
Surgical Site Infection (SSI) Surveillance...
21
Where we started and where we’re going… Anjum Khan MBBS MSc CIC Infection Control Professional Department of Risk Management and Quality Improvement Infection Prevention & Control Service Surgical Site Infection (SSI) Surgical Site Infection (SSI) Surveillance Update Surveillance Update (with special reference to Colorectal Surgeries) (with special reference to Colorectal Surgeries)
Transcript of Surgical Site Infection (SSI) Surveillance...
Where we started and where we’re going…
Anjum Khan MBBS MSc CICInfection Control Professional
Department of Risk Management and Quality Improvement
Infection Prevention & Control Service
Surgical Site Infection (SSI)Surgical Site Infection (SSI)Surveillance UpdateSurveillance Update
(with special reference to Colorectal Surgeries)(with special reference to Colorectal Surgeries)

OutlineIntroduction
Our SSI Surveillance Framework
NNIS/NHSN definitions and Risk Stratification Methods
Data on Process Indicators
Challenges
IntroductionSurgical Site Infections (SSI) are the second most common type of adverse event in hospitalized patients
SSI increase mortality, readmission rate, length of stay and cost of care
SSIs are preventable
Surveillance first step towards any prevention strategy

Objectives of SSI SurveillanceTo measure baseline rates and performances
To monitor process indicators as the appropriateness of antimicrobial prophylaxis ordered and given to the patient
Systematic reporting and regular feedback to all stakeholders such as individual Surgeons, Medical and Program Directors and the Chief of Surgery to engage their attention for Patient Safety and Continuous Quality Improvement (CQI) programmes
To drive the conduct of interventions that reduce the surgical site infection rates and morbidity and mortality associated with it
Accreditation Requirement

Surveillance ByInfection Control Professional
Department of Risk ManagementSSI Surveillance Framework
MDT RoundsM &M Rounds
ER Admission list
Review ofMicrobiology culture
reports
Post Discharge SSI Form Surgeon Self Reporting
Denominator data- OR data base
Review by IC service
Report to Division Head, Program DirectorPeri operative Directors
Surgeon in Chief & individual surgeons
Service reportsICC, SMC, MAC
Board-Balanced Score Card
Recommendations for altering
any processes
ASS
ESS
ME
NT
AN
AL
YSI
SA
CT
ION
Calculation of crude and Risk Stratified rates
Surveillance ByInfection Control Professional
Department of Risk ManagementSSI Surveillance Framework
MDT RoundsM &M Rounds
ER Admission list
Review ofMicrobiology culture
reports
Post Discharge SSI Form Surgeon Self Reporting
Denominator data- OR data base
Review by IC service
Report to Division Head, Program DirectorPeri operative Directors
Surgeon in Chief & individual surgeons
Service reportsICC, SMC, MAC
Board-Balanced Score Card
Recommendations for altering
any processes
ASS
ESS
ME
NT
AN
AL
YSI
SA
CT
ION
Calculation of crude and Risk Stratified rates

SSI Surveillance for Selected Procedures
Cardiovascular (1998/1999)Ophthalmology (2001)Neurosurgery (Jan- 2006)General surgery (March- 2006)Obstetrics (June- 2006)Orthopedics (Jan- 2005)Vascular (TBD, initiated the discussions)

Selected Procedures in General Surgery
Colorectal Surgeries – March 2006
Quality/Outcome Indicators-Rate of SSI among wound class I and II
Process Indicators-% of surgical patients receiving appropriate abx within 1 hour of cut time- % of surgical patients with normothermia
in PACU (36-380C)
SSI Surveillance MethodsInpatient SSI Surveillance
MDT RoundsM&M RoundsMicrobiology ReportsDaily Admission list
Post Discharge SSI SurveillancePost discharge Surveillance form


SSI Risk StratificationPredictors of SSI Risk
Host susceptibility-ASA score
Degree of microbial contamination of surgical site
Duration of operation

SSI Risk Stratification-cont’dNNIS Risk Index
ASA > 2 =1
Contaminated or dirty/infected wounds=1
Length of operation >T hours (T=75%ile)=1
NNIS Risk Index can range from 0-3

SSI Risk Stratification- cont’d
Laparoscopic Procedures
1 is subtracted from the calculated NNIS Risk Index e.g. when 2 risk factors are present and the procedure is done laparoscopically the new modified risk index category is 1 (i.e., 2-1=1)
When no risk factors are present and the procedure is performed with a laparoscope the risk category is 0-1=-1. “ -1=M ”

SSI can be classified as: (CDC)
1. Superficial incisional-skin and subcutaneous tissue involvement
2. Deep incisional-Muscle and fascial layer
3 Organ/Space – Organs/structures beneath the area of incision
58%
7.2%
34.5%

Calculating SSI RatesNumerator Definition
Number of clean surgery patients (wound class I & II) having a post operative wound infection
Denominator DefinitionNumber of clean surgery patients (wound class I & II)
Exclusion CriteriaPatients < 18 years of ageSurgeries classified as wound class III & IV
SSI Rate = Numerator x 100Denominator
Percent of Surgical Patients w ith Antibiotic Administration Within 60 minutes Prior to Surgical Incision for Colon Surgery
020406080
100120
Apr-06 M ay-06 Jun-06 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 M ar-07 Apr-07 M ay-07 Jun-07
Months
Perc
enat
ge
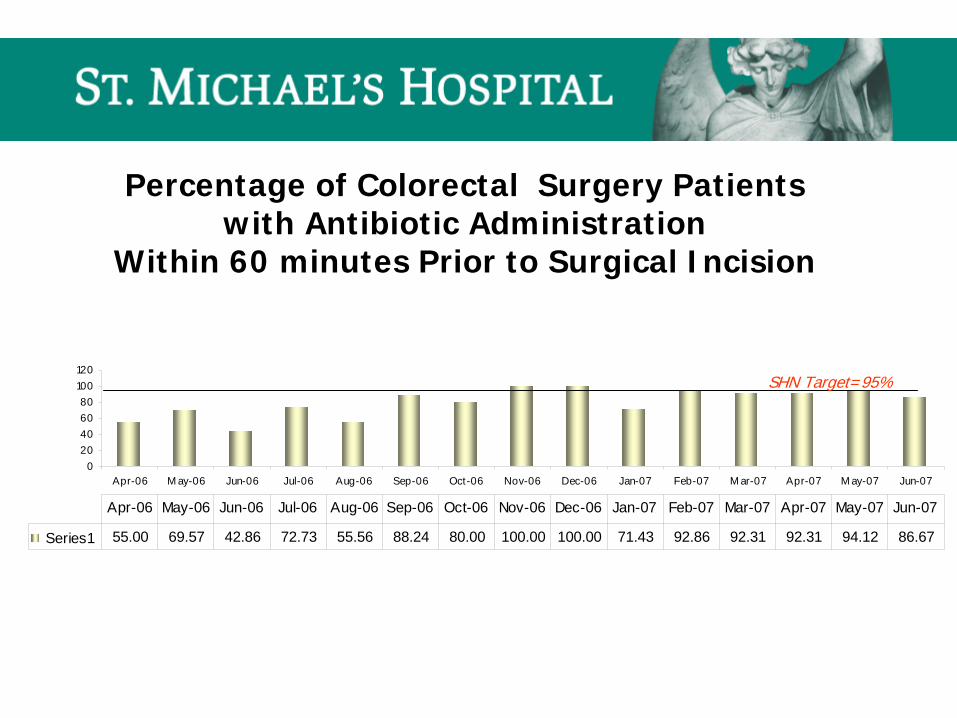
Series1 55.00 69.57 42.86 72.73 55.56 88.24 80.00 100.00 100.00 71.43 92.86 92.31 92.31 94.12 86.67
Apr-06 May-06 Jun-06 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07
Percentage of Colorectal Surgery Patients with Antibiotic Administration
Within 60 minutes Prior to Surgical Incision
SHN Target=95%

Percent Colon Surgery Patients with Normothermia in PACU
0
20
40
60
80
100
Apr-06 May-06 Jun-06 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07
Months
Perc
enta
ge
Series1 15.00 56.52 47.62 18.18 44.44 47.06 60.00 50.00 25.00 78.57 50.00 23.08 30.77 35.29 46.67
Apr-06 May- Jun-06 Jul-06 Aug- Sep- Oct- Nov- Dec- Jan-07 Feb- Mar- Apr-07 May- Jun-07
Percentage of Colorectal Surgery Patients with Normothermia in PACU (36-38)
THE LANCET Vol 358: Sept 15, 2001THE NEW ENGLAND JOURNAL OF MEDICINE Vol 334, No 19, 1996
SHN Target=95%

Percentage Return Rateof Post Discharge Surveillance Forms
0
10
20
30
40
50
60
Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07 Jul-07 Aug-07
Months
Perc
enta
ge
27.27 11.11 52.94 20.00 27.78 33.33 21.43 25.00 31.25 7.69 17.65 26.67 6.67 11.76
Jul-06 Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- May- Jun- Jul-07 Aug-
53% Returns from our own Surgeons19% of returned forms reported an infection
Between 12% and 84% of SSI are detected after patients are discharged from the hospitalInfection Control and hospital Epidemiology Apr 1999; 20,4250-269

ChallengesWound ClassificationAssign the surgical wound classification upon completion of an operation. A surgical team member should make the assignment. CDC Recommendation Category II
Manual Data Abstraction
Return Rate of Post Discharge SSI forms When post discharge surveillance is performed for detecting SSI following certain
operations, use a method that accomodates available resources and data needsCDC Recommendation Category II
Challenges-cont’dBreakdowns in delivery of Post Discharge Surveillance Form
Placement in the chartCorrect placement in the chartDelivery and proper instructions by RNPatient bringing the form to Surgeon/GPSurgeon/GP sending the form back to us
– Don’t seem to have any control over last 2 factors

Preventing Surgical Site InfectionFour Components of Care
Appropriate Hair Removal
Appropriate Use of Prophylactic antibiotics
Maintenance of Post Operative Glucose Control
Peri Operative Normothermia (Colorectal Surgeries)
PLAN
DO
STUDY
ACT

Questions ?


















