The Role of Gene Body Cytosine Modifications in MGMT ... · repairand are highly cytotoxic (5,...
12
Cancer Biology and Signal Transduction The Role of Gene Body Cytosine Modifications in MGMT Expression and Sensitivity to Temozolomide Erika L. Moen 1 , Amy L. Stark 2 , Wei Zhang 4 , M. Eileen Dolan 1,2,3 , and Lucy A. Godley 1,2,3 Abstract The DNA repair protein O 6 -methylguanine-DNA methyltransferase (MGMT) is known to play a role in sensitivity to temozolomide. Promoter hypermethylation of MGMT is commonly used to predict low expression levels of MGMT in gliomas, despite observed discordance between promoter methylation and protein levels. Here, we investigated the functional role of gene body cytosine modification in regulating levels of MGMT gene expression and sensitivity to temozolomide. In 91 human glioblastoma samples, we observed significant variation in MGMT expression levels in patients with an unmethylated promoter, with higher levels of gene body cytosine modification correlating with higher gene expression levels. Furthermore, inducing hypomethylation across the MGMT gene body with decitabine corresponded with decreased levels of MGMT gene expression in lymphoblastoid and glioblastoma cell lines, indicating an important functional role for gene body cytosine modifications in maintaining gene expression. We reasoned that the decrease in MGMT expression induced by decitabine may render resistant glioblastoma cell lines more sensitive to temozolomide. Consistent with this reasoning, we found that the MGMT-expressing glioblastoma cell lines exhibiting an unmethylated MGMT promoter that were pretreated with decitabine became significantly more sensitive to temozolomide. Overall, our results suggest a functional role for gene body cytosine modification in regulating gene expression of MGMT and indicate that pretreating patients whose tumors have an unmethylated MGMT promoter with decitabine before temozolomide treatment may increase their response to therapy. Mol Cancer Ther; 13(5); 1334–44. Ó2014 AACR. Introduction The O 6 -methylguanine-DNA methyltransferase (MGMT) gene encodes for a DNA repair protein that repairs O 6 - alkylguanine-DNA adducts (1). This type of DNA damage can occur after certain environmental exposures, such as tobacco-specific nitrosamines, and from DNA alkylating agents used for chemotherapy (2, 3). Temozolomide is an alkylating agent that was FDA approved to treat brain tumors in 2005, including anaplastic astrocytoma and glioblastoma multiforme, the most aggressive form of brain cancer (4). Only 5% to 10% of the methylation adducts on DNA resulting from temozolomide treatment are O 6 -methylguanine, but if MGMT is not present to repair the damage, these adducts trigger DNA mismatch repair and are highly cytotoxic (5, 6). Upon repair, MGMT is irreversibly inactivated, thereby requiring new protein synthesis for additional repair (7). Consequently, epige- netic alterations that affect transcriptional activity of MGMT, such as promoter hypermethylation, can have a significant effect on the number of O 6 -guanine lesions that are repaired (8, 9). Patients with gliomas with an aberrantly hypermethylated MGMT promoter respond better to temozolomide treatment compared with patients with an unmethylated MGMT promoter, because they lack MGMT protein expression (10, 11). Although approximately 40% to 70% of patients with gliomas have a methylated MGMT promoter (9, 12–14), promoter methylation does not always show a strong correlation with MGMT protein levels (13, 15). For example, one study investigating the correla- tion between MGMT promoter methylation and protein levels showed that 7 of 40 gliomas had an unmethylated promoter yet no detectable MGMT protein, and 16 of 40 gliomas had aberrant methylation at the promoter yet still had detectable MGMT protein (13). Therefore, additional mechanisms of transcriptional and translational regulation are likely affecting expression of MGMT. The role of gene body cytosine methylation and hydro- xymethylation in regulating gene expression levels is not fully understood, but several studies have observed a positive correlation between gene body cytosine modifi- cations and gene expression levels (16–18). For MGMT in particular, gene body methylation was first shown to correlate with gene expression levels in 1992 (19). Two Authors' Affiliations: 1 Committee on Cancer Biology, 2 Department of Medicine, and 3 Comprehensive Cancer Center, The University of Chicago; and 4 Institute of Human Genetics, University of Illinois, Chicago, Illinois Note: Supplementary data for this article are available at Molecular Cancer Therapeutics Online (http://mct.aacrjournals.org/). Corresponding Authors: Lucy Godley, Room 7124, 900 E. 57th St., Chicago, IL 60637. Phone: 773-702-4140; Fax: 773-702-9268; E-mail: [email protected]; and M. Eileen Dolan, [email protected] doi: 10.1158/1535-7163.MCT-13-0924 Ó2014 American Association for Cancer Research. Molecular Cancer Therapeutics Mol Cancer Ther; 13(5) May 2014 1334 on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924
Transcript of The Role of Gene Body Cytosine Modifications in MGMT ... · repairand are highly cytotoxic (5,...

Cancer Biology and Signal Transduction
The Role of Gene Body Cytosine Modifications in MGMTExpression and Sensitivity to Temozolomide
Erika L. Moen1, Amy L. Stark2, Wei Zhang4, M. Eileen Dolan1,2,3, and Lucy A. Godley1,2,3
AbstractThe DNA repair protein O6-methylguanine-DNA methyltransferase (MGMT) is known to play a role in
sensitivity to temozolomide. Promoter hypermethylation of MGMT is commonly used to predict low
expression levels of MGMT in gliomas, despite observed discordance between promoter methylation and
protein levels. Here, we investigated the functional role of gene body cytosinemodification in regulating levels
ofMGMT gene expression and sensitivity to temozolomide. In 91 human glioblastoma samples, we observed
significant variation inMGMT expression levels in patientswith anunmethylated promoter,with higher levels
of gene body cytosine modification correlating with higher gene expression levels. Furthermore, inducing
hypomethylation across theMGMT gene body with decitabine corresponded with decreased levels ofMGMT
gene expression in lymphoblastoid and glioblastoma cell lines, indicating an important functional role for gene
body cytosine modifications in maintaining gene expression. We reasoned that the decrease in MGMT
expression induced by decitabinemay render resistant glioblastoma cell linesmore sensitive to temozolomide.
Consistent with this reasoning, we found that the MGMT-expressing glioblastoma cell lines exhibiting an
unmethylated MGMT promoter that were pretreated with decitabine became significantly more sensitive to
temozolomide. Overall, our results suggest a functional role for gene body cytosine modification in regulating
gene expression ofMGMT and indicate that pretreating patients whose tumors have an unmethylatedMGMT
promoter with decitabine before temozolomide treatment may increase their response to therapy.Mol Cancer
Ther; 13(5); 1334–44. �2014 AACR.
IntroductionThe O6-methylguanine-DNA methyltransferase (MGMT)
gene encodes for a DNA repair protein that repairs O6-alkylguanine-DNA adducts (1). This type of DNA damagecan occur after certain environmental exposures, such astobacco-specific nitrosamines, and from DNA alkylatingagents used for chemotherapy (2, 3). Temozolomide is analkylating agent that was FDA approved to treat braintumors in 2005, including anaplastic astrocytoma andglioblastoma multiforme, the most aggressive form ofbrain cancer (4). Only 5% to 10% of the methylationadducts on DNA resulting from temozolomide treatmentare O6-methylguanine, but if MGMT is not present torepair the damage, these adducts trigger DNA mismatchrepair and are highly cytotoxic (5, 6). Upon repair, MGMT
is irreversibly inactivated, thereby requiring new proteinsynthesis for additional repair (7). Consequently, epige-netic alterations that affect transcriptional activity ofMGMT, such as promoter hypermethylation, can have asignificant effect on the number ofO6-guanine lesions thatare repaired (8, 9). Patientswith gliomaswith an aberrantlyhypermethylated MGMT promoter respond better totemozolomide treatment compared with patients with anunmethylatedMGMT promoter, because they lackMGMTprotein expression (10, 11). Although approximately 40%to 70% of patients with gliomas have a methylatedMGMTpromoter (9, 12–14), promotermethylationdoesnot alwaysshow a strong correlation with MGMT protein levels(13, 15). For example, one study investigating the correla-tion between MGMT promoter methylation and proteinlevels showed that 7 of 40 gliomas had an unmethylatedpromoter yet no detectable MGMT protein, and 16 of 40gliomas had aberrant methylation at the promoter yet stillhad detectable MGMT protein (13). Therefore, additionalmechanisms of transcriptional and translational regulationare likely affecting expression of MGMT.
The role of gene body cytosine methylation and hydro-xymethylation in regulating gene expression levels is notfully understood, but several studies have observed apositive correlation between gene body cytosine modifi-cations and gene expression levels (16–18). ForMGMT inparticular, gene body methylation was first shown tocorrelate with gene expression levels in 1992 (19). Two
Authors' Affiliations: 1Committee on Cancer Biology, 2Department ofMedicine, and 3Comprehensive Cancer Center, The University of Chicago;and 4Institute of Human Genetics, University of Illinois, Chicago, Illinois
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Corresponding Authors: Lucy Godley, Room 7124, 900 E. 57th St.,Chicago, IL 60637. Phone: 773-702-4140; Fax: 773-702-9268; E-mail:[email protected]; and M. Eileen Dolan,[email protected]
doi: 10.1158/1535-7163.MCT-13-0924
�2014 American Association for Cancer Research.
MolecularCancer
Therapeutics
Mol Cancer Ther; 13(5) May 20141334
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

years later, it was demonstrated that glioma cell lineswithlower expression of MGMT tend to have a more highlymethylated promoter and low levels of methylation alongthe gene body compared with glioma cell lines showinghigher levels ofMGMT expression (8, 19). However, thesestudies have only shown correlation, and the field hasbeen focused primarily on methylation of the promoterregion after it was shown to predict survival amongpatients with glioblastoma. It remains unclear whethermodulationof genebody cytosinemodificationswouldbesufficient to disrupt gene expression levels without anychange in the status of cytosine modification in the pro-moter region.We hypothesized that incorporating gene body cytosine
modification levels in models of temozolomide responsemay lead to better prediction of MGMT expression levelsand, more importantly, improved methods of predictionfor temozolomide response in patients with glioma. In thisstudy, we used lymphoblastoid cell lines, glioblastomacell lines, and human glioblastoma tissue data from TheCancer Genome Atlas (TCGA) to investigate the role ofgene body cytosine modification in regulating MGMTexpression levels and sensitivity to temozolomide.
Materials and MethodsCell lines and reagentsLymphoblastoid cell lines were cultured in RPMI sup-
plemented with 15% FBS and 1% L-glutamine at 37�C.Confirmation of cell line identities for the lymphoblastoidcell lines is described previously (18). The glioblastomacell line U118MG (HTB-15) was purchased from theAmerican Type Culture Collection (ATCC) in March2013, and was authenticated by ATCC by evaluating theshort tandem repeat (STR) profile. U-87MG and A-172were obtained from Dr. M. Lesniak in February 2013, andT98G was obtained from Dr. B. Yamini in March 2013 atthe University of Chicago and no subsequent authentica-tion was performed on these cell lines. SF-188 wasobtained from Dr. J. Costello at the Neurosurgery TissueBank at University of California, San Francisco, in August2013. These cells were authenticated by UCSF using thePowerPlex16 System (Promega Corp.). Glioblastoma cellswere grown in Dulbecco’s modified Eagle medium(ATCCCatalogNo. 30-2002) supplementedwith 10% FBSand 1% penicillin/streptomycin.
IDH1/2 genotypingAll 6 glioblastoma cell linesweregenotyped for the IDH1
and IDH2 mutations. Primers for IDH1 (R132) are asfollows: forward-GGTGGCACGGTCTTCAGAG, reverse-ATGTGTTGAGATGGACGCCT. Primers for IDH2 (R140and R172) are as follows: forward-TTCTGGTTGA-AAGATGGCGG, reverse-GGATGGCTAGGCGAGGAG.Genomic DNA was PCR-amplified using Platinum HiFiTaq polymerase (Life Technologies) under the followingconditions: initial denaturation at 94�C for 2minutes, 94�Cfor 30 seconds, 62�C for 30 seconds, and 68�C for 1minutefor 35 cycles, and a final extension at 68�C for 5 minutes.
Drug treatmentCells in a T25 flask were treated with 200 nmol/L
decitabine or vehicle control (H2O) every 24 hours for 5days. At the end of the fifth day, cellswere plated at 10,000cells/well (lymphoblastoid cell lines) or 5,000 cells/well(glioblastoma cell lines) in a 96-well plate, and the remain-der was spun down into 2 pellets and kept at�80�C untilsubsequent DNA and RNA isolation. Twenty-four hoursafter plating, cells were treated with a range of doses oftemozolomide (Sigma Aldrich): 0, 50, 100, 200, 500, 750,and 1,000 mmol/L for lymphoblastoid cell lines and 0, 10,50, 100, 500, 1,000, and 2,000 mmol/L for the glioblastomacell lines for a total of 72 hours. AlamarBlue was added 24hours before absorbance reading at wavelengths of 570and 600 nm (Synergy-HT multidetection plate reader;BioTek). The percentage of cells that survived was quan-tified relative to vehicle control wells, and at least 2separate experiments for each glioblastoma cell line wereperformed in technical triplicates for each concentration.To determine the significance of the effect of decitabinepretreatment on temozolomide cytotoxicity, we fit thefollowing linear model: survival ¼ temozolomide dose� decitabine, where decitabine is 1 for decitabine pre-treatment and 0 for vehicle control. This model wascompared with a baseline model without the interactionterm using ANOVA to determine if the interactionbetween decitabine and temozolomide dose was signifi-cant. The linearmodelswere fit using the lm function in R.
Bisulfite sequencingDNAwas isolated fromwhole cell lysates using phenol–
chloroform, and genomic DNA was treated with sodiumbisulfite (20). For bisulfite PCR amplification, primers(Supplementary Table S1) were designed to amplify�250 base pair fragmentswithin theMGMT promoter andgene body that included CpG sites interrogated by theIllumina InfiniumHumanMethylation450Beadchip (450Karray) aswell as adjacentCpGs. Primers for theCpG islandin the promoter region were designed and optimized in aprevious publication (21). ZymoTaq polymerase (ZymoResearch) was used for PCR amplification at the indicatedtemperatures, according to manufacturer’s instructions.For the glioblastoma cell lines, the PCR product was TAcloned using the TOPO Cloning Kit (Invitrogen), and atleast 10 clones per condition were sequenced. Lympho-blastoid cell lines were sequenced by bulk sequencing ofthe PCR product. DNA sequencing was performed at TheUniversity of Chicago Sequencing Core Facility.
Quantitative real-time PCRTotal RNA was extracted from 1 million cells using
TRizol (Life Technologies) following the manufacturer’sprotocol. RNA quality assessment and quantificationwere conducted using the optical spectrometry 260 to280 nm ratio. Subsequently, mRNA was reverse tran-scribed to cDNA using Applied Biosystems High Capac-ity Reverse Transcription Kit (Applied Biosystems).Quantitative RT-PCR (qRT-PCR) was performed for
Cytosine Modifications in MGMT and Temozolomide Sensitivity
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1335
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

MGMT, and huB2M (beta-2-microglobulin) and GAPDH(glyceraldehyde 3-phosphate dehydrogenase) were includedas endogenous controls for lymphoblastoid and glioblas-toma cell lines, respectively, using TaqMan Gene Expres-sion Assays on the Applied Biosystems Viia7 RT-PCRsystem.
Statistical analyses of 450K array dataInitial analyses of the 450K array cytosine modification
data (GSE39672) in the CEU and YRI lymphoblastoid celllines are explained in detail previously (18). Level 3 450Karray, exon array, and survival data were downloadedfrom TCGAData Matrix. All 3 datasets were available for91 patients with glioblastoma. All of our analyses ofpatient with TCGA glioblastoma data were performedusing the R statistical software.
K-means clustering was performed using the "kmeans"function in R. K-means clustering aims to divide n obser-vations into k clusters in which each observation belongsto the cluster with the nearest mean, so as to minimize thewithin-cluster sum of squares. A plot of the within clustersum of squares by number of clusters helped us to deter-mine that 3 groupswas the appropriatenumber of clustersto minimize the within-cluster sum of squares for clus-tering our data. After 3 groups, the within-group sum ofsquares plateaus, so increasing the number of groupswould not significantly decrease the within-group sumof squares (Supplementary Fig. S1).
ResultsA temozolomide-associated SNP is a modifiedcytosine quantitative trait locus for MGMT genebody cytosine modification levels
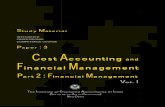
Our group has generated 450K array data for 60 Cau-casian (CEU) and 73 African (YRI) lymphoblastoid celllines (18). This array requires bisulfite-modifiedDNA, andmodified cytosines, both 5-methylcytosine (5-mC) and 5-hydroxymethylcytosine (5-hmC), are distinguished fromunmodified cytosines using this technique (22). Our anal-ysis of cytosine modification and gene expression levelsrevealed that the averaged levels of cytosine modificationwithin the gene body of MGMT were strongly positivelycorrelated at genome-wide significance with gene expres-sion levels (P < 5.3 � 10�12; Fig. 1A). Thus, we aimed toinvestigate the biological function of gene body cytosinemodification in regulatingMGMT transcription andhow itmay affect sensitivity to temozolomide. Interestingly, arecent genome-wide association study of temozolomidesensitivity in a cohort of Caucasian lymphoblastoid celllines identified several SNPs in high linkage disequilibri-um within the gene body of MGMT to be significantlyassociated with cellular sensitivity to temozolomide (23).Themost significant SNP they identifiedwas anexpressionquantitative trait locus (QTL) forMGMT expression, but itwas not correlated with promoter methylation levels intheir lymphoblastoid cell line cohort. We hypothesizedthat the most significant temozolomide-associated SNPand MGMT expression quantitative trait locus (rs477692)
identified in that study would be associated with genebody cytosine modification levels in our cohort of Cauca-sian (CEU) lymphoblastoid cell lines.
First, we validated that the SNP was an expressionquantitative trait locus for MGMT in our Caucasian lym-phoblastoid cell lines (P ¼ 0.004; Fig. 1B). We did notobserve this SNP to be an expression quantitative traitlocus for MGMT expression in the African (YRI) lympho-blastoid cell lines (P ¼ 0.6), suggesting different geneticpredictors ofMGMTexpressionbetween the2populations.Furthermore,we found that this SNP is amodified cytosineQTL (mQTL) for the averaged levels ofMGMT gene bodycytosine modification (Fig. 1C). We also analyzed the SNPagainst each CpG within MGMT individually (n ¼ 94)using a linear model in the Caucasian lymphoblastoid celllines, and identified 5 CpGs that were significantly associ-atedwith expression atP< 0.05 after correcting formultipletesting. We performed bisulfite sequencing around 3 ofthese CpGs to demonstrate technical validation of theassociation using a separate methodology (SupplementaryFig. S2). From these results, we hypothesized that MGMTgene body cytosine modification levels are functionallyimportant in regulatingMGMT expression, thereby effect-ing cellular sensitivity to temozolomide.
Cytosinemodification levels are correlatedacross thegene body of MGMT
We were interested in determining whether a certainpattern or region of cytosine modification across theMGMT gene would be able to predict gene expressionlevels more precisely than promoter methylation levelsalone. In the Caucasian lymphoblastoid cell lines, a cor-relation matrix including all CpGs across the promoterregion and gene body showed that the gene body cytosinemodifications were positively correlated with each other,and theywere slightly negatively correlatedwith CpGs inthe promoter region (Fig. 1D). Across the gene body, thereare several regions that show higher association withexpression than others. Using a backward eliminationregression model (24), we were able to identify 4 CpGs,whichwere all locatedwithin the second intron, that couldexplain 69% of the variance in expression levels in theCaucasian lymphoblastoid cell lines (Fig. 1D marked byasterisks and Table 1). When we performed a backwardselimination regression model using the African lympho-blastoid cell lines,wewere able to identify 3CpGs, 1 in thepromoter and 2 in the second intron, that could explain29% of the variance in expression levels (Table 1). There-fore, in Caucasian and African lymphoblastoid cell lines,the second intron,which spansmore than 171 kb, containsseveral CpGs whose cytosine modification levels are sig-nificantly associated with expression levels of MGMT.
Gene body cytosine modification levels predictMGMT expression levels in patients withglioblastoma with an unmodified MGMT promoter
We next investigated whether MGMT gene body cyto-sine modification levels were correlated with gene
Moen et al.
Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics1336
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

expression levels in human glioblastoma samples. Weobtained the 450K array, expression, and survival datafor 91 glioblastoma samples from TCGA. To determinewhether a certain pattern of cytosine modification acrossthe entire gene was predictive of MGMT expression orpatient survival, we performed K-means clustering togroup the patients into 3 groups based on similar cytosinemodification patterns across the MGMT promoter andgene body (Fig. 2A). Our rationale for clustering thepatients into 3 groups is described in Methods and in
Supplementary Fig. S1. Group 1 patients (black circles)had the highest levels of cytosine modification across thegene body, with themean b value for all CpGs being 0.803(80.3% modified). This group has the highest levels ofgene expression compared with the other 2 groups (Fig.2B). Group 2 (gray circles) hadmoderate levels of cytosinemodification across the gene body, with the mean b valuefor all CpGs being 0.702 (70.2%modified; Fig. 2A). Group3 (white circles) had the lowest levels of cytosine modi-fication across the gene body,with themean b value for all
0.5
0.0
–0.5
–1.0
0.5
0.0
–0.5
–1.0
3
2
1
00 1 2 3CC C
TTT
TTCT
CC
Averaged levels of MGMT gene body cytosine modification rs477692 rs477692
rs477692Promoter
0
4
8
12
-lo
g1
0 P
va
lue
wit
h
ex
pre
ss
ion
MG
MT
ex
pre
ss
ion
MG
MT
ex
pre
ss
ion
Ge
ne
bo
dy
cy
tos
ine
mo
dif
ica
tio
n
P < 5.3e-12 r2 = 0.58
P = 0.004 P = 0.01
*
*
**
–1
–0.8
–0.6
–0.4
–0.2
0.2
0.4
0.6
0.8
1
0
A B C
D
Figure 1. MGMT gene body cytosine modification is positively correlated with gene expression levels in lymphoblastoid cell lines. A, MGMT expression ispositively correlated with the averaged levels of cytosine modification across the gene body. B, a temozolomide-associated SNP (rs477692) is anexpression quantitative trait locus for MGMT gene expression levels in the CEU HapMap lymphoblastoid cell lines. C, a temozolomide-associated SNP(rs477692) is amQTL forMGMT gene body cytosine modification levels in CEUHapMap lymphoblastoid cell lines. D, cytosine modifications across the genebody are positively correlatedwith eachother andnegatively correlatedwith the promoter region. Gray bars, the�log10P value of the association of eachCpGwith expression. Starred bars indicate the CpGs that, together, explain 69% of the variance of MGMT expression in CEU lymphoblastoid cell lines.
Cytosine Modifications in MGMT and Temozolomide Sensitivity
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1337
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

CpGs being 0.460 (46.0%modified; Fig. 2A). These groupswere not predictive of survival, which may be a result ofthe significant number of the patients with glioblastomawho were lost to follow-up (Supplementary Fig. S3).
As expected, cytosine modification within the genepromoter was negatively associatedwith gene expression(Fig. 2C). However, we observed a significant amount ofvariation in expression levels among patients with glio-blastoma with an unmodified promoter (Fig. 2C). Whenanalyzing only patients with an unmodified promoter(averaged b values between 0 and 0.2), we found thatlevels of gene body cytosine modification were linearlycorrelated with expression levels of MGMT (Fig. 2D,right). Hence, among the patients with an unmodifiedpromoter, patientswhohad the lowest levels of gene bodymodification (Group 3) expressed significantly lowerlevels ofMGMT compared with patients with an unmod-ified promoter and high levels of gene body cytosinemodification (Group 1). The patients whose cytosinemodification levels within the promoter averaged to beat least 20%modified (average b value > 0.2) did not showa correlation between gene body cytosine modificationlevels and expression, and, as expected, all groups hadvery low levels of expression (Fig. 2D, left). This suggeststhat disruption of cytosine modification levels across thegene body may introduce variability in expression levelsin patientswhohave anunmodifiedpromoter. To identifywhich CpGs along the gene body contributed most tovariation in expression within patients with an unmod-
ified promoter, we performed backward elimination toidentify 5 CpGs, 1 in the first intron and 4 in the secondintron, that explained 18% of the variation in expression(Table 1).
Decitabine decreasesMGMT expression in cell lineswith an unmethylated MGMT promoter
We next investigated whether hypomethylating theMGMT gene body correlated with reduced gene expres-sion levels. To do so, we treated lymphoblastoid cell linesthat have an unmodified promoter and high levels ofMGMT expression with decitabine, a hypomethylatingagent. After a 5-day treatment with a low dose of decita-bine (200 nmol/L), we examined changes in gene expres-sion and gene body cytosine modification levels. Weincluded 6 lymphoblastoid cell lines that all had relativelyequal baseline levels of MGMT expression and genebody cytosine modification: GM7000, GM7357, GM12005,GM12043, GM12810, andGM12812. After decitabine treat-ment, 3 lymphoblastoid cell lines (GM7357, GM12005, andGM12810) showedadecrease inMGMT expression,whichcorresponded to a decrease in cytosinemodification levelsin the examined regions along the gene body,measured bybisulfite sequencing (Fig. 3A–C, black bars, left). The other3 lymphoblastoid cell lines (GM7000, GM12043, andGM12812) showed no change in expression and experi-enced less hypomethylation across the gene (Fig. 3A–C,white bars, right) after decitabine treatment. These phe-notypes were reproducible over 2 biologic replicates, indi-cating that decitabine was consistently more effective inthe same3 cell lines.Wenoted that the growth rates of the 3lymphoblastoid cell lines that showedhypomethylation ofthe MGMT gene body were faster than the other 3 lym-phoblastoid cell lines. It is thought that decitabine isdependent on cell division (25), and the cells that dividemore frequently will incorporatemore of the drug into thenascent DNA strand. Thus, the difference in MGMT genebody hypomethylation and expression observed betweenthese 2groups is likelybecauseof thedifferences in cellulargrowth rate. The unmethylated MGMT promoter statusremained completely unchanged among the lymphoblas-toid cell lines that showedadecrease inMGMT expression,confirming that the change in gene expression was notbecause of changes within the promoter (SupplementaryFig. S4).
We also tested this observation in 5 glioblastoma celllines. We obtained 2 glioblastoma cell lines that had highexpression levels ofMGMT (T98G and SF188), 1 glioblas-toma cell line with low expression of MGMT (U118MG),and 2 glioblastoma cell lines with no MGMT expressionbecause of promoter hypermethylation (U87MG andA172). It has been reported that IDH1/2 mutation statusis associated with distinct methylation and hydroxy-methylation patterns (26–28), so we genotyped all 6 celllines for IDH1 and IDH2 mutations and found that theywere all wild-type for both. Therefore, IDH1/2 mutationscould not explain changes in cytosine modificationsbetween these cell lines.
Table 1. Certain gene bodyCpGs explain a highproportion of variance of MGMT expressionlevels
Population CpGs r2 P value
CEU cg11309842 0.69 1.13 � 10�13
cg18502933cg06179303cg14485787
YRI cg14194875 0.29 9.73 � 10�5
cg18651291cg19680672
Patients withglioblastoma withan unmodifiedpromoter
cg25394042 0.18 0.001cg14485787cg26976729cg25063211cg24755725
NOTE: Backward elimination regression identifies 4 CpGsthat explain 69%of variation and 3CpGs that explain 29%ofvariation ofMGMT expression levels in the Caucasian (CEU)and African (YRI) populations, respectively. In patients withglioblastoma with an unmodified promoter, 5 CpGs wereidentified that explain 18% of the variance in expressionlevels, calculated using Spearman correlation backwardelimination.
Moen et al.
Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics1338
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

We observed that a 5-day treatment of low-dose deci-tabine (200 nmol/L) resulted in a significant decrease inMGMT expression inT98G, SF188, andU118MG(Fig. 4A).
This correlated with loss of modified cytosines acrossregions of the gene body ofMGMT, measured by bisulfitesequencing (Fig. 4B). Conversely, U87MG and A172 have
MGMT (300.82 kb)
5E 4E3noxE2noxE1noxE
β V
alu
e
A
MGMT expression
Cp
G isla
nd
ave
rag
e β
va
lue
r = –0.61
P < 2.2e–16
MG
MT
exp
ressio
n
Group 1 Group 2 Group 3
All patients
Group 1 Group 2 Group 3
MG
MT
exp
ressio
n
Patients with a modified promoter
n = 8n = 9
n = 16
Patients with an unmodified promoter
n = 50 n = 4
n = 4
Group 1 Group 2 Group 3
P = 0.007
CB
D
Group 1
Group 2
Group 3
–3
–3
–2
–1
01
–2
–1
01
0.1
0.2
0.3
0.4
0.5
0.6
–3 –2 –1 0 1
131300000 131350000 131400000 131500000131450000 131550000
Figure 2. MGMT gene body cytosine modification levels predict expression levels in patients with glioblastoma with an unmodified MGMT promoter.A, K-means clustering of cytosine modification patterns alongMGMT in 91 TCGA patients with glioblastoma. Group 1 patients (black) have the highest levelsof modification across the gene body, Group 2 patients (gray) have intermediate levels of modification across the gene body, and Group 3 patients(white) have the lowest levels ofmodification across the gene body. B, Group 1 patients have higher levels of gene expression comparedwith Groups 2 and 3.C, cytosine modification within the promoter is negatively correlated with gene expression. Patients with an unmodified promoter (b value between 0and 0.2, denoted by dotted line) still show significant variation in expression levels. D, MGMT gene body cytosine modification levels predict expressionin patients with glioblastoma with an unmodified promoter but not patients with a modified promoter.
Cytosine Modifications in MGMT and Temozolomide Sensitivity
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1339
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

a methylated promoter, and decitabine treatment couldtherefore hypomethylate the promoter and increaseMGMT expression. In U87 and A172, we observed somehypomethylation of the promoter region after decitabinetreatment (P < 0.05; Supplementary Fig. S5). U87 experi-enced a very small increase in MGMT expression, yetA172 experienced no increase in MGMT expression (Fig.4C). This suggests that increased hypomethylation and/or other factorsmay be required for reactivation ofMGMTexpression in these cell lines.
Pretreatment with decitabine sensitizes MGMT-expressing glioblastoma cell lines to temozolomide
A significant clinical problem is that patients withglioblastoma whose tumors express MGMT, typicallywith an unmethylated MGMT promoter, respond poorlyto temozolomide, which is the drug of choice in thisdisease. To determine whether the decrease in MGMTexpression observed in the decitabine-treated glioblasto-ma cell lines is sufficient to sensitize the cells to temozo-lomide, we pretreated the glioblastoma cell lines withdecitabine to determine the effect on cellular sensitivityto temozolomide. The cells were treated with 200 nmol/Lof decitabine every 24 hours for 5 days and then platedfor a temozolomide dose-curve cytotoxicity assay. T98G,SF188, and U118MG, each of which experienced a de-crease in MGMT expression following the decitabinepretreatment, were significantly more sensitive to temo-zolomide compared with vehicle-treated controls (Fig.5A). Interestingly, decitabine did not affect the sensitivityto temozolomide in either of the cell lines that had amethylatedMGMT promoter (Fig. 5B). This suggests thatthe effectiveness of decitabine pretreatment is more pro-nounced in glioblastoma cell lines that have an unmethy-lated MGMT promoter and are initially resistant totemozolomide.
We also tested the effect of decitabine pretreatment tocellular sensitivity to temozolomide in lymphoblastoidcell lines that showed both no change (GM7000 andGM12812) and a decrease inMGMT expression (GM7357)following decitabine treatment. We observed that none ofthe lymphoblastoid cell lines tested were sensitized totemozolomide (Supplementary Fig. S6). Lymphoblastoidcell lines are noncancerous cells with high levels ofMGMT, which makes them highly resistant to temozolo-mide compared with cancer cell lines, even when thelevels ofMGMT in lymphoblastoid cell lines are reduced.Thus, decitabine pretreatment may increase sensitivity ofcancer cells to temozolomide with no increase in sensi-tivity in normal cells, which would potentially reduceunwanted toxicities during combination treatment.
DiscussionIn this study, we investigated the role of MGMT gene
body cytosine modification in regulating MGMT expres-sion levels. Using primary human glioblastoma datafrom TCGA, we demonstrated that levels of cytosine
B
C
GM7357 GM12005 GM12810 GM7000 GM12043 GM12812
A
MGMT (300.82 kb)
MGMT (300.82 kb)
GM7357 GM12005 GM12810 GM7000 GM12043 GM12812
P = 0.008
P = 1.5e–06
1.5
1.0
0.5
0.0
0.2
0.0
–0.2
–0.4
–0.6
0.2
0.0
–0.2
–0.4
–0.6
M
GM
T e
xp
ressio
n a
fter
DA
C
rela
tive t
o u
ntr
eate
dD
mC
aft
er
DA
C t
reatm
en
tD
mC
aft
er
DA
C t
reatm
en
t
Figure 3. Lymphoblastoid cell lines that show a decrease of MGMTexpression after decitabine treatment are more hypomethylated acrossthe gene body. A, qRT-PCRof 6 lymphoblastoid cell lines after decitabinetreatment, normalized to vehicle-treatedcontrols. Three showadecreasein MGMT expression after decitabine (DAC) treatment (black bars, left)and 3 show no change inMGMT expression (white bars, right). B and C,bisulfite sequencing to measure hypomethylation across a region at thebeginning of intron 2 (B) and a region at the end of intron 2 (C). Eachvertical bar represents a CpG captured by the bisulfite PCR. The degreeof cytosine hypomethylation after decitabine treatment is represented onthe y-axis. P values were calculated using the Student t test.
Moen et al.
Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics1340
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

modification across the MGMT gene body are associatedwith expression levels specifically in patients with anunmodified promoter, and those patients with the lowestlevels of gene body cytosine modification have similarlevels of MGMT expression as those patients with amethylated promoter. Our results may shed light onprevious studies that show discordance between MGMTpromoter methylation and MGMT protein levels (13, 15),at least in the cases where the promoter is unmethylatedyet there is little or no detectable MGMT protein. Anunmethylated promoter leaves the MGMT gene open fortranscription, but additional transcription factors andchromatin states, including histone marks and DNAmethylation and hydroxymethylation, are likely requiredfor transcriptional initiation and elongation. This inter-play between epigenetic modifications and transcriptionfactorsmay contribute to the variation in expression levelsseen in patients with glioblastoma with an unmethylatedpromoter.The importance of gene body cytosine modifications in
regulating gene transcription is not completely under-stood. In fact, the interaction between gene body cytosinemodification and expression may be bi-directional. It hasbeen shown that transcriptional elongation may promoteDNAmethylation along gene bodies (29, 30), whereas theinteraction of 5-mC with histone marks, such asH3K36me3, may be important for transcriptional elonga-tion (29). It is also thought that gene body cytosine mod-
ifications may be important in defining exon–intronboundaries and alternative splicing (31). Furthermore,levels of 5-mC and 5-hmC located within gene bodiesmay have distinct effects on gene expression. A recentstudy demonstrated that, in the brain, the ratio of 5-hmC:5-mC within the gene body is a better predictor ofgene expression than either epigenetic mark on their own(32). We propose that gene body cytosine modificationsmay be one of the factors influencing expression levels ofMGMT, such that when the gene body becomes hypo-methylated, the cell may not be able to successfully tran-scribe the gene even when the transcriptional machineryhas access to the promoter. This implies that, at least in thecase of MGMT, maintaining high levels of cytosine mod-ification along the gene body may be required for the cellto continue to transcribe high levels of the gene. Gaining abetter understanding of the functional importance ofcytosine modifications along the gene body will help usto predict gene expression patterns better, which couldhave implications on downstream phenotypes such asresponse to chemotherapeutic agents.
In addition, previous work by our group investigatingpopulation-specific gene expression patterns has shownthatMGMT is differentially expressed at baseline betweenCaucasian and African lymphoblastoid cell lines, withCaucasians expressing lower levels of MGMT comparedwith Africans (33). However, the overall poor prognosisfor all patients has made it difficult to discern if health
U118
+ DAC
U118
T98G
+ DAC
T98G
P =
0.0
004
CA
B
30 30 30 30 60 30 50 80 100 67 22
100100 100 100 100 100 100 90 90 100 100
.S.
NP
= 7
.3e–13
MGMT (300.82 kb)
*
*
*
42 50 58 42 42 50 42
27 18 27 18 18 18 18
P =
0.0
02
100 9 9 9 9 9 9 9 9 9 9
SF188
+ DAC
SF188
P =
1.8
e–
14
59 41 41 47 47 41 41
35 24 18 18 18 6 24
60 40 50 30 60 70 40 40 80 70 70
73 64 64 73 64 55 82 82 62 73 64
30 40 10 60 80 30 30 50 50 60 10
9283 67 83 9292100
50 58 67 67 75 67 50
P =
6.2
e–
07
0.04
0.03
0.02
0.01
0.00
T98G
SF188
U11
8U87
A17
2
ControlControl
DACDAC
0.00012
0.00008
0.00004
0.00000
MG
MT
mR
NA
rela
tive t
o G
AP
DH
MG
MT
mR
NA
rela
tive t
o G
AP
DH
Figure 4. Glioblastoma cell linesthat express MGMT show adecrease in expression and genebody cytosine modification levelsfollowing decitabine treatment. Aand C, qRT-PCR of MGMTexpression levels in MGMT-expressing glioblastoma cell lines(A) and MGMT-silencedglioblastoma cell lines (C) treatedwith either 200 nmol/L decitabine(DAC) for 5 days or vehiclecontrols. Each bar represents themean of 3 independentexperiments, and error bars denotethe standard deviation of themean.P values were calculated using theStudent t test. �, P < 0.05. B,bisulfite sequencing of 2 regionswithin the gene body of MGMT inMGMT-expression glioblastomacell lines treated with decitabine orvehicle control. Each pie chartrepresents the proportion ofmodified cytosines at a particularCpG, calculated from at least 10clones. P values were calculatedusing a x
2 statistical test. N.S., notsignificant.
Cytosine Modifications in MGMT and Temozolomide Sensitivity
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1341
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

disparities exist betweendifferent ethnic populations (34).Overall, our results indicate that measuring cytosinemodification levels in the gene body in addition to thosein the promoter will more accurately predict MGMTexpression. Importantly, inclusion of gene body cytosinemodification levels may allow for better prediction oftemozolomide response and long-term survival inpatients with glioblastoma. A study of long-term survivalof patients with glioblastoma showed that 8 of 36 ofglioblastoma long-term survivors had an unmethylatedMGMT promoter (35). Our data would suggest that thesepatients would have low MGMT gene body cytosinemodification levels.
The primary model for the mechanism of action ofhypomethylating agents decitabine and azacitidine is thatthey incorporate into DNA to induce global hypomethy-lation by covalently trapping the maintenance methyl-transferase, DNMT1, to the DNA strand (36). Thus, overthe course of cell divisions, the genome becomes hypo-methylated. Several studies have investigated decitabine-induced hypomethylation of promoter regions and haveshown subsequent upregulation of gene expression (37–39). However, decitabine has been shown to induce bothupregulation and downregulation of genes (38, 40). Onestudy investigated genome-wide changes in methylationinduced by decitabine and azacitidine and showed thathypomethylation had a preference for CpGs that were notin CpG islands (41). Gene body CpGs may be frequentlyaffected by decitabine, but the effects on gene expression
may be more subtle than changes in the promoter region,which acts more like an on/off switch. After treatmentwith decitabine, DNMT1may not be able to keep levels ofmethylation high across the MGMT gene body after sev-eral replication events, leading to a decrease in geneexpression. Although this gene may be more dependenton gene body cytosinemodification levels comparedwithother genes, this phenomenon could occur in other genesas well, and may explain why certain genes becomedownregulated following decitabine treatment. Howev-er, because decitabine causes global hypomethylation, wecannot rule out the possibility that treatment with deci-tabine is affecting the expression levels of transcriptionfactors involved inMGMT expression, leading to changesinMGMT expression that are independent of theobservedchanges in gene body methylation levels.
Arecentavenue in current strategies for cancer treatmentis the combination of hypomethylating agents with cyto-toxic chemotherapy to increase response to the chemother-apeutic agent (42–45). The goal of precision medicine is touse patient-specific biomarkers to help determine theirindividualized treatment strategy. In this work, we havedemonstrated that decitabine can be used to sensitizeresistant glioblastoma cell lines with an unmethylatedMGMT promoter status to temozolomide. Importantly, theeffects ofdecitabine seemtobedependenton the changes tothe MGMT expression levels. Cells that express MGMTbecome hypomethylated across the gene body after deci-tabine treatment, corresponding with a decrease in
150
100
50
0
150
100
50
0
150
100
50
0
150
100
50
0
150
100
50
0
0 500 1,000 1,500 2,000 2,500 0 500 1,000 1,500 2,000 2,500 0 500 1,000 1,500 2,000 2,500
0 500 1,000 1,500 2,000 2,500 0 500 1,000 1,500 2,000 2,500
% S
urv
ival
% S
urv
ival
% S
urv
ival
% S
urv
ival
% S
urv
ival
T98G
T98G DAC SF188 DAC
SF188U118MG
U118MG DAC
U87MG DAC
U87MG A172
A172 DAC
Dose TMZ (mmol/L) Dose TMZ (mmol/L) Dose TMZ (mmol/L)
Dose TMZ (mmol/L)Dose TMZ (mmol/L)
A
B
P = 7.96e–06 P = 9.8e–07
P = 1.52e–05
Figure 5. Glioblastoma cell lines that express MGMT are sensitized to temozolomide following decitabine treatment. A, temozolomide cytotoxicity assay ofT98G, SF-188, and U118MG with or without a 5-day pretreatment with 200 nmol/L decitabine (DAC). Each graph represents at least 2 biologic replicatesperformed in technical triplicates. B, temozolomide cytotoxicity assay of U87MG and A172 with or without a 5-day pretreatment with 200 nmol/L decitabine.Each graph represents at least 2 biologic replicates performed in technical triplicates.
Moen et al.
Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics1342
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

expression levels and an increase in temozolomide sensi-tivity. However, cells with a hypermethylated MGMTpromoter are not sensitized further to temozolomide fol-lowingdecitabine pretreatment.AlthoughMGMTpromot-er methylation status is one of the most requested molec-ular assays in clinical neuro-oncology, there are few ther-apeutic alternatives to temozolomide for patients with anunmethylated MGMT promoter even though it has beenshown that those patients are less likely to respond totreatment (46). In fact, many of the other agents used totreat brain tumors such as carmustine (BCNU), streptozo-tocin, and dacarbazine also form O6-alkylguanine DNAadducts that are repaired by MGMT (5). Therefore, ourstrategy of combining decitabinewould likely be beneficialwith these other agents. In addition, MGMT promotermethylation status and low MGMT expression both wereidentified as positive prognosticators in patients with new-ly diagnosed glioblastoma who underwent surgical resec-tion and received Gliadel wafer implants followed byadjuvant radiotherapy and concomitant oral TMZ chemo-therapy (47). Finally, we observed that lymphoblastoid celllines were not sensitized to temozolomide by pretreatmentwith decitabine, suggesting that this combination may notsignificantly increase toxicities in noncancerous tissues.Decitabine crosses the blood–brain barrier, but the dose
of decitabine needed to induce hypomethylation in thebrain in human patients is not yet known (48). Decitabineis thought to require cell division to induce hypomethyla-tion, and thereforemay only be effective on tumors that areactively proliferating. Thus, more work is needed to deter-mine the appropriate combination of decitabine and temo-zolomide in human patients. For example, to ensure thecancer cells are exposed to decitabine during cellular divi-sions, a longer duration of a lowerdosemaybe required. Inaddition, this drug combination may be beneficial to thesurvival of patients with other malignancies. Diffuse large
B-cell lymphoma is another disease in which the promoterofMGMT is hypermethylated and is predictive of survivalamong patients treatedwith alkylating chemotherapy (49).Thus, it will be worthwhile to study this drug combinationin a lymphoma model as well. In conclusion, our workargues that pretreating patients with glioblastoma with anunmethylatedMGMT promoter with decitabine before thestart of temozolomide treatmentmay sensitize their tumorsto the chemotherapy.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: E.L. Moen, A.L. Stark, W. Zhang, M.E. Dolan,L.A. GodleyDevelopment of methodology: W. Zhang, L.A. GodleyAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis): E.L. Moen, W. Zhang, M.E. Dolan, L.A.GodleyWriting, review, and/or revision of themanuscript:E.L.Moen,A.L. Stark,W. Zhang, M.E. Dolan, L.A. GodleyAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): M.E. Dolan, L.A. GodleyStudy supervision: M.E. Dolan, L.A. Godley
AcknowledgmentsThe authors thanks Dr. H. Wheeler for insightful conversations about
statistical analyses.
Grant SupportThis work was supported by grants from the NIH R21HG006367
(to W. Zhang, L.A. Godley, M.E. Dolan) and U01GM061393 (to M.E.Dolan). E.L. Moen is supported by an HHMI:Med-into-Grad Fel-lowship (56006772) and a Cancer Biology Training Grant (T32-CA009594).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received October 25, 2013; revised January 30, 2014; accepted February20, 2014; published OnlineFirst February 25, 2014.
References1. Pegg AE, Dolan ME,Moschel RC. Structure, function, and inhibition of
O6-alkylguanine-DNA alkyltransferase. Prog Nucleic Acid Res MolBiol 1995;51:167–223.
2. Weller M, Steinbach JP, Wick W. Temozolomide: a milestone in thepharmacotherapy of brain tumors. Future Oncol 2005;1:747–54.
3. Hecht SS. DNA adduct formation from tobacco-specific N-nitrosa-mines. Mutat Res 1999;424:127–42.
4. CohenMH, Johnson JR,PazdurR. FoodandDrugAdministrationDrugapproval summary: temozolomide plus radiation therapy for the treat-ment of newly diagnosed glioblastoma multiforme. Clin Cancer Res2005;11:6767–71.
5. Gerson SL. Clinical relevance of MGMT in the treatment of cancer. JClin Oncol 2002;20:2388–99.
6. Kaina B, Christmann M. DNA repair in resistance to alkylating anti-cancer drugs. Int J Clin Pharmacol Ther 2002;40:354–67.
7. Pegg AE. Mammalian O6-alkylguanine-DNA alkyltransferase: regula-tion and importance in response to alkylating carcinogenic and ther-apeutic agents. Cancer Res 1990;50:6119–29.
8. Costello JF, Futscher BW, Tano K, Graunke DM, Pieper RO. Gradedmethylation in the promoter and body of the O6-methylguanine DNAmethyltransferase (MGMT) gene correlates with MGMT expression inhuman glioma cells. J Biol Chem 1994;269:17228–37.
9. Esteller M, Hamilton SR, Burger PC, Baylin SB, Herman JG. Inactiva-tion of theDNA repair geneO6-methylguanine-DNAmethyltransferaseby promoter hypermethylation is a common event in primary humanneoplasia. Cancer Res 1999;59:793–7.
10. Esteller M, Garcia-Foncillas J, Andion E, Goodman SN, Hidalgo OF,Vanaclocha V, et al. Inactivation of theDNA-repair geneMGMTand theclinical response of gliomas to alkylating agents. N Engl J Med2000;343:1350–4.
11. Hegi ME, Liu L, Herman JG, Stupp R, Wick W, Weller M, et al.Correlation of O6-methylguaninemethyltransferase (MGMT) promotermethylation with clinical outcomes in glioblastoma and clinical strat-egies to modulate MGMT activity. J Clin Oncol 2008;26:4189–99.
12. Blanc JL, Wager M, Guilhot J, Kusy S, Bataille B, Chantereau T, et al.Correlation of clinical features and methylation status of MGMT genepromoter in glioblastomas. J Neurooncol 2004;68:275–83.
13. Brell M, Tortosa A, Verger E, Gil JM, Vi~nolas N, Vill�a S, et al. Prognosticsignificance of O6-methylguanine-DNAmethyltransferase determinedby promoter hypermethylation and immunohistochemical expressionin anaplastic gliomas. Clin Cancer Res 2005;11:5167–74.
14. KomineC,WatanabeT,KatayamaY,YoshinoA,YokoyamaT,Fukush-ima T. Promoter hypermethylation of the DNA repair gene O6-methyl-guanine-DNA methyltransferase is an independent predictor of
Cytosine Modifications in MGMT and Temozolomide Sensitivity
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1343
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

shortened progression free survival in patients with low-grade diffuseastrocytomas. Brain Pathol 2003;13:176–84.
15. ChristmannM,NagelG,HornS,KrahnU,WiewrodtD,SommerC, et al.MGMT activity, promoter methylation and immunohistochemistry ofpretreatment and recurrentmalignant gliomas: a comparative study onastrocytoma and glioblastoma. Int J Cancer 2010;127:2106–18.
16. BallMP, Li JB,GaoY, Lee JH, LeProust EM,Park IH, et al. Targeted andgenome-scale strategies reveal gene-body methylation signatures inhuman cells. Nat Biotechnol 2009;27:361–8.
17. Bell JT, Pai AA, Pickrell JK, Gaffney DJ, Pique-Regi R, Degner JF, et al.DNAmethylation patterns associate with genetic and gene expressionvariation in HapMap cell lines. Genome Biol 2011;12:R10.
18. Moen EL, Zhang X, Mu W, Delaney SM, Wing C, McQuade J, et al.Genome-wide variation of Cytosine modifications between Europeanand African populations and the implications for complex traits.Genetics 2013;194:987–96.
19. FritzG,KainaB.GenomicdifferencesbetweenO6-methylguanine-DNAmethyltransferase proficient (Mexþ) and deficient (Mex-) cell lines:possible role of genetic and epigenetic changes in conversion of Mexþinto Mex�. Biochem Biophys Res Commun 1992;183:1184–90.
20. Clark SJ, Harrison J, Paul CL, Frommer M. High sensitivity mapping ofmethylated cytosines. Nucleic Acids Res 1994;22:2990–7.
21. Mikeska T, Bock C, El-Maarri O, H€ubner A, Ehrentraut D, Schramm J,et al. Optimization of quantitative MGMT promoter methylation anal-ysis using pyrosequencing and combined bisulfite restriction analysis.J Mol Diagn 2007;9:368–81.
22. HuangY, PastorWA, ShenY, TahilianiM, LiuDR,RaoA. Thebehaviourof 5-hydroxymethylcytosine in bisulfite sequencing. PLoSOne2010;5:e8888.
23. Brown CC, Havener TM, Medina MW, Auman JT, Mangravite LM,Krauss RM, et al. A genome-wide association analysis of temozolo-mide response using lymphoblastoid cell lines shows a clinicallyrelevant association with MGMT. Pharmacogenet Genomics 2012;22:796–802.
24. Eadon MT, Wheeler HE, Stark AL, Zhang X, Moen EL, Delaney SM,et al. Genetic and epigenetic variants contributing to clofarabinecytotoxicity. Hum Mol Genet 2013;22:4007–20.
25. Stresemann C, Lyko F. Modes of action of the DNA methyltransferaseinhibitors azacytidine and decitabine. Int J Cancer 2008;123:8–13.
26. Noushmehr H, Weisenberger DJ, Diefes K, Phillips HS, Pujara K,Berman BP, et al. Identification of a CpG island methylator phenotypethat defines a distinct subgroup of glioma. Cancer Cell 2010;17:510–22.
27. Christensen BC, Smith AA, Zheng S, Koestler DC, Houseman EA,Marsit CJ, et al. DNAmethylation, isocitrate dehydrogenase mutation,and survival in glioma. J Natl Cancer Inst 2011;103:143–53.
28. Turcan S, Rohle D, Goenka A, Walsh LA, Fang F, Yilmaz E, et al. IDH1mutation is sufficient to establish the glioma hypermethylator pheno-type. Nature 2012;483:479–83.
29. HahnMA,Wu X, Li AX, Hahn T, Pfeifer GP. Relationship between genebody DNA methylation and intragenic H3K9me3 and H3K36me3chromatin marks. PLoS One 2011;6:e18844.
30. Jones PA. Functions of DNA methylation: islands, start sites, genebodies and beyond. Nat Rev Genet 2012;13:484–92.
31. Laurent L, Wong E, Li G, Huynh T, Tsirigos A, Ong CT, et al. Dynamicchanges in the human methylome during differentiation. Genome Res2010;20:320–31.
32. Mell�en M, Ayata P, Dewell S, Kriaucionis S, Heintz N. MeCP2 binds to5hmC enriched within active genes and accessible chromatin in thenervous system. Cell 2012;151:1417–30.
33. Zhang W, Duan S, Kistner EO, Bleibel WK, Huang RS, Clark TA, et al.Evaluation of genetic variation contributing to differences in geneexpression between populations. Am J Hum Genet 2008;82:631–40.
34. Curry WT, Barker FG. Racial, ethnic and socioeconomic disparities inthe treatment of brain tumors. J Neurooncol 2009;93:25–39.
35. Krex D, Klink B, HartmannC, vonDeimling A, Pietsch T, SimonM, et al.Long-term survival with glioblastoma multiforme. Brain 2007;130:2596–606.
36. Kihslinger JE, Godley LA. The use of hypomethylating agents in thetreatment of hematologic malignancies. Leuk Lymphoma 2007;48:1676–95.
37. Negrotto S, NgKP, Jankowska AM, Bodo J, Gopalan B,Guinta K, et al.CpGmethylation patterns and decitabine treatment response in acutemyeloid leukemia cells and normal hematopoietic precursors. Leuke-mia 2012;26:244–54.
38. Fabiani E, Leone G, Giachelia M, D'alo' F, Greco M, Criscuolo M, et al.Analysis of genome-widemethylation andgene expression inducedby5-aza-20-deoxycytidine identifies BCL2L10 as a frequent methylationtarget in acute myeloid leukemia. Leuk Lymphoma 2010;51:2275–84.
39. DaskalakisM,Nguyen TT, NguyenC,GuldbergP, K€ohlerG,WijermansP, et al. Demethylation of a hypermethylated P15/INK4B gene inpatients with myelodysplastic syndrome by 5-Aza-20-deoxycytidine(decitabine) treatment. Blood 2002;100:2957–64.
40. Hollenbach PW, Nguyen AN, Brady H, Williams M, Ning Y, Richard N,et al. A comparison of azacitidine and decitabine activities in acutemyeloid leukemia cell lines. PLoS One 2010;5:e9001.
41. Hagemann S, Heil O, Lyko F, Brueckner B. Azacytidine and decitabineinduce gene-specific and non-random DNA demethylation in humancancer cell lines. PLoS One 2011;6:e17388.
42. Plimack ER, Stewart DJ, Issa JP. Combining epigenetic and cytotoxictherapy in the treatment of solid tumors. J Clin Oncol 2007;25:4519–21.
43. Gravina GL, Festuccia C, Marampon F, Popov VM, Pestell RG, ZaniBM, et al. Biological rationale for the use of DNA methyltransferaseinhibitors as new strategy for modulation of tumor response to che-motherapy and radiation. Mol Cancer 2010;9:305.
44. Appleton K, Mackay HJ, Judson I, Plumb JA,McCormick C, StrathdeeG, et al. Phase I and pharmacodynamic trial of the DNA methyltrans-ferase inhibitor decitabine and carboplatin in solid tumors. JClin Oncol2007;25:4603–9.
45. Scandura JM, Roboz GJ, Moh M, Morawa E, Brenet F, Bose JR, et al.Phase 1 study of epigenetic priming with decitabine prior to standardinduction chemotherapy for patients with AML. Blood 2011;118:1472–80.
46. von Deimling A, Korshunov A, Hartmann C. The next generation ofglioma biomarkers: MGMTmethylation, BRAF fusions and IDH1muta-tions. Brain Pathol 2011;21:74–87.
47. Lechapt-Zalcman E, Levallet G, Dugu�e AE, Vital A, Diebold MD, MeneiP, et al. O(6)-methylguanine-DNAmethyltransferase (MGMT)promotermethylation and low MGMT-encoded protein expression as prognos-tic markers in glioblastoma patients treated with biodegradable car-mustine wafer implants after initial surgery followed by radiotherapywith concomitant and adjuvant temozolomide. Cancer 2012;118:4545–54.
48. Momparler RL. Pharmacology of 5-Aza-20-deoxycytidine (decitabine).Semin Hematol 2005;42:S9–16.
49. Esteller M, Gaidano G, Goodman SN, Zagonel V, Capello D, Botto B,et al. Hypermethylation of the DNA repair gene O(6)-methylguanineDNAmethyltransferase and survival of patientswith diffuse largeB-celllymphoma. J Natl Cancer Inst 2002;94:26–32.
Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics1344
Moen et al.
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924

2014;13:1334-1344. Published OnlineFirst February 25, 2014.Mol Cancer Ther Erika L. Moen, Amy L. Stark, Wei Zhang, et al. Expression and Sensitivity to Temozolomide
MGMTThe Role of Gene Body Cytosine Modifications in
Updated version
10.1158/1535-7163.MCT-13-0924doi:
Access the most recent version of this article at:
Cited articles
http://mct.aacrjournals.org/content/13/5/1334.full#ref-list-1
This article cites 49 articles, 13 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/13/5/1334To request permission to re-use all or part of this article, use this link
on October 5, 2020. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 25, 2014; DOI: 10.1158/1535-7163.MCT-13-0924