Stone Diseases in Algeria: URS Replaces Slowly Open Surgery H. KOUICEM, Algeria Algerian Association...
22
Stone Diseases in Algeria: URS Replaces Slowly Open Surgery H. KOUICEM, Algeria Algerian Association of Urology
-
Upload
vincent-jacobs -
Category
Documents
-
view
219 -
download
1
Transcript of Stone Diseases in Algeria: URS Replaces Slowly Open Surgery H. KOUICEM, Algeria Algerian Association...

Stone Diseases in Algeria:URS Replaces Slowly Open
Surgery
H. KOUICEM, Algeria
Algerian Association of Urology

In Algeria, urolithiasis is a wide-spread health problem. Until recently, stone diseases were almost exclusively treated via open surgery, due to financial restrictions leading to a lack of minimally invasive technological infrastructure. Only recently, ureterorenoscopy and LASER stone fragmentation are introduced.
Introduction
Open Surgery Ureteroscopy

OPEN SURGERY
Therapeutic Options
available Until 2014
Roboflex Avicenna 2014
SWL
PCNL
Davancci Robot
MET
Laparoscopy
Ureteroscopy

Study Cases
A case series of 6 large ureter stones 1-2 cm are treated through a modern approach and would have otherwise undergone open surgery.
The underneath mentioned cases reflect the endourological approaches adopted even going back to OPEN SURGERY though abrasive and morbid.

Case One
DiagnosisFemale, 36 Years
L P U stone: 14 mm
Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?
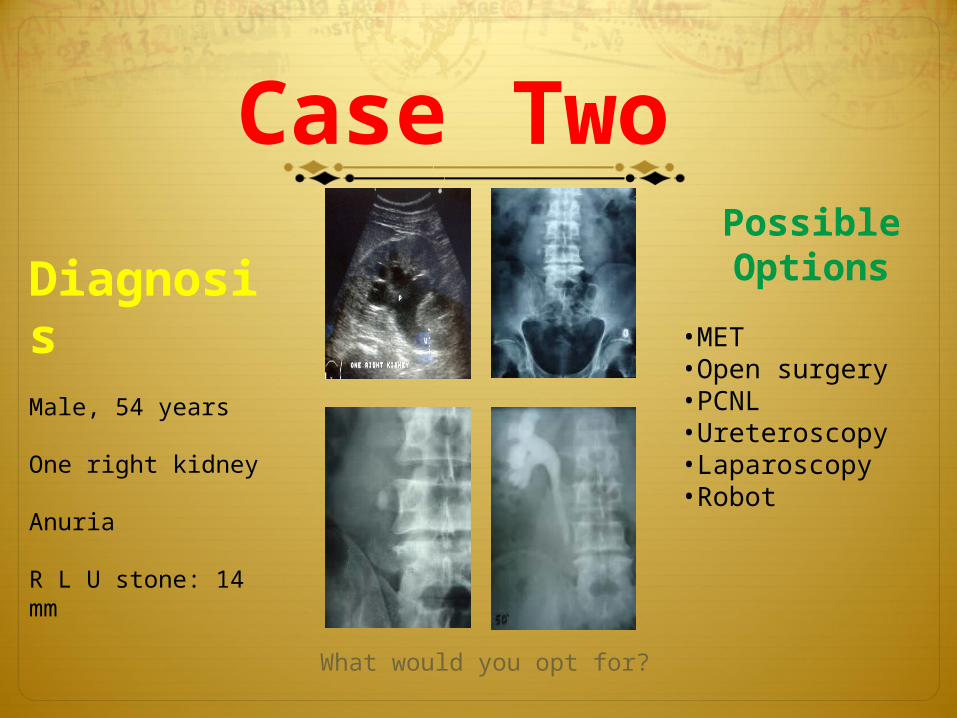
DiagnosisMale, 54 years
One right kidney
Anuria
R L U stone: 14 mm
Case Two Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?

Case
ThreeDiagnosisFemale, 35 years
L P U stone: 15 mm
Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?

Case
FourDiagnosisMale, 47 years
R P U stone: 10 mm MET failed
Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?

Case
Five
DiagnosisMale, 44 years
L L U stone: 22 mm
Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?

Case
Six
DiagnosisFemale, 56 years
R K stone : 20 mm
Possible Options
•MET•Open surgery•PCNL•Ureteroscopy•Laparoscopy•Robot
What would you opt for?

EAU Recommendat
ions
EAU Algorithm 2014
Recommendations for MET LE GR
For MET, α-blockers are recommended 1a A
Patients should be counselled about the attendant risks of MET, including associated drug side effects, and should be informed that it is administered off-label ϯ**
A*
Patients who elect for an attempt at spontaneous passage or MET, should have well-controlled pain, no clinical evidence of sepsis, and adequate renal functional reserve.
A
Patients should be followed once between 1 and 14 days to monitor stone position and be assessed for hydronephrosis.
4 A*
Stone location and size First choice Second choice
Proximal ureter < 10 mm SWL
Proximal ureter > 10 mm URS (retrograde or antegrade or SWL
Distal ureter < 10 mm URS or SWL
Distal ureter > 10 mm URS SWL
Recommended treatment option (if indicated for active stone removal) (GR: A*)

EAU Guidelines 2014
Kidney stones • Complex stone burden
• Failure of SWL, PNL, or ureteroscopic procedure
• Intrarenal anatomical abnormalities: infundibular stenosis; stone in the calyceal diverticulum (particularly in an anterior calyx); obstruction of the ureteropelvic junction; and stricture if endourologic procedures have failed or are not promising
• Morbid obesity
• Skeletal deformity, contractures and fixed deformities of hips and legs
• Comorbidity
• Concomitant open surgery
• Non-functioning in lower pole (partial nephrectomy), non-functioning kidney (nephrectomy)
• Patient choice (after failed minimally invasive procedures, a single procedure avoiding the risk of multiple PNL procedures might be preferred by the case)
• Stone in an ectopic kidney where percutaneous access and SWL may be difficult or impossible.
• For the paediatric population, the same considerations apply as for adults.
Indications for open surgery

Fallouts
Sometimes, though financial resources and technical platforms are available, the urologist is obliged to opt for a decision that does NOT logically shadow the EAU Recommendations!!!

Case One
URS scheduled. Spontaneous stone passage through MET after 3 weeks.

Case TwoSemi-rigid ureteroscopy. Fragmentation with ballistic lithotripter.
Post-OP JJ.

Case ThreeSemi-rigid ureteroscopy. Fragmentation with ballistic lithotripter.
Post-OP JJ.

Cases Four & Five
Case Four
Case FiveFragmentation with semi-rigid ureteroscope LASER.
Post-OP JJ.

Case SixThe stone was found embedded in the ureteropelvic
junction. Up to 50% of the stone was fragmented with flexible LASER. Cloudy urines observed. JJ placed. Treatment completed using delayed SWL.

Comments
Though MET and Open Surgery are still practiced due to the restricted financial resources of patients as well as the availability and the limits of the technical platforms;
URS is gaining ground slowly!
What are the appropriate treatment choices to be recommended?
All in All

Open surgery has been the main if not the only treatment for stones in Algeria. Ureteroscopy has opened a path towards minimally invasive surgery in our country:
It has re-instated confidence in the use of conservative treatments as a first option.
Algeria has embarked towards a path to negligibly aggressive modern stone treatment.
The successful management of all aspects of stones treatment requires both competence and equipments.
The Algerian urologist is obliged to find the best solution to relieve his patients’ sufferings; nevertheless reality is rather problematic!
Conclusions