Prevention of Surgical Site Infections (SSI) MSIPC Fundamentals of Infection Prevention & Control...
47
Prevention of Surgical Site Infections (SSI) MSIPC Fundamentals of Infection Prevention & Control October 2014 Karen Hoover, RN Infection Prevention Coordinator St. Mary’s of Michigan, Saginaw
-
Upload
vivien-simmons -
Category
Documents
-
view
217 -
download
0
Transcript of Prevention of Surgical Site Infections (SSI) MSIPC Fundamentals of Infection Prevention & Control...

Prevention of Surgical Site Infections (SSI)
MSIPC Fundamentals of Infection Prevention & Control October 2014Karen Hoover, RNInfection Prevention Coordinator St. Mary’s of Michigan, Saginaw
SSI: A Complication of Surgical Care
• > 51.4 million surgical procedures/year in US• 31% of all HAI’s due to SSI, second only to UTI• > 91,000 readmissions for SSI Rx• 1 million additional inpatient days• 1.6 billion excess costs• Associated mortality rate of 3%
Cost… Pay for performance …patient safety
CDC’s Guideline for Prevention of Surgical Site Infection, 1999.8
• Jan 2014 CDC

Common surgical/Procedures• 719,000/year Total knee • 498,000 hysters• 395,000 CABG• 332,000 Total Hip
• Ambulatory• 1.3 million cataracts• 923,000 Lens implants• 779,000 Endoscopies• 735,000 Injections of spine• Approx. 40% have more than 1 procedure
CDC www.cdc.gov/nchs/data/nhsr/nhsr011.pdf
Risk Factors for SSI: identification & opportunities for intervention
• Risk factor: variable with significant, independent association with development of SSI
• Patient: age, nutrition, diabetes, smoking, obesity, immunocompromised, pre-op LOS, micro-flora, other infection
• SSI prevention measure: action(s) to reduce SSI risk, antibiotic prophylaxis, skin prep/antisepsis
• Operation: …patient & peri-op personnel, duration, antibiotic redosing,, surgical asepsis, traffic flow, surgical technique (robotic), hair removal, immediate use sterilization
• Environmental: cleaning, disinfectant contact time, UV light, OR environment-HVAC
• Risk of SSI after receipt of blood products 3.5%

Principles for Prevention of SSI
• Minimize access of bacteria to the surgical site
• Measures to neutralize that do gain access to site
• Reduce that which is conducive to infection
• Enhance the host defenses - look at risk factors
• Follow established guidelines

Pathogenesis of Surgical Site Infection (SSI)• Dose x virulence Resistance of Host = risk of SSI• > 105 / gm tissue risk; with
foreign body only 100/gm is needed to cause SSI
• Pathogens:Endogenous – flora normally containedExogenous – healthcare personnel, environment, devices/materials used

Key Concepts on Source of SSI Pathogen: OR personnel or patient?
• Every surgical site has bacteria by the end of the procedure!
• Four Clinical variables determine infection:
• Inoculum of bacteria• Virulence of bacteria• Microenvironment• Host defensesEndogenous – flora normally contained

Distribution of Pathogens Causing SSIs
S. aureus 20%
Coag.-neg Staph. 14%
Enterococci 12%
P. aeruginosa 8%
E. coli 8%
Enterobacter spp. 7%
Other gram neg. 8%
B. fragilis 2% Mangram AJ. AJIC 1999;27:97-134

Risk Classification for SSI:• CLASS I/CLEAN WOUNDS--an
uninfected surgical wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tracts are not entered.
• CLASS II/CLEAN-CONTAMINATED WOUNDS--a surgical wound in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination.
• CLASS III/CONTAMINATED WOUNDS--open, fresh, accidental wounds. In addition, surgical procedures in which a major break in sterile technique occurs (eg, open cardiac massage) or there is gross spillage from the gastrointestinal tract and incisions in which acute, nonpurulent inflammation is encountered are included in this category.
http://findarticles.com/p/articles/mi_m0FSL/is_1_88/ai_n27912210/

Smoking & Surgery: Bad combination• Randomized, controlled trial: 48
smokers(S) vs 30 never smoked (NS)
• 228 wounds evaluated• SSI rate 12% S vs 2 % in NS• SSI rate significantly less for S if
abstain for 4wks (27% vs.1.1%)• Wound rupture: 12% S vs. 0% NS• When to stop … 30 days? 2-6months?
Sorensen LT. Ann Surg 2003;238:1-5

Preoperative Patient Shower with Antimicrobial Soap
• Bacterial counts on skin are 9-fold lower after shower - chlorhexidine
• CDC SSI Guidelines: Require patients to bathe with antiseptic on at least the night before their operation
• CHG cloth use night before & day of surgery

Intranasal Mupirocin & Prevention of SSI
• Orthopedic & cardiothoracic patients - significant reduction in SSI among treated1-3
• However these were retrospective & used historical controls
• Another randomized trial in ortho.surg found less S. aureus nasal carriage but no signif. Reduction in SSI rate4
1. Kluytmans JAJW. ICHE 1996;17:780-5.2. Cimochowski GE. Ann ThoracSurg 2001;71:1572-9.3. Wilcox MH. J Hosp Infect 2003;54(3):196-201.4. Kalmeijer MD. Clin Infect Dis2002;35:353

0
0.5
1
1.5
2
2.5
3
Overall Superficial
Sternal SSI Rates/100 Procedures
BaselineInterven
RatePer100 CABGs
Preventing Surgical Site Infection: System-level success [Usry GH, et al. AJIC 2002;30:434-6.]
Intervention: Intranasal mupirocin48 hrs prior to through 5
days post op
Results:94% of patients RxRate of SSI dropped by:
53% overall55% for deep sternal
Surgical Care Improvement Project (SCIP)
• Antibiotic Timing - <60min
• Antibiotic Selection – type/body location
of procedure - dosing for body wt. - duration of procedure - PCN allergy? - cost of antibiotic
• 2006
• http://www.medscape.org/
viewarticle/531895_2•Ancef• Vancomycin or Clindamycin

Surgical Care Improvement Project (SCIP)
within 24 hours surgery end time (SStop ATB 24 Hours end time 48 for Cardiac Surgery
Blood sugar <200 at 6 am POD 1 & 2S Controlled @ < 200 by 6STTTTTTGKLBLK a.m. POD 1 & 2
forAppropriate Hair removal …no razors
DVT Prophylaxis
Beta-blocker given before OR and after unless contraindicated
DVTeICD (Int. Compression Device), TED’s, Heparin, Warfarin
Foley cath …remove by POD 2 or physician note why not

Centers for Medicare & Medicaid Services (CMS) Actions• Payment reforms for inpatient hospital services in 2008:
• …ensure that Medicare no longer pays for the additional costs of certain preventable conditions (including certain infections) acquired in the hospital…
1) Serious preventable events: Object left in during surgery; air embolism; Delivering ABO-incompatible blood or blood products
2) catheter-associated urinary tract infections3) pressure ulcers4) Vascular catheter associated infection5) Mediastinitis after CABG surgery6) Patient falls7) VAE8) Influenza vaccination rates9) Future: MRSA, S. aureus BSI, CDAD (C. diff)

Impact of SSI Occurring After Discharge
* Many/Most SSI not identified until after discharge
• Cost for care with SSI were 2.9 times greater
• 23% of readmits & 18% of ER visit …some at other facilities
• Post discharge SSIs can impair physical & mental health
• Surveillance (PDS) is inconsistent …phone/paper …honest
• Education - ? enough/consistent/updated
• Host defense – acute and chronic medical conditions
• Effective management to minimize consequences

Stitch/ Superficial Deep
Pt. DOB Surg Class Room Procedure Description Staple Incisional Incisional
J 5/22/63 3/7 1 OR 12 DECOMPRESSIVE LAMINECTOMY L4-5, L5-S1, NEURO FORAMOTOMY L4-5, L5-S1
J 4/8/54 3/7 1 OR 12 KNEE ARTHROSCOPY LEFT
J 7/29/59 3/30 1 OR 12 KNEE ARTHROSCOPY RIGHT, PARTIAL MENISCECTOMY,
J 6/20/62 3/14 1 OR 12 KNEE ARTHROSCOPY LEFT, PARTIAL MENISECTOMY, PARTIAL CHONDROPLASTY
J 11/19/68 3/21 1 OR 12 KNEE ARTHROSCOPY RIGHT, PARTIAL CHONDROPLASTY, RELEASE PLICA
J 1/28/32 3/28 1 OR 12 KNEE TOTAL ARTHROPLASTY LEFT
J 8/31/91 3/28 1 OR 12 left KNEE ARTHROSCOPY with fixation of osteochondyle fx, debridement of
J 8/18/40 3/21 1 OR 12 LEFT TOTAL HIP REPLACEMENT
J 9/10/30 3/11 1 OR 10 OPEN REDUCTION, PINNING RIGHT FEMORAL NECK
J 1/29/05 3/15 1 OR 8 REALINEMENT WITH PINNING AND CASTING LEFT ELBOW
J 9/16/60 3/14 1 OR 12 RELEASE OF ACHILLES TENDON RIGHT
J 2/24/32 3/7 1 OR 12 REMOVAL OF FOREIGN BODY RIGHT THIGH ANTIBIOTIC BEADS
J 5/14/59 3/30 1 OR 12 REVISION LEFT TOTAL KNEE ARTHROPLASTY, EXTENSIVE SYNOVECTOMY
J 11/1/44 3/28 1 OR 12 REVISION, POLY LEFT KNEE, DEBRIDMENT, LATERAL RELEASE
J 1/13/25 3/21 1 OR 12 RIGHT KNEE ARTHROSCOPY, CHONDROPLASTY, PARTIAL MENISCECTOMY
J 12/1/38 3/28 1 OR 12 RIGHT OPEN QUADRICEPS REPAIR WITH AFLEX GRAFT
Stitch/staple: minimal inflammation and discharge confined to the points of suture penetration
Superficial Incisional: Purlent drainage from the superficial incision; or pain or tenderness, localized swelling, redness, or
heat, and superficial incision is deliberately opened by surgeon, and is culture-positive or not cultured
If from secondary incison (e.g., donor site [leg] incision for CABG), please note: Y- SIS
Deep incisional : a. purulent drainage from the deep incision but not from the organ/space
b. incision spontaneously dehisces or is deliberately opened by a surgeon and is culture-positive or not cultured
a. purulent drainage from the deep incision but not from the organ/space
during reoperation, or by histopathologic or radiologic examination .
ICD – 9 – CM codes

The Challenge of Surveillance of SSIs: expanding universe of health care delivery
• Major trend towards delivery in wide range of settings
• Short lengths of stay + inter-facility transfer is common
Networking!
Ambulatory Surgery: Risk Free?
• Cluster of fungal contamination of saline breast implant
• Saline bottle stored under water-damaged ceiling &
• OR in negative pressure• Kainer MA. 40th IDSA
(abstr)
Cluster of Endoph-thalmitis after cataract surg.Acremonium kiliense4 patientsRisk Factor (RF): 1st case, MondaysHumidified air in ventilation likely source
Fridkin SK. Clin Infect Dis 1996;
Steroid Injection Outbreak

CMS for Ambulatory Care
• 42 CFR Part 416 Medicare and Medicaid Programs; Ambulatory Surgical Centers (ASC), Conditions for Coverage:
• …require the ASC to designate a qualified professional, such as a registered nurse, as the infection control officer
• The infection control condition places accountability on ASCs to prevent, control, and
• investigate infections and communicable diseases, and take action that result in improvements…

Waterless Alcohol-based Hand Rub for Surgical Hand Antisepsis
• Randomized trial, 4387 pts.
• Hand rub vs scrub with antimicrobial soap + water
• SSI rate in hand rub (2.4%) vs scrub (2.5%) not signif.
• Better compliance, less skin irritation/dryness with hand rub in personnel WHO
Parienti JJ. JAMA 2002;288:722-77

Possible SSI Prevention Measures
• Subcuticular suturing vs skin stapling technique, CABG - 2 studies; no consistent results (Mullen JC. Can J Cardiol 1999;15:65- ; Chughtai T. Can J Cardiol 2000;16:1403-)
• Quill Suturing? …expensive• Anemia & leukocyte-depleted red blood cell transfusion
- studies have had mixed results; more study needed(Jensen LS. Transfusion 1995;35:719-; Titlestad IL. Int J Colorectal Dis 2001;16:147-;van de Watering LM. Circulation 1998;97:562-)
• Laminar Airflow & Orthopedic Surgery - Mixed results & difficult to demonstrate clear cost effectiveness (Berbari EF.
Clin Infect Dis 1998;27:1247-)
Possible SSI Prevention Measures
• Supplemental perioperative oxygen- randomized trial found lower SSI with 80% O2 among 500 colorectal surgery pts.;however-high SSI rate & risk index in control population - Need confirmation (Grief R. N Engl J Med 2000;342:161-7)
• Periop. normothermia - randomized trial of 200 patients, colorectal surgery pts. = lower SSI rate with additional warming(forced air + IV fluids) vs those with regular care; more investigation needed for wider application (Kurz A. N Engl J Med 1996;334:1209-15)

Category IA SSI Prevention Recommendations
• Patient-focus: • treat existing infections first
before OR• avoid hair removal but if
needed use clippers• Asepsis & technique:
• aseptic principles: IV, inserting catheters, administering medications
AJIC 1999;27:97-132

Category IB SSI Prevention Recommendations
• Patient-focus: • control serum blood glucose• encourage tobacco cessation• preop shower• clean skin incision site + apply
antiseptics• Surgical Team:
• no artificial nails• surgical hand antisepsis
AJIC 1999;27:97-132

Category IB SSI Prevention Recommendations
• Intraoperative: • Positive pressure in OR• Min. 15 air changes/hour• Filter supply air • Keep OR doors closed as much as possible• sterilize surgical instruments; limit flash
sterilization
• Surgical Team:• surgical mask, hair cover• gown & sterile gloves• Gentle handling of tissue
AJIC 1999;27:97-132
Category IB SSI Prevention Recommendations
• Surveillance: • Use CDC definitions• Apply risk index• Periodically calculate risk stratified SSI
rates• Report SSI rates to surgical personnel• Use standard case finding methods
AJIC 1999;27:97-132

Surgical Site Infection Criteria
• Superficial incisional SSI • Infection occurs within 30 days after any NHSN operative procedure and • involves only skin and subcutaneous tissue of the incision and
• patient has at least one of the following: • a. purulent drainage from the superficial incision. • b. organisms isolated from an aseptically-obtained culture of fluid or tissue from the
superficial incision. • c. superficial incision that is deliberately opened by a surgeon and is culture-positive or
not cultured • and patient has at least one of the following signs or symptoms: pain or tenderness;
localized swelling; • redness; or heat. A culture negative finding does not meet this criterion. • d. diagnosis of a superficial incisional SSI by the surgeon or attending • physician or other designee (see reporting instructions).

Two specific types of superficial incisional SSIs
• Superficial Incisional Primary (SIP) superficial incisional SSI that is identified in the primary incision in a patient that has had an operation with one or more incisions (e.g., C-section incision or chest incision for CABG)
• Superficial Incisional Secondary (SIS) superficial incisional SSI that is identified in the secondary incision in a patient that has had an operation with more than one incision (e.g., donor site incision for CBGB)
• Do not report a stitch abscess, stab wound or pin site infection as SSI • Diagnosis of “cellulitis”, by itself, does not meet criterion d for superficial incisional SSI.

Deep incisional SSI • Infection occurs within 30 or 90 days after the NHSN operative procedure and involves deep soft tissues of the incision (e.g., fascial and muscle layers) and patient has at least one of the following: • a. purulent drainage from the deep incision. • b. a deep incision that spontaneously dehisces or is deliberately opened by a surgeon and is culture-positive or not cultured and patient has at least one of the following S/S: fever (>38°C); localized pain or tenderness. • c. an abscess or other evidence of infection involving the deep incision • d. diagnosis of a deep incisional SSI by a surgeon or attending physician or other designee

Organ/Space SSI
• Infection occurs within 30 or 90 days after the NHSN operative procedure and
infection involves any part of the body, excluding the skin incision, fascia, or muscle layers, that is opened or manipulated during the operative procedure and
patient has at least one of the following: • a. purulent drainage from a drain that is placed into the
organ/space • b. organisms isolated from an aseptically-obtained culture of fluid or tissue in the organ/space • c. an abscess or other evidence of infection involving the organ/space

Special Comments:
• Occasionally an organ/space infection drains through the incision and is considered a complication of the incision. Therefore, classify it as a deep incisional SSI.
• • Report mediastinitis following cardiac surgery that is accompanied byosteomyelitis as SSI-MED rather than SSI-BONE. • • If meningitis (MEN) and a brain abscess (IC) are present together after operation, report as SSI-IC. • • Report CSF shunt infection as SSI-MEN if it occurs within 90 days of placement; if later or after manipulation/access, it is considered CNS-MEN • Report spinal abscess with meningitis as SSI-MEN following spinal surgery.

Environmental Infection Control Guidelines, 2003
• HVAC: • Positive pressure ventilation• Filtration
• Environmental Cleaning• Preventing water-associated
illness• Preventive maintenance MMWR 2003;52:RR-10

A Surgeon’s Perspective on Prevention of SSI
“The most critical factors in the prevention of postoperative infections, although difficult to quantify, are the sound judgment and proper technique of the surgeon and surgical team, as well as the general health and disease state of the patient”
-Nichols RL. Emerg Infect Dis 2001;7(No.2):220-4.

How to Display SSI data:• Target …state in IP Plan• Just %? …what if 1 of 2 procedures develop SSI?• Denominator & numerator?• Graphs• Previous year …2 years?• Scorecards• Compare with NNIS vs Standard Infection Ratio (SIR)• Special Investigations• High volume surgery• Surgeon specific?• “Tell them/show them what they need to see”
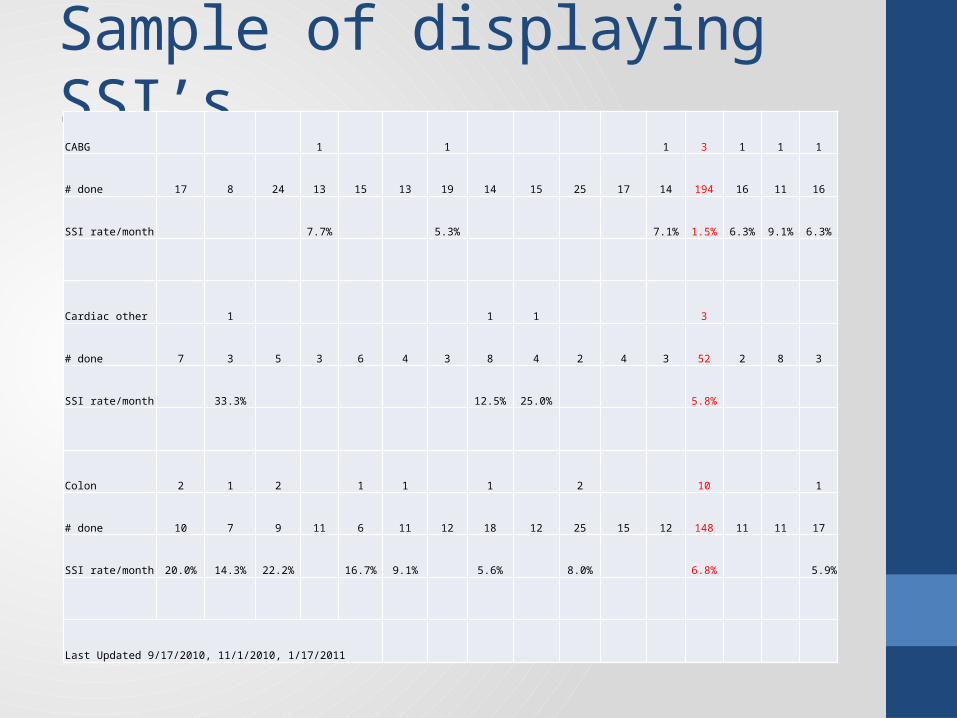
Sample of displaying SSI’sCABG 1 1 1 3 1 1 1
# done 17 8 24 13 15 13 19 14 15 25 17 14 194 16 11 16
SSI rate/month 7.7% 5.3% 7.1% 1.5% 6.3% 9.1% 6.3%
Cardiac other 1 1 1 3
# done 7 3 5 3 6 4 3 8 4 2 4 3 52 2 8 3
SSI rate/month 33.3% 12.5% 25.0% 5.8%
Colon 2 1 2 1 1 1 2 10 1
# done 10 7 9 11 6 11 12 18 12 25 15 12 148 11 11 17
SSI rate/month 20.0% 14.3% 22.2% 16.7% 9.1% 5.6% 8.0% 6.8% 5.9%
Last Updated 9/17/2010, 11/1/2010, 1/17/2011

Post discharge Data Surveillance:
Patient Name DOB Surgery Class Room Procedure DescriptionName of hospital_________________Education: New surgeons/Annually (definitions)Skin/staple related? …don’t count Incisional … skin or sub-Q , drainage, dehisence, I&DAny cultures?Readmit? Within 30 days vs NEW 2013: 90 days (implants)

SSI Surveillance & Prevention Intervention
• Feedback: surgeon/surgical personnel or committee (s)
• Result: Overall SSI rate/SIR for given (targeted) surgeries
• Action Plan: Quality Improvement – education, equipment, timing, etc. 0
2
4
6
8
10
1994 1997
Yr
SSI: Joint Arthroplasty, 94-99
DeepSSISuperfic. SSI
Summary Aspects of Surveillance Program for Prevention of SSIs• SSIs cause considerable morbidity and mortality
and are expensive complications to treat - prevention therefore is cost effective
• Surveillance & Interventional Epidemiology is an effective component of a facility’s patient safety/performance improvement program
• Feedback of process & outcome data is helpful but broad partnership involving multiple disciplines is likely key to success
Skin & Soft Tissue Infections
• Changing Pattern of Community- Associated Skin and Soft-Tissue Infection with methicillin-Resistant Staphylococcus aureus (CA-MRSA)
• Almost three quarters of the soft-tissue infections were caused by CA-MRSA (N=389 patients)• King MD, et al. Ann Intern Med 2006; 144:309-317.

Conclusions:
• SSI’s will always be with us• MDRO’s will challenge us• New techniques and technology will evolve• Government agencies will change how we
measure quality performance• Reimbursement can effect our process, advancing
to new equipment or products, how we stay in business
• Do you know what and how to collect data?

Sterile Processing• From Acquisition to Reuse

Sterilization of Equipment• Certified technicians
• Cleaning …ultrasonic (5 to 10 min) open instruments …DRY/inspect
• Wrapping … trays

Sterilization• - Steam 121oC (250oF) and 132oC (270oF). Manufacturers
recommendation. Bowie-Dick test is used to detect air leaks and inadequate air removal
Biological monitor: Geobacillus stearothermophilus (formerly Bacillus stearothermophilus)
Monitored using a printout (or graphically) by measuring temperature, the time at the temperature, and pressure - Sterrad• -Portable (table-top) steam sterilizers • - Immediate use
• www.roboz.com/catalog%20pdfs/Sterilization_and_Maintenance.pdf quick chart• www.cdc.gov/hicpac/Disinfection_Sterilization/13_0Sterilization.html
Correct loading /unloading• Sufficient space must occur around the packages • place items on edge and no chamber wall touching• do not stack packages or cassettes one upon the other• paper of one pouch next to the plastic of the adjacent pouch• Basins, bowls or other devices on their sides • running a load with both linens and medical instruments,
place the linen packs on the top shelf • heavy medical items or large trays flat on the bottom shelves
• Some steam sterilizers have an automatic dry cycle • opening the door about ½ inch after the pressure equalizes
and let items sit inside the chamber for 30 to 60 minutes• Wet packages that exist at the end of steam-sterilization cycles
should not be handled

Steam Sterilizer recall• Recalls due mechanical, chemical and biological -Who you going to call?• Retrieval of processed items • Notify your sterilizer service representative • Re-validated with three consecutive negative biological
monitors in three consecutive cycles
• AAMI recommends that sterilizers be biologically monitored at least once a week, preferably daily, when normal cycles are used, in each flash sterilization load and in any load containing an implantable device.
• http://www.spdceus.com/recalls.htm for online info & quiz