvement by thegranulomatous process is shown here. Note the rather sparseinterstitial lymphocytic inltrate, which is typical of the rather mildinterstitial pneumonitis accompanying sarcoidosis (H&E,100).
62 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
positive and negative predictive values of sPAP estima-tion for PAH were 85%, 55%, 52%, and 87%, respec-tively. DE was less accurate in patients with interstitiallung disease (ILD) compared with obstructive lungdisease (OLD). The negative predictive value (NPV)of sPAP for DE was 96% among patients with OLD butonly 44% for ILD.When right ventricular (RV) ndings(e.g., RV dilatation, hypertrophy, or systolic dysfunc-tion) were considered, NPV of DE was 96% for OLDand 74% for ILD. Thus a normal DE does not excludePAH in patients with ILD. Further, an abnormal DE isnot a reliable marker of PAH. When PAH is suspectedin patients with sarcoidosis, a conrmatory RHC shouldbe performed to assess the extent of PAP and respon-siveness to vasodilators.
The presence of PAH in sarcoidosis markedlyworsens survival. In one recent study of sarcoid patientswith PAH, 2 and 5 year survival rates were 74% and59%, respectively.202 In sharp contrast, 5 year survivalamong sarcoid controls without PAH was 96.4%. Dataregarding treatment of PAH complicating sarcoidosisare limited. Anecdotal successes were noted with corti-costeroids in some patients. In a retrospective review,three of ve sarcoid patients with PAH and no evidencefor pulmonary brosis responded favorably to high-dosecorticosteroids.202 In contrast, none of ve with radio-graphic evidence for pulmonary brosis improved.202
The role of vasodilators206 in sarcoid-associated PAHhas not been elucidated, but short- and long-termresponses were noted in case reports192 or small ser-ies.201,207 In the series of 22 patients with sarcoidosis andPAH reported by Nunes et al, none received long-termvasodilator therapy.202 The authors urged caution inusing vasodilator therapy because of the potential forprecipitating pulmonary edema in patients with veno-oclusive disease.202
Other rare vascular complications of sarcoidosis(limited to a few case reports) include pulmonary arterialstenoses from granulomatous involvement of the ves-sels,203,208 extrinsic compression of pulmonary arteriesby enlarged hilar lymph nodes or brosing mediastini-tis,209,210 and pulmonary veno-occlusive disease (result-ing from obstruction of interlobular septa veins bygranulomata or perivascular brosis).211,212 Extensivebrosis of mediastinal or vascular structures may resultin narrowing or obstruction of innominate veins213 orsuperior vena cava (SVC).208,214220
Necrotizing Sarcoid AngiitisNecrotizing sarcoid angiitis and granulomatosis (NSG),initially described by Liebow in 1973,221 is a raredisorder characterized by pulmonary vasculitis, gra-nulomas, and pulmonary nodules on chest radio-graphs.222227 Hilar adenopathy has been cited in 10%to 60% of patients.224227 Lung biopsies in NSG
demonstrate a granulomatous vasculitis involving arteriesand veins, conuent nonnecrotizing granulomata involv-ing bronchi, bronchioles, and lung, and foci of paren-chymal necrosis.222,225 Vascular involvement (angiitis)typically consists of intramural granulomata or lympho-cytic and plasma cell inltrates conned to vesselswalls.227 Systemic vasculitis does not occur. Since theoriginal description, seven series of NSG,222,223,225229 aswell as case reports224,230234 have been published, for atotal of 100 cases. In a recent review of 14 cases ofNSG, 12 had extrapulmonary symptoms; pulmonaryfunction was normal in 13, but DLCO was decreased ineight of 11 patients tested.227 Chest radiographs dem-onstrated alveolar inltrates in seven; nodules in seven;cavitation in two.227 Clinical and radiographic features ofNSG are similar to nodular sarcoid or nummularsarcoidosis235238. Nodular sarcoidosis demonstrates fo-cal nodules composed of masses of granulomas andhyalinized connective tissue.235 We believe that NSGand nodular sarcoid are simply variants of sarcoidosis.Prognosis of these entities is usually excellent. Thedisease resolves in most patients (either spontaneouslyor in response to therapy). In one recent series, favorableresponses to corticosteroids were noted in ve of vetreated patients with NSG.227
BronchostenosisStenosis or compression of bronchi may result fromgranulomatous inammation of the bronchial wall,extrinsic compression from enlarged hilar nodes, ordistortion of major bronchi caused by parenchymal b-rosis.72,73,239241 Proximal endobronchial stenosis is typ-ically associated with dyspnea, cough, wheezing, andextrapulmonary manifestations.72,73 Atelectasis of in-volved lobes or segments may result.239,240,242244 Theright middle lobe is most often affected because of thesmall orice, sharp angulation from the bronchus inter-medius, and large number of local lymph nodes.34 Theincidence of bronchostenosis (by bronchoscopic assess-ment) in patients with sarcoidosis ranged from 2 to 26%in two studies,72,241 but severe bronchostenosis is rare. Ina retrospective study of 2500 patients with sarcoidosis,French investigators identied 18 patients with > 50%stenosis of proximal bronchi.73 Bronchoscopic patternsincluded single focal stenosis, multiple focal stenoses, anddiffuse narrowing of the bronchial tree.73 Edema andinammation of the mucosa at sites of stenosis were auniversal nding. Endobronchial biopsies revealed non-necrotizing granulomata in 77% of patients.73 Wheezing,high-pitched inspiratory squeaks, or stridor may beevident on chest auscultation in patients with sympto-matic bronchostenosis.72 Helical CT scans are useful todetermine the extent and nature of stenotic lesions in thelower respiratory tract,78 but CT overestimates the degreeof stenosis.78,245 Early initiation of corticosteroid therapy
PULMONARY SARCOIDOSIS/LYNCH ET AL 63
-
may be efcacious.73 Conversely, delay in therapy mayresult in acquired xed stenoses and persistent ventilatorydefects.73 Dilatation of endobronchial stenoses should beconsidered for patients refractory to medical therapy.246
MycetomasMycetomas (typically due to Aspergillus species) maydevelop in cystic spaces (typically in the upper lobes) inpatients with advanced (stage III or IV) sarcoido-sis.39,40,247,248 Ipsilateral pleural thickening usually pre-cedes the fungus ball or air-crescent sign.249 Mycetomasare often asymptomatic, but fatal hemorrhage can occurdue to invasion of vessel walls.243,247,250 Prognosis ofaspergilloma is poor (fatality rates > 50%); most fatal-ities reect progression of the underlying disease ratherthan a direct complication of mycetoma.39,40 Surgicalresection is advised for localized lesions in patients ableto tolerate surgery39,40,247 but the risk of surgery may beprohibitive in patients with severe parenchymal diseaseor extensive pleural adhesions.39,247 Anecdotal successhas been cited with topical or intracavitary therapy, butexperience is limited.251,252 Systemic antifungal therapyis of unproven value. Bronchial embolization may con-trol intractable bleeding.40
Pleural Involvement in SarcoidosisClinically signicant pleural manifestations (e.g., pneu-mothorax, pleural effusions, chylothorax) occur in 2 to4% of patients with sarcoidosis.253259 Pleural thickeningmay be observed when sensitive techniques are appliedbut is usually not associated with clinical symptoms. Twostudies using HRCT cited pleural thickening in 9%32
and 11%260 of sarcoid patients, respectively. The inci-dence is higher in patients with chronic brocysticsarcoidosis. A study of 61 patients with chronic sarcoi-dosis (> 2 years duration) cited pleural involvement onchest CT in 25 (41%); this included 20 cases of pleuralthickening and ve effusions.261 Pleural thickening wasmore common among patients with parenchymal brosis(stage IV), restrictive PFTs, and low DLCO. Earlierreports noted that pleural involvement in sarcoidosiswas typically associated with widespread parenchymallung disease.262,263 Subpleural or pleural nodules264,265
may be observed by HRCT in 22 to 76% of sarcoidosiscases,101,266,267 but rarely cause symptoms. Pleural effu-sions complicate sarcoidosis in < 3% of patients and,when present, are usually asymptomatic.259 Kostina et aldetected only three pleural effusions among 2775 pa-tients with pulmonary sarcoidosis.268 The incidence ismore common when more sensitive tests are used. In arecent prospective study, thoracic ultrasonograms wereperformed in 181 consecutive outpatients with sarcoi-dosis.257 Pleural effusions were detected in ve (2.8%)but only three were attributed to sarcoidosis; two were a
manifestation of congestive heart failure. Sarcoid pleuraleffusions may be either transudative or exudative; lym-phocytosis occurs in two thirds of cases,253,254,257,259
with predominance of CD4 lymphocytes.259,269,270 A
few cases of eosinophilic pleural effusions were de-scribed.271,272 Although exceedingly rare, cases of mas-sive pleural effusions have been described.273277 In onecase, pleural sarcoidosis with trapped lung requireddecortication for relief of symptoms.278 Pneumothoraxmay complicate sarcoidosis,255,259,268,279282 due to rup-ture of bullae or necrosis of subpleural granulomas.259
Only a few cases of chylothorax complicating sarcoidosishave been reported.283287
Sarcoidosis in HIV-Infected PatientsSarcoid-like granulomatous response is a rare complica-tion of infection due to human immunodeciency virus(HIV).288293 Chest radiographic288 and histological292
ndings are similar to sarcoidosis in non-HIV infectedpatients. Most cases occur after beginning highly activeantiretroviral therapy (HAART),288,291295 but sarcoi-dosis can precede institution of HAART.288,296 Thesarcoid-like granulomas following HAART likely reectimmune reconstitution, with inux of naive and IL-2receptor-positive CD4 cells.
292,297,298 However, CD8alveolitis was noted in one case.299 Administration ofexogenous IL-2, which leads to a sustained increase inCD4 T cells,
300 may precipitate sarcoid-like lesions inHIV-infected patients. In one HIV-infected patientwith undetectable viral load under HAART, sarcoidosisdeveloped 2 months after initiation of IL-2 treat-ment.293 Symptoms resolved following discontinuationof IL-2. Treatment of sarcoid-like reaction in HIV-infected patients is controversial, but favorable responsesto corticosteroids have been noted.290,298
Sarcoidosis Complicating Type 1 InterferonTherapyType 1 interferons (e.g., IFN-a or IFN-b), used to treatviral hepatitis, multiple sclerosis, and diverse autoimmuneand malignant disorders, may increase IFN-g and IL-2levels, evoking a Th1 lymphocyte bias and granulomatousinammation.301303 Sarcoidosis is a rare complication ofIFN-a or IFN-b, therapy.301,302,304311 In a review of 60cases of sarcoidosis following recombinant IFN-a (rIFN-a) therapy; 52 (87%) were receiving pegylated a-INF forhepatitis C virus (HCV) infection.303 The remainingcases were associated with hepatitis B infection,309 lym-phoproliferative malignancies,312,313 and other hemato-logic conditions. The incidence of sarcoidosis amongpatients with HCV infection treated with rIFN-a was< 0.5% in most studies302304 but one study cited anincidence of 5%.314 Ramos-Casals et al reported 68cases of sarcoidosis associated with chronic HCV
64 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
infection; 76% had lung involvement; 30%, skin involve-ment.304 Sarcoidosis developed within 6 months ofantiviral therapy in two thirds of patients. HCV-positivepatients with sarcoidosis had a lower incidence oflymphadenopathy (hilar or extrapulmonary) and a higherfrequency of cutaneous and articular involvement com-pared with HCV-negative sarcoid patients.304 Mostcases of sarcoidosis resolve with withdrawal of rIFN-aor dose reduction303,304 but corticosteroids are requiredin some patients.302,315 However, corticosteroids orimmunosuppressive agents may increase the viralload304 and should be reserved for highly selectedpatients.
Treatment of SarcoidosisTreatment of sarcoidosis remains controversial. Cortico-steroids (CSs) are the cornerstone of therapy for severeor progressive sarcoidosis (pulmonary or extrapulmo-nary), and often produce dramatic resolution of dis-ease.65,316,317 The long-term benet of CS therapy hasnot been established because relapses may occur upontaper or cessation of therapy.4,23,25 The decision to treatrequires a careful assessment of acuity and severity ofdisease, likelihood of SR, and risks associated withtherapy. Treatment should be circumscribed and fo-cused. Treatment is rarely appropriate for stage I diseaseunless extrapulmonary symptoms are prominent. Insymptomatic patients with stage II or III disease, a trialof CSs should be considered after an initial observationperiod (6 to 12 months). Immediate treatment, however,is appropriate for patients with severe symptoms orpulmonary dysfunction and presumed active alveolitis.Therapy is rarely efcacious, however, and may beassociated with signicant toxicities in patients withfar-advanced brosis, honeycombing, or bullae (radio-graphic stage IV).
The appropriate dose and duration of CS therapyhas not been evaluated in controlled, randomized trials.For most patients, initial daily dose of prednisone 40mg/day (or equivalent) for 4 weeks, tapered to 40 mgalternate days by 3 months, is sufcient. Higher dosesmay be appropriate for patients with cardiac or centralnervous system involvement, or selected patients withsevere pulmonary sarcoidosis. Responses to CSs areusually evident within 4 to 8 weeks. Failure to respondto CSs may reect inadequate dose or duration oftherapy, presence of irreversible brotic or cystic disease,noncompliance, or intrinsic CS resistance. Among CS-responders, we continue prednisone, albeit in a taperingfashion. The rate of taper is individualized according toresponse and adverse effects. A minimum of 12 monthsof therapy (among responders) is recommended. Inselected patients, long-term (often years) of low-dose,alternate-day prednisone may be required to preventrelapses.
Inhaled CSs suppress endobronchial or alveolarinammation but have limited efcacy.318323 InhaledCSs are expensive, and we do not employ these agentsfor patients with symptomatic pulmonary sarcoidosis.However, inhaled CSs may have an adjunctive roleamong patients manifesting bronchial hyperreactivityor cough.
Alternatives to CorticosteroidsImmunosuppressive, cytotoxic, and immunomodulatoryagents have been used to treat patients failing or expe-riencing adverse effects from CSs.324 The optimalagent(s) has not been determined because controlledstudies comparing various agents are lacking. Favorableresponses have been cited with methotrexate,325327
azathioprine,328330; leunamide,331,332 cyclophospha-mide,333335 chlorambucil,336 cyclosporine A,337 antima-larials (chloroquine or hydroxychloroquine),338340
pentoxyfylline,341,342 thalidomide,343345 and TNF-ainhibitors346 (particularly iniximab).347349 Because ofpotential serious toxicities (including oncogenesis) asso-ciated with cyclophosphamide and chlorambucil,350 wedo not use these agents to treat pulmonary sarcoidosis.We reserve the use of thalidomide and pentoxyfyline forresearch trials. For patients with progressive pulmonarysarcoidosis refractory to CSs, we initiate treatment withazathioprine (dose 100 to 150 mg/d PO) or methotrex-ate (dose 1525 mg once weekly PO). These agents canbe used in lieu of or in addition to CSs. Hydroxychlor-oquine (dose 200 mg twice daily) has minimal toxicityand may have modest benet as adjunctive therapy inselected patients with pulmonary or extrapulmonarysarcoidosis. Iniximab is reserved for severe cases refrac-tory to CSs and these alternative agents. Novel medicaltherapies for sarcoidosis are discussed in detail byDrs. Baughman and Lower in this issue.
Lung Transplantation for SarcoidosisLT (either single or bilateral) is a viable option forpatients with end-stage pulmonary sarcoidosis refractoryto medical therapy.198,351 Dr. Shah discusses LT forsarcoidosis in depth elsewhere in this issue.
REFERENCES
1. Lynch JP III, Baughman R, Sharma O. Extrapulmonarysarcoidosis. Semin Respir Infect 1998;13:229254
2. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl JMed 1997;336:12241234
3. Statement on sarcoidosis. Joint Statement of the AmericanThoracic Society (ATS), the European Respiratory Society(ERS) and the World Association of Sarcoidosis and OtherGranulomatous Disorders (WASOG) adopted by the ATSBoard of Directors and by the ERS Executive Committee,
PULMONARY SARCOIDOSIS/LYNCH ET AL 65
-
February 1999. Am J Respir Crit Care Med 1999;160:736755
4. Johns CJ, Michele TM. The clinical management ofsarcoidosis: a 50-year experience at the Johns HopkinsHospital. Medicine (Baltimore) 1999;78:65111
5. Lynch JP III, Kazerooni EA, Gay SE. Pulmonarysarcoidosis. Clin Chest Med 1997;18:755785
6. Baughman RP, Teirstein AS, Judson MA, et al. Clinicalcharacteristics of patients in a case control study of sarcoidosis.Am J Respir Crit Care Med 2001;164(10 Pt 1):18851889
7. Neville E, Walker A, James DG. Prognostic factorspredicting the outcome of sarcoidosis: an analysis of 818patients. Q J Med 1983;52(208):525533
8. Romer FK. Presentation of sarcoidosis and outcome ofpulmonary changes. Dan Med Bull 1982;29:2732
9. Scadding JG. Prognosis of intrathoracic sarcoidosis inEngland: a review of 136 cases after ve years observation.BMJ 1961;2:11651172
10. Hillerdal G, Nou E, Osterman K, Schmekel B. Sarcoidosis:epidemiology and prognosis: a 15-year European study. AmRev Respir Dis 1984;130:2932
11. Henke CE, Henke G, Elveback LR, Beard CM, Ballard DJ,Kurland LT. The epidemiology of sarcoidosis in Rochester,Minnesota: a population-based study of incidence andsurvival. Am J Epidemiol 1986;123:840845
12. Bechtel JJ, Starr T III, Dantzker DR, Bower JS. Airwayhyperreactivity in patients with sarcoidosis. Am Rev RespirDis 1981;124:759761
13. Reich JM, Johnson RE. Course and prognosis of sarcoidosisin a nonreferral setting: analysis of 86 patients observed for10 years. Am J Med 1985;78:6167
14. Reich JM. Mortality of intrathoracic sarcoidosis in referralvs population-based settings: inuence of stage, ethnicity,and corticosteroid therapy. Chest 2002;121:3239
15. Judson MA, Baughman RP, Thompson BW, et al. Twoyear prognosis of sarcoidosis: the ACCESS experience.Sarcoidosis Vasc Diffuse Lung Dis 2003;20:204211
16. Baughman RP, Winget DB, Bowen EH, Lower EE.Predicting respiratory failure in sarcoidosis patients. Sarcoi-dosis Vasc Diffuse Lung Dis 1997;14:154158
17. Huang CT, Heurich AE, Sutton AL, Lyons HA. Mortalityin sarcoidosis: a changing pattern of the causes of death.Eur J Respir Dis 1981;62:231238
18. Perry A, Vuitch F. Causes of death in patients withsarcoidosis: a morphologic study of 38 autopsies with clini-copathologic correlations. Arch Pathol Lab Med 1995;119:167172
19. Siltzbach LE, James DG, Neville E, et al. Course andprognosis of sarcoidosis around the world. Am J Med 1974;57:847852
20. Gribbin J, Hubbard RB, Le Jeune I, Smith CJ, West J,Tata LJ. The incidence and mortality of idiopathicpulmonary brosis and sarcoidosis in the UK. Thorax2006;61:980985
21. Yamamoto M, Kosuda T, Yanagawa H, et al. Long-termfollow-up in sarcoidosis in Japan. Z Erkr Atmungsorgane1977;149:191196
22. Israel HL, Karlin P, Menduke H, DeLisser OG. Factorsaffecting outcome of sarcoidosis. Inuence of race, extra-thoracic involvement, and initial radiologic lung lesions. AnnN Y Acad Sci 1986;465:609618
23. Johns CJ, Schonfeld SA, Scott PP, Zachary JB, MacGregorMI. Longitudinal study of chronic sarcoidosis with low-dose
maintenance corticosteroid therapy: outcome and compli-cations. Ann NY Acad Sci 1986;465:702712
24. Siltzbach LE. Sarcoidosis: clinical features and manage-ment. Med Clin North Am 1967;51:483502
25. Gottlieb JE, Israel HL, Steiner RM, Triolo J, Patrick H.Outcome in sarcoidosis: the relationship of relapse tocorticosteroid therapy. Chest 1997;111:623631
26. Gideon NM, Mannino DM. Sarcoidosis mortality in theUnited States 19791991: an analysis of multiple-causemortality data. Am J Med 1996;100:423427
27. Iwai K, Takemura T, Kitaichi M, Kawabata Y, Matsui Y.Pathological studies on sarcoidosis autopsy, II: Early change,mode of progression and death pattern. Acta Pathol Jpn 1993;43:377385
28. Lynch JP III, Wurfel M, Flaherty K, et al. Usualinterstitial pneumonia. Semin Respir Crit Care Med2001;22:357387
29. De Vries J, Rothkrantz-Kos S, van Dieijen-Visser MP,Drent M. The relationship between fatigue and clinicalparameters in pulmonary sarcoidosis. Sarcoidosis VascDiffuse Lung Dis 2004;21:127136
30. Wirnsberger RM, de Vries J, Breteler MH, van Heck GL,Wouters EF, Drent M. Evaluation of quality of life insarcoidosis patients. Respir Med 1998;92:750756
31. Bergin CJ, Bell DY, Coblentz CL, et al. Sarcoidosis:correlation of pulmonary parenchymal pattern at CT withresults of pulmonary function tests. Radiology 1989;171:619624
32. Brauner MW, Grenier P, Mompoint D, Lenoir S, deCremoux H. Pulmonary sarcoidosis: evaluation with high-resolution CT. Radiology 1989;172:467471
33. Cetinkaya E, Yildiz P, Altin S, Yilmaz V. Diagnostic valueof transbronchial needle aspiration by Wang 22-gaugecytology needle in intrathoracic lymphadenopathy. Chest2004;125:527531
34. Lynch JP III. Computed tomographic scanning in sarcoi-dosis. Semin Respir Crit Care Med 2003;24:393418
35. Packe GE, Ayres JG, Citron KM, Stableforth DE. Largelung bullae in sarcoidosis. Thorax 1986;41:792797
36. Zar HJ, Cole RP. Bullous emphysema occurring inpulmonary sarcoidosis. Respiration 1995;62:290293
37. Biem J, Hoffstein V. Aggressive cavitary pulmonary sarcoi-dosis. Am Rev Respir Dis 1991;143:428430
38. Ichikawa Y, Fujimoto K, Shiraishi T, Oizumi K. Primarycavitary sarcoidosis: high-resolution CT ndings. AJR Am JRoentgenol 1994;163:745
39. Israel HL, Lenchner GS, Atkinson GW. Sarcoidosis andaspergilloma: the role of surgery. Chest 1982;82:430432
40. Tomlinson JR, Sahn SA. Aspergilloma in sarcoid andtuberculosis. Chest 1987;92:505508
41. Lewis MM, Mortelliti MP, Yeager H Jr, ,Tsou E. Clinicalbronchiectasis complicating pulmonary sarcoidosis: caseseries of seven patients. Sarcoidosis Vasc Diffuse Lung Dis2002;19:154159
42. Mana J, Gomez-Vaquero C, Montero A, et al. Lofgrenssyndrome revisited: a study of 186 patients. Am J Med1999;107:240245
43. Gibson GJ, Prescott RJ, Muers MF, et al. British ThoracicSociety Sarcoidosis study: effects of long term corticosteroidtreatment. Thorax 1996;51:238247
44. Hunninghake GW, Gilbert S, Pueringer R, et al. Outcomeof the treatment for sarcoidosis. Am J Respir Crit Care Med1994;149(4 Pt 1):893898
66 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
45. Chappell AG, Cheung WY, Hutchings HA. Sarcoidosis: along-term follow-up study. Sarcoidosis Vasc Diffuse LungDis 2000;17:167173
46. Nagai S, Shigematsu M, Hamada K, Izumi T. Clinicalcourses and prognoses of pulmonary sarcoidosis. Curr OpinPulm Med 1999;5:293298
47. Mana J, Salazar A, Manresa F. Clinical factors predictingpersistence of activity in sarcoidosis: a multivariate analysisof 193 cases. Respiration 1994;61:219225
48. Pietinalho A, Ohmichi M, Lofroos AB, Hiraga Y, Selroos O.The prognosis of pulmonary sarcoidosis in Finland andHokkaido, Japan: a comparative ve-year study of biopsy-proven cases. Sarcoidosis Vasc Diffuse Lung Dis 2000;17:158166
49. Grunewald J, Eklund A, Olerup O. Human leukocyteantigen class I alleles and the disease course in sarcoidosispatients. Am J Respir Crit Care Med 2004;169:696702
50. Pasturenzi L, Martinetti M, Cuccia M, Cipriani A,Semenzato G, Luisetti M. HLA class I, II, and III poly-morphism in Italian patients with sarcoidosis: the Pavia-Padova Sarcoidosis Study Group. Chest 1993;104:11701175
51. Ina Y, Takada K, YamamotoM,MorishitaM, Senda Y, ToriiY. HLA and sarcoidosis in the Japanese. Chest 1989;95:12571261
52. Lenhart K, Kolek V, Bartova A. HLA antigens associatedwith sarcoidosis. Dis Markers 1990;8:2329
53. Gran JT, Bohmer E. Acute sarcoid arthritis: a favourableoutcome? A retrospective survey of 49 patients with reviewof the literature. Scand J Rheumatol 1996;25:7073
54. Sider L, Horton ES Jr. Hilar and mediastinal adenopathy insarcoidosis as detected by computed tomography. J ThoracImaging 1990;5:7780
55. Hennebicque AS, Nunes H, Brillet PY, Moulahi H, ValeyreD, Brauner MW. CT ndings in severe thoracic sarcoidosis.Eur Radiol 2005;15:2330
56. Nishimura K, Itoh H, Kitaichi M, Nagai S, Izumi T. CTand pathological correlation of pulmonary sarcoidosis.Semin Ultrasound CT MR 1995;16:361370
57. Brauner MW, Lenoir S, Grenier P, Cluzel P, Battesti JP,Valeyre D. Pulmonary sarcoidosis: CT assessment of lesionreversibility. Radiology 1992;182:349354
58. Abehsera M, Valeyre D, Grenier P, Jaillet H, Battesti JP,Brauner MW. Sarcoidosis with pulmonary brosis: CTpatterns and correlation with pulmonary function. AJR AmJ Roentgenol 2000;174:17511757
59. Muller NL, Miller RR. Ground-glass attenuation, nodules,alveolitis, and sarcoid granulomas. Radiology 1993;189:3132
60. Remy-Jardin M, Giraud F, Remy J, Copin MC, Gosselin B,Duhamel A. Importance of ground-glass attenuation inchronic diffuse inltrative lung disease: pathologic-CTcorrelation. Radiology 1993;189:693698
61. Murdoch J, Muller NL. Pulmonary sarcoidosis: changes onfollow-up CT examination. AJR Am J Roentgenol 1992;159:473477
62. Mana J, Teirstein AS, Mendelson DS, Padilla ML, DePaloLR. Excessive thoracic computed tomographic scanning insarcoidosis. Thorax 1995;50:12641266
63. Alhamad EH, Lynch JP III, Martinez FJ. Pulmonaryfunction tests in interstitial lung disease: what role do theyhave? Clin Chest Med 2001;22:715750 ix
64. Sharma OP, Johnson R. Airway obstruction in sarcoidosis: astudy of 123 nonsmoking black American patients withsarcoidosis. Chest 1988;94:343346
65. Sharma OP. Pulmonary sarcoidosis and corticosteroids.Am Rev Respir Dis 1993;147(6 Pt 1):15981600
66. Subramanian I, Flaherty K, Martinez F. Pulmonary functiontesting in sarcoidosis. In: Baughman RP, ed. Sarcoidosis.New York: Taylor and Francis Group; 2006;210:415433
67. Dunn TL, Watters LC, Hendrix C, Cherniack RM,Schwarz MI, King TE Jr. Gas exchange at a given degreeof volume restriction is different in sarcoidosis andidiopathic pulmonary brosis. Am J Med 1988;85:221224
68. Harrison BD, Shaylor JM, Stokes TC, Wilkes AR. Airowlimitation in sarcoidosis: a study of pulmonary function in107 patients with newly diagnosed disease. Respir Med1991;85:5964
69. McCann BG, Harrison BD. Bronchiolar narrowing andocclusion in sarcoidosis: correlation of pathology withphysiology. Respir Med 1991;85:6567
70. Stjernberg N, Thunell M. Pulmonary function in patientswith endobronchial sarcoidosis. Acta Med Scand 1984;215:121126
71. Benatar SR, Clark TJ. Pulmonary function in a case ofendobronchial sarcoidosis. Am Rev Respir Dis 1974;110:490496
72. Udwadia ZF, Pilling JR, Jenkins PF, Harrison BD.Bronchoscopic and bronchographic ndings in 12 patientswith sarcoidosis and severe or progressive airways obstruc-tion. Thorax 1990;45:272275
73. Chambellan A, Turbie P, Nunes H, Brauner M, Battesti JP,Valeyre D. Endoluminal stenosis of proximal bronchi insarcoidosis: bronchoscopy, function, and evolution. Chest2005;127:472481
74. Carrington CB. Structure and function in sarcoidosis. AnnNY Acad Sci 1976;278:265283
75. Miller A, Brown LK, Sloane MF, Bhuptani A, TeirsteinAS. Cardiorespiratory responses to incremental exercise insarcoidosis patients with normal spirometry. Chest 1995;107:323329
76. Radwan L, Grebska E, Koziorowski A. Small airwaysfunction in pulmonary sarcoidosis. Scand J Respir Dis 1978;59:3743
77. Levinson RS, Metzger LF, Stanley NN, et al. Airwayfunction in sarcoidosis. Am J Med 1977;62:5159
78. Lenique F, Brauner MW, Grenier P, Battesti JP, Loiseau A,Valeyre D. CT assessment of bronchi in sarcoidosis:endoscopic and pathologic correlations. Radiology 1995;194:419423
79. Lavergne F, Clerici C, Sadoun D, Brauner M, Battesti JP,Valeyre D. Airway obstruction in bronchial sarcoidosis:outcome with treatment. Chest 1999;116:11941199
80. Gleeson FV, Traill ZC, Hansell DM. Evidence ofexpiratory CT scans of small-airway obstruction in sarcoi-dosis. AJR Am J Roentgenol 1996;166:10521054
81. Viskum K, Vestbo J. Vital prognosis in intrathoracicsarcoidosis with special reference to pulmonary functionand radiological stage. Eur Respir J 1993;6:349353
82. Ohrn MB, Skold CM, van Hage-Hamsten M, Sigurdar-dottir O, Zetterstrom O, Eklund A. Sarcoidosis patientshave bronchial hyperreactivity and signs of mast cell acti-vation in their bronchoalveolar lavage. Respiration 1995;62:136142
PULMONARY SARCOIDOSIS/LYNCH ET AL 67
-
83. Manresa Presas F, Romero Colomer P, Rodriguez SanchonB. Bronchial hyperreactivity in fresh stage I sarcoidosis. AnnNY Acad Sci 1986;465:523529
84. Mihailovic-Vucinic V, Zugic V, Videnovic-Ivanov J. Newobservations on pulmonary function changes in sarcoidosis.Curr Opin Pulm Med 2003;9:436441
85. Delobbe A, Perrault H, Maitre J, et al. Impaired exerciseresponse in sarcoid patients with normal pulmonary function.Sarcoidosis Vasc Diffuse Lung Dis 2002;19:148153
86. Wirnsberger RM, Drent M, Hekelaar N, et al. Relationshipbetween respiratory muscle function and quality of life insarcoidosis. Eur Respir J 1997;10:14501455
87. Brancaleone P, Perez T, Robin S, Neviere R, Wallaert B.Clinical impact of inspiratory muscle impairment in sarcoi-dosis. Sarcoidosis Vasc Diffuse Lung Dis 2004;21:219227
88. Baydur A, Alsalek M, Louie SG, Sharma OP. Respiratorymuscle strength, lung function, and dyspnea in patients withsarcoidosis. Chest 2001;120:102108
89. Sietsema KE, Kraft M, Ginzton L, Sharma OP. Abnormaloxygen uptake responses to exercise in patients with mildpulmonary sarcoidosis. Chest 1992;102:838845
90. Karetzky M, McDonough M. Exercise and resting pulmo-nary function in sarcoidosis. Sarcoidosis Vasc Diffuse LungDis 1996;13:4349
91. Bradvik I, Wollmer P, Blom-Bulow B, Albrechtsson U,Jonson B. Lung mechanics and gas exchange during exercisein pulmonary sarcoidosis. Chest 1991;99:572578
92. Medinger AE, Khouri S, Rohatgi PK. Sarcoidosis: the valueof exercise testing. Chest 2001;120:93101
93. Barros WG, Neder JA, Pereira CA, Nery LE. Clinical,radiographic and functional predictors of pulmonary gasexchange impairment at moderate exercise in patients withsarcoidosis. Respiration 2004;71:367373
94. Lamberto C, Nunes H, Le Toumelin P, Duperron F, ValeyreD, Clerici C. Membrane and capillary blood components ofdiffusion capacity of the lung for carbon monoxide inpulmonary sarcoidosis: relation to exercise gas exchange.Chest 2004;125:20612068
95. Young RL, Lordon RE, Krumholz RA, Harkleroad LE,Branam GE, Weg JG. Pulmonary sarcoidosis, I: Pathophy-siologic correlations. Am Rev Respir Dis 1968;97:9971008
96. Young RC Jr, Carr C, Shelton TG, et al. Sarcoidosis:relationship between changes in lung structure and function.Am Rev Respir Dis 1967;95:224238
97. Huang CT, Heurich AE, Rosen Y, Moon S, Lyons HA.Pulmonary sarcoidosis: roentgenographic, functional, andpathologic correlations. Respiration 1979;37:337345
98. Winterbauer RH, Hutchinson JF. Use of pulmonary functiontests in the management of sarcoidosis. Chest 1980;78:640647
99. McLoud TC, Epler GR, Gaensler EA, Burke GW,Carrington CB. A radiographic classication for sarcoidosis:physiologic correlation. Invest Radiol 1982;17:129138
100. Lin YH, Haslam PL, Turner-Warwick M. Chronicpulmonary sarcoidosis: relationship between lung lavage cellcounts, chest radiograph, and results of standard lungfunction tests. Thorax 1985;40:501507
101. Muller NL, Mawson JB, Mathieson JR, Abboud R, OstrowDN, Champion P. Sarcoidosis: correlation of extent ofdisease at CT with clinical, functional, and radiographicndings. Radiology 1989;171:613618
102. Nugent KM, Peterson MW, Jolles H, Monick MM,Hunninghake GW. Correlation of chest roentgenograms
with pulmonary function and bronchoalveolar lavage ininterstitial lung disease. Chest 1989;96:12241227
103. Remy-Jardin M, Giraud F, Remy J, Wattinne L, WallaertB, Duhamel A. Pulmonary sarcoidosis: role of CT in theevaluation of disease activity and functional impairment andin prognosis assessment. Radiology 1994;191:675680
104. Muers MF, Middleton WG, Gibson GJ, et al. A simpleradiographic scoring method for monitoring pulmonarysarcoidosis: relations between radiographic scores, dyspnoeagrade and respiratory function in the British ThoracicSociety Study of Long-Term Corticosteroid Treatment.Sarcoidosis Vasc Diffuse Lung Dis 1997;14:4656
105. Oberstein A, von Zitzewitz H, Schweden F, Muller-Quernheim J. Noninvasive evaluation of the inammatoryactivity in sarcoidosis with high-resolution computed tomog-raphy. Sarcoidosis Vasc Diffuse Lung Dis 1997;14:6572
106. Drent M, De Vries J, Lenters M, et al. Sarcoidosis:assessment of disease severity using HRCT. Eur Radiol2003;13:24622471
107. Hansell DM, Milne DG, Wilsher ML, Wells AU.Pulmonary sarcoidosis: morphologic associations of airowobstruction at thin-section CT. Radiology 1998;209:697704
108. Akira M, Kozuka T, Inoue Y, Sakatani M. Long-termfollow-up CT scan evaluation in patients with pulmonarysarcoidosis. Chest 2005;127:185191
109. Finkel R, Teirstein AS, Levine R, Brown LK, Miller A.Pulmonary function tests, serum angiotensin-convertingenzyme levels, and clinical ndings as prognostic indicatorsin sarcoidosis. Ann NY Acad Sci 1986;465:665671
110. Keogh BA, Hunninghake GW, Line BR, Crystal RG. Thealveolitis of pulmonary sarcoidosis: evaluation of naturalhistory and alveolitis-dependent changes in lung function.Am Rev Respir Dis 1983;128:256265
111. Lieberman J, Schleissner LA, Nosal A, Sastre A, MishkinFS. Clinical correlations of serum angiotensin-convertingenzyme (ACE) in sarcoidosis: a longitudinal study of serumACE, 67gallium scans, chest roentgenograms, and pulmo-nary function. Chest 1983;84:522528
112. Johns CJ, Macgregor MI, Zachary JB, Ball WC. Extendedexperience in the long-term corticosteroid treatment ofpulmonary sarcoidosis. Ann NY Acad Sci 1976;278:722731
113. Odlum CM, FitzGerald MX. Evidence that steroids alterthe natural history of previously untreated progressivepulmonary sarcoidosis. Sarcoidosis 1986;3:4046
114. Bradvik I, Wollmer P, Blom-Bulow B, Albrechtsson U,Jonson B. Lung mechanics and gas exchange in steroidtreated pulmonary sarcoidosis: a seven year follow-up.Sarcoidosis 1991;8:105114
115. Zaki MH, Lyons H, Leilop L, Huang C. Corticosteroidtherapy in sarcoidosis: a ve-year, controlled follow-upstudy. NY State J Med 1987;87:496499
116. Goldstein DS, Williams MH. Rate of improvement ofpulmonary function in sarcoidosis during treatment withcorticosteroids. Thorax 1986;41:473474
117. Muller-Quernheim J, Pfeifer S, Strausz J, Ferlinz R.Correlation of clinical and immunologic parameters of theinammatory activity of pulmonary sarcoidosis. Am RevRespir Dis 1991;144:13221329
118. Siltzbach LE. The Kveim test in sarcoidosis: a study of 750patients. JAMA 1961;178:476482
119. Agostini C, Trentin L, Zambello R, et al. CD8 alveolitis insarcoidosis: incidence, phenotypic characteristics, and clin-ical features. Am J Med 1993;95:466472
68 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 1 2007
-
120. Semenzato G, Bortoli M, Brunetti E, Agostini C.Immunology and pathophysiology. In: European Respira-tory Monography on Sarcoidosis 2006;10 (monograph 32):4963
121. Robinson BW, McLemore TL, Crystal RG. Gammainterferon is spontaneously released by alveolar macrophagesand lung T lymphocytes in patients with pulmonarysarcoidosis. J Clin Invest 1985;75:14881495
122. Pinkston P, Bitterman PB, Crystal RG. Spontaneous releaseof interleukin-2 by lung T lymphocytes in active pulmonarysarcoidosis. N Engl J Med 1983;308:793800
123. Moller DR, Forman JD, Liu MC, et al. Enhancedexpression of IL-12 associated with Th1 cytokine prolesin active pulmonary sarcoidosis. J Immunol 1996;156:49524960
124. Dinarello CA. IL-18: a TH1-inducing, proinammatorycytokine and new member of the IL-1 family. J Allergy ClinImmunol 1999;103(1 Pt 1):1124
125. Shigehara K, Shijubo N, Ohmichi M, et al. Increased levelsof interleukin-18 in patients with pulmonary sarcoidosis.Am J Respir Crit Care Med 2000;162:19791982
126. Baughman RP, Strohofer SA, Buchsbaum J, Lower EE.Release of tumor necrosis factor by alveolar macrophages ofpatients with sarcoidosis. J Lab Clin Med 1990;115:3642
127. Steffen M, Petersen J, Oldigs M, et al. Increased secretionof tumor necrosis factor-alpha, interleukin-1-beta, andinterleukin-6 by alveolar macrophages from patients withsarcoidosis. J Allergy Clin Immunol 1993;91:939949
128. Agostini C, Trentin L, Facco M, et al. Role of IL-15, IL-2,and their receptors in the development of T cell alveolitis inpulmonary sarcoidosis. J Immunol 1996;157:910918
129. Petrek M, Pantelidis P, Southcott AM, et al. The sourceand role of RANTES in interstitial lung disease. Eur RespirJ 1997;10:12071216
130. Capelli A, Di Stefano A, Lusuardi M, Gnemmi I, DonnerCF. Increased macrophage inammatory protein-1alphaand macrophage inammatory protein-1beta levels inbronchoalveolar lavage uid of patients affected by differentstages of pulmonary sarcoidosis. Am J Respir Crit Care Med2002;165:236241
131. Kunkel SL, Lukacs NW, Strieter RM, Chensue SW. Th1and Th2 responses regulate experimental lung granulomadevelopment. Sarcoidosis Vasc Diffuse Lung Dis1996;13:120128
132. Ward K, OConnor C, Odlum C, Fitzgerald MX.Prognostic value of bronchoalveolar lavage in sarcoidosis:the critical inuence of disease presentation. Thorax 1989;44:612
133. Gibejova A, Mrazek F, Subrtova D, et al. Expression ofmacrophage inammatory protein-3 beta/CCL19 in pul-monary sarcoidosis. Am J Respir Crit Care Med 2003;167:16951703
134. Petrek M, Kolek V, Szotkowska J, du Bois RM. CC and Cchemokine expression in pulmonary sarcoidosis. Eur RespirJ 2002;20:12061212
135. Agostini C, Cassatella M, Zambello R, et al. Involvement ofthe IP-10 chemokine in sarcoid granulomatous reactions.J Immunol 1998;161:64136420
136. Armstrong L, Foley NM, Millar AB. Inter-relationshipbetween tumour necrosis factor-alpha (TNF-alpha) andTNF soluble receptors in pulmonary sarcoidosis. Thorax1999;54:524530
137. Hino T, Nakamura H, Shibata Y, Abe S, Kato S, TomoikeH. Elevated levels of type II soluble tumor necrosis factorreceptors in the bronchoalveolar lavage uids of patientswith sarcoidosis. Lung 1997;175:187193
138. Hauber HP, Gholami D, Meyer A, Pforte A. Increasedinterleukin-13 expression in patients with sarcoidosis.Thorax 2003;58:519524
139. Minshall EM, Tsicopoulos A, Yasruel Z, et al. CytokinemRNA gene expression in active and nonactive pulmonarysarcoidosis. Eur Respir J 1997;10:20342039
140. Bingisser R, Speich R, Zollinger A, Russi E, Frei K.Interleukin-10 secretion by alveolar macrophages andmonocytes in sarcoidosis. Respiration 2000;67:280286
141. Grunewald J, Berlin M, Olerup O, Eklund A. Lung T-helper cells expressing T-cell receptor AV2S3 associate withclinical features of pulmonary sarcoidosis. Am J Respir CritCare Med 2000;161(3 Pt 1):814818
142. Spagnolo P, Renzoni EA, Wells AU, et al. CC chemokinereceptor 2 and sarcoidosis: association with Lofgrenssyndrome. Am J Respir Crit Care Med 2003;168:11621166
143. BerlinM, Fogdell-Hahn A,OlerupO, Eklund A,GrunewaldJ. HLA-DR predicts the prognosis in Scandinavian patientswith pulmonary sarcoidosis. Am J Respir Crit Care Med1997;156:16011605
144. Sato H, Grutters JC, Pantelidis P, et al. HLA-DQB1*0201:a marker for good prognosis in British and Dutch patientswith sarcoidosis. Am J Respir Cell Mol Biol 2002;27:406412
145. Costabel U, Guzman J, Albera A, Baughman RP. Bron-choalveolar lavage in sarcoidosis. In: Baughman RP, ed.Sarcoidosis. New York: Taylor and Francis Group; 2006;210:399414
146. Welker L, Jorres RA, Costabel U, Magnussen H. Predictivevalue of BAL cell differentials in the diagnosis of interstitiallung diseases. Eur Respir J 2004;24:10001006
147. Drent M, van Velzen-Blad H, Diamant M, HoogstedenHC, van den Bosch JM. Relationship between presentationof sarcoidosis and T lymphocyte prole: a study inbronchoalveolar lavage uid. Chest 1993;104:795800
148. Drent M, Mulder PG, Wagenaar SS, Hoogsteden HC, vanVelzen-Blad H, van den Bosch JM. Differences in BALuid variables in interstitial lung diseases evaluated bydiscriminant analysis. Eur Respir J 1993;6:803810
149. Bjermer L, Back O, Roos G, Thunell M. Mast cells andlysozyme positive macrophages in bronchoalveolar lavagefrom patients with sarcoidosis: valuable prognostic andactivity marking parameters of disease? Acta Med Scand1986;220:161166
150. Drent M, Jacobs JA, de Vries J, Lamers RJ, Liem IH,Wouters EF. Does the cellular bronchoalveolar lavage uidprole reect the severity of sarcoidosis? Eur Respir J 1999;13:13381344
151. Ziegenhagen MW, Rothe ME, Schlaak M, Muller-Quer-nheim J. Bronchoalveolar and serological parameters reect-ing the severity of sarcoidosis. Eur Respir J 2003;21:407413
152. Laviolette M, La Forge J, Tennina S, Boulet LP. Prognosticvalue of bronchoalveolar lavage lymphocyte count in recentlydiagnosed pulmonary sarcoidosis. Chest 1991;100:380384
153. Verstraeten A, Demedts M, Verwilghen J, et al. Predictivevalue of bronchoalveolar lavage in pulmonary sarcoidosis.Chest 1990;98:560567
PULMONARY SARCOIDOSIS/LYNCH ET AL 69
-
154. Valeyre D, Saumon G, Georges R, et al. The relationshipbetween disease duration and noninvasive pulmonaryexplorations in sarcoidosis with erythema nodosum. AmRev Respir Dis 1984;129:938942
155. Mana J. Nuclear imaging: 67Gallium, 201thallium, 18F-labeled uoro-2-deoxy-D-glucose positron emission tomog-raphy. Clin Chest Med 1997;18:799811
156. Schuster DM, Alazraki N. Gallium and other agents indiseases of the lung. Semin Nucl Med 2002;32:193211
157. Kwekkeboom DJ, Krenning EP, Kho GS, Breeman WA,Van Hagen PM. Somatostatin receptor imaging in patientswith sarcoidosis. Eur J Nucl Med 1998;25:12841292
158. Lebtahi R, Crestani B, Belmatoug N, et al. Somatostatinreceptor scintigraphy and gallium scintigraphy in patientswith sarcoidosis. J Nucl Med 2001;42:2126
159. Shorr AF, Helman DL, Lettieri CJ, Montilla JL, BridwellRS. Depreotide scanning in sarcoidosis: a pilot study. Chest2004;126:13371343
160. El-Haddad G, Zhuang H, Gupta N, Alavi A. Evolving roleof positron emission tomography in the management ofpatients with inammatory and other benign disorders.Semin Nucl Med 2004;34:313329
161. Alavi A, Gupta N, Alberini JL, et al. Positron emissiontomography imaging in nonmalignant thoracic disorders.Semin Nucl Med 2002;32:293321
162. Halter G, Buck AK, Schirrmeister H, et al. [18F] 3-deoxy-30-uorothymidine positron emission tomography: alternative ordiagnostic adjunct to 2-[18f]-uoro-2-deoxy-D-glucose posi-tron emission tomography in the workup of suspicious centralfocal lesions? J Thorac Cardiovasc Surg 2004;127:10931099
163. Mana J, Vankroonenburgh M. Nuclear imaging techniquesin sarcoidosis. Eur Respir Monograph on Sarcoidosis 2005;10(monograph 32):284300
164. Mediwake R, Wells A, Desai D. Radiological imaging insarcoidosis. In: Baughman RP, ed. Sarcoidosis. New York:Taylor and Francis Group; 2006;210:365398
165. Lewis PJ, Salama A. Uptake of uorine-18-uorodeoxy-glucose in sarcoidosis. J Nucl Med 1994;35:16471649
166. Brudin LH, Valind SO, Rhodes CG, et al. Fluorine-18deoxyglucose uptake in sarcoidosis measured with positronemission tomography. Eur J Nucl Med 1994;21:297305
167. Aberg C, Ponzo F, Raphael B, Amorosi E, Moran V, KramerE. FDG positron emission tomography of bone involve-ment in sarcoidosis. AJR Am J Roentgenol 2004;182:975977
168. Takeda N, Yokoyama I, Hiroi Y, et al. Positron emissiontomography predicted recovery of complete A-V nodaldysfunction in a patient with cardiac sarcoidosis. Circulation2002;105:11441145
169. Dubey N, Miletich RS, Wasay M, Mechtler LL, Bakshi R.Role of uorodeoxyglucose positron emission tomography inthe diagnosis of neurosarcoidosis. J Neurol Sci 2002;205:7781
170. Gilman MJ, Wang KP. Transbronchial lung biopsy insarcoidosis: an approach to determine the optimal number ofbiopsies. Am Rev Respir Dis 1980;122:721724
171. Poe RH, Israel RH, Utell MJ, Hall WJ. Probability of apositive transbronchial lung biopsy result in sarcoidosis.Arch Intern Med 1979;139:761763
172. Wang KP, Fuenning C, Johns CJ, Terry PB. Flexibletransbronchial needle aspiration for the diagnosis ofsarcoidosis. Ann Otol Rhinol Laryngol 1989;98(4 Pt 1):298300
173. Leonard C, Tormey V, Lennon A, Burke CM. Utility ofWang transbronchial needle biopsy in sarcoidosis. Ir J MedSci 1997;166:4143
174. Cetinkaya E, Yildiz P, Kadakal F, et al. Transbronchialneedle aspiration in the diagnosis of intrathoracic lympha-denopathy. Respiration 2002;69:335338
175. Sharafkhaneh A, Baaklini W, Gorin AB, Green L. Yield oftransbronchial needle aspiration in diagnosis of mediastinallesions. Chest 2003;124:21312135
176. Trisolini R, Agli LL, Cancellieri A, et al. The value ofexible transbronchial needle aspiration in the diagnosis ofstage I sarcoidosis. Chest 2003;124:21262130
177. Morales CF, Pateeld AJ, Strollo PJ Jr, Schenk DA.Flexible transbronchial needle aspiration in the diagnosis ofsarcoidosis. Chest 1994;106:709711
178. Trisolini R, Lazzari Agli L, Cancellieri A, et al. Trans-bronchial needle aspiration improves the diagnostic yield ofbronchoscopy in sarcoidosis. Sarcoidosis Vasc Diffuse LungDis 2004;21:147151
179. Khoo KL, Ho KY, Nilsson B, Lim TK. EUS-guided FNAimmediately after unrevealing transbronchial needl






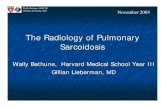

![Treatment of Sarcoidosis - WASOG...sessment in extra-pulmonary sarcoidosis. For cutaneous sar-coidosis, several instruments have been reported [6]. These include the sarcoidosis activity](https://static.fdocuments.net/doc/165x107/5e6355752530ca396d712283/treatment-of-sarcoidosis-wasog-sessment-in-extra-pulmonary-sarcoidosis-for.jpg)