Sudden Cardiac Death
117
Sudden Cardiac Death Sudhir Chandra Sinha MD DM FACC FSCAI Member, European Heart Rhythm Association Consultant Interventional Cardiologist INDUS Hospitals, Visakhapatnam
description
Sudden Cardiac death, CPR
Transcript of Sudden Cardiac Death

Sudden Cardiac Death
Sudhir Chandra SinhaMD DM FACC FSCAI
Member, European Heart Rhythm AssociationConsultant Interventional Cardiologist
INDUS Hospitals, Visakhapatnam

Case#1: 48 year male with syncope
• Sudden onset palpitations
• BP-90/60, No SOB/Chest Pain
• ECG- monomorphic VT
• Cardioverted with 200 Jx1
• Echo- Non obstructive HCM



Risk factors for sudden death in Hypertrophic cardiomyopathy
• Syncope especially recurrent• Family H/O sudden death and
hypertrophic cardiomyopathy• Ventricular tachycardia• Subnormal(<20mmHg) increas in systolic
blood pressure on maximal exercise testing
• Marked (especially if >30mm) left ventricular hypertrophy


Case #2: 72 y male
• Sudden onset of chest pain
• Cardiac arrest while being transported to hospital
• CPR started
• Shifted to cath lab




Case #3: 12 y male child
• h/o collapse when he goes for cycling
• No other relevent history
• Seen by neurologist and cardiologist



Case #4: 40y male
• Admitted with h/o acute onset chest pain and pulmonary edema
• ECG- STE ASMI
• ECHO- RWMA in LAD territory
• Treated as STEASMI medically
• Coronary angiogram-predischarge



After 4 month
• Routine follow up
• Sudden collapse in OPD outside chamber
• CPR-Defibrillation
• ICD


Case #5
• 4 y child
• Congenital deafness
• Develops seizures whenever cries
• No symptoms otherwise


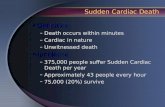
Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Drew, B. J. et al. J Am Coll Cardiol 2010;55:934-947
QTc distribution curves in normal males and females and in a cohort of patients with congenital LQTS

Case #6
• 64y/F
• Admitted with sepsis and MOD
• Developed cardiac arrest
• Cardiology consultation sought


Case #7
• 52y/F
• Presented with h/o one vomiting and weakness, fits like episodes
• Had recurrent fits while being transported from Orissa
• O/E patient has flaccid paralysis of all four limbs
• K-not recordable


Case # 8
• 82y/M
• No h/o HT/DM
• H/o loose motion and collapse
• ECG
• Had cardiac arrest


Case #9
• 20 y/M
• Daily vendor
• Has sudden episode of seizure despite treatment
• Seen by an anaesthetist and brought to hospital


Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Drew, B. J. et al. J Am Coll Cardiol 2010;55:934-947
Onset of TdP during the recording of a standard 12-lead ECG in a young male with a history of drug addiction treated with chronic methadone therapy who presented to a
hospital emergency department after ingesting an overdose of prescription and over-the-counter drugs from his parent's drug cabinet
Case# 10

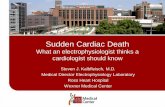
Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Drew, B. J. et al. J Am Coll Cardiol 2010;55:934-947
Top rhythm strip, TdP degenerating into ventricular fibrillation in an 83-year-old female hospitalized in the intensive care unit for pneumonia
CASE #11

Case #12
• 40y/F
• Admitted with CCF—DCM, NYHA IV
• Developed syncope
• Monitor - VF


•DEFINITION OF SCD
Any modification on the slide of the presentation are under the sole responsibility of his author

What is SCD ?Death by malfunctions in the electrical
system of the heart
SCD is often caused by a rhythm dysfunction called ventricular fibrillation (VF)
The ventricular muscle twitches randomly and the ventricles fail to pump blood into the arteries and into systemic circulation
Consequence : lack of oxygen in the body and finally death

SCD is not a Heart Attack
Sudden cardiac death
Rhythm dysfunction
Prevents heart from delivering blood into
the arteries and systemic circulation
Myocardial infarction
Obstruction problem
Interruption in the supply of blood to
the heart
Heart muscle diesDeath

SCD causes
Albert CM. Circulation. 2003;107:2096-2101.

SCD arrhythmic causes
Most SCD are due to ventricular tachy-arrhythmias
Huikur H. N Engl J Med 2001; 345(20): 1473-82

Tachy-arrhythmiasVentricular TachycardiaAtrial Flutter
LVLVRVRV
RARA
LALA
LVLVRVRV
RARA
LALAOne extra Focus
LVLVRVRV
RARA
LALA
LVLVRVRV
RARA
LALA
Atrial Fibrillation Ventricular Fibrillation
Multiple Extra Foci

Fundamental difference
Atrial Flutter
Atrial Fibrillation
Ventricular Tachycardia
Ventricular Fibrillation
Not directly
Life threatening
Directly
Life threatening

Ventricular Arrhythmias
Sinus Rhythm
Fast Ventricular Tachycardia
Ventricular Arrhythmias start without warning !

Ventricular Arrhythmias
Ventricular fibrillation
Sinus rhythm
…Degenerate to a lethal rhythm...
unless a shock is delivered to restore sinus rhythm

Typical Sequence of SCD
Patient profile courtesy of M. Akhtar, M.D., Sinal-Samaritan Medical Center, Milwaukee, WL.
Has electrical foci so rapid that the heart turns into a twitching muscle with effectively no cardiac output
Within seconds the patient becomes unconscious; within minutes the patient dies

SCD survival depends on early defibrillation
An electrical shock may be delivered by:
an Automated External Defibrillator
(AED)
Time is crucial :
Each minute of delay reduces survival rates by about 10%
an Implantable Cardioverter Defibrillator
(ICD)

•EPIDEMIOLOGY •OF SCD
Any modification on the slide of the presentation are under the sole responsibility of his author

Incidence of SCD
1st cause of death across developed countries
1st cause of death across developed countries
SCD across Europe
USA 300/400.000 death/year Europe 350.000 death/year
SCD is a worldwide epidemic:
Myerburg RJ, et al. Heart disease : a text book of Cardiovascular Medecine, 6th edition; 2001 : 890-931


Size of the problem
1NASPE, May 20002American Heart Association 2000
3National Cancer Institute 2001
4National Transportation Safety Board 20005Center for Disease Control 20016NFPA, US Facts & Figures 2000

Incidence of SCD in specific populations
Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.

Survival rate after an Sudden Cardiac Arrest
Only 1 person in 20 usually survives an episode of SCD
The other 19 people die before reaching the hospital
American Heart Association. Heart Disease and Stroke Statistics. 2003 Update. Dallas, Texas: American Heart Association; 2002:3.

Two major risk factors for SCD
Huikur H. N Engl J Med 2001; 345(20): 1473-82
Underlying causes of fatal arrhymthmias

People with a prior SCD
People with a family history of SCD
People with history of renal dysfunction
People who have had a Myocardial Infarction (MI)
People with Congestive Heart Failure (CHF)
People with a Left Ventricular Ejection Fraction (LVEF) less than or equal to 35%
Who is at Risk of SCD?

SCD and post-MI
• People who have had a heart attack, have a sudden cardiac death rate that is 4-6 times that of the general population.
American Heart Association. Heart and Stroke Statistical – 2003 Update. Dallas, Tex.. American Heart Association. 2002

Risk of SCD in post-MI patientsMortality risk in contemporary post-MI patients with EF ≤ 30%
tends to increase as a function of time from last MI
Wilber D et al. Circulation 2004;109:1082-84

SCD and HF
• In people diagnosed with heart failure, sudden cardiac death occurs at 6-9 times the rate of the general population.
American Heart Association. Heart and Stroke Statistical – 2003 Update. Dallas, Tex.. American Heart Association. 2002

Risk of SCD: many HF patients concerned
SCD is More Prevalent in NYHA class II/III
The international steering committee. Rational, design, and organization of the Metoprolol CR/XL randomized intervention trail in heart failure(Merit-HF). Am J Cardiol 1997;80:54J-58J.

Reduced LVEF : an important risk factor
Maggioni AP. Circulation. 1993;87:312-322. *premature ventricular beat
*

LVEF related to SCD
0
1
2
3
4
5
6
7
8
0-30% 31-40% 41-50% >50%
Gorgels PMA. European Heart Journal. 2003;24:1204-1209.
7.5%
5.1%
2.8%
1.4%% o
f S
CD
vic
tim
s
LVEF

Emergency management of SCD
• Cardio Pulmonary Resuscitation (CPR)

Hands-Only CPR - No More Mouth-to-Mouth?Medical Author: Melissa Conrad Stöppler, MDMedical Editor: William C. Shiel, Jr., MD, FACP, FACR
In April, 2008, the American Heart Association (AHA) took steps to
simplify the process of helping victims of cardiac arrest by introducing "hands-only" CPR.
It is estimated that each year, around 310,000 Americans die of cardiac arrest that occurs at home or in a public place.

The Importance of CPR
Heart disease is the number 1 killer in the United States. Each year, almost 330,000 Americans die from heart disease. Half of these will die suddenly, outside of the hospital,
because their heart stops beating.
The most common cause of death from a heart attack in adults is a disturbance in the electrical rhythm of the heart called ventricular fibrillation.
Ventricular fibrillation can be treated, but it requires applying an electrical shock to the chest called defibrillation.
If a defibrillator is not readily available, brain death will occur in less than 10 minutes.

One way of buying time until a defibrillator becomes available is to provide artificial breathing and circulation by performing cardiopulmonary resuscitation, or CPR.
The earlier you give CPR to a person in cardiopulmonary arrest (no breathing, no heartbeat), the greater the chance of a successful resuscitation.
By performing CPR, you keep oxygenated blood flowing to the heart and brain until a defibrillator becomes available
Because up to 80% of all cardiac arrests occur in the home, you are most likely to perform CPR on a family member or loved one.
CPR is one link in what the American Heart Association calls the "chain of survival." The chain of survival is a series of actions that, when performed in
sequence, will give a person having a heart attack the greatest chance of survival


Chain of Survival

Timing is Everything
Time After the Onset of Attack
Survival Chances
With every minute Chances are reduced by 7-10%
Within 4-6 minutes Brain damage and permanent death start to occur
After 10 minutes Few attempts at resuscitation succeed
Early Access to Emergency Care must be provided by calling emergency Early CPR should be started and maintained until emergency medical services arrive. Early Defibrillation is the only one that can re-start the heart function of a person with
ventricular fibrillation (VF). Early Advanced Care, the final link, can then be administered as needed by EMS
personnel.

Type of Care for SCA Victims after Collapse Chance of Survival
No care after collapse 0%
No CPR and delayed defibrillation (after 10 minutes) 0-2%
CPR from a non-medical person (such as a bystander or family member) begun within 2 minutes, but delayed defibrillation
2-8%
CPR and defibrillation within 8 minutes 20%
CPR and defibrillation within 4 minutes; paramedic help within 8 minutes
43%
more than 70% of SCA cases occur at home, and another 10% to 15% occur at work
where the Chain is strong and when defibrillation occurs within the first few minutes of cardiac arrest, survival rates can approach 80% to 100%

People who survive sudden cardiac arrest have an excellent prognosis: 83% survive for at least one year, and 57% survive for five years or longer. In fact, when analyzed by age group, survival rates for SCA survivors are comparable to survival rates of people who have never had an event. Clearly, early intervention can offer years of productivity and fulfillment to victims of SCA

Early Access
Could you recognize the symptoms of SCA?
Unresponsiveness
Loss of consciousness Lack of pulse
Cessation of breathing
SCA is not the same as a heart attack

Early CPR
Cardiopulmonary resuscitation (CPR) is the second link in the Chain of Survival; it is the link that can buy life-saving time between the first link (Early
Access to Emergency Care) and the third link (Early Defibrillation

Please Note
INTUBATION and VENTILATION are not necessary during CPR- DoNOT waste initial few minutes in trying to intubate patient or calling an anaesthetist

Early Defibrillation
Although it is an important link in the Chain of Survival, CPR alone cannot fully resuscitate a person in SCA. Early defibrillation is the third and perhaps most significant link. Most SCA victims are in ventricular fibrillation (VF), an electrical malfunction of the heart that causes the heart to twitch irregularly. Defibrillation, the delivery of an electrical shock to the heart muscle, can restore normal heart function if it occurs within minutes of SCA onset. When CPR and defibrillation are provided within eight minutes of an episode, a person's chance of survival increases to 20%. 1 When these steps are provided within four minutes and a paramedic arrives within eight minutes, the likelihood of survival increases to over 40%.

Early Advanced Care
The fourth link in the Chain of Survival is advanced care. Paramedics and
other highly trained EMS personnel provide this care, which can include basic life support, defibrillation, administration of cardiac drugs, and the insertion
of endotracheal breathing tubes. This type of advanced care can help the heart in VF respond to defibrillation and maintain a normal rhythm after
successful defibrillation.

•REVIEW OF DRUG AND ICD TRIALS
Any modification on the slide of the presentation are under the sole responsibility of his author

Long Term Management of SCD

Major VT/SCD Drug Trials to Date
CAST-I (1991) CHF-STAT (1992) ESVEM (1993)GESICA (1994)SWORD (1996)EMIAT (1997)CAMIAT (1997)

Summary of Drug TrialsTrial Patients Trial Design Result
CAST-I1 1498 Encainide, Flecainide / Placebo
Terminated due to excessive death in treatment arm
CHF-STAT2 674 Amiodarone / Placebo
No change in overall mortality
SWORD3 546 d-Sotalol / Placebo Terminated due to excessive death in treatment arm
ESVEM4 486 EPS-guided / Holter-guided
Mortality high in both arms
EMIAT5 1500 Amiodarone / Placebo
No change in overall mortality
CAMIAT6 1200 Amiodarone / Placebo
No change in overall mortality
1 Echt, et al. N Engl J Med. 1991;324:781–8.2 Singh, et al. N Engl J Med. 1995;333:77–82 (supported by Sanofi & Wyeth).3 Waldo A.L. The Lancet; 1996;348:7–12. (supported by Bristol-Myers Squibb).
4 Mason J.W. N Engl J Med. 1993;329(7):452–8. (Supported by Bristol-Myers Squibb, Knoll Pharmaceutical, Boehringer-Ingelheim, Parke-Davis, and Ciba-Geigy). 5 Julian D.G. The Lancet. 1997;349:667–74.(Supported by Sanofi)6 Cairns J.A. The Lancet. 1997;349:675–82.

Summary of Drug Trials Most anti-arrhythmic drugs worsen mortality Amiodarone is not effective in improving SCD
mortality and carries significant toxicity In prior and post MI patients with LVD, anti-
arrhythmic drugs do not effectively reduce mortality and they can actually decrease survival
1 Echt, et al. N Engl J Med. 1991;324:781–8.2 Singh, et al. N Engl J Med. 1995;333:77–82.3 Waldo A.L. The Lancet; 1996;348:7–12.
4 Mason J.W. N Engl J Med. 1993;329(7):452–8.5 Julian D.G. The Lancet. 1997;349:667–74.6 Cairns J.A. The Lancet. 1997;349:675–82.

Secondary Prevention
An event has already occurred: Survivors of ventricular fibrillation or Sustained ventricular tachycardia
Connolly SH et al: Eur Heart J. 2000 Dec;21(24):2071-8.
USA 300/400.000 death/y.Europe 350.000 death/y.
Those patients already have demonstrated that they are at risk
Only 10% - 20% survive

CASH: 1986 – 1997 (1)
• 8 centers / 191 patients, Follow-up 4.48 years
CIDS: 1990 – 1997 (2)
• 24 centers / 659 patients, Follow-up 2.96 years
AVID: 1993 – 1997 (3)
• 62 centers / 1016 patients, Follow-up 1.51 years• Decreasing total study duration also reflects therapy
acceptance. Transvenous systems only became available in the early
nineties.
ICD Trials : Secondary Prevention
1- Kuck K. Circulation. 2000;102:748-754. Supported by Guidant, Astra
2- Connolly SJ. Circulation. 2000;101:1297-1302. Supported by MRC Canada, Wyeth-Ayerst3- The AVID Investigators. N Engl J Med. 1997;337(22):1576-1583. Supported by NHLBI

CASH
Objective :
Evaluate the effectiveness of ICD therapy (n = 99) versus Metoprolol (n = 97), Amiodarone (n = 92), and Propafenone (n = 58) in SCA survivors.
Inclusion Criteria :
Cardiac arrest survivor with documented VT
Kuck K. Circulation. 2000;102:748-754.

CASH24% Mortality reduction with ICD
Circulation. 2000;102:748-754

CIDS
Objective:
Evaluate the effectiveness of ICD therapy (n = 328) versus amiodarone (n = 331) in patients with life-threatening ventricular tachyarrhythmias
Inclusion Criteria:
Documented VFCardiac arrestSustained VT with hemodynamic compromise
Connolly SJ. Circulation. 2000;101:1297-1302.

CIDS20% Mortality reduction with ICD
Circulation. 2000;101:1297-1302

AVID Objective:
To evaluate the effectiveness of ICD therapy (n = 507) in reduction of total mortality, when compared with amiodarone (n = 435) or sotalol (n = 74) in patients resuscitated from SCD who are at very high risk of mortality from arrhythmic causes
Inclusion Criteria:
Primary VF, orSustained VT with syncope, orSustained VT and LVEF < 40% with hypotension/chest
pain or presyncopeThe AVID Investigators. N Engl J Med. 1997;337(22):1576-1583.

AVIDMortality reduction ICD vs antiarrhythmic
drug
NEJM 1997; 337:1576-1583
Mortality reduction with ICD
1 year: 39%
2 years: 27%
3 years: 31%

Secondary Prevention Trialsoutcomes
* Non-significant results.1 The AVID Investigators. N Engl J Med. 1997;337:1576-1583.2 Kuck K. Circulation. 2000;102:748-754.3 Connolly S. Circulation. 2000;101:1297-1302.
0
20
40
60
80
AVID CASH CIDS
Overall Death
Arrhythmic Death
1 2 3
31%
56%
23%*
58%
20%*
33%
% M
ort
alit
y R
edu
cti
on
w/
ICD
Rx
3 Years 4.75 Years 3 Years
Reduction in Mortality with ICD Therapy

Secondary Prevention Trials Conclusions
In resuscitated VT/VF patients :
no benefit in survival with amiodarone.other antiarrhythmic drugs are ineffective
or potentially harmful
CASH / CIDS / AVID have shown that ICD therapy is effective in reducing overall mortality and arrhythmic death in resuscitated VT/VF patients.

ICD Trials : Primary prevention MADIT (1)
CABG-Patch (2)
CAT (1)
MUSTT (3)
AMIOVIRT (1)
MADIT II (1)
SCD-HeFT (4)
DINAMIT (5)
DEFINITE (5)
1- supported by Guidant2- supported by Guidant & NHLBI3- supported by Guidant, Medtronic, StJude/Ventritex et al.4- Supported by NIH, Medtronic, Wyeth-Ayerst et al.5- Supported by St Jude

MADIT MADIT: 1990 – 1995
Multicenter RCT* of ICD vs. Antiarrhythmic drugs as conventional therapy
32 centers/196 patients, Follow-up 27 months Inclusion criteria: MI ≥ 3 weeks before entry, EF ≤ 35 %Additional risk factors: asymptomatic NSVT unrelated to
an acute MI with inducible VT not suppressed after procainamide
Outcomes:
16% mortality in ICD vs. 39% in conventional therapy. Absolute risk reduction 23%.
*Randomized Clinical TrialMoss AJ et al. NEJM 1996;335:1933-40

CABG CABG: 1990 – 1995
Multicenter RCT of ICD vs. Antiarrhythmic drugs as conventional therapy
37 centers/1055 patients, Follow-up 32 months Inclusion criteria: CABG, EF ≤ 35 % Additional risk factors: Abnormal SAECG (signal averaged
ECG)
Outcomes:23% mortality in ICD vs. 21% in control patients. No difference in all cause mortality.
Issues: Epicardial leads. CABG surgery has a strong effect on mortality, that could have confounded the overall results.
Bigger et al. NEJM 1997;337:1569-75

CAT
CAT: 1991 – 1997 Multicenter RCT of ICD vs. Antiarrhythmic drugs as
conventional therapy 15 centers/104 patients, Follow-up 23 months Inclusion criteria: Symptomatic recent onset DCM, LVEF ≤ 30
%, NYHA II or III Additional risk factors: Not specified
Outcomes:
Mortality 8% in ICD vs. 7% in control (not significant! P = 0.54) Issues: Low baseline risk for death due to improved therapy
options. Early termination after 1 year
Bansch, Kuck et al. Circulation 2002;105:1453-901458.

MUSTT MUSTT: 1989 – 1998
Multicenter ICD VS. Anitiarrythmic Drug Treatment in Post-MI Patients 85 centers/704 patients, Follow-up 39 months Inclusion criteria: Coronary artery disease (CAD), Asymptomatic,
unsustained VT, LVEF ≤ 40%, inducible VT on EP testing, history of MI in 95%
Outcomes:For post-MI patients with EF < 40%, and asymptomatic NSVT:
• 44% death rate in Registry Patients (non-inducible VT) • ICD therapy significantly reduced the incidence of death in the
patients with inducible VT:Arrhythmic death or cardiac arrest (73% - 76%
reduction)Overall mortality (55% - 60% reduction)
• EP-guided pharmacologic antiarrhythmic therapy provides no survival benefit
Buxton AE et al. NEJM 1999;331:1882-90.

AMIOVIRT AMIOVIRT: 1996 – 2000
Multicenter RCT of ICD vs. Antiarrhythmic drugs as conventional therapy
10 centers/101 patients, Follow-up 24 months Inclusion criteria: NIDCM, EF ≤ 35%, asymptomatic
NSVT, NYHA class I to IIIAdditional risk factors: NSVTOutcomes:
Survival 88% in ICD vs. 87% with Amiodarone. Issues: Low baseline risk for death due to
improved therapy. Early termination after 3 years due to low 3 year mortality in both arms.

MADIT II
MADIT II: 1997 – 2001
Multicenter RCT of ICD vs. optimized medical therapy 76 centers/1232 patients, Follow-up 20 months Inclusion criteria: Prior MI, EF ≤ 30% Additional risk factors: Not specified
Outcomes: 14.2% in ICD vs. 19.8 in optimized group. Absolute risk reduction 5.6%. p=0.007
Moss JA et al. NEJM 2002;346:887-83

SCD-HeFT SCD-HeFT: 1997 – 2001
Multicenter RCT of ICD vs. optimized medical therapy vs optimzed medical therapy with amiodarone
10 centers/2521 patients, Follow-up 48 months Inclusion criteria: Ischemic and non ischemic
cardiomyopathy, EF ≤ 35 % Additional risk factors: Not specifiedOutcomes:
22% mortality in ICD group, 28% in amiodarone, 29% in control. 7% of absolute risk reduction ICD vs control. p=0.007
Bardy GH et al. NEJM 2002;346:877-83

DINAMIT
DINAMIT: 1998 – 2002
Multicenter RCT of ICD vs. optimized medical therapy 73 centers/674 patients, Follow-up 30 months Inclusion criteria: 6 to 40 days after MI, LVEF ≤ 35% Additional risk factors: depressed HRV or elevated average
heart rate on 24 hour holter
Outcomes: 7.5% mortality in ICD vs. 6.9% in non ICD group, not significant.
Issues: Therapy with strong effects on mortality, that could have confounded the overall results.
Hohnloser Kuck, Connolly et al. NEJM 2004;351:2481-88

DEFINITE
DEFINITE: 1998 – 2002
Multicenter RCT of ICD vs. optimized medical therapy 47 centers/458 patients, Follow-up 29 months Inclusion criteria: NIDCM, EF < 36 % Additional risk factors: NSVT or frequent premature
complexes Outcomes:
8.1% overall mortality in ICD vs. 13.8% in optimized therapy. Absolute risk reduction 5.7%, but not significant (p=0.6). The risk for sudden death from arrhythmia was significantly reduced (p=0.006).
Kadish, Levine et al. NEJM 2004;350:2151-58

Indications for ICD Therapy

Implantable Cardioverter-Defibrillators
ICD therapy is indicated in patients who are survivors of cardiac arrest due to ventricular fibrillation or hemodynamically unstable sustained VT after evaluation to define the cause of the event and to exclude any completely reversible causes.
ICD therapy is indicated in patients with structural heart disease and spontaneous sustained VT, whether hemodynamically stable or unstable.
ICD therapy is indicated in patients with syncope of undetermined origin with clinically relevant, hemodynamically significant sustained VT or VF induced at electrophysiological study.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.

ICD therapy is indicated in patients with LVEF less than or equal to 35% due to prior MI who are at least 40 days post-MI and are in NYHA functional Class II or III.
ICD therapy is indicated in patients with nonischemic DCM who have an LVEF less than or equal to 35% and who are in NYHA functional Class II or III.
ICD therapy is indicated in patients with LV dysfunction due to prior MI who are at least 40 days post-MI, have an LVEF less than or equal to 30%, and are in NYHA functional Class I.
ICD therapy is indicated in patients with nonsustained VT due to prior MI, LVEF less than or equal to 40%, and inducible VF or sustained VT at electrophysiological study.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators

ICD implantation is reasonable for patients with unexplained syncope, significant LV dysfunction, and nonischemic DCM.
ICD implantation is reasonable for patients with sustained VT and normal or near-normal ventricular function.
ICD implantation is reasonable for patients with HCM who have 1 or more major† risk factors for SCD.
ICD implantation is reasonable for the prevention of SCD in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) who have 1 or more risk factors for SCD.
ICD implantation is reasonable to reduce SCD in patients with long-QT syndrome who are experiencing syncope and/or VT while receiving beta blockers.
I IIaIIbIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
† See Section 3.2.4, “Hypertrophic Cardiomyopathy,” in the full-text guidelines for definition of major risk factors.
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
Implantable Cardioverter-Defibrillators

ICD implantation is reasonable for nonhospitalized patients awaiting transplantation.
ICD implantation is reasonable for patients with Brugada syndrome who have had syncope.
ICD implantation is reasonable for patients with Brugada syndrome who have documented VT that has not resulted in cardiac arrest.
ICD implantation is reasonable for patients with catecholaminergic polymorphic VT who have syncope and/or documented sustained VT while receiving beta blockers.
ICD implantation is reasonable for patients with cardiac sarcoidosis, giant cell myocarditis, or Chagas disease.
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators

ICD therapy may be considered in patients with nonischemic heart disease who have an LVEF of less than or equal to 35% and who are in NYHA functional Class I.
ICD therapy may be considered for patients with long-QT syndrome and risk factors for SCD.
ICD therapy may be considered in patients with syncope and advanced structural heart disease in whom thorough invasive and noninvasive investigations have failed to define a cause.
ICD therapy may be considered in patients with a familial cardiomyopathy associated with sudden death.
ICD therapy may be considered in patients with LV noncompaction.
III IIaIIaIIa IIbIIbIIbIIIIIIIIIIII IIaIIaIIa IIbIIbIIbIIIIIIIIIIII IIaIIaIIa IIbIIbIIbIIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators

ICD therapy is not indicated for patients who do not have a reasonable expectation of survival with an acceptable functional status for at least 1 year, even if they meet ICD implantation criteria specified in the Class I, IIa, and IIb recommendations above.
ICD therapy is not indicated for patients with incessant VT or VF.
ICD therapy is not indicated in patients with significant psychiatric illnesses that may be aggravated by device implantation or that may preclude systematic follow-up.
ICD therapy is not indicated for NYHA Class IV patients with drug-refractory congestive heart failure who are not candidates for cardiac transplantation or cardiac resynchronization therapy defibrillators (CRT-D).
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators

ICD therapy is not indicated for syncope of undetermined cause in a patient without inducible ventricular tachyarrhythmias and without structural heart disease.
ICD therapy is not indicated when VF or VT is amenable to surgical or catheter ablation (e.g., atrial arrhythmias associated with the Wolff-Parkinson-White syndrome, RV or LV outflow tract VT, idiopathic VT, or fascicular VT in the absence of structural heart disease).
ICD therapy is not indicated for patients with ventricular tachyarrhythmias due to a completely reversible disorder in the absence of structural heart disease (e.g., electrolyte imbalance, drugs, or trauma).
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators

ICDs in Pediatric Patients and Patients With Congenital Heart Disease
ICD implantation is indicated in the survivor of cardiac arrest after evaluation to define the cause of the event and exclusion of any reversible causes.
ICD implantation is indicated for patients with symptomatic sustained VT in association with congenital heart disease who have undergone hemodynamic and electrophysiological evaluation. Catheter ablation or surgical repair may offer possible alternatives in carefully selected patients.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.

ICDs in Pediatric Patients and Patients With Congenital Heart Disease
ICD implantation is reasonable for patients with congenital heart disease with recurrent syncope of undetermined origin in the presence of either ventricular dysfunction or inducible ventricular arrhythmias at electrophysiological study.
ICD implantation may be considered for patients with recurrent syncope associated with complex congenital heart disease and advanced systemic ventricular dysfunction when thorough invasive and noninvasive investigations have failed to define a cause.
All Class III recommendations found in Section 3 of the full-text guidelines, “Indications for Implantable Cardioverter-Defibrillator Therapy,” apply to pediatric patients and patients with congenital heart disease, and ICD implantation is not indicated in these patient populations.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.

Major Implantable Cardioverter-Defibrillator Trials for Prevention of
Sudden Cardiac DeathTrial Year Patients
(n)LVEF Additional Study
FeaturesHazardRatio*
95% CI p
MADIT I 1996 196 < 35% NSVT and EP+ 0.46 (0.26-0.82) p=0.009
MADIT II 2002 1232 < 30% Prior MI 0.69 (0.51-0.93) p=0.016
CABG-Patch 1997 900 < 36% +SAECG and CABG 1.07 (0.81-1.42) p=0.63
DEFINITE 2004 485 < 35% NICM, PVCs or NSVT 0.65 (0.40-1.06) p=0.08
DINAMIT 2004 674 < 35% 6-40 days post-MI and Impaired HRV
1.08 (0.76-1.55) p=0.66
SCD-HeFT 2006 1676 < 35% Prior MI of NICM 0.77 (0.62-0.96) p=0.007
AVID 1997 1016 Prior cardiac arrest
NA 0.62 (0.43-0.82) NS
CASH† 2000 191 Prior cardiac arrest
NA 0.766 ‡ 1-sided p=0.081
CIDS 2000 659 Prior cardiac arrest, syncope
NA 0.82 (0.60-1.1) NS
* Hazard ratios for death from any cause in the ICD group compared with the non-ICD group. Includes only ICD and amiodarone patients from CASH.‡CI Upper Bound 1.112 CI indicates Confidence Interval, NS = Not statistically significant, NSVT = nonsustained ventricular tachycardia, SAECG = signal-averaged electrocardiogram.
Epstein A, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. J Am Coll Cardiol 2008; 51:e1–62. Table 5.

Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure
(COMPANION) Trial
• 1520 patients with NYHA Class III or IV HF, ischemic cardiomyopathy (ICM) or nonischemic cardiomyopathy (NICM) and QRS ≥ 120 ms
• Randomized 1:2:2 to optimal pharmacological therapy (OPT) alone or in combination with cardiac resynchronization therapy with either a pacemaker (CRT-P) or pacemaker-defibrillator (CRT-D)
• Both device arms significantly ↓ combined risk of all-cause hospitalization and all-cause mortality by ~20% compared with OPT
• CRT-D ↓ mortality by 36% compared with OPT (p=0.003)• Insufficient evidence to conclude that CRT-P inferior to
CRT-DBristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med 2004;350:2140-50.

Implantable Cardioverter-Defibrillators and Prevention of Sudden Cardiac Death in
Hypertrophic Cardiomyopathy
• Multicenter registry study of implanted ICDs in 506 unrelated patients with HCM @ high risk for SCD (family hx of SCD, [septal thickness ≥ 30 mm], NSVT, syncope)
• Mean patient age 42 years (SD=17) and 87% had no or only mildly limiting symptoms
• Appropriate ICD discharge rates were 11% per year for 2o prevention and 4% per year for 1o prevention
• For 1o prevention, 35% of patients with appropriate ICD interventions had undergone implantation for only 1 risk factor
Maron BJ, Spirito P, Shen WK, et al. Implantable cardioverter-defibrillators and prevention of sudden cardiac death in hypertrophic cardiomyopathy. JAMA 2007;298:405-12.

Multicenter Automatic Defibrillator Implantation Trial II (MADIT II)
• 1232 patients ≥ 1 month post-MI and LVEF ≤ 30%• Randomized to ICD (n=742) or medical therapy (n=490)• No spontaneous or induced arrhythmia required for
enrollment• 6% absolute and 31% relative risk ↓ in all-cause mortality
with ICD therapy (p=0.016)
Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877-83.

Sudden Death in Heart Failure (SCD-HeFT) Trial
• 2521 patients with NYHA Class II or III HF, ICM, or NICM and LVEF ≤ 35%
• Randomized to 1) conventional rx for HF + placebo; 2) conventional rx + amiodarone; or 3) conventional rx + conservatively programmed shock-only single lead ICD
• No survival benefit for amiodarone• 23% ↓ in overall mortality with ICD therapy• Absolute ↓ in mortality of 7.2% after 5 y in the overall
population
Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005;352:225-37.

Defibrillator in Acute Myocardial Infarction (DINAMIT) Trial
• 674 patients 6 to 40 days post-MI with LVEF ≤ 35% and impaired cardiac autonomic function
• Randomized to ICD therapy (n=332) or no ICD therapy (n=342)
• Arrhythmic death ↓ in ICD group, but ↑ in nonarrhythmic death (6.1% per year vs. 3.5% per year, HR 1.75 (95% CI 1.11 to 2.76; p=0.016)
• No difference in total mortality
Hohnloser SH, Kuck KH, Dorian P, et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med 2004;351:2481-8.

Defibrillators in Nonischemic Cardiomyopathy Treatment Evaluation
(DEFINITE) Trial
• 458 patients with NYHA Class I to III, NICM, LVEF ≤ 35% and premature ventricular contractions (> 10/h) or NSVT
• Randomized to standard medical rx alone or in combination with single-chamber ICD
• Strong trend toward ↓ all-cause mortality with ICD therapy, although not statistically significant (p=0.08)
Kadish A, Dyer A, Daubert JP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med 2004;350:2151-8.

Notable Changes in 2008 ACC/AHA/HRS Guidelines
1. ICD recommendations are combined into a single list because of overlap between primary and secondary indications.
2. Primary prevention ICD indications in nonischemic cardiomyopathy are clarified using data from SCD-HeFT (i.e., ischemic and nonischemic cardiomyopathies and LVEF ≤35%, NYHA II-III) for support.
3. Indications for ICD therapy in inherited arrhythmia syndromes and selected nonischemic cardiomyopathies are listed.
4. MADIT II indication (i.e., ischemic cardiomypathy and LVEF ≤30%, NYHA I) is now Class I, elevated from Class IIa.
5. EF criteria for primary prevention ICD indications are based on entry criteria for trials on which the recommendations are based.
6. Emphasized primary SCD prevention ICD recommendations apply only to patients receiving optimal medical therapy and reasonable expectation of survival with good functional capacity for >1 year.
7. Independent risk assessment preceding ICD implantation is emphasized, including consideration of patient preference.
8. Optimization of pacemaker programming to minimize unneeded RV pacing is encouraged.
9. Pacemaker insertion is discouraged for asymptomatic bradycardia, particularly at night.
10. A section has been added that addresses ICD and pacemaker programming at end of life.

Conclusion
• Identifying SCD is prime importance• Correctible causes like dysselectrolytemia,
proarrythmia to be corrected promptly• AMI and myocarditis are two leading cause of
SCD• Knowledge of CPR is must for every medical
professional including skills of Defibillation• Defibrillators should be made available every
where in hospital including wards• ICD is advisable in secondary and primary
prevention

Thank you very much