SUDDEN CARDIAC DEATH
110
SUDDEN CARDIAC DEATH Yuanxiu Chen, MD, Ph.D DEPT. OF CARDIOLOG Y RENMIN HOSPITAL WUHAN UNIVERSITY
description
SUDDEN CARDIAC DEATH. Yuanxiu Chen, MD, Ph.D DEPT. OF CARDIOLOGY RENMIN HOSPITAL WUHAN UNIVERSITY. DEFINITION. - PowerPoint PPT Presentation
Transcript of SUDDEN CARDIAC DEATH

SUDDEN CARDIAC DEATH
Yuanxiu Chen, MD, Ph.D
DEPT. OF CARDIOLOGY
RENMIN HOSPITAL
WUHAN UNIVERSITY

DEFINITION
• Sudden cardiac death :unexpected natural death due to a cardiac cause within a short time period from the onset of symptoms in a person without any prior condition that would appear fatal

Key points
• Time ≤1 hour (24hours) from the onset• Cardiac arrest Discontinuation of
blood supply to brain• Die or survive• History of heart disease: with or without

Pathophysiological Mechanism病理生理机制
• Life threaten arrhythmias arising from several pathological condition– Tachyarrhythmias– Bradyarrhythmias or asystolic arrest– Pulseless electrical activity,PEA

• Tachyarrhythmias 快速性心律失常
Ventricular fibrillation 70%
心室颤动

Sustained ventricular tachycardia <2% 持续性室速

• Bradyarrhythmias or asystolic arrest 缓慢性心律失常 心搏停顿
Sinus asystole

• Pulseless electrical activity,PEA
( 无脉搏性电活动 )
Electromechanical dissociation
( 电机械分离 )

EPIDEMIOLOGY (流行病学)
• Incidence 发生率300,000-400,000 yearly in USA
• Account for >50% cardiac death• In China no accurate figure huge population victims must might be numerous

Influence of Age, Race, and Gender
• AGE 年龄The incidence of sudden cardiac death in
creases with age, in both men and women
as well as whites and nonwhites because o
f the higher prevalence of ischemic heart
disease at older age

• RACIAL DIFFERENCES 种族差异rate of sudden coronary death is hig
her in blacks than in whites
• GENDER 性别Higher in men than in women

ETIOLOGY ( 病因学)• The relationship between structure and
function of the heart in sudden cardiac
death:
Cardiac death is related to a
lot of heart diseases

Coronary Heart Disease 冠心病• Account for more than 80% of SCDs in wes
tern countries
• First manifestation in 25% of CHD patients
• LVEF<30% is a strong predict factor for SCD in patients with coronary heart disease
• Atherosclerosis of multiple coronary arteries is the underlying pathophysiologic changes in such patients


Major Risk factors for CHD冠心病的主要危险因素
• Risk factors of atherosclerosis• Not well confirmed, but lots of
evidence prove that there are some factors might be related to CHD
• Multiple factors work together but at different aspects to cause CHD to happen

• Age >40 years older than 49 years — speed up some young people

• Gender more male suffer than female , 2 : 1 female suffer after menopause ( 绝经期后) because of decrease of Estrogens( 雌激素 ) in
the circulation, with resulted in a drop of
HDL (high density lipoprotein)
(Estrogens) provides a protection for women against CHD?

• Abnormal in blood lipid 血脂异常 Hyperlipedamia 高脂血症 Total cholesterol 总胆固醇 Triglyceride 甘油三酯 Low density lipoprotein LDL 低密度脂蛋白 Very low density lipoprotein 极低密度脂蛋白 Apoprotein B 载脂蛋白 B Apoprotein A 载脂蛋白 A High density lipoprotein 高密度脂蛋白

• Hypertension
60-70%CHD patients have hypertension
4 times than normal blood pressure pts
both SBP and DBP are significant

• Smoking 吸烟 risk raises 2-6 times

•Diabetes mellitus 糖尿病2 times danger than the non-diabetes patient

• Body weight 体重 (Obesity 肥胖 )

• Occupation 职业• Diet 饮食• Heredity 遗传• Others

Cardiomyopathies
• Idiopathic dilated cardiomyopathy
• Hypertrophic cardiomyopathy
• Hypertensive cardiomyopathy
• Arrhythmogenic right ventricular dysplasia ( 致
心律失常性右室发育不良)

Valvular heart disease
• Mitral valve prolapse syndrome
二尖瓣脱垂综合征• Other valvular heart diseases
– Aortic stenosis( 主动脉瓣狭窄)

Inflammatory myocardial disease
• Myocarditis 心肌炎 several kind of arrhythmia might develop
atrioventricular block

Congenital heart disease 先天性心脏病
• Arrhythmia
• Hemodynamic changes 血流动力学改变

Long QT syndrome
• Congenital • Acquired
torsades de points (TDP, 尖端扭转性室速) twisting ( 扭转) of the peaks and troughs of the QRS complexes in relation to the baseline

Brugada Syndrome
• Died suddenly during night• Young patient without any evidence of
heart disease• Family histroy• Elevated ST segment ( V1-3 ) with r
ight bundle block • Some defect in certain gene

Wolff-Parkinson-white syndrom
• Accessory AV pathway 房室旁路• Also called “preexciteation syndrome”

• paroxysmal supraventricular tachycardia
阵发性室上性心动过速

•Atrail fibrillation ----ventricular fibrillation

Idiopathic ventricular fibrillation原发性室颤

Drugs and other toxic agents Proarrhythmia 致心律失常作用
• Antiarrhythmic agents
quinidine (奎尼丁) flecainide (氟卡尼) encainide (恩卡尼) CAST(Cardiac Arrhythmia Suppression Tra
il ) Evidence Based Medicine

Evidence Based Medicine循症医学
• Multicenter
• Randomized
• Double blind
• Placebo controlled

Cocaine and alcohol 可卡因及酒精
• Drug abuse : Cocaine Marihuana (大麻)
• Alcoholic : excessive drinking

Electrolyte abnormalities 电解质紊乱
• Hypokalemia 低钾血症• Magnesium deficiency 低镁• Increase in intracellular calcium

Pathology of SCD Caused by CHD
• The coronary arteries
Extensive atherosclorosis
Acute atherothrombosis
Coronary arteries spasm

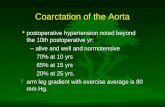
What is Atherothrombosis?• Atherothrombosis is characterized by a sudden
(unpredictable) atherosclerotic plaque disruption (rupture or erosion) leading to platelet activation and thrombus formation
Plaque rupture1Plaque erosion2
1. Falk E et al. Circulation 1995; 92: 657–71. 2. Arbustini E et al. Heart 1999; 82: 269–72.

• Atherothrombosis is the underlying condition that results in events leading to myocardial infarction, ischemic stroke, and vascular death

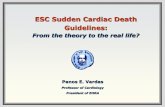
• Atherothrombosis

Plaquerupture
Platelet activation and aggregation
Non-occlusivethrombus
Acute syndrome:• coronary• cerebrovascular• peripheral
Occlusivethrombus
Healing andresolution
Plaque growth
The Development of Atherothrombosis – a Generalized and Progressive Process
Adapted from: Drouet L. Cerebrovasc Dis 2002; 13(suppl 1): 1–6.

Atherothrombosis and Microcirculation
Adapted from: Topol EJ, Yadav JS. Circulation 2000; 101: 570–80, and Falk E et al. Circulation 1995; 92: 657–71.
Plaquerupture
Microvascular obstruction
Embolization

Major Clinical Manifestations of Atherothrombosis
Adapted from: Drouet L. Cerebrovasc Dis 2002; 13(suppl 1): 1–6.
Transient ischemic attack
Angina:• Stable• Unstable
Ischemicstroke
Myocardial infarction
Peripheral arterialdisease:• Intermittent claudication• Rest Pain• Gangrene• Necrosis

• The myocardium(of sudden cardiac
death by autopsy)
– Healed myocardial infarction is a common
finding of autopsy in the victims
– Frequency ranging from 40-70%
– Acute myocardial infarction is about 20%

Mechanism and Pathophysiology of SCD
• Mechanism of tachyarrhythmias resulted from
coronary atherosclorosis is not clear
• Coronary artery disease caused the blood flow t
o myocardium decrease, which resulted in meta
bolic change and electrophysiological( 电生理) instability, both could lead to ventricular
fibrillation

• Long term left ventricle overload (负荷过
重) and ischemic injury could cause the distur
bance of cellular electrophysiology, resulted in
ventricular fibrillation

• At the level of myocyte, acute ischemia cause :
– Loss of integrity of cell membranes
– Efflux of K+
– Influx of Ca2+
– Acidosis
– Reduction of transmembrane resting potentials
– Alpha- and/or beta-adrenocepter and autonomous n
ever activity alteration
As the result, the electrical instability increased

• Ischemia increases the dispersion ( 离散度)of repolarization (复极) between the nor
mal and diseased tissue, induces afterpolariza
tion (后除极) as triggering response for C
a2+-dependent arrhythmia, finally leads to ve
ntricular fibrillation


• SCD caused by bradyarrhythmias and as
ystolic arrest often appeared in severely d
iseased hearts
• Probably represent diffuse( 广泛) invol
vement of subendocardial Purkinje fibers

• Systemic influences that increase extracellular K+ concentration including:– Acidosis– Shock– renal failure– Trauma– HypoxiaResult in partial depolarization of cells in His-Pur
kinje system, with a decrease in the slope (斜率) of spontaneous phase 4 depolarization and ultimate loss of automaticity( 自律性)

• Long time asystolic arrest may degenerat
e to ventricular fibrillation or persistent a
systole

• Pulseless electrical activity (PEA)
• Electromechanical dissociation(EMD)
• Could be separated into
– Primary form
– Secondary form

• Primary form:
– Failure of electromechanical coupling
– Usually occurs as an end-stage event of
advanced heart disease, acute ischemic
events or after electrical resuscitation
from a prolonged cardiac arrest

• Secondary form:
– Result from abrupt cessation of cardiac venous return
( 静脉回流中断)– Massive pulmonary embolism (巨大肺栓塞)– Acute mulfunction of prosthetic valves (人工瓣膜急
性失效)– Cardiac tamponade from hemopericardium 心包积血

How to?
• Pulseless electrical activity (PEA) is related
to metabolic disorder of intracellular Ca2+,in
tracellular acidosis and deficiency of ATP

Clinical presentation
• Prodromes ( 前驱症状)• Onset of terminal events (终末事件开
始)• Cardiac arrest (心脏骤停)• Biological death (生物学死亡)
---- Differ greatly from one to another

OMENOUS SYMPTOMS 前兆症状
• Chest pain 胸痛• Dyspnea 呼吸困难• Fatigue 疲劳• Palpitation 心悸
• Some patients may not have prodromes and cardiac arrest might be the first manifestation

Terminal events
• Beginning of cardiac arrest
• Due to the abrupt change of cardiovascular function
• Duration: within 1 hour
• Heart rate increase, ventricular ectopic beat, ventricular tachycardia might develop

Cardiac arrest• Abrupt loss of consciousness 意识丧失 Cardiac arrest cause the blood supply to tbe brain drop abru
ptly • Pulse at carotid artery ( 颈动脉 ) or femoral artery ( 股动
脉) disappeared• Breath stoped (呼吸停止)• Heart sound disappeared (心音消失)• Paleness of the skin ( 皮肤苍白)
Observation should be done rapidly so that resuscitation ( 复苏 ) could begin in short time

Biological death
• Time from cardiac death to biological death depends on :– Underlying disease
– Time from SCD to the beginning CPR

• Irreversible brain injure occurs 4-6
min after ventricular fibrillation
biological death gradually

• Time from VT to biological death: lo
nger, VT might turn to VF or asystol
ic arrest ( 心室停搏) if not termina
ted automatically of by therapy(medi
cal, electrical)

• Asystolic arrest or bradyarrhythmia
s: biological death occurs shortly

MANAGEMENT OF CARDIAC ARREST心脏骤停的处理
• Outside hospital
• Community emergency system important社区急救系统

TRY FOLLOWING MEARSURES IMMEDIATELY • THUMPVERSION (捶击复律) using fist (拳头) to hit the victim at
the middle-lower part of the breast bone (胸骨中下段交界处)
• COUGH-VERSION (咳嗽复律) increasing of intra-thoracic pressure (胸腔内
压) might stop the tachyarrhythmias • KEEP THE AIRWAY OPEN

BASIC LIFE SUPPORTcardiac pulmonary resuscitation
( 心肺复苏 )• Airway
• Breathing
• Circulation
• Defibrillation

• Airway head tilt – chin lift ( 头倾抬颏) if trauma is present, use jaw thrust
( 如果存在创伤,需行颌牵引)

• Breathing look, listen, and feel for no more than
10 seconds mouth-to-mouth artificial breath 人工呼吸 10-12 breaths/min
intubation if possible
(better)

• Circulation
Check for sign of circulation
(breathing, cough, movement)
including pulse for no more than
10 seconds

• If signs of circulation/pulse present but no breathing, provide rescue breathing
• If signs of circulation/pulse absent, begin chest compression interposed with breaths
• If signs of circulation/pulse present but < 60bpm in child or infant with poor perfusion, begin chest compression

• Compression landmarks lower half of sternum• Compression method heel of one hand, other hand on top• Compression depth
11/2 to 2 inches• Compression rate
approximate 100/min• Compression/ventilation ratio 15:2(single rescuer or two rescuers.)

• Defibrillation
Using automated external
defibrillators is now considered an
integral part of adult basic life support
by healthcare provider
VT: synchronized
VF: non-synchronized

ADVANCED LIFE SUPPORT
• IV ACCESS Drug therapy
anti-arrhythmic agents
tachycardia
bradycardia• MORNITORING AFTER CPR
PREVENTION AND TREADMENT OF
ENCEPHALO edema
prevention and treatment of renal failure

• Cardiopulmonary resuscitation(CPR) Airway 气道 Breath 人工呼吸 Circulation 循环( Chest compression 胸按压) Defibrillation , Drugs 除颤,药物 Electrolyte 电解质 Fluids 体液 Gas 气体

Treatment of Ventricular fibrillation 室颤的处理
• Witnessed arrest Unwitnessed arrestCheck pulse—if no pulse check pulse—if no
pulsePrecordial thump Check pulse—if no pulseCPR until a defibrillator is availableCheck monitor for rhythm—if Vf or VT Defibrillate, 200JDefibrillate, up to 360JCPR if no pulse

Establish IV accessEpinephrine, 1:10,000,0.5-1mg iv PUSHIntubate, if possibleDefibrillate with up to 360JLidocaine, 1mg/kg IV PUSHDefibrillate with up to 360JBretylium, 5mg/kg IV PUSH(Consider bicarbonate)Defibrillate with up to 360JBretylium, 10mg/kg IV PUSHDefibrillate with up to 360JRepeated lidocaine or bretyliumDefibrillate with up to 360J

MENAGEMENT FOR ASYSTOLEIf rhythm is unclear and possibly ventricular Fibrillation, defibrillate as for ventricular fibrillation.If asystole is presentContinue CPREstablish IV accessEpinephrine,1:10,000, 0.5-1mg IV PUSHIntubate when possibleAtropine, 1.0mg IV PUSH(repeated in 5 min)(Consider bicarbonate)Consider pacing

MANEGEMENT FOR ELECTRO-MECHANIC
AL DISSOCIATION
( Pulseless electrical activity 无脉性电活动)
Continue CPREstablish IV accessEpinephrine, 1:10,000,0.5-1.0mg IV PUSHIntubate when possibleConsider bicarbonateConsider hypovolemia 低血容量 , cardiac tamponade 心包填塞 , tension pneumothorax 张力性气胸 , hypoxemia 低氧血症, acidosis 酸中毒, pulmonary embolism 肺栓塞

Some advance in CPR
• Amiodarone (胺碘酮) or lidocaine
• Intubation (插管) or mask (面罩)

Monitoring after CPR
• 48-72h monitoring in ICU ( CCU ) after CPR• Treatment of original disease leading to SCD• Maintenance of effective circulation and
respiration• Prevention of recur of SCD• Balance of fluid , electrolyte and acid-base• Prevention of cerebral edema and acute renal
failure

Prognosis 预后• Associated with the cause
Structural heart disease : poor
Nonstructural heart disease : depends
resulting from severe illness such as cancer,
multiple organs failure( 多器官衰竭): poor
arising from intoxication 中毒 , Electrolyte
abnormalities( 电解质紊乱) , etc : might be better

Prevention
• Medicine
• RFCA
• Implantable cardioversor defibrillator (ICD)
• Revascularization ( PTCA , Surgery )

Medicine
• Prevention of coronary heart disease– Antihypertensive agents– Lipid lowering medicine– Blood sugar lowering madicine – Aspirin
• Antiarrhythmic agents

• Antiarrhythmic agents– Flecainide , encainide , sotalol have been pr
oven to increase the death rate in ischemic heart disease
– ß-blocker Metolol is said to be benefit for patients with myocardial infarction in lowering arrhythmic mortality and total mortality
– Amiodarone: lowering arrhythmic mortality

ICD
• Implantable cardioverter and difibrillator

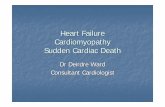
心脏骤停发作时心律
Source: After Josephson, ME
6:02 AM
6:05 AM
6:07 AM
6:11 AM

ICD 的作用是什么 ?
• 挽救病人生命 Save patients’ life – 降低病死率
decrease the mortality
• 改善生活质量 Improve the quality of life– 减少对死亡的担忧 worry– 减少 VT 治疗花费 expense– 减少药物副作用 side effect– 增加安全 - 即使无药物,仍然起作用 safety
…

ICD 主要功能 Main function
1. 抗心动过缓起搏 Anti-bradycardia pacing
2. 识别室性快速心律失常— Recognizing VT/VF
3. VF 的治疗:电击除颤 Difibrillation
4. VT 的治疗: ATP(Anti-tachycardia pacing) 、同步复
律 Synchronized cardioversion)
5. 存储心内电图和事件资料 Storage of events

91

一例真实的病人 A real case 6060 岁,男性;岁,男性; 19781978 年第年第 11 次心脏病发作;次心脏病发作; 19841984 年第年第 22 次心脏病发作;次心脏病发作; 19881988 年第年第 33 次心脏病发作后,接受冠状动脉搭桥手术;次心脏病发作后,接受冠状动脉搭桥手术; 20002000 年年 1111 月,第月,第 44 次心脏病轻微发作后,接受次心脏病轻微发作后,接受 PTCAPTCA 手术;手术; 20012001 年年 33 月,胸痛,再次接受月,胸痛,再次接受 PTCAPTCA 手术,改善冠状动脉堵塞状况;手术,改善冠状动脉堵塞状况; 20012001 年年 66 月,月, HolterHolter 记录发现记录发现 2 s2 s 多的多的 135bpm 135bpm 短阵心动过速短阵心动过速


2001 年 6 月 30 日 ( 星期六 ) 8:00am
Dick Cheney接受心脏电生理检查,医生诱发出持续
室速并及时终止

ICD 型号— 美敦力 GEM III


手术植入时间 1 小时
Dick Cheney 在医院作短暂休息观察后,当天 3:00pm离开医院,回到家中休养




2001 年 7 月 2 日 ( 星期一 )上午
美国白宫总统椭圆型办公室


PTCA+Stent
• Percutaneous transluminal coronary angioplasty
• Percutaneous intracoronary stent implantation


造影示冠状动脉狭窄

支架置入术中

支架置入后,狭窄消
失

冠状动脉介入治疗前后影像对比

Question
• What is SCD?
• What’s the major cause of SCD?
• What’s the pathophysiological mechanism of SCD?
• What is CPR? How to perform CPR?

THANK YOU !