
The Role of Rehabilitation in the Intensive Care Unit Kimberly Hartman, MD Assistant Professor of...
65
The Role of Rehabilitation in the Intensive Care Unit Kimberly Hartman, MD Assistant Professor of Pediatrics, UMKC SOM Faculty, Division of Rehabilitation Medicine, Children’s Mercy Hospital January 15, 2015
-
Upload
clifford-whitehead -
Category
Documents
-
view
218 -
download
1
Transcript of The Role of Rehabilitation in the Intensive Care Unit Kimberly Hartman, MD Assistant Professor of...

The Role of Rehabilitation in the Intensive Care Unit
Kimberly Hartman, MDAssistant Professor of Pediatrics, UMKC SOM
Faculty, Division of Rehabilitation Medicine, Children’s Mercy Hospital
January 15, 2015

Objectives
• Define and recognize ICU-acquired weakness• Understand implications of critical illness on
function• Review current interventions and state of the
evidence• Understand barriers to implementing rehab
strategies in the ICU

Critical Illness: Who
• > 5 million patients per year• 55,000 patients per day• Nearly 80% of all Americans will experience
critical illness or injury (as patient or loved one)
Ref 30
Critical Illness: Costs
• ICU length of stay: 6.1-9.3 days• Hospital costs:– 2000: $56.6 billion– 2005: $81.7 billion
Ref 30

Critical Illness: What
Adults• Respiratory
insufficiency/failure• Post-operative management• Ischemic heart disorder• Sepsis• Heart failure
Children and Neonates• Respiratory dysfunction• Hematologic instability• Central nervous system
disorders• Mixed respiratory and
hemodynamic dysfunction• Postcardiac arrest• Hepatic dysfunction• Renal dysfunction
Ref 30
Critical Illness: Common Ground
• Mechanical ventilation• Cardiovascular support• Invasive monitoring• Intensive observation• Frequent interventions (ave. 178 actions per
day)

Critical Illness: Common Ground
Critical Illness: Common Ground

Immobility
Circulation:• VTE• Increased edema• Increased workload on heart• Orthostasis
Endocrine:• Glucose intolerance• Increased fat stores• Disturbed Na-waterbalance
GI:• Aspiration• GER• Poor appetite• Malnutrition• Constipation• Vomiting
GU:• Difficulty voiding• Incontinence• UTI
Skin:• Pressure wound• Friction/shearing
Neuro:• Functional deficits• Delirium• Behavior changes• Sleep dysfunction
Respiratory:• Poor lung expansion• Weak cough• Secretions• Pneumonia
Musculoskeletal:• Loss of muscle mass• Weakness• Osteoporosis• Contractures

Nomenclature
Ref 27
Consensus
Intensive Care Unit-Acquired Weakness(ICU-AW)
Ref 9,27

ICU-AW
• Definition:“Syndrome of generalized limb weakness that
develops while the patient is critically ill and for which there is no alternative explanation other than the critical illness itself”
Ref 9, 19

ICU-AW: “Dx of Exclusion”
Ref 19
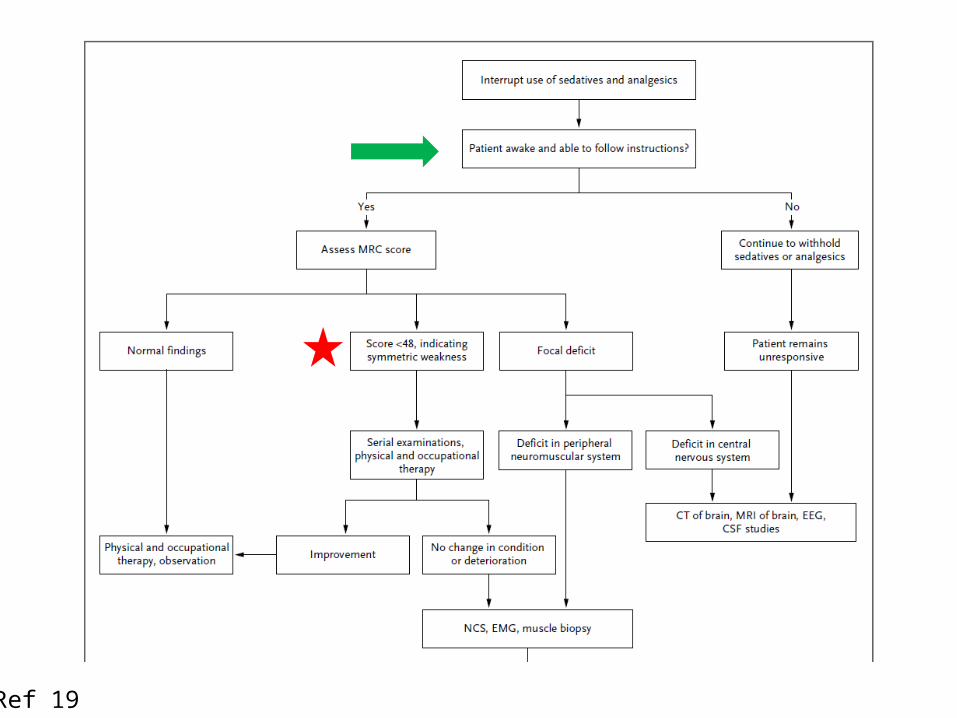
Ref 19

ICU-AW: Diagnosis
• Screen for awakening• Respond to at least 3
orders on 2 consecutive occasions separated by 6 hours
• Open/close your eyes• Look at me• Open your mouth and
put out your tongue• Nod your head• Raise your eyebrows
when I have counted up to 5
Ref 8

ICU-AW: Diagnosis
• Medical Research Council (MRC) score < 48– MMT grades 0-5– Six muscle groups bilaterally
– Total possible: 60
Shoulder abduction Hip flexion
Elbow flexion Knee extension
Wrist extension Ankle dorsiflexion
Ref 8 , 9

ICU-AW: Diagnosis
• Challenges– Awake and able to follow commands– Limitations of lines, catheters, trauma– Difficult to assess smaller changes
• Multiple studies ongoing for different assessment tool
Ref 15

ICU-AW: Subcategories
Ref 9 ,19
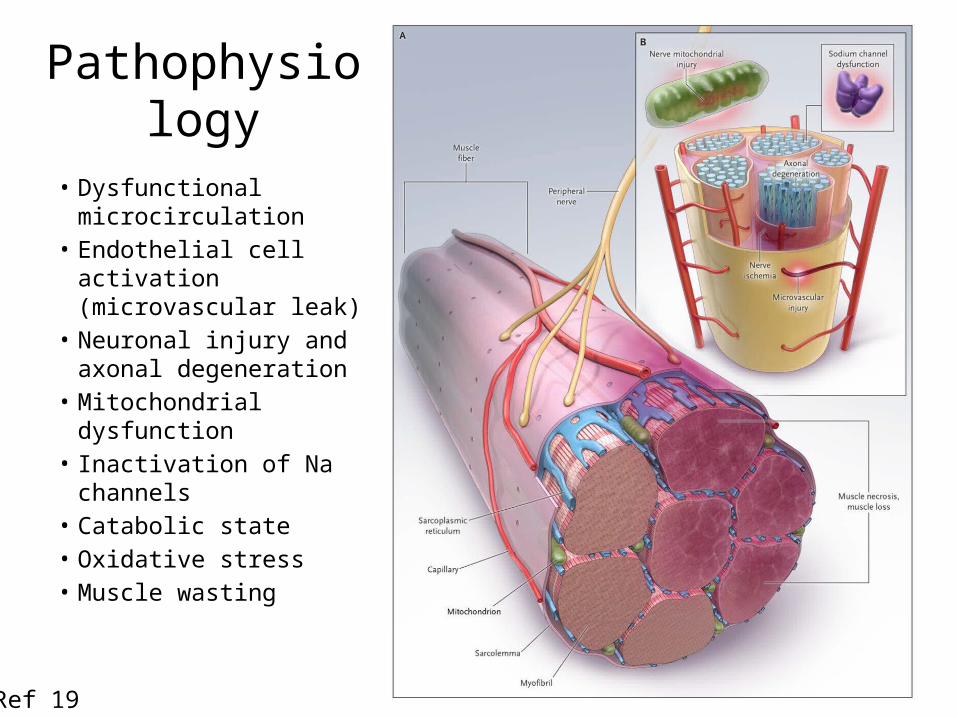
Pathophysiology
• Dysfunctional microcirculation
• Endothelial cell activation (microvascular leak)
• Neuronal injury and axonal degeneration
• Mitochondrial dysfunction
• Inactivation of Na channels
• Catabolic state• Oxidative stress• Muscle wasting
Ref 19
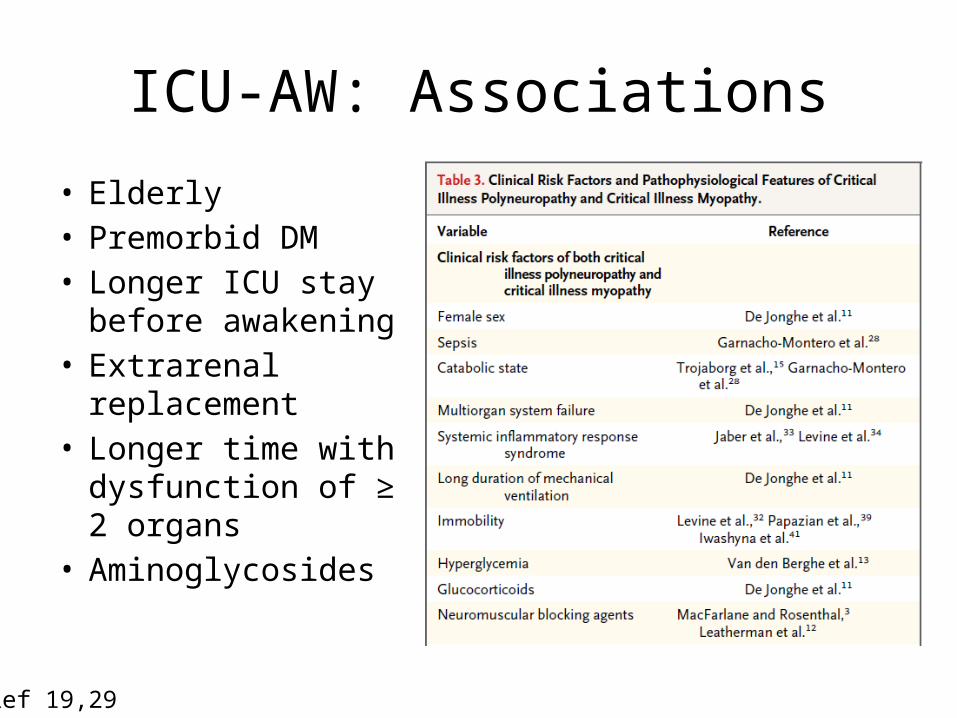
ICU-AW: Associations
• Elderly• Premorbid DM• Longer ICU stay
before awakening• Extrarenal
replacement• Longer time with
dysfunction of ≥ 2 organs
• Aminoglycosides
Ref 19,29

Functional Implications
• Physical– Weakness– Joint contractures– Long-term deficits
• Cognitive– Delirium– Long-term deficits
• Psychological
Up to 65% of patients with prolonged ventilation have functional limitations
after discharge
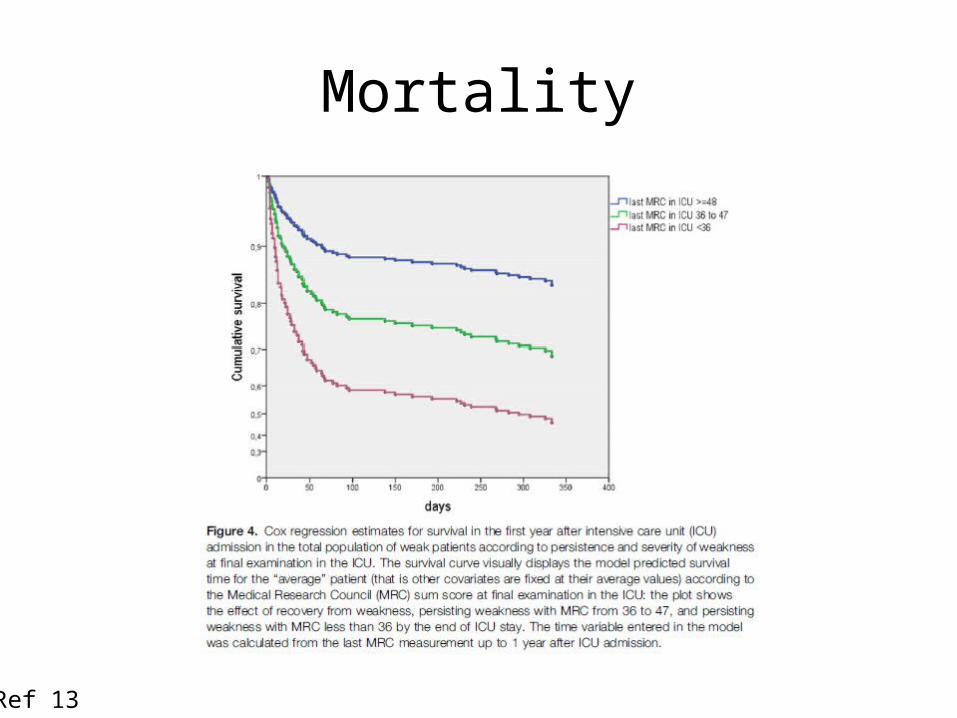
Mortality
Ref 13
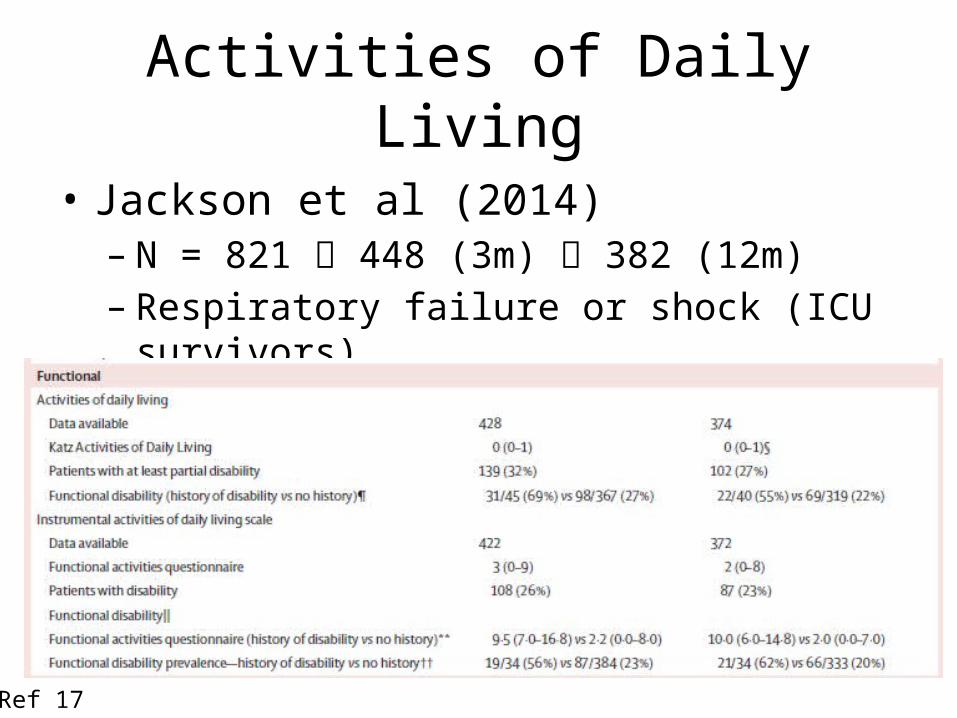
Activities of Daily Living
• Jackson et al (2014)– N = 821 448 (3m) 382 (12m)– Respiratory failure or shock (ICU survivors)
Ref 17
ICU-AW and Function
• Fan et al (2014)– N = 222– Acute lung injury, ICU survivors– High severity– Outcomes:• 36% with ICUAW at discharge• Strength generally improved by 12m• Duration of bedrest associated with worsened
weakness at 24m
Ref 10

ICU-AW and Function
• Function remained decreased (also grip strength, mean inspiratory force)
Ref 10
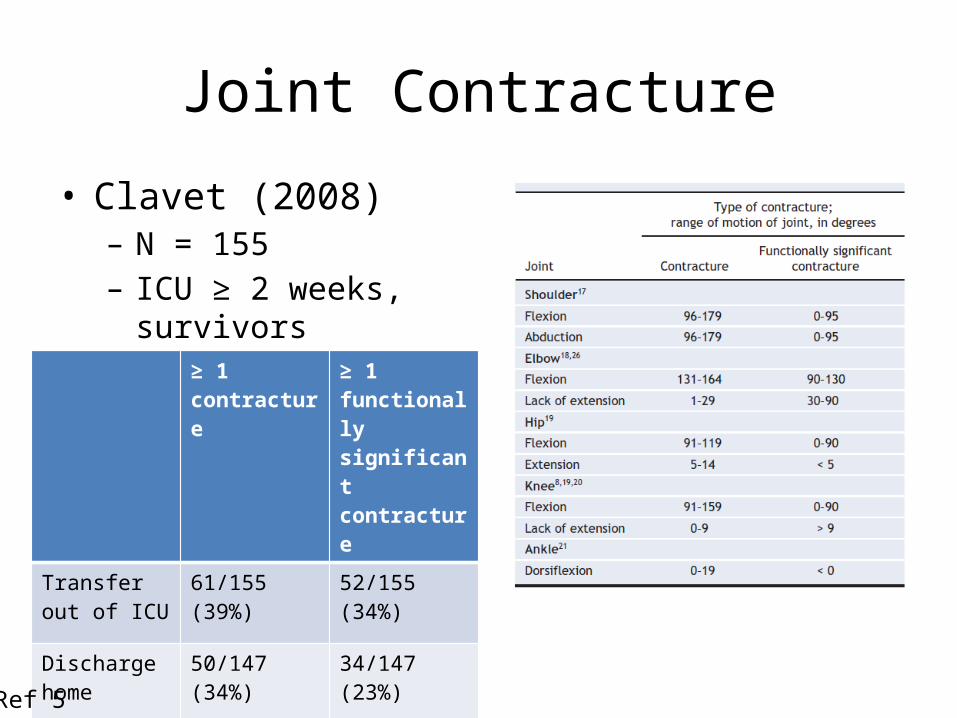
Joint Contracture
• Clavet (2008)– N = 155– ICU ≥ 2 weeks, survivors
≥ 1 contracture
≥ 1 functionally significant contracture
Transfer out of ICU
61/155 (39%) 52/155 (34%)
Discharge home
50/147 (34%) 34/147 (23%)
Ref 5

Joint Contracture
• Risk: 8+ weeks ICU stay (vs. 2-3 weeks)• Protection: steroids
Joint location Number of joints with contracture (total 212 in 61 patients)
Elbow 76 (36%)
Ankle 51 (24%)
Knee 31 (15%)
Hip 30 (14%)
Shoulder 24 (11%)
Ref 5

Joint Contracture
• Clavet (2008, 2014)– Outcomes:• Significantly fewer patients with contractures were
mobilized (55.3% vs. 79.4%)• Low ambulatory status (64.4% vs. 51.0%)• Associated with higher mortality• Associated with more difficulty with mobility 3.3 years
after discharge
Ref 6,28

Interventions

Passive Mobility
• Griffiths et al. (1995)– N =5– 1 leg CPM for 3x/day for 3h per session for 7 days– 1 leg routine nursing care– CPM leg:• Fiber area preserved or slightly increased (mean 11%)• Less protein loss
– Control leg:• Fiber area decreased (-35%)
Ref 11

Ergometry
• Burtin et al. (2009)– N = 90, RCT– Bedside ergometry (active or passive)– Starting day 5; 20 minutes per day– Control: standard PROM/AROM– At hospital discharge, significant improvement in:• 6MWD• Isometric quadriceps force• Functional well-being on SF36 PFS
Ref 4
Early Mobilization
• Schweikert et al. (2009)– N =104 mechanically ventilated– RCT– Intervention: mobilization 1.5 days after ETT– Control: usual care (mobilization 7.3 days)– Outcomes:• return to independent function (59% vs 35%)• physical function (median Barthel Index 75 vs 55)• ventilator-free days (median 23.5 vs 21.1)
Ref 24
Early Mobilization
• Decreased ICU length of stay• Decreased hospital length of stay• Improved survival without readmission at 1
year
Ref 20

Electrical Muscular Stimulation
• Amplitude (mA/A): amount of energy flowing per unit time
• Frequency (Hz): number of pulses per second• Pulse width (μs): duration of stimulation pulse• Ramp up and ramp down: current intensity
will increase or decrease to set intensity• On:off time: length of time the pulse is
delivered vs. no stimulation
Ref 23

EMS: Who responds
• Segers et al. (2014)– Response = muscle
contraction in >75% of sessions
– 50% responders– 50% nonresponders– Nonresponders:
• Sepsis• Edema• Vasopressors
Ref 25

EMS: Outcomes
• Parry et al. (2013): Review– Timing:• <3d: not shown to attenuate quad or bicep wasting• >14d: improved quad thickness (+4.9% vs. -3.2%)
– Severity of illness:• APACHE II > 20: greater muscle loss in general (16-20%);
did not demonstrate muscle preservation• APACHE II < 20: greater degree of preservation (8-14%
reduction)
Ref 23
EMS: Outcomes
• Strength: Increased in 4 studies• ICU AW diagnosis by MRC: – Control: 39%– EMS: 12.5%
• No difference (small study)
Ref 18,23

EMS: Challenges
Ref 23
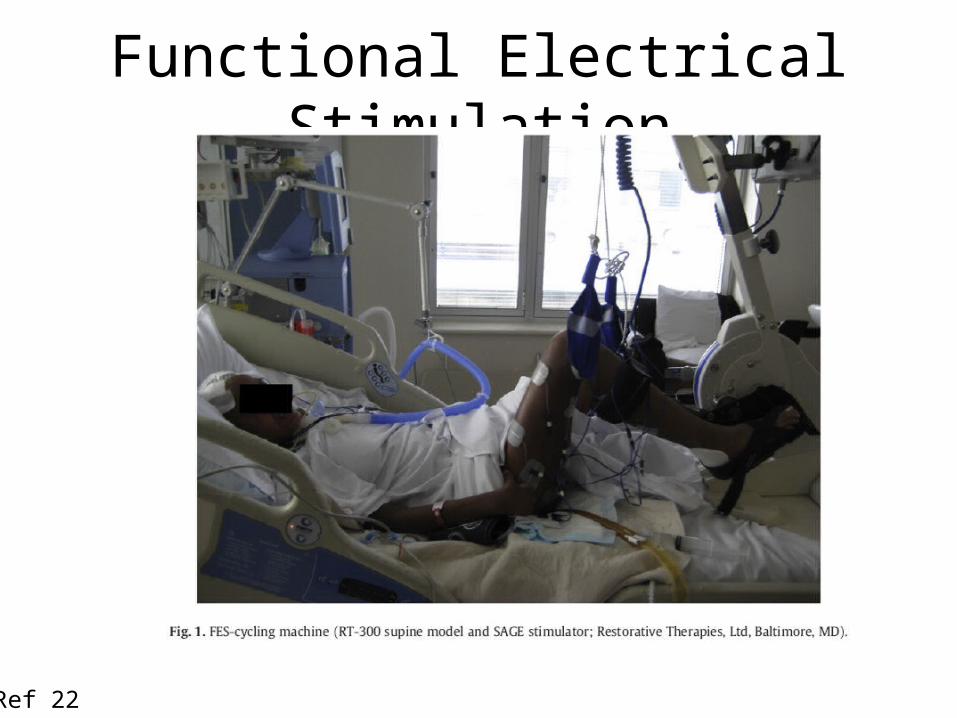
Functional Electrical Stimulation
Ref 22

FES
• Parry et al. (2014)– N = 16 (8 intervention, 8 matched controls)– Trend toward statistical significance
Ref 22
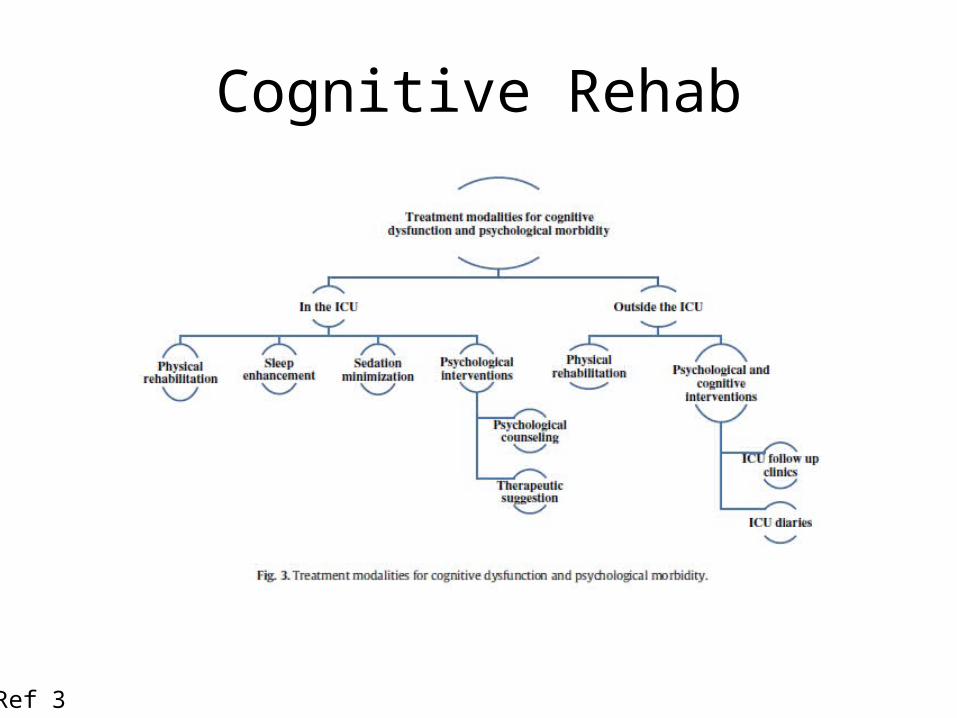
Cognitive Rehab
Ref 3

Barriers
Ref 2
Safety: Mobilization
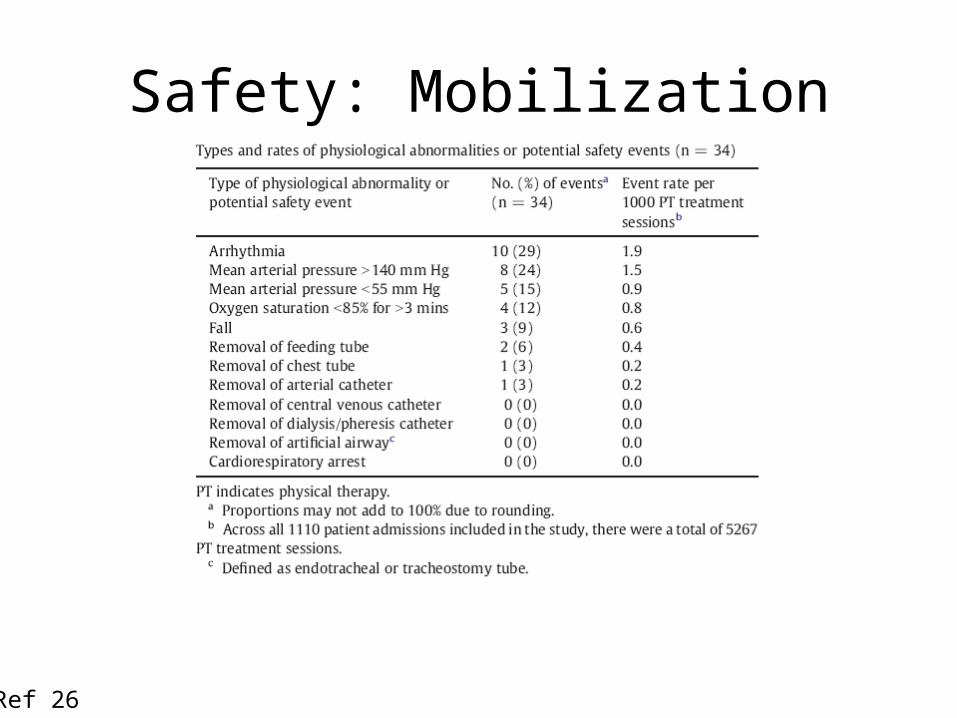
• Sricharoenchai 2014– N = 1110 patients; 5267 PT sessions– Median PT start: 2 days (IQR: 1-3)– Physiological abnormalities: 34 events in 25
patients• 0.6% of sessions• 2% of admissions
– Median time of event: 6 days (IQR 2-11)
Ref 26

Safety: Mobilization
Ref 26

Safety: Mobilization
Ref 26
Safety: Mobilization
Ref 26
Safety: Mobilization
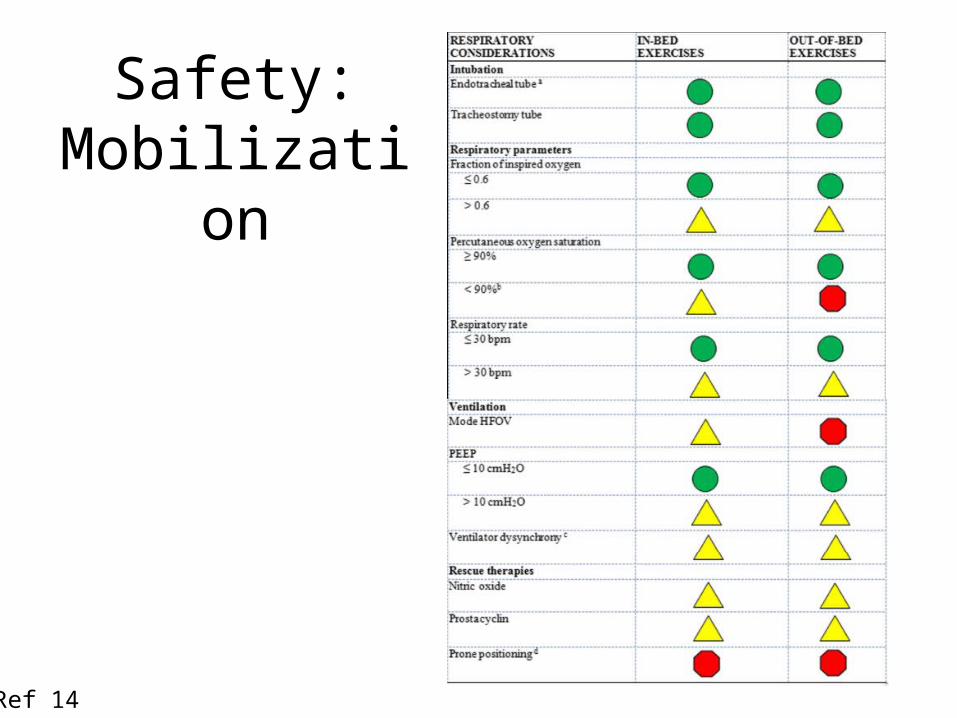
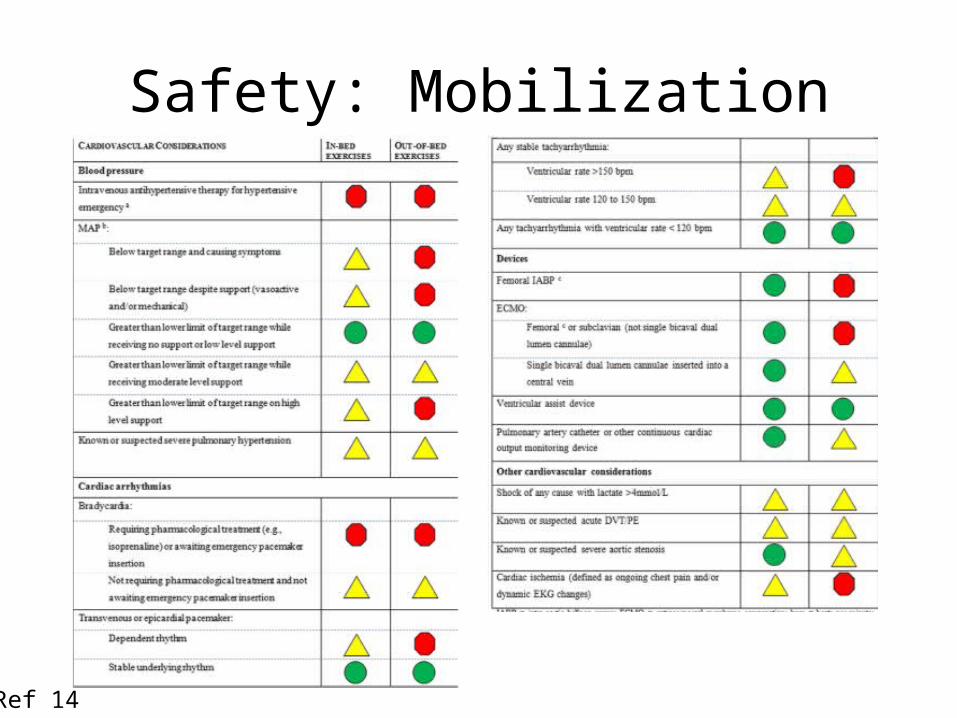
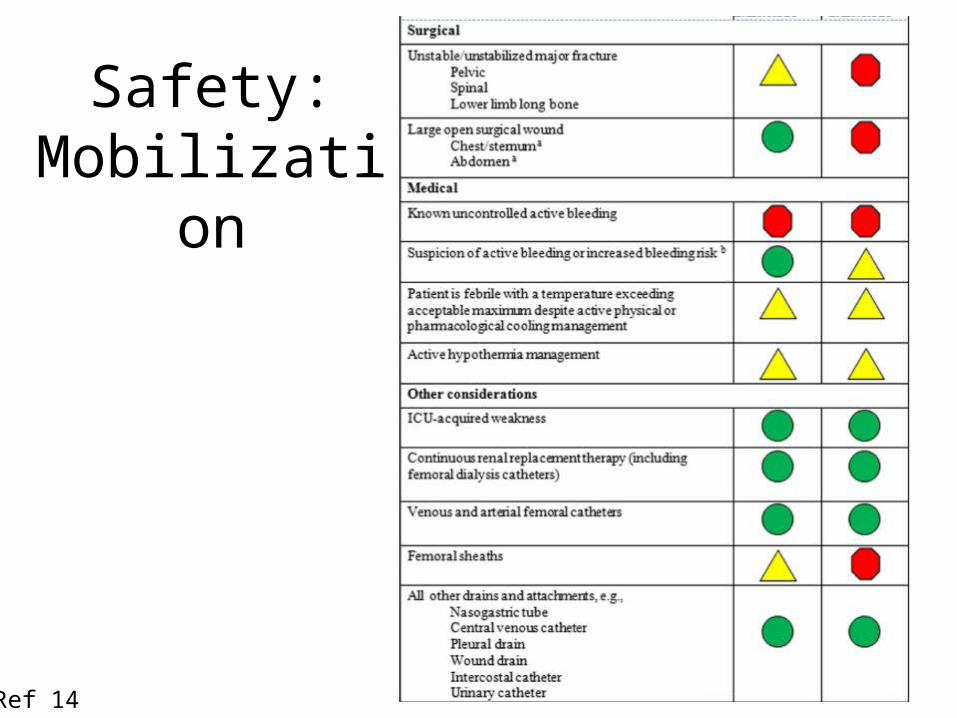
• Consensus guidelines (94 clinicians): Dec 2014• Active mobility:
– “any activity where the patient assists with the activity using their own muscle strength and control: the patient may need assistance from staff or equipment, but they are actively participating in the exercise.”
– Activities included:• Out-of-bed mobilization (i.e. any activity where the patient sits over
the edge of the bed [dangling], stands, walks, marches on the spot or sits out of bed)
• In-bed mobilization (i.e. any activity undertaken whilst the patient is sitting or lying in bed such as rolling, bridging, upper limb weight training).
Ref 14
Safety: Mobilization
Ref 14
Safety: Mobilization
Ref 14
Safety: Mobilization
Ref 14

Safety: Mobilization
Ref 14

Safety: Mobilization
Ref 14
Safety: Mobilization
Ref 14

Safety: Mobilization
• Respiratory– Airway secure– Supplemental O2 if
anticipated need– FiO2 < 0.6
• Cardiovascular– Vasoactive drugs?
• Absolute dose• Changing dose• Clinically well perfused
Ref 14
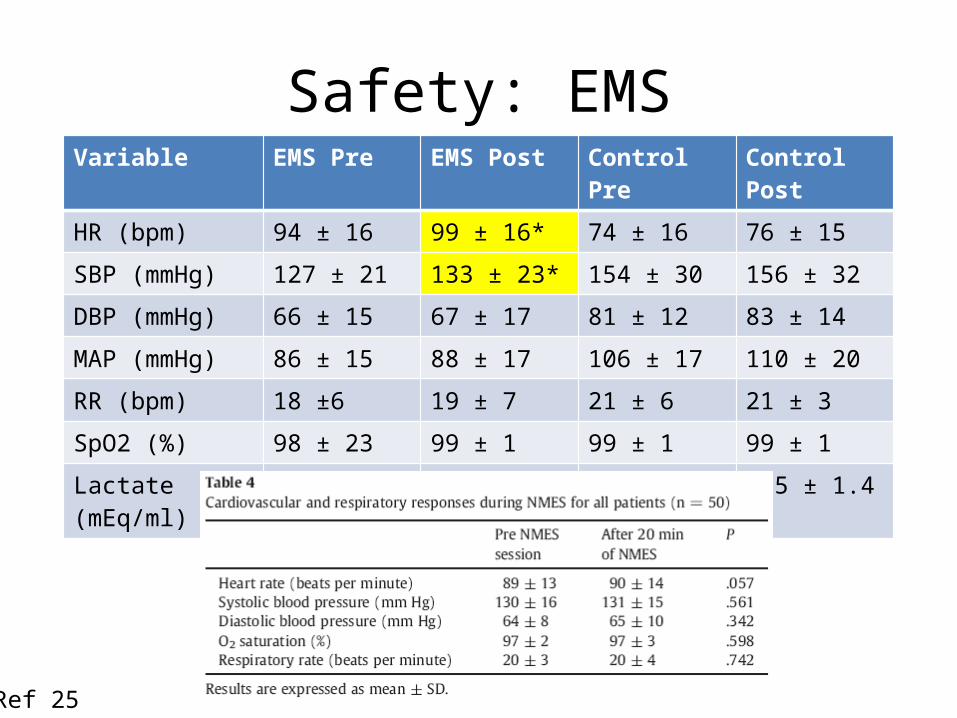
Safety: EMSVariable EMS Pre EMS Post Control Pre Control Post
HR (bpm) 94 ± 16 99 ± 16* 74 ± 16 76 ± 15
SBP (mmHg) 127 ± 21 133 ± 23* 154 ± 30 156 ± 32
DBP (mmHg) 66 ± 15 67 ± 17 81 ± 12 83 ± 14
MAP (mmHg) 86 ± 15 88 ± 17 106 ± 17 110 ± 20
RR (bpm) 18 ±6 19 ± 7 21 ± 6 21 ± 3
SpO2 (%) 98 ± 23 99 ± 1 99 ± 1 99 ± 1
Lactate (mEq/ml) 1.4 ± 0.8 1.3 ± 0.7 1.5 ± 1.1 1.5 ± 1.4
Ref 25

Safety: FES
• Iwatsu et al. (2014)– N = 61– Post-operative cardiovascular patients on inotropic
and/or vasopressor support– No vent, no renal failure/insufficiency, no control– Outcomes:
• No significant changes in BP or HR• No pacemaker malfunction• No increase in ventricular arrhythmia• Atrial fibrillation noted but reported as no different than
anticipated
Ref 16
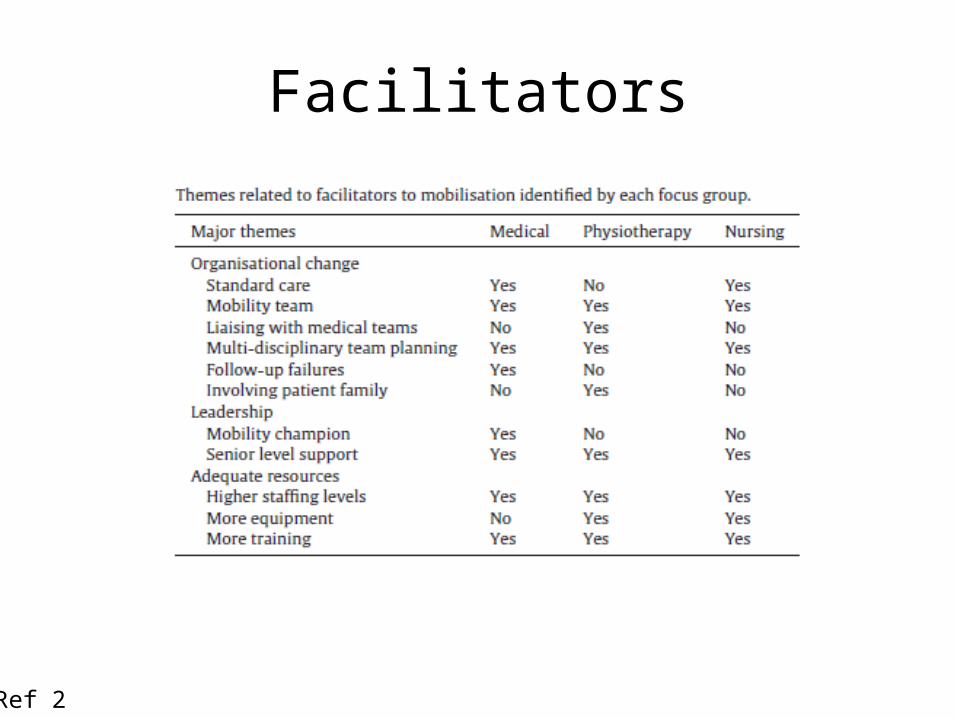
Facilitators
Ref 2

Consult Algorithm
Ref 20

ICU Protocols• Awakening and Breathing Coordination, Delirium
monitoring/management and Early exercise/mobility (ABCDE Bundle)1. spontaneous awakening trials (SATs)2. spontaneous breathing trials (SBTs)3. coordination of components 1 and 2 (so that sedation is held before
the breathing trial begins)4. routine delirium and sedation/agitation screening and management5. early progressive mobilization.
– Each component (except delirium monitoring/ management) is guided by predefined safety screen questions and success/failure criteria derived from RCTs
Ref 1,20
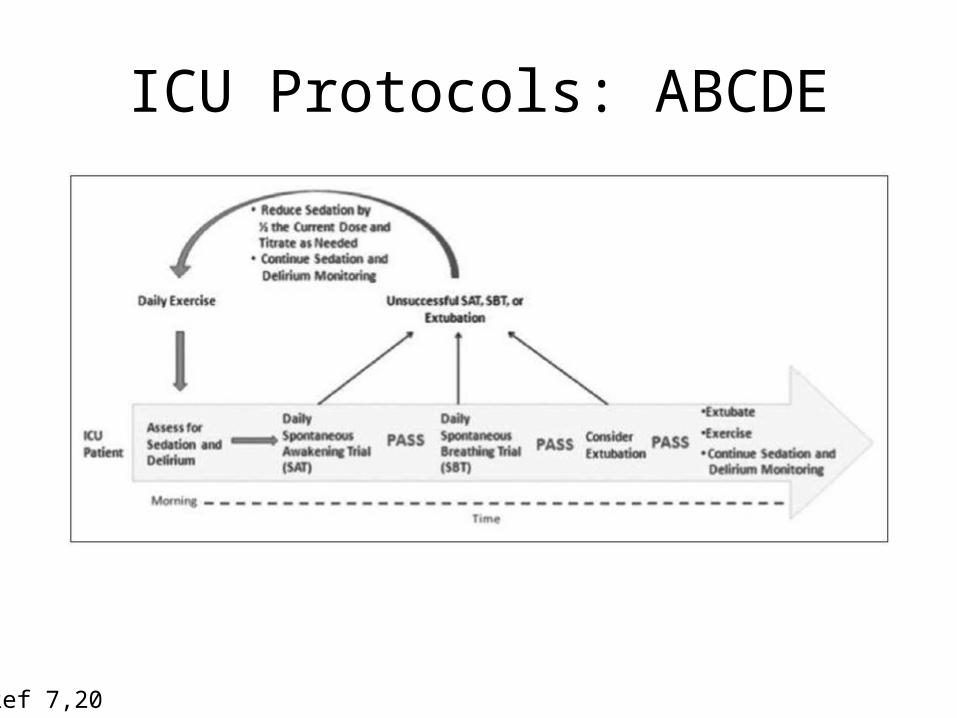
ICU Protocols: ABCDE
Ref 7,20
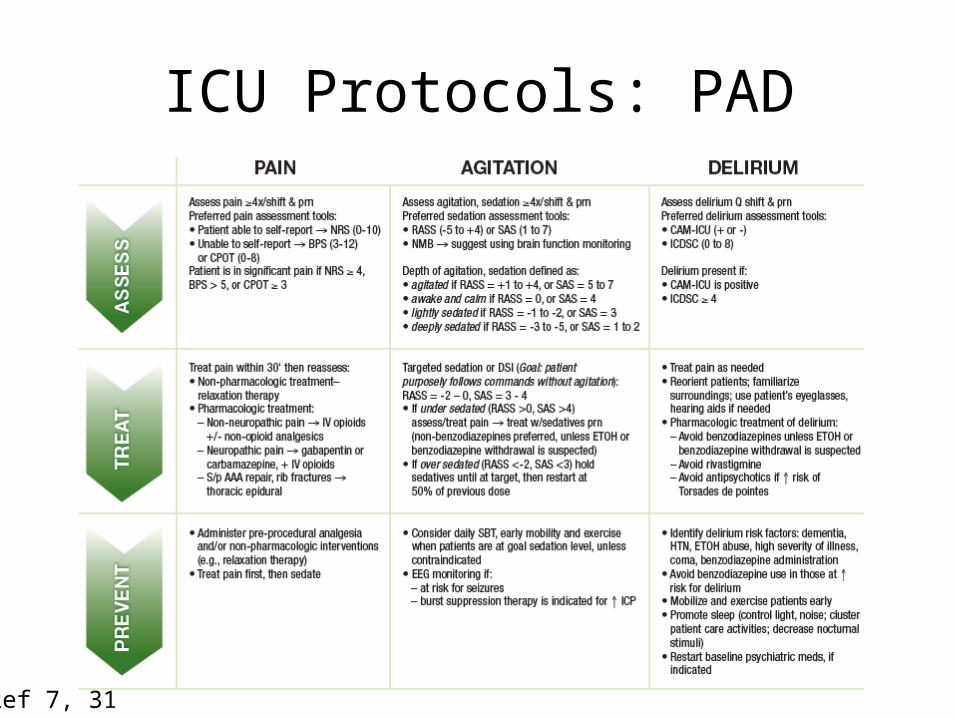
ICU Protocols: PAD
Ref 7, 31
Future Directions
• Improved method of diagnosis for ICU-AW• Determination of who benefits and resource
utilization• Standardized intervention trials• Prior disability and outcomes• Cognitive and psychological rehab• Pediatrics!
Ref 9
Summary
• ICU-AW is generalized, symmetric weakness defined by MRC < 48 with no attributable cause other than critical illness
• Many challenges to assessing for ICU-AW based on current measures
• ICU-AW leads to functional deficits• Inconsistent protocols lead to difficulty
interpreting results of interventions• Safe mobilization can be achieved
References1. Balas MC, et al. Implementing the ABCDE Bundle into everyday care: Opportunities, challenges and lessons learned for implementing the ICU Pain,
Agitation and Delirium (PAD) guidelines. Crit Care Med 2013 Sept;41(901):S116-S127.2. Barber EA, et al. Barriers and facilitators to early mobilisation in intensive care: A qualitative study. Aust Crit Care 2014;
http://dx.doi.org/10.1016/j.aucc.2014.11.0013. Brummel NE, et al. A combined early cognitive and physical rehabilitation program for people who are critically ill: the activity and cognitive therapy in
the intensive care unit (ACT-ICU) trial. Phys Ther 2012;92:1580-1592.4. Burtin C, et al. Early exercise in critically ill patients enhances short-term functional recovery. Crit Care Med 2009 Sep;37(9):2499-505.5. Clavet H, Hebert PC, Fergusson D, Doucette S, Trudel G. Joint contracture following prolonged stay in the intensive care unit. CMAJ 2008 Mar;178(6):691-
7.6. Clavet H, Doucette S, Trudel G. Joint contractures in the intensive care unit: quality of life and function 3.3 years after hospital discharge. Disabil Rehabil.
2014 May 2:1-7. [Epub ahead of print]7. DavidsonJE, et a. Implementation of the pain, agitation, and delirium clinical practice guidelines and promoting patient mobility to prevent post-intensive
care syndrome. Crit Care Med 2013;41:S136-S145.8. De Jonghe B, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA 2002 Dec 11;288(22):2859-67.9. Fan E, et al. An official American Thoracic Society clinical practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. Am J Respir
Crit Care Med 2014 Dec 15;190(12):1437-1446.10. Fan E, et al. Physical complications in acute lung injury survivors: a two-year longitudinal prospective study. Crit Care Med 2014 Apr;42(4):849-59.11. Griffiths RD, Palmer TEA, Helliwell T, MacLennan P, MacMillan RR. Effect of passive stretching on the wasting of muscle in the critically ill. Nutrition
1996;12:297-99.12. Haas JS, et al. Factors influencing physical functional status in intensive care unit survivors two years after discharge. BMC Anes 2013;13:11.13. Hermans G, et al. Acute outcomes and 1-year mortality of intensive care unit-acquired weakness: a cohort study and propensity-matched analysis. Am J
Respir Crit Care Med 2014 Aug;190(4):410-20.14. Hodgson CL, et al. Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Critical
Care 2014;18:658.15. Hough CL, Lieu BK, Caldwell ES. Manual muscle strength testing of critically ill patients: feasibility and interobserver agreement. Critical Care 2011;15:R4316. Iwatsu K, et al. Feasibility of neuromuscular electrical stimulation immediately after cardiovascular surgery. Arch Phys Med Rehabil2015;96:63-8.17. Jackson JC, et al. Depression, post-traumatic stress disorder, and functional disability in survivors of critical illness in the BRAIN-ICU study: a longitudinal
cohort study. Lancet Respir Med 2014;2:369-79.
References18. Kho ME, et al. Neuromuscular electrical stimulation in mechanically ventilated patients: a randomized, sham-controlled pilot trial
with blinded outcome assessment. J Crit Care 2014, http://dx.doi.org/10.1016/j.jcrc.2014.09.014.19. Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. N Engl J Med 2014;370:1626-35.20. Mendez-Tellez PA, Nusr R, Feldman D, Needham DM. Early physical rehabilitation in the ICU: a review for the neurohospitalist. The
Neuroohospitalist 2012;2(3):96-105.21. Morandi A, Brummel NE, Ely EW. Sedation, delirium and mechanical ventilation: the ‘ABCDE’ approach. Curr Opin Crit Care. 2001
Feb;17(1):43-9.22. Parry SM, et al. Functional electrical stimulation with cycling in the critically ill: a pilot case-matched control study. J Crit Care
2014(29):695e1-695e7.23. Parry SM, et al. Electrical muscular stimulation in the intensive care setting: a systematic review. Crit Care Med 2013
Oct;41(10):2406-18.24. Schweikert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically venitlated, critically ill
patients: a randomized controlled trial. Lancet 2009;373(9678):1874-82.25. Segers J, et al. Feasibility of neuromuscular electrical stimulation in critically ill patients. J Crit Care 2014;29:1082-1088.26. Sricharoenchai T, et al. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110
intensive care unit admissions. J Crit Care 2014;29:395-400.27. Stevens RD, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med
2009;37(Suppl.):S299-S308.28. Trudel G, Uhthoff HK. Contractures secondary to immobility: is the restriction articular or muscular? An experimental longitudinal
study in the rat knee. Arch Phys Med Rehabil 2000;81:6-13.29. Wieske L, et al. Early prediction of intensive care unit-acquired weakness using easily available parameters: a prospective
observaional study. PLoS ONE 2014;9(10): e111259.
30. http://www.sccm.org/Communications/Pages/CriticalCareStats.aspx31. http://www.iculiberation.org/SiteCollectionDocuments/Guidelines-Pain-Agitation-Delirium-Care-Bundle-Final.pdf


















