
SOK P. Final IP MSW May25 2008
59
Case Management/SMI 1 INDIVIDUALS WITH SERIUOUS MENTAL ILLNESS: WHAT DO WE KNOW ABOUT CASE MANGEMENT? By Phan Sok, MD, MPH An Integrative Project Submitted in Partial Fulfillment of The Requirements for a Master of Social Work Degree, Rhode Island College School of Social Work May 2008
Transcript of SOK P. Final IP MSW May25 2008

Case Management/SMI 1
INDIVIDUALS WITH SERIUOUS MENTAL ILLNESS: WHAT DO WE KNOW ABOUT CASE MANGEMENT?
By
Phan Sok, MD, MPH
An Integrative Project
Submitted in Partial Fulfillment
of
The Requirements for a Master of Social Work Degree,
Rhode Island College School of Social Work
May 2008
Case Management/SMI 2
Acknowledgements
My journey is still in a long path… This project would not be achieved without generous support from many people.
I would like to thank the Fellowship Health Resources, Inc. for allowing me to
collect data at Fall River Network. I thank Denise Amoral, regional director, Stephanie Dzialo, program clinician, all staff, program directors, and program nurses at Fall River Network for their prompt responses related to this project. I, especially, thank Joseph Dziobek, the CEO, for his commitment and moral support for my internship, and providing my tuition during Fall 2007 and Spring 2008.
I appreciate and thank Dr. Roberta Sue Pearlmutter, my professor and Integrative Project advisor, for all her help and advice with this project. Particularly, I thank Dr. Mary Ann Bromley, my professor and field instructor; and Dr. Jayashree Nimmagadda, my field supervisor, for their time, advice and guidance during my academic career, as well as introducing me to the Fellowship. I extend my sincere thanks the dean, Dr. Carol Bennett-Speight, and all my professors at Rhode Island College School of Social Work, who have taught me to become a social worker. I thank Eileen Ryan for her secretarial help to meet my needs at the school.
I cannot forget to thank Karen Cunningham, former vice president at Family Services of Rhode Island, who gave advice and introduced me to the MSW program at Rhode Island College.
I would like to thank Alan Ellis Symonds and his wife Dr. Patricia V. Symonds (anthropologist, Brown University); my wife’s relatives in Canada, Try Vannary and his family; my uncle in France Thou Bernard; my sister’s family in Cambodia, Sin Rany; and my wife’s relatives in Texas and New Hampshire, the Khiev and Keo families, and a few friends in Providence for their moral and physical support to my family’s needs here. I cannot deny my gratefulness to my friends and their families in the Rhode Island Church of Christ for their love, kindnesses, and physical support since my family fist stepped into Providence, Rhode Island. They are the Wing, Lawson, Sutherland, Fackler, Gadoury, McPhee families and others. In particular, this project may not have been initiated if I had not received the special assistance of Theodore W. Blickwedel, my classmate, and his wife Julita O. Blickwedel during our family’s financial crisis in Fall 2007. I am thankful to them for their compassion and human sensitivity to my family.
Last, all my work at the School of Social Work, Rhode Island College would not have been accomplished without my family. I present special thanks and a great amount of love to my wife Dr. Saylinda Muorng, and my older son, Pagna Sok, and my younger son, Visal Sok, for their respect, truthfulness, and encouragement of me.

Case Management/SMI 3
េសចក�ីែថ�ងអំណរគុណ
ដំេណ ររបស់ខ�ុំគឺឋិតេនេលផ�ូវដ៏ែវងឆា� យ… ក្រមងករងរ េនះមិនអចបានសេ្រមចបានេទ
េបសិនគា� ន ករជួយទំនុកបំរងុពីបុគ�លជាេ្រចនរបូ។
ខ�ុំសូមអរគុណ Fellowship Health Resources, Inc. ក�ុងករអនុ�� តឱ្យខ�ុំយកទិន�័យេន Fall
River Network។ ខ�ុំសូមអរគុណនាយិកតំបន់ Denise Amoral ្របធានគ�ីនិក Stephanie Dzialo
បុគ�លិកទំងអស់ ្របធានគេ្រមាងនិងគិលនុបដ� យិកទំងអស់េន Fall River Network ស្រមាប់ករេឆ�យ
តបរបស់ពួកេគេទនឹង ករងរេនះ។ ខ�ុំសូមអរគុណជាពិេសសដល់េលកនាយក Joseph Dziobek
ស្រមាប់ករពុះពរនិងករគំា្រទ
េលកទឹកចិត�របស់គាត់េលកម�សិក្សោរបស់ខ�ុំនិងករផ�ល់ថវកិរស្រមាប់ៃថ�់សលក�ុងសរទររដូវឆា� ំ ២០០៧
និងនិទឃរដូវឆា� ំ ២០០៨។
ខ�ុំសូមសរេសរនិងអរគុណបណ�ិ ត Roberta Sue Pearlmutter
ជាស�ស� ចរ្យនិង្រគ�្រត�តកិច�ករខ�ុំ ចំេពះករជួយនិងករផ�ល់េយាបល់របស់គាត់េលករងរេនះ។
ជាពិេសស ខ�ុំសូមអរគុណបណ�ិ ត Mary Ann Bromley ជាស�ស� ចរ្យនិង្រគ�កម�សិក្សោ បណ�ិ ត
Jayashree Nimmagadda ជា្រគ�្រគប់្រគងកម�សិក្សោខ�ុំ ែដលឱ្យ េពលេវល
េយាបល់និងករែណនំារបស់ពួកគាត់ក�ុងអំឡុងេពលេធ�កម�សិក្សោរបស់ខ�ុំ ក៏ដូចជាករនំាខ�ុំឱ្យស� ល់ the
Fellowship។ ខ�ុំសូមអរគុណេដយេស� ះដល់្រពឹទ�បុរសបណ�ិ ត Carol Bennett-Speight និងស�ស� ចរ្យ
របស់ខ�ុំ ទំងអស់េន Rhode Island College School of Social Work ែដលបានបេ្រង�នខ�ុំ ឱ្យេទជា
Social Worker។ ខ�ុំសូមអរគុណ Eileen Ryan ក�ុងករជួយែផ�កេលខធិករ
េដម្បបំីេពញនូវរល់េសចក�ី្រត�វករ របស់ ខ�ុំក�ុងសល។
ខ�ុំមិនអចបំេភ�ចករដឹងគុណដល់ Karen Cunningham អតីតអនុនាយិកេន Family Service of
Rhode Island ក�ុងករឱ្យេយាបល់និងែណនំាខ�ុំឱ្យចូលសល Social Work េន Rhode Island College។
Case Management/SMI 4
ខ�ុំសូមអរគុណេលក Alan Ellis Symonds និងភរយិារបស់គាត់បណ�ិ ត Patricia V. Symonds
(anthropologist, Brown University) បងប�ូនរបស់ភរយិាខ�ុំ ្រទី វណា� រ ីនិង្រគ�សរឯេទៀតេនកណាដ
ឪពុកមា របស់ខ�ុំ Thou Bernard េន�ស�កបារងំ បង�សីខ�ុំ សិុន រ៉នី
និង្រគ�សររបស់គាត់េនកម�ុជានិងបងប�ូន ភរយិា ខ�ុំេន Texas និង New Hampshire មានជាអទិ៍្រគ�សរ
េខៀវ វណា� និង ែកវ វណា� ្រពមទំងមិត�ភ័ក�ិមួយ ចំនួនេទៀតេន្រក�ង Providence
ែដលជួយជាទឹកចិត�និងថវកិដល់េសចក�ី្រត�វកររបស់្រគ�សរខ�ុំេនទីេនះ។
ខ�ុំមិនអចបដិេសធេសចក�ីដឹងគុណរបស់ខ�ុំដល់មិត�ភក�ិនិង្រគ�សររបស់ពួកេគេនក�ុង Rhode Island
Church of Christ ស្រមាប់េសចក�ី�សឡាញ់ សប្ុបរសធម៌
និងករផ�ល់ជាថវកិចប់តំងពី្រគ�សររបស់ខ�ុំបានមកដល់្រក�ង Providence ៃនរដ� Rhode Island
ដំបូងមកេម៉�ះ។ អ�កទំងេនាះមាន្រគ�សរ Wing Lawson Sutherland Fackler Gadoury និង McPhee
និង្រគ�សរមួយចំនួនេទៀត។
កិច�ករេនះមិនអចចប់បដិសន�ិបានេទ
េបសិនខ�ុំមិនបានទទួលករឧបត�ម�ពិេសសពីមិត�រមួថា� ក់ខ�ុំ គឺ Theodore W. Blickwedel និងភរយិាគាត់
Julita O. Blickwedel ក�ុងខណៈេពលែដល្រគ�សរខ�ុំ មានហិរ��វបិត�ិ នាសរទររដូវឆា� ំ ២០០៧។
ជាប�� ប់ រល់ករេរៀនសូ្រតរបស់ខ�ុំេន Rhode Island College School of Social Work
នឹងមិនអច សេ្រមចបានេទេបពំុមាន្រគ�សរខ�ុំចូលរមួ។ ខ�ុំសូមសំែដងករអរគុណដ៏ពិេសស
និងករ�សឡាញ់ដ៏ធំេធង ដល់ភរយិាខ�ុំ េវជ�បណ�ិ ត មួង សយលីនដ និង សុខ ប�� ជាកូនច្បង និង សុខ
វសិល ជាកូនប�ូន រល់ករ េគារពេសចក�ីេជឿទុកចិត� និងករេលកទឹកចិត�របស់ពួកេគមកេលរបូខ�ុំ។
Case Management/SMI 1
Abstract
Individuals with serious mental illness often need case management because of
cognitive impairments. This study evaluated case management services delivered to 80
individuals with serious mental illness at a community-based mental heath clinic, the Fall
River Network of the Fellowship. Sixty percent of this sample of clients was male. Sixty-
six percent had been diagnosed with schizophrenia and 85% had co-morbid medical
conditions. A higher proportion of men had two or more co-morbid medical conditions
when compared to women, 71% vs. 50%, p = .07, respectively. Case management
services included help with medication independence (93%), health maintenance (74%),
socialization (36%), and household maintenance (21%). Many (64%-67%) individuals
with serious mental illness had been prescribed differential medication regimens.
Although not statistically significant, males were less likely to reach medication step two
or higher compared to females, 66% vs. 80%, respectively. The frequency of hospital
admission decreased significantly during the past ten years and two years from a mean
(SD) of 4.1 (4.68) to 1.9 (2.6), p = .000, respectively. These findings suggest that
additional efforts need to be made for more effective case management services in this
setting, especially for men, and for developing a protocol of case management related to
adherence to differential medication regimens.
Case Management/SMI 2
Table of Contents
Page Acknowledgements ..…………………………………………………. 2
Abstract …………….….…………………………………………….. 5
List of Tables …………….………………………………………….. 8
List of Figures ……………………………………………………….. 9
Problem Statement ….……………………………………………….. 10 Introduction ……………………………………………………… 10 Literature Review ……………………………………………….. 11
Epidemiology ………………………………………………… 11 Importance of the issue ……………………………………… 11
Policy Analysis ………..…………………………………………. 15 Conceptual Framework ………………………………………….. 19
Methods …………….……………………………………………….. 21 Research Design …………………………………………………. 21 Sampling ……………………………………………………….... 21 Data Collection ………………………………………………….. 22 Limitations ……………………………………………………….. 23 Ethical Issues …………………………………………………….. 24 Data Analysis …………………………………………………….. 25
Results ……………..………………………………………………… 27 Demographics of Individuals with
Serious Mental Illness & Case Managers…………………… 27 Clinical Characteristics among Individuals with SMI ………….. 29 Case Management and Outcomes at FRN …..………………….. 32 Summary………….……………………………………………… 37 Discussion ………….………………………………………………… 38 Demographics of Clients and Case Managers …………………... 38 Clinical Characteristics of Clients ……………………………… 38 Case Management Services: ……………………………………... 40 Outcomes of Case Management …………………………………. 43 Implications for Policy …………………………………………… 44 Implications for Practice and Research ………………..……….. 44
Conclusion ……………………………………………………….. 46 References …………………………………………………………… 47

Case Management/SMI 3
Appendices ………..…………………………………………………. 53
Acronyms
ACT Assertiveness Community Treatment
CM Case management
CM-3 3-month of case management
CM-6 6-month of case management
CM-9 9-month of case management
CMC Co-morbid Medical Conditions
CMHC Community Mental Health Centers
CMI Chronic Mental Illness
CMR Commonwealth of Massachusetts Regulations
DMH Department of Mental Health
FHR Fellowship Health Resources
FRN Fall River Network
GED General Equivalence Diploma
MDD Major Depression Disorder
OCD Obsessive Compulsive Disorder
PRISM Person-Centered, Respectful, Individualized, Strengths-Based Mission Driven
PTSD Posttraumatic Stress Disorder
SD Standard Deviation
SMI Serious Mental Illness

Case Management/SMI 4
List of Tables
Page Table 1: Demographics of Individuals with Serious Mental Illness …..……………………………………….. 27-28
Table 2: Demographics of Case Managers at Fall River Network ………………………………………………. 29
Table 3: Clinical Characteristics among Individuals with Serious Mental Illness ……..……………………………………. 30
Table 4: Case Management Services Provided by Fall River Network …….………………………………………… 32 Table 5: The Effect of Outcomes of Case Management Services …… 35
Table 6: Trend of Hospitalizations in past Ten Years and Two Years ………………………………………. 36
Case Management/SMI 5
List of Figures
Page Figure 1: Consumers in Different Programs at
Fall River Network ……………………………………………… 28 Figure 2: Type of Schizophrenia among Individuals with Serious Mental Illness ……..……………………………………. 31 Figure 3: Type of Schizoaffective Disorders among
Individuals with Serious Mental Illness …………………………. 31
Figure 4: Number of Co-morbid Medical Conditions ………………. 32
Figure 5: Medications Steps among Consumers …………………….. 33
Figure 6: Number and Differential Medication Regimens Prescribed to Consumers ………………………………………… 34
Figure 7: Health Care Providers Needed among Consumers ………... 34
Figure 8: Outcomes of Case Management Services at FRN over Period of Time ……..………………………………… 35
Figure 9: Number of Hospitalizations in past Ten Years and Two Years …………………………………….… 36

Case Management/SMI 6
Problem Statement
Introduction
Serious mental illness (SMI), such as schizophrenia or schizoaffective disorder, is
a complex psychiatric disorder that has influenced human lives either directly or
indirectly. This influence affects not only those who suffer with the illness, but also the
caregivers who are family members of the ill relative. Long-term standard assessment
and treatment planning is required to assist the recovery process for individuals with
SMI, regardless of whether they live in communities or residential programs. SMI results
in economic challenges, as well as other human services costs and issues for society. One
study estimated that the total financial burden of SMI (or chronic mental illness) in the
United States in 2002 was $62.7 billion (Wu et al., 2005).
Many individuals with chronic mental illness (CMI) are able to live in the
community after discharge from a hospital. But many need supports from case
management (CM) services because they are limited in their ability to manage simple
daily tasks, for instance taking prescribed medications or maintaining daily living
activities, such as shopping, cooking, or budgeting (Björkman & Hansson, 2000, 2007;
Björkman, Hansson, & Sandlund, 2002).
To date policymakers do not fully agree on diagnostic classifications; however
SMI refers to those who are disabled by their mental illness and in need of effective
treatment (Kelly, 2002). According to the National Alliance for the Mentally Illness
(NAMI), SMI includes major depressive disorder (MDD), schizophrenia, bipolar
Case Management/SMI 7
disorder, obsessive compulsive disorder (OCD), panic disorder, post traumatic stress
disorder (PTSD), and borderline personality disorder (NAMI, n.d.).
Literature Review
Epidemiology
Overall, the prevalence of SMI is varied. The lifetime prevalence of schizophrenia
in the United States is estimated at 1%; MDD is approximately 17%; and PTSD is 8%
(Jablensky, 1999, as cited in Pratt & Mueser, 2004; Kessler et al. 1994; Kessler, Sonnega,
Bromet, Hughes, & Nelson, 1995). Schizophrenia frequently occurs in onset during early
adulthood, and males tend to have an earlier illness-onset (Canuso & Pandina, 2007,
Castle, Sham, & Murray, 1998, Gureje, 1991).
Importance of the issue
According to Pratt and Mueser (2004), co-morbid psychiatric conditions, for
instance mood and anxiety or substance use disorders, play an important role in
diminishing the ability to recover and rehabilitate cognitive and vocational functioning
among patients with schizophrenia and schizoaffective disorder. This is because each of
these disorders may impact on or interact with the disease. The authors also point out that
the two common co-morbid disorders in schizophrenia are substance use and
posttraumatic stress disorder.
Cognitive impairment is critical among those with schizophrenia or
schizoaffective disorder, resulting from the deficit of working memory (immediate
storage and access of information), verbal memory (recall and retrieval of information),
sustained attention (difficulty to focus), as well as lack of executive function (Breier,
Schreiber, Dyer, & Pickar, 1991, as cited in Pratt & Mueser, 2004; Docherty et al., 1996;
Case Management/SMI 8
Saykin et al., 1991; Tollefson, 1996). Individuals who suffer from SMI experience
difficulty with social and role functioning, which requires both basic level neuro-
cognitive functions like memory and attention and higher-level processing, such as
planning, organizing, reasoning, decision making, information processing, and mental
flexibility (Breier et al., 1991; Tollefson, 1996, as cited in Pratt & Mueser, 2004). The
higher-level processing is considered as executive function, which is handled primarily at
the frontal lobe of the cerebral cortex.
As Pratt and Mueser (2004) indicated, the illness pervades many aspects of an
individual’s life. Therefore, it is crucial to evaluate the commonly associated features of
clients who share the disorder, such as schizophrenia or schizoaffective disorder. The
commonly associated features include medication noncompliance, problems in social and
role functioning, housing instability, family planning, and occupational functioning (Pratt
& Mueser, 2004).
Certainly, due to the natural disease characteristics, individuals who recover from
SMI need help with case management services. Many individuals with SMI both in the
community and in residential programs require multiple levels of interventions, including
CM services. These services attempt to assist individuals with CMI to become
independent in terms of vocational and cognitive rehabilitation (Bryson & Bell, 1997)
According to Yank, Bentley, and Hargrove (1993) mental health CM models
include “Expanded Broker,” “Personal Strengths,” “Rehabilitation,” “Full Support,” and
“Clinical Case Management.” Although the models differ from each other in regard to
philosophy, assessment techniques, and range of responsibilities, the overall aims of CM
are to attain the ill client’s goals.

Case Management/SMI 9
Björkman & Hansson (2000) reported that individuals with SMI are in need of
CM services that offer more than brokerage services and coordination. More recently
these authors investigated changes over six years of follow-up with regards to symptoms,
need for care, psychological functioning, quality of life, and social networks, using CM
services for individuals with SMI. This study found improvements in a number of clinical
aspects, quality of life, and social networks, as well as a decrease in use of psychological
services during the follow-up period (Björkman & Hansson, 2007).
Medication noncompliance is found in over half (55%) of individuals with SMI,
especially those who have been diagnosed with schizophrenia. These individuals have
significant difficulty following treatment recommendation (Fenton, Blyler, & Heinssen,
1997; Weiden et al, 1991, as cited in Pratt & Mueser, 2004). Several studies indicated
that a number of factors raise barriers to medication adherence, including substance
abuse, recent alcohol use, history of aggressive behavior, less education, prior treatment
with antidepressants, higher positive and negative total score, and paranoia about
medications (Ascher-Svanum, Zhu, Faries, Lacro, & Dolder, 2006; Chandler, Meisel, Hu,
McGowen, & Madison, 1997; Hudson et al., 2004). Poor insight about illness or disliking
the side effects of medications also contributes to medication noncompliance (NIMH,
2007). Pratt and Mueser (2004) reported that elevated symptoms levels, functional
impairments, and readmission to hospitals also cause poor medication compliance.
Co-morbid medical conditions (CMC) may contribute to outcomes of social and
role-functioning of individuals with SMI (Dixon, Postrado, Delahanty, Fisher, &
Lehman, 1999). Co-morbid medical conditions are commonly seen among mentally ill
persons (Sokal, et al. 2004). Researchers found that people with schizophrenia with poor
Case Management/SMI 10
social and role functioning are more vulnerable to relapse and often have poor outcomes
(Penn, Mueser, Spaulding, Hope, & Reed, 1995, as cited in Pratt & Mueser, 2004). There
are a number of areas in which it is necessary to be assessed with regards to social and
role dysfunctions, such as interpersonal relationships, social problem solving, use of
leisure time, grooming and hygiene, care of personal possessions, money management,
and conflict resolution (Bellack, Mueser, Gingerich, & Agresta, 1997; Mueser & Sayers,
1992, as cited in Pratt & Mueser, 2004).
Mueser, Bond, and Drake (2001) reviewed treatment outcomes in community-
based treatment for SMI. They indicated that community interventions can improve the
long-term outcomes of these psychiatric illnesses. These interventions include Assertive
Community Treatment (ACT), family intervention, supported employment, skills
training, illness self-management, cognitive interventions (cognitive therapy for
psychosis and cognitive rehabilitation), and treatment for dual diagnosis disorders.
According to the authors, the ACT model, one of the CM models that has been
articulated, is applied to those who have SMI and are noncompliant with treatment or for
other reasons have failed to use clinical mental health services. Mueser, Bond, and Drake
(2001) reported that the positive effects of the ACT model were decreases in the use of
hospitalization in 61% of the studies (14/23); improvement in housing stability in 75%
(9/12); significant decreases in symptoms in 50% (8/16); and improved quality of life in
54% (7/13). The ACT model did not do well in increasing social adjustment and work;
for instance vocational functioning increased in only 38% of the studies (3/8).
Studies of gender difference related to demographics and clinical characteristics
with schizophrenia have been conducted widely. Individuals with schizophrenia did not
Case Management/SMI 11
differ in terms of age, ethnicity, and education, as well as clinical characteristics
(Lindamer, Lohr, Harris, McAdams, & Jeste, 1999). But little is known with respect to
outcomes of CM services and gender difference between men and women affected by
SMI.
Policy Analysis
The Community Mental Health Centers Act (CMHC) was passed under Public
Law 88-164, Title II (NIH, n.d.). Overall, the CMHC Act of 1963 gave attention to
people in need of mental health services. Section 203 of this law states that all the states
must establish “…community mental health services needed to provide adequate mental
health services for persons residing in a State” (NIH, n.d., p. 291). After it was enacted,
the CMHC Act played a crucial role in serving individuals with mental illnesses in
communities.
Grob (2000) indicated that mental health policy in the United States has shifted
from mental hospitals to mental health clinics in communities. He pointed out that the
numbers of CMHC in United States grew sharply during the last 50 years. During the
1930’s, approximately 80% of mental hospital beds in Massachusetts were occupied by
patients with long-term care needs (Dayton, 1940, as cited in Grob, 2000). But after the
1960’s, individuals with SMI received short and intermediate-term care and treatment at
mental hospitals (Kramer, 1976, as cited in Grob, 2000). In general, the law requires that
only persons with mental illness who are dangerous to themselves or to others will be
sent to the state hospital. This also would mean that others could benefit from therapeutic
interventions at community mental health clinics (Grob, 2000).
Case Management/SMI 12
The Commonwealth of Massachusetts Regulations (CMR) 104, section 29.00 of
Department of Mental Health (DMH) provides clearly in its scope that it “applies to the
initiation and provision of DMH continuing care services to clients in community
programs …” in which the purpose of “…DMH continuing care services are provided in
the community to adults with serious and long term mental illness …” (DMH, 1999, p.
383).
Under Section 29.04 of 104 CMR 29.00, case management services should be
provided to individuals who are eligible (some or all) through clinical criteria for DMH
continuing care services. In order to meet the clinical criteria for DMH continuing care
services, an adult individual must have mental illness that:
1. includes a substantial disorder of thought, mood, perception,…
2. has lasted, or is expected to last, at least one year; and
3. has resulted in functional impairment…
4. meets diagnostic criteria specified within the current edition of Diagnostic and
Statistical Manual of Mental Disorders,… (DMH, 1999, p. 385).
According to 104 CMR, case management services include but are not limited to
comprehensive assessment of service needs, developing and reviewing the individual
service plan, and coordinating services and (or) monitoring the coordination of DMH
continuing care services provided to individuals with mental illness. The comprehensive
assessment of service needs can be found under Service Planning, in section 29.06.
In more than 460 pages written in 104 CMR, this regulation appears not to
address the degree or qualifications of a case manager. In addition, this regulation does
not provide information about training programs that might be available prior to an

Case Management/SMI 13
individual’s becoming a case manager, or training programs that might be in place while
an individual is in the position. In terms of gender diversity in the workplace, this
regulation fails to discuss any balance between male and female case managers.
According to the Quality Improvement (QI) Policy and Procedure Manual of the
Fellowship Health Resources, Inc. (FHR), comprehensive treatment planning guidelines
are developed with the client, based on areas of need, goals, and desires that have been
identified from the assessment process (FHR, 2007). This policy also states that “staff
(mental health counselors) should be creative in the treatment planning process and work
with the client to incorporate their preferences in developing goals, objectives, and
interventions” (FHR, 2007, p. 8). A case manager at FRN is employed under the title as
mental health counselor.
In 2005, the Fellowship implemented a new clinical approach, called the PRISM
model, which is comprised of core elements, including Person-Centered, Respectful,
Individualized, Strengths-Based and Mission-Driven. The model serves as the principal
key for clinical practices, including case management services. For instance, Person-
Centered aspects assume the inherent individuality and goodness of all people and a
treatment plan that reflects individual needs and preferences (FHR, 2006).
Although the QI policy and the PRISM model attempt to provide a comprehensive
view of treatment planning for individuals with SMI, both seem not to realize that it is
very important to assess the help needed and help received at FRN. A study conducted by
Crane-Ross, Roth, and Lauber (2000) had discussed on the importance of increasing
consensus between consumers and case managers readings needs. This means treatment
planning may not accomplish its goals based solely on the preferences of the client.

Case Management/SMI 14
Furthermore, the policy of FHR at FRN fails to indicate how a case manager is able to
assess for help that might be needed, for instance using Axis IV of Diagnostic of
Statistical Manual IV-TR (DSM, 2000).
In addition, Fellowship Health Resources at FRN has implemented its protocol of
medication administration based on medication step procedures. The medication step
procedures can be reviewed in Appendix C. The medication step procedures are offered
as part of the Medication Administration Program (MAP) policy manual of the
Commonwealth of Massachusetts foe the DMH, Department of Public Health, and
Department of Mental Retardation (MAP, 2007).
Although the medication step procedure is a core intervention in CM services at
FRN, this procedure has never been examined for effectiveness. This procedure was
never tested for compliance before implementation. Also, this procedure has no known
reliability and validity.
For years, numbers of studies related to SMI have been conducted nationwide. To
date, however, there has been little knowledge available in social work literature in
regard to types of case management and their outcomes provided for individuals with
SMI, in particular people with schizophrenia (Bernstein & Rose, 1991; Björkman &
Hansson, 2000, 2002, 2007; Phillips, 2003; Rubin, 2004). This study analyzed case
management services delivered to individuals with SMI at the mental health community-
based clinic known as Fall River Network (FRN) in Fall River, Massachusetts. The Fall
River Network, one of the Fellowship Health Resources’ programs, has offered case
management services for individuals with SMI, through community and residential
Case Management/SMI 15
programs, including Harbor Hill, Meadow Street, Pleasant Street, and Fulton Street, using
the PRISM model (FHR, 2006).
The Fellowship has provided both clinical and support services to people
recovering from mental illness, co-occurring disorders, and other life challenges in seven
states, including Rhode Island, Massachusetts, Maine, Delaware, Virginia, Pennsylvania,
and North Carolina. Since 1975, the Fellowship has helped many thousands of people
begin new lives of dignity and purpose, and it has developed creative solutions for
rebuilding lives and restoring hopes to the recovery of the serious mental illness (FHR,
n.d.).
Conceptual Framework
Case management is mandatory for individuals with mental illness in order to
provide help to them. However, little about outcomes or effects of case management
services for SMI is described in the literature.
Three primary research questions guided this research study. First, what types of
case management services were provided to clients at FRN? Second, what outcomes
accrued to clients who received case management services? And last, were there any
differences in intervention services or outcomes related to the demographics of the
sample?
Specifically, the study examined the following:
• Demographics of the study sample (i.e. gender, age, race, marital status, level of
education) and case managers (i.e. gender, age, level of education, and year of
service in FRN).
Case Management/SMI 16
• History of illness of individuals with SMI (i.e. age of onset of illness, frequency
of hospitalizations in the past 10 years and two years, DSM-IV-TR diagnosis,
number of co-morbid medical conditions, and prescribed medications).
• Case management services provided during the last 9 consecutive months (i.e.
medication independence, social and role functioning (daily living skills,
household maintenance, and health maintenance), socialization, insight regarding
illness, money management, and occupational functioning).
• Effects or outcomes of case management, looking at progress in achieving the
client’s treatment goals over time at 3-months (CM-3), 6-months (CM-6) and 9-
months (CM-9) of CM.

Case Management/SMI 17
Methods
Research Design
This research study utilized a descriptive and exploratory design to examine the
outcomes of case management for individuals with SMI at FRN of the Fellowship in Fall
River, Massachusetts. Specifically, this was a case-level research design using a
retrospective method. This means that all cases that met the inclusion criteria of the study
were reviewed based on a case report form designed for the purposes of this research.
Those eligible for inclusion in this study were adult individuals diagnosed with SMI who
had received case management services for nine consecutive months prior to December
30, 2007, either in the community program (South or North) or group home facilities of
the FRN.
Sampling
The unit of analysis in this study was at the individual level. It included
individuals with SMI, who had been active in the programs during the nine consecutive
months prior to December 30, 2007, at FRN in Fall River, Massachusetts. This purposive
sample was recruited from patient records (hard copies and electronic files). By January
2008, there were 95 individuals with SMI who had been receiving services at FRN. Of
these, 80 (84%) were active clients who met the inclusion criteria of this research,
including 48 men (60%) and 32 women (40%) (See Appendix A for a description of the
sample). A purposive sample was suitable for this research study but the results may lack
Case Management/SMI 18
generalizability. The sample was taken from one facility and was cross-sectional in
nature. However, this was an exploratory study, so no attempt was made to infer or
describe causation.
Data Collection
The data were retrieved from the patient records at FRN of the Fellowship in Fall
River, Massachusetts, between January and February 2008. A case report form was
developed for research study purposes. The form included 36 primary items and 51 sub-
items. The case report form is divided into three sections: demographics, history of
illness, and case management activities (See Appendix B for a copy of the form). The
demographic section includes basic information about clients and case managers. The
history of illness section primarily addresses the individual’s diagnosis of SMI and
relevant information related to the disorders. The case management section is focused on
two parts, type of case management services and outcomes of services.
Most questions in the case report form used nominal level of measurement, for
instance “Yes=1, No=2” or “Single=1, Married=2, Divorced=3, Widowed=4,
Separated=5.” An ordinal level scale (from 0 to 3) was used for measuring the objectives
of the treatment goal. Zero (0) means the object was dropped out or cancelled from the
treatment plan. One (1) means the objective was not met or required further interventions
or actions in order to accomplish the needs. Two (2) means the objective was ongoing,
continued, or the individual was making progress toward a current goal, but had no
evidence of moving to a higher goal. Three (3) means the objective was met, and there
was preparation or consideration of a higher goal.
Case Management/SMI 19
As stated earlier, the case report form was administered to retrieve individual
information, using hard copies and electronic files. Data were collected at the FRN office,
1700 President Ave., and group home facilities Harbor Hill and Pleasant Street, Fall
River, MA. Records of all individuals who met inclusion criteria were carefully examined
three times, CM-3, CM-6, and CM-9. Individual case manager information was drawn
from the organization’s Human Resources database. Because the case report form was
created for this study, its reliability and validity are not known. However, the form was
reviewed by experienced peers before implementation. The content of the questions
became much more clear in that process. The form used simple language, short questions
and no double-barreled or negative questions. Its closed-ended questions elicited data on
issues that would have required interpretation in a more open-ended format.
Limitations
Due to the nature of this research design, which did not have randomization, this
study is limited by selection bias. The sample was purposive. It was a cross-sectional
study with no control or comparison group. There was no way to know if the sample was
similar to the entire population of clients who have received case management services at
FRN, or to any other population of people with SMI.
The study also was limited by history and maturation. There is no way to know
the effects of prior treatment experiences of clients who were in the study. Nor is there a
way to know the effects of growth and development in the lives of these clients.
Case Management/SMI 20
Instrumentation effects also limited the study. However, the internal validity of
this research study may be increased by improving measurement error in the instrument
as discussed above.
The external validity of this research study is unknown, though the purposes of
this research study were stated in a clear manner, ensuring that only relevant data were
obtained to meet the study aims. The case report form kept sensitive questions to a
minimum. Also, because it was a retrospective study using administrative data, there
were no threats as a result of socially desirable responses. In addition, only relevant
questions were used to retrieve information for research study purposes.
Ethical Issues
This study was exempt from oversight by the Institutional Review Board (IRB) of
Rhode Island College. It examined only client records without access to personal
identification of clients or case managers, such as individual names, individual social
security numbers, and client record numbers.
However, the research study had to meet the privacy standards of the Health
Insurance Portability and Accountability Act before access to patient records was
permitted. The researcher assured that clients were informed that there personal data
could be used for evaluation or research purposes.
All the data and information related to client records is stored in a safe and locked
place at the researcher’s home, where only the researcher can access the materials. All the
data and information regarding this study will be destroyed three years after the study’s
completion. The National Association of Social Workers Code of Ethics states,
Case Management/SMI 21
“...evaluation or research should carefully consider possible consequences and should
follow guidelines developed for the protection of evaluation and research participants”
(NASW, Code of Ethics, 1996, as cited in Reamer, 1999, p. 156-7).
Data Analysis
The data were double checked to ensure the quality of data entry. The data were
then entered directly into SPSS for Windows version 15.0 for data analysis. Data analysis
was performed at different levels.
First, descriptive analysis was the major analytic method for this research study,
including frequencies, measures of central tendency, and cross tabs. Specifically,
descriptive analysis was utilized to provide the distribution of demographics of
individuals with SMI and case managers. Also, descriptive analysis was performed to
present the distribution of history of illness and case management services. Second,
crosstabs analyses were generated for comparing the differences in demographics of
individuals with SMI; the demographics of individuals with case managers; clinical
characteristics; and case management services for men vs. women). Also the crosstabs
analyses were utilized for comparison of the trends in hospitalization among men and
women.
Additionally, independent samples t-tests were utilized to compare ratio variables,
including age, age at illness onset, and duration of being in the programs. Also, a paired
sample t-test was utilized to compare the means of frequent hospitalizations during the
past 10 years and 2 years. A p value ≤.05 was considered a statistically significant test
and was based on Pearson Chi-square of 2-sided, Likelihood ratio, or 2-tailed t-test.
Case Management/SMI 22
Finally, in-depth data analysis was generated to examine the outcomes of case
management. This research study measured the outcomes of case management, using the
formula of Cohen’s d to assess the effect at CM-3, CM-6 and CM-9. The direction of
outcomes of case management was measured based on the effect size of Cohen’s d,
testing the strength of the relationship between two variables (gender and each type of
case management).
d = MeanMale – MeanFemale / SDpooled,
Where SDpooled = √[(SDMale2 + SDFemale
2) / 2].
The effect of the relationships was interpreted where 0.2 is indicative of a small
effect, 0.5 means a medium, and 0.8 or higher is a large effect size (Becker, 2000).

Case Management/SMI 23
Results
Results are presented according to gender as early analyses had indicated that
gender appeared to provide a mechanism for organizing the data.
Demographics of Individuals with Serious Mental Illness & Case Managers
Program Participants with Serious Mental Illness
The distribution of individuals with SMI demographics is shown in Table 1
below. The 80 individuals in this study ranged in age from 26 to 70 years. The mean age
(SD) of the women was 4.5 years older than that of the men, 52.1 years (9.7) vs. 47.6
years (9.4), p = .05, respectively. The gender ratio between men and women was 1.5:1. In
this study, the majority of consumers (90%) were white. Males were more likely to be
single than females, 73% vs. 56%, respectively. Only a few (6%) had an associate’s or
higher degree. Many (67%) in this sample received Supplemental Security Income. Less
than half (44%, 43%) of individuals with SMI had either Medicaid or a combination of
Medicaid and Medicare, respectively.
Table 1. Demographics of Individuals with Serious Mental Illness Characteristics Total Males Females n = 80 (%) n = 48 (%) n = 32 (%) χ2 (t)
Age: Mean (SD) 49.4 (9.7) 47.6 (9.4) 52.1 (9.7) (-2.03)* Race
Asian 6 (8) 3 (6) 3 (10) 5.3 White 71 (90) 45 (94) 26 (84) Black 2 (2) - 2 (6) Missing 1 - 1
Marital Status Single 53 (66) 35 (73) 18 (56) 4.3 Married 4 (5) 2 (4) 2 (6) Divorced 16 (20) 9 (19) 7 (22) Widowed 1 (1) - 1 (3) Separated 6 (8) 2 (4) 4 (13)
Sexual Orientation Heterosexual 75 (98) 47 (100) 28 (94) 3.2 Bisexual 1 (1) - 1 (3) Gay/Lesbian 1 (1) - 1 (3) Missing 3 1 2

Case Management/SMI 24
(10)
(18) (20)(13)
(9) (10)
0
10
20
30
40
50
South North Group Home
Program in Services
Prop
ortio
n of
Clie
nts
(n)
Male (n=48) Female (n=32)
Characteristics Total Males Females n = 80 (%) n = 48 (%) n = 32 (%) χ2 (t)
Level of Education
No HS 39 (53) 24 (57) 15 (47) 3.3 HS/GED 30 (41) 17 (41) 13 (41) Associate 4 (5) 1 (2) 3 (9) Bachelor 1 (1) - 1 (3) Missing 6 6 -
Insurance Types Medicaid 35 (44) 19 (40) 16 (50) 4.7 Medicare 4 (5) 3 (6) 1 (3) Medicaid/care 35 (43) 23 (48) 12 (38) No Insurance 2 (3) 2 (4) - Others 4 (5) 1 (2) 3 (9)
Source of Income SSI 52 (67) 31 (66) 21 (68) 1.7 SSDI 20 (26) 11 (24) 9 (29) SSI/SSDI 5 (6) 4 (8) 1 (3) Other 1 (1) 1 (2) - Missing 2 1 1
Being in Services (Month) Mean (SD) 76.8 (50.5) 68 (51.4) 90 (46.7) (-1.98)*
Note: HS, High School; GED, General Equivalence Diploma; SSI, Supplemental Security Income; SSDI, Social Security Disability Benefits. *p = .04; .05 (t-test, 2-tailed). Source: Study data; Analysis: Phan Sok.
Overall, the mean (SD) length of stay in the program among men was shorter than
for women, 68 months (51.4) vs. 90 months (46.7), p =.05. Figure 1 shows the proportion
of consumers scattered in each program.
Figure 1. Consumers in Different Programs at Fall River Network
Case Management/SMI 25
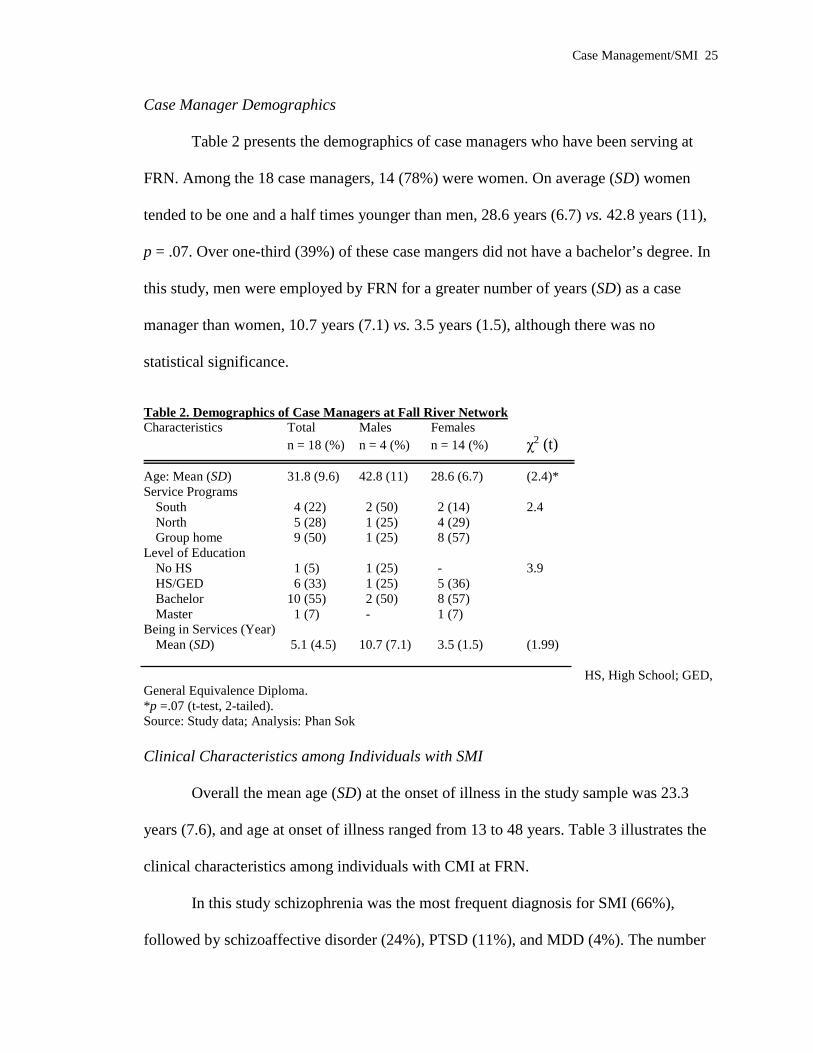
Case Manager Demographics
Table 2 presents the demographics of case managers who have been serving at
FRN. Among the 18 case managers, 14 (78%) were women. On average (SD) women
tended to be one and a half times younger than men, 28.6 years (6.7) vs. 42.8 years (11),
p = .07. Over one-third (39%) of these case mangers did not have a bachelor’s degree. In
this study, men were employed by FRN for a greater number of years (SD) as a case
manager than women, 10.7 years (7.1) vs. 3.5 years (1.5), although there was no
statistical significance.
Table 2. Demographics of Case Managers at Fall River Network Characteristics Total Males Females n = 18 (%) n = 4 (%) n = 14 (%) χ2 (t)
Age: Mean (SD) 31.8 (9.6) 42.8 (11) 28.6 (6.7) (2.4)* Service Programs
South 4 (22) 2 (50) 2 (14) 2.4 North 5 (28) 1 (25) 4 (29) Group home 9 (50) 1 (25) 8 (57)
Level of Education No HS 1 (5) 1 (25) - 3.9 HS/GED 6 (33) 1 (25) 5 (36) Bachelor 10 (55) 2 (50) 8 (57) Master 1 (7) - 1 (7)
Being in Services (Year) Mean (SD) 5.1 (4.5) 10.7 (7.1) 3.5 (1.5) (1.99)
HS, High School; GED,
General Equivalence Diploma. *p =.07 (t-test, 2-tailed). Source: Study data; Analysis: Phan Sok Clinical Characteristics among Individuals with SMI
Overall the mean age (SD) at the onset of illness in the study sample was 23.3
years (7.6), and age at onset of illness ranged from 13 to 48 years. Table 3 illustrates the
clinical characteristics among individuals with CMI at FRN.
In this study schizophrenia was the most frequent diagnosis for SMI (66%),
followed by schizoaffective disorder (24%), PTSD (11%), and MDD (4%). The number

Case Management/SMI 26
of men diagnosed with schizophrenia was slightly higher than women, 69% vs. 63%,
respectively. Types of schizophrenia and schizoaffective disorders are shown in Figures 2
and 3, respectively.
Table 3. Clinical Characteristics among Individuals with Serious Mental Illness Characteristics Total Males Females n = 80 (%) n = 48 (%) n = 32 (%) χ2 (t)
Age onset illness (n=63)
Mean (SD) 23.3 (7.6) 22.3 (7) 24.2 (8.4) (-.75) Axis I 80 (100) 48 (100) 32 (100)
Schizophrenia 53 (66) 33 (69) 20 (63) .33 Schizoaffective disorder 19 (24) 12 (25) 7 (22) .1 Bipolar I 1 (1) - 1 (3) MDD 3 (4) 3 (6) - PTSD 9 (11) 4 (8) 5 (17) 1 OCD 2 (3) 1 (2) 1 (3) Others 14 (18) 9 (11) 5 (6)
Axis II 13 (16) 8 (17) 5 (16) Axis III 68 (85) 42 (88) 26 (81)
Nervous diseases 9 (12) 6 (13) 3 (10) .13 Endocrine diseases 41 (53) 30 (64) 11 (37) 5.4* Respiratory diseases 19 (25) 13 (28) 6 (20) .57 Digestive diseases 25 (33) 12 (26) 13 (43) 2.6 Cardiovascular diseases 10 (13) 6 (13) 4 (13) Skeletal diseases 5 (7) 2 (4) 3 (11) Nutritional diseases 13 (17) 8 (17) 5 (17)
Axis IV 79 (99) 47 (98) 32 (100) PEP 72 (91) 44 (94) 28 (88) .88 Others 7 (9) 3 (6) 4 (13)
Axis V (n=57)** Mean (SD) 54.7 (9.3) 52.9 (8.4) 57.3 (10.2) (-1.7)
MDD, Major Depression Disorder; PTSD, Posttraumatic Stress Disorder; OCD, Obsessive Compulsive Disorder; PEP, Psycho-environmental Problems. Others: Alcohol abuse, n = 2 (14%); alcohol dependent, n = 3 (21%); ADHD, n = 1 (7%); cocaine dependent, n = 1 (7%); poly-substance abuse, n = 3 (21%); poly-substance dependence, n = 1 (7%); and dementia not otherwise specified, n = 3 (21%). Axis II: Antisocial personality disorder and mild retardation. Axis III: Based on DSM-IV-TRTM. Nervous diseases: Head trauma, insomnia, seizure, and sleep apnea. Endocrine diseases: Diabetes Type I or II, hypercholesterolemia or lipidemia, and hypothyroids. Respiratory diseases: Asthma and chronic obstructive pulmonary disease. Digestive diseases: Gastritis, gastro-esophageal reflux disease, irritable bowel syndrome, and hepatitis B or C. Cardiovascular diseases: Atrial fibrillation and hypertension. Skeletal diseases: Arthritis. Nutritional diseases: Obesity. *p = .02 (Chi-square, 2-sided). **p = .008 (Likelihood ratio). Source: Study data; Analysis: Phan Sok.

Case Management/SMI 27
6%
60%
8%
26%
Disorganized Paranoid Residual Undifferentiated
90%
10%
Bipolar Depressive
Many (85%) individuals with SMI also were diagnosed on Axis III. The most
frequently occurring general medical conditions were endocrine diseases (53%), followed
by digestive diseases (33%), respiratory diseases (25%), nutritional diseases (17%),
cardiovascular disease (13%), and nervous diseases (12%). Men in this study were
Figure 2. Type of Schizophrenia among Individual with Serious Mental Illness
Figure 3. Type of Schizoaffective Disorders among Individual with Serious Mental Illness
more likely to be diagnosed with endocrine diseases than women, 64% vs. 37%, p = .02.
Overall, the Likelihood ratio of average (SD) GAF score among men was lower than that
of women, 52.9 (8.4) vs. 57.3 (10.2), p = .008. Additionally, a higher proportion of men

Case Management/SMI 28
(12)
(17)
(7)(6)
(13)
(7)
(2)(4)
0
10
20
30
40
50
60
One Two Three Four or more
Co-morbid Medical Conditions
Prop
ortio
n of
Clie
nts
(n)
Male (n=42) Female (n=26)
had two or more co-morbid medical conditions (CMC) than women, 71% vs. 50%, (Chi-
square = 3.2) p = .07, respectively. The number of CMC is shown in Figure 4.
Figure 4. Number of Co-morbid Medical Conditions Case Management Services and Outcomes at Fall River Network
The most frequent case management service was medication independence (93%),
followed by health maintenance (74%), socialization (36%), household maintenance
(21%), daily living skills (18%), and money management (16%). Case management
services are shown in Table 4.
Table 4. Case Management Services Provided by Fall River Network Characteristics Total Males Females n = 80 (%) n = 48 (%) n = 32 (%) χ2
Medication independence 74 (93) 44 (92) 30 (94) .34 Daily living skills 14 (18) 10 (21) 4 (13) .33 Household maintenance 17 (21) 10 (21) 7 (22) .91 Health maintenance 59 (74) 35 (73) 24 (75) .83 Socialization 29 (36) 19 (40) 10 (31) .44 Money management 13 (16) 6 (13) 7 (22) .26 Occupational functioning 7 (9) 4 (8) 3 (9) - Family environment 1 (1) 1 (2) - - Others 16 (20) 10 (20) 6 (19) -
Note: Others: Attain citizenship, n = 1; discharge planning, n = 4; health lifestyle, n = 1; hygiene, n = 2; nutrition, n = 1; self-esteem, n = 1; smoke cessation, n = 1; stress management, n = 1; substance abuse, n = 1; transportation, n = 2; and sobriety, n = 1. Source: Study data; Analysis: Phan Sok
Case Management/SMI 29
(3)
(12)(14)(15)
(2)
(12)
(10)
(6)
05
1015202530354045
Step 1 Step 2 Step 3 Step 4
Medication Steps
Prop
ortio
n of
Clie
nts (
n)
Male (n=44) Female (n=30)
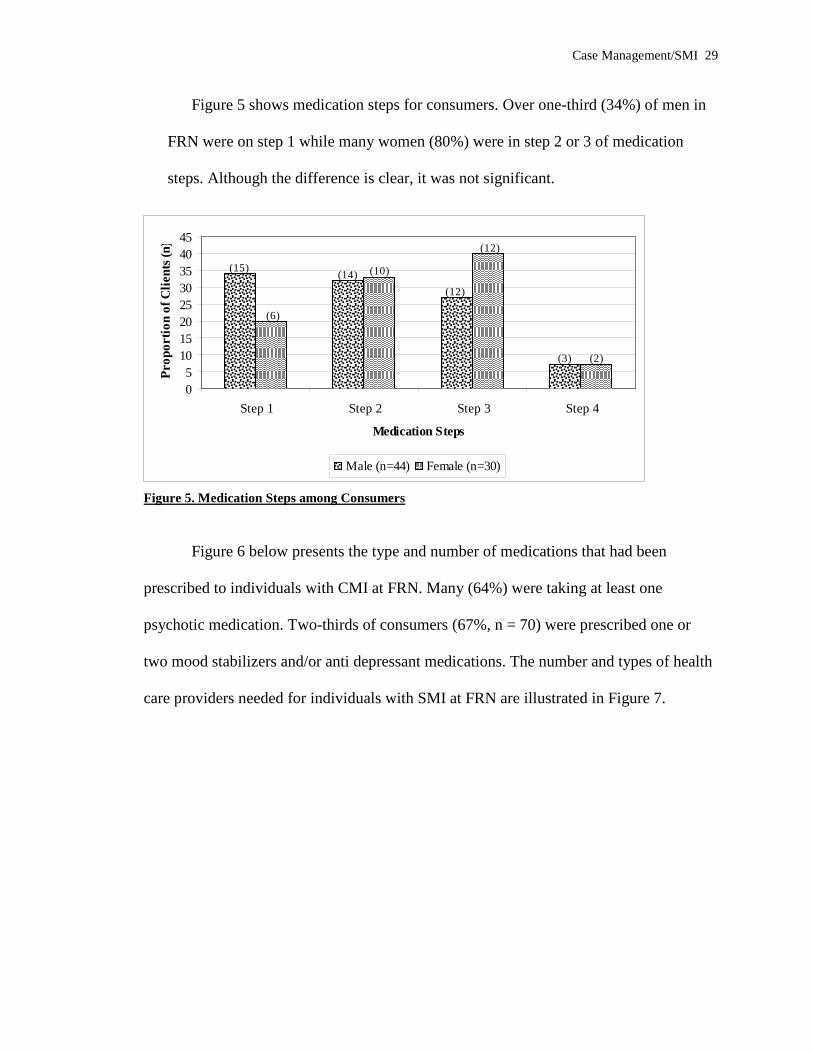
Figure 5 shows medication steps for consumers. Over one-third (34%) of men in
FRN were on step 1 while many women (80%) were in step 2 or 3 of medication
steps. Although the difference is clear, it was not significant.
Figure 5. Medication Steps among Consumers
Figure 6 below presents the type and number of medications that had been
prescribed to individuals with CMI at FRN. Many (64%) were taking at least one
psychotic medication. Two-thirds of consumers (67%, n = 70) were prescribed one or
two mood stabilizers and/or anti depressant medications. The number and types of health
care providers needed for individuals with SMI at FRN are illustrated in Figure 7.

Case Management/SMI 30
020406080
100120
One ≥Two One ≥Two One Two ≥Three
Psychiastrist (n=80) PCP (n=80)
Specialist (n=57)
Health Care Providers
Prop
ortio
n of
Clie
nts
Male Female
010203040506070
One Two ≥Three One Two ≥Three One toFour
Five toSeven
≥Eight
Antipsychotics (n=78) Mood stabilizers/Anti-depressants (n=70)
Nonpsy meds (n=76)
Medications
Prop
ortio
n of
Clie
nts
Male Female
Note: Antipsychotics: i.e. Abilify, Risperdal/Risperdal Consta, Seroquel, Prolixin, Trilafon, & Zyprexa. Mood stabilizers/Anti depressants: i.e. Depakote, Effexor, Lamictal, Lithium, Luvox, Tegretol, Celexa, Lexapro, Paxil, Wellbutrin, Zoloft, Prozac, Cymbalta, Clonazepam, Lorazepam, & Ativan. Nonpsychiatric medications: (Exclusion) Topical cream/lotion, Inhalers, Laxative, Oral hygiene, Treatment for narcotic addiction, Antibiotics, & Cough medications. Figure 6. Number and Differential Medication Regimens Prescribed to Consumers †
Figure 7. Health Care Providers Needed among Consumers Outcomes of CM services for individuals with SMI at FRN are shown in Table 5.
I computed between-group effect sizes, comparing the males and females at CM-3, CM-
6, and CM-9, based on Cohen’s d formula:
d = MeanMale – MeanFemale / SDpooled
Where SDpooled = √[(SDMale2 + SDFemale
2) / 2]

Case Management/SMI 31
-2
-1.5
-1
-0.5
0
0.5
1
CM-3 CM-6 CM-9
Outcomes of Case Management Services
Mea
n C
hang
ed O
ver P
erio
d of
Ti
mes
Medication Independence Health Maintenance Socialization
Household Maintenance Money Management
Table 5. The Effect of Outcomes of Case Management Services Between Group Effect Case management† CM-3 CM-6 CM-9 Size Based on M (SD) M (SD) M (SD) Cohen’s d: CM-3 CM-6 CM-9 Medication independence (n=48)
Female 1.9 (.43) 1.85 (.28) 1.8 (.43) -.2 .2 .1 Male 1.83 (.26) 1.89 (.26) 1.83 (.48)
Health maintenance (n=36) Female 1.61 (.33) 1.5 (.33) 1.6 (.5) .1 .7 .5 Male 1.63 (.5) 1.7 (.28) 1.8 (.29)
Socialization (n=18) Female 1.44 (.44) 1.59 (.43) 1.55 (.67) -.1 -.4 -.4 Male 1.41 (.66) 1.37 (.61) 1.26 (.78)
Household maintenance (n=12) Female 1.67 (.42) 1.56 (.5) 1.61 (.33) -.6 .2 .2 Male 1.34 (.74) 1.67 (.42) 1.69 (.44)
Money management (n=8) Female 2 (.0) 2 (.0) 1.9 (.17) -.7 -1.6 -1.2 Male 1.92 (.17) 1.5 (.43) 1.5 (.43)
†Sample size is varied as individuals have received different types of services. Source: Study data; Analysis: Phan Sok
Overall, based on CM-6, the effect size for medication independence and
household maintenance indicated of a small effect (.2), while health maintenance showed
a medium effect (.7) at the same period. The outcomes of CM services are shown in
Figure 8.
Figure 8. Outcomes of Case Management Services at FRN over Period of Time
Case Management/SMI 32
(6)(4)
(13)
(6)
(16) (19)
(12) (7)(5)
(2)
(6)
(16)
(11)
(3)
0
20
40
60
80
0 Time 1 Time 2 Times ≥3 Times 0 Time 1 Time 2 Times ≥3 Times
Admission in past 10Ys (n=59) Admission in past 2Ys (n=67)
Prop
ortio
n of
Clie
nts (
n)
Male Female
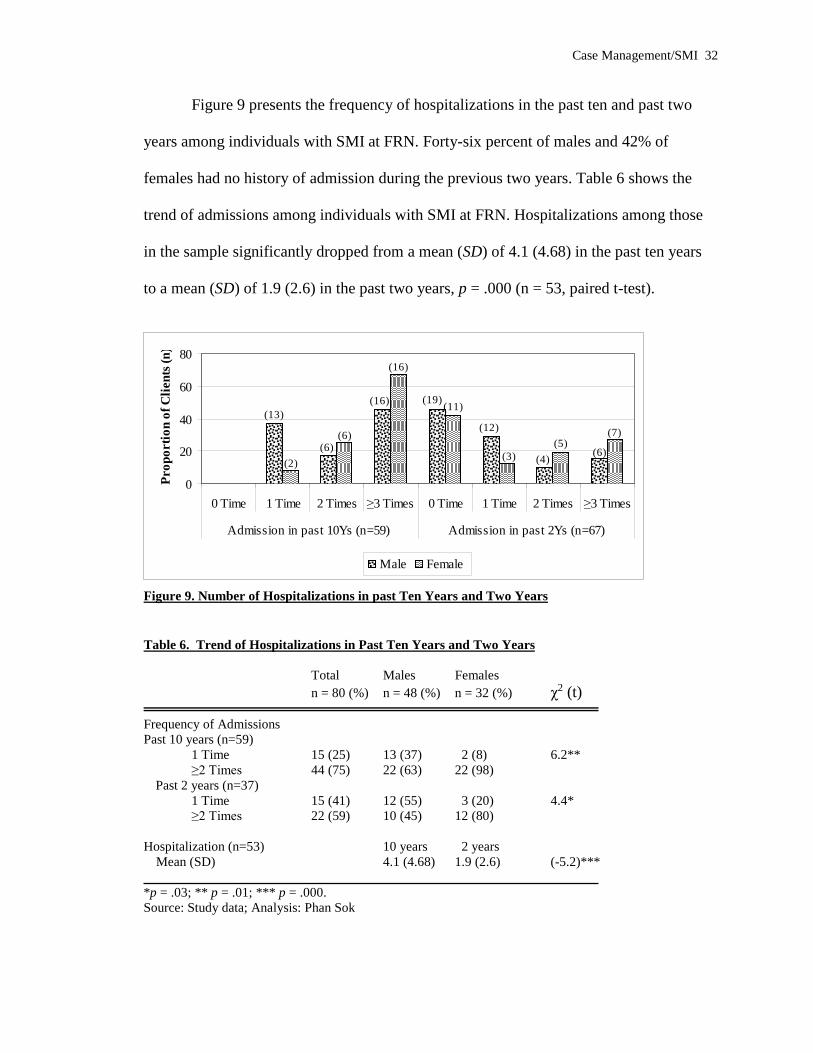
Figure 9 presents the frequency of hospitalizations in the past ten and past two
years among individuals with SMI at FRN. Forty-six percent of males and 42% of
females had no history of admission during the previous two years. Table 6 shows the
trend of admissions among individuals with SMI at FRN. Hospitalizations among those
in the sample significantly dropped from a mean (SD) of 4.1 (4.68) in the past ten years
to a mean (SD) of 1.9 (2.6) in the past two years, p = .000 (n = 53, paired t-test).
Figure 9. Number of Hospitalizations in past Ten Years and Two Years Table 6. Trend of Hospitalizations in Past Ten Years and Two Years
Total Males Females
n = 80 (%) n = 48 (%) n = 32 (%) χ2 (t)
Frequency of Admissions Past 10 years (n=59) 1 Time 15 (25) 13 (37) 2 (8) 6.2** ≥2 Times 44 (75) 22 (63) 22 (98)
Past 2 years (n=37) 1 Time 15 (41) 12 (55) 3 (20) 4.4* ≥2 Times 22 (59) 10 (45) 12 (80)
Hospitalization (n=53) 10 years 2 years
Mean (SD) 4.1 (4.68) 1.9 (2.6) (-5.2)***
*p = .03; ** p = .01; *** p = .000. Source: Study data; Analysis: Phan Sok
Case Management/SMI 33
Summary
In this study, CM services included medication independence (93%), health
maintenance (74%), socialization (36%), household maintenance (21%), and daily living
skills (18%). Of these, health maintenance showed a medium effect (.7) at CM-6. A
higher proportion of men had two or more CMC than women, 71% vs. 50%, p = .07,
respectively. In addition, the Likelihood ratio of average GAF among men was lower
than women, χ2= 31.1 (df = 15), p = .008. Furthermore, 34% of men were on medication
step 1, while many women (80%) were in medication step 2 or higher, although the
difference was not significant. Overall, differential medication regimens had been
prescribed to individuals with SMI. In addition, the average (SD) number of
hospitalizations dropped from 4.1 (4.68) in the past ten years to 1.9 (2.6) in the previous
two years, p = .000.
Case Management/SMI 34
Discussion
Demographics of Clients and Case Managers
In this cohort, 60% (n=48) of the sample of individuals with SMI were males
(Table 1). Seventy-seven percent (n=14) of the case managers were female. Overall, one-
third of the case managers (36%, n=7) had only a GED or high school degree (Table 2).
Yet, the average amount of time (SD) that clients spent in case management services with
the women was shorter than with the men, 3.5 years (1.5) vs. 10.7 years.(7.1),
respectively.
Overall there were no statistically significant differences between men and
women in this sample with respect to ethnicity, education, sexual orientation, insurance
types, and sources of income (Table 1). At least one earlier study among older
schizophrenia patients (46 to 85 years old) showed that subjects did not differ in regard to
age, education and ethnicity (Lindamer, Lohr, Harris, McAdams, & Jeste, 1999). The
current study found men were more likely to be single, though the difference in status
was not statistically significant. This finding is consistent with an Australian study,
reporting the powerful predictors of early-onset schizophrenia were poor pre-morbid
occupational functioning, single status, and being male (Castle, Sham, & Murray, 1998).
It may also be that because males tend to have an earlier onset of mental illness, they are
more likely to be single (Eaton, 1975, as cited in Pratt & Mueser, 2004).
Clinical Characteristics of Clients
Worldwide studies in schizophrenia have suggested that men tend to have earlier
age of onset than women (Caste, Sham, & Murray, 1998; Gureje, 1991; Leung & Chue,
Case Management/SMI 35
2000; Tang et al., 2007). In Table 3, the mean (SD) age of illness onset among males with
SMI was two years earlier than females, 22 (7.6) vs. 24 (8.4), respectively.
Overall, men and women in the sample with CMI at FRN showed an almost equal
proportion of clinical assessments. Men were more likely to be assessed with
schizophrenia (paranoid) and less likely to be assessed with schizoaffective disorder
(bipolar) than women, 64% vs. 55% and 83% vs. 100%, respectively (Figure 2). However
none of these findings were statistically significant. One study has indicated no
differences in assessment of schizophrenia between men and women (Lindamer, Lohr,
Harris, McAdams, & Jeste, 1999). Tang et al. (2007) concluded that the paranoid subtype
of schizophrenia was less common in males. Diagnosis of paranoid schizophrenia in the
current study was based on assessments completed at the state’s psychiatric practice,
Corrigan Mental Health Center, in Fall River, MA. This points to a limitation in the
current study, as there were no controls for third party assessments in this retrospective
design. However, determining a clinical diagnosis for individuals with SMI at FRN was
not practical considering the culture at the agency.
In terms of CMC, the current study found many (85%) individuals with SMI
presented with CMC. This finding is consistent with studies that showed that persons
with SMI are more likely to have CMC (Carney, Jones, & Woolson, 2006; Sokal et al.,
2004). Individual men at FRN had a higher proportion of two or more of CMC than
women, 71% vs. 50%, p = .07, respectively (Figure 4). Additionally, men were more
likely to have endocrine diseases than females, 64% vs. 37%, p = .02, respectively (Table
3). Dixon, Postrado, Delahanty, Fisher, and Lehman (1999) stated that a greater number
of CMC among males with SMI independently contributes to worse psychotic symptoms,
Case Management/SMI 36
physical health care, and a greater likelihood of a history of a suicide attempt. The results
in the current study highlight that males with SMI were at risk of poorer functional
outcomes, as suggested by Moriarty et al. (2001).
In addition, the finding (Table 1) that men at FRN were likely to be in the
program for a shorter time than women, on average 68 months vs. 90 months, may
indicate that males were delayed in accessing services. This may have occurred because
releases from a hospital and/or referral to community-based mental health outpatient
services were delayed for men. This finding supports the idea that men in this setting may
have poorer functional outcomes (Moriarty et al., 2001). However, once again, it also
reinforces the study limitations of history and maturation.
Case Management Services: Medication Steps,
Differential Medication Regimen Adherence, and Health Services
Crane-Ross, Roth, and Lauber (2000) provided a wide list of case management
services for individuals with SMI. The authors rated the amount of help needed and
amount of help received at community support service programs. The core of case
management services at the Fellowship at FRN included medication independence, health
maintenance, socialization, household maintenance, daily living skills, and money
management (Table 4). These services were mainly driven by the clinical approach called
the PRISM model, designed by the Fellowship Health Resources (FHR, 2006), as well as
the ACT model. Unfortunately, assessment of Axis IV (social and environmental issues)
was not the culture at FRN. The Axis IV data in Table 3 showed that the majority (91%)
of individuals with SMI had psycho-environmental problems. This assessment was based
Case Management/SMI 37
on the Corrigan Mental Health Center’s assessment and it is very limited in detailing the
community support service needs for individuals with SMI at FRN. It highlights the
problem of identifying specific CM service needs in this setting. The limited use of Axis
IV at the Fellowship may explain the missing insights into individual illnesses and CM
services in this setting.
This study found that the majority of the sample (93%) with SMI needed help
with medications, with only a small difference between males and females, 93% vs. 94%,
respectively (Table 4). This finding means that many individuals with SMI were
concerned about medication adherence.
Over half (55%) of individuals with SMI had problems with medication
adherence (Fenton, Blyler, & Heiseen, 1997, as cited in Pratt & Mueser, 2004). The
current study did not have data with respect to medication non-adherence. Many
variables are associated with barriers to medication adherence among individuals with
CMI (Ascher-Svanum, Zhu, Faries, Lacro, & Dolder, 2006; Chandler, Meisel, Hu,
McGowen, & Madison, 1997; Hudson et al., 2004; NIMH, 2007; Pratt and Mueser,
2004). Some have suggested that medication adherence among those with psychosis is
associated with their level of insight into the illness (Droulout, Liraud, & Verdoux 2003,
NIMH, 2007). However, no individuals with SMI at FRN had received treatment
planning regarding insight into their illness during the last nine consecutive months. This
may raise the question of medication adherence as well as the medication step issue.
As stated in the problem statement, the medication step procedures are limited in
assessing how an individual with SMI complies with all medication regimens. Many
(64%-67%) individuals with CMI must take at least one antipsychotic, and/or mood

Case Management/SMI 38
stabilizers and/or an anti-depressant medication at FRN (Figure 5). In addition, roughly
one-third (27%) were put on non-psychiatric medications because of the high proportion
of CMC (85%, Table 3). Thus, it is clear that many individuals with SMI at FRN needed
differential medication regimens.
Many standardize scales for evaluating compliance and attitude toward
medications among individuals with CMI are available (Hogan, Awad, & Eastwood,
1983, Weiden et al., 1994, as cited in Pratt & Mueser, 2004). Piette, Heisler, Ganoczy,
McCarthy, and Valenstein (2007) reported using medication possession ratios to assess
differential medication-regimen adherence, including antipsychotics and nonpsychiatric
medications.
With respect to medication steps, the current study also found that men were less
likely to be in medication step 2 or higher than were women, 66% vs. 80%, ns (Figure 7),
again suggesting that those men may have poorer functional outcomes.
Crane-Ross, Roth, and Lauber (2000) reported that individuals with schizophrenia
had greater needs for and received more assistance with medical and dental care. As
mentioned earlier, some studies have shown that individuals with SMI are more likely to
have CMC (Carney, Jones, & Woolson, 2006; Sokal et al., 2004). Many (74%)
individuals with SMI in the current study needed help with health maintenance through
CM services. The majority (85%) of people in this sample had CMC (Table 3). At least
one study of the use of general medical services found high levels of service use among
clients at outpatient settings, but very low levels of primary and preventive services
among individuals with CMI (Salsberry, Chipps, & Kennedy, 2005).
Case Management/SMI 39
Outcomes of Case Management
Sun, Liu, Christensen, and Fu (2007) estimated that the national re-hospitalization
costs related to medication non-adherence amounted to $1.479 million. Another study
found that there are roughly 87,000 annual acute care inpatient admissions among
Medicaid schizophrenia patients, comprising approximately 930,000 hospital days, and
costing $806 million (Marcus & Olfson, 2008).
Interestingly enough, CM services had some effect on medication independence
(d = .2), health maintenance (d = .7), and household maintenance (d = .2) (Table 5),
particularly at six months. In addition, the current study showed that the admissions trend
rates among individuals with SMI dropped significantly (Table 6), from a mean (SD) of
4.1 (4.68) in the past 10 years to a mean (SD) of 1.9 (2.6) in the past two years, p = .000,
(n = 53). Björkman & Hanson (2007) also found there was a diminishing use of
psychological services during the follow-up period. As reviewed by Mueser, Bond, and
Drake (2001), the effects of the ACT model included decreases in accessing
hospitalization in 61% or 14 of 23 studies.
The findings that men with SMI were more likely to have lower rates of being
admitted two or more times in the past ten and two years compared to women with SMI,
63% vs. 98%, and 45% vs. 80%, p = .01 and p = .03 respectively, may be because women
stayed in the programs for a longer period of time than men, an average of 68 months
(51.4) vs. 90 months (46.7) p = .05 (Table 1).
Case Management/SMI 40
Implications for Policy
The results of the distribution of education among the case managers in this study
suggest that a minimum education level should be specified in the regulation of 104 CMR
in order to strengthen CM services at community mental health organizations. The title of
mental health counselor for a case manager at FRN may require a credential for assuming
counselor roles. The idea of a credential is not stated either in the regulations of 104
CMR nor the Quality Improvement Policy and Procedure Manual of the Fellowship.
In addition, as discussed about CM services, both 104 CMR and the Quality
Improvement Policy and Procedure Manual of the Fellowship should be reviewed to
determine whether assessing for Axis IV is necessary to improve assistance provided to
individuals with SMI. Also, the findings about CMC highlight that the Fellowship at
FRN might consider extending its knowledge about this matter.
Furthermore, a new policy related to differential medication management should
be established at FRN since the current policy of the Fellowship does not address this
issue. Finally, a policy for medication step procedures may be revised or established if
further evaluations suggest doing so.
Implications for Practice and Research
Several implications related to the results of this study are suggested below:
1. The contradictions between clients and case managers with respect to gender, low
level of education, and length of time in case management services at FRN may raise
an issue of effectiveness of CM services. This matter has been raised infrequently in
previous literature. Providing professional knowledge (for instance, collaborating
Case Management/SMI 41
with the Case Management Certificate Program at the School Social Work, Rhode
Island College) for case managers, as well as balancing the issue of gender diversity
at the workplace may enhance the effectiveness of case management. Further study is
needed to investigate in detail whether the case manager and client gender
differences, case manager level of education, and experience in CM have an impact
for case management outcomes.
2. Clinical diagnosis by independent clinicians at FRN should be reviewed regularly and
re-evaluated. Discussion should occur with the Corrigan Mental Health Center in
order to maintain reliability of the diagnosis with other findings.
3. Every effort should be made to encourage effective case management strategies at
FRN, especially with male schizophrenic clients, since the results of this study have
highlighted that men may be at risk of poor social and role functioning.
4. The lack of assessment on Axis IV at FRN may affect CM services as well as goals
and objectives of treatment planning. Axis IV should be assessed at FRN. This study
did not attempt to examine CM service satisfaction in regard to help needed and help
received. Additional studies are needed to investigate this issue.
5. The current study did not investigate factors that might be barriers to medication
independence. Additional studies could examine this issue.
6. This study has insufficient knowledge of the use of general medical services. Further
studies could attempt to gain a more full understanding of this issue at the Fellowship
at FRN.

Case Management/SMI 42
Conclusion
Case management at FRN was shown to be somewhat effective, particularly for
household maintenance. The reduction of admission rates among these individuals
reflects the efforts of programs at FRN that delivered services to individuals with SMI.
However, it is difficult to understand whether the outcomes of CM resulted from the
clinical approach called the PRISM model, the ACT model of CM, or other factors.

Case Management/SMI 43
References Ascher-Svanum, H., Zhu, B., Faries, D., Lacro, J. P., & Dolder, C. R. (2006). A
prospective study of risk factors for nonadherence with antipsychotic medication
in the treatment of schizophrenia. Journal of Clinical Psychiatry, 67,1114-23.
Becker, A. L. (2000). Basic and applied research methods. Retrieved March 5, 2008 from
http://web.uccs.edu/lbecker/Psy590/contentII.htm
Bernstein, M. A. & Rose, D. (1991). Psychosocial programming for the elderly who are
mentally ill. Psychosocial Rehabilitation Journal, 14(3), 3-15.
Björkman, T. & Hansson, L. (2000). What do case management do? An investigation of
case manger interventions and their relationship to client outcome. Journal of
Social Psychiatry and Psychiatric Epidemiology, 35, 43-50.
Björkman, T. & Hansson, L. (2002). Outcome of case management based on the
strengths model compared to standard care. A randomized controlled trial.
Journal of Social Psychiatry and Psychiatric Epidemiology, 37(4), 147-52.
Björkman, T. & Hansson, L. (2007). Case management for individuals with a severe
mental illness: a 6-year follow-up study. International Journal of Social
Psychiatry, 53(1), 12-22.
Björkman, T. Hansson, L., & Sandlund, M. (2002). Outcome of case management based
on the strengths model compared to standard care. A randomized controlled trial.
Journal of Social Psychiatry and Psychiatric Epidemiology, 37(4), 147-52.
Bryson, G. & Bell, M. (1997). The work behavior inventory: A scale for assessment of
work behavior for people with severe mental illness. Psychiatric Rehabilitation
Journal, 20(4), 47-56.

Case Management/SMI 44
Canuso, C. M. & Pandina, G. (2007). Gender and schizophrenia. Psychopharmacological
Bulletin, 40,178-90.
Carney, C. P., Jones, L., & Woolson, R. F. (2006). Medical comorbidity in women and
men with schizophrenia: a population-based controlled study. Journal of General
Internal Medicine 21, 1133-37.
Castle D., Sham, P., & Murray, R. (1998). Differences in distribution of ages of onset in
males and females with schizophrenia. Schizophrenia Research, 33, 179-83.
Chandler, D., Meisel, J., Hu, T. W., McGowen, M., & Madison, K. (1997). Client
outcomes in a three-year controlled study of an integrated service agency model.
Journal of Psychiatric Services, 47, 1337-43.
Crane-Ross, D., Roth, D., & Lauber, G. B. (2000). Consumers’ and case managers’
perceptions of mental health and community support service needs. Community
Mental Health Journal, 36, 161-78.
Department of Mental Health. (1999). Service planning. Commonwealth of
Massachusetts Regulations: 104 CMR 29.00 (pp. 385). Retrieved November 4,
2007 from http://www.mass.gov/Eeohhs2/docs/dmh/regs/reg_104cmr25.pdf
Diagnostic and statistical manual IV-TR. (2000). American Psychiatric Association:
Washington: DC.
Dixon, L., Postrado, L., Delahanty, J., Fisher, P. J., & Lehman, A. (1999). The
association of medical comorbidity in schizophrenia with poor physical and
mental health. The Journal of Nervous and Mental Disease, 187, 496-502.
Droulout, T. Liraud, F., & Verdoux, H. (2003). Relationship between insight and
medication adherence in subjects with psychosis. Encephale, 29, 430-37.
Case Management/SMI 45
Eaton, W. W. (1975). Marital status and schizophrenia. Acta Psychiatrica Scandinvica,
52, 320-329.
Fellowship Health Resources, Inc. (n.d.). Retrieved November 10, 2007, from
http://www.fellowshiphr.org/
Fellowship Health Resources, Inc. (2006). Fellowship clinical approach. Retrieved
November 10, 2007, from http://www.fellowshiphr.org/prismmodel.pdf.
Fellowship Health Resources, Inc. (2007). Quality Improvement Policy and Procedure
Manual. Chapter Care: Treatment planning guidelines (pp. 8). FHR author.
Reamer, G. F. (1999). Social work values and ethics (ed. 2nd), Research and evaluation
(pp. 156-7). New York: Columbia University Press.
Grob, N. G. (2000). Section 1: Looking ahead and reflecting upon the past. Retrieved
November 4, 2007 from
http://mentalhealth.samhsa.gov/publications/allpubs/SMA01-3537/chapter2.asp
Gureje, O. (1991). Gender and schizophrenia: age at onset and sociodemographic
attributes. Acta psychiatrica Scandinavica, 83, 402-05.
Hogan, T. P., Awad, A. G., & Eastwood, R. (1983). A self-report scale predictive of drug
compliance in schizophrenics: reliability and discriminative validity.
Psychological Medicines, 13, 177-83.
Hudson, T. J., Owen, R. R., Thrush, C. R., Han, X., Pyne, J. M., Thapa, P., & Sullivan,
G. (2004). A pilot study of barriers to medication adherence in schizophrenia.
Journal of Clinical Psychiatry, 65, 211-16.
Kessler, R. C., McGonagle, T. R., Zhoa, S., Nelson, C. B., Hughes, M., Eshleman, S.,
Wittchen, H., & Kendler, K. S. (1994). Lifetime and 12-month prevalence of

Case Management/SMI 46
DSM-III-R psychiatric disorders in the United States: Results from the National
Comorbidity Survey. Archives of General Psychiatry, 51, 8-19.
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995).
Posttraumatic stress disorder in the National Comorbidity Survey. Archives of
General Psychiatry, 52, 1048-60.
Kelly, A. T. (2002). A policymaker’s guide to mental illness. Retrieved October 26, 2007
from http://www.heritage.org/Research/HealthCare/BG1522.cfm.
Leung, A. & Chue, P. (2000). Sex differences in schizophrenia, a review of the literature.
Acta psychiatrica Scandinavica Suppl., 401, 3-38.
Lindamer, L. A., Lohr, J. B., Harris, M. J., McAdams, L. A., & Jeste, D. V. (1999).
Gender-related clinical differences in older patients with schizophrenia. Journal
of Clinical Psychiatry, 60, 61-67.
MAP. (2007). The Commonwealth of Massachusetts. Medication administration
program. Retrieved March 28, 2008 from
http://www.mass.gov/?pageID=eohhs2terminal&L=7&L0=Home&L1=Governme
nt&L2=Laws%2c+Regulations+and+Policies&L3=Department+of+Public+Healt
h+Regulations+%26+Policies&L4=Regulations+and+Other+Publications+-
+A+to+D&L5=Drug+Control&L6=Medication+Administration+Program+(MAP
)+Policies&sid=Eeohhs2&b=terminalcontent&f=dph_quality_drugcontrol_g_map
_policy_manual&csid=Eeohhs2
Marcus, S. C. & Olfson, M. (2008). Outpatient antipsychotic treatment and patient costs
of schizophrenia. Schizophrenia Bulletin, 34, 173-80.
Moriarty, P. J., Lieber, D., Bennett, A., White, L., Parrella, M., Harvey, P. D., & Davis,
Case Management/SMI 47
K. L. (2001). Gender differences in poor outcome patients with lifelong
schizophrenia. Schizophrenia Bulletin, 27, 103-13.
Mueser, T. K., Bond, R. G., & Drake, E. R. (2001). Community-based treatment of
schizophrenia and other severe mental disorders: treatment outcomes. Medscape
General Medicine 3(1), 1-24.
NAMI. (n.d). About mental illness. Retrieved October 26, 2007 from
http://www.nami.org/NASW. 1996. Code of Ethics. Washington, D.C.: author.
NIH. (n.d.). Community Mental Health Centers (CMHC) Act. Pubic Law 88-164 (1963)
(pp. 291). Retrieved November 4, 2007 from
http://history.nih.gov/01Docs/historical/documents/PL88-164.pdf
NIMH. (2007). How is schizophrenia treated? Retrieved October 17, 2007 from
http://www.nimh.nih.gov/health/publications/schizophrenia/summary.shtml
Phillips, E. S. (2003). A longitudinal examination of gender and ethnicity across two
models of community treatment for individuals with schizophrenia and related
disorders. Dissertation Abstracts International, A: The Humanities and Social
Science, 64, 2258-A-2259-A.
Piette, J. D., Heisler, M., Ganoczy, D., McCarthy, J. F., & Valenstein, M. (2007).
Differential medication adherence among patients with schizophrenia and
comorbid diabetes and hypertension. Psychiatric Services, 58, 207-12.
Pratt, S. & Mueser, K. T. (2004). Schizophrenia. In Anthony, M. M. & Barlow, D. H.
(Eds.), Handbook of assessment and treatment planning for psychological
disorders (pp. 375-414). New York: The Guilford Press.
Rubin, M. (2004). Multiple interventions and outcomes in Schizophrenia. Dissertation
Case Management/SMI 48
Abstracts International, A: The Humanities and Social Science, 65(4), 1543-A.
Salsberry, P. J., Chipps, E., & Kennedy, C. (2005). Use of general medical services
among Medicaid patients with severe and persistent medical illness. Psychiatric
Services, 56, 458-62.
Sokal J., Messias, E., Dickerson, F. B., Krevenbuhl, J., Brown C. H., Goldberg, R. W.,
& Dixon, L. B. (2004). Comorbidity of medical illnesses among adults with
serious mental illness who are receiving community psychiatric services. The
Journal of Nervous and Mental Disease, 192, 421-27.
Sun, S. X., Liu, G. G., Christensen, D. B., & Fu, A. Z. (2007). Review and analysis of
hospitalization costs associated with antipsychotic nonadherence in the treatment
of schizophrenia in the United States. Current Medical Research and Opinion, 23,
2305-12.
Tang, Y. L., Gillespie, C. F., Epstein, M. P., Mao, P. X., Jiang, F., Chen, Q., Cai, Z., J., &
Mitchell, P. B. (2007). Gender differences in 452 Chinese inpatients with
schizophrenia. Schizophrenia Research, 97(1-3), 88-96.
Yank, R. G., Bentley, J. K., & Hargrove, S. D. (1993). The vulnerability-stress model of
schizophrenia: Advances in psychosocial treatment. American Journal of
Orthopsychiatry, 63, 55-69.
Wu, E. Q., Birnbaum, H. G., Shi, L., Ball, D. E., Kessler, R. C., Moulis, M., & Aggarwal,
J. (2005). The economic burden of schizophrenia in the United States in 2002.
Journal of Clinical Psychiatry, 66, 1122-29.
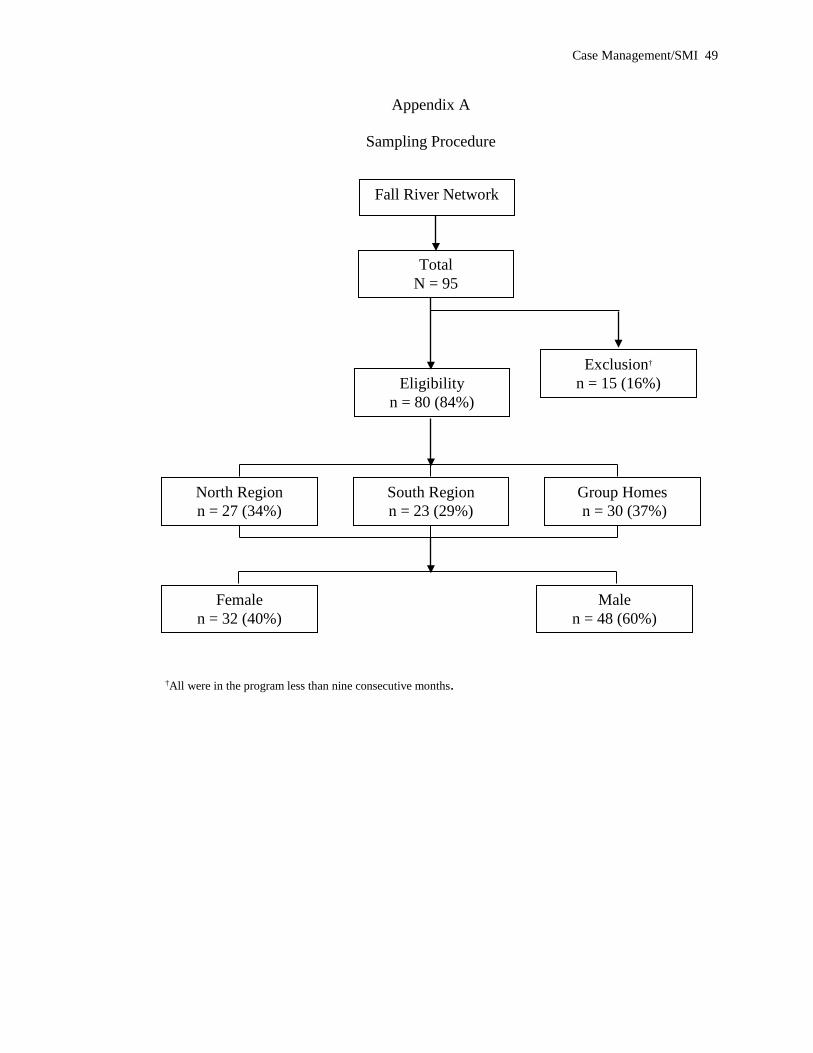
Case Management/SMI 49
Appendix A
Sampling Procedure
†All were in the program less than nine consecutive months.
Fall River Network
Eligibility n = 80 (84%)
Exclusion† n = 15 (16%)
Total N = 95
South Region n = 23 (29%)
North Region n = 27 (34%)
Group Homes n = 30 (37%)
Female n = 32 (40%)
Male n = 48 (60%)
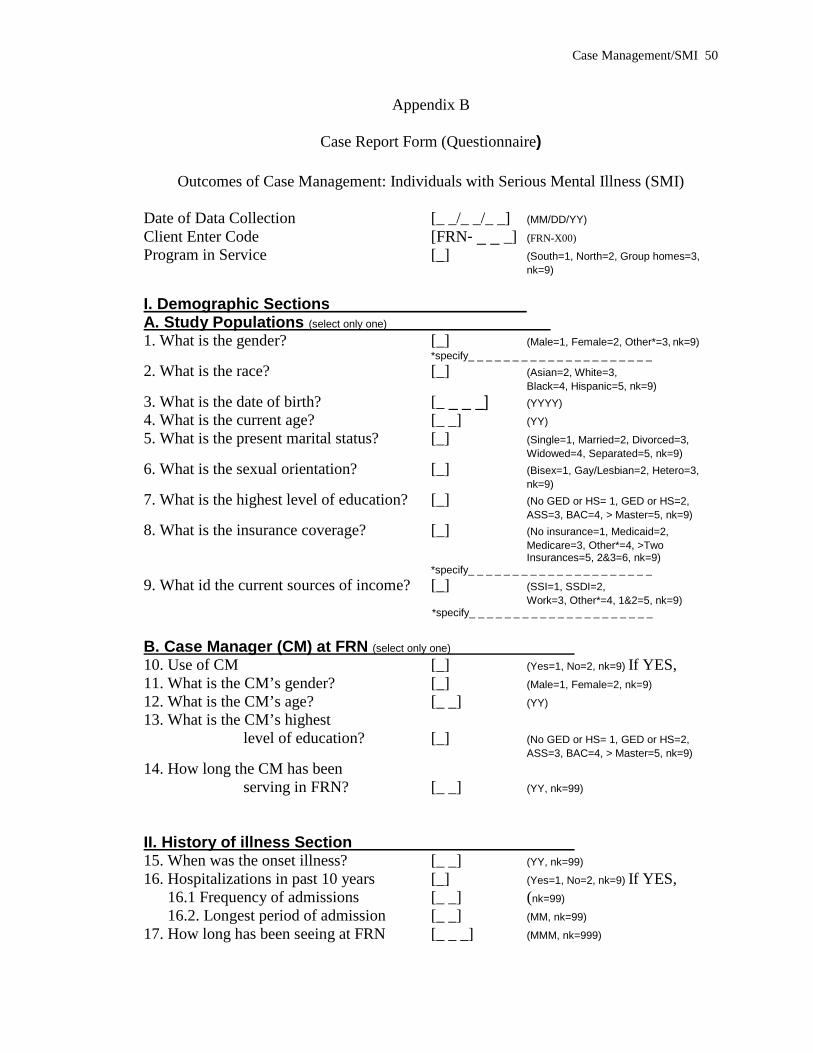
Case Management/SMI 50
Appendix B
Case Report Form (Questionnaire)
Outcomes of Case Management: Individuals with Serious Mental Illness (SMI) Date of Data Collection [_ _/_ _/_ _] (MM/DD/YY) Client Enter Code [FRN- _ _ _] (FRN-X00) Program in Service [_] (South=1, North=2, Group homes=3,
nk=9) I. Demographic Sections A. Study Populations (select only one) 1. What is the gender? [_] (Male=1, Female=2, Other*=3, nk=9) *specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ 2. What is the race? [_] (Asian=2, White=3,
Black=4, Hispanic=5, nk=9) 3. What is the date of birth? [_ _ _ _] (YYYY) 4. What is the current age? [_ _] (YY) 5. What is the present marital status? [_] (Single=1, Married=2, Divorced=3,
Widowed=4, Separated=5, nk=9) 6. What is the sexual orientation? [_] (Bisex=1, Gay/Lesbian=2, Hetero=3,
nk=9) 7. What is the highest level of education? [_] (No GED or HS= 1, GED or HS=2,
ASS=3, BAC=4, > Master=5, nk=9) 8. What is the insurance coverage? [_] (No insurance=1, Medicaid=2,
Medicare=3, Other*=4, >Two Insurances=5, 2&3=6, nk=9)
*specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ 9. What id the current sources of income? [_] (SSI=1, SSDI=2,
Work=3, Other*=4, 1&2=5, nk=9) *specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ B. Case Manager (CM) at FRN (select only one) 10. Use of CM [_] (Yes=1, No=2, nk=9) If YES, 11. What is the CM’s gender? [_] (Male=1, Female=2, nk=9) 12. What is the CM’s age? [_ _] (YY) 13. What is the CM’s highest
level of education? [_] (No GED or HS= 1, GED or HS=2, ASS=3, BAC=4, > Master=5, nk=9)
14. How long the CM has been serving in FRN? [_ _] (YY, nk=99)
II. History of illness Section 15. When was the onset illness? [_ _] (YY, nk=99) 16. Hospitalizations in past 10 years [_] (Yes=1, No=2, nk=9) If YES,
16.1 Frequency of admissions [_ _] (nk=99) 16.2. Longest period of admission [_ _] (MM, nk=99)
17. How long has been seeing at FRN [_ _ _] (MMM, nk=999)

Case Management/SMI 51
18. Has diagnosis on Axis I (SMI) [_] (Yes=1, No=2, nk=9) 18.1. If YES (check all applied)
a. Schizophrenia [_] (Yes=1, No=2, nk=9) b. Schizoaffective d/o [_] (Yes=1, No=2, nk=9) c. Bipolar I [_] (Yes=1, No=2, nk=9) d. Bipolar II [_] (Yes=1, No=2, nk=9) e. MDD [_] (Yes=1, No=2, nk=9)
f. PTSD [_] (Yes=1, No=2, nk=9) g. OCD [_] (Yes=1, No=2, nk=9) h. Other specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
19. Has diagnosis on Axis II [_] (Yes=1, No=2, nk=9; current) Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
20. Has diagnosis on Axis III (CMC**) [_] (Yes=1, No=2, nk=9; current)
(Numbers of CMC [_ _]) Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
21. Has diagnosis on Axis IV (PEP***) [_] (Yes=1, No=2, nk=9; current) Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yes, specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
22. Indicate Axis V (last GAF†) [_ _ _] 23. Current using psy meds [_] (Yes=1, No=2, nk=9)
23.1. Yes, numbers of psy meds [_ _] 23.2. Yes, numbers of mood/anti
depressed meds [_ _] 24. Current using non-psy meds [_] (Yes=1, No=2, nk=9)
24.1. Yes, numbers of non-psy meds [_ _] 25. Has health provider(s) [_] (Yes=1, No=2, nk=9)
25.1. Has seen by psychiatric(s) [_] (Yes=1, No=2, nk=9)
If Yes, numbers psychiatric(s) [_ _] 25.2. Has seen by PCP(s) [_] (Yes=1, No=2, nk=9)
If Yes, numbers PCP(s) [_ _] 25.3. Has seen by specialist(s) [_] (Yes=1, No=2, nk=9)
If Yes, numbers specialist(s) [_ _] ** CMC, Comorbid Medical Conditions *** PEP, Psychosocial & environmental problems †GAF, Global Assessment of Functioning III. Case Management Sections A. Type of Services (select only one) 26. Service1 [_] 27. Service2 [_] 28. Service3 [_] 29. Other (1) specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
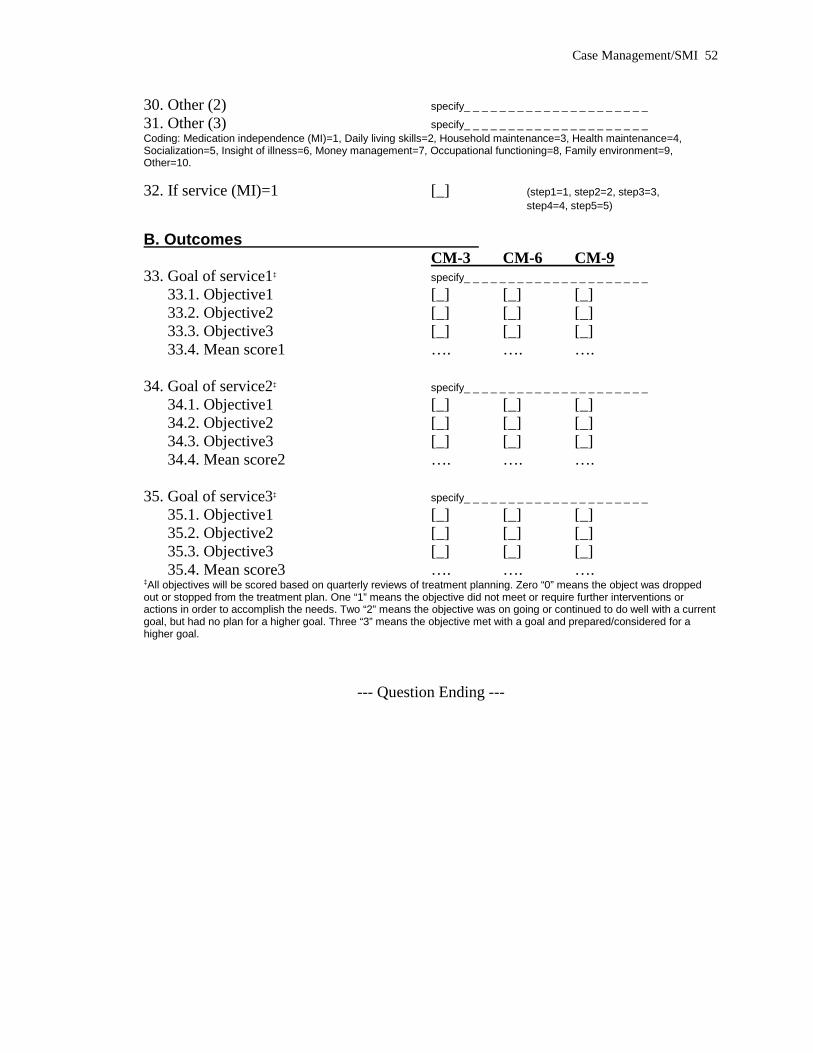
Case Management/SMI 52
30. Other (2) specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
31. Other (3) specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Coding: Medication independence (MI)=1, Daily living skills=2, Household maintenance=3, Health maintenance=4, Socialization=5, Insight of illness=6, Money management=7, Occupational functioning=8, Family environment=9, Other=10. 32. If service (MI)=1 [_] (step1=1, step2=2, step3=3, step4=4, step5=5) B. Outcomes CM-3 CM-6 CM-9 33. Goal of service1‡ specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
33.1. Objective1 [_] [_] [_] 33.2. Objective2 [_] [_] [_] 33.3. Objective3 [_] [_] [_] 33.4. Mean score1 …. …. ….
34. Goal of service2‡ specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
34.1. Objective1 [_] [_] [_] 34.2. Objective2 [_] [_] [_] 34.3. Objective3 [_] [_] [_] 34.4. Mean score2 …. …. ….
35. Goal of service3‡ specify_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
35.1. Objective1 [_] [_] [_] 35.2. Objective2 [_] [_] [_] 35.3. Objective3 [_] [_] [_] 35.4. Mean score3 …. …. ….
‡All objectives will be scored based on quarterly reviews of treatment planning. Zero “0” means the object was dropped out or stopped from the treatment plan. One “1” means the objective did not meet or require further interventions or actions in order to accomplish the needs. Two “2” means the objective was on going or continued to do well with a current goal, but had no plan for a higher goal. Three “3” means the objective met with a goal and prepared/considered for a higher goal.
--- Question Ending ---

Case Management/SMI 53
Appendix C

Case Management/SMI 54

Case Management/SMI 55


















