The Quality-Value Proposition in Health Care · 2017-11-02 · AS236-01 September 30, 2003 12:40...
29
AS236-01 September 30, 2003 12:40 Char Count= 0 The Quality-Value Proposition in Health Care G. Landon Feazell and John P. Marren Powerful forces are converging in US health care to finally cause recognition of the inherently logical relationship between quality and money. The forces, or marketplace “drivers,” which are converging to compel recognition of the relationship between cost and quality are: (1) the increasing costs of care; (2) the recurrence of another medical malpractice crisis; and (3) the recognition inside and outside of health care that quality is inconsistent and unacceptable. It is apparent that hospital administrators, financial officers, board members, and medical staff lead- ership do not routinely do two things: (1) relate quality to finance; and (2) appreciate the intra-hospital structural problems that impede quality attainment. This article discusses these factors and offers a positive method for re-structuring quality efforts and focusing the hospital and its medical staff on quality. The simple but compelling thesis of the authors is that health care must immediately engage in the transformation to making quality of medical care the fundamental business strategy of the organization. Key words: quality, value, patient safety, busi- ness case, medical staff culture, organizational structure, clinical performance, peer review, Institute for Healthcare Quality and Value (IHQV). P OWERFUL forces are converging in US health care to finally cause recog- nition of the inherently logical rela- tionship between quality and money. Within the health care community, it has been too difficult politically and professionally to confront, much less solve, the mounting quality deficiencies. To the payers, employ- ers, patients, and the government, faced with the spiraling costs of care and the perceived value of the care received, these same qual- ity deficiencies are increasingly apparent and unacceptable. The forces, or marketplace “drivers,” that are converging to compel recognition of the relationship between cost and quality are: (1) the increasing costs of care; (2) the occur- rence of another medical malpractice crisis; and (3) the recognition inside and outside of health care that quality is inconsistent and unacceptable. The potential for quality to have a major effect on the cost of health care is fundamentally and intuitively logical. Health care costs have risen in the United States to $1.4 trillion per year in total expen- ditures. Yet, the plea from the providers of health care is that there is not enough money. G. Landon Feazell is a co-founder of the Institute for Healthcare Quality and Value (IHQV), which will con- duct research in affiliation with numerous hospitals and health care organizations primarily focused on applied health services. He serves as the President and CEO of QualVal Health Systems, Inc., which he founded in 1973. Mr. Feazell received the BS degree from Duke University and has extensive post-graduate education in medical science from the University of West Virginia Medical Center and the University of Denver College of Law, where he served as Chairman of the National Conference of Law Reviews. John P. Marren is a co-founder of the Institute for Healthcare Quality and Value (IHQV), and is a partner in Hogan Marren, LLC, in Chicago, Illinois. He has 30 years of experience in health care, including 10 years of hospital administrative experience before becoming an attorney specializing in health care law. Mr. Marren received his BA degree from St. Xavier University and his JD degree from Loyola University Chicago School of Law, where he is currently an Adjunct Professor in health care law. J Health Care Finance 2003;30(2):1–29 c 2003 Aspen Publishers, Inc. 1
Transcript of The Quality-Value Proposition in Health Care · 2017-11-02 · AS236-01 September 30, 2003 12:40...

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Propositionin Health Care
G. Landon Feazell and John P. Marren
Powerful forces are converging in US health care to finally cause recognition of the inherently logicalrelationship between quality and money. The forces, or marketplace “drivers,” which are converging tocompel recognition of the relationship between cost and quality are: (1) the increasing costs of care; (2)the recurrence of another medical malpractice crisis; and (3) the recognition inside and outside of healthcare that quality is inconsistent and unacceptable.
It is apparent that hospital administrators, financial officers, board members, and medical staff lead-ership do not routinely do two things: (1) relate quality to finance; and (2) appreciate the intra-hospitalstructural problems that impede quality attainment.
This article discusses these factors and offers a positive method for re-structuring quality efforts andfocusing the hospital and its medical staff on quality. The simple but compelling thesis of the authorsis that health care must immediately engage in the transformation to making quality of medical carethe fundamental business strategy of the organization. Key words: quality, value, patient safety, busi-ness case, medical staff culture, organizational structure, clinical performance, peer review, Institute forHealthcare Quality and Value (IHQV).
POWERFUL forces are converging inUS health care to finally cause recog-nition of the inherently logical rela-
tionship between quality and money. Withinthe health care community, it has beentoo difficult politically and professionallyto confront, much less solve, the mountingquality deficiencies. To the payers, employ-ers, patients, and the government, faced withthe spiraling costs of care and the perceivedvalue of the care received, these same qual-ity deficiencies are increasingly apparent andunacceptable.
The forces, or marketplace “drivers,” thatare converging to compel recognition of therelationship between cost and quality are:(1) the increasing costs of care; (2) the occur-rence of another medical malpractice crisis;and (3) the recognition inside and outside ofhealth care that quality is inconsistent andunacceptable. The potential for quality tohave a major effect on the cost of health careis fundamentally and intuitively logical.Health care costs have risen in the UnitedStates to $1.4 trillion per year in total expen-
ditures. Yet, the plea from the providers ofhealth care is that there is not enough money.
G. Landon Feazell is a co-founder of the Institute forHealthcare Quality and Value (IHQV), which will con-duct research in affiliation with numerous hospitalsand health care organizations primarily focused onapplied health services. He serves as the Presidentand CEO of QualVal Health Systems, Inc., which hefounded in 1973. Mr. Feazell received the BS degreefrom Duke University and has extensive post-graduateeducation in medical science from the University ofWest Virginia Medical Center and the University ofDenver College of Law, where he served as Chairmanof the National Conference of Law Reviews.
John P. Marren is a co-founder of the Institute forHealthcare Quality and Value (IHQV), and is a partnerin Hogan Marren, LLC, in Chicago, Illinois. He has 30years of experience in health care, including 10 yearsof hospital administrative experience before becomingan attorney specializing in health care law. Mr. Marrenreceived his BA degree from St. Xavier University andhis JD degree from Loyola University Chicago Schoolof Law, where he is currently an Adjunct Professor inhealth care law.
J Health Care Finance 2003;30(2):1–29c© 2003 Aspen Publishers, Inc.
1

AS236-01 September 30, 2003 12:40 Char Count= 0
2 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
Health care simply cannot and will not con-tinue to operate as a “cost plus” enterprise.
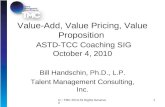
When the 14 percent gross national prod-uct (GNP) for health care in the UnitedStates, with some 40 percent of our popu-lation uninsured, is compared with 9 percentand less in other industrialized nations withaccess to health care for all, and with spi-raling increases in costs returning, the pres-sure from employers and payers will againbe as relentless as it was at the inception ofmanaged care. The present economic envi-ronment of health care demands the realiza-tion that there is enough money. Solutionsmust be found to provide more efficient andeffective care with less cost impact from pa-tient injury and malpractice premiums. Theper capita expenditure on health care com-pared to other industrialized nations (shownin Figure 1) clearly demonstrates the need for
Figure 1. Per Capita Expenditures on Health
health care to reorganize to deliver consis-tently reliable, high quality, error-free healthcare more efficiently and more effectively.
There is now a dramatic and suddeninterest in health care centering on the ques-tion of whether there is a financial relation-ship between quality and cost—a “businesscase”—for quality and patient safety inhealth care. This phenomenon, which is evi-dent in the press1 and in the literature,2 is notbecause of the inherent logic in the proposi-tion or because it is the expectation of profes-sional conduct, but because of the realizationthat changes in quality will not occur inhealth care unless a financial benefit can beproven to drive the movement and motivatethe participants.3
Health care quality is best analyzedwithin the framework proposed by Mark R.Chassin, MD—overuse, underuse, and

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 3
misuse. After evaluation of the medical liter-ature within this framework, Chassin, a lead-ing expert in health care quality, reaches thefollowing conclusion:
As the research literature makes clear,quality problems of all three varietiesabound in American medicine. The ma-jority of these problems are not rare, un-predictable, or inevitable concomitants ofthe delivery of complex, modern healthcare. Rather, they are frighteningly com-mon, often predictable, and frequently pre-ventable. Viewed by those companies thathave committed themselves to the most ad-vanced applications of industrial qualitymanagement, the magnitude of the fail-ures or quality defects in the provision ofhealth care must seem stupefying.4 (Em-phasis added.)
During the past years, health care has at-tempted to transform the quality movementto continuous quality improvement or totalquality improvement models. The existinghealth care quality movement, however, hasbeen unable to significantly impact and im-prove the quality of health care in the UnitedStates. Indeed, at the 10th anniversary meet-ing of the Institute for Healthcare Improve-ment, the president and chief executiveofficer (CEO) of this leading and prestigiousorganization stated that despite all of their ef-forts over the past 10 years, no improvementin quality was achieved. In view of these con-verging forces to compel quality and patientsafety accompanied by the realization thatexisting quality efforts are not adequatelychanging the quality of care, the issues thenbecome: (1) why the quality improvementis not achieving a dramatic impact in healthcare; and (2) what the reasons are for thisfailure.
Some indicators of the magnitude of thequality of care deficiencies in US health care
leading to preventable injuries and deaths areevident in the following insights:
• Medical error results in as many as400,000 deaths per year and as many as98,000 hospital deaths per year (equiv-alent of one jumbo jet crashing daily);5
• 1/4 of hospital deaths are preventable;6
• 1/3 of hospital procedures expose pa-tients to risk without improving health;7
• 1/3 of all laboratory tests with abnor-mal results are not followed up by thephysician; and
• 30 percent of acute care patients and20 percent of chronically ill patients re-ceive care that is not indicated.8
According to the Robert Wood JohnsonFoundation, the risk of death from riding ona set of recalled Firestone tires is much lowerthan the risk of death from avoidable hospitalerror. The startling contrast for risk of deathis 91 per million vs. 2,917 per million, or a32 times greater risk of death in health care.9
This perspective states the magnitude of theproblem in a recent and easily understand-able context.
A recent RAND study further confirmsthe problems with quality of care based ona study of 20,000 adults from 12 cities, with30 acute and chronic conditions, using 439quality indicators. The study concludes thatonly 55 percent of US patients receive thecare recommended by experts and the mostcurrent medical science. Two specific prob-lems highlighted by the study are that only45 percent of those presenting with heartattacks receive beta-blockers and only 24percent of diabetics received three or moreglycosylated hemoglobin tests within a two-year period.10
Variation in health care rates presents verycompelling evidence of the discrepanciesthat will later be considered as overuse and

AS236-01 September 30, 2003 12:40 Char Count= 0
4 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
underuse. Cardiac bypass surgery rates rangefrom 3/1000 in Albuquerque, New Mexico,to more than 11/1000 in Redding, California.During 1995 and 1996, the average num-ber of specialist visits by decedents (patientsin the last six months of life) ranged fromtwo in Mason City, Iowa, to more than 25 inMiami, Florida. The average number of daysper decedent spent in the hospital rangedfrom 4.6 in Ogden, Utah, to 21.4 in Newark,New Jersey. In addition, one-half of dece-dents experienced an intensive care unitadmission in Miami, Florida, vs. only 14 per-cent in Sun City, Arizona.11
There are widely accepted indications ofadditional factors that seriously affect thequality of health care in the United States.For example, patient non-compliance is es-timated to cause 125,000 deaths annually,while 50 percent of all prescriptions filledare not taken correctly and 20 percent arenot even picked up from the pharmacy whenprescriptions are ordered.
The failure in the United States to es-tablish the fundamentals of a market-basedhealth care system with such key capabili-ties as standardized measures of quality mustbe the focus of efforts to improve qual-ity and patient safety. Further, as this anal-ysis is presented, the distinction betweenhealth care and health of Americans shouldnot be overlooked when addressing accessand inconsistencies in quality care. Indeed,some authors, such as Barbara Starfield, MD,conclude: “The fact is that the US pop-ulation does not have anywhere near thebest health in the world.”12 Infant morbid-ity and mortality rates in the United States,compared to other industrialized nations,certainly create concerns about this overallhealth perspective. Certainly, in the contextof value, with the disproportionate spend-ing on health care in the United States, we
should expect more as a society than is ourreality.
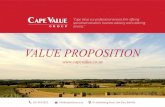
As an introduction to the discussion ofthe quality-value proposition, some consid-eration of costs and distribution of costs ishelpful to evaluating the challenges andopportunities to impact costs of care withquality initiatives. George C. Halvorson,chairman and CEO of the Kaiser Founda-tion Health Plan, recently gave the followinganalysis of the cost distribution of care: 20percent of people account for zero percentof the total cost of care; 70 percent of peopleaccount for 10 percent of the total cost ofcare; 5 percent of people account for 50 per-cent of the total cost of care; while 1 percentof people account for 30 percent of the totalcost of care.
The cost distribution among workingAmericans is diagramed in Figure 2.
The purposes of this article are to presentand to consider the following aspects of therelationship between quality and cost in UShealth care:
• The six elements of the health carequality-value proposition, including abrief discussion of their causes and ef-fects;
• Current research efforts to establish thevalidity of the cost-quality relationship;
• Fundamental causes of the failure to af-fect quality; and
• The basis for solutions to dramaticallyimprove quality while reducing costs.
Elements of the Quality-ValueProposition
What we know for sure is that there isfar too much overuse, underuse, and misuseto tolerate in a complex, high-risk, patientdependent, and financially burdensome in-dustry. We also know that there are seven

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 5
Figure 2. Cost Distribution on Health among Working Americans
compelling reasons for the profound andundisputable correlation between cost andquality in health care. Five of these rea-sons are negative impacts from financiallosses, while two of these elements arefrom positive additions of money to the bot-tom line. Reading the literature and con-sulting with health care clients suggest thatthese seven reasons are not well recog-nized and understood. These reasons areconsidered the elements of the quality-valueproposition.
The five negative impacts from financiallosses are:
1. The aggregate cost of preventableinjuries (morbidity) and preventable
deaths (mortality) in inpatient and out-patient care;
2. The indirect cost of unnecessary med-ical malpractice insurance premiums;
3. The intangible cost of public percep-tion of quality on the selection ofproviders;
4. The increased costs of directors and of-ficers (D&O) insurance; and
5. The regulatory costs from poor quality.
The two positive additions to the bottomline are:
1. The value of financial incentivesnow being paid and contemplated(increased revenue) to correct the

AS236-01 September 30, 2003 12:40 Char Count= 0
6 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
exiting perverse payment system;and
2. The increased profit margins from ef-fectiveness and efficiency in healthcare delivery.
The Cost of Preventable Injuries and Deaths
The total financial impact of the costs ofpreventable medical injuries is $17 to $29billion, which includes costs in addition tohealth care costs, such as lost income, losthousehold production, and disability.13 Overone-half of the costs of these preventableinjuries go exclusively toward health carecosts. This means that $8.5 to $14.5 billionare spent annually for additional health carecaused by preventable medical injuries. In1996, based on these calculations, these fig-ures represented roughly 2 percent of totalnational health care expenditures. Broughtforward to the year 2002, with a total costof $1.4 trillion, 2 percent for the additionalcosts of preventable injuries translates to $28billion annually.
These calculations present the cost of pre-ventable injuries. The Institute of Medicine(IOM) focused on preventable deaths, ashave other authors, such as Lucian Leape,MD, and Michael Millenson. Millenson re-minds us of the study by Don Harper Mills,MD, JD, years ago during the 1970s med-ical malpractice premium crisis, based on21,000 medical records from 23 Califor-nia hospitals, which concluded that morethan 10,000 hospital patients a year die fromiatrogenic causes in California.14 Mills cal-culated from his methodology that approxi-mately 120,000 preventable hospital deathsoccurred per year. After reviewing the IOMreport and findings, Millenson concludesthat between 1978, when Mills’ work waspublished and the subsequent work of Leape
and the IOM in 1999, a total of some 2.5million preventable deaths occurred duringthat entire span of 21 years from what hecharacterizes as the “toll of inaction.” Hecomments:
The sheer size of such statistics can renderthem impersonal. So divide the number ofdeaths by the average number of acute carehospitals during this period (generously,about 5,500). What you end up with is nineto twenty-two patients unnecessarily dy-ing every year at every community hospitalin the country, every year, for twenty-oneyears. One can argue what percentage ofthese deaths was preventable; one cannotargue that there was any serious effort byproviders to prevent them.15
After the release of the IOM report, ToErr Is Human,16 hospital deaths from medi-cal “errors” became the focus of the healthcare quality debate. The impact of this reportand the subsequent controversy are clearlycaused by its most frequently referenceddeath toll figures of 44,000 to 98,000 peryear. The accuracy of these figures has beenwidely challenged, ranging from criticismsof the methodology of the original studieson which the report is based17 to criticismsof the terminology used in the report byan author of the original study, Troyen A.Brennan, MD.18
The surprise in health care quality shouldnot be the attention generated by the IOMreport, but rather that so little is knownabout the fundamental statistics on healthcare quality in the United States. It is signif-icant to recognize that the IOM figures werederived from studies of the medical recordsof several relatively small patient popula-tions dating back to 1984 in NY hospitals,and then extended to Utah and Colorado

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 7
hospitals. The original Harvard MedicalPractice study, which reviewed over 30,000hospital records, found that injuries fromcare itself (adverse events) occur in 3.7 per-cent of hospital admissions, over half ofthese injuries are preventable, and 13.6 per-cent of these injuries lead to death.19
While there may be debate as to the pre-cise rate of preventable deaths in US hospi-tals, there is a developing body of knowledgeabout the “defect rates” in the current deliv-ery of health care. Many important contri-butions to understanding health care qualityinclude studies that classify quality chal-lenges into the following three categories:
1. Overuse—defined as providing ahealth service when its risk of harmexceeds its potential benefit;
2. Underuse—defined as failing to pro-vide an effective service when it wouldhave produced favorable outcomes;and
3. Misuse—defined as avoidable compli-cations to appropriate health care.1
Insight into examples of clinical qualityfor each of the categories of overuse, under-use, and misuse for specific medical condi-tions and the causes of those defects can besummarized as follows:
• Overuse etiology:
– Payment incentive, such as fee-for-service;
– Physician enthusiasm for interven-tion;
– Primary care physician expectationof specialist (e.g., coronary angiog-raphy, upper-GI endoscopy, kneearthroscopy, etc.);
– Patient expectation (e.g., antibiotic,x-ray, laboratory, etc.); and
– Fear of malpractice (i.e., defensivemedicine).21
Examples of overuse from medical re-search include hysterectomies, in which16 percent performed in a group of man-aged care plans were determined to beinappropriate (ranging from 10 percentto 27 percent among plans),22 coronaryangiography and revascularization,23
and antibiotic therapy.24
• Underuse etiology:
– Financial barriers (e.g., lack of insur-ance, the imposition of co-paymentsand deductibles, benefit packagesnot covering preventive care, etc.);25
and– Rapid and recent accumulation of an
enormous amount of clinical efficacydata.26
Underuse of beta-blockers is an ex-ample from medical research. Seventy-nine percent of eligible heart attacksurvivors fail to receive beta-blockers,which results in a defect rate of790,000 per million (less than SigmaLevel One).27 Another example is thealarming rate of patients with clinicaldepression who are not detected ortreated adequately: 58 percent, with adefect rate if 580,000 per million.28
• Misuse etiology:
– Errors in diagnosis (22 percent);– Mishaps related to non-invasive, non-
drug-related treatment (21 percent);– Mistakes in medication use (12 per-
cent);– Technical complications of surgery
(8 percent); and– Surgical wound infections (6 per-
cent).29

AS236-01 September 30, 2003 12:40 Char Count= 0
8 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
The medical literature is much lessdefinitive about the causes of mis-use than the other two categories ofproblems.30
Chassin considered these quality concernsand examples of health care performance andobserved:
If the performance of certain high-reliability industries, whose standards ofexcellence we take for granted, suddenlydeteriorated to the level of most health careservices, some astounding results wouldoccur. At the defect rate of 20 percent,which occurs in the use of antibioticsfor colds, the credit card industry wouldmake daily mistakes on nine million trans-actions; banks would deposit 36 millionchecks in the wrong accounts every day;and deaths from airplane crashes would in-crease one thousand fold.31
Preventable injuries and deaths are best il-lustrated by misuse (i.e., avoidable compli-cations to appropriate health care). Chassinmakes the point that relatively little is knownabout misuse,32 and certainly even less ispublished about misuse. However, compli-cations of medical care are the heart and soulof peer review in US hospitals, as well as thesource of professional liability litigation andclaims. QualVal Systems has learned fromextensive consulting engagements through-out the United States over some 30 years ofexperience that there is a significant nega-tive financial effect on the cost of provid-ing health care services from a variety ofsources that all converge on quality of care.These impacts are from overuse, underuse,and misuse. While we are not able to pub-lish our studies due to the highly confidentialand privileged nature of external peer re-view consultations, we can state unequivo-
cally that there is tremendous financial wastein the health care system from all three cat-egories of clinical performance. In the con-text of the cost of preventable injuries andmortality, we will focus on misuse for thiscategory and comment on overuse and un-deruse in the section titled “Increased ProfitMargins from Effectiveness and Efficiency.”
Misuse manifests in our experience in in-stances, such as:
• Removal of the wrong kidney, surgeryat the wrong level or on the wrong limb;
• Failure to timely perform cesarean sec-tions;
• Hemorrhage and brain damage fromlaceration of blood vessels during lum-bar laminectomy;
• Shock from accidental injection ofundiluted epinephrine; and
• Death from failure to properly monitorconscious sedation during endoscopy.
These are but a few of the medicaltragedies that QualVal routinely investigatesusing peer review, including root cause anal-ysis, to determine if these are isolated eventsor patterns with likely potential for repeti-tion. The cost of increased lengths of stay,increased levels of care, and supportive mea-sures is tremendous in these events.
Most of the efforts to solve quality de-ficiencies leading to medical errors have fo-cused on medication errors. Indeed, the costsof medication errors are high in financialterms, when the estimate of the cost for eachpreventable adverse drug event in one teach-ing hospital is almost $4,700.33 However, asthe studies on overuse, underuse, and mis-use clearly demonstrate, and the IOM reportemphatically states, the primary source ofmedical errors and the greatest health carequality challenge is the failure to diagnose

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 9
(approximately 21 percent of the medical er-rors). After a careful review of proprietarydatabases of liability insurance carriers, itseems clear that medical malpractice claimsdata would reveal exactly the same conclu-sion. As Leape points out, autopsy studiesalso suggest that preventable deaths may alsobe many more than 98,000 per year. Thereare serious concerns from these studies re-garding incorrect or missed clinical diag-noses, as well.34
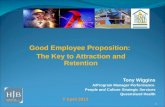
Recalling the Six Sigma cost of poor qual-ity as a function of Six Sigma performancelevels (see Figure 3), it is insightful to con-sider the cost of poor quality in a $1.4 tril-lion industry that functions at a Two Sigmato Four Sigma performance level.
It is clear that the quality of health care inour communities places a tremendous bur-den on patients and their families from thecosts of preventable injuries. This cost ex-tends to employers and third-party payers.A recent report developed by the MidwestBusiness Group on Health, in collaborationwith the Juran Institute, asserts that theseerrors:
[N]ot only exact a human toll in termsof lost lives and pain and suffering, butthey also create a huge economic burden
Figure 3. Cost of Poor Quality as a Functionof 6Σ Performance Levels
in terms of both the direct costs of treatingcomplications and the indirect costs of lostproductivity and premature death.35
This study estimates that poor qualityhealth care costs the typical employer be-tween $1,700 and $2,000 per covered em-ployee each year.
Indirect Costs of Medical MalpracticeInsurance
The global insurance and reinsurance in-dustry faced the January 1, 2003, renewalseason having lost $175 billion (US) of cap-ital over the last two years. This unprece-dented erosion of capital has arisen from acombination of underwriting losses, under-reserving on earlier years, and investmentlosses.36
Within this dismal insurance and reinsur-ance marketplace, medical malpractice in-surance (health care professional liabilityinsurance) has gone from being the mostprofitable of all property and casualty linesof insurance in the mid-1990s to now beingthe least profitable. As a result, medicalmalpractice insurance premiums are soaringfaster than at any time since the mid-1980s.These trends are the result of increased ver-dicts settlements and the rising legal and re-lated expenses to defend cases. Within thisbackdrop, some insurance carriers are evenpulling back from offering health care pro-fessional liability insurance. St. Paul Insur-ance, faced with $940 million in medicalprofessional losses in 2002, has com-pletely withdrawn from the business, send-ing 40,000 physicians, 72,000 other healthcare professionals, 750 hospitals, and alarge number of nursing homes lookingfor a new insurer. St. Paul’s staggeringlosses were based on runaway frequency

AS236-01 September 30, 2003 12:40 Char Count= 0
10 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
and severity, a phenomenon shared by othercompanies.37
Jury Verdict Research reported a 43 per-cent rise in the median medical malprac-tice awards between 1999 and 2000, hittingthe highest median ever of one million dol-lars. The statistics on median verdicts can bemisleading, however, unless the observerunderstands that cases for the defense, zeroverdicts, and cases dropped or settled arenot included in this number. This is theoft-quoted basis for the current problem inmedical malpractice called “frequency ofseverity,” with unprecedented large verdictsand settlements experienced nationally. Thepresentation of Troyen A. Brennan, MD, JD,at the Harvard Quality Colloquium summa-rized the relationship between premiums be-
Figure 4. Median Medical Malpractice Awards and Settlements in the US
ing driven by increasing awards from JuryVerdict Research as shown in Figure 4.
Brennan summarized the frequency ofclaims as rising slowly, but still farfrom the frequency in the mid-1980s (seeFigure 5).
In this marketplace, primary purchasersof health care professional insurance can ex-pect to see double to triple digit increasesfor the next two years. Reinsurance pricinghas hardened in 2002, but London/Europeanreinsurers have created a market for this busi-ness. Reinsurance pricing is now subject tostringent actuarial analysis, not just from thelead underwriters, but also from the major-ity of reinsurers, with reinsurance buyers ex-pected to see at least double digit increasesin the next two years.38

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 11
Figure 5. Claims per 100 Physicians per Year in the US
Medical historian James Mohr concludesthat malpractice litigation in many ways is adirect consequence of the clinical laxity ofphysicians. He recently wrote that patientshad no alternative but to “try to hold indi-vidual practitioners, one at a time, to what-ever standards they or their (malpractice)lawyers, one at a time, wanted to impose.”39
Michael Millenson, the noted author ofDemanding Medical Excellence, commentson this article by stating: “Put differently, it isthe doctors, not the lawyers, who have turnedpatients into plaintiffs.40 Millenson remindsus of an article by medical sociologist EliotFreidson in the early 1970s when he wrote:“When doctors were asked what they woulddo about a colleague whose behavior vio-
lated technical norms of conduct, the mostcommon response was ‘nothing.”’41 Theresponse of individual physicians and orga-nized medicine to the current wave of spiral-ing medical malpractice premiums—to capdamages for pain and suffering and othertort reforms—fails to recognize the currentinsurance realities of losses in the total in-surance and reinsurance marketplace. Theimpacts of both the depletion of reservesfrom 9/11, and the reality that malprac-tice premiums increase when the bond mar-ket falters, are root causes of premiumincreases. Those who point to the successin stabilizing the California malpractice pre-miums with such a cap fail to recognizethat this phenomenon occurred when the

AS236-01 September 30, 2003 12:40 Char Count= 0
12 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
state introduced strict regulatory controls onpremiums.
The essence of the malpractice premiumtragedy in the United States, however, is thatmalpractice insurance companies have failedand refused to invest significantly from theirvast financial resources in the reduction ofmedical errors that lead to losses and, ulti-mately, to premium increases. The prevail-ing notion among most malpractice carriers,with notable exceptions (e.g., COPIC, themedical society company in Colorado, andMMI Companies), is that they corporatelybelieve and behave on the premise that med-ical errors cannot be prevented. They havetraditionally seen risk management as “losscontrol,” from a purely financial perspective,rather than significantly investing in risk andliability reduction strategies.
The current insurance and reinsurancemarketplace, particularly demonstrated inLondon and European companies, has re-cently undertaken a much more rigorous pro-gram of providing real financial incentivesand premium reductions to insureds whodemonstrate real risk reduction programs.When premiums are doubling and tripling,the “pain” may be enough from these im-mense additional costs to motivate healthcare organizations to see the financial benefitof quality and patient safety.
In recent months, the crisis in premiumsfor medical malpractice insurance has re-sulted in a large number of hospitals, bothlarge and small, increasing the initial portionof their retained liability exposure in hugeamounts and proportions. In large hospitalsthat retained the first $5 million of exposureper claim (and not capitated by an aggregateamount), the retention has increased to $15to $20 million per claim. The net effect ofsuch liability retention is to risk the very exis-
tence of the institution on not suffering largenumbers of large verdicts. These health careinstitutions must immediately look beyondtheir current efforts to limit liability expo-sure with legislative capitation on damages.It is an imperative of the highest magnitudethat boards of trustees immediately committhemselves and their organizations to mini-mizing liability exposure by drastic improve-ments in quality and reduction of patientinjuries. The gradual approach to quality inthe past must be replaced with the sense ofurgency demanded by the circumstances ofsuch massive retention in liability. They mustfurther guard carefully against the tempta-tion to skimp on the investigation of claimsand the preparation for the defense of cases.With the retention of liability also comes thecost of investigation and defense. Proactiveapproaches to early recognition and settle-ment of claims are examples of the sur-vival strategies that must be understood andundertaken.
A recent editorial published in many USnewspapers by a leading health care qualityexpert cautioned against the continued be-lief that bad doctors and bad people are re-sponsible for errors in medicine and that it isa problem with systems and processes, notpeople. This has been the mantra for manyyears in the United States, and it has becomea part of the problem and not a part of thesolution for liability costs in US medicine.Among experts in medical malpractice lia-bility, it is well known that a small percent-age of physicians are responsible for a verylarge percentage of financial loses.
Public Perception of Quality
The US public is only just beginningto become aware of the magnitude of thehealth care quality problem. There has been

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 13
comparatively little public outcry aboutpatient safety in health care. However, thepublic is rapidly coming to understand thatcompared with other industries, the expecta-tion for health care quality is very low.
There are ominous signs that the pub-lic perception, distrust, and anger are read-ily apparent, however. The first barometeris always sentinel jury verdicts in medicalmalpractice lawsuits. Juries throughout theUnited States are speaking clearly and loudlyin failure to diagnose cancer cases, for ex-ample. These verdicts are heightened whenthere is apparent financial greed in businessincentives for the hospital(s) or physician(s)involved.
When QualVal was retained in the 1990sto review the quality issues inherent in re-moving the wrong kidney in a patient, itwas a national news story highly publicizedon CNN and in the local Boston newspa-per. On the taxicab ride to the hospital, weasked the driver what effect the event wouldhave on the local community in terms offuture patient selection of hospitals. His an-swer was basically that no one in the commu-nity would consider going there again. Uponentering the hospital and during the introduc-tory meeting with the hospital CEO, the samequestion was asked. His response to the ex-act question was that it would “blow over in amonth or so.” Of course, the cab driver wasright. News sources now focus on medicalerrors in a daily barrage of negative public-ity for specific institutions and practitioners.The impact of such negative publicity andthe resulting public perception can be finan-cially devastating, especially in competitivemarkets.
Public perception, however, should alsobe viewed from the positive perspective ofadding revenue to the bottom line. QualVal
has experienced dramatic results from physi-cian groups that have organized to publicizethe quality of their outcomes, particularly inmarkets in which payers and large group pur-chasing consortia select and de-select physi-cian groups for eligibility on their panels.The Federal Trade Commission rendered afavorable opinion to a coalition of the promi-nent cardiology practices in Denver, Col-orado, to share financial information on thebasis of the organization’s mission to im-prove quality and patient outcomes. Somemedical specialty organizations and evenphysicians and physician groups are morefrequently electing to collect data and publi-cize results of the quality of their outcomesto attract patients, using organizations, suchas Outcome Sciences in Boston. The logicand the argument favoring such an approachare well articulated by Steven F. Isenberg,MD, and Richard E. Glicklich, MD, in Prof-iting from Quality: Outcomes Strategies forMedical Practice.42
Cost of D&O Insurance
While we do not typically think of D&Oliability insurance and possible exposure toliability related to medical malpractice at theboard level, imagine the following scenario.Because of the well documented (in the lit-erature) reluctance of physicians to conductenthusiastic peer review, Hospital A con-tinues to renew the privileges of Doctor Xwho routinely performs endoscopies on pa-tients when it is not clinically appropriate(overuse), and in a manner that hurts thepatient (misuse). Doctor X is a popularphysician, and even though there have beenincidents reported about Doctor X, he has notbeen sanctioned or recommended for mon-itoring or any other corrective action. Re-member, the board of the hospital remains

AS236-01 September 30, 2003 12:40 Char Count= 0
14 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
responsible for the quality of care and tomake sure that peer review, although con-ducted by the medical staff, is nonethelesseffective. In an action brought by a plaintiffwho is harmed by Doctor X, the plaintiff’slawyer requests a history of incidents involv-ing Doctor X. The hospital attempts to fightsuch a subpoena arguing that any peer reviewmaterial is exempt from discovery understate law. The plaintiff counters by offeringthat the information sought is not sought forthe purpose of proving anything against Doc-tor X, but rather to ascertain the hospital’sculpability for having Doctor X available,on-staff and on-call. There is no guaranteethat such information could not be discov-ered, and that it could not form the basisfor an action against the board, and its D&Ocoverage. Or, worse, what if the D&O carrierfinds the board’s continued failure to provideeffective oversight to the peer review processas grossly negligent and refuses to providecoverage for damages awarded to the plain-tiff against the board, and the board is there-fore personally liable. The factual scenariocould become particularly alarming in lightof any testimony of hospital personnel whoidentify facts indicating the lack of congru-ent quality processes and the integration ofclearly defined quality information.
Regulatory Costs from Poor Quality
The federal government has become in-creasingly engaged in regulatory efforts toforce health care to improve quality. One dra-matic example is the current approach of theUS Department of Justice to review medicalerror allegations by whistleblowers and oth-ers, looking for cases against hospitals thatwould make good cases for claims of vio-lations of the False Claims Act for inade-quate quality of care. The Bureau of NationalAffairs’ Health Law Reporter published a
“Lead Report” in July 2003 that acute carehospitals may see fraudulent billing suitsover systematic medical errors. This legaltheory has been used successfully as a qual-ity theory pioneered in many nursing homecases by the US Attorney’s Office. Thesewould be cases in which hospitals demon-strated patterns of poor care and continuingincidents in which there is billing for ser-vices when the organization fails to have anadequate remedial system to reduce such er-rors. It is important to note that the reportof this review of claims for medical errorsdiscusses the approach of the IOM report onmedical error. Apparently, prosecutors willfocus on patient injury and not on systemsfailures that do not cause injury. However,the IOM report makes clear that a compre-hensive patient safety system must track bothbad outcomes and near misses.
Another more traditional example of pay-ing regulatory fines for poor quality is causedby the quality category of overuse. Unnec-essary treatments and procedures have led tonumerous claims for civil and even criminalprosecution, with huge payments of settle-ments and legal expenses.
Of course, such regulatory investigationsand allegations, much less the devastation ifsuch cases were tried, result in the erosion ofconfidence in health care in general and in thepublic perception of specific organizations.
Financial Incentives
Several observations regarding the rapidlyevolving health care environment are criti-cal to putting these quality challenges intoproper perspective for hospitals committedto thriving. First, the most recent report ofthe IOM titled Leadership by Example: Co-ordinating Government Roles in ImprovingHealthcare Quality,43 clearly establishes theagenda of the federal government to develop

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 15
clinical performance measures for compara-tive analysis of hospitals to be regularly pub-lished for the public, similar to the recentnursing home/long-term care facilities mea-sures. Second, recent pronouncements byThomas Scully, Administrator of the Centersfor Medicare and Medicaid Services (CMS),clearly state the federal agenda to pay moremoney to hospitals that provide quality carebased on developed criteria.
A variety of financial incentive programsto induce both physicians and patients to be-come actively engaged in endeavors to im-prove quality of care are now being piloted inthe United States. Employer groups, such asGeneral Electric Company (GE), Ford MotorCompany, Verizon Communications, UnitedParcel Service, and Proctor & Gamble arelaunching pilot programs to pay bonuses tophysicians of up to 10 percent in selectedcities if they prove they are taking better careof cardiovascular and diabetes patients. Theleader for health care initiatives at GE at-tributes the bonus programs to the alarmingrates of medical error and studies of qual-ity problems in health care, citing recentstudies that indicate 70 percent of diabeticpatients do not get care meeting standards ofthe American Diabetic Association, whichcan lead to serious health complications. On-line interactive tools for the patient to en-ter data about their hemoglobin levels andmedication compliance can be used for suchchronically ill patients to earn “CareReward”points for following doctors’ orders betweenoffice visits. These points can be redeemednot as cash bonuses but for merchandise cou-pons, time off from work, and other perks.
Doctors in such bonus programs would re-ceive a yearly cash bonus of $100 for eachpatient covered by a participating employerif their practices have a high percentageof diabetic patients whose blood pressure,
blood sugar, and lipid levels are sufficientlymeasured and controlled. Estimated sav-ings from the program are $350 per dia-betic patient per year, with employers’ costof no more than $175 per diabetic patientannually.
The “Bridges of Excellence” program is a“pay for performance” movement, with Inte-grated Healthcare Association expecting tomake bonus payments to physicians in Cali-fornia next year that could exceed $100 mil-lion. In Boston, a third example of financialincentives is the Partners Healthcare System,in which physicians will get bonuses of $55per patient annually for investing in systems,such as computer-based medical records andcare-management software programs forchronically ill patients. The Leapfrog Groupand the Robert Wood Johnson Foundationare also reported to be evaluating pay forperformance pilot projects.
In an article summarizing and analyzingcase studies investigating the business casefor quality improvements discussed later inthis article, the nationally renowned authorscomment on the “perverse” health care pay-ment system that fails to pay for quality whilepaying for defects, as follows: “In effect,the rewards in the payment system are per-verse; ordinary, even defective care, receivesthe same payment as optimal care.” Theygo on to state: “To overcome these barriers[to achieving quality], perverse reimburse-ments for care need to be designed out of thesystem.”44
Increased Profit Margins from Effectivenessand Efficiency
Many of our initial consulting engage-ments in the 1980s were from overuse ofservices, such as unnecessary spine surgery,carotid endarterectomies, coronary angiog-raphy and revascularization procedures, and

AS236-01 September 30, 2003 12:40 Char Count= 0
16 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
unnecessary cesarean sections. These costsaffected the payers of health care, whilegenerating revenue for hospitals and physi-cians. In capitated arrangements, however,these problems present real opportunities forquality improvement with financial gains.At Stanford University School of Medicine,physician-directed institutional peer review,coupled with positive physician feedback,decreased morbidity and mortality rates as-sociated with carotid endarterectomy whiledecreasing total cost of the procedure by 28percent.45 Peer review processes such as de-scribed by Stanford are essential to boards,senior management, and medical staffs inbreakthrough improvements in health carequality in the United States.
More recent experiences have focused onreducing length of stay, where overuse hasnot only cost the health care organization andpayers significant money but subjected pa-tients to unreasonable and unnecessary riskof harm. Examples of such overuse includeupper and lower gastrointestinal endoscopywhen patients do not have valid indications,delays in discharge from incidental findingsof enlarged prostates for prostatectomyworkup, and extensive spine surgeries withinstrumentation when minimally invasivesurgeries are clinically indicated.
QualVal’s experience with underuse, inthe deterioration of documentation and per-formance of adequate patient histories andphysical examinations, has been most dra-matic and disconcerting in recent years. Un-deruse of recognized and evidence-basedprocedures in the emergency departmentto institute timely reperfusion techniquesin acute coronary syndrome and appropri-ate medication for stroke within appropriatetime parameters are unfortunate and frequentfindings in our engagements, as examples.Failures to respond to and treat presenting
conditions such as anemia are not uncom-mon. In both the inpatient and outpatient set-tings, however, the most common example ofunderuse is failure to follow up on abnormallaboratory studies.
Developing diagnostic and treatmentplans based on evidence-based medicine andmonitoring quality to track effective and ef-ficient implementation of those plans is thefuture for this element of the quality-costproposition. A particularly striking exampleof such an opportunity is illustrated in thework of Stanley W. Dziuban, Jr., MD, and hiscolleagues at St. Peter’s Hospital in Albany,New York. The published NY risk-adjusteddata showed a higher than expected surgicalmortality in cardiac operations for this insti-tution. Initial medical record reviews failedto identify any quality of care problems.Statistical analysis was more revealing andlocalized the excess mortality to patientshaving high acuity, emergency coronaryartery bypass grafting (CABG). Theseoutcomes were remarkably different fromthe non-emergent patients who were stabi-lized prior to surgery. The staff instituteda focused effort to optimize the manage-ment of these emergency CABG patients.The result was zero mortality for emergencyCABG during the following year, down fromthe hospital’s actual mortality of 4.6 percent,which had been third highest in the state (ex-pected mortality for this facility was low at2.1 percent, the second lowest in the state forthe subject year, resulting in the conclusionof high mortality with low-risk cases).46
Joseph P. Newhouse correctly states in hisconsideration of the barriers that result in a“quality chasm”:
Greater use of information technology canhelp; if a patient’s medical history and allavailable test and medication data were

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 17
available online at the time a physician wasmaking a diagnostic or treatment decision,quality would surely improve. Greater useof computerized decision support systemsalso would improve quality.47
The national agenda for implementingquality improvement in health care and themethodology to measure quality have beenclearly established by the IOM and relatedentities. After a careful review of the collec-tion of reports from the IOM, including theroundtable quality studies, it is certain thatthe IOM is recommending a two-pronged ap-proach to the solution to errors in health careand improving patient safety:
1. Selection of appropriate treatmentplans rooted in evidence-basedmedicine; and
2. Monitoring proper and safe implemen-tation once the right performance stan-dard is selected.
Current Quality-Cost Research
A recent edition of Health Affairs was de-voted to “Quality: Where Is The Incentive?”with the lead article by Donald M. Berwick,MD, Sheila Leatherman, and their asso-ciates titled “The Business Case for Quality:Case Studies and an Analysis.”48 It summa-rized the findings of four case studies ofseven funded in part by the CommonwealthFund. The operational definition of the term“business case” was specifically stated asfollows:
A business case for a health care improve-ment intervention exists if the entity thatinvests in the intervention realizes a finan-cial return on its investment in a reason-able time frame, using a reasonable rateof discounting. This may be realized as
“bankable dollars” (profit), a reduction inlosses for a given program or population,or avoided costs. In addition, the businesscase may exist if the investing entity be-lieves that a positive indirect effect on orga-nizational function and sustainability willaccrue within a reasonable time frame.49
The authors make a distinction betweena business case, an economic case, and thesocial case for a quality improvement. In theeconomic case, financial benefits to the in-vestor occur “more than several years later.”The social case is essentially professional re-sponsibility in the traditional definition ofplacing the interests of the patient above fi-nancial interests.
Indeed, the studies selected for researchfunding are in and of themselves fascinating,with selection criteria summarized in thearticle as “Study Methods: Basic ProjectDesign.” The seven topics selected for casestudies were as follows:
1. Management of high-cost pharmaceu-ticals (low molecular weight heparin(LMWH) and statins);
2. Chronic care (diabetes management);3. Management of encounters (drop-in
group medical appointments);4. Prevention (smoking cessation);5. Health maintenance (wellness pro-
grams in the workplace);6. Hospital contracting (selective referral
to high-volume facilities); and7. Medical error reduction (computerized
physician order entry, or CPOE, formedications).
As the authors state: “Most of these in-terventions reflect attempts to correct under-use of effective care processes, rather thanto reduce overuse or misuse.”50 When therepresentatives of health care quality have

AS236-01 September 30, 2003 12:40 Char Count= 0
18 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
funds available to research this most impor-tant and compelling topic of the relationshipbetween quality and cost, review of the med-ical literature, such as the studies cited pre-viously considering underuse, overuse, andmisuse, would mandate very different casestudies in most instances. Clearly, the sav-ings from improved efficiencies of care fromeliminating or significantly reducing unnec-essary medical care, subjecting the patient tounreasonable harm, and the reduction of mis-use and avoidable complications and theirdirect and indirect costs, would be far moresignificant studies even if more politicallydangerous.
The Wall Street Journal story comment-ing on this article concluded from readingthe case studies and the authors’ summaryof these studies: “[T]he business case forquality is ‘weak or nonexistent’ in healthcare . . . .”51 This perception of the case stud-ies is particularly tragic in the context of thestated position of these distinguished authorsregarding motivation for quality improve-ment: “Without a business case for quality,we think it unlikely that the private sectorwill move quickly and reliably to widelyadopt proven quality improvements.”52
The most compelling case study summa-rized in this Health Affairs article is thestudy of the management of high-cost phar-maceuticals at the Henry Ford Health Sys-tem in Detroit. The study reports that inthe first six months of the study year 2001,only 29 of a cohort of 500 potentially el-igible patients were put on the LMWHprotocol. LMWH, for the purpose of thisstudy, was to treat deep vein thrombosis(DVT), a condition accounting for approx-imately 300,000 hospitalizations annually.Even though the cost of LMWH exceeds thecost of the most commonly prescribed al-
ternative by approximately $45 to $49 perday:
• Its proper use reduces hospitalizationsbecause it can be provided on an outpa-tient basis;
• It diminishes the need for laboratorytesting;
• It shortens lengths of stay for hospital-ized patients; and
• It reduces the overall costs by approxi-mately $800 per patient.
The potential savings at Henry FordHealth System from this LMWH protocolwas $360,000 per year, and it is significantthat some of the eligible patients are in itsown capitated health plan. It is further im-portant to note that another companion find-ing from the case study was that there wascontemporaneous use of LMWH in patientsfor whom it was not clinically approved(overuse).53
The significant finding of the study, fromthe perspective of our analysis, is stated inthe summary conclusions from the findingsof this study, as follows:
[A]t Henry Ford, harvesting the potentialof LMWH or lipid management provedvery difficult (at least in the early stages) inthe face of barriers in organizational cul-ture, communication, and habit. Poor im-plementation of a potentially effective in-novation is not a business-case problem;it is a management problem, although anoutsider may have a hard time telling thedifference.54 (Emphasis added.)
It is clear from this study and others, aswell as the experience of the authors, thatthe barriers to quality from organizationalstructure and culture cannot be overcomeby piecemeal quality and risk reduction

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 19
strategies. It is equally clear that physicianautonomy, as the barrier to efficient andeffective medical care, as well as patientsafety cannot continue to be acknowledgedbut ignored. At the recent Harvard Qual-ity Colloquium held in Cambridge, Mas-sachusetts, one of the physician participantsstated his opinion that the root cause of thecurrent health care quality dilemma is thatmedicine is “eminence-based, not evidence-based.” These barriers will be discussed indetail later in this article.
However, before leaving the consider-ation of the business case for quality, thedefinition presented previously must beconsidered as to its validity and relevance tothe current discussion of the quality-valueproposition. Harvey V. Fineberg, MD, PhD,president of the Institute of Medicine, doesnot include the restrictive time constrainton the definition of business case. Indeed,such a short-term restriction on return oninvestment is inconsistent with many of theinitiatives to measure performance for pay-ment mechanisms to discriminate betweenquality and disquality care. For example,Arnold Milstein, MD, medical director ofthe Pacific Business Group on Health and aco-founder of the Leapfrog Group, believesthat future payment incentives will be basedon longitudinal measures of health carequality rather than fixed, isolated points ofspecific services.
Those of us who work in health care soft-ware development endeavors know that thereare a number of different approaches and for-mulas used to determine return on invest-ment. Some examples are the business valueindex, scorecard economics, performancemanagement scorecard, total economic im-pact, and total value of opportunity. A morecarefully designed approach to return on in-
vestment will be essential in future researchand demonstration projects to build the sta-tistical business case for quality.
Fundamental Causes of theQuality Dilemma
Health care quality initiatives and risk re-duction strategies are not new in the UnitedStates. Indeed, after 10 years of impressiveendeavors to implement continuous qualityimprovement in health care through the Insti-tute for Healthcare Improvement, its leaderreported at its 10th anniversary annual meet-ing that despite these efforts, essentially noprogress toward improving quality had beenachieved. In addition, after years of veryambitious and well-conceived proactive riskreduction strategies by MMI medical mal-practice insurance company, the companywas purchased by St. Paul Insurance Com-pany and fell victim to St. Paul’s decision toexit the malpractice market completely.
There are two formidable obstacles to hos-pitals moving from this condition to theinevitable, optimal business model: (1) hos-pitals do not have the organizational struc-ture to maximize and realize their potentialas businesses; and (2) hospitals do not seethe quality of their product, health care, astheir fundamental business strategy.
The fundamental flaw in the existing orga-nizational structure of hospitals exists in theform of interdependent yet independent anddiscordant relationships between the hospi-tal boards of trustees and the medical staffs.The unquestionable result of this flaw, nomatter how the health care organization isstructured, is the type of barriers in organi-zational culture encountered and reported inthe case study at Henry Ford Health System,as discussed previously. The solution must

AS236-01 September 30, 2003 12:40 Char Count= 0
20 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
correct the fundamental structural flaw andbring boundary management to the culturaldivergence. Martin Merry, MD, describes thecultures of the board and medical staff as“silos.” We propose that Merry’s conceptof silos is correct, and we believe thathealth care culture traditionally encountersobstacles to promoting quality in hospitalswhen the various existing “cultures” are un-derstood in terms of the following threesilos:
1. Organizational culture (our structuralsilos);
2. Professional cultures (our professionalsilos, including Merry’s third “cultureof blame, it’s someone else’s responsi-bility” silo); and
3. Fragmented quality information cul-ture (our informational silos).
An organizational diagram of existingboard-medical staff relationships, shown inFigure 6, can best visualize the first two si-
Figure 6. Structural Silos of OrganizationalCulture
los, the organizational culture and the pro-fessional cultures.
The second silo, the professional cultures,must be carefully examined in the contextsof both internal deliberations of the medicalprofession and from outside medicine. Or-ganized medicine at the national and statelevels has focused considerable efforts in re-cent years to support the fundamental con-cept of physicians through their medical staffstructure being “self-regulating.” These con-cepts have achieved a degree of reverenceand a sacrosanct nature.55 When these con-cepts are advocated, they are not typicallyexpressed with reservation tied to the ex-plicit role of the hospital governing body.56
It is important to remember that these termsare a product of history, AMA dedication,and to some extent, a reading of the JointCommittee on Accreditation of HealthcareOrganizations (JCAHO) accreditation stan-dards focusing primarily on those governingthe medical staff. It is therefore necessaryto consider the problems these concepts cre-ate and further consider whether they makesense in light of modern quality concerns.
Jerome P. Kassirer, MD, former editor ofthe New England Journal of Medicine, statesthat a “fundamental tenet of a learned pro-fession is its obligation to self-regulate, self-monitor, and self-discipline its members.”57
His assessment of medicine concludes:
Unfortunately, when it comes to settingstandards of accountability and ethical be-havior, our professional organizations andmedical institutions have often faltered. Inthe guise of accountability, their effortshave often yielded lax standards that wereintentionally and flagrantly self-serving.This is pseudoaccountability. When suchdeceptive practices are uncovered, the pub-lic reacts—sometimes overreacts—and so

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 21
do legislators. The aspirations of our pro-fession would be better served if we set ourstandards of self-regulation unimpeach-ably high.58
Understanding why there is a quality prob-lem in developing a solution (or at least partsof a solution) at the hospital level requires anappreciation of stressors on the ability of theunderlying, traditionally independent medi-cal staff’s ability to apply correction. In ex-amining the stressors affecting the medicalstaff’s ability to implement modern qualitymeasures, we are forced to ask the follow-ing questions: (1) is it likely that they willbe able to overcome such difficulties; and(2) whether the board, under the current “del-egated quality” model, is able to assist themedical staff in overcoming these qualityhurdles.
Recognition of these two silos and theinherent solutions does not mean that themedical staff is excluded from the qualityimprovement and risk reduction processes.Rather, the medical staff is supported in itsrole by the board, and the board is supportedin its role by the medical staff. In otherwords, there is an integration of efforts. Thisapproach further supports the current qualityphilosophy focusing measurement and im-provement on systems, inherently includinga multidisciplinary architecture. Physiciansand the medical staff should not be blamedfor defects or deficiencies in clinical pro-cesses or emerging from non-physicianclinical professionals or from physical facil-ity or equipment over whom/which they haveno control. The medical staff should not betreated as a source of the problem; rather, themedical staff should be engaged as a victimof a structure that gives it the misapprehen-sion that it is solely responsible for quality.
Without such a process, quality enhance-ment efforts take on a “band aid” approach.
The informational silo resulting fromfragmented quality information is best con-sidered and understood in the context ofFigure 7, illustrating all of the disparatesources of clinical quality data and infor-mation in hospitals. Quality data and infor-mation are developed in a wide variety ofcontexts, using different methodologies tocollect different data for different purposesby a variety of different professionals fre-quently reporting to different senior man-agers. As a result, quality information hasbecome extremely fragmented and is notintegrated for clinical quality insight, de-cisions, and is not coordinated with orga-nizational strategic planning. The diagramin Figure 7 shows some of these disparatesources of quality data.
It can be argued that this third qualityinformation silo is simply a manifestationof the first two silos. However, the real-ity is that these fragmented and disparatedata sources have evolved from various well-intended quality initiatives propounded fromwithin the quality and risk management pro-fessional community and adopted for sep-arate JCAHO standards. The data and theprocesses generating the data have rarelybeen integrated, and data remains data ratherthan being transformed into information andknowledge on which the organization canact meaningfully and insightfully to improvequality and to reduce risk of patient harm.
A complete consideration of these threesilos is thoroughly detailed in another recentarticle.59 The solution proposed must first ad-dress the organizational flaw of the structuralsilo and the professional silo, augmentedby integrated and enhanced quality and pa-tient safety information formatted for the

AS236-01 September 30, 2003 12:40 Char Count= 0
22 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
Figure 7. Fragmented Clinical Quality Information Sources inthe Informational Silo
various constituencies within the health careorganization.
The Basis for Solutions to AchieveQuality While Reducing Costs
The basis for solutions to achieve con-sistently high quality, error-free health caremust be founded on recognition and un-derstanding of the fundamental flaws fromthe three silos of structure, function, andinformation. These three categories of im-
pediments to health care quality and patientsafety have sub-categories of root causes,which are summarized in Figure 8.
The reason quality improvement andrisk reduction strategies have failed in thepast is that there has been no recogni-tion and understanding of these root causesof the quality and safety challenges. Anyefforts to rapidly change these dynam-ics must focus on these multi-factorial el-ements for a meaningful and successfulsolution.

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 23
Figure 8. Impediments to Health Care Quality and Patient Safety
A primary obstacle to making quality adriving business strategy is that there aremany constituencies in health care, andwhenever there is a financial incentive forone or several constituent(s) there is almostalways a negative effect on another or otherconstituencies. What is good for physiciansmay not be good for hospitals, and what isin the best interests of patients may not be inthe best interests of payers. These financialincentives and disincentives become veryconvoluted between and even among thevarious parties in what should be a simpleand straightforward business proposition.
US medicine, with its exceptionallywell-trained and devoted physicians and
clinicians, and with all of its technology andinnovations, is without parallel in the world.Yet, the quality of health care in the UnitedStates has become the subject of intensecontroversy in recent years. The disparitybetween these two realities results frominconsistencies in care, not from potentialcapability. Quality, in so many ways andthroughout industries and businesses, isabout consistency, reducing “defects”and variability in systems and processes.However, unlike so many other industries inwhich there are other outside mechanisms inplace to support internal endeavors to reduceerror, focusing on only the systems and pro-cesses and not on the people dynamic will

AS236-01 September 30, 2003 12:40 Char Count= 0
24 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
not totally solve the problems. For example,in the oft cited airline industry with its noblame approach to errors and near misses,physicians and clinicians do not get intosimulators to receive clinical privileges, arenot required to train in approved learningsituations to undertake new procedures withnew equipment, do not go through rigorouschecklists to perform their tasks, and donot surrender investigation of accidents to afederal agency of outside experts.
We recently sat with a former CEO ofseveral major hospital corporations duringa distinguished career. The topic was toprobe the incentives for health care orga-nizations to undertake quality improvementand risk reduction programs from a new andcompelling perspective. The response, whiledevastating and alarming, seems to be true—
Figure 9. Six Sigma Diagram of Costs of Disquality to an Employer
“there isn’t enough pain.” It is truly apparentthat hospital administrators, financial offi-cers board members, and medical staff lead-ership do not routinely do two things: (1) re-late quality to finance; and (2) appreciatethe intra-hospital structural problems thatimpede quality attainment. Thus, the busi-ness case for quality—the return on invest-ment from quality improvement and patientsafety—is neither understood nor embraced.
The pressures on payers and employers,including the federal government, will in-evitably result in pressures on health careproviders to measure performance to achievemarketplace position for payment based onquality. Many in health care mistakenly be-lieve that this is just another threat that willnot achieve fruition. However, recent presen-tations on efforts of payers and particularly

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 25
employers demonstrate that this pressure iseminent in certain markets. The pressuresin some markets from the Leapfrog Groupshould be noted. A recent presentation fromGE, however, elevates the need for healthcare organizations to understand how thesepressures will become manifest.
As an employer, GE has evaluated the op-portunities for savings on health care ex-penditures in a familiar Six Sigma graphicfashion (shown in Figure 9).
GE studied public accessible databases toevaluate the efficiency and effectiveness ofhospitals in specific areas. It compared thisevaluation with where its employees receivecare and determined that the most effective
Figure 10. Employer Determinations of Hospitals Demonstrating Efficiency andEffectiveness vs. Where Their Employees Are Receiving Health Care
and efficient hospitals were not the hospitalswhere most of its employees were receivingcare. This information is presented as “bub-ble charts” in Figure 10.
The bubbles centered around zero percentrepresent hospitals demonstrating effective-ness as determined from actual vs. expectedmortality or complications. These were de-termined as the most effective hospitals inthese selected regions. The numbers in theother bubbles as compared to these mosteffective hospitals demonstrate that the GEemployees go to other hospitals rather thanthese hospitals in each region. Based on thesedeterminations, GE will attempt to influenceits employees in selected regions to select the

AS236-01 September 30, 2003 12:40 Char Count= 0
26 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
most effective hospitals by having a small orno co-pay for the effective hospitals vs. largeco-pay for relatively ineffective hospitals.
This approach from employers, as wellas the federal initiative to develop perfor-mance measures to be implemented by CMS,should alert health care providers that thereis an absolute imperative to become involvedimmediately in the analysis of health carequality information and to restructure toeliminate the impediments to quality fromorganizational structure and culture. Thiswill further demand integrated quality datafor consideration at the board level qualitycommittee. Competitive health care organi-zations will not wait for these external forcesto compel these recommendations. Astute
Figure 11. Incremental Opportunities on the Health Care Continuum for FinancialIncentives to Influence Patient Decisions
organizations will want to become involvedin the formulation of performance measures,as well as in the organizational impera-tives to transform to a quality-value businessstrategy.
Long term, the solutions will come froma four-pronged approach that the authors de-scribe as having the following elements andterm “QReview”:
• Prospective design of systems to pro-vide effective, efficient, and safe healthcare processes premised on evidence-based best practice models using pro-cess modeling and FMEA;
• Concurrent monitoring to be certain thatthe correct health care protocol has been

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 27
selected and is being implemented foreach patient;
• Retrospective assessment of integratedquality, risk, and clinical performanceinformation databases; and
• Quality, risk, and clinical performanceinformation feedback loops to contin-uously learn from clinical experienceand to integrate new experiential andresearch information into continuousprospective design.
It will be important for health care orga-nizations to consider the same points alongthe continuum of care for quality interven-tions and opportunities to implement qual-ity initiatives that employers are using toconsider intervention strategies. An exam-ple of such intervention points is shown inFigure 11.
The dotted box shows prevention, physi-cian selection, treatment decisions, selectionof specialists and hospitals, and health status/return to work as the key intervention pointsalong this continuum of care.
In the short and immediate term, the so-lutions must immediately focus on the retro-spective and then rapidly move to concurrentelements of this formula. These immediatesolutions will require:
• Creating board level, multi-disciplinaryquality and safety committees withboard level commitment to improv-ing quality and patient safety and
restructuring beyond simple restructur-ing efforts now underway in many or-ganizations;
• Providing integrated quality and riskinformation to these entities with com-mitment of resources from senior man-agement;
• Training of board members to interpretand understand quality and risk datawith the same level of sophistication asthey review audited financial informa-tion and to understand interventions andmonitoring available to them for solu-tions to defects in the system;
• Addressing the cultural impedimentsinculcated into the silos and addressingthe hard issue of physician expectationsof independence and autonomy and theexpectations of boards and senior man-agement that the doctors will handle thequality; and
• Moving to organizations that devote sig-nificant resources to quality and safetyand to the development of predeter-mined and monitored systems and pro-cesses of care, far beyond the isolatedand piloted protocols for several chronicconditions.
The simple but compelling thesis of theauthors is that health care must immedi-ately engage in the transformation to mak-ing quality of medical care the fundamentalbusiness strategy of the organization.
REFERENCES
1. See, e.g., “A New Way to Get Doctors to TakeBetter Care of Patients: Bribe Them,” The WallStreet Journal, April 10, 2003.
2. See, e.g., Health Affairs, Volume 22, Number2 (March/April 2003).
3. S. Leatherman, D. Berwick, D. Iles, and L.S.Lewin, et al., “The Business Case for Quality:
Case Studies and an Analysis,” Health Affairs,22, 2: 17–30 (March/April 2003).
4. M.R. Chassin, “Is Health Care Ready for SixSigma Quality?,” Milbank Quarterly, 76, 4:565–591 at p.567 (1998).
5. See Committee on Quality of Health Carein America, Institute of Medicine, To Err Is

AS236-01 September 30, 2003 12:40 Char Count= 0
28 JOURNAL OF HEALTH CARE FINANCE/WINTER 2003
Human: Building a Safer Health Care System(LT Kohn et al., editors, 2000).
6. R.W. Dubois and R.H. Brook, “PreventableDeaths: Who, How Often, and Why?,” An-nals of Internal Medicine, 109: 582–589(1988).
7. R.H. Brook, C.J. Kamberg, and A. Mayer-Oakes, et al., “Appropriateness of Acute Med-ical Care for the Elderly: An Analysis of theLiterature,” Health Policy, 14: 225–242(1990).
8. National Quality Forum (Forum for HealthCare Quality Measurement and Reporting),“A Call to Action,” p.2 (2001) available atwww.qualityforum.org; Institute of Medicine,supra n.5 at p.1.
9. Robert Wood Johnson Foundation, “Call forProposals: Pursuing Perfection, Raising the Barfor Health Care Performance” (02/15/2000).
10. J. Wennberg, Dartmouth Atlas of Health Carein the United States (1999).
11. E.A. McGlynn, S.M. Asch, and J. Adams, et al.,“The Quality of Health Care Delivered toAdults in the United States,” New EnglandJournal of Medicine, 348, 26: 2,635–2,645(2003).
12. B. Starfield, “Commentary: Is US Health Re-ally the Best in the World?,” Journal of theAmerican Medical Association, 284, 4: 483–485 (2000).
13. E.J. Thomas and D.M. Studdert, et al., “Costsof Medical Injuries in Colorado and Utah,”Inquiry, 36: 255–264 (1999); W.G. Johnsonand T.A. Brennan, et al., “The EconomicConsequences of Medical Injuries,” Journalof the American Medical Association, 267:2,487–2,492 (1992); cited in the Institute ofMedicine’s, To Err Is Human: Building a SaferHealth System at p.1 (2000).
14. D.H. Mills, “Medical Insurance FeasibilityStudy—A Technical Summary,” Western Jour-nal of Medicine: 360–365 (1978).
15. M.L. Millenson, “The Silence,” Health Affairs,22, 2: 103–112 at p.106 (2003).
16. See Institute of Medicine, supra n.5.17. See, e.g., R.A. Hayward and T.P. Hofer, “Esti-
mating Hospital Deaths Due to Medical Errors:Preventability Is in the Eye of the Reviewer,”Journal of the American Medical Association,286, 4: 415–420 (2001); H.C. Sox and S.Woloshin, “How Many Deaths Are Due toMedical Error? Getting the Number Right,” Ef-fective Clinical Practice, American College ofPhysicians, www.acponline.org/journals/ecp/
novdec00/sox.htm (last visited May 9, 2003);“An ‘Epidemic’ of Medical Malpractice? ACommentary on the Harvard Medical Prac-tice Study,” www.thedoctors.com/advocacy/ourcause/harvardstudy/commentary.asp (lastvisited January 19, 2003).
18. T.A. Brennan, “Sounding Board: The Insti-tute of Medicine Report on Medical Errors—Could It Do Harm?,” New England Journal ofMedicine, 342, 15: 1,123–1,125 (2000); Fora different perspective of the methodology toimprove quality in health care from the sys-tems approach of the IOM, see also StephenR. Latham, “System and Responsibility: ThreeReadings of the IOM Report on Medical Er-rors,” American Journal of Law & Medicine,27: 163–179 (2001).
19. L.L. Leape, T.A. Brennan, and N. Laird, et al.,“The Nature of Adverse Events in Hospital-ized Patients,” The New England Journal ofMedicine, 324, 6: 377–384 (1991).
20. M.R. Chassin, supra n.4 at p.570.21. M.R. Chassin, supra n.4 at p.566.22. S.J. Bernstein, E.A. McGlynn, and A.L. Siu,
et al., “The Appropriateness of Hysterectomy:A Comparison of Core in Seven Health Sys-tems,” Journal of the American Medical Asso-ciation, 269: 2,398 (1993).
23. See R.A. Lange and L.D. Hillis, “Use andOveruse of Angiography and Revasculariza-tion for Acute Coronary Syndromes,” NewEngland Journal of Medicine, 338: 1,838–1,839 (1998).
24. R. Gonzales, J.F. Steiner, and M.A. Sande,“Antibiotic Prescribing for Adults with Colds,Upper Respiratory Tract Infections, and Bron-chitis by Ambulatory Care Physicians,” Jour-nal of the American Medical Association, 278:901–904 (1997) (21 percent prescribed antibi-otics to ambulatory patients to treat colds orother viral respiratory infections, conditions forwhich they are useless, and the defect rate was210,000 per million).
25. M.R. Chassin, supra n.4 at p.573.26. M.R. Chassin, supra n.4 at p.574.27. S.B. Soumerai, T.J. McLaughlin, and D.
Spiegelman, et al., “Adverse Outcomes of Un-der Use of Beta-Blockers in Elder Survivorsof Acute Myocardial Infarction,” Journal ofthe American Medical Association, 277: 115–121 (1997) (only 21 percent receive beta-blockers).
28. K.B. Wells, R.D. Hays, and M.A. Burnam,et al., “Detection of Depressive Disorder for

AS236-01 September 30, 2003 12:40 Char Count= 0
The Quality-Value Proposition in Health Care 29
Patients Receiving Prepaid or Fee-for-ServiceCare,” Journal of the American Medical Asso-ciation, 262: 3,298–3,302 (1989).
29. M.R. Chassin, supra n.4 at pp.576–577.30. The experience and insight of the authors is far
greater than the literature with the problem ofmisuse; however, this discussion is beyond thescope of this article.
31. M.R. Chassin, supra n.4 at pp.569–570.32. Supra n.4.33. D. Bates, N. Spell, and D. Cullen, et al., “Costs
of Adverse Drug Events in Hospitalized Pa-tients,” Journal of the American Medical As-sociation, 277: 307–311 (1997).
34. See, e.g., L Goldman et al., “The Value of theAutopsy in Three Medical Eras,” The New Eng-land Journal of Medicine, 308: 1,000–1,005(1983); E.C. Burton et al., “Autopsy Diag-noses of Malignant Neoplasms: How Often AreClinical Diagnoses Incorrect?,” Journal of theAmerican Medical Ass’n, 280: 1,245–1,248(1997).
35. Midwest Business Group on Health in collab-oration with the Juran Institute, Inc. and theSeveryn Group, Inc., “Reducing the Costs ofPoor-Quality Health Care Through Responsi-ble Purchasing Leadership (2002).
36. “Reinsurance Market Review, November2002” at p.1 (Willis Limited, London, UnitedKingdom, 2002).
37. “Marketplace Realities and Risk ManagementSolutions,” at p.66 (Willis Limited, London,United Kingdom 2002).
38. Supra n.36 at p.24.39. J.C. Mohr, “American Medical Malpractice Lit-
igation in Historical Perspective,” Journal ofthe American Medical Ass’n, 283, 13: 1,731–1,737 (2000).
40. M.L. Millenson, supra n.15 at p.105.41. E. Freidson, Profession of Medicine: A Study of
the Sociology of Applied Knowledge at p.347(New York: Dodd, Mead, 1970).
42. Jossey-Bass Publishers (San Francisco, 1999).43. Committee on Enhancing Federal Healthcare
Quality Programs, The National AcademiesPress (Washington, D.C., 2002).
44. S. Leatherman, D. Berwick, D. Iles, and L.S.Lewin, et al., “The Business Case for Quality:Case Studies and an Analysis,” Health Affairs,22, 2: 17–30 (March/April 2003).
45. C. Olcott, R.S. Mitchell, and G.K. Steinberg,et al., “Institutional Peer Review Can Re-duce the Risk and Cost of Carotid Endarterec-
tomy,” Archives of Surgery, 135: 939–942(2000).
46. S.W. Dziubian, J.B. McIlduff, and S.J. Miller,et al., “How a New York Cardiac Surgery Pro-gram Uses Outcomes Data,” Annals of Tho-racic Surgery, 58: 1,871–1,876 (1994).
47. J.P. Newhouse, “Why Is There a QualityChasm?,” Health Affairs, 21, 4: 13–25 at p.23(2002) (while the authors agree with the quotedconclusion, the barriers to achieving quality aspresented in the body of the article are at oddswith the thesis of the authors of this article).
48. Leatherman et al., supra n.44.49. Id. at p.18.50. Id.51. Supra n.1.52. Supra n.44 at p.18.53. For a detailed report of this study, see H. Smits,
B. Zarowitz, V.K. Sahney, and L. Suvitz, FieldReport, “The Business Case for Pharmaceuti-cal Management: A Case Study,” (April 2003),available from The Commonwealth Fund Website www.cmwf.org (report #613).
54. Supra n.44 at p.23.55. See, e.g., J.P. Kassirer, “Financial Conflict of In-
terest: An Unresolved Ethical Frontier,” Ameri-can Journal of Law & Medicine, 27, 2–3: 149–162 (2001).
56. Exeter Hospital Medical Staff et al v. Board ofTrustees of Exeter Health Resources Inc. (NHstate court) (AMA files amicus brief in casein which medical staff sues hospital govern-ing body for unilaterally removing the medicalstaff president from the board of directors andrefusing to allow him to speak at meeting; thetrial court dismissed the cause of action be-cause the medical staff, as an entity, has nostanding to sue the hospital with which it isaffiliated). The AMA further reported the hold-ing as “leaving doctors with no legal resourceagainst hospitals.” www.ama-assn.org/sci-bs/amnews/pick 02/prsb0318.htm, last visitedOctober 28, 2002.
57. J.P. Kassirer, “Perspective: Pseudoaccountabil-ity,” Annals of Internal Medicine, 134: 587–590 (2001).
58. Id. at p.587.59. J.P. Marren, G.L. Feazell, and M.W. Paddock,
“The Hospital Board at Risk and the Need toRestructure the Relationship with the MedicalStaff: Bylaws, Peer Review and Related Solu-tions,” Annals of Health Law, 12, 2: 179–234(2003).