SPINE Volume 26, Number 22, pp 2472–2477 ©2001, Lippincott...
6
SPINE Volume 26, Number 22, pp 2472–2477 ©2001, Lippincott Williams & Wilkins, Inc. Morphometric Study of the Human Lumbar Spine for Operation–Workspace Specifications Alon Wolf, MSc,* Moshe Shoham, DSc,* Shnider Michael, MD, and Roffman Moshe, MD Study Design. The anatomy of the lumbar vertebrae of 55 patients was measured by use of data provided by computed tomography. On the basis of these measure- ments, the location of puncture points and the orientation of the surgical instruments for pedicle, vertebral body, and disc entry points were calculated for open as well as percutaneous surgery. Objective. Normal anatomic variations of the lumbar spine were investigated to define the workspace for several spinal procedures and to define the workspace of a robot designed to guide the physician during those procedures. Summary of Background. Several comprehensive studies of vertebrae dimensions have been conducted in the past, but they lack several dimensions that are needed to determine the exact location of the entry point and orientation of the tool, in particular when a computerized guidance system is used. Methods. Fifty-five spinal columns (L1–L5, total 250 vertebrae) were measured by computed tomography. These data provide geometric relations that determine entry points and tool orientations for different spinal interventions. Results. The workspace for spinal operations was de- fined on the basis of anatomic data taken from computed tomography scans. The data included 15 measurements for each vertebra that defined its shape. The processed data provided puncture points for several spinal proce- dures in both open and percutaneous surgery. Conclusions. This study provides additional informa- tion on vertebral structure needed to calculate accurately the entry point and tool orientation in various spinal pro- cedures. These statistical data are also valuable for model and implant designs and for workspace specifications for a robot-assisted surgery system. [Key words: lumbar anatomy, vertebrae, medical robots, model and implant design] Spine 2001;26:2472–2477 Several quantitative investigations focusing on lumbar vertebral dimensions have been published. Berry et al 1 manually measured 30 skeletons, creating a database for implants. Nissan and Gilad 8 measured the sagittal plane dimension of several anatomic structures of the vertebrae using lateral radiographs of 157 patients. Scoles et al 10 studied multiple morphologic parameters in 50 normal adults. Zindrick et al 16 reported on 2905 pedicle mea- surements taken from computed tomography data. Van Schaik et al 15 also used computed tomography (CT) to provide morphologic data on anatomic structures of the vertebrae. When the exact entry point and path orientation are needed, for example in a computerized medical robot- assisted surgery system, several vertebral dimensions are missing in the literature. In Berry et al, 1 not all pedicle di- mensions were measured, and there was insufficient infor- mation to calculate lateral vertebral body and disc entry. In Nissan and Gilad 8 and Scoles et al, 10 limited anatomic mea- surements were given, and no data on L2 and L4 were provided. In Zindrick et al, 16 no information other than for pedicles was provided. The investigation of Van Schaik et al 15 focused on the transverse process structure and dimen- sions. Other works studied different anatomic spine struc- tures such as the lumbar vertebral canal, 4 as well as the pedicle and vertebra body in different spinal sections, for instance, the cervical spine 5,8,9 and the thoracic spine. 11 In the new systems of computer-assisted surgery, such as medical robotics, the tool trajectory’s coordinates have to be accurately defined. Moreover, for such robots to be successfully designed, the operation workspace has to be predetermined in such a manner that the required tool trajectory falls within the robot’s reachable region. Hence, workspace definition is essential for the design of the robot’s type, size, weight, and structure (mechanical strength, motors, sensors, etc.). 2,3,6,7,14 Other parame- ters, such as forces, velocity, and accuracy, are also needed to complete the design stage 12,13 but are not re- lated to the workspace definition, which is the focus of the present investigation. To define the operational workspace for surgical pro- cedures on the lumbar spine, morphologic data of the lumbar spine are needed. To accomplish this, the lumbar vertebral anatomy of 55 patients was measured using data from CT, and 15 anatomic measurements were taken for each vertebra. On the basis of the measure- ments taken, the locations of puncture points and tool orientations for pedicle, vertebral body, and disc entry points were calculated for percutaneous as well as for open surgery. These calculations were used to define the workspace for a medical robot system for spinal surgery. Materials and Methods The anatomic dimensions of 55 patients (25 women, 30 men) were measured from CT scans of L1–L5. The age distribution of the patients is given in Table 1. The mean value and variance of each dimension were calculated, and the data distribution was found. These measurements were taken as a necessary step toward the design of the work envelope of a medical robot. Several dimensions measured in this investigation had not previously From the *Robotics Laboratory, Department of Mechanical Engineer- ing, Technion–Israel Institute of Technology, and the Carmel Medical Center, Orthopedic Department, Haifa, Israel. Supported in part by the Israeli Ministry of Science. Acknowledgment date: September 12, 2000. First revision date: February 23, 2001. Acceptance date: April 24, 2001. Device status category: 1. Conflict of interest category: 14. 2472
Transcript of SPINE Volume 26, Number 22, pp 2472–2477 ©2001, Lippincott...

SPINE Volume 26, Number 22, pp 2472–2477©2001, Lippincott Williams & Wilkins, Inc.
Morphometric Study of the Human Lumbar Spine forOperation–Workspace Specifications
Alon Wolf, MSc,* Moshe Shoham, DSc,* Shnider Michael, MD,† and Roffman Moshe, MD†
Study Design. The anatomy of the lumbar vertebrae of55 patients was measured by use of data provided bycomputed tomography. On the basis of these measure-ments, the location of puncture points and the orientationof the surgical instruments for pedicle, vertebral body,and disc entry points were calculated for open as well aspercutaneous surgery.
Objective. Normal anatomic variations of the lumbarspine were investigated to define the workspace for severalspinal procedures and to define the workspace of a robotdesigned to guide the physician during those procedures.
Summary of Background. Several comprehensivestudies of vertebrae dimensions have been conducted inthe past, but they lack several dimensions that are neededto determine the exact location of the entry point andorientation of the tool, in particular when a computerizedguidance system is used.
Methods. Fifty-five spinal columns (L1–L5, total 250vertebrae) were measured by computed tomography.These data provide geometric relations that determine entrypoints and tool orientations for different spinal interventions.
Results. The workspace for spinal operations was de-fined on the basis of anatomic data taken from computedtomography scans. The data included 15 measurementsfor each vertebra that defined its shape. The processeddata provided puncture points for several spinal proce-dures in both open and percutaneous surgery.
Conclusions. This study provides additional informa-tion on vertebral structure needed to calculate accuratelythe entry point and tool orientation in various spinal pro-cedures. These statistical data are also valuable for modeland implant designs and for workspace specifications fora robot-assisted surgery system. [Key words: lumbaranatomy, vertebrae, medical robots, model and implantdesign] Spine 2001;26:2472–2477
Several quantitative investigations focusing on lumbarvertebral dimensions have been published. Berry et al1
manually measured 30 skeletons, creating a database forimplants. Nissan and Gilad8 measured the sagittal planedimension of several anatomic structures of the vertebraeusing lateral radiographs of 157 patients. Scoles et al10
studied multiple morphologic parameters in 50 normaladults. Zindrick et al16 reported on 2905 pedicle mea-surements taken from computed tomography data. VanSchaik et al15 also used computed tomography (CT) to
provide morphologic data on anatomic structures of thevertebrae.
When the exact entry point and path orientation areneeded, for example in a computerized medical robot-assisted surgery system, several vertebral dimensions aremissing in the literature. In Berry et al,1 not all pedicle di-mensions were measured, and there was insufficient infor-mation to calculate lateral vertebral body and disc entry. InNissan and Gilad8 and Scoles et al,10 limited anatomic mea-surements were given, and no data on L2 and L4 wereprovided. In Zindrick et al,16 no information other than forpedicles was provided. The investigation of Van Schaik etal15 focused on the transverse process structure and dimen-sions. Other works studied different anatomic spine struc-tures such as the lumbar vertebral canal,4 as well as thepedicle and vertebra body in different spinal sections, forinstance, the cervical spine5,8,9 and the thoracic spine.11
In the new systems of computer-assisted surgery, suchas medical robotics, the tool trajectory’s coordinateshave to be accurately defined. Moreover, for such robotsto be successfully designed, the operation workspace hasto be predetermined in such a manner that the requiredtool trajectory falls within the robot’s reachable region.Hence, workspace definition is essential for the design ofthe robot’s type, size, weight, and structure (mechanicalstrength, motors, sensors, etc.).2,3,6,7,14 Other parame-ters, such as forces, velocity, and accuracy, are alsoneeded to complete the design stage12,13 but are not re-lated to the workspace definition, which is the focus ofthe present investigation.
To define the operational workspace for surgical pro-cedures on the lumbar spine, morphologic data of thelumbar spine are needed. To accomplish this, the lumbarvertebral anatomy of 55 patients was measured usingdata from CT, and 15 anatomic measurements weretaken for each vertebra. On the basis of the measure-ments taken, the locations of puncture points and toolorientations for pedicle, vertebral body, and disc entrypoints were calculated for percutaneous as well as foropen surgery. These calculations were used to define theworkspace for a medical robot system for spinal surgery.
Materials and MethodsThe anatomic dimensions of 55 patients (25 women, 30 men)were measured from CT scans of L1–L5. The age distributionof the patients is given in Table 1. The mean value and varianceof each dimension were calculated, and the data distributionwas found.
These measurements were taken as a necessary step towardthe design of the work envelope of a medical robot. Severaldimensions measured in this investigation had not previously
From the *Robotics Laboratory, Department of Mechanical Engineer-ing, Technion–Israel Institute of Technology, and the †Carmel MedicalCenter, Orthopedic Department, Haifa, Israel.Supported in part by the Israeli Ministry of Science.Acknowledgment date: September 12, 2000.First revision date: February 23, 2001.Acceptance date: April 24, 2001.Device status category: 1.Conflict of interest category: 14.
2472

been clearly defined in the literature. These dimensions can alsobe used for implant design and modeling.
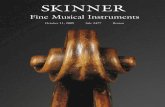
Figure 1 depicts the 15 measured vertebral dimensions.
ResultsStatistical Data and Data Analysis
Tables 2 and 3 show the anatomic dimensions measured(Figure 1) and their statistics. From an analysis of the
data in these tables, one can derive the location of thepuncture point and tool orientation for percutaneousand open surgery performed on the spine. These proce-dures include, for example, pedicle screw fixation, per-cutaneous pedicle screw fixation, discectomy, discogra-phy, and vertebral biopsy.
To confirm that the data are normally distributed, anormal probability graph has been drawn for each di-mension, and the results are given in Figure 2, A throughE. In these graphs, the y axis represents the theoreticalfractions of the distribution, and the ordered data arepresented along the x axis. Because normally distributeddata result in a straight line, Figure 2, A through E im-plies that all measurement data for all vertebrae are nor-mally distributed. These results indicate that in order toinclude the entire population in the workspace, each mea-sured parameter of the vertebra varies in the range x# 6 3s,where x# ; is its mean value (Table 2), and s is its standard
Figure 1. Measured anatomical parameters. A, A–F measured parameters in cut view of vertebra. B, G–J measured parameters in cutview of vertebra. C, Posteroanterior view. D, Posteroanterior section. A, length of midline of pedicle, connecting anterior wall of vertebralbody to tip of transverse process. B, anteroposterior width of vertebral body. C, length of spinous process. D, width of spinous process.E, pedicle angle relative to spinous process midline. F, width of pedicle. G, distance between two extreme tips of transverse processes.H, lateral width of vertebral body. I, distance from tip of spinous process to anterior wall of vertebral body. J, distance from tip of spinousprocess to posterior wall of vertebral body. K, distance between right and left facet joints. L, height of vertebral body. M, distance betweenmiddle of transverse process to middle of spinous process in anteroposterior view. N, distance between middle of spinous process to superioredge of vertebral body in anteroposterior view. P, distance between superior and inferior pedicle edges in anteroposterior cut view.
Table 1. Age Distribution of Patients
Age Group N
0–20 yr 120–30 yr 230–40 yr 540–50 yr 1350–60 yr 860–70 yr 1070–80 yr 1080–90 yr 6
Table 2. Mean Values of Measured Dimensions (mm, *degrees)
Vertebra
Dimension
A B C D E* F G H I J K L M N P
L1 44.8 28.9 30.0 5.0 11.8 5.6 81.8 40.7 76.0 49.4 37.5 24.9 11.5 22.4 15.1L2 46.9 29.8 31.5 4.3 11.0 7.7 80.4 39.8 79.1 48.5 36.9 25.4 10.8 21.6 14.8L3 47.6 32.3 33.5 4.7 12.8 8.9 89.4 43.1 80.1 48.9 39.8 25.6 11.8 19.4 14.5L4 47.6 31.7 32.8 5.3 14.1 11.4 90.5 44.1 79.6 47.2 43.9 26.5 11.4 23.2 14.8L5 46.6 32.5 26.0 5.8 18.5 13.7 93.7 48.1 77.1 43.6 53.5 28.6 11.2 21.6 15.6
Table 3. Standard Deviation of Measured Dimensions in Table 2 (mm, *degrees)
Vertebra
Dimension
A B C D E* F G H I J K L M N P
L1 2.8 2.3 3.7 1.1 1.3 1.3 5.1 3.8 9.0 7.2 5.5 2.4 2.5 2.5 1.9L2 3.6 2.3 4.6 1.3 1.7 1.5 4.6 4.6 7.0 7.0 2.9 1.1 3.2 3.4 1.6L3 3.7 1.3 5.7 1.2 2.2 1.9 5.5 3.8 6.7 5.7 2.7 1.6 2.8 5.4 1.9L4 4.4 2.1 5.3 1.4 2.1 1.8 5.7 4.6 5.0 5.0 3.6 0.6 3.5 7.6 2.1L5 5.3 2.1 5.7 1.4 3.9 2.2 5.9 3.8 6.7 7.4 5.3 1.3 3.7 4.9 2.3
2473Morphometric Study of Lumbar Spine • Wolf et al

deviation (Table 3). In that process, 99.7% of the popula-tion is included.
By use of the data provided above, the workspace ofentry points needed to reach the vertebrae for severalspinal procedures was estimated. The workspace evalu-ation can be divided into two groups, one for percutane-ous procedures and one for open surgery procedures.Workspace evaluation for spinal operational proceduresis given next.
Workspace Evaluation for Vertebral Body and DiscPuncture Points
In Figure 3, the unknown parameters are D and a. Thefollowing definitions are used:
X 5 SI 1 Sk 2B
2D 2 ~C 1 Sk! (1)
Figure 2. Normal probability plot of data. A, L1. B, L2. C, L3. D, L4.E, L5.
2474 Spine • Volume 26 • Number 22 • 2001

Y 5G
22
H
21 « (2)
sin~a! 5dC
lCf lC 5
dC
sin~a!(3)
In which Sk is the skin thickness; «, a given error; anddc, cannula diameter (I, B, C, G, and H are given inFigure 1).
By use of a trigonometric definition for tangent, thefollowing is obtained:
tan~a! 5X
~Y 1 lC!(4)
Solving (4) for a by substituting (1), (2), and (3) for X,Y, and lc, respectively, one obtains:
a1 5 a tanSX z ÎY2~X2 1 Y2 2 dC2 ! 2 dCY2
Y@dCX 1 ÎY2~X2 1 Y2 2 dC2 !#
D (5)
a2 5 a tanS2X z ÎY2~X2 1 Y2 2 dC2 ! 2 dCY2
Y@dCX 2 ÎY2~X2 1 Y2 2 dC2 #
Dwhere a1 and a2 are two solution for a, given in
Figure 3.The second parameter needed for the determination
of a puncture point is D, measured from the back centralline. Using Figure 3, D can be defined as:
D 5C 1 Sk
tan~a!1
G
21 « 1 lC (6)
It can be seen from Equation 6 that D is most affectedby G, which is the transverse process length; as G in-creases in length, D increases. D is also affected by C 1Sk, representing the length of the spinous process (C) andthe skin thickness (Sk); the larger the sum of the two, thelonger D becomes. Equations (5) and (6) were simulatedby calculating a1 and a2 using the statistical data pro-vided in Table 2, with « 5 2 mm, dc 5 1.2 mm. Thesimulation results for percutaneous and open surgeryprocedures are given in Tables 4 and 5.
Workspace Evaluation for Pedicle Entry PointFrom Figure 4, the following are defined:
Z 5 ~C 1 Sk! z Tan21~E! (7)
D 5K
21 Z (8)
The results for Equation 8 are given in Tables 6 and 7.Next, using the length of the pedicle axis (Table 2),
one can calculate the trajectory of the axis in a directionperpendicular to the spinous process. This trajectory isthe screw entry distance denoted by dl (Figure 5). Thesedata are essential in determining the workspace of thevertebra.
The screw entry distance, dl, is given by:
dl5A z cos~E! (9)
Solutions for Equation 9 are shown in Table 8.
Figure 3. Location and angle of tool for disk and vertebral bodypuncture point.
Figure 4. Puncture point location and angle for pedicle area.
Table 4. Workspace Evaluation for Percutaneous Casesin Figure 3
Vertebra
L1 L2 L3 L4 L5
Spacer length, D (mm) 66.2 65.3 74.6 74.6 71.2Workspace (half) (mm) 20.3 21.3 31.2 34.0 31.2Angle, a (degrees) 66.5 68.1 64.8 65.0 66.7Angular workspace (half) (degrees) 3.8 1.3 1.5 3.3 2.7
Table 5. Workspace Evaluation for Open SurgeryDescribed in Figure 3
Vertebra
L1 L2 L3 L4 L5
Spacer length, D (mm) 65.9 65.2 75.9 75.5 68.9Workspace (half) (mm) 12.3 15.4 21.3 22.2 24.9Angle, a (degrees) 54.4 55.6 53.4 54.9 54.5Angular workspace (half) (degrees) 1.0 3.2 2.2 5.9 3.7
2475Morphometric Study of Lumbar Spine • Wolf et al

Discussion
In this investigation, the regions in which entry pointsand tool orientations of several spinal operations residewere defined. These regions were calculated by use ofanatomic data taken from CT of the lumbar spine. Thesedata are helpful for conventional procedures and essen-tial for implant design, modeling, and workspace defini-tion for robot-assisted surgery.
The workspace of surgical tools during insertion wasdivided into angular and displacement regions, and itdiffers from one vertebra to another. It has been shownthat for percutaneous surgical procedures such as verte-bral body biopsy and discectomy, the mean value of thepuncture point is 70.4 mm from the midline, with a min-imum value of 45.9 mm in L1 and a maximum value of108.6 mm in L5. In this case, the entry angle has a meanvalue of 24 degrees, with a minimum of 20.7 degrees inL1 and a maximum of 27.3 degrees in L5. For opensurgery cases, the mean value of the puncture point is70.3 mm from the midline, with a minimum value of49.8 mm in L2 and a maximum value of 97.7 mm in L4.In this case, the entry angle has a mean value of 35.4degrees, with a minimum of 29.2 degrees in L3 and amaximum of 38.8 degrees in L5. For the pedicle entry
point in percutaneous cases, a mean value of 34.2 mmfrom the midline was found, with a minimum value of14.6 mm in L1 and a maximum value of 72 mm in L5.For open surgery cases, a mean value of 28.5 mm fromthe midline was found, with a minimum value of 14.1mm in L1 and a maximum value of 53.1 mm in L5. Inboth cases, the average entry angle is 13.7 degrees, witha minimum value of 10.5 degrees and a maximum valueof 22.5 degrees. This angle is dictated by the anatomy ofthe pedicle.
Analyzing the data given above, one can see that forangular workspace, the maximum required tilt angle isabout 40 degrees, and for displacement workspace, therange varies between 46 mm and 109 mm for disc entrypoint, and from 14.1 mm to 53.1 mm for pedicle entry.Hence, a 60-mm displacement workspace is sufficient. Asfor the displacement along the pedicle axis, a range of 10mm is sufficient.
The data given here confine the surgical tool work-space in a box of 12 3 60 3 10[mm3], with a tilt angle of5 degrees to 40 degrees relative to the surface’s normal.Assuming that these data are a representative sample ofthe population, this box covers 99.7% of patients’ entrypoints and tool orientations for several spinal interven-tions, such as pedicle screw fixation, percutaneous pedi-cle screw fixation, discectomy, discography, and verte-bral biopsy.
Key Points
● This study provides additional information onvertebral structure needed to calculate accuratelythe entry point and tool orientation in various spi-nal procedures.● These statistical data are also valuable for modeland implant designs and for workspace specifica-tions for a robot-assisted surgery system.
Acknowledgment
The authors thank Mr. Mati Shnap, Carmel HospitalComputed Tomography Center, for providing the data.
References
1. Berry JL, Moran JM, Berg WS, et al. A morphometric study of humanlumbar, selected thoracic vertebrae. Spine 1987;12:362–7.
2. Gupa KC. On the nature of robot workspace. Int J Robotics Res 1986;5:112–21.
3. Gupta KC, Roth B. Design considerations for manipulator workspace.ASME J Mech Design 1982;104:704–11.Figure 5. Trajectory of the pedicle axis.
Table 6. Workspace Evaluation for Percutaneous CasesDescribed in Figure 4
Vertebra
L1 L2 L3 L4 L5
D (mm) 29.8 29.1 32.8 36.0 43.1Maximum value (mm) 61.4 54.4 63.2 68.0 72.4Minimum value (mm) 14.6 14.9 16.9 18.0 19.4
Table 7. Workspace Evaluation for Open Surgery CasesDescribed in Figure 4
Vertebra
L1 L2 L3 L4 L5
D (mm) 25.0 24.6 27.5 30.2 35.4Maximum value (mm) 43.5 38.8 44.9 48.7 53.1Minimum value (mm) 14.1 14.9 16.7 17.9 19.3
Table 8. Workspace Evaluation for the Trajectory of thePedicle Axis
Vertebra
L1 L2 L3 L4 L5
Mean distance, dl (mm) 43.8 46.0 46.4 43.2 41.4Workspace (mm) 12.8 18.5 18.2 21.6 22.1
2476 Spine • Volume 26 • Number 22 • 2001

4. Huizinga J, van der Heiden JA, Vinken PJJG. The human lumbar vertebralcanal: A biomechanic study. Proc R Neth Acad Sci 1952;C55:22–33.
5. Karaikovic EE, Daubs MD, Madsen RW, et al. Morphologic characteristicsof human cervical pedicle. Spine 1997;22;5:493–500.
6. Kumar A, Waldron KJ. The workspace of a mechanical manipulator. ASMEJ Mech Design 1982;103:665–72.
7. Lin PN, Duffy J. The mapping and structure of the workspace of robotmanipulators with revolute and prismatic pairs. Proceedings of the ASME,2nd International Computer Engineering Conference 1982:165–72.
8. Nissan, M, Gilad I, The cervical and lumbar vertebrae: An anthropometricmodel. Eng Med 1984;13:111–4.
9. Panjabi MM, Shin EK, Wang J-L. Internal morphology of human cervicalpedicles. Spine 2000;25:1197–205.
10. Scoles PV, Linton AE, Latimer B, et al. Vertebral body, posterior elementmorphology: The normal spine in middle life. Spine 1988;13:1082–6.
11. Stefee AD, Stikowski DJ, Topham LS. Total vertebral body and pediclearthroplasty. Clin Orthop 1986;203:203–8.
12. Shoham M, Roffman M, Goldberger S, et al. Robot construction for medicalapplications. Proceedings of the 2nd Israeli Symposium on Computer As-sisted Surgery, Medical Robotics and Medical Imaging, Jerusalem, 1999.
13. Simaan N, Shoham M. Robot construction for surgical applications. Pro-ceedings of the 1st International Federation of Automatic Control Confer-ence on Mechatronics, Darmstadt, Germany, 2000.
14. Tsai CY, Soni HA. The effect of link parameters on the working space ofgeneral 3R robot arms. Proceedings of the 7th Applied Mechanisms Confer-ence, 1981:3.1–6.
15. Van Schaik JJ, Verbiest H, van Schaik FD. Morphometry of lower lumbarvertebrae as seen on CT scans: Newly recognized characteristics. AJR Am JRoentgenol 1985;145:327–35.
16. Zindrick MR, Wiltse LL, Doornik A, et al. Analysis of the morphometriccharacteristics of the thoracic and lumbar pedicles. Spine 1987;12:160–6.
Address reprint requests to
Alon Wolf, MScMechanical Engineering Department
Technion CityHaifa, 32000
IsraelE-mail: [email protected]
2477Morphometric Study of Lumbar Spine • Wolf et al