The Blumgart Preoperative Staging System for Hilar...
13
The Blumgart Preoperative Staging System for Hilar Cholangiocarcinoma: Analysis of Resectability and Outcomes in 380 Patients Kenichi Matsuo, MD, Flavio G Rocha, MD, Kaori Ito, MD, Michael I D’Angelica, MD, FACS, Peter J Allen, MD, FACS, Yuman Fong, MD, FACS, Ronald P DeMatteo, MD, FACS, Mithat Gonen, PhD, Itaru Endo, MD, William R Jarnagin, MD, FACS BACKGROUND: Complete resection of hilar cholangiocarcinoma (HCCA) is a critical determinant of long-term survival. This study validates a previously reported preoperative clinical T staging system for determining resectability of HCCA. STUDY DESIGN: Consecutive patients with confirmed HCCA treated over an 18-year period were included. Patient demographics, preoperative imaging studies, resection type, margin status, lymph node status, histopathologic findings, morbidity, and outcomes were entered prospectively and ana- lyzed retrospectively; changes in these variables over time were assessed. All patients were placed into 1 of 3 stages based on the extent of ductal involvement by tumor, portal vein compromise, or lobar atrophy. RESULTS: From March 1991 through December 2008, 380 patients were evaluated. Eighty-five patients had unresectable disease; 295 patients underwent exploration with curative intent. One hun- dred fifty-seven patients underwent resection: 129 (82.2%) had a concomitant hepatic resec- tion and 120 (76.4%) had an R0 resection. Of the 32 actual 5-year survivors (120 at risk), 30 patients (93.8%) had a concomitant hepatic resection. In patients who underwent an R0 resection, concomitant partial hepatectomy, well-differentiated histology, and negative lymph nodes were independent predictors of long-term survival. In the 376 patients whose disease could be staged, the preoperative clinical T staging system predicted resectability (p 0.001), metastatic disease (p 0.001), and R0 resection (p 0.007). CONCLUSIONS: The preoperative clinical T staging system of Blumgart, defined by the radial and longitudinal tumor extent, accurately predicts resectability of HCCA. The full outcomes benefit of resection is realized only if a concomitant partial hepatectomy is performed. ( J Am Coll Surg 2012;215: 343–355. © 2012 by the American College of Surgeons) Cholangiocarcinoma is a rare disease, accounting for less than 2% of all human malignancies. 1 Adenocarcinoma may arise anywhere within the biliary tree, from the intrahepatic radicles to just proximal to the ampulla of Vater. Excluding gallbladder carcinoma, tumors involv- ing the biliary confluence or the right or left hepatic ducts, known as hilar cholangiocarcinoma (HCCA), ap- pear to be the most common cancers of the extrahepatic ductal system. It is notable, however, that the proportion of patients with hilar tumors has generally remained constant over the past several years, 2,3 but recent reports have shown a rising incidence of tumors originating from the intrahepatic biliary tree (ie, intrahepatic cholangiocarcinoma). 4 Complete resection is the most effective treatment for HCCA, although most patients have unresectable disease, either at presentation or at exploration. 5-7 Most studies on HCCA originate from surgical departments and tend to focus on operative findings and results, excluding those with unresectable disease, and do not account fully for all CME questions for this article available at http://jacscme.facs.org Disclosure Information: Authors have nothing to disclose. Timothy J Eberlein, Editor-in-Chief, has nothing to disclose. Received March 2, 2012; Revised May 4, 2012; Accepted May 9, 2012. From the Department of Surgery (Matsuo, Rocha, Ito, D’Angelica, Allen, Fong, DeMatteo, Jarnagin), Department of Epidemiology and Biostatistics (Gonen), Memorial Sloan-Kettering Cancer Center, New York, NY; the De- partment of Gastroenterological Surgery, Yokohama City University, Gradu- ate School of Medicine, Yokohama, Japan (Matsuo, Endo). Correspondence address: William R Jarnagin, MD, FACS, Department of Surgery, Memorial Sloan-Kettering Cancer Center, 1275 York Ave, New York, NY 10065. email: [email protected] 343 © 2012 by the American College of Surgeons ISSN 1072-7515/12/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jamcollsurg.2012.05.025
Transcript of The Blumgart Preoperative Staging System for Hilar...

The Blumgart Preoperative Staging System for HilarCholangiocarcinoma: Analysis of Resectability andOutcomes in 380 PatientsKenichi Matsuo, MD, Flavio G Rocha, MD, Kaori Ito, MD, Michael I D’Angelica, MD, FACS,Peter J Allen, MD, FACS, Yuman Fong, MD, FACS, Ronald P DeMatteo, MD, FACS, Mithat Gonen, PhD,Itaru Endo, MD, William R Jarnagin, MD, FACS
BACKGROUND: Complete resection of hilar cholangiocarcinoma (HCCA) is a critical determinant of long-termsurvival. This study validates a previously reported preoperative clinical T staging system fordetermining resectability of HCCA.
STUDY DESIGN: Consecutive patients with confirmed HCCA treated over an 18-year period were included.Patient demographics, preoperative imaging studies, resection type, margin status, lymph nodestatus, histopathologic findings, morbidity, and outcomes were entered prospectively and ana-lyzed retrospectively; changes in these variables over time were assessed. All patients were placedinto 1 of 3 stages based on the extent of ductal involvement by tumor, portal vein compromise,or lobar atrophy.
RESULTS: From March 1991 through December 2008, 380 patients were evaluated. Eighty-five patientshad unresectable disease; 295 patients underwent exploration with curative intent. One hun-dred fifty-seven patients underwent resection: 129 (82.2%) had a concomitant hepatic resec-tion and 120 (76.4%) had an R0 resection. Of the 32 actual 5-year survivors (120 at risk), 30patients (93.8%) had a concomitant hepatic resection. In patients who underwent an R0resection, concomitant partial hepatectomy, well-differentiated histology, and negative lymphnodes were independent predictors of long-term survival. In the 376 patients whose diseasecould be staged, the preoperative clinical T staging system predicted resectability (p � 0.001),metastatic disease (p � 0.001), and R0 resection (p � 0.007).
CONCLUSIONS: The preoperative clinical T staging system of Blumgart, defined by the radial and longitudinaltumor extent, accurately predicts resectability of HCCA. The full outcomes benefit of resectionis realized only if a concomitant partial hepatectomy is performed. (J Am Coll Surg 2012;215:343–355. © 2012 by the American College of Surgeons)
Cholangiocarcinoma is a rare disease, accounting for lessthan 2% of all human malignancies.1 Adenocarcinomamay arise anywhere within the biliary tree, from theintrahepatic radicles to just proximal to the ampulla of
Vater. Excluding gallbladder carcinoma, tumors involv-ing the biliary confluence or the right or left hepaticducts, known as hilar cholangiocarcinoma (HCCA), ap-pear to be the most common cancers of the extrahepaticductal system. It is notable, however, that the proportionof patients with hilar tumors has generally remainedconstant over the past several years,2,3 but recent reportshave shown a rising incidence of tumors originatingfrom the intrahepatic biliary tree (ie, intrahepaticcholangiocarcinoma).4
Complete resection is the most effective treatment forHCCA, although most patients have unresectable disease,either at presentation or at exploration.5-7 Most studies onHCCA originate from surgical departments and tend tofocus on operative findings and results, excluding thosewith unresectable disease, and do not account fully for all
CME questions for this article available athttp://jacscme.facs.orgDisclosure Information: Authors have nothing to disclose. Timothy JEberlein, Editor-in-Chief, has nothing to disclose.
Received March 2, 2012; Revised May 4, 2012; Accepted May 9, 2012.From the Department of Surgery (Matsuo, Rocha, Ito, D’Angelica, Allen,Fong, DeMatteo, Jarnagin), Department of Epidemiology and Biostatistics(Gonen), Memorial Sloan-Kettering Cancer Center, New York, NY; the De-partment of Gastroenterological Surgery, Yokohama City University, Gradu-ate School of Medicine, Yokohama, Japan (Matsuo, Endo).Correspondence address: William R Jarnagin, MD, FACS, Department ofSurgery, Memorial Sloan-Kettering Cancer Center, 1275 York Ave, NewYork, NY 10065. email: [email protected]
343© 2012 by the American College of Surgeons ISSN 1072-7515/12/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jamcollsurg.2012.05.025

evaluated patients.3, 8-12 Additionally, criteria of irresectabil-ity related to technical and oncologic variables, may varyfrom center to center.
Although these and other variables make it difficult to esti-mate the resectability rate of HCCA, there is no debate thatlong-term survival depends on complete tumor resection,with an en bloc partial hepatectomy in most cases.6-7,9,13 How-ever, accurate assessment of the factors that contribute to re-sectability, even with multiple complementary imaging stud-ies, is challenging, as evidenced by the high proportion ofpatients identified with irresectable disease at operation. Apreoperative clinical staging system that accurately assesses re-sectability, unlike the American Joint Committee on Cancer(AJCC)14 and the Bismuth-Corlette classifications,15-16 wouldbe of value clinically.
We have shown previously that a preoperative T stagingsystem, defined by biliary tumor extent, the presence orabsence of portal vein involvement, and the presence orabsence of hepatic lobar atrophy, may be useful for predict-ing resectability and the likelihood of finding metastaticdisease.5,6 This study represents an analysis of all patientswith HCCA who were evaluated and treated during an18-year period at a single institution, including those withunresectable disease. The primary aim was to validate thepredictive value of a preoperative clinical staging system;the secondary aim was to update the long-term results.
METHODSThis study was approved by the Memorial Sloan-KetteringCancer Center (MSKCC) Institutional Review Board;HIPAA compliance was assured. All patients with a diag-nosis of HCCA evaluated and treated at MSKCC since1991 were identified from a Department of Surgery data-base. Demographic, laboratory, radiologic, histopatho-logic, operative, perioperative, and survival data wereentered prospectively and analyzed retrospectively. Addi-tional data were obtained as necessary from review of themedical record. In this study, only patients with biliaryadenocarcinoma arising from the biliary confluence or theright or left main hepatic ducts were included; patients
with other histologies such as carcinoid and lymphomawere excluded. Patients with tumors originating in theproximal common hepatic duct were included if the tumorextended to the biliary confluence. Patients with diffuse ormultifocal cholangiocarcinoma were included, providedthat the right or left hepatic duct or the biliary confluencewas involved. Patients with papillary cholangiocarcinomawere included.
Patient evaluationInitial assessment of all patients included a complete his-tory and physical examination, assessment of generalhealth, and review of available test results, imaging studies,and histopathology. Patients were usually referred after atleast partial radiographic evaluation had been completed,which, in most instances, consisted of a CT scan and eitherendoscopic or percutaneous cholangiography. In manycases, biliary stents were placed as part of the cholangio-graphic procedure. After referral, further evaluation ofbiliary tumor extent and assessment of possible vascularinvolvement and/or metastatic disease were typically per-formed with magnetic resonance cholangiopancreatogra-phy (MRCP) and duplex ultrasonography; CT angiogra-phy was also used frequently. More recently, positronemission tomography with [(18)F]fluoro-2-deoxy-D-glucose(FDG-PET) has been used to identify occult metastatic dis-ease, although not in all patients, and its use remains investi-gational.17 All cases were reviewed at a multidisciplinary hepa-tobiliary disease management conference.
Criteria precluding patients from resection includedgeneral factors such as the presence of hepatic cirrhosis orother medical unfitness, local tumor-related factors such asinvasion of the secondary biliary radicles, main portal vein,or any combination of unilateral secondary biliary in-volvement or portal vein involvement with contralateralliver atrophy, and histologically proven metastasis to dis-tant sites such as liver, lung, peritoneum, and N2-lymphnodes (defined as peripancreatic, periduodenal, celiac,superior mesenteric, or posterior pancreaticoduode-nal).5,6 Patients with potentially resectable tumors un-derwent further evaluation with a screening chest radio-graph, routine laboratory studies, assessment by ananesthesiologist, and formal cardiopulmonary testing ifwarranted. Complications related to biliary tract ob-struction or previous biliary intervention (ie, cholangi-tis, pancreatitis, biliary injury), if present, were treatedbefore surgery. In some patients, this required replace-ment of existing biliary catheters, insertion of new cath-eters to drain contaminated and obstructed areas of thebiliary tree, drainage of extrahepatic collections, and/ora prolonged course of antibiotics. Routine biliary drain-age of jaundiced patients, not previously stented and
Abbreviations and Acronyms
AJCC � American Joint Committee on CancerDSS � disease-specific survivalFDG-PET � positron emission tomography with [(18) F]
fluoro-2-deoxy-D-glucoseHCCA � hilar cholangiocarcinomaMDCT � multidetector-row computed tomographyMRCP � magnetic resonance cholangiopancreatographyMSKCC � Memorial Sloan-Kettering Cancer Center
344 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

without cholangitis, was not performed18,19 if an opera-tion could be performed in a timely fashion (withinapproximately 1 week). Preoperative portal vein embo-lization (in patients without lobar atrophy) was rarelyused.
Biopsy material from the referring institution was re-examined. In patients with advanced disease or in thoseunfit for surgery, biopsy confirmation of the diagnosis wasperformed, if not done previously, and plastic biliary drain-age catheters were converted to self-expandable metallicstents. However, when the imaging studies suggested a po-tentially resectable HCCA, histologic confirmation of ma-lignancy was not pursued before operation.
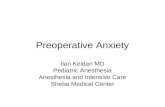
Preoperative tumor stagingUsing preoperative imaging studies, all patients were stagedaccording to the preoperative clinical T staging system de-scribed previously (Fig. 1).6 This staging system stratifiestumors based on local tumor extent within the biliary tree,the presence or absence of portal venous involvement, andthe presence or absence of hepatic lobar atrophy. The first225 patients in this series had been staged previously usingthis system.5,6 Of the 6 patients who could not be staged atthat time, 2 patients were subsequently staged in this studyafter obtaining and re-evaluating preoperative imagingstudies including those done at the referring hospitals. Theremaining patients were staged after thorough review of allimaging studies.
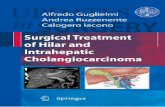
The extent of biliary and portal venous involvement bytumor was assessed with a combination of duplex ultra-sonography, MRCP, and CT. Direct cholangiography wasused selectively, but it was generally not performed solelyfor diagnostic purposes. When appropriate, MRCP wasused instead of invasive biliary intervention to identify ob-structed or isolated ducts not seen on percutaneous or en-doscopic procedures.18,19 Portal venous involvement wasconsidered present if the tumor contacted and either dis-torted or narrowed the vein, or if the vein was encased oroccluded. Hepatic lobar atrophy was considered present ifcross-sectional imaging showed a small, often hypoper-fused lobe with crowding of dilated intrahepatic bile ducts(Fig. 2).5,6,20
Conduct of the operationIn patients undergoing a potentially curative resection, astandard operative approach was used as previously de-scribed.5,6,21 Removal of the supraduodenal bile duct andgallbladder was performed en bloc with a complete sub-hilar lymphadenectomy and concomitant partial hepatec-tomy in nearly all cases. Caudate lobectomy was performedroutinely for tumors involving the left hepatic duct or,when necessary, to accomplish complete tumor clearance.Histologic assessment of resection margins was performedintraoperatively. Additional tissue was resected, if feasible,when residual microscopic disease was suspected based onfrozen-section histology.22 Resection and reconstruction of
Figure 1. Proposed T stage criteria for hilar cholangiocarcinoma. T1 corresponds to tumorinvolving biliary confluence with unilateral extension to second-order biliary radicles. T2 corre-sponds to tumor involving biliary confluence with unilateral extension to second-order biliaryradicles and ipsilateral portal vein involvement or ipsilateral hepatic atrophy. T3 corresponds totumor involving biliary confluence with bilateral extension to second-order biliary radicles; orunilateral extension to second-order biliary radicles with contralateral portal vein involvement; orunilateral extension to second-order biliary radicles with contralateral hepatic lobar atrophy;or main or bilateral portal venous involvement.
345Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes

major vascular structures were performed when necessaryto achieve complete tumor clearance in patients whose dis-ease was otherwise resectable. Roux-en-Y biliary-enteric re-construction was performed to a segment of jejunum ap-proximately 70 cm in length.
Some patients with unresectable tumors were often re-ferred for systemic chemotherapy or chemoradiation ther-apy, as appropriate, based on disease extent. However, ad-juvant chemotherapy was not used routinely in patientswho underwent a complete resection.
Data analysisPatient demographics, findings of radiographic investiga-tions, and final patient disposition were recorded. In pa-tients who underwent surgery, the operative findings, op-erative procedures, estimated blood loss (as recorded by theanesthesiologist), length of hospital stay (from the time of
operation to discharge), and postoperative complicationswere recorded. Postoperative complications were recordedprospectively into a department database and graded inseverity using a score of 0 (no complication) to 5 (periop-erative mortality), as described previously.23 Surgery-related mortality was defined as any death resulting from acomplication of the operation, whenever it occurred.Transfusion of any blood products (packed red cells, wholeblood, fresh frozen plasma, or platelets) during the opera-tion or at any time during the hospital stay after surgery wasalso recorded. Tumor size, differentiation, status of the re-section margin (negative [R0] or positive [R1]), metastaticdisease to resected lymph nodes, and final tumor stageaccording to the AJCC staging system14 were analyzed. Anyevidence of microscopic tumor at the biliary, vascular, he-patic, or soft-tissue resection margin constituted an R1resection.Tumor differentiation (well, moderate, poor) was
Figure 2. (A) Axial magnetic resonance cholangiopancreatography (MRCP) image of a patientwith hilar cholangiocarcinoma and left lobe atrophy. The bile ducts appear white (black arrow).The left liver is shrunken, with crowding and dilatation of the bile ducts. (B) Axial MRCP imageof a patient with papillary hilar cholangiocarcinoma. An ill-defined mass is identified at the portalhilum (black arrow) abutting the junction of the right sectorial ducts (white arrow). The left lobeis atrophic, with dilated and crowded bile ducts (white arrowhead). (C) Axial contrast-enhancedCT of a patient with considerable atrophy of the left liver and dilatation of the left, right, andcaudate biliary ducts. (D) Marked tapering of the portal vein (PV) at the hilum (black arrow)secondary to encasement by the tumor with occlusion of the left portal vein. There is an internalbiliary stent in situ extending to the atrophic left hepatic lobe.
346 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

determined on histologic review of the resected specimen.In this study, invasive cancers classified as well to moder-ately differentiated, or well differentiated with areas ofmoderate differentiation, were included with the moder-ately differentiated lesions. Trends in treatment-relatedvariables and outcomes over time (before and after 2000)were assessed.
Statistical analysis was performed using SPSS, version16.0 for Windows (Statistical Package for the Social Sci-ences). All quantitative data were expressed as median andrange, unless otherwise indicated. Continuous variableswere compared using Mann-Whitney U test and categori-cal variables with either 2-sided chi-square test or 2-sidedFisher exact test. Survival probabilities were estimatedusing the Kaplan-Meier method24 and compared usingthe log-rank test. Survival (in months) was measured fromthe date initially seen at MSKCC, to the date of death ordate of last contact. Cox regression25 was used to determineindependent predictors of outcomes, using survival as thedependent variable and factors significant (p � 0.05) onunivariate analysis as covariates; perioperative deaths wereincluded in the survival analyses. Values of p � 0.05 wereconsidered significant.
RESULTSDemographics, results of initial evaluationFrom March 1, 1991, to December 31, 2008, 380 patientswith HCCA were evaluated and treated at MSKCC, thefirst 225 of whom have been reported previously.5,6 Thisstudy represents a substantial increase of 155 patients or68% from the last publication. There were 223 men(58.7%) and 157 women (41.3%), with a mean age of
65.0 � 12.0 years (median 67.5 years, range 23 to 87years).
Eighty-five patients (22.3%) had unresectable disease orwere unfit for surgery at initial presentation (Fig. 3).Thirty-eight patients had locally advanced lesions with ex-tensive biliary involvement (n � 14), unreconstructablevascular involvement (n � 20), or both (n � 4). Thirty-eight patients had metastatic disease, with 9 also havingunresectable, locally advanced tumors. Thirty-two of the38 patients had distant metastases: liver only (n � 16),liver � N2-lymph nodes (n � 1), liver � peritoneum (n �1), liver � lung (n � 2), liver � lung � diaphragm (n �1), lung only (n � 1), peritoneum only (n � 7), perito-neum � N2-lymph nodes (n � 2), isolated bone metasta-ses (n � 1), or isolated N2-lymph nodes (n � 6). Twelvepatients were unfit for surgery, principally due to comorbidconditions that prevented a major operation; 4 of thesepatients died of septic complications during evaluation and2 patients had locally advanced disease. Of the remaining 4patients, 2 transferred their care to another institution and2 obtained a consultation only. Two patients declined toundergo operation.
Operative procedures and findingsTwo hundred ninety-five patients (77.6%) were exploredfor a potentially curative resection, 157 (53.2%) of whomunderwent a complete gross resection. One hundredthirty-eight patients (46.8%) had unresectable disease atexploration. Eighty patients had metastatic disease: liveronly (n � 13), liver � N2-lymph nodes (n � 2), liver �peritoneum (n � 5), peritoneum only (n � 18), lung �peritoneum (n � 1), and 41 had proven disease in N2-
Figure 3. Flow diagram showing the results of the initial investigation and surgical findings of allpatients in the series. *Eight patients were judged unfit for extended hepatic resection, 2because of unexpected cirrhosis, and 5 because of significant underlying coronary arterydisease. **Resection of supraduodenal bile duct, cholecystectomy, subhilar lymphadenectomy.
347Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes

lymph nodes. Fifty-nine patients had locally advanced tu-mors, 27 with extensive biliary involvement by tumor, 28with nonreconstructable vascular invasion, and 4 withboth. In 3 of these patients, the combination of local tumorextent with adhesions from either previous surgery, radia-tion therapy, or both, precluded resection. Eight patientswere judged unfit for extended hepatic resection: 1 becauseof chronic renal failure, 2 because of unexpected cirrhosis,and 5 because of significant underlying coronary arterydisease (Fig. 3).
One hundred fifty-seven patients (41.3% of the entirecohort, or 53.2% of those considered to have resectabledisease before surgery) underwent a potentially curativeresection. Resectional procedures consisted of excision ofthe extrahepatic biliary tree and subhilar lymphadenec-tomy in all patients, and this was combined with an en blocpartial hepatectomy in 129 patients (82.2%). The hepaticresections performed were as follows: right extended hepa-tectomy (n � 56), right hepatectomy (n � 16), left ex-tended hepatectomy (n � 8), left hepatectomy (n � 45),central hepatectomy (n � 4); en bloc caudate resection wasperformed in 56 (43.4%), 16 underwent a formal vascularresection and reconstruction, and 2 underwent a concom-
itant pancreaticoduodenectomy. Since 2000, the percent-age of patients undergoing concomitant hepatectomy in-creased significantly (74% vs 90%, p � 0.009) as well asthose submitted to caudate resection (26% vs 45%, p �0.002) compared with the period from 1991through 1999.
HistopathologyThe final histology findings of resected tumors were ade-nocarcinoma in 155 and adenosquamous carcinoma in 2.An R0 resection was achieved in 120 patients (76.4%),with the significant majority occurring in patients submit-ted to a concomitant hepatic resection compared with abile duct resection alone (83.7% vs 42.9%, p � 0.001)(Table 1). The average tumor size was 3.0 � 2.2 cm; 24.8%were well differentiated and 24.2% were papillary tumors.There was a 26.1% overall incidence of metastatic diseaseto hepatoduodenal lymph nodes resected with the primarytumor. Tumors in the hepatic resection group were largerthan those removed without hepatic resection (3.2 � 2.4cm vs 2.1 � 1.0 cm; p � 0.007) and were less often welldifferentiated (22.5% vs 35.7%; p � 0.2), but the latterdifference was not statistically significant (Table 1).
Table 1. Histopathologic Features of Resected Tumor, Perioperative Results, and Survival
VariableAll resections
(n � 157)Hepatic resection
(n � 129)No hepatic resection
(n � 28) p Value
HistopathologyNegative margin, n (%) 120 (76.4) 108 (83.7) 12 (42.9) � 0.001Tumor size, cm 3.0 � 2.2 3.2 � 2.4 2.1 � 1.0 0.007Tumor � 2.5 cm, n (%) 65 (41.4) 58 (45.0) 7 (25.0) 0.117Well differentiated, n (%) 39 (24.8) 29 (22.5) 10 (35.7) 0.149Node positive, n (%) 41 (26.1) 33 (25.6) 8 (28.6) 0.813Papillary tumor, n (%) 38 (24.2) 31 (24.0) 7 (25.0) 1
Perioperative resultsEstimated blood loss, mL
Mean � SD 994 � 1,136 1,105 � 1,218 481 � 306 �0.001Median (range) 770 (30–7,500) 800 (130 – 7,500) 400 (30 – 1,200) 0.002
Number (%) transfused 69 (43.9) 64 (49.6) 5 (17.9)Total units transfused
Mean � SD 3.2 � 8.4 3.6 � 9.0 1.6 � 5.0 0.109Median (range) 0 (0–71) 1 (0–71) 0 (0–25) 0.002
Length of hospital stay, dMean � SD 15 � 9 16 � 9 12 � 7Median (range) 13 (4– 49) 14 (4–49) 10 (4–37) 0.004
Complications, n (%) 93 (59.2) 81 (62.8) 12 (42.9) 0.052Surgical related deaths, n (%) 12 (7.6) 11 (8.5) 1 (3.6) 0.695Survival
Median, mo 39 42.9 28.8 �0.0015-year, actuarial, % 31.6 37.5 85-year, actual, % 26.7 (32/120 at risk) 31.6 (30/95 at risk) 8.0 (2/25 at risk)
Survival calculations include the perioperative deaths.
348 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

Perioperative results and complicationsThe median blood loss for all resections was 770 mL (range30 to 7,500 mL). Sixty-nine patients (43.9%) requiredtransfusion of blood products during or after surgery, andthe median number of transfused units was 0 (range 0 to 71units). There was a trend toward decreased estimated bloodloss between the early and late time periods, from 1,300mL to 1,000 mL, but this was not statistically significant.However, the transfusion rate was significantly lower in thelatter time period, (p � 0.001). Operative estimated bloodloss was greater in the hepatic resection group (hepaticresection 800 mL, range 130 to 7,500 mL; nonhepaticresection 400 mL, range 30 to 1,200 mL, p � 0.001). Inaddition, the proportion of patients who required transfu-sion of blood products was greater in the hepatic resectiongroup compared with the nonhepatic resection group (n �64, 49.6% vs n � 5, 17.9%; p � 0.002) (Table 1). Themedian hospital stay was 13 days (range 4 to 49 days)overall and was significantly longer in the hepatic resectiongroup than in the nonhepatic resection group (14 days[range 4 to 49 days] vs 10 days [range 4 to 37 days], p �0.004). The length of stay was not different between theearly and late time periods.
A total of 130 complications were observed in 93 pa-tients (59.2%). Seventy-two infective complications wereobserved in 66 patients, accounting for 55% of the totalnumber of complications and consisting primarily of intra-abdominal abscess (n � 47) and wound infection (n � 15).Meanwhile, 42 patients presented with a total of 58 non-infective complications, accounting for the remaining 45%and consisting primarily of bile leak (n � 18) and hepaticfailure (n � 6). Morbidity rates were not statistically dif-ferent over time.
The overall perioperative mortality was 7.6% (n � 12)at a median time of 0.8 months (range 0.4 to 2.2 months)from the time of surgery. Perioperative mortality in theearly period (1991 to 1999) was 9.1% (7 of 77), but itdeclined during the most recent period (2000 to 2008) to6.2% (5 of 81). Among the causes of death, 8 patients(66.7%) died of infective complications including intra-abdominal abscess (n � 5), infected ascites/pneumonia(n � 1), pneumonia or gastrointestinal hemorrhage (n �1), and bile leak or hepatic failure (n � 1). The 4 remainingpatients died of hepatic failure (n � 2), gastrointestinalhemorrhage (n � 1), and acute myocardial infarction (n �1). Of the 8 patients who died of infective complications, 7patients (87.5%) had positive intraoperative bile cultures.Among the 4 patients who died of noninfective causes,only 1 patient (25.0%) had a positive intraoperative bileculture (p � 0.067).
SurvivalThe median follow-up period was 15.9 months. The me-dian and 5-year disease-specific survival (DSS) rates for theentire cohort were 19.4 months and 15.4%, respectively.Patients who underwent resection (median follow-up 29.9months) had significantly longer median survival thanthose who did not (39.0 vs 11.6 months; p � 0.001).Furthermore, median DSS after an R0 resection was sig-nificantly longer than after an R1 resection (43.5 vs 23.1months: p � 0.001) (Fig. 4). Likewise, median disease-freesurvival in patients with an R0 resection was significantlylonger than in patients with an R1 resection (33.4 vs 14.0months; p � 0.001). However, even if the resection marginwas positive, the median DSS in resection patients wasgreater than that in patients who did not undergo resection(23.1 vs 11.6 months; p � 0.001). There was no differencein disease-free survival and DSS between time periods. Me-dian survival was greater in the hepatic resection groupthan in the nonhepatic resection group (42.9 vs 28.8months; p � 0.001). The actuarial 5-year survival rate was37.5% in patients who underwent hepatic resection vs8.0% in those who underwent bile duct excision alone(Table 1).
At the time of this analysis, 40 of the 157 patients(25.5%) in the resection group were alive at a medianfollow-up of 42 months; 30 patients remained with noevidence of disease and 10 were alive with disease recur-rence. Ninety-five patients had died of disease at a medianof 29.9 months. Twenty-one patients died of other causes:
Figure 4. Survival after resection stratified by margin status. Resec-tion with a negative histologic margin is indicated by the solid line (n �120; median survival 43.5 months), and resection with a positivemargin is indicated by the dashed line (n � 37; median survival 23.1months). No-resection group is indicated by the dotted line (n � 223;median survival 11.6 months); p � 0.001 by log-rank test.
349Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes

12 from perioperative complications and 9 after surgery foran unrelated illness. Of the 32 actual 5-year survivors, 12were alive without disease (median follow-up 108.1months) and 15 had died of disease recurrence and progres-sion (median follow-up 75.9 months).
Blumgart preoperative clinical T-staging systemThree hundred seventy-six patients were staged accordingto the preoperative clinical T staging system previously de-scribed;5,6 4 patients had incomplete data. One hundredforty-three patients had tumor involvement of the biliaryconfluence (with or without unilateral extension to second-order biliary radicles), no portal vein involvement, and nolobar atrophy and were therefore classified as having T1tumors. One hundred fifty-five patients had T2 lesions:ipsilateral portal vein involvement (n � 31), ipsilateral lo-bar atrophy (n � 25), or both findings (n � 99). Seventy-eight patients had T3 tumors: 8 because of biliary extentalone, 47 because of main portal vein involvement, 7 be-cause of bilateral portal vein involvement, and 16 becauseof a combination of vascular involvement, biliary extent,and/or lobar atrophy. A similar proportion of patients withT1 (85.3%) and T2 (85.8%) tumors underwent explora-tion with curative intent. Forty patients with T3 tumors(51.3%) were also considered to have potentially resectabledisease; half of these patients (n � 22) had main portal veininvolvement that was possibly amenable to resection withportal vein reconstruction (Table 2).
As T stage increased, both resectability and the likeli-hood of achieving an R0 resection decreased progressively.On logistic regression analysis, increasing T stage signifi-cantly reduced the resectability rate (p � 0.001, odds ratio0.22 [95% CI 0.15 to 0.32]) and the likelihood of an R0resection (p � 0.007, odds ratio 0.31 [95% CI 0.13 to0.72]). Among the 92 patients with T1 tumors who under-went resection, 65 (70.7%) had a concomitant partial hep-atectomy and 2 (2.2%) required portal vein resection be-cause of tumor invasion. This is in contrast to patients withT2 lesions, all but 1 of whom underwent hepatic resection;14 (21.9%) required a portal vein resection and reconstruc-tion. In addition, metastatic disease to N2-level lymphnodes or to distant sites (ie, metastatic disease that contra-indicated resection) correlated with increasing T stage (T1to T3) (p � 0.001, odds ratio 0.5 [95% CI 0.37 to 0.68]).
Median survival (including perioperative deaths) was22.8 months for patients with T1 tumors, 23.0 months forpatients with T2 tumors, and 10.8 months for patientswith T3 lesions (Table 2). Using Cox regression with Tstage as a categorical covariate and T1 as the reference stage,median survival was reduced significantly in moving fromstage T1 to T3 (p � 0.001, odds ratio 0.45 [95% CI 0.33to 0.61]) and from stage T2 to T3 (p � 0.001, odds ratio
0.42 [95% CI 0.30 to 0.57]), as would be expected basedon resectability. However, there was no difference in mov-ing from stage T1 to T2 (p � 0.6, odds ratio 1.09 [95% CI0.84 to 1.41]). This observation likely reflects the signifi-cant contribution of en bloc partial hepatectomy, whichwas more commonly performed for resectable T2 tumors.
Three hundred seventy-three patients were staged ac-cording to the AJCC system. Stage was determined fromanalysis of the resected specimen in 157 patients and fromthe imaging studies or operative findings for the remaining216 patients. Seven patients could not be adequately stagedwith the available information. On logistic regression,AJCC tumor stage, unlike the proposed T staging system,neither correlated with resectability (p � 0.9), nor pre-dicted the likelihood of an R0 resection (p � 0.2). Like-wise, using Cox regression, AJCC tumor stage did not cor-relate with survival (p � 0.23), likelihood ratio test foroverall significance with 5 df.
Prognostic factors associated withimproved survivalUnivariate and multivariate analyses of the clinical andtumor-related factors associated with improved survival arelisted in Table 3. This analysis excluded 12 patients whohad surgery-related deaths in the perioperative period and1 patient who died 6 months after surgery of an unrelatedillness. Because of the importance of resection margin sta-
Table 2. Resectability, Incidence of Metastatic Disease,and Survival Stratified by T Stage
VariableT stage
T1 T2 T3 Total
n 143 155 78 376Explored with
curative intent,n (%) 122 (85.3) 133 (85.8) 40 (51.3) 295 (78.5)
Resected, n (%)* 92 (64.3) 64 (41.3) 1 (1.3) 157 (41.8)R0 resection, n
(%)† 63 (44.1) 56 (36.1) 1 (1.3) 120 (31.9)Hepatic resection,
n (%) 65 (45.4) 63 (40.6) 1 (1.3) 129 (34.3)Portal vein
resection, n 2 14 0 16Metastatic disease,
n (%)‡ 28 (19.6) 54 (34.8) 38 (48.7) 120 (31.9)Median survival,
mo 22.8 23.0 10.8 19.4
Four patients had incomplete data and could not be accurately staged. Thepercentages indicate the proportion of patients within each stage grouping orof the total number of patients. Metastatic disease refers to metastases toN2-level lymph nodes or to distant sites.*p � 0.001.†p � 0.007.‡p � 0.001.
350 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

Table 3. Factors Associated with Improved SurvivalVariable Median survival, mo p Value (univariate) p Value (multivariate) Odds ratio (95% CI)
All resections (n � 144)
Resection margin
Positive (n � 36) 24 0 0.007 2.0 (1.2–3.4)
Negative (n � 108) 51
Hepatic resection
Yes (n � 117) 47 0 0.005 2.2 (1.2–3.8)
No (n � 27) 29
Well differentiated*
Yes (n � 37) 66 0 0 2.6 (1.6–4.4)
No (n � 102) 36
Lymph node positive
Yes (n � 38) 23 0 0.006 1.9 (1.2–3.0)
No (n � 106) 51
Papillary tumor
Yes (n � 36) 58 0.01 0.234 �
No (n � 108) 36
Lobar atrophy
Yes (n � 43) 46 0.036 0.929 �
No (n � 101) 39
Portal vein involvement
Yes (n � 45) 52 0.077 � �
No (n � 99) 39
Tumor � 2.5 cm†
Yes (n � 62) 47 0.469 � �
No (n � 71) 37
R0 resections (n � 108)
Hepatic resection
Yes (n � 96) 53 0.005 0 3.9 (1.9–8.0)
No (n � 12) 30
Well differentiated*
Yes (n � 28) 100 0 0 3.8 (1.9–7.4)
No (n � 76) 41
Lymph node positive
Yes (n � 24) 28 0.001 0.01 2.1(1.2–3.8)
No (n � 84) 53
Papillary tumor
Yes (n � 31) 77 0.038 0.253 �
No (n � 77) 39
Lobar atrophy
Yes (n � 35) 54 0.126 � �
No (n � 73) 47
Portal vein involvement
Yes (n � 42) 54 0.593 � �
No (n � 66) 47
Tumor � 2.5 cm†
Yes (n � 49) 47 0.68 � �
No (n � 54) 53
Analysis of factors associated with favorable long-term survival after any resection and after R0 resection (negative margins). This analysis excluded 12 patientswho died of surgery-related causes in the perioperative period and 1 patient who died 6 months after surgery of an unrelated illness. Cox regression analysis wasperformed using only variables that were significant on univariate analysis.*Five patients in the overall resection group and 4 patients in the R0 group had incomplete data.†Eleven patients in the overall resection group and 5 patients in the R0 group had incomplete data.
351Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes

tus in affecting prognosis, a second analysis was performedfor patients who underwent R0 resections to determinewhether additional significant variables might emerge. Inthe multivariate analysis model, concomitant hepatic resec-tion, well-differentiated histopathology, and lymph nodemetastasis were the only significant factors associated withimproved survival.
DISCUSSIONThis study provides convincing evidence that a preopera-tive clinical T staging system, originally proposed by Blum-gart and subsequently modified, effectively predicts resect-ability and likelihood of metastatic disease. In this cohortof 380 patients at a single institution, managed over an18-year period, approximately 60% of all patients had un-resectable disease, either at presentation or exploration. Al-though locally advanced disease was an important factor,the most common reason for irresectability was metastaticdisease. The aggressive nature of this disease underscoresthe importance of a staging system to help with preopera-tive decision making, which will help improve patient se-lection for operative intervention.
To date, a reliable and clinically relevant means of strat-ifying HCCA patients into subgroups based on potentialfor resection has been lacking. The often cited Bismuth-Corlette classification has been used to define the longitu-dinal tumor spread in 1 dimension along the bile duct.16
This system, however, stratifies patients based only on bil-iary involvement of the tumor and does not incorporateradial tumor growth. The AJCC staging system is basedlargely on pathologic criteria, generally after an attempt atresection, and has little applicability in the preoperativestaging setting.14 Using our cohort of patients, the AJCCstaging system failed to predict presence of metastatic dis-ease or survival. Furthermore, neither system is useful forpredicting resectability. More recently, DeOliveira and col-leagues26 have attempted to combine elements from these 2staging systems while adding remnant liver volume andunderlying disease, specific degrees of vascular invasion,and tumor size and type into one all-encompassing classi-fication.26 The purpose of this new proposal is to comparepreoperative with postresectional stage in order to compareoutcomes and guide therapy among groups of patientsfrom different institutions. Unfortunately, as it is currentlydescribed, this system relies on determination of very spe-cific information on vascular involvement and tumor size,which may not be accurately determined based on preop-erative imaging. In addition, it requires extensive patho-logic evaluation of resected liver tissue and tumor speci-men, which may not be available preoperatively forevaluation of resectability. Therefore, we believe it is too
complex to be applied broadly and to date has not beenvalidated in any actual patient cohort.
The authors’ earlier work suggested that the preopera-tive clinical T staging system,6 which takes into account allfactors related to both the radical and longitudinal exten-sion of the tumors based on preoperative imaging studies,might be useful in assessing patients preoperatively. In thisanalysis of 380 patients, the resectability rate was 64.3% inT1 tumors, 41.3% in T2 tumors, and 1.3% (1 patient) inT3 tumors. Resectability, the probability of an R0 resec-tion, and the likelihood of metastatic disease correlatedsignificantly with the clinical T stage. By contrast, this stag-ing scheme was less useful for predicting survival; a signif-icant difference in outcomes was found only between T1and T3 or between T2 and T3 tumors, but not between T1and T2 tumors. The likely explanation for this is that treat-ment differed among the stages. Specifically, complete re-section with negative margins almost never occurred for T3tumors but was much more frequent inT1 (44.1%) andT2(36.3%) tumors. In addition, all but 1 of the patients in theT2 group underwent hepatic resection. It seems entirelyplausible that increased tumor clearance afforded by hepa-tectomy, performed more often in the T2 group, blurredthe distinction between it and T1 lesions. Perhaps moreimportant, the presence of distant metastatic disease in-creased with more locally advanced and higher clinical Tstage tumors, with 48.7% of T3 tumors harboring meta-static disease, followed by 34.8% of T2 and 19.6% of T1lesions. This information, when identified preoperatively,is useful in selecting patients who would potentially benefitfrom more intensive radiologic investigation such as PET27
or staging laparoscopy,28 thereby sparing them a nonthera-peutic laparotomy.6,29Alternatively, as more effective che-motherapeutic agents for cholangiocarcinoma emerge, thissubgroup might be best served with neoadjuvant treat-ment. The yield of laparoscopy was 36% in patients withT2/T3 tumors while only 9% in patients with T1 tumors.Therefore, we have generally reserved staging laparoscopyfor T2 tumors and for the rare T3 tumors that are selectedfor potential resection. Meanwhile, FDG-PET is used pri-marily to identify potential sites of distant disease that areequivocal on cross-sectional imaging. However, it is not agood modality to determine local resectability given thepoor resolution for small tumors near major vascular struc-tures such as those found in the hilus of the liver. In ourexperience it has changed management in 24% of patientswith cholangiocarcinoma with a higher sensitivity in thosewith intrahepatic tumors.
Significant prognostic factors associated with survivalafter R0 resection were concomitant partial hepatectomy,well-differentiated histopathology, and lymph node metas-
352 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

tasis on multivariate analysis. Papillary phenotype, whichhas been previously reported as an important prognosticfactor in patients with HCCA21 and acknowledged in the7th edition of the AJCC staging manual, was associatedwith survival on univariate analysis but lost significance inthe multivariate model in this cohort. This is likely due tothe competing effect of tumor grade, as all papillary tumorsare well differentiated. Lymph node involvement has beenrecognized as a common and important prognostic factorinfluencing survival after resection for HCCA8,30,31 and itsrelevance was confirmed in this study. Another significantfinding of this study is that patients undergoing R1 resec-tion had longer survival than patients with unresectabledisease at the time of exploration. This may be due to thefact that more patients with R1 resection received adjuvantchemotherapy and/or radiotherapy (41%) than in the past.In addition, although all patients with R1 resection under-went biliary enteric bypass, this procedure was performedin only 45 patients (20%) with unresectable disease. There-fore, it is possible that the more durable relief of biliaryobstruction may have affected outcomes. Although the sur-vival benefit of R1 resection compared with no resection isyet unresolved, we still advocate for a margin-negativeresection.7,8,32-34
As was noted in our last report, most patients in thisseries had disease that was not amenable to resection. Ap-proximately half of the patients who underwent explora-tion with curative intent (41% of the entire group) under-went a resection of all gross tumor; 40.7% of those explored(31.9% of the entire group) underwent an R0 resection.Nearly 80% of resections were performed with negativemargins, which correlated strongly with concomitant he-patic resection, including en bloc caudate lobectomy whenappropriate. Numerous retrospective and prospective serieshave demonstrated a long-term survival benefit of concom-itant hepatic resection to achieve a complete resection forpatients with HCCA.32-36 Our data demonstrate thatnearly 90% of resections since 2000 included a concomi-tant partial hepatectomy and appeared to be associatedwith an improvement in perioperative mortality from9.1% to 6.2%.6 Despite an increase in blood loss and trans-fusion rate, survival was significantly extended using thisapproach. This observation suggests that an aggressive re-sectional approach is safe and feasible with acceptableresults.29
The overall morbidity rate after resection for HCCA hasremained relatively high compared with resection of othertumor types, ranging from 14% to 66% from high volumecenters.3,6-12,29,30,32,34,36-40 In this study, the overall morbid-ity rate was 59%; however, it must be emphasized that alladverse postoperative events were recorded prospectively,
regardless of type or severity. Infective complications dom-inated the postoperative course for many patients and wereresponsible for approximately half of all complications seenand 8 of 12 surgery-related deaths. Hepatic failure as theprimary cause of death, in the absence of other contribut-ing factors, is difficult to ascertain with certainty, but ap-peared to be relatively uncommon. Infectious complica-tions related to initial biliary drainage remain a significantchallenge.5,6 It seems clear that a balance must be struckregarding preoperative maneuvers aimed at reducing peri-operative morbidity, such as biliary drainage and portalvein embolization, and morbidity related to these proce-dures. We have previously shown that in patients with anadequate liver remnant volume, routine biliary drainagebefore operation probably improves outcomes minimallyand may be harmful;41 on the other hand, a subgroup ofpatients with small, jaundiced future liver remnants aremost likely to benefit,19,42-44 and attempts to reduce com-plication rates in patients with HCCA should be pursued.However, to our knowledge there is no level of bilirubinthat mandates preoperative biliary drainage. This decisionshould be made in the individual context of each patient.
Recently, multidetector-row CT has been applied to thepreoperative diagnosis of perihilar cholangiocarcinoma as anoninvasive modality for providing high-quality imagesthat can evaluate biliary involvement as well as portal veininvasion.45,46 Multidetector-row CT may be a useful ad-junctive tool to stratify patients by preoperative T stagingsystem and help predict resectability without the need forcatheter-based biliary interventions.
CONCLUSIONSIn summary, this study shows that the preoperative clinicalT staging system of Blumgart predicts resectability andlikelihood of metastatic disease. This system accounts forfactors related to local tumor extent within the porta hepa-tis and stratifies patients using noninvasive preoperativeimaging. The progressive use of en bloc partial hepatec-tomy has been a significant advancement in the operativestrategy for HCCA. Although operative mortality has de-clined, morbidity rates remain high, affecting approxi-mately half of all patients undergoing resection, and high-lighting the need for continued improvements inperioperative management.
Author ContributionsStudy conception and design: Matsuo, Rocha, D’Angelica,
Allen, DeMatteo, Gonen, Endo, JarnaginAcquisition of data: Matsuo, Rocha, Ito, Endo, JarnaginAnalysis and interpretation of data: Matsuo, Rocha,
353Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes

D’Angelica, Allen, Fong, DeMatteo, Gonene, Endo,Jarnagin
Drafting of manuscript: Matsuo, Rocha, Ito, D’Angelica,Allen, Fong, DeMatteo, Gonen, Endo, Jarnagin
Critical analysis: Matsuo, Rocha, Ito, D’Angelica, Allen,Fong, DeMatteo, Gonen, Endo, Jarnagin
REFERENCES
1. Parker SL, Tong T, Bolden S, Wingo PA. Cancer statistics, 1996.CA Cancer J Clin 1996;46:5–27.
2. Launois B, Reding R, Lebeau G, et al. Surgery for hilar cholan-giocarcinoma: French experience in a collective survey of 552extrahepatic bile duct cancers. J Hepatobiliary Pancreat Surg2000;7:128–134.
3. Nakeeb A, Pitt HA, Sohn TA, et al. Cholangiocarcinoma. Aspectrum of intrahepatic, perihilar, and distal tumors. Ann Surg1996;224:463–473; discussion 473.
4. Endo I, Gonen M, Yopp AC, et al. Intrahepatic cholangiocarci-noma: rising frequency, improved survival, and determinants ofoutcome after resection. Ann Surg 2008;248:84–96.
5. Burke EC, Jarnagin WR, Hochwald SN, et al. Hilar cholangio-carcinoma: patterns of spread, the importance of hepatic resec-tion for curative operation, and a presurgical clinical stagingsystem. Ann Surg 1998;228:385–394.
6. Jarnagin WR, Fong Y, DeMatteo RP, et al. Staging, resectability,and outcome in 225 patients with hilar cholangiocarcinoma.Ann Surg 2001;234:507–517; discussion 517.
7. Ito F, Agni R, Rettammel R, et al. Resection of hilar cholangio-carcinoma: concomitant liver resection decreases hepatic recur-rence. Ann Surg 2008;248:273–279.
8. Klempnauer J, Ridder GJ, von Wasielewski R, et al. Resectionalsurgery of hilar cholangiocarcinoma: a multivariate analysis ofprognostic factors. J Clin Oncol 1997;15:947–954.
9. Neuhaus P, Jonas S, Bechstein WO, et al. Extended resectionsfor hilar cholangiocarcinoma. Ann Surg 1999;230:808–818;discussion 819.
10. Nimura Y, Kamiya J, Kondo S, et al. Aggressive preoperativemanagement and extended surgery for hilar cholangiocarcino-ma: Nagoya experience. J Hepatobiliary Pancreat Surg 2000;7:155–162.
11. Kawasaki S, Imamura H, Kobayashi A, et al. Results of surgicalresection for patients with hilar bile duct cancer: application ofextended hepatectomy after biliary drainage and hemihepaticportal vein embolization. Ann Surg 2003;238:84–92.
12. Dinant S, Gerhards MF, Rauws EA, et al. Improved outcome ofresection of hilar cholangiocarcinoma (Klatskin tumor). AnnSurg Oncol 2006;13:872–880.
13. Lee SG, Lee YJ, Park KM, et al. One hundred and eleven liverresections for hilar bile duct cancer. J Hepatobiliary PancreatSurg 2000;7:135–141.
14. Greene FL, Page PD, Fleming ID, et al. AJCC cancer stagingmanual. 6th edition. New York: Springer-Verlag; 2002.
15. Bismuth H, Corlette MB. Intrahepatic cholangioenteric anasto-mosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet1975;140:170–178.
16. Bismuth H, Nakache R, Diamond T. Management strategiesin resection for hilar cholangiocarcinoma. Ann Surg 1992;215:31–38.
17. Kluge R, Schmidt F, Caca K, et al. Positron emission tomogra-phy with [(18)F]fluoro-2-deoxy-D-glucose for diagnosis andstaging of bile duct cancer. Hepatology 2001;33:1029–1035.
18. Povoski SP, Karpeh MS Jr, Conlon KC, et al. Preoperative bili-ary drainage: impact on intraoperative bile cultures and infec-tious morbidity and mortality after pancreaticoduodenectomy. JGastrointest Surg 1999;3:496–505.
19. Hochwald SN, Burke EC, Jarnagin WR, et al. Association ofpreoperative biliary stenting with increased postoperative infec-tious complications in proximal cholangiocarcinoma. Arch Surg1999;134:261–266.
20. Czerniak A, Soreide O, Gibson RN, et al. Liver atrophy com-plicating benign bile duct strictures. Surgical and interventionalradiologic approaches. Am J Surg 1986;152:294–300.
21. Jarnagin WR, Bowne W, Klimstra DS, et al. Papillary phenotypeconfers improved survival after resection of hilar cholangiocar-cinoma. Ann Surg 2005;241:703–712; discussion 712–714.
22. Endo I, House M, Klimstra D, et al. Clinical significance ofintraoperative bile duct margin assessment for hilar cholangio-carcinoma. Ann Surg Oncol 2008;15:2104–2112.
23. Martin RC 2nd, Jaques DP, Brennan MF, et al. Achieving ROresection for locally advanced gastric cancer: is it worth the riskof multiorgan resection? J Am Coll Surg 2002;194:568–577.
24. Kaplan EL, Meier P. Nonparameteric estimation from imcom-plete observations. J Am Statist Assoc 1958:53:457–481.
25. Cox DR. Regression models and life tables. J R Stat Soc 1972:187–220.
26. DeOliveira ML, Schulick RD, Nimura Y, et al. New stagingsystem and a registry for perihilar cholangiocarcinoma. Hepa-tology 2011;53:1363–1371.
27. Corvera CU, Blumgart LH, Akhurst T, et al. 18F-fluorodeoxyglucose positron emission tomography influ-ences management decisions in patients with biliary cancer.J Am Coll Surg 2008;206:57–65.
28. D’Angelica M, Fong Y, Weber S, et al. The role of staging lapa-roscopy in hepatobiliary malignancy: prospective analysis of 401cases. Ann Surg Oncol 2003;10:183–189.
29. Rocha FG, Matsuo K, Blumgart LH, et al. Hilar cholangiocar-cinoma: the Memorial Sloan-Kettering Cancer Center experi-ence. J Hepatobiliary Pancreat Sci 2010;17:490–496.
30. Kosuge T, Yamamoto J, Shimada K, et al. Improved surgicalresults for hilar cholangiocarcinoma with procedures includingmajor hepatic resection. Ann Surg 1999;230:663–671.
31. Kitagawa Y, Nagino M, Kamiya J, et al. Lymph node metastasisfrom hilar cholangiocarcinoma: audit of 110 patients who un-derwent regional and paraaortic node dissection. Ann Surg2001;233:385–392.
32. Seyama Y, Kubota K, Sano K, et al. Long-term outcome ofextended hemihepatectomy for hilar bile duct cancer with nomortality and high survival rate. Ann Surg 2003;238:73–83.
33. Baton O, Azoulay D, Adam DV, et al. Major hepatectomy forhilar cholangiocarcinoma type 3 and 4: prognostic factors andlongterm outcomes. J Am Coll Surg 2007; 204:250–260.
34. Hemming AW, Reed AI, Fujita S, et al. Surgical management ofhilar cholangiocarcinoma. Ann Surg 2005;241:693–699; dis-cussion 699–702.
35. Nagino M, Kamiya J, Arai T, et al. “Anatomic” right hepatictrisectionectomy (extended right hepatectomy) with caudatelobectomy for hilar cholangiocarcinoma. Ann Surg 2006;243:28–32.
354 Matsuo et al Cholangiocarcinoma: Staging, Outcomes J Am Coll Surg

36. Kondo S, Hirano S, Ambo Y, et al. Forty consecutive resectionsof hilar cholangiocarcinoma with no postoperative mortalityand no positive ductal margins: results of a prospective study.Ann Surg 2004;240:95–101.
37. Jarnagin WR, Shoup M. Surgical management of cholangiocar-cinoma. Semin Liver Dis 2004;24:189–199.
38. Nguyen KT, Steel J, Vanounou T, et al. Initial presentationand management of hilar and peripheral cholangiocarcinoma:is a node-positive status or potential margin-positive result a con-traindication to resection? Ann Surg Oncol 2009;16:3308–3315.
39. Nagino M, Kamiya J, Arai T, et al. One hundred consecutivehepatobiliary resections for biliary hilar malignancy: preopera-tive blood donation, blood loss, transfusion, and outcome. Sur-gery 2005;137:148–155.
40. Sano T, Shimada K, Sakamoto Y, et al. One hundred twoconsecutive hepatobiliary resections for perihilar cholangio-carcinoma with zero mortality. Ann Surg 2006;244:240–247.
41. Kennedy T, Yopp A, Qin Y, et al. Role of preoperative biliarydrainage of liver remnant prior to extended liver resection forhilar cholangiocarcinoma. HPB 2009;11:445–451.
42. Nagino M, Takada T, Miyazaki M, et al. Preoperative biliarydrainage for biliary tract and ampullary carcinomas. J Hepato-biliary Pancreat Surg 2008;15:25–30.
43. Laurent A, Tayar C, Cherqui D. Cholangiocarcinoma: preoper-ative biliary drainage (Con). HPB (Oxford) 2008;10:126–129.
44. Cherqui D, Benoist S, Malassagne B, et al. Major liver resectionfor carcinoma in jaundiced patients without preoperative biliarydrainage. Arch Surg 2000;135:302–308.
45. Sugiura T, Nishio H, Nagino M, et al. Value of multidetector-rowcomputed tomography in diagnosis of portal vein invasion by peri-hilar cholangiocarcinoma. World J Surg 2008;32:1478–1484.
46. Senda Y, Nishio H, Oda K, et al. Value of multidetector row CTin the assessment of longitudinal extension of cholangiocarci-noma: correlation between MDCT and microscopic findings.World J Surg 2009;33:1459–1467.
355Vol. 215, No. 3, September 2012 Matsuo et al Cholangiocarcinoma: Staging, Outcomes