Sclerosing Cholangitis Associated with Hypereosinophilic ...
4
CASE REPORT Sclerosing Cholangitis Associated with Hypereosinophilic Syndrome Naomi Ichikawa, Atsuo Taniguchi, Hideto Akama, Hisataka Ishiguro*, Takeshi Kurihara*, Chihiro Terai, Masako Hara and Sadao Kashiwazaki A 15-year-old male with hypereosinophilic syndromewas admitted to our hospital because of general malaise and abnormal liver function tests. Endoscopic retrograde cholangiopancreatography demonstrated bile duct changes consistent with primary sclerosing cholangitis. The patient's liver profile tests returned to normal after treatment with prednisolone and ursodeoxycholic acid. In this case, eosinophils might have played an important role in the pathogenesis of the bile duct lesion. (Internal Medicine 36: 561-564, 1997) Key words: eosinophilia, endoscopic retrograde cholangiopancreatography (ERCP), corticoste- roid, ursodeoxycholic acid (UDCA) Introduction Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disorder of unknown origin, and there is no effective treatment for this disease at present (1). Onrare occasions the bile duct lesion consistent with PSC is associated with hypereosinophilic syndrome (HES), and the significance of this association deserves attention from the standpoint of patho- physiology and therapy of PSC. Wepresent here a case of sclerosing cholangitis with HES, successfully treated with corticosteroid and ursodeoxycholic acid (UDCA). Other cases hitherto reported in the literature are briefly reviewed. Case Report A 15-year-old male was admitted to a local hospital on the basis of general malaise. The patient had been well until 13 years of age when he developed untypical feelings of fatigue and anorexia. Evaluation showed lymphadenopathy and hepatomegaly. Laboratory data at that time included white blood cell (WBC) 9,900/mm3 with 45% eosinophils, absolute eosinophils 4,455/mm3, aspartate aminotransferase (AST) 25 1 IU//, alanine aminotransferase (ALT) 236 IU//, alkaline phos- phatase 1,304 IU// (normal 66-220 IU//), y-glutamyl transpeptidase 308 mU/ml (normal <60 mU/ml) and total bilirubin 1.6 mg/dl. Stools were negative for ova and parasites. He was not taking any medications and no evidence of allergies was found serologically. Bone marrow aspiration showed a normal myeloid-erythroid ratio and eosinophilia; there was no excess of blasts. During the next 6 months, eosinophils rose to a peak of 6,882/mm3. A diagnosis of HES (2) with hepatic involvement was made and the patient was treated with pred- nisolone (60 mg/day). The dose ofprednisolone was tapered as symptoms improved with the return of WBC toward normal. The levels of AST, ALT, alkaline phosphatase and y-glutamyl transpeptidase decreased to 53 IU//, 52 IU//, 247 IU// and 242 mU/ml, respectively. When prednisolone was discontinued, the general malaise reappeared and he was transferred to our hospital (July 25, 1995). Onadmission to our hospital, physical examination revealed a temperature of 37.4°C, no jaundice, no lymphadenopathy, mild hepatomegaly, and no splenomegaly. Neurological ex- amination was not remarkable. Laboratory tests on admission showed WBC5,400/mm3 with 18.5% eosinophils, absolute eosinophils 999/mm3. Electrolytes, blood urea nitrogen (BUN), creatinine and glucose were normal. The ASTwas 77 IU//, ALT 120 IU//, lactate dehydrogenase (LDH) 264 U, alkaline phos- phatase 1,246 mU/ml (normal 100-280 mU/ml), y-glutamyl transpeptidase 203 mU/ml, total bilirubin 1.2 mg/ml, and amy- lase 191 mU/ml. Total protein was 6.8 g/dl with no hypergammaglobulinemia. Immunoglobulin E (IgE) was 55 U/ ml (normal 43-303 U/ml). The level of eosinophil protein X (EPX) was 59.3 ng/ml [normal 1 1.43±2.46 ng/ml (3)] with akit for EPX radioimmunoassay (Pharmacia AB, Uppsala, Swe- From the Department of Rheumatology, Institute of Rheumatology, Tokyo Women's Medical College and *the Aoyama Hospital, Tokyo Women's Medical College, Tokyo Received for publication August 26, 1996; Accepted for publication April 25, 1997 Reprint requests should be addressed to Dr. Naomi Ichikawa, the Department of Rheumatology, Institute of Rheumatology, Tokyo Women's Medical College, KS Bldg , 9-12, Wakamatsu-cho, Shmjuku-ku, Tokyo 162 Internal Medicine Vol. 36, No. 8 (August 1997) 561
Transcript of Sclerosing Cholangitis Associated with Hypereosinophilic ...

CASE REPORT
Sclerosing Cholangitis Associated withHypereosinophilic Syndrome
Naomi Ichikawa, Atsuo Taniguchi, Hideto Akama, Hisataka Ishiguro*,Takeshi Kurihara*, Chihiro Terai, Masako Hara and Sadao Kashiwazaki
A 15-year-old male with hypereosinophilic syndromewas admitted to our hospital because ofgeneral malaise and abnormal liver function tests. Endoscopic retrograde cholangiopancreatographydemonstrated bile duct changes consistent with primary sclerosing cholangitis. The patient's liverprofile tests returned to normal after treatment with prednisolone and ursodeoxycholic acid. In thiscase, eosinophils might have played an important role in the pathogenesis of the bile duct lesion.(Internal Medicine 36: 561-564, 1997)
Key words: eosinophilia, endoscopic retrograde cholangiopancreatography (ERCP), corticoste-roid, ursodeoxycholic acid (UDCA)
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestaticliver disorder of unknown origin, and there is no effective
treatment for this disease at present (1). Onrare occasions thebile duct lesion consistent with PSC is associated withhypereosinophilic syndrome (HES), and the significance of thisassociation deserves attention from the standpoint of patho-physiology and therapy of PSC. Wepresent here a case ofsclerosing cholangitis with HES, successfully treated withcorticosteroid and ursodeoxycholic acid (UDCA). Other caseshitherto reported in the literature are briefly reviewed.
Case ReportA 15-year-old male was admitted to a local hospital on thebasis of general malaise. The patient had been well until 13years of age when he developed untypical feelings of fatigueand anorexia. Evaluation showed lymphadenopathy and
hepatomegaly. Laboratory data at that time included whiteblood cell (WBC) 9,900/mm3 with 45% eosinophils, absoluteeosinophils 4,455/mm3, aspartate aminotransferase (AST) 25 1IU//, alanine aminotransferase (ALT) 236 IU//, alkaline phos-phatase 1,304 IU// (normal 66-220 IU//), y-glutamyl
transpeptidase 308 mU/ml (normal <60 mU/ml) and totalbilirubin 1.6 mg/dl. Stools were negative for ova and parasites.He was not taking any medications and no evidence of allergies
was found serologically. Bone marrow aspiration showed anormal myeloid-erythroid ratio and eosinophilia; there was noexcess of blasts. During the next 6 months, eosinophils rose toa peak of 6,882/mm3. A diagnosis of HES (2) with hepaticinvolvement was made and the patient was treated with pred-nisolone (60 mg/day). The dose ofprednisolone was tapered assymptoms improved with the return of WBCtoward normal.The levels of AST, ALT, alkaline phosphatase and y-glutamyltranspeptidase decreased to 53 IU//, 52 IU//, 247 IU// and 242mU/ml, respectively. Whenprednisolone was discontinued,the general malaise reappeared and he was transferred to ourhospital (July 25, 1995).Onadmission to our hospital, physical examination revealeda temperature of 37.4°C, no jaundice, no lymphadenopathy,mild hepatomegaly, and no splenomegaly. Neurological ex-amination wasnot remarkable. Laboratory tests on admissionshowed WBC5,400/mm3 with 18.5% eosinophils, absoluteeosinophils 999/mm3. Electrolytes, blood urea nitrogen (BUN),creatinine and glucose were normal. The ASTwas 77 IU//, ALT120 IU//, lactate dehydrogenase (LDH) 264 U, alkaline phos-phatase 1,246 mU/ml (normal 100-280 mU/ml), y-glutamyltranspeptidase 203 mU/ml, total bilirubin 1.2 mg/ml, and amy-lase 191 mU/ml. Total protein was 6.8 g/dl with no
hypergammaglobulinemia. Immunoglobulin E (IgE) was 55 U/ml (normal 43-303 U/ml). The level of eosinophil protein X(EPX) was 59.3 ng/ml [normal 1 1.43±2.46 ng/ml (3)] with akitfor EPX radioimmunoassay (Pharmacia AB, Uppsala, Swe-
From the Department of Rheumatology, Institute of Rheumatology, Tokyo Women's Medical College and *the AoyamaHospital, Tokyo Women's MedicalCollege, Tokyo
Received for publication August 26, 1996; Accepted for publication April 25, 1997Reprint requests should be addressed to Dr. Naomi Ichikawa, the Department of Rheumatology, Institute of Rheumatology, Tokyo Women's Medical College,
KS Bldg , 9-12, Wakamatsu-cho, Shmjuku-ku, Tokyo 162
Internal Medicine Vol. 36, No. 8 (August 1997) 561

Ichikawa et al
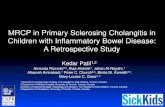
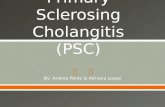
den). A test for antinuclear antibody was weakly positive in atiter of 1 :40 with a homogeneous pattern; antimitochondrialand antismooth muscle antibodies, as well as antineutrophilcytoplasmic antibody, were negative. AFPand carcino-embry-onic antigen (CEA) were within normal limits. Hepatitis Bsurface (HBs) antigen and antihepatitis C antibody were nega-tive. A computed tomography (CT) scan of the abdomenrevealed hepatosplenomegaly and intrahepatic biliary dilata-tion. Colonoscopy showed hyperplastic lymph follicles in thececumand ascending colon. Histologic examinationshowedslightly inflamed colonic mucosa with moderate infiltrationof eosinophils. An endoscopic retrograde cholangiopancreato-graphy (ERCP) (Fig. 1) revealed extensive irregularities in thewall of the intrahepatic bile ducts. Extrahepatic bile duct andgallbladder were normal. There was no evidence of choledo-cholithiasis nor of congenital abnormalities. The picture wasconsistent with PSC.A diagnosis ofsclerosing cholangitis with HESwas based onthese observations, and therapy was started with intravenousmethylprednisolone (300 mg/day) for three days followed byprednisolone (30 mg/day) and UDCA (1,200 mg/day). Allsymptoms, abnormal liver function tests and eosinophilia dis-appeared after two months. One year later, the patient is takingprednisolone (9 mg/day) and remains completely asympto-matic with normal WBCand liver function tests (Fig. 2). Thelevel of EPXalso returned to normal.
Figure 1. Endoscopic retrograde cholangiogram showingdiffuse irregular appearance of the intrahepatic bile ducts.
July, 1995 Aug. Sept. Oct. Nov.
UDCA ' i ' ' '
1,200mg/day' _ ; " " " å
30mg/day
General malaise (BB^^__Eosinophil 2,000- «L (^2000
(/mm3) - /\^ - '1,000 -à" *s^ - 1,000
oJ V-#-à"-à"à"-o à" à"Lo
ALp 1'500 1#^A_ r 1,500(mU/ml) 1,000-^^ ^^ -1,000500- ^^^^^ m -500
oJ à""^-^- . . [0
7-GTP 200 -] à"-à"--à" P 200(mU/ml) j ^^^à"^^^
Figure 2. Clinical course of the patient.UDCA:ursodeoxycholic acid, mPSL:methylprednisolone (arrows), PSL: prednisolone.
562Internal Medicine Vol. 36, No. 8 (August 1997)

Sclerosing Cholangitis with HES
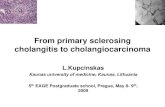
Ca s e re po r t (y ea r) A g e / S e x E o s m o p h i l ( / m m ) C o m p lic a tio n T re a tm e n t P ro g n o sis R e fer en c e
M ir-M a d jle ss i et a l ( 19 8 6 ) 2 6 /M 6 ,4 9 6 u c P S L I m p r o v e d ( 4 )N e e m a n e t a l ( 1 9 8 7 ) 5 5 /M 1 ,9 0 0 N o n e N D N D (5 )K a g a w a e t a l ( 1 9 8 8 ) 6 8 /F 2 ,9 7 5 a N o n e P S L Im p ro v e d (6 )S c h e u r l e n e t a l ( 1 9 9 2 ) 2 8 /M 5 ,0 5 7 a IB D H y d ro x y u re a Im p ro v e d (7 )G r a u e r e t a l ( 1 9 9 3 ) 4 1/M l ,6 4 7 a C h o l e c y s t i t i s P S L , U D C A I m p r o v e d O ( 8 )Sc h o o n b r o o d t e t a l ( 1 9 9 5 ) >0 /M 1 ,4 1 1 E G , c o l i t i s P S L Im p ro v e d O (9 )P r e s e n t c a s e ( 1 9 9 6 ) 1 5 /M 6 ,8 8 2 a N o n e P S L , U D C A I m p r ov e d
aHES was diagnosed, bthe patient died of cholangiocarcmoma and pulmonary embolism 3 years later, improvement wasconfirmed by repeated ERCP, UC: ulcerative colitis, IBD: inflammatory bowel disease, EG: eosinophilic gastroenteritis,PSL: prednisolone, ND:not described, UDCA:ursodeoxycholic acid.
Discussion
HESis a disorder marked by a sustained overproduction ofeosinophils and multisystem organ dysfunction. The presentpatient meets the diagnostic criteria for HESproposed by Fauciet al (2). In HES, involvement of heart, lungs and nervoussystem are usually present, but sclerosing cholangitis associ-ated with HEShas rarely been reported. The patient in thepresent study was diagnosed as having sclerosing cholangitison the basis ofa cholestatic biochemical profile and the cholan-giographic picture. Details on 6 previously reported (4-9) casesof sclerosing cholangitis with eosinophilia are listed in Table 1.In every case, the ERCPfinding was consistent with PSC. Threeof the 6 cases were recognized as having HES. In the casereported by Mir-Madjlessi et al (4), coexistence with
cholangiocarcinomaadded confusion to the association. Graueret al (8) termed their case 'eosinophilic sclerosing cholangitis'since the patient had bile duct involvement on ERCP consistentwith PSC and eosinophilic infiltration of bile ducts seen on liverbiopsy. In these cases, as well as in ourpatient, eosinophils mayplay an important role in the pathogenesis of bile duct involve-ment.The organ damage in HESis thought to be mediated byeosinophil granule contents such as eosinophil cationic protein,eosinophil peroxidase, major basic protein (MBP) and EPX.Each can exert toxicities on host cells. Foong et al (10) reporteda case of HESassociated with eosinophil-induced chronicactive hepatitis. Using an antibody against MBPand immuno-histological staining, they showed that activated, degranulatingeosinophils had infiltrated into areas ofhepatocyte injury. Theirdata might suggest an etiological role for eosinophils as a causefor the liver lesion. In the presentpatient, we found an increasedlevel of EPX(59.3 ng/ml). Since EPXpossesses markedribonuclease activity and is thought to play a pathogenic role inthe tissue damage of HES, eosinophil granule proteins such asEPXmay have been partially responsible for the establishmentof the bile duct lesion in our patient.
A variety of immunosuppressive, antiinflammatory,
antifibrotic agents have been used to treat PSC but to date notherapy routine has been universally effective. However, a
prompt response to prednisolone was shownby our patient aswell as by most of the cases listed in Table 1. Furthermore, inthe cases reported by Grauer et al (8) and Schoonbroodt et al (9),improvementof the bile duct lesion was confirmed by repeatedERCP(Table 1). Such a dramatic response to corticosteroidmay suggest that the bile duct involvement of these patients isclosely related to eosinophilia.UDCAwas added to prednisolone in view of its efficacy forpatients with chronic cholestatic liver disorders. UDCAmightbe effective to someextent in the present case because UDCAmight displace toxic hydrophobic bile acids from both the bileacid pool and hepatocyte membranes, thereby protecting thehepatocytes ( 1 1). However, immunomodulatoryproperties ofUDCAare a current topic and recently Tanaka et al (12) haveshown the therapeutic kinship between UDCA andglucocorticoids. It might be interesting to note that the
immunomodulatoryproperties of UDCAare, at least in part,shared by glucocorticoids.In conclusion, wereport here a case ofsclerosing cholangitisassociated with HES. It is important to recognize the existenceof a subgroup of patients with sclerosing cholangitis associatedwith eosinophilia that may respond to corticosteroid.
Acknowledgements: We thank Dr M. W. Schein for useful comments onthe manuscript.
References
1) Lee YM, KaplanMM. Primary sclerosing cholangitis. NEngl JMed332:924, 1995.
2) Fauci AS, Harley JB, Roberts WC, Ferraris VJ, Gralnick HR, BjornsonBHNIHConference. The ldiopathic hypereosinophilic syndrome. Clini-cal, pathophysiologic, and therapeutic considerations Ann Intern Med
97: 78, 1982.
3) Tomassini M, Magnni L, Bonini S, Lambiase A, Bonini S Increasedserum levels ofeosinophil catiomc protein and eosinophil-denved neuro-
toxin (protein X) in vernal keratoconjunctivitis. Ophthalmology 101:808, 1994.
4) Mir-Madjlessi SH, Sivak MVJr, Farmer RG. Hypereosinophiha, ulcera-tive colitis, sclerosing cholangitis, and bile duct carcinoma. Am JGastroenterol 81: 483, 1986.
5) Neeman A, Kadish U. Marked eosinophiha in a patient with primarysclerosing cholangitis Am J Med 83: 378, 1987 (letter)
Internal Medicine Vol. 36, No. 8 (August 1997) 563
Tablel・ReportedCasesofScleroslngCholangitiswithEosinophilia●

Ichikawa et al
Kagawa K, Suematsu M, Miura S, Komatsu H, Oda M, Tsuchiya M. Acase of primary sclerosing cholangitis with marked eosinophilia.
Sogorinsho 37: 2339, 1988 (in Japanese).Scheurlen M, Mork H, Weber P. Hypereosinophilic syndrome resem-bling chronic inflammatory bowel disease with primary sclerosing cholan-gitis. J Clin Gastroenterol 14: 59, 1992.Grauer L, Padilla III VM, Bouza L, Barkin JS. Eosinophilic sclerosing
cholangitis associated with hypereosinophilic syndrome. Am JGastroenterol 88: 1764, 1993.
Schoonbroodt D, Horsmans Y, Laka A, Geubel AP, Hoang P. Eosi-nophilic gastroenteritis presenting with colitis and cholangitis. Dig Dis
Sci 40: 308, 1995.
Foong A, Scholes JV, Gleich GJ, Kephart GM, Holt PR. Eosinophil-induced chronic active hepatitis in the idiopathic hypereosinophilicsyndrome. Hepatology 13: 1090, 1991.Heuman DM, Pandak WM,Hylemon PB, Vlahcevic ZR. Conjugates ofursodeoxycholate protect against cytotoxicity of more hydrophobic bilesalts : in vitro studies in rat hepatocytes and humanerythrocytes. Hepatology14: 920, 1991.
Tanaka H, Makino Y, Miura T, Hirano F, Okamoto K, Komura K, SatoY, Makino I. Ligand-independent activation of the glucocorticoid receptorby ursodeoxycholic acid. Repression of IFN-y-induced MHCclass IIgene expression via a glucocorticoid receptor-dependent pathway. JImmunol 156: 1601, 1996.
564 Internal Medicine Vol. 36, No. 8 (August 1997)