Steroid-Induced Diabetes Mellitus and Related Risk Factors in Patients with Neurologic Diseases
7
Steroid-Induced Diabetes Mellitus and Related Risk Factors in Patients with Neurologic Diseases Takuya Iwamoto, M.S., Yoshiyuki Kagawa, Ph.D., Yutaka Naito, M.D., Shigeki Kuzuhara, M.D., and Michio Kojima, Ph.D. Study Objective. To determine the frequency of steroid-induced diabetes mellitus (SDM) and the related risk factors in patients with neurologic diseases who receive high doses of steroids. Design. Retrospective chart review. Setting. Neurology ward of a university-affiliated hospital. Patients. Twenty-five patients with neurologic diseases who received prednisolone 30–60 mg/day orally after breakfast for more than 2 weeks. Measurements and Main Results. Plasma glucose concentrations were determined immediately before and 2 hours after each meal. Steroid- induced diabetes mellitus was diagnosed if the patient had either a fasting glucose concentration of 126 mg/dl or greater, or a random glucose concentration of 200 mg/dl or greater. The patients were divided into two groups on the basis of whether SDM had developed (13 patients) or not (12 patients). Ages, body mass indexes, cumulative total doses and daily doses of prednisolone, duration of therapy, and serum cholesterol and triglyceride concentrations were compared between the groups. Thirteen of the 25 patients were identified with SDM, and all of them had plasma glucose concentrations of 200 mg/dl or greater 2 hours after lunch. Mean age (59.1 ± 10.2 yrs) and cholesterol concentration after prednisolone treatment (226.8 ± 36.4 mg/dl) in the SDM group were significantly higher than those values in the non-SDM group (41.3 ± 18.0 yrs and 188.1 ± 27.2 mg/dl, respectively, p<0.01). Conclusions. A close relationship among postprandial hyperglycemia, advanced age, and hypercholesterolemia is a characteristic of SDM in patients with neurologic diseases. Therefore, monitoring the plasma glucose concentration 2 hours after lunch may be useful to detect SDM in these patients. Key Words: diabetes mellitus, steroid dosages, neurologic diseases, risk factors. (Pharmacotherapy 2004;24(4):508–514) Steroids have been known to inhibit the production of cytokines concerned with the development of inflammatory foci. 1 Steroids also prevent the production of metalloprotease, which enables inflammatory cells to break down the blood-brain barrier. 2, 3 Through these pharmacologic actions, steroids have been widely used in the treatment of neurologic diseases such as From the Departments of Pharmacy (Mr. Iwamoto and Drs. Kagawa and Kojima) and Neurology (Drs. Naito and Kuzuhara), Mie University Hospital, Mie, Japan. Presented in part at a meeting of the 19th Congress of the Federation of Asian Pharmaceutical Associations, Seoul, Korea, October 7, 2002. Address reprint requests to Takuya Iwamoto, Department of Pharmacy, Mie University Hospital, 2-174 Edobashi, Tsu, Mie 514-8507, Japan; e-mail: [email protected] u.ac.jp.
-
Upload
takuya-iwamoto -
Category
Documents
-
view
213 -
download
1
Transcript of Steroid-Induced Diabetes Mellitus and Related Risk Factors in Patients with Neurologic Diseases

Steroid-Induced Diabetes Mellitus and Related Risk Factors in Patients with Neurologic Diseases
Takuya Iwamoto, M.S., Yoshiyuki Kagawa, Ph.D., Yutaka Naito, M.D., Shigeki Kuzuhara, M.D., and Michio Kojima, Ph.D.
Study Objective. To determine the frequency of steroid-induced diabetesmellitus (SDM) and the related risk factors in patients with neurologicdiseases who receive high doses of steroids.
Design. Retrospective chart review.Setting. Neurology ward of a university-affiliated hospital.Patients. Twenty-five patients with neurologic diseases who received
prednisolone 30–60 mg/day orally after breakfast for more than 2 weeks.Measurements and Main Results. Plasma glucose concentrations were
determined immediately before and 2 hours after each meal. Steroid-induced diabetes mellitus was diagnosed if the patient had either a fastingglucose concentration of 126 mg/dl or greater, or a random glucoseconcentration of 200 mg/dl or greater. The patients were divided into twogroups on the basis of whether SDM had developed (13 patients) or not (12patients). Ages, body mass indexes, cumulative total doses and daily dosesof prednisolone, duration of therapy, and serum cholesterol and triglycerideconcentrations were compared between the groups. Thirteen of the 25patients were identified with SDM, and all of them had plasma glucoseconcentrations of 200 mg/dl or greater 2 hours after lunch. Mean age (59.1± 10.2 yrs) and cholesterol concentration after prednisolone treatment(226.8 ± 36.4 mg/dl) in the SDM group were significantly higher than thosevalues in the non-SDM group (41.3 ± 18.0 yrs and 188.1 ± 27.2 mg/dl,respectively, p<0.01).
Conclusions. A close relationship among postprandial hyperglycemia,advanced age, and hypercholesterolemia is a characteristic of SDM inpatients with neurologic diseases. Therefore, monitoring the plasmaglucose concentration 2 hours after lunch may be useful to detect SDM inthese patients.
Key Words: diabetes mellitus, steroid dosages, neurologic diseases, riskfactors.
(Pharmacotherapy 2004;24(4):508–514)
Steroids have been known to inhibit theproduction of cytokines concerned with thedevelopment of inflammatory foci.1 Steroids alsoprevent the production of metalloprotease, whichenables inflammatory cells to break down theblood-brain barrier.2, 3 Through these pharmacologicactions, steroids have been widely used in thetreatment of neurologic diseases such as
From the Departments of Pharmacy (Mr. Iwamoto andDrs. Kagawa and Kojima) and Neurology (Drs. Naito andKuzuhara), Mie University Hospital, Mie, Japan.
Presented in part at a meeting of the 19th Congress of theFederation of Asian Pharmaceutical Associations, Seoul,Korea, October 7, 2002.
Address reprint requests to Takuya Iwamoto, Departmentof Pharmacy, Mie University Hospital, 2-174 Edobashi, Tsu,Mie 514-8507, Japan; e-mail: [email protected].

STEROID-INDUCED DIABETES IN PATIENTS WITH NEUROLOGIC DISEASES Iwamoto et al
myasthenia gravis, chronic inflammatorydemyelinating polyneuropathy, and multiplesclerosis. Patients with neurologic diseases oftenreceive high doses of steroids for years. Thesesteroids usually are administered once/day afterbreakfast so as to fit their blood concentrations tothe circadian rhythm levels of intrinsic steroidhormones.
An excess of steroids impairs the suppressionof glucose production and stimulation of glucoseutilization, which might cause diabetes mellitusor aggravate preexistent diabetes.4, 5 According tothese mechanisms, abnormal glucose metabolisminduced by steroids may reflect both fasting andpostprandial hyperglycemia. The report thatperipheral glucose metabolism was impaired inpatients with myotonic dystrophy6 suggests thatglucose utilization is likely to decrease in patientswith neuromuscular disorders. Diabetes mellitusis defined not only by fasting plasma glucoseconcentrations, but also by random glucoseconcentrations.7 The Diabetes Epidemiology:Collaborative Analysis of Diagnostic Criteria inAsia study in Japan demonstrated that more than70% of diabetes mellitus cases were diagnosed
based on postprandial hyperglycemia.8 It waspreviously reported that when only fastingglucose concentrations were monitored to detectsteroid-induced diabetes mellitus (SDM), thefrequency of SDM was 46% in renal transplantrecipients who received high-dose steroidregimens.9 However, if the plasma glucoseconcentrations after a meal also are monitored inthis patient population, the frequency of SDMmay be higher than that reported. To ourknowledge, few reports have investigated thepostprandial plasma glucose concentrations inpatients receiving high doses of steroids.
In this study, we monitored the daily plasmaglucose concentrations and estimated thefrequency of SDM in patients with neurologicdiseases who received high doses of steroids.Furthermore, we investigated the risk factors forSDM in these patients.
Methods
Subjects
The records of 25 patients (age range 19–75yrs) in the neurologic ward of Mie University
509
Table 1. Patient Baseline Characteristics Before Prednisolone Therapy
Duration of Body Mass Fasting PlasmaAge Prednisolone Therapy Index Glucose Levela
Sex Diagnosis (yrs) (mo) (g/m2) (mg/dl)F Myasthenia gravis 19 2.6 18.7 72.0F ADEM 28 1.2 17.1 76.5F Encephalitis 24 1.0 24.4 74.0M Neuro-Behçet disease 41 12 20.2 75.0M Multiple sclerosis 64 7 20.0 104.0M Neuro-Behçet disease 33 4 21.1 53.0F Multiple sclerosis 47 19 27.1 81.5M CIDP 75 20 22.6 84.5F Multiple sclerosis 27 0.5 17.1 78.5F Myasthenia gravis 39 12 23.3 64.5M CIDP 53 0.6 23.1 99.0F Myasthenia gravis 59 1.5 21.8 78.0F Polymyositis 42 1.0 18.2 76.5F Multiple mononeuropathy 66 2.2 17.2 66.0F CIDP 53 20 39.8 100.0F Myasthenia gravis 52 1.5 20.8 75.0M Churg-Strauss syndrome 59 7.5 19.2 83.0F Myasthenia gravis 71 17 23.2 98.5F Churg-Strauss syndrome 54 0.5 22.7 106.0F Myasthenia gravis 65 1.3 18.2 75.5M CIDP 57 0.8 22.8 78.5F Polymyositis 63 12 21.1 101.0M CIDP 69 23 22.2 94.5F Multiple mononeuropathy 60 1.0 15.1 72.0F Polymyositis 44 1.3 18.8 71.5
Mean 50.6 6.8 21.4 81.5ADEM = acute disseminated encephalomyelitis, CIDP = chronic inflammatory demyelinating polyneuropathy.aMean concentration from measurements on 2 different days.

PHARMACOTHERAPY Volume 24, Number 4, 2004
Hospital, Mie, Japan, were reviewed in thisretrospective study. The patients’ neurologicdiseases were myasthenia gravis (six patients),chronic inflammatory demyelinating polyneuro-pathy (five), multiple sclerosis (three), polymyositis(three), neuro-Behçet disease (two), Churg-Strausssyndrome (two), multiple mononeuropathy(two), encephalitis (one), and acute disseminatedencephalomyelitis (one) (Table 1). We selectedpatients who met the following six requirements:began to receive steroid therapy between January2000 and October 2002; received prednisolone30–60 mg/day orally after breakfast for more than2 weeks; received a normal hospital dietaccording to caloric requirement; had no historyof diabetes, drug therapy for diabetes, or familyhistory of diabetes before the study; did notreceive antihyperglycemic agents, antihyper-lipidemic agents, thiazide diuretics, b-blockers,or immunosuppressive agents, except steroids,that might affect blood glucose concentrationsduring the study; and were provided withpharmaceutical care for drug-related problems tomaintain compliance with prednisolone therapy.Seventeen of 25 patients received intravenousmethylprednisolone pulse therapy 1000 mg/dayfor 3 days followed by oral prednisolone therapy.Although we did not evaluate the level of activityof the patients, activity levels might have beenlow because of the neuromuscular disorders.
Daily Plasma Glucose Profile
Plasma glucose profiles were determinedimmediately before and 2 hours after each mealonce in each patient by using the peak acceler-ation method with a glucose oxidase-immobilizedmembrane-oxygen electrode (Glucoroder; A&T,Kanagawa, Japan). The diagnosis and classificationof diabetes were based on the recent definition bythe World Health Organization.7 Table 2 givesthe parameters for the diagnosis of diabetesmellitus and impaired glucose tolerance used in
this study. We classified the 25 patients intothree groups according to the fasting plasmaglucose and random plasma glucose concen-trations and assessed the sensitivity for detectionof SDM at each sampling point. We also examinedthe daily plasma glucose concentrations on theday of administration or no administration ofprednisolone in the four patients with SDM whoreceived prednisolone every other day.
Risk Factors for SDM
To investigate the risk factors for SDM, thepatients were divided into two groups on thebasis of whether SDM developed (13 patients) ornot (12 patients). We compared the daily plasmaglucose concentrations between the SDM andnon-SDM groups. Ages; body mass indexes;number of pulse methylprednisolone episodes;prednisolone cumulative doses, daily doses,dosage regimen, and duration of treatment; andconcentrations of serum cholesterol andtriglycerides were compared between the twogroups. The cumulative doses of prednisolonedid not include the dose of pulse methylpred-nisolone. The serum cholesterol and triglycerideconcentrations were measured before and afterprednisolone treatment.
Statistical Analysis
All data are given as the mean ± SD. Theplasma glucose concentrations at six samplingpoints were analyzed by using the Tukey method.A paired t test was performed to analyze thedifference in plasma glucose concentrationsbetween the days of administration and noadministration of prednisolone in each alternate-day dosage regimen. When the data of the twogroups were compared, an independent t test(Welch or Student) was performed. A p value ofless than 0.05 was considered to indicate astatistically significant difference.
Results
Daily Plasma Glucose Profiles
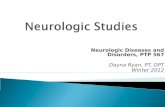
The daily changes in plasma glucose concen-trations in the 25 patients receiving prednisoloneare shown in Figure 1. The mean glucoseconcentration (236.0 ± 90.6 mg/dl) 2 hours afterlunch was the highest among the six samplingpoints. Table 3 presents the diagnosis and thesensitivity for detection of SDM at four samplingpoints: before breakfast, and 2 hours afterbreakfast, lunch, and dinner. Thirteen (25%) of
510
Table 2. Definitions of Diabetes Mellitus and ImpairedGlucose Tolerance Used in This Study7
Plasma Glucose Concentration (mg/dl)Diagnosis Fasting RandomDiabetes mellitus ≥ 126 ≥ 200
Impaired glucosetoleranceFasting ≥ 110 but < 126 —Postprandial — ≥ 140 but < 200
Normal < 110 < 140

STEROID-INDUCED DIABETES IN PATIENTS WITH NEUROLOGIC DISEASES Iwamoto et al
the 25 patients developed SDM by finaldiagnosis. All of the patients with a diagnosis ofSDM had plasma glucose concentrations of morethan 200 mg/dl 2 hours after lunch. Thesensitivity of monitoring plasma glucose at 2hours after lunch was regarded as 100% fordetecting SDM in the patients with SDM. Thesecond highest detection rate (76.9%) was thepoint 2 hours after dinner. The glucoseconcentrations before breakfast (fasting plasmaglucose) did not contribute to detecting SDMbecause 24 of the 25 patients had a normalglucose tolerance at this sampling point.
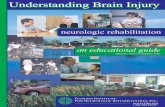
Figure 2 shows the daily changes in the plasmaglucose concentrations on the day of adminis-tration or no administration of prednisolone inthe four patients with SDM who receivedprednisolone with the alternate-day dosageregimen. This small subgroup analysis revealedthat mean plasma glucose concentrations 2 hours
after each meal were significantly higher on thedays of prednisolone treatment than on the dayswithout.
Risk Factors for SDM
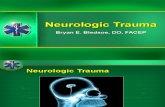
In Table 4, demographic characteristics andlaboratory data are compared between the SDMand non-SDM groups. The SDM group hadhigher plasma glucose concentrations beforelunch and dinner and after every meal than thosevalues in the non-SDM group (p<0.01; Figure 3).The mean age of the SDM group (59.1 ± 10.2 yrs)was significantly higher than that of the non-SDM group (41.3 ± 18.0 yrs). The mean serumcholesterol concentration after prednisolonetherapy was also significantly higher in the SDMgroup (226.8 ± 36.4 mg/dl) than in the non-SDMgroup (188.1 ± 27.2 mg/dl). No significant
511
Table 3. Diagnosis and Sensitivity for Detection of Steroid-Induced Diabetes Mellitus at Each Sampling Point
No. of PatientsNormal Impaired
Plasma Glucose Fasting or Postprandial Steroid-InducedSampling Point Concentration Glucose Tolerance Diabetes Mellitus Sensitivity (%)a
Before breakfast 24 1 0 0.02 hrs after breakfast 17 4 4 30.82 hrs after lunch 2 10 13 100.02 hrs after dinner 7 7 10 76.9Final diagnosisb 2 10 13 —aThis rate was estimated by dividing the number of patients with SDM at each sampling point by that (n=13) at the finaldiagnosis.bClassification of diabetes based on the plasma glucose concentrations throughout the day.
Figure 1. Daily profiles of plasma glucose concentrations in25 patients with neurologic diseases who received oralprednisolone. Daily profiles of blood glucose concentrationswere obtained once in each patient. ap<0.01, bp<0.05 (usingthe Tukey method).
Figure 2. Daily profiles of plasma glucose concentrationson the day of administration or no administration ofprednisolone in the four patients with SDM who receivedoral prednisolone every other day. ap<0.05, bp<0.01 (usingthe paired t test).

PHARMACOTHERAPY Volume 24, Number 4, 2004
differences were found between the two groupswith regard to the other factors investigated (i.e.,body mass indexes, prednisolone cumulativetotal doses, dosage regimens, treatment duration,and serum triglyceride concentrations).
Discussion
Prednisolone diminishes glucose utilization,increases protein breakdown, and activateslipolysis in the periphery. It thereby provides
amino acids and glycerol for gluconeogenesis,resulting in an increase in blood glucoseconcentrations. After absorption, 90% or more ofprednisolone in plasma is reversibly bound toplasma protein under normal circumstances, andonly the unbound fraction can enter cells tomediate various actions.10 At normal or lowconcentrations of prednisolone, most of the drugis bound to proteins. At higher concentrations,however, the amount of prednisolone exceeds thecapacity of protein binding, and a significantlygreater fraction of the prednisolone exists in thefree state.10 For these reasons, abnormal glucosetolerance often is observed in patients receivinghigh-dose steroid therapy. A previous studyreported that the frequency of SDM in renaltransplant recipients was 46%.9 However, theplasma glucose concentrations were monitoredonly before meals. Our study showed that 52%of patients with neurologic diseases who receivedhigh doses of prednisolone developed SDM,although the mean duration of steroid therapy(6.9 ± 8.3 wks) was shorter than that in theprevious study9 (at least 1 yr). However, theinfluence of steroid administration on bloodglucose concentrations might have beenoverestimated in our study because of the smallnumber of patients with heterogeneousneurologic diseases. It also might be difficult topredict the influence of steroids on blood glucoseconcentrations in patients with other diseases
512
Table 4. Patient Demographic Characteristics and Laboratory Data of the SDM and Non-SDMGroups
SDM Group Non-SDM GroupParameter (n=13) (n=12)Age (yrs)a 59.1 ± 10.2b 41.3 ± 18.0
Body mass index (g/m2)a 21.3 ± 6.2 21.4 ± 3.0
Patients with pulse methylprednisolone (no.) 9 8
Cumulative total dose of prednisolone (g)a 6.5 ± 7.7 5.4 ± 7.4
Dosage of prednisolone (mg/day)a 42.7 ± 11.4 42.1 ± 11.2
Prednisolone dosage regimen (no.)Daily 9 6Alternate day 4 6
Duration of prednisolone therapy (wks)a 6.9 ± 8.3 6.7 ± 7.2
Serum cholesterol level (mg/dl)a
Before prednisolone treatment 186.2 ± 28.7 186.2 ± 36.6After prednisolone treatment 226.8 ± 36.4b 188.1 ± 27.2
Serum triglyceride level (mg/dl)a
Before prednisolone treatment 112.5 ± 23.3 96.3 ± 28.6After prednisolone treatment 115.2 ± 22.5 105.3 ± 35.0
SDM = steroid-induced diabetes mellitus.aData are mean ± SD.bSignificant difference between the two groups (Student t test, p<0.01).
Figure 3. Daily profiles of plasma glucose concentrations inthe SDM (13 patients) and non-SDM (12 patients) groups.ap<0.01 (using the independent t test).

STEROID-INDUCED DIABETES IN PATIENTS WITH NEUROLOGIC DISEASES Iwamoto et al
that require long-term steroid therapy. Highplasma glucose concentrations (≥ 200 mg/dl)quite often were observed 2 hours after lunch.All of the patients with SDM had postprandialhyperglycemia at this sampling point. If we hadnot monitored the glucose concentrations afterlunch, we would not have detected most of theSDM cases. Thus, plasma glucose concentrationsafter lunch should be monitored to detect SDMin patients with neurologic diseases who receivehigh-dose steroid therapy.
We showed that postprandial glucoseconcentrations were significantly higher on thedays of drug treatment than on the days withoutin the four patients with SDM who receivedprednisolone every other day. Since thissubgroup study consisted of a small number ofpatients, more studies are needed. We suspect,however, that impaired glucose tolerance inducedby steroids may continue for about 24 hourswhen the steroids are administered once/day.One group of authors11 reported that plasmaglucose concentrations after lunch were similarto those after breakfast or dinner in patients withtype 2 diabetes, without administration ofantihyperglycemic drugs. Our study, however,showed that the mean plasma glucose concen-tration after lunch was highest among theconcentrations at postprandial points. Althoughthe mean time of maximum plasma concentrationand the half-life of prednisolone are 1.3 and 2.2hours after oral administration, respectively,10 thedrug might continue to be active during thedaytime. Several studies have revealed thatpostprandial hyperglycemia including impairedglucose tolerance is a risk factor for mortality12–14
and is closely associated with cardiovasculardisease.15–17 In addition, the authors of anotherstudy18 found that acute hyperglycemia (> 270mg/dl) induced significant increases in plateletaggregation and blood viscosity, which areregarded as important cardiovascular riskfactors.19 In our study, 23 of the 25 patientsdeveloped postprandial hyperglycemia (SDM orimpaired glucose tolerance), and 9 patients hadmaximum glucose concentrations of greater than270 mg/dl.
It was reported that aging and cumulativedoses of steroids were risk factors for thedevelopment of SDM in patients with renaltransplants who received high doses of steroidsfor more than 1 year.9 We did not find anydifference between the SDM and non-SDMgroups with regard to the cumulative doses ofprednisolone. These results suggest that
cumulative doses of steroids are minimallyassociated with the development of SDM whenpatients receive high-dose, short-term steroidtherapy. Similar to a previous study,9 we foundthat aging is a risk factor for SDM. Severalarticles report that advancing age is a major riskfactor for diabetes mellitus.20–22 Glucoseintolerance may be due, in part, to a decreasedsensitivity of pancreatic cells to glucagon-likepeptide 1 and to alterations of hepatic glucoseproduction.23 These mechanisms may explainthe development of SDM in the elderly. We alsorevealed that the serum cholesterol concentrationsafter prednisolone treatment were significantlydifferent between the SDM and non-SDM groups.Serum cholesterol concentrations before steroidtherapy were comparable between the twogroups. These results suggest that hypercholes-terolemia is caused by the use of prednisolone.Many patients with type 2 diabetes are reportedto have high serum concentrations of cholesterol.24
The generation of postprandial lipoprotein hasbeen thought to be promoted by postprandialhyperglycemia in these patients.25 Long-termsteroid therapy also has been implicated inhypercholesterolemia.26 Therefore, it is notsurprising that the SDM group had higher serumcholesterol concentrations than those of the non-SDM group. In addition to hyperglycemia,hypercholesterolemia is known to be a significantrisk factor for cardiovascular complications ormortality in patients with diabetes mellitus.27, 28
Conclusion
Our findings strongly suggest that high-doseprednisolone increases the risk for developingtype 2 diabetes, especially in elderly patients,although the study sample size was small. Theclose relationship among postprandial hyper-glycemia, advanced age, and hypercholesterolemia,which are risk factors for cardiovascular disease,seems a characteristic of SDM in patients withneurologic diseases. To detect SDM and begintherapy for it in the early stages, the monitoringof plasma glucose concentrations 2 hours afterlunch is recommended in all patients receivinghigh doses of steroids. These findings shouldprovide useful information for health careworkers regarding the pharmaceutical care ofthese patients.
References1. Garrelds IM, van Hal PT, Haakmat RC, Hoogsteden HC,
Saxena PR, Zijlstra FJ. Time dependent production ofcytokines and eicosanoids by human monocytic leukaemia
513

PHARMACOTHERAPY Volume 24, Number 4, 2004
U937 cells: effects of glucocorticosteroids. Mediators Inflamm1999;8:229–35.
2. Paul R, Lorenzl S, Koedel U, et al. Matrix metalloproteinasescontribute to the blood-brain barrier disruption duringbacterial meningitis. Ann Neurol 1998;44:592–600.
3. Rosenberg GA, Estrada EY, Dencoff JE. Matrix metallo-proteinases and TIMPs are associated with blood-brain barrieropening after reperfusion in rat brain. Stroke 1998;29:2189–95.
4. Rizza RA, Mandarino LJ, Gerich JE. Cortisol-induced insulinresistance in man: impaired suppression of glucose productionand stimulation of glucose utilization due to a postreceptordetect of insulin action. J Clin Endocrinol Metab 1982;54:131–8.
5. Paquot N, Schneiter P, Jequier E, Tappy L . Effects ofglucocorticoids and sympathomimetic agents on basal andinsulin-stimulated glucose metabolism. Clin Physiol1995;15:231–40.
6. Krentz AJ, Williams AC, Nattrass M. Insulin resistance inmultiple aspects of intermediary metabolism in myotonicdystrophy. Metabolism 1991;40:866–72.
7. World Health Organization. Definition, diagnosis andclassification of diabetes mellitus and its complications. I.Diagnosis and classification of diabetes mellitus. In: Report of aWHO consultation. Geneva: World Health Organization,1999:1–59.
8. The DECODA Study Group, International DiabetesEpidemiology Group. Cardiovascular risk profile assessment inglucose-intolerant Asian individuals: an evaluation of theWorld Health Organization two-step strategy—the DECODAstudy (diabetes epidemiology: collaborative analysis ofdiagnostic criteria in Asia). Diabet Med 2002;19:549–57.
9. Arner P, Gunnarsson R, Blomdahl S, Groth CG. Somecharacteristics of steroid diabetes: a study in renal-transplantrecipients receiving high-dose corticosteroid therapy. DiabetesCare 1983;6:23–5.
10. Schummer BP, Parker KL. Adrenocortical steroids and theirsynthetic analogs. In: Hardman JG, Limbird LE, Gilman AG,eds. Goodman and Gilman’s the pharmacological basisof therapeutics, 10th ed. New York: McGraw-Hill, 2001:1655–75.
11. Bonora E, Calcaterra F, Lombardi S, et al. Plasma glucoselevels throughout the day and HbA(1c) interrelationships intype 2 diabetes: implications for treatment and monitoring ofmetabolic control. Diabetes Care 2001;24:2023–9.
12. Temelkova-Kurktschiev TS, Koehler C, Henkel E, LeonhardtW, Fuecker K, Hanefeld M. Postchallenge plasma glucose andglycemic spikes are more strongly associated with athero-sclerosis than fasting glucose or HbA1c level. Diabetes Care2000;23:1830–4.
13. Barrett-Connor E, Ferrara A . Isolated postchallengehyperglycemia and the risk of fatal cardiovascular disease inolder women and men. Diabetes Care 1998;21:1236–9.
14. Tominaga M, Eguchi H, Manaka H, Igarashi K, Kato T,Sekikawa A. Impaired glucose tolerance is a risk factor for
cardiovascular disease, but not impaired fasting glucose: theFunagata diabetes study. Diabetes Care 1999;22:920–4.
15. The DECODE Study Group, European Diabetes EpidemiologyGroup. Glucose tolerance and mortality: comparison of WHOand American Diabetes Association diagnostic criteria. Diabetesepidemiology: collaborative analysis of diagnostic criteria inEurope. Lancet 1999;354:617–21.
16. Barrett-Connor E, Ferrara A . Isolated postchallengehyperglycemia and the risk of fatal cardiovascular disease inolder women and men: the Rancho Bernardo study. DiabetesCare 1998;21:1236–9.
17. Sievers ML, Bennett PH, Nelson RG. Effect of glycemia onmortality in Pima Indians with type 2 diabetes. Diabetes1999;48:896–902.
18. Giugliano D, Marfella R, Coppola L, et al. Vascular effects ofacute hyperglycemia in humans are reversed by L-arginine:evidence for reduced availability of nitric oxide duringhyperglycemia. Circulation 1997;95:1783–90.
19. Koenig W, Sund M, Lowe GD, et al. Geographical variations inplasma viscosity and relation to coronary event rates. Lancet1994;344:711–14.
20. Andres R. Aging and diabetes: symposium on diabetes mellitus.Med Clin North Am 1971;55:835–46.
21. Wahl PW, Savage PJ, Psaty BM, Orchard TJ, Robbins JA,Tracy RP. Diabetes in older adults: comparison of 1997American Diabetes Association classification of diabetesmellitus with 1985 WHO classification. Lancet 1998;352:1012–15.
22. Resnick HE, Harris MI, Brock DB, Harris TB. AmericanDiabetes Association diabetes diagnostic criteria, advancingage, and cardiovascular disease risk profiles. Diabetes Care2000;23:176–80.
23. Elahi D, Muller DC, Egan JM, Andres R, Veldhuist J, MeneillyGS. Glucose tolerance, glucose utilization and insulin secretionin ageing. Novartis Found Symp 2002;242:222–42.
24. Liebl A, Mata M, Eschwege E. Evaluation of risk factors fordevelopment of complications in type II diabetes in Europe.Diabetologia 2002;45:23–8.
25. Ceriello A. The post-prandial state and cardiovascular disease:relevance to diabetes mellitus. Diabetes Metab Res Rev2000;16:125–32.
26. Fernandez-Miranda C, Guijarro C, de la Calle A, et al. Lipidabnormalities in stable liver transplant recipients: effects ofcyclosporin, tacrolimus, and steroids. Transpl Int 1998;11:137–42.
27. Morrish NJ, Stevens LK, Head J, Fuller JH, Jarrett RJ, Keen H.A prospective study of mortality among middle-aged diabeticpatients (the London cohort of the WHO multinational studyof vascular disease in diabetics) II: associated risk factors.Diabetologia 1990;33:542–8.
28. Lehto S, Ronnemaa T, Haffner SM, Pyorala K, Kallio V, LaaksoM. Dyslipidemia and hyperglycemia predict coronary heartdisease events in middle-aged patients with NIDDM. Diabetes1997;46:1354–9.
514